

When Mad in America received a notice this past June that Joanna Moncrieff, Mark Horowitz, and colleagues would soon publish a paper concluding that there were no research findings that supported the low-serotonin hypothesis of depression, I initially wondered whether we should bother to report on it. Mad in America readers know well that the low-serotonin theory had long ago been debunked, with numerous articles on our site telling of that fact, and so I quipped to other MIA staff that reviewing the article would be like “beating a dead horse.”
But such is our little cocoon here at Mad in America. For much of the mainstream media, their paper made for a stunning finding. In print, radio, and television, the paper has been described as a “landmark” finding, as a “game changer” and so forth, the media telling of how it has shaken up accepted wisdom about antidepressants and “how they work.”
This was rather amusing, I thought, as the exclamations of surprise revealed the media’s utter failure regarding their reporting on psychiatry for the past decades. Their surprise served as a tacit confession that they had been publishing propaganda for some time.
Then, as psychiatrists publicly commented on the paper, a second confession appeared, this one indeed of “landmark” importance. Their comments serve as an admission that, for the past several decades, their profession committed medical fraud. And I am using that term in its legal sense.
As Moncrieff and colleagues noted, there is a long line of research that failed to find evidence supporting the low-serotonin theory of depression. What was new about their work was that they performed a comprehensive review of this research, looking at the different “types” of studies that had been done, and finding that all had failed to produce evidence supporting the theory. In response, a number of prominent psychiatrists in the UK and the United States dismissed the paper as old news. Here is a sampling:
From UK psychiatrists:
“The findings from this review are really unsurprising. Depression has lots of different symptoms and I don’t think I’ve met any serious scientists or psychiatrists who think that all causes of depression are caused by a simple chemical imbalance in serotonin.” —Michael Bloomfield, University College London (UCL)
“This paper does not present any new findings but just reports results which have been published elsewhere and it is certainly not news that depression is not caused by ‘low serotonin levels.'” —David Curtis, UCL Genetics Institute
From US psychiatrists:
“Nothing is new here. And the fuss surrounding the paper reveals much ignorance about psychiatry. The serotonin hypothesis of depression which became popular from the 1990s until now, is false, and has known to be false for a long time, and never was proven to begin with.” —Nassir Ghaemi, Tufts University School of Medicine
“When I was doing research for [my] book, I was reading the same studies that I am sure that Dr. Moncrieff and colleagues read, which were basically saying that there’s no direct evidence of a serotonin deficiency. So it’s not really new.” —Daniel Carlat, publisher of the Carlat Psychiatry Report
The psychiatrists making these comments are correct. The psychiatric research community has long known that the low-serotonin theory didn’t pan out and that, in fact, the field long ago moved on to new theories about the possible pathology that gives rise to depression. Yet, as is easy to show, the American Psychiatric Association, in concert with pharmaceutical companies, promoted the low-serotonin theory to the public long after the low-serotonin theory had been found to be without merit. Scientific advisory councils populated by professors of psychiatry at prestigious medical schools also signed off on such pronouncements by non-profit advocacy associations, and in that manner, share culpability for telling this “falsehood” to the public.
That fraudulent story-telling worked, in the sense of deluding the public. As Moncrieff and colleagues noted, surveys in recent years found that 85% to 90% of the public believed that low serotonin was the cause of depression, and that antidepressants helped fix that imbalance.
There you have the basis for a class action lawsuit: the psychiatric community long ago knew that the low-serotonin story of depression hadn’t panned out, yet the American Psychiatric Association, pharmaceutical companies, and scientific advisory councils told the public otherwise, and this created a societal belief in that false story. The surveys prove that many millions of patients acted upon that falsehood and incorporated it into their sense of self.
The Legal Standard for Medical Fraud
In the wake of World War II, the discovery of Nazi medical experiments on Jewish prisoners and the mentally ill led to the principle, codified in law in the United States, of the duty to provide volunteers in research studies with informed consent. Potential study subjects need to be informed about the risks of a study before they can give consent.
In the 1950s and 1960s, this principle of informed consent was extended to ordinary medical care. The principle is grounded in the concept of personal autonomy: the individual has a right to self-determination. A 1972 landmark case in federal court, Canterbury v. Spence, ruled that providing patients with informed consent was not just an ethical obligation, but a legal one. The court wrote:
“The patient’s right of self-decision shapes the boundaries of the duty to reveal. That right can be exercised only if the patient possesses enough information to enable an intelligent choice.”
The court also set forth a standard for assessing whether this legal obligation had been met: “What would a reasonable patient want to know with respect to the proposed therapy and the dangers that may be inherently or potentially involved?”
While it is the physician or medical caregiver who is required to obtain the informed consent of the patient, this legal standard clearly imposes an ethical duty, by proxy, on the medical specialty that provides individual physicians with the information that should be disclosed. The medical specialty must provide physicians with the best possible accounting of the risks and benefits of any proposed therapy, and in its communications to the public, do the same.
The diagnosis of a disease is obviously a first step in obtaining informed consent. What is the illness that needs to be treated? If the presenting symptoms do not lead to a diagnosis with a known pathology, that is okay—the absence of knowledge helps inform the patient’s decision-making. If it isn’t understood why a drug works, that is okay too. Once again, the absence of knowledge helps inform the patient’s decision-making. At that point, the patient can focus on the risks and benefits of the proposed treatment: what have clinical studies shown?
The chemical imbalance story violated those principles at every step. Patients were informed that they had a known pathology, and that an antidepressant fixed that pathology. That was a story of an antidote to a disease, and thus was a medically necessary treatment. If a patient didn’t take the antidepressant, he or she could expect to continue to suffer from depression.
This isn’t simply a failure to give patients the information needed to make an “informed choice.” Instead, from a legal standpoint, this is a case of a patient being told a lie.
Here is how one Arizona law firm describes the legal consequences for a doctor that lies to a patient:
“You can sue your doctor for lying, provided certain breaches of duty of care occur. A doctor’s duty of care is to be truthful about your diagnosis, treatment options, and prognosis. If a doctor has lied about any of this information, it could be proof of a medical malpractice claim. The law considers it medical negligence if a doctor fails to provide the truth for informed consent, which may also bring a battery lawsuit.”
Medical malpractice is the charge if the action was due to negligence; medical battery requires the action to be intentional. Here is how a Washington D.C. law firm describes medical battery:
“When you visit a doctor and they prescribe a treatment or procedure, an essential element is your consent. You have the right to know what will be done to you, to learn the risk or potential side effects of a procedure, and to be informed of any alternative treatment options available to you . . . Medical battery occurs when the doctor or other medical professional violates your right to decide what kinds of medical treatments you will receive and which you do not wish to receive.”
The FDA, of course, approved the prescribing of antidepressants for depression. And it may be that many individual prescribers who told their patients that antidepressants fixed a chemical imbalance thought that was true. They believed they were providing patients with “informed consent.”
As such, in this instance of the chemical-imbalance story, the medical malpractice and battery can be understood as not necessarily originating in the doctor-patient interaction, but rather in the telling of a false story to the public by the American Psychiatric Association (APA) and pharmaceutical companies that knowingly promoted this falsehood. The academic psychiatrists that served on the scientific advisory boards of non-profit advocacy organizations that peddled this story share in this collective guilt.
The Trail of Fraud
As is well-known, the low-serotonin theory of depression had its roots in findings, dating back to the 1960s, that the first generation of antidepressants, tricyclics and monoamine oxidase inhibitors, both prevented the usual removal of neurotransmitters known as monoamines from the synaptic cleft between neurons. This led researchers in the 1965 to hypothesize that a deficit in monamines could be a cause of depression.
Once this hypothesis was floated, researchers then sought to determine whether if patients with depression actually suffered from a monamine deficiency. It’s a history of one negative finding after another.
As early as 1974, researchers concluded that all such studies up to that time indicated that “the depletion of brain norepinephrine, dopamine, or serotonin is in itself not sufficient to account for the development of the clinical syndrome of depression.” This was the first round of findings, and after that there was speculation that a monoamine deficit might be present in a subset of depressed patients (as opposed to being a pathology common to all such patients.) In 1984, the NIMH conducted a study to investigate that possibility. Once more, the bottom-line findings were negative, which led the NIMH researchers to conclude that “elevations or decrements in the functioning of serotonergic systems per are not likely to be associated with depression.”
At that point, the hypothesis had been around for nearly two decades and found to be wanting. In the research community, there was a sense that the hypothesis had always presented an overly reductive picture of how the brain functioned, and thus it wasn’t a surprise that research had failed to support the hypothesis. Even so, after that 1984 report, investigators continued to study whether depressed patients suffered from low serotonin, with this research quickening after Prozac arrived on the market in 1988. Many different investigative methods were tried, but once again, the results were negative. The hypothesis was officially buried by the American Psychiatric Association in 1999, when it published the third edition of its Textbook of Psychiatry. The authors of a section on mood disorders even pointed out the faulty logic that had led to the chemical imbalance theory of depression in the first place. They wrote:
“The monoamine hypothesis, which was first proposed in 1965, holds that monoamines such as norepinephrine and 5-HT [serotonin] are deficient in depression and that the action of antidepressants depends on increasing the synaptic availability of these monoamines. The monoamine hypothesis was based on observations that that antidepressants block reuptake inhibition of norepinephrine, 5-HT, and/or dopamine. However, inferring neurotransmitter pathophysiology from an observed action of a class of medications on neurotransmitter availability is similar to concluding that because aspirin causes gastrointestinal bleeding, headaches are caused by too much blood and the therapeutic action of aspirin in headaches involves blood loss. Additional experience has not confirmed the monoamine depletion hypothesis.”1
Other experts in the field echoed this point in the next few years. In his 2000 textbook Essential Psychopharmacology, psychiatrist Stephen Stahl wrote that “there is no clear and convincing evidence that monamine deficiency accounts for depression; that is, there is no ‘real’ monoamine deficit.”2
More such confessions appeared in the research literature, and finally, in a 2010 paper, Eric Nestler, famous for his work on the biology of mental disorders, detailed how the many types of inquiries into the low-serotonin theory had all come to the same conclusion:
“After more than a decade of PET studies (positioned aptly to quantitatively measure receptor and transporter numbers and occupancy), monoamine depletion studies (which transiently and experimentally reduce brain monoamine levels), as well as genetic association analyses examining polymorphisms in monoaminergic genes, there is little evidence to implicate true deficits in serotonergic, noradrenergic, or dopaminergic neurotransmission in the pathophysiology of depression. This is not surprising, as there is no a priori reason that the mechanism of action of a treatment is the opposite of disease pathophysiology.”
This is the research history that psychiatrists today, when asked to comment about Moncrieff’s paper, are referring to when they state, “there is nothing new here.” They are right. The theory was abandoned long ago. In a 2011 blog, Ronald Pies, editor of Psychiatric Times, put it this way: “In truth, the ‘chemical imbalance’ notion was always a kind of urban legend—never a theory seriously propounded by well-informed psychiatrists.”
From a legal standpoint, the APA’s publication of the third edition of its Textbook of Psychiatry in 1999 is the pivotal moment in this history. Up until that time, the argument could be made that while the biology of depression remained unknown, one hypothesis was that it was due to low serotonin, and that there were still efforts to see if that might be true. However, after that date, the APA, the pharmaceutical companies, and the academic psychiatrists that populated the scientific advisory councils had an obligation to inform the public that the low-serotonin theory had not panned out. If instead these three groups informed the public that depressed patients suffered from a chemical imbalance that could be fixed by a drug, they were knowingly telling the public a lie, and thus, by informed consent standards, they were abetting medical malpractice and the medical battery of patients.
And it’s easy to document that is exactly what the APA, the pharmaceutical companies, and the scientific advisory boards did.
The APA’s Promotion of the Chemical Imbalance Story
The APA’s promotion of the chemical imbalance theory of mental disorders can be traced back to 1980, when it published the third edition of its Diagnostic and Statistical Manual. That publication is regularly characterized as a transformative moment for American psychiatry, as this was when the APA adopted a “disease” model for diagnosing and treating psychiatric disorders.
There were no scientific findings that spurred this transformation. The scientific impulse that was present arose from the failure of DSM II: the diagnoses in that edition were understood to “lack reliability and validity.” That led a team of researchers at Washington University in St. Louis to advocate that psychiatry should start fresh: it could develop categories for grouping patients with like symptoms, with the hope that subsequent research would “validate” the groupings as real diseases. DSM II would be abandoned, and new categories would be drawn up for research purposes.
However, during the 1970s, APA leaders spoke of how, in the face of various criticisms, psychiatry was fighting for its survival. Its diagnostic manual was understood to lack validity; psychologists and counselors were offering talk therapies that appeared to be as effective as psychoanalysis; One Flew Over the Cuckoo’s Nest depicted staff in mental hospitals as the truly crazy ones; and an “antipsychiatry” movement described psychiatry as an agency of social control.
The criticism that stung the most was that psychiatrists were not “real doctors.” There was an obvious solution that beckoned: if they adopted a disease model, they could present themselves as physicians who treated real diseases. This would enable them to don the “white coat”—both figuratively and literally—that society recognized as the garb of “real” doctors.
DSM III, said APA president Jack Weinberg in 1977, would “clarify to anyone who may be in doubt that we regard psychiatry as a specialty of medicine.”3
Once DSM III was published, the APA set out to market its new disease model to the public. In 1981, it established a “division of publications and marketing” to “deepen the medical identification of psychiatrists.” That same year it established a press to bring “psychiatry’s best talent and current knowledge before the reading public.” It developed a nationwide roster of experts to promote this disease model, and it set up a “public affairs institute” to run workshops that trained its members “in techniques for dealing with radio and television.”4
This PR effort told of a revolution in psychiatry, with the media informed that researchers were discovering the very “molecules” that caused psychiatric symptoms. The APA held “media days” to promote this understanding, with awards given to media that reported on this revolution, and soon newspapers and magazines were writing stories about extraordinary advances that heralded a day when mental disorders could be “cured.”
The Baltimore Sun, in a seven-part series titled “The Mind-Fixers,” which won a Pulitzer Prize for expository journalism in 1984, described the revolution in this way:
“For a decade and more, research psychiatrists have been working quietly in laboratories, dissecting the brains of mice and men and teasing out the chemical formulas that unlock the secrets of the mind. Now, in the 1980s, their work is paying off. They are rapidly identifying the interlocking molecules that produce human thought and emotion . . . As a result, psychiatry today stands on the threshold of becoming an exact science, as precise and quantifiable as molecular genetics. Ahead lies an era of psychic engineering, and the development of specialized drugs and therapies.”5
Pharmaceutical companies, of course, were thrilled with the APA’s adoption of a disease model, for they understood it would greatly expand the market for their drugs, and they began funneling money to the APA and to psychiatrists at academic medical centers to support this PR effort.
The chemical imbalance story served, in essence, as the soundbite that could best sell this disease model to the public. It was a claim that fit into a larger societal narrative about the march of medicine in the 20th century: insulin as a treatment for diabetes, antibiotics for infectious diseases, a vaccine for polio, and so forth. Now it was psychiatry’s turn to take its place at the head of this parade.
The public began hearing this soundbite immediately after DSM III was published. In 1981, an Associated Press article featuring an interview with University of Chicago psychiatrist Herbert Meltzer informed readers that “researchers believe clinical depression is caused by a chemical imbalance in the brain,” and that there were already two drugs in development that “restore the chemical imbalance” to normal.6
Three years later, Nancy Andreasen, who would soon become editor-in-chief of the American Journal of Psychiatry, published a best-selling book titled The Broken Brain: The Biological Revolution. The new understanding in psychiatry, she wrote, was that the “major psychiatric illnesses are diseases,” and that each “different illness has a different specific cause . . . there are many hints that mental illness is due to chemical imbalances in their brain and that treatment involves correcting these chemical imbalances.”7
Eli Lilly brought Prozac to market in 1988, and soon the public was hearing that this “selective serotonin reuptake inhibitor” restored serotonin to normal levels, and thus was like “insulin for diabetes.” New York magazine featured the pill on its cover: “Bye, Bye Blues” declared the headline.8 Newsweek’s did as well, with this headline atop the pill: “Prozac, A Breakthrough Drug for Depression.”9
Magazine and newspaper stories told of how patients were feeling better than ever. In the spring of 1990, the New York Times, in an article by Natalie Angier, who arguably was the nation’s most well-known science writer, informed readers that “all antidepressants work by restoring the balance of neurotransmitter activity in the brain, correcting an abnormal excess or inhibition of the electrochemical signals that control mood, thoughts, appetite, pain, and other sensations.” This new drug, Dr. Francis Mondimore told Angier, “is not like alcohol or Valium. It’s like antibiotics.”
Television shows weighed in with a similar message, and on 60 Minutes, Lesley Stahl told the inspiring story of a woman, Maria Romero, who, after a decade of horrible depression, had been reborn on Prozac. “Somebody, something left my body and another person came in,” Romero said. Stahl explained the biological cure that was at work: “Most doctors believe that chronic depression like Romero’s is caused by a chemical imbalance in the brain. To correct it, the doctors prescribed Prozac.”10
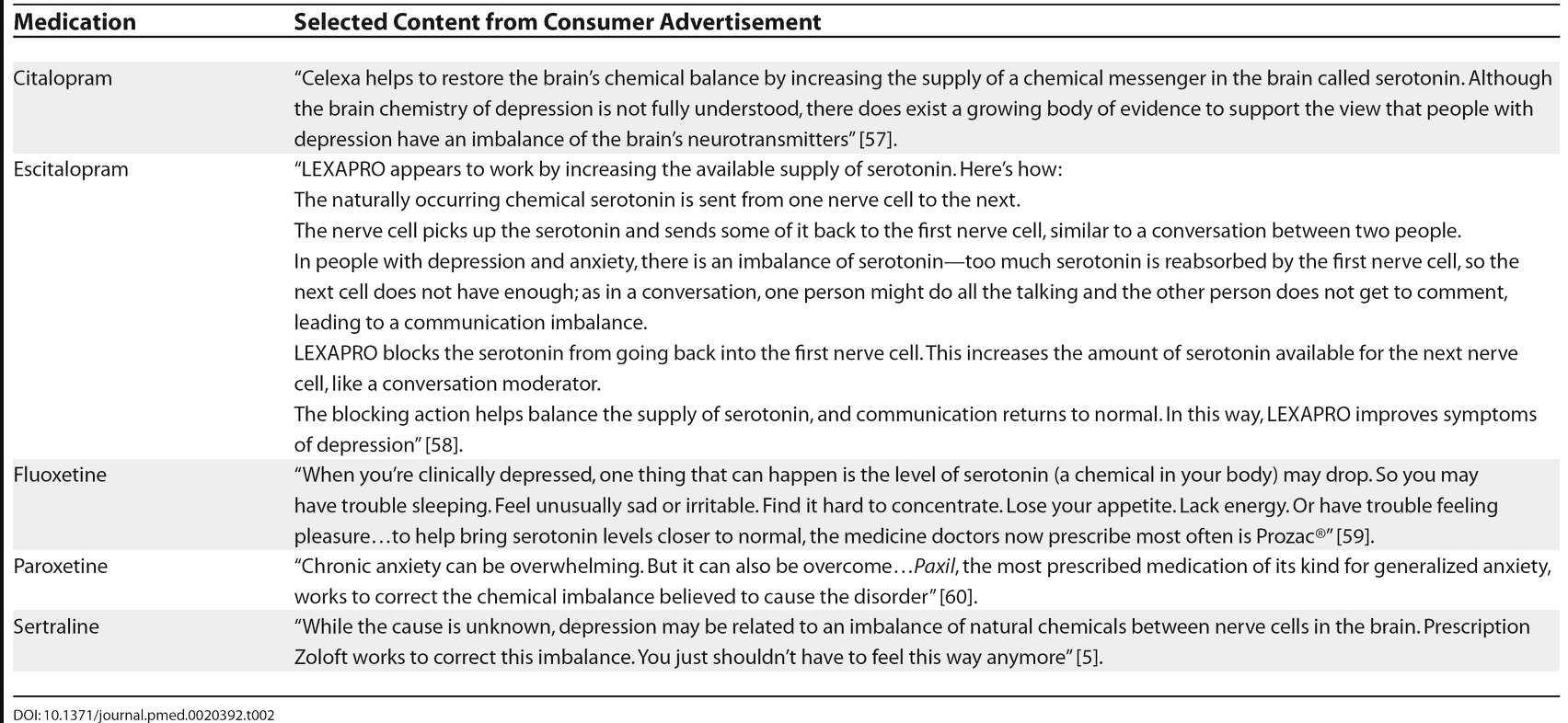
Sales of Prozac soared, and as other drug companies brought new “SSRI” antidepressants to market—Zoloft, Paxil, Celexa, Lexapro, and so forth—they relied on the chemical imbalance soundbite to market their products. The National Alliance on Mental Illness grew in prominence during this period, and its core message was that psychiatric disorders were diseases caused by chemical imbalances in the brain, and that psychiatric drugs fixed those imbalances.
The American population, and populations around the globe, came to understand this story as scientific truth. The new millennium arrived, and although the APA’s own textbook had declared the low-serotonin theory dead and buried, the APA publicly doubled-down on the chemical imbalance story, informing the public that it was now proven.
“In the last decade, neuroscience and psychiatric research has begun to unleash the brain’s secrets,” wrote APA president Richard Harding, in a 2001 article published in Family Circle. “We now know that mental illnesses—such as depression or schizophrenia—are not ‘moral weaknesses’ or ‘imagined’, but real diseases caused by abnormalities of brain structure and imbalances of chemicals in the brain.”11
In the same issue, future APA president Nada Stotland informed readers that antidepressants “restore brain chemistry to normal.”
And the public believed. On May 4, 2005, the APA issued a press release celebrating the fact that a survey it conducted had found that “75 percent of consumers believe that mental illnesses are usually caused by a chemical imbalance in the brain.” This, said APA president Steven Sharfstein, was evidence of “good news for [public] understanding of mental health.” A psychiatrist, the press release helpfully noted, was “a specialist specifically trained to diagnose and treat chemical imbalances.”
That same year, the APA published its “Let’s Talk Facts about Depression” brochure, which delivered the same message: “Antidepressants may be prescribed to correct imbalances in the levels of chemicals in the brain.”
The APA’s “public education website” continued to tell of chemical imbalances for the next 16 years. Finally, in early 2021, Ronald Pies wrote that he had, at last, managed to get the APA to “delete” that message.
Even so, the APA website still tells the public a limited version of that story. Visitors to a page titled “What is Depression” learn that “brain chemistry may contribute to an individual’s depression and may factor into their treatment. For this reason, antidepressants may be prescribed to modify one’s brain chemistry.”
The Scientific Advisory Councils
In the 1980s and 1990s, the pharmaceutical companies—and the American Psychiatric Association—realized that non-profit advocacy organizations, like the National Alliance on Mental Illness, could help them sell their disease model to the public and inform the public of the effectiveness of psychiatric drugs. Pharmaceutical money flowed to NAMI and other advocacy organizations, and soon the academic psychiatrists that served as industry thought leaders were populating the scientific advisory councils of the non-profit advocacy groups.
In a 2014 blog published on Mad in America, Philip Hickey identified three prominent consumer organizations that informed the public that depression was due to a chemical imbalance, and published the names of the psychiatrists that served on their scientific advisory boards. Here is the list:
Child and Adolescent Bipolar Foundation
-
- Joseph Biederman, MD, Professor of Psychiatry at Harvard Medical School
- Gabrielle Carlson, MD, Professor of Psychiatry and Pediatrics, Director of Child and Adolescent Psychiatry, Stonybrook State University
- Kiki Chang, MD, Associate Professor and Director of Pediatric Bipolar Disorders Program, Child and Adolescent Psychiatry, Stanford University
- Melissa DelBello, MD, Professor of Psychiatry and Pediatrics, University of Cincinnati
- Robert L. Findling, MD, Professor of Child & Adolescent Psychiatry, Case Western Reserve University
- Janet Wozniak, MD, Assistant Professor of Psychiatry, Harvard Medical School
Depression and Bipolar Support Alliance
-
- Gregory E. Simon, MD, MPH, Psychiatrist and Senior Investigator, GroupHealth Research Institute, Seattle
- Michael E. Thase, MD, Professor of Psychiatry. University of Pittsburgh
- Mark S. Bauer, MD, Associate Professor of Psychiatry, Brown University School of Medicine
- Joseph R. Calabrese, MD, Professor of Psychiatry and Director of Mood Disorders Program, Case Western Reserve University
- David J. Kupfer, MD, Professor & Chairman Department of Psychiatry, University of Pittsburgh
- George S. Alexopoulos, MD, Professor of Psychiatry, Cornell University
- Gary Sachs, MD, Director, Bipolar Research Program, Harvard University
- Mark A. Frye, MD, Professor of Psychiatry, Mayo Clinic
- J. Raymond DePaulo Jr. MD, Professor of Psychiatry, Johns Hopkins
- William Beardslee, MD, Psychiatrist-in-Chief, Children’s Hospital, Boston
NAMI
-
- Nancy Andreasen, MD, Chair of Psychiatry at The University of Iowa College of Medicine.
- Ellen Frank, PhD, Professor of Psychiatry and Psychology at the University of Pittsburgh School of Medicine.
- David Kupfer, MD, Professor of Psychiatry and Professor of Neuroscience, University of Pittsburgh School of Medicine.
- Jeffrey Lieberman, MD, Chair of Psychiatry, Columbia University and Director of the New York State Psychiatric Institute.
- Henry Nasrallah, MD: Associate Dean; Professor of Psychiatry and Neuroscience, University of Cincinnati.
- Charles Nemeroff, MD: Chair of Psychiatry and Behavioral Sciences, University of Miami Health System.
- S. Charles Schulz, MD: Professor and Chair, Department of Psychiatry, University of Minnesota Medical School.
The names on the list constituted a “who’s who” of prominent academic psychiatrists at that time, many of whom were known to have been paid hundreds of thousands of dollars for their “thought leader” services to industry. Theirs was a collective voice informing the American public that depression was due to a chemical imbalance, which could be successfully treated by antidepressants that helped correct that imbalance. Fifteen years after the APA declared the low-serotonin theory dead, antidepressants—on these websites—were still being presented as an antidote to a disease.
While many consumer organizations have now scrubbed such claims from their sites, they have not disappeared altogether. For example, the Child Mind Institute website, on a page titled “Medication for Kids with Depression,” provides this description of antidepressants:
The founder of the Child Mind Institute is one of the most prominent child psychiatrists in the United States, Harold Koplewicz. He is chair of the Department of Child and Adolescent Psychiatry at NYU School of Medicine and has been editor-in-chief of the Journal of Child and Adolescent Psychopharmacology since 1997. A primary mission of the Child Mind institute, his profile page states, is to “educate and empower parents by providing trustworthy information and resources.”
Pharmaceutical Companies
As anyone who watched television in the first decade of the new millennium knows, pharmaceutical companies used the chemical imbalance story to sell their antidepressants. Pfizer, for instance, flooded the airways with its “Sad Blob” ad, and if you pay close attention, you’ll see that Pfizer knows the chemical imbalance story is unfounded. Yet, it uses the chemical story to sell its drug anyway. It accomplishes this verbal sleight of hand in two brief sentences: “While the cause (of depression) is unknown, depression may be related to an imbalance of natural brain chemicals between nerve cells in the brain. Prescription Zoloft works to correct this imbalance.”
The ad closes with this reminder: “When you know more about what is wrong, you can help make it right.”
Such is the trail of fraud that lawyers could present if they mounted a class action lawsuit. They could detail how there is a long line of research, dating back to the 1970s, that failed to find that low serotonin was a cause of depression. They could show that in 1999 the APA’s own textbook declared the theory dead and buried. And then they could detail how the APA, scientific advisory boards at advocacy organizations, and pharmaceutical companies continued to promote the chemical imbalance theory after that, with antidepressants presented as drugs that fixed chemical imbalances. That continued promotion is evidence that from 1999 forward these three groups were knowingly promoting a falsehood, which patients could be expected to act upon.
This is evidence of medical fraud—and, one might say, societal medical battery—committed on a grand scale.
The Other Half of the Chemical Imbalance Story
While researchers did not discover that people diagnosed with depression had abnormal serotonin systems before they took an antidepressant, they did discover that the compounds induced the very abnormality hypothesized to cause the disorder in the first place.
The basic mechanism of an SSRI is well known. When a presynaptic neuron releases serotonin into the tiny gap between neurons (known as the synapse), the serotonin molecules bind with receptors on the post-synaptic neuron, and then, in a flash, the serotonin is removed from the synapse. An enzyme metabolizes a small amount of the serotonin; the rest is quickly pumped back into the presynaptic neuron, entering via a channel known as SERT. In a 1975 paper, Eli Lilly scientists reported that fluoxetine, the compound that would be marketed as Prozac, blocked this reuptake process, causing a “pile-up of serotonin at the synapse.”
However, the presynaptic neuron has “autoreceptors” on its terminal membrane that monitor serotonin levels in the synapse, and with serotonin levels piling up, these autoreceptors begin to scream, as one scientist quipped, “turn off the serotonin machine.” The presynaptic neurons begin to fire at a lower rate, while the postsynaptic neurons decrease the density of their receptors for serotonin.
In other words, the drug puts down the accelerator on serotonergic transmission, and the brain responds by putting on the brake.
Over time, other changes may kick in. There are feedback loops that connect different neurotransmitter systems to each other, and so this initial response to the drug is likely a prelude to a host of downstream changes that have yet to be identified. However, the initial response to fluoxetine was fleshed out early, and it told of how fluoxetine, rather than normalize serotonergic pathways, induced profound abnormalities in this system.
In 1996, NIMH director Steven Hyman published a paper titled “Initiation and Adaptation: A Paradigm for Understanding Psychotropic Drug Action” that told of how all psychiatric drugs could be understood to create abnormalities in brain function.
Psychiatric drugs, he wrote, create “create perturbations in neurotransmitter function.” In response to this perturbation, the brain goes through a series of compensatory adaptations, and in each instance, the immediate adaption is for the brain to oppose the effects of the drug. An antipsychotic blocks dopamine transmission, and in response the brain’s dopaminergic pathways spring into high gear, at least for a time. An antidepressant ups serotonergic levels in the synapse, and in response, the brain puts a brake on its serotonergic pathways. These compensatory adaptations, Hyman wrote, “are rooted in homeostatic mechanisms that exist, presumably, to permit cells to maintain their equilibrium in the face of alterations in the environment or changes in the internal mileu.”
Hyman was describing adaptive changes known as “oppositional tolerance” to a drug. After a period of time, he continued, the “chronic administration” of the drug causes “substantial and long-lasting alterations in neural function.” As part of this process, there are changes in intracellular signaling pathways and gene expression. After a few weeks, he concluded, the person’s brain is functioning in a manner that is “qualitatively as well as quantitatively different from the normal state.”
“Qualitatively as well as quantitatively different” than normal. Indeed, two Eli Lilly scientists, Ray Fuller and David Wong, early on observed that fluoxetine, since it disrupted serotonergic pathways, could be used to study “the role of serotonin neurons in various brain functions—behavior, sleep, regulation of pituitary hormone releases, pain responsiveness and so on.” To conduct such experiments, researchers could administer fluoxetine to animals to observe which functions became compromised. They would look for pathologies to appear.
Such was the state of scientific knowledge about antidepressants as a treatment for depression by the end of the 1990s. There was no evidence that depressed patients suffered from low serotonin before they took an antidepressant, but research had shown that once they did, their brain would begin functioning in a manner that was “qualitatively as well as quantitatively different from the normal state.”
Antidepressants were promoted to the public as “normalizing agents,” when in fact researchers knew they were “abnormalizing” agents.
Harm Done
In their responses to Moncrieff’s paper, many psychiatrists sounded a “no harm, no foul” argument. “Antidepressants work,” they stated, and thus the prescribing of antidepressants was a helpful practice, even if there was some confusion about the cause of depression and what the drugs did.
Here is how Massachusetts psychiatrist Daniel Carlat put it, in his interview on National Public Radio’s “On Point” program:
“Doctors don’t know exactly about how (antidepressants) work. Patients do want to know there is an explanation out there. And there are times when we do have to give them a shorthand explanation, even if it is not entirely accurate.”
In terms of harm done by the chemical imbalance lie, whether an antidepressant reduces the patient’s symptoms over some period of time is beside the point. The chemical imbalance story informs the patient that he or she suffers from a brain pathology, which requires treatment with a drug that treats that pathology. That is a diagnostic story that changes a patient’s sense of self and understanding of his or her own mind. Moreover, the treatment is designed to change how the individual emotionally responds to the world—this is an intervention of a most profound sort.
Indeed, the decision to take an antidepressant puts the patient on a different life course. It puts a person on a path of a medicated future, as opposed to the life the person had known before and the life that the person might have if he or she sought some other non-medical form of treatment. In that sense, the decision of whether to take an antidepressant acts as the proverbial fork in the road—two different lives stretch ahead.
That is the harm done when the chemical imbalance story was told to patients seeking help for depression: They made a profound decision about their future based on a lie.
The chemical imbalance story also did harm at a societal level. It remade our collective sense of self.
Before Prozac arrived on the market, a NIMH survey found that only 12% of American adults said they would take a pill to treat depression. This was a survey that told of a public that understood, at some level, that to experience periods of suffering was normal, that life had its ups and downs, and that often people could call on an inner resilience—and environmental support—to lead them out of the tunnel of darkness.
But then came the selling of psychiatry’s disease model, and in fairly quick order the public came to see human nature in a new light: our moods were directed by a molecule called serotonin, and if a person experienced depression, they had, in the words of Nancy Andreasen, a “broken brain.”
This is a conception that also stifles political efforts to create a society that better nurtures mental and emotional well-being. The chemical imbalance story placed the cause of depression within the brain of the individual, which fits a neoliberal agenda, but produces a blindness to social conditions that promote suffering and depression: poverty, lack of access to decent housing, poor childcare support, and so on.
As Moncrieff wrote, surveys have found that more than 85% of the public came to believe that depression is caused by low serotonin. That number tells of a conspiracy—by a guild, pharmaceutical companies, and academic psychiatrists—that profoundly betrayed our society. They told us a story that their own research had shown to be false, and they did so because it benefitted guild interests and the financial interests of pharmaceutical companies. As for the members of the scientific councils, they were signing off on a story that kept them in good standing as industry “thought leaders” and further burnished their public reputations as leaders in the field.
From a legal standpoint, it doesn’t really matter whether “antidepressants work.” Lying to patients and to society is a form of medical battery, and any possible therapeutic benefit doesn’t excuse that deception. However, when that “antidepressants work” claim is examined, it can be seen that it is a continuation of the false marketing of these drugs.
Do Antidepressants Work?
When the public is told that a drug “works,” they are being led to believe that most people who take the drug can expect to receive a benefit. An antibiotic, for instance, is a drug that can be said to “work.” When penicillin and other antibiotics were introduced in the 1940s, they cured bacterial infections and any number of bacterial illnesses: pneumonia, scarlet fever, diphtheria, and tuberculosis, to name a few. But an antidepressant cannot be said to work in this way.
What can be said is that there are clinical studies that provide information about the possible risks and benefits of antidepressants, both over the short-term and long-term. The relevant information can be grouped into three types.
Placebo-controlled trials
When psychiatrists state that antidepressants “work,” they are mostly citing findings from industry-funded trials of the drugs. Meta-analyses of these short-term trials have found that the difference in the reduction of symptoms between the drug-treated and placebo groups is about two points on the 52-point Hamilton Depression Rating Scale. While this difference may be statistically significant, it is of questionable clinical significance.
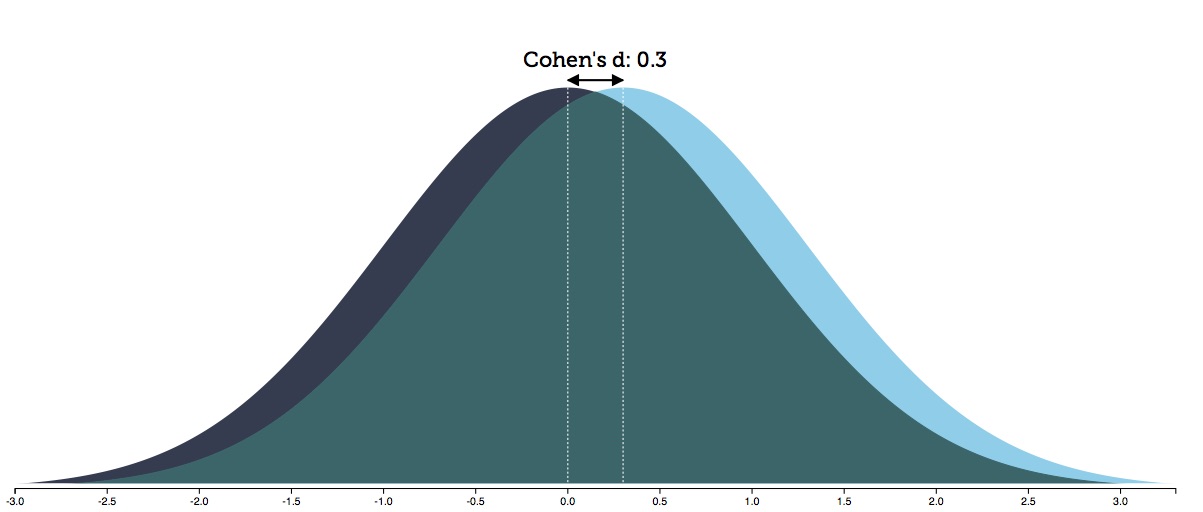
The best way to understand this difference is to look at its effect size. At an individual level, responses fall along a bell curve, and a visualization of the effect size reveals how the bell curves for the placebo and drug-treated groups differ. Researchers have concluded that the “effect size” in the industry trials is 0.3 (effect sizes can range from 0 to 3.0).
As the graphic below reveals, when a treatment has an effect size of 0.3, there is an 88% overlap in the bell curves of the two groups. That means you need to treat eight people with an antidepressant to produce one additional person who benefits from the treatment. Seven of eight treated with the drug will be exposed to the adverse effects of the drug without any additional benefit beyond placebo.
Studies in “real-world” patients
The industry-funded trials are typically conducted in a subset of patients who could be expected most likely to respond well to the drug (without comorbidities and so forth), and thus are understood to not necessarily reflect outcomes in the general population. Studies in “real-world” patients, which in the U.S. are usually funded by the National Institute of Mental Health, are typically not placebo-controlled, but rather simply seek to assess what percentage of patients respond, in a significant way, to the treatment.
These studies have reported lower “response” rates to antidepressants than the industry-funded trials do, and particularly poor stay-well rates.
In a 2004 study of 118 real-world patients treated with an antidepressant, only 26% of the patients “responded” to the treatment (meaning that their symptoms decreased at least 50% on a rating scale), and fewer than 13% were in remission at the end of 12 months. These findings, the investigators concluded, “reveal remarkably low response and remission rates.”
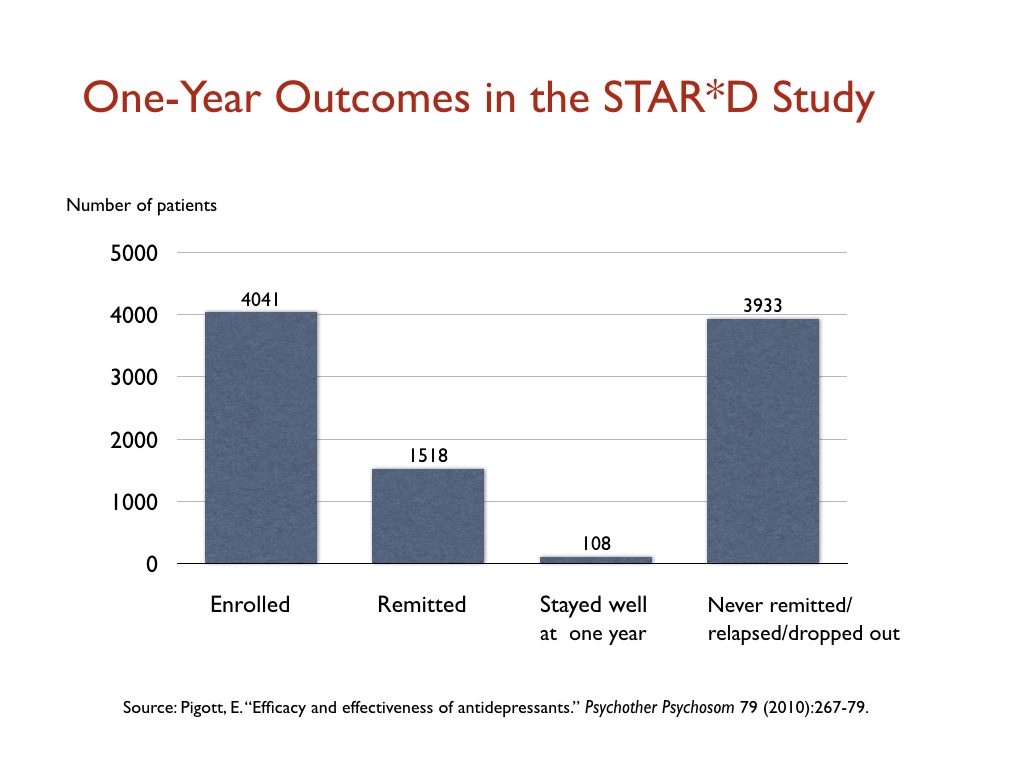
The STAR*D trial funded by the NIMH, which was heralded as the largest antidepressant trial ever conducted, produced similarly poor results in “real-world” patients. The 4,041 patients enrolled into the trial were given up to four trials on an antidepressant to find one that led to remission (defined as a score below 7 on the Hamilton scale), and only 38% achieved this level of improvement.
Those who remitted were then whisked into a longer-term follow-up study, where they would get the best clinical care possible. Yet, at the end of one year, only 108 of the 4,041 patients entered into the STAR*D trial had remitted, and then stayed well and in the trial to its end. All the rest had either never remitted, relapsed, or dropped out at some point. That is a one-year stay-well rate of 3%.
More recently, an international group of researchers, in a study of 1,217 patients diagnosed with major depressive disorder, reported that only 24% responded to treatment with an antidepressant (either alone or in combination with psychotherapy.) Thirty-four percent were “non-responders” to antidepressants, and the remaining 41% fared so poorly that they were deemed “treatment resistant.” Nearly 60% ended up ended up on multiple medications, including multiple antidepressants, antipsychotics, benzodiazepines, and other combinations of drugs.
These real-world studies were not placebo controlled, and thus there wasn’t a comparison with a similar group of untreated patients. This raises the obvious question: What is the natural course of depression?
Prior to the antidepressant era, depression was understood to be an episodic disorder, as opposed to a chronic illness. Spontaneous recovery rates were said to exceed 50% within a few months, with this recovery rate reaching 85% or so by the end of one year. As Dean Schuyler, head of the depression section at the NIMH explained in a 1974 book, most depressive episodes “run their course and terminate with virtually complete recovery without specific intervention.”12
However, after the introduction of antidepressants, the disorder began running a much more chronic course. In the 1970s, several clinicians observed that the drug was causing a “chronification” of the disease, and subsequent epidemiological studies confirmed that the long-term course of depression had changed. The APA’s 1999 textbook summed up the findings from the newer studies: “Only 15% of people with unipolar depression experience a single bout of the illness,” and for the remaining 85%, with each new episode, remission becomes “less complete and new recurrences develop with less provocation.”13
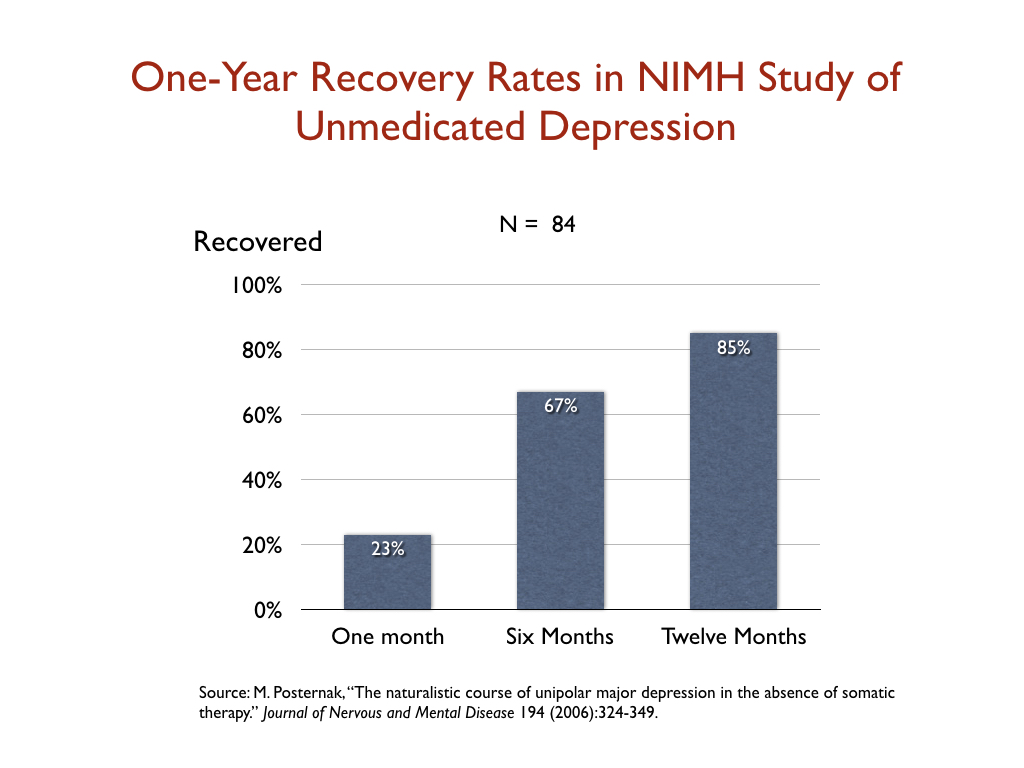
With the outcomes for medicated patients so poor, the NIMH funded a study to assess the course of “untreated depression” in the modern era. Perhaps the natural course of depression had changed? In 2006, researchers reported that 23% of the non-medicated patients recovered in one month; 67% in six months; and 85% within a year. These were outcomes, the researchers concluded, that echoed those in the pre-antidepressant era. “If as many as 85% of depressed individuals who go without somatic treatment spontaneously recover within one year, it would be extremely difficult for any intervention to demonstrate a superior result to this,” they wrote.
Such is the risk-benefit equation that emerges from studies of real-world patients. Perhaps 25% will respond to an antidepressant, and perhaps 15% or so respond to treatment and stay well. There is also reason to believe that the one-year recovery rate for untreated patients is much higher than that.
Long-term outcomes
The industry-funded trials provide a risk-benefit equation at the end of six weeks on the drug. The clinical studies in real-world patients provide information about the percentage of people diagnosed with major depression who, at some point during studies of longer duration (typically six months to a year), will respond to an antidepressant and still be well at the end of the study. The third question that needs to be assessed is this: How do patients treated with antidepressants fare over longer periods of time—two years or more?
This question harkens back to the same one that arises in the clinical studies of one year in length: what is the natural long-term course of the illness? For an antidepressant to be effective over the long term, it would need to improve on that natural recovery rate.
Unfortunately, there is abundant evidence that antidepressants, on the whole, increase the risk that a person will become chronically depressed and functionally impaired. I reviewed that collection of evidence in Anatomy of An Epidemic; a summary of that research can be found here on Mad in America.
In the mid 1990s, Italian psychiatrist Giovanni Fava raised this concern in a series of papers. He wrote:
“Antidepressant drugs in depression might be beneficial in the short term, but worsen the progression of the disease in the long term, by increasing the biochemical vulnerability to depression . . . Use of antidepressant drugs may propel the illness to a more malignant and treatment unresponsive course.”
In his articles on this topic, Fava noted that antidepressants induce changes in the serotonin system the opposite of their intended effect, and reasoned that this might be the mechanism that “sensitized” the brain to depression.
In 2012, American psychiatrist Rif El-Mallakh, an expert in mood disorders, concluded that SSRIs could induce a chronic “tardive dysphoria.” He noted that up to 40% of patients initially treated with an antidepressant end up “treatment resistant,” and up to 80% maintained on the drugs suffer a recurrence of symptoms.
“A chronic and treatment-resistant depressive state is proposed to occur in individuals who are exposed to potent antagonists of serotonin reuptake pumps (SSRIs) for prolonged periods. Due to the delay in the onset of this chronic depressive state, it is labeled tardive dysphoria. Tardive dysphoria manifests as a chronic dysphoric state that is initially transiently relieved by—but ultimately becomes unresponsive to—antidepressant medication. Serotonergic antidepressants may be of particular importance in the development of tardive dysphoria.”
Such is the gap between what depressed patients—and society at large—have been told about antidepressants for the past 30-plus years and the story told in the scientific literature. The public was led to believe that antidepressants fixed a chemical imbalance in the brain and thus could be considered an antidote to the pathology that caused depression, and that clinical studies have shown that these drugs “work.” In fact, the research literature told the following story:
- Depression is not caused by a known chemical imbalance in the brain
- An antidepressant causes the brain to begin functioning in a manner that is both “qualitatively and quantitatively different” than normal
- In industry-funded trials, only one in eight patients could be said to benefit from the treatment
- Studies in real-world patients found that only a minority of patients respond to an antidepressant and relatively few remain well at the end of one year
- Long-term outcomes for treated patients are particularly poor, and there is evidence that their use increases the risk that a person will become chronically ill
This, of course, is information that would enable patients to make an informed choice about whether to take an antidepressant. Yet—and this is an example of how the APA continues to misinform the public—here is what the APA currently tells the public about the efficacy of antidepressants:
“Between 80% and 90% of people with depression eventually respond well to treatment. Almost all patients gain some relief from their symptoms.”
Why a Lawsuit Is Needed
All societies need their medical communities to provide the public with honest information about what is known about the nature of an illness, and the risks and benefits of a treatment for that illness.
The chemical imbalance story of depression violated that obligation of honesty, and egregiously so. In lieu of information necessary for a depressed patient to give informed consent, patients—and the public—were told a false story that benefitted guild interests and the financial interests of pharmaceutical companies. In essence, a marketing story was substituted for a scientific one.
Mad in America has published numerous stories by people who were told they suffered a chemical imbalance in the brain, and whose lives then crashed and burned after they took an antidepressant, with so many ending up on drug cocktails. Their stories just begin to hint at the extraordinary harm done by the chemical-imbalance deception.
And yet, even as psychiatrists have said there was “nothing new” with Moncrieff’s paper, there has been no public admission of wrongdoing, or apology, for the misleading of patients and society in this way for decades. Carlat, in his comments on NPR’s On Point show, even justified it, at least to a degree, putting it into the category of a little white lie. At times, he said, psychiatric patients need to be given information about psychiatric drugs that “is not entirely accurate.”
Meanwhile, the APA just keeps on with its propaganda, telling the public that nearly all patients eventually respond well to antidepressants. That is a whopper that trumps the antidepressants-fix-chemical-imbalance story for its mendaciousness.
This is why a class-action lawsuit is needed. To this point, those promoting the chemical imbalance suffered have suffered no cost for doing so. Rather, money has been made, careers have been burnished, and all the while our society has borne the cost.
A class-action suit would serve society well. It would put teeth into the legal obligation for doctors to provide “informed consent,” and for a medical discipline to provide society with information that met this standard too.
***
Sources: Much of the history and research recounted here is taken from Anatomy of an Epidemic: Magic Bullets, Psychiatric Drugs and the Astonishing Rise of Mental Illness in America, a book I published in 2010, and Psychiatry Under the Influence: Institutional Corruption, Social Injury, and Prescriptions for Reform, a book I co-wrote with Lisa Cosgrove, published in 2015.
Correction: In the quote above by Ronald Pies, I identified Psychiatric Times as a publication of the American Psychiatric Association. That was in error. Psychiatric Times is a trade publication published by MHS associates.
Where do we sign up?
Report comment
As someone who has been poisoned by these meds at least 9 times in the past 30 years, being told the same lie, I too, would be interested in where I sign up! After the last time, I was declared disabled, and I have been diagnosed by 2 separate psychologists with C-PTSD and medically resistant severe depressive disorder. I have also been red flagged by my pharmacist and they will not fill ANY prescription for ANY type of serotonergic meds. After being made literally psychotic so many times, simply due to known lies is definitely something I want in on taking down! It’s not just antidepressants. Tramadol is a synthetic opioid/SSNRI combo, and the muscle relaxer, Soma, also boosts serotonin in the brain. My best advice is to research any and all drugs prescribed by ANY doctor before taking it. Do your own research, because this article has shown us all that the “professionals” can’t be trusted to even know the truth, let alone tell it to us as patients.
Report comment
No informed consent- ever. 100% misdiagnosed a physical health issue. Had NO problems with informed consent in 2 other countries about everything and an accurate diagnosis as fast as possible. No gaslighting and lies.
Report comment
As a child of cure I’m in.
Report comment
Great Article this is ground breaking, how do we get organized what are the next steps?
Report comment
Start by asking for your medical records from your own doctor and you may be surprised that it contains evidence of incompetence and negligence.
Report comment
“Start by asking for your medical records from your own doctor and you may be surprised that it contains evidence of incompetence and negligence.”
Not sure about the ‘system’ in the US Gilbert, but in Australia they do what they call “editing”. In my case this meant removing the documents that showed I had been ‘spiked’ with date rape drugs, and that a Community Nurse had lied to police telling them I was his “Outpatient”, and have them use a little rough stuff to make me talk to him This is the sort of ‘treatment’ that may be necessary to get you the ‘help’ you need.
https://www.youtube.com/watch?v=oZ9UQKBUrsg
Now that your ‘willing’ to talk to him (because you did actually have the right to silence when you weren’t his “Outpatient”) he could put words in your mouth and produce a false statutory declaration for others to utter with (including our Chief Psychiatrist).
Now, a legal representative on provision of a confidentiality agreement actually gets to examine unredacted documents, with the hospital identifying areas which are not to be disclosed to their clients highlighted, and a reason for the non disclosure to be given (in writing). This is a protection of human rights, that someone with your interest at heart gets to look and check if you’ve been abused.
However, in my instance the documents provided to my ‘legal representatives’ was also “edited”, and the documented crimes removed, other documents containing sensitive information inserted in their place. I went from being the victim of serious criminal offending to a violent psychotic mental patient who had been being treated for more than 10 years by the hospital, and who was delusional about being ‘spiked’ with date rape drugs.
Sure they can deny me access to the documents, or parts of. But I had no idea they were concealing human rights abuses from legal representatives, who then actively conspire to “fucking destroy” the person who has been abused.
Given the power by the State to do this type of “editing”, and the removal of legal protections from the Mental Health Act by the Chief Psychiatrist rewriting our Act (care to see the letter?), and enabling arbitrary detention and torture of citizens, I think my concerns about the ‘legal protections’ contained in our new Euthanasia Act are legitimate.
The State does the crimes (human rights abuses), and the ‘legal representatives’ set up their ‘clients’ for a fall. Drafting complaints and then forging and uttering the responses from the Chief Psychiatrist. It worked a treat….. for a long while anyway. Next…….
Report comment
Removed for moderation.
Report comment
Removed for moderation.
Report comment
In commenting about Dr. Pies,Mr. Whitaker states that Psychiatric Times is the trade publication of the American Psychiatric Association (APA). That couldn’t be further from the truth. It is a separate publication, often publishing articles much different than that of Psychiatric News, which is the trade publication of the APA. I hope there aren’t other untruths in this article.
-Steven Moffic, MD
Report comment
“If we were to cast aside every man who had made a mistake once, useful men could probably not be come by. A man who makes a mistake once will be considerably more prudent and useful because of his repentance. I feel that he should be promoted.’’
From the Hagakure by Yamamoto Tsunetomo
Report comment
C’mon, we all know you have a strong stomach when it comes to untruths!
Report comment
Steven Moffit is correct regarding Psychiatric Times. It is a trade publication published by MHS Associates, not the American Psychiatric Association. Psychiatric Times describes itself as “the voice of psychiatry.” I have noted the correction at the bottom of the article.
Report comment
And, Bob, my last name is spelled Moffic. Remember, I did write for MIA some time ago!
Report comment
I expect forever to feel grateful to the humble Stephen Moffic for the extremely and typically candid response he so generously offered when I asked in the comments of some Psychiatric Times blog if “burnout necessarily includes depression as a symptom, and if depression is a mental disorder, supposedly, how come “burnout” (in physician or others) supposedly is not.
Stephen frankly replied that they (doctors and psychiatrists, I understood him to mean) preferred to call it “a psychological condition” as to do otherwise might stigmatize those affected and inhibit colleagues from coming forward to seek appropriate treatment.
There is no man I admire more than H. Stephen Moffic.
And I thank him and bless him, daily, and pray “God” rests him and all his family very merry.
How various European and other countries/jurisdictions view “burnout” is fascinating in itself…
Tom.
Report comment
Straining out gnats and swallowing camels, are we, Stevie? I notice Bob readily corrected this error, and I doubt anyone was hurt by it. Are there any errors you and your colleagues would care to correct? People have been VERY hurt and some even killed by the professional lies and negligence mentioned in this article!
Report comment
Exactly.
Report comment
Hi, Russell.
I fully agree with you than countless people have been and continue to be grievously harmed by delusional, coercive psychopharmacology and the all the falsehoods which it has fed and continues to feed society.
I certainly count myself among them, having lost my career and more to coercive psychiatry and its myths.
Like what is called the “Judeo-Christian” – but might more accurately, I suggest, be called the Judeo-Pauline – tradition from which it has arisen, it seeks to divide humanity in two – those supposedly with and those without “mental disorders” and “personality disorders’ – very much as previous clerics/arbiters of correct human behavior spoke of “saints” and “sinners,’ any “There but for the grace of God go I,” statements notwithstanding.
“Good” guys and “bad” guys. Them and us. Victims and perps. Demonizers and supposed evildoers. Wicked, mendacious, coercive psychopharmacologists and us, their hapless, innocent victims.
Or are we all in this together?
And, by endeavoring to remain as objective and nonjudgmental as Robert Whitaker, may we not hope to make best progress?
A prominent colleague of Stephen Moffic’s, one who also frequently wrote to Psychiatric Times, continually insisted on the validity of “mental disorder” diagnoses.
To persuade us just how mad folks could be, he once used the unforgettable example of one of his own early “patients.”
That man “bled from his fingertips and nails” (as I recall) in trying to claw his way out of that psychiatrist’s office.
It takes a lot to render me speechless. This did.
Which of us is not a victim of the distorted point of view and conditioned responses we have inherited?
Unlike H. Stephen Moffic, who habitually responded respectfully and courteously to all comments following blogs, his colleague tended not to waste his time on “the uncredentialled.”
Stephen wrote a great deal about “burnout” in such away as to lead one to suppose he knew a great deal about it, and presumably had earned his understanding, and his compassion, the hard way.
Stephen told us that he had a son a rabbi.
Jackie Mason became a rabbi to please his dad, who, according to Jackie, thought everyone (and his dog) should be a rabbi.
I reckon that, if we were all meant to be Jackie Mason or the Dalai Lama or Stephen Moffic or his rabbi son, we would be.
The Dalai Lama asked us to be kind whenever we can…and knew and said that we (all) always can be.
When the day comes that we are – soon – perhaps we will no longer have two kinds of people, those who divide people into two kinds of people and those who do not, and, thanks in large measure to Bob Whitaker and MIA, coercive psychiatry will have died a natural death?
Comfort and joy.
With supreme gratitude to MIA,
Tom.
Report comment
Thank you, Tom. Your comments bring to mind this quote from Aleksandr Solzhenitsyn:
“If only there were evil people somewhere insidiously committing evil deeds, and it were necessary only to separate them from the rest of us and destroy them. But the line dividing good and evil cuts through the heart of every human being. And who is willing to destroy a piece of his own heart?”
Report comment
Well, funny you should ask. The clarion call might be a collective action. How to frame the challenge. From the past, a major player in filing civil rights challenges would file the legal challenges himself. He would explain that lawyers wanted to work in Louisville and to advance the challenge, the risks of being shut out were greater than what he perceived to be the merits of the case.
Hence, I went to the Clerk’s Office of the Federal Courts in the Federal Building in Louisville and requested the packet/information on how to file a challenge.
Hence, go to the United States District Court, and request the following: Pro Se Handbook for Non-Prisoners, 2) Non-prisoner application to proceed without prepayment of fees and affidavit, 3) About these forms
So, perhaps a movement of We, as citizens begin to move the challenge, collectively and individually might focus the discussion. The clerks who work are not attorneys and as such, to expect legal advice when we are asking for the corrective action…. will flesh out perhaps the issues that have been and are creating the problems…
So, perhaps this sharing of information might be of interest. More later.
Report comment
Psychiatry is not one big monolithe. “Low levels of certain neurotransmitters” is a figure of speech. It was used as a benign means to communicate in a general fashion a complex medical phenomenon. A lawsuit of the kind contemplated will cost the plaintiff’s attorney fees, big time, imo.
Report comment
Removed for moderation
Report comment
“Researchers have concluded that the “effect size” in the industry trials is 0.3 (effect sizes can range from 0 to 3.0).”
Just a slight correction here. There is no limit of 3 to Cohen’s d. It maps to [0,infty) if you look at the absolute value or (-infty, infty) if you don’t.
Report comment
Technically, yes, you’re correct; however, we report Cohen’s d from 0 to 3.0. 3.0 would be 3 standard deviations or 99.9 percent.
Report comment
Now, this is sort of strange, technically speaking, since the brain has become a technical extension of something or another, to be studied through the lens of the Liberal Arts. So, are you saying, that for the most part, the thinking about the unique human being observed and perhaps listened to, can fall within a range of what is normal? For that particular label?
Because in Kentucky, we once had Governor Wallace Wilkson, who also had the contracts for the bookstore, one being the University of Louisville. So, a whole fish bowl of the little squeezy brains from http://www.cerebellum.com, in colors of Black, White, Yellow and even Pink would be available to the customers. I order a couple of of the bowls and only sold a couple.
Most did not grasp the serious significance of their label, Standard Deviants!
So, how does the deviance in the professional practice be guided into realizing a better truth?
Seems to me, a few people including myself, have made some errors in life, but when the process is killing “those people” in the act of creating social schizophrenia, there seems to be a problem, from the floor of seclusion to the highest echelons of governance?
If the legal challenge is to be filed, the practices need to be shown. Even for the ones whose lives were destroyed? Help me on this one, please.
Report comment
The class-action lawsuit sounds like an excellent idea.
It would not surprise me if the crazy-making, gas-lighting psychiatry establishment and their legal defense team attempt to make the case that patients were never told by psychiatrists – except in rare instances by “bad apples” — that patients had a chemical imbalance.
Of course, millions of patients could counter this, but a witness that would be most difficult for psychiatry and its apologists in mainstream media to discredit would be National Public Radio (NPR) correspondent Alix Spiegel who reported in her 2012 story about her Johns Hopkins psychiatrists.
Spiegel stated the following:
When I was 17 years old, I got so depressed that what felt like an enormous black hole appeared in my chest. Everywhere I went, the black hole went, too. So to address the black-hole issue, my parents took me to a psychiatrist at Johns Hopkins Hospital. She did an evaluation and then told me this story:
“The problem with you,” she explained, “is that you have a chemical imbalance. It’s biological, just like diabetes, but it’s in your brain. This chemical in your brain called serotonin is too, too low. There’s not enough of it, and that’s what’s causing the chemical imbalance. We need to give you medication to correct that.”
Then she handed my mother a prescription for Prozac.
This Alix Spiegel account is, of course, the experience, of millions of people.
Report comment
Patients should start by asking for their medical records from their own doctor and you may be surprised that it contains evidence of incompetence and negligence. Few patients ever do.
Report comment
Many if not most will be denied as I was. They are legally allowed to deny psychiatric patients access to treatment notes because doctors are afraid of retribution for what they write about their patients.
Report comment
“Many if not most will be denied as I was. They are legally allowed to deny psychiatric patients access to treatment notes because doctors are afraid of retribution for what they write about their patients.”
This it true kindredspirit. In my State there is a legal protection allowing a legal representative the right to examine unredacted documents on provision of a confidentiality agreement.
The hospital identifies the information they do not want disclosed, and provides a reason for the non disclosure.
This creates problems when the hospital wants to conceal criminal offenses and human rights abuses, because the lawyers have a right to the documents, and the hospital doesn’t want to ask them in writing to conspire to pervert the course of justice.
Knowing that the ‘client’ will not be allowed to see what they, the lawyers. have done, they are free to conspire with the hospitals over such matters (eg acts of torture). There is nobody watching the watchers, or so they think.
Tends to be that the hospital will arrange an ‘unintended negative outcome’ while they put the lawyers on ‘hold’ with “edited” documents.
Once a mental health fatwah (diagnosis) has been issued by the Mullahs, it really is forever. The idea of getting access to the legal system, when the legal system has ordered you ‘treated’ is ludicrous.
The lawyers are fully aware of the vulnerability faced by their ‘clients’, and will take full advantage of that situation by throwing them under a bus, for an increase in their State funding to provide ‘access to the law’ (yep, it’s a joke they play on the community). And the general public will say “they wouldn’t do that” while they refuse to examine the facts.
Consider this for example.
From the Mental Health Act 1996
29 . Referring potential involuntary patients for psychiatric examination
(1) Subject to section 194, a medical practitioner or an authorised mental health practitioner who suspects on reasonable grounds that a person should be made an involuntary patient may refer the person for examination by a psychiatrist.
Who should be an “involuntary patient” is set out in s. 26 Persons who should be involuntary patients of the MHA 1996
The Chief Psychiatrist in his letter of response to the Law Centre writes
“The referrer, in this case, a mental health clinician who has undergone training as an Authorised Mental Health Practitioner (AMHP), has only to ‘suspect’ on grounds they believe to be reasonable that the person requires an examination by a psychiatrist.”
Firstly, the “reasonable grounds ” standard has been removed, thus authorising arbitrary detentions based on nothing more than a suspicion. Secondly, the criteria for detention has been removed by changing the belief that must be formed by the AMHP from “the person should be made into an involuntary patient” to “requires an examination by a psychiatrist”. The MHA clearly sets out “who should be an involuntary patient” whereas, the Act has nothing to say about who should be referred for an examination by a psychiatrist. Possibly because it is quite easy to make a decision that someone ‘needs their head examined’.
The issue was that this was someone attempting to conceal KNOWN criminal offenses and human rights abuses, and the only way to achieve that was with such acts of gross negligence, and a belief that the Chief Psychiatrist has the right to change the law and remove the protections afforded the community by our lawmakers.
The Community Nurse had not met the burden placed on him by the Mental Health Act, so have the Chief Psychiatrist remove the burden with the above misrepresentation of the law and what was criminal, now becomes lawful. Having police retrieve the documents showing that the Chief Psychiatrist was fully aware of the offending before distributing the fraudulent and slanderous set of documents (the “edited” set) will be of benefit before sending out the letter of response.
Quite a three card monte, and such a shame that there were people harmed as a direct result of the deliberate delays and the overt threats and attempt to “fucking destroy” me by the State. For trying to exercise my human and civil rights, and the protection of the law?
I find it fascinating that despite looking, that people simply can’t see what I’m saying. A large number of lawyers…. though do they obtain a benefit by NOT looking? Lawyers who deliberately don’t look at what they’re told to not look at by the State? Emergency torture provisions? (whispers of ‘did I mention he’s related to the Cohens?’)
I can see how this “editing” of legal narratives for legal representatives might make a mess of the justice system. But in this instance we are talking about people being deliberately brain damaged as a result of the ‘Fatwah’ that is issued against them by psychiatrists. One would have thought the legal protections would have been stricter (as opposed to the Chief Psychiatrists removal of protections creating carte blanche) given the damage that can be done with drugs and electricity based on a ‘suspicion’. Particularly when the paranoia caused by concealing your criminal offending may cloud the decision making process.
You’d think someone with an interest in making the ‘system’ better might want to take a look at such a document, where the Chief Psychiatrist removes ALL legal protections from the law that he is charged with enforcing but……… seems that ‘advocates’ is code for throw them under a bus service because they pay better than the victims who are being loaded onto carriages. Always the stragglers who will pull the gold teeth of course but ….. to be expected I guess. Hi to the lawyer who said “I thought you were mad, but you’ve got the proof”…. look out for that number 27 Bus….. Bang.
One lawyer even ‘unreading’ the letter. lol
Report comment
A note on confidentiality.
I had someone who looked at these documents who was an ‘advocate’ for the organisation which was brought into effect by the MH Act, and as someone who was being paid to protect the vulnerable people being taken into custody and force drugged and electrocuted. You’d expect him to be aware of the protections but …… he seems to think that the Chief Psychiatrist response was ‘thorough’, and that it was just ‘sour grapes’ on the mental patients part.
However, what I noticed was that he offered to keep all of the information ‘confidential’ and on a ‘just between you an me’ basis.
So I wrote back and said, “Please don’t”, because that’s exactly what the criminals want. They don’t want people knowing that they’re doing this sort of thing and the Chief Psychiatrist is covering it up for them. The ‘squealer’ is the biggest problem these people can have, going around wanting the protection of the law, when they have a rigged game of ‘find the lady’ going on, and police being paid off? (Police telling me they didn’t have a copy of the Criminal Code when presented with the documents. Later sent to retrieve them before the fraudulent set was sent to the Law Centre, and a ‘flag’ placed on me for immediate referral should I turn up in a Station with the proof)
Classis Erving Goffman in cooling out the ‘mark’.
I’m sure the people whose children were being raped by priests were told their information would be kept ‘strictly confidential’ and that it would do damage to the child if it were talked about…… and how did that all work out?
So my attitude is that the vicious slander done by releasing my “edited” medical records to the public has resulted in me being harmed anyway. So why not show the public the proof of what is being done and called ‘medicine’? Not a day of my life has been worth living since I was introduced to the Community Nurse who told police I was his “Outpatient” (and was in possession of the knife he had arranged to have planted on me, along with the cannabis). Just in case they had to shoot me, me being ‘spiked’ with date rape drugs without my knowledge being a risk, and requiring the protection of a ‘throw down’. bang, bang, put down the knife…… (edit)…… Put down the knife bang, bang.
So why on earth should I feel the shame of being tortured and kidnapped, and only to have a psychiatrist ask, ‘why is this man even here?’.
Because they meant well? I’d like to see them defend that position. A bank robber means well, he just has to hurt a few people for others to benefit, so lets “edit” the evidence and ensure he isn’t held to account for his crimes eh? Hey look, a man sticks a gun in a tellers face becomes a legitimate withdrawal if we forge this withdrawal slip, and retrieve the video evidence……. a few threats to the families of the tellers won’t go astray either. “they wouldn’t do that”
Silence and ‘confidentiality’ is the dark shadows where these people are actively operating.
“And cover not Truth with falsehood, nor conceal the Truth when ye know (what it is)” (al Baqarah 42)
It’s not a falsehood (or criminal fraud) if you call it “editing” and everyone knows their families safety is at risk if they dare look. And those who fail to learn from history…..have probably lost their memory due to drugs and electricity.
I actually liked this quote form Orwell about Journalism.
“Journalism is printing what someone else does not want printed. Everything else is Public Relations”.
I don’t know about ‘selective’ publishing, he doesn’t seem to cover that scenario.
Report comment
Excellent article, Robert!
A legal framework created by Allen Scheflin may help with lawsuits for the “chemical imbalance” lie that has harmed so many. May be particularly useful for undue influence & manipulation of psych patients by doctors, but perhaps on a larger scale against organizations like APA & RCP.
Keep fighting the good fight! Change is happening!
~Jill Edwards
twitter.com/jclariceedwards
https://www.icsahome.com/articles/supporting-human-rights
https://youtu.be/ye5qv55S6ig
Report comment
Removed at request of poster.
Report comment
The only thing that will stop the lies is a lawsuit. There is a similar action being prepared in the UK, on the basis that ECT patients did not give fully informed consent. Most of the UK ECT patient information leaflets make false claims about correcting chemical imbalances and so on – see extract from article:
Inaccurate Information. The most frequently made inaccurate statements, made by more than half of the Trusts, are: claims that ECT corrects biological deficits (28); claims of very low mortality risk (28 Trusts); minimization of memory loss (23); claims that ECT saves lives (22); depression described as an “illness” (21); minimization of the current strength (19); and claims of very high improvement percentages (19). Just over half the Trusts (19; 52.7%) make seven or more inaccurate statements, out of a possible 11. The worst score, of nine, was attained by both Cornwall and Derbyshire.
https://www.sciencegate.app/document/10.1891/ehpp-d-21-00003
And then…. the ‘antipsychotics’ and dopamine levels…. the castle is crumbling.
Report comment
I hope so but I have/am suffering to much and I am almost 60.
I just can’t imagine how David will actually slay Goliath. Both the bibles, Christian and psychiatric, are crap. Writers will write anything to be read, sold and achieve everlasting fame.
Egos and power and money. How can this side compete?
Report comment
Psychiatry is highly successful at destabilizing patients and leading them onto a rollercoaster ride and musical chairs type of trajectory- a great business model. Never ending “meds adjustments”, hospitalizations and leading the patients to get worse over the long haul. Outcomes do not matter and these creatures can always say ” well these are difficult illnesses to treat, we did our best and don’t look at me”.
Report comment
Please the Bible is not “crap.” If you want to take on Goliath, i.e. Psychiatry, etc. you will need “Bible Believing Christians” too in your fight. Have you ever heard the phrase, “Politics make strange bedfellows.” You never know whom you will need to be your ally in any fight. In my opinion, what you criticize about psychiatry is fine, but, please don’t criticize the religious views of others. That is so wrong! Thank you.
Report comment
I suffer from depression anxiety and PTSD, Zoloft 100% has helped improve my quality of life and helped me regain control of my life! I am so grateful for this treatment option. Here in the USA I have been in therapy about 10 years and seen 4 different psychiatrists NONE of which had ever said my depression is from a chemical imbalance…. My depression is from a multitude of factors, and SSRI’s have been proven a therapeutic treatment for depression. This entire article is pointless 100%
Report comment
I am thinking you have missed the point of this article. Johanna did not say that SSRIs can’t work nor that all psychiatrists are telling their clients that they have a “chemical imbalance” or something wrong with their brains. She is saying that the claim that “depression” is caused by low serotonin is FALSE. It has been shown that over 80% of US citizens polled believed that depression is caused by low serotonin. Someone is telling this story, and if you read others’ posts, you can see that this story is indeed told to many by their doctors. The reactions she has received also seem to indicate that some of the psychiatric establishment is quite upset at her for stating this fact out loud.
Science is not built on individual experiences. Nor is culture. I am glad that you have had such a positive experience yourself. But that does nothing to invalidate Johanna’s summary of the research. Depression is not caused by low serotonin. That is all she is saying. She is saying nothing about what works for you. I hope I have made this distinction clear enough.
Report comment
These powerful CNS drugs have powerful effects, but the main issue in MIA is the LONG TERM consequences of taking antipsychotics and antidepressants. These drugs may have stabilizing effects at the beginning but long term patients are often worse off than they started. Just go to askapatient.com.
Report comment
I’m very happy for you that it works. It cost me my sanity, home, family, everything I hold dear. It was literally the worst of the bunch, but hey, what woman REALLY WANTS orgasms anyway, right? They’ve tried everything from amitryptaline to zoloft, every one of them only made everything worse. Congrats. I’d literally kill for them to get off this serotonin kick and figure out something that works WITHOUT making so many people psychotic.
Report comment
If SSRIs help you, you should take them. If ECT helps you, you should have it. But those who have been harmed by it can speak about it too.
Report comment
Thank you for continuing to expose psychiatry’s fraudulent behavior, Mr. Whitaker.
There is the “serotonin deficiency causes depression and we have drugs to fix that” lie that in my experience was the first lie in a series of lies that led to me being permanently disabled. I don’t think I’m alone in this. When I didn’t respond to Prozac, Paxil, Zoloft, etc, my diagnosis was changed from depression to treatment resistant depression and I was sent for a consultation with a colleague of the psychiatrist who’d been dragging me for 6 years. That psychiatrist said that because of my treatment resistant depression, he recommended ECT. When I inquired about the possibility of cognitive impairment, memory loss etc from ECT, he told me that he had never had a patient who experienced memory loss following ECT.
After the ECT, I was impaired, greatly, and had severe short-term memory loss to the point that I could no longer perform at work. At that point the psychiatrist who had performed the ECT treatments told me that the ECT hadn’t “worked” because I was not depressed after all but instead I had something called borderline personality disorder. At that point, I was kept on antidepressants (which made no sense after being told that I wasn’t in fact depressed but instead had a personality disorder), but I was already getting the message very strongly that questioning the doctors would not lead to anything good. I was kept on the antidepressants but antipsychotics were added to the regiment as well as mood stabilizers. At that point the prevailing logic was that there was no drug for borderline but there were drugs to treat the symptoms. I started a DBT program and almost everyone I knew in that program was on a cocktail of psychiatric drugs.
When I think back on the years I spent in treatment, I try to pinpoint the moment that I realized it was all made up. Everything they were telling me was a lie. There were so many moments like that, but I was so desperate from the damage they had already done and everyone in my life kept pushing me back to treatment over and over again and denying me any form of support, I didn’t feel that I had a choice but to continue.
At one point a DBT therapist and a psychiatrist told me together that I needed to go inpatient for an ECT consultation. They happened to be close colleagues of the psychiatrist who had done the ECT that disabled me years before and who had told me that it didn’t work because I was not depressed but borderline. I explained this to them, explained the history, in as clear and uncertain terms as I possibly could. I saw that it didn’t matter. Logic didn’t matter. History didn’t matter. I saw that they just said whatever they needed to say in the moment to suit their own interests. That’s how it had always been. Lies on top of lies.
The mainstream media seems to have a problem reporting on the reality of psychiatry. Eventually, they did real reporting on the causes of the opiate epidemic, but it doesn’t seem like they’re prepared for a reckoning regarding the epidemic of death and disability caused by psychiatry. Maybe because the mainstream media played such a huge role in spreading the lies.
Report comment
“Lies on top of lies.” Indeed.
Thank you Mr. Whitaker for this brilliant blog. And as one who had the “chemical imbalance” lie spewed at me, I’m in.
Report comment
I wonder so often how come more people did not see this coming. My father was a psychiatrist and a generation before Peter Breggin, when Valium and Librium started to come on the market he very vocally declared he would not prescribe psychopharmaca and practice talk therapy only. He thought the whole thing was a fallacy, and refused. A generation later, Dr. Breggin saw the damage and became an expert witness against big pharma, while, like my father once did, he likewise committed himself to talk therapy only. But the bulk of people fell for this nonsense, because it seemed so easy.
Report comment
So easy, and so profitable. Kudos to your father for refusing to participate.
Report comment
It also shift the blame to the “client/patient,” so the actual powers that be can pretend everything is OK and that anyone having a hard time with the status quo is themselves to blame for not “adjusting properly to reality.” It can be a seductive idea for troubled individuals as well, as it promises path to feel better without having to examine any of one’s own beliefs or behavior. Of course, this leads to further troubles, because no one is looking for root causes, but it does keep the Benjamins coming in to psychiatry and their close cousins in the pharmaceutical industry.
Report comment
most of medicine is not much better than giving somebody a cup of coffee after ten drinks and telling them they are safe to drive. Giving them an aspirin to suppress the fever and putting them back on the assembly line, contagious as they may be, just because they can still walk. Or, for that matter, dressing up the slaves for sale with shea butter, and making them look better than they are in truth. All the same: make-believe medicine, suppressing the symptoms.
Report comment
SSRIs are not even good as that. Instead of “suppressing symptoms” they often cause severe problems, like akathisia. If they were just worthless sugar pills it would be bad enough, but they actually cause huge suffering for many people.
Report comment
All too true, Rogier. The hard question is why their shenanigans and dishonesty are still not obvious to those in society at large. It’s not even a very good con. I think it’s only our culture’s faith in “science” and “medicine” that allows them to get away with it, that and a massive dose of pharmaceutical company marketing. Hard to know what to do with such irrationality!
Report comment
Steve, I think there is an element of our cultures willingness to turn a blind eye. In much the same way the people of Germany did during the time of the National Socialists.
At this point in time they are obtaining a benefit from it. In much the same way that the books looked pretty good while the N.S. were stripping resources and obtaining free labour from various stigmatised groups. At some point the people who have been damaged are going to be a financial burden……….. and what is going to be done then?
Here’s one we prepared earlier, a Euthanasia Act demanded by the community. One with no numbers being collected, and the ability to “edit” documents to conceal the facts of matters and undermine the legal protections boasted about when it was passed. And we know that once your under the ‘care’ of the Mental Health Act that basically anything that is done to you can be called ‘medicine’, and the police can be used to stomp your head for non compliance with ‘doctors orders’. This includes ‘assisting’ you to die, the voluntary nature of it can be “edited” post hoc. Ask the Mental Health Law Centre principle lawyer about how that works lol
You going to complain to the Schutzstaffel about the Schutzstaffel? I tried, and got ‘referred’ for a ‘snow job’ for my “hallucinations” that police take complaints about criminals rather than refuse to take the proof while they call the criminals to pick up the complainant. I know I know, a few threats to the witnesses and their families and “It never happened”.
I think there’s more to it than just culture, more our regression to a state of fascism but…… time will tell.
Report comment
I think it is fairly simple. The time of enlightenment and the scientific revolution took away the authority of the Church, and faith was moved to the new secular priesthood. And the masses place their belief there, and it will be abused. It always will be. The old Roman saying mundus vult decipi, decipiatur ergo. The world wants to be fooled, and therefore she will be.
Report comment
Or as I said to the Catholic Priest/Senior Medical Officer who thought he would take advantage of someone in his ‘care’ who had been ‘spiked’ with date rape drugs without their knowledge, and who he forced to remove their clothing before inserting objects into their mouth or anus when consent had been expressly denied…….. “vulpes pilum mutat non mores” (The wolf can change his fur, but not his nature).
Some people lack the ability to pick up on these ‘deviants’…. me, i’m a little more sensitive to the signs. The Anglican Arch Bishop seeing child rape as being a “character flaw” and not a criminal offence worthy of reporting to the authorities. Amazing what you can do when your working with grounds we consider to be reasonable (as opposed to “reasonable grounds to suspect”). Negligence becomes your friend.
And what better place to find potential non consenting victims that can be easily silenced than in the Adolescent Unit? No wonder it took him three minutes to do the “Provisional Diagnosis”…. he was in a hurry to get back to the beauty of youth. Still, better he does further damage to already ‘damaged goods’, than target the children of the rich and famous? Not my position on the ‘care’ of vulnerable individuals, but I’m not the person running the ‘show’. Nor am I of the opinion that the non professionals simply wouldn’t understand how difficult the job is.
And perfectly positioned (as a psychiatrist, or someone bluffing he is to obtain interviews he would have otherwise been denied….. ie “implied consent”, I just didn’t tell them I wasn’t the psychiatrist and they went along with my instructions….. or got ‘smacked’ by the staff.) to ensure than any of the victims of his colleagues (from the Church) never get to see the light of day again until they cease complaining? Who needs an Ellis Defense when you have prison and forced drugging as a defense?
I note they gave Rolf Harris an Order of Australia too….. despite his well earned nickname of “the octopus”.
Forging prescriptions for the administration of date rape drugs, conspiring to pervert the course of justice, conspire to kidnap (in collusion with the Community Nurse, just tell police he is our “outpatient”), medical records from a Private Clinic presented as being his ‘work’,……. the list goes on eh Doc? Lucky you have ‘friends’ in High places and can forgive yourself and never…… under any circumstances, EVER confess huh? Eavesdropping another breach of the trust of the community?
Report comment
Peter Breggin sparked my questioning of the SSRI mythologies/dogma. Another Dr. writer, first name Peter last name can’t remember, came out with a book extollling the virtues of Prozac/SSRIs around the same time. I read both. I found Breggin’s more compelling, the other one more appealing. The difficulty of standing up to popular orthodoxy is even harder when our own desire for a miracle cure lurks within, waiting to jump on bait like Prozac.
Report comment
Peter Kramer: “Listening to Prozac.” I think Breggin wrote a critique of that book called, “Talking Back to Prozac!”
Report comment
Yes, that was it. Thanks.
Report comment
I am ecstatic to see a lawsuit being considered. Problems with the mental health system should be handled in court rooms and attorneys’ offices, but never in psychotherapists’ offices. In a civilized society a court room is where you restore your public honor.
And I say this now as California Governor Gavin Newsom is on the verge of getting his Care Courts SB-1338 passed, special courts to subject the unhoused to involuntary psychiatric procedures, and conservatorship for those who don’t cooperate and adhere to a “treatment plan”.
https://www.madinamerica.com/2022/04/saving-lives-cementing-stigma-review-just-like-you/#comment-200120
The mental health system is central to familial abuse. Behind Gavin’s mental health approach is Sacramento Mayor Darrell Steinberg, who tracked his daughter into the mental health system at the age of 13. We still don’t know much about this except that today at the age of 27, she still believes she has a bad brain, bipolar 2. Steinberg has built his entire political career around mental health, and he has started the Steinberg Institute, with Thomas Insel in charge of it.
And then State Senator Susan Eggman, whose family tracked someone into the mental health system, saying that mental health issues “drove her onto the street.” And Eggman laments that she “refused all of their efforts when they tried to help,” trying to legitimate forced treatment. Eggman has built her entire career out of targeting family scapegoats, via mental health and via euthanasia.
And then Thomas Insel supports all kinds of drugs, and forced treatment and electroshock.
He has drugs which create the euphoria of sex, and he has LSD. And he has a startup company which will have everyone checking in for auditing via their cell phone.
So of course we should be suing. This is all government licensed practitioners using imaginary illness to try and advance their theories. So it is clearly within Nuremberg precedent for Crimes Against Humanity. It should be prosecuted in the International Court, and then no one is above the law and there is no Statue of Limitations.
But for now we start with the legal actions we can.
I try to find out what legal actions are underway and I think this is very important, but finding out is very hard.
Joshua
Report comment
First I want to say that I feel very positive about what seems to have become more and more an anti-psychiatry viewpoint being presented by MIA.
As far as a class action lawsuit, I think it is a great idea, but if it happens it will take a small army of public interest lawyers. The other side will gather a large army of high-powered corporate lawyers, and a large fortune of funding from the drug companies. But I am sure you know that.
I wish my law practice had been more high-powered, and that I was still practicing, so I could help with this enterprise. Any lawyers who take on this challenge, will, I think, be performing a great service to humanity.
Report comment
I keep wondering about the attorneys who took on Purdue Pharma over Oxycontin and the other drug companies that marketed opiates based on lies.
It seems like taking on SSRI manufacturers over false claims of their mechanism of action and failure to provide informed consent, etc, the lawsuits would utilize some of the same strategies? I wonder if the successful class action suits against Purdue, etc, have established precedents for suits against psych drug makers?
I’m also wondering if not only the pharma companies but the FDA could be held liable for failure to warn consumers of the risks, etc?
Report comment
A handful of law firms took on the various Big Pharmas over SSRI-caused suicides/homicides and won big awards. I suspect this is still happening, one case at a time. Though such cases are not what Bob proposes here, perhaps they could be included in the broad definition of “damage done”.
Report comment
I wondered the same thing about the FDA. They clearly lowered their standards for drugs treating DSM conditions. They seem to have a history of believing bad research and then not taking corrective action when new side effects are learned. The drug companies all plead guilty to making false claims about these drugs yet never made them correct the harm.
Report comment
Bravo! Keep up the pressure. Those of us in the trenches keep trying, client by client, to educate on these issues but it feels like a Sisyphean task. The myth of chemical imbalance is firmly implanted in the cultural zeitgeist and will take several generations to eradicate. Heartbreaking to see the lives destroyed. But they don’t listen to me, because their PCP or psychiatrist “MUST” be smarter and more well informed than I am.
Report comment
I am eager to join such a class action if one were to materialize. I can be reached through MIA’s moderator Steve McCrea if any lawyers want to reach out.
Report comment
Kindredspirit
(I posted this recent comment in another very old thread that you might not have seen)
Kindredspirit
I am so glad you are posting here at MIA again. I read some of your past comments regarding your decision to step back for a while.
I wholeheartedly agree that MIA has lost some of its past activist edge, and has somewhat retreated into a more limited “educational” role. This “educational” role has unfortunately been divorced (and consciously steered away) from some of the more volatile polarizing developments in the broader society.
It is a mistake to separate the intense battles over science (on many fronts) and “alternative realities” in the current political realm, from what is happening in the overall battle to end psychiatric oppression and the medical model.
I DO understand the intense political pull (“on the path of least resistance”) to steer things away (and separate out) these struggles, for fear of losing part of your audience. I also believe all this was happening (at the same time) as the earlier wave of anti-psychiatric activism was suffering an overall ebb from a previous high water mark of activism – that is, the 6-8 years following the 2010 arrival of RW’s path breaking book, “Anatomy of an Epidemic.”
During those years there was a failure on the part of existing activists to consolidate some type (or types) of advanced anti-psychiatry organizations to take advantage of the current crest of political exposures and activism at that time. These rises and falls (ebbs and flows) are a natural occurrence in long term political struggles, and we have to analyze and sum up these developments (and our mistakes) in light of current political developments.
I don’t have to tell you just how polarized and dangerous the current political climate is, and how important it is for us to chart a course that will move things away from a devastating form of Right Wing totalitarianism.
On a positive note, I do notice a growing deeper political frustration and anger in MIA content, that reflects the awareness that simply doing more and better exposures of psychiatry and the medical model will not just somehow cause their “house of cards” to fall.
Psychiatry and their medical model has now evolved into such an important cog in the maintenance of the profit based capitalist system, that simply doing more scientific type exposures (and desperately seeking the broadest audience) will not fundamentally bring down psychiatry. Anti-medical model critiques will just be labelled as another “alternative reality” in the vast “marketplace of ideas.”
The struggle against psychiatric oppression and the medical model IS (by its nature) and must (more and more) become connected to all the other major struggles for social justice in an overall oppressive world. And this will require activism and political exposures, that are willing to risk losing part of ones audience, in order to uphold the truth and draw the very real connections between all of these important struggles. I certainly hope this is the direction things are going, and I will do my best to encourage things in this direction.
Carry on! Richard
Report comment
Mr. Whitaker,
Thank you from the bottom of my heart & soul.
Humbly, I would be honored to join/help the suit, give a deposition, bring my 10 years of medical records, including hospitalizations & ER’s, correspondence, 9 months of texts with my ‘exit doctor’,..including his text request for a date (before I left his service) that I preserved, (he’s still the CMO/VP in a major SW city), and medical history of micrography & 19 seizures post 2 1/2 years of guided withdrawal. All those records given to me (my request) as I ran for my life out the door.
I’m the one who got them to remove my lifetime diagnosis-they had no problem jettisoning the 11 years of dogma to avoid a possible (minor settlement) lawsuit regarding anaphylaxis they had caused. I never mentioned one, but…. I ‘negotiated’ for myself. So they called me ‘cured’ (!) of lifetime bipolar 1 and an Arizona SMI certification plus permanent disability.
Who knew anaphylaxis was apparently ‘a cure’ for a bipolar disorder? A miracle!!…they kept it quiet, but it’s ‘on-the-record’ as I have ALL the paperwork.
I sent an email to the APA asking why this wasn’t ground breaking news?
The other person I found that paralleled my timeline and diagnosis removal sued for $35 million (K.C & Chicago) but reportedly was thwarted by statute of limitations. If your disabled/drugged by the defendant during those years, it seems inequitable…
Anything I can do. Anything at all. Or nothing, I’m just a grateful past target.
(I wrote for MIA 2019-“Full Moral Status”, 2 parts. RxISK.org 2018 “The Unicorn: Changing a Diagnosis”, 4-parts)
So stoked.
To the APA & Pharma…..
Suck it.
Report comment
Krista,
I have some questions. Can you please private message me on Twitter?
https://twitter.com/JClariceEdwards
Report comment
I am very interested in what can be done with this, as it regards filing a suit. I’m not sure how one would go about it, but I would be completely on board. I was given my first SSRI (prozac) in 1998-1999 and over the next several years I was prescribed a few others- not at the same time, of course.
At the age of 21, I had a heart attack. I was healthy, had never used street drugs, nothing. My doctor had just put me on Zoloft and I kept telling him that something was off/wrong, that I didn’t feel right but he just told me that the drug had to get to theraputic levels and I needed to trust the process. He just wouldn’t hear it. Meanwhile, I was unable to sit still, my heartbeat was off, jumping out of my skin, I was so hot that my ears and face were red and if I held ice cubes in my hands water would just pour out.
The day I ended up in the ER I had collapsed at work and was so sick the co-worker who took me to the hospital though I was going to die. This was 32 days after I began taking the Zoloft. The suspected that I had serotonin syndrome, but I was stabilized in the ER, referred to a cardiologist, and sent home. After this I was so scared I refused to take them for a few years- but eventually I found my was back because my family said I wasn’t functioning. I was put on Celexa and later Lexapro.
Still, I took them, weaned off of them, and tried to feel normal. I was on Lexapro when I found myself pregnant with my first, then back on Prozac several months before becoming pregnant with my second, and continued with it after giving birth. I worry about what those drugs could have potentially done to my kids.
And now I’m told that there could be a link between SSRI and subsequent diagnosis of Bipolar Disorder. Well, I was just diagnosed with Bipolar I with phychotic features & rapid cycling. My new doctor told me that SSRI meds could definitely have played a part in the rapid cycling.
And there are so many more with very similar stories. So many people- human beings- who have been essentially sacrificed on the alter of big pharma and corporate greed. Vultures.
Yeah, I am completely invested in a lawsuit. Just tell me how to help.
Report comment
This article leaves me gobsmacked!!!. I am the unfortunate beneficiary of this unholy Trinity of lies. My introduction to psychotropics begain in 1995 and have evolved from Prozac to now a combination of six. I had kidney failure from lithium in the early oo’s, healed thank goodness. At 70 I still take this plethora of stuff that’s never made me feel better, constipates my bowels and my brain. But I ‘ve been made to be afraid to not take my medication. Yes to a Class Action Suit, make them accountable.
Report comment
So they fold up the card table on the corner, put the three cards in their pockets, and run with the money they have scammed from people.
That money will be well hidden by the time any lawyers manage to get anything to court.
Shave their beards off, and set up on another corner within a week.
Always good to dream though. Not a chance of anything happening in Australia due to the corrupt nature of our legal system which would allow the lawyers who brought the claim to take a ‘back hander’ and throw their clients under the bus. The Mental Health Law Centre has been doing it for years. Violation of human rights? Not a problem, find out what the victim has got, and then conspire with the State to “fucking destroy” them. They simply refuse to allow anyone to complain, and call them mentally ill and require treatment. Works an absolute treat, people think this is a good place. Till you ask an aboriginal….. well, avoid that and it’s a good place. Mind you, Germany was looking good there for a while. Truth causes all sorts of problems once it gets out.
We don’t even have a right to consent. Hospitals ‘spiking’ citizens and then writing fraudulent prescriptions for the covert administration of these drugs? Australian Health Practitioners Regulation Agency board doesn’t even see the problem. ‘Consent? What’s that? We do what we want, and silence any complaints with the Mental Health Act and the criminal negligence of police’
I’ve got a letter here from the Law Centre with a complaint about me being ‘spiked’ and snatched from my bed and not informed I had been drugged with date rape drugs before being interrogated. And the response from our Chief Psychiatrist which make good reading. Care to take a look?
I know the ‘advocates’ took a look and then ‘unread’ the letter, along with a number of lawyers (and a Member of Parliament). Quality of the work is questionable, given that I don’t think the Chief Psychiatrist has the power to rewrite the Mental Health Act and remove legal protections afforded the community. How can he do his job when he doesn’t know what the protections of the law are? No need when you can threaten and intimidate peoples families while you ‘treat’ the victims. But if none of you look then ………. what is that smell coming from those chimneys?
Report comment
Boans,
I’d love to see the chief psychiatrist’s letter. Also, what is “spiked”?
Report comment
Hi skeetbeet.
‘spiked’ is when you put drugs into someone’s drink or food without their knowledge with the intention of stupefying them. Do it with the intent to commit further offenses (such as kidnapping, or sexual assault) and you can be in serious trouble…….. If police have a copy of the Criminal Code in the particular station where you try and report the offences. Otherwise they call mental health services and try and have you hit over the head with the ‘chemical kosh’ and removed from their fine establishment.
There are four ‘date rape drugs’ called ‘intoxicants’ (unless administered by a doctor who can write prescriptions [even then there can be problems, see the case of Prof John Kearsley] at which point they are ‘medicine’) and which are used by many rapists in nite clubs in particular.
Ketamine
GHB
Rhohypnol
Benzodiazepines.
There is a defense in law;
“to prove that the accused person had reasonable cause to believe that each person who was likely to consume the drink or food would not have objected to consuming the drink or food if the person had been aware of the presence and quantity of the intoxicating substance in the drink or food.”
In my situation the fact that the people who KNEW that I had been intoxicated by deception conspired to conceal the offence……… so they obviously thought I would object. And in fact, I have NEVER been prescribed these drugs, and when a nurse in the locked ward offered them to me, I suggested he use them as a suppository (ie stick em up your …… ).
So I wasn’t informed until it was apparent that my legal representatives were to be provided with unredacted documents showing the offenses, 6 weeks after. They had tried all sorts of deceptions to ensure I didn’t find out. Trying to have me sign documents to make me into someone’s ‘patient’ after the fact to enable their conspiring to be ‘medical care’.
The Senior Medical Officer who I had never met, writing a prescription for the administration of these date rape drugs hours AFTER they had been administered, and despite knowing I had been subjected to interrogations by a Community Nurse AND Police. How easy is it to conceal acts of torture in my State, who have actually complained about this being done in African Nations. Torturers that they are, but when ‘we’ do it, it’s ‘medicine’
I have the letter in PDF form, and have redacted the names. I feel sure that the way the law has been rewritten to remove the protections afforded the community is clear for all to see, but have had lawyers ‘unread’ the letter to ‘unsee’ what they are instructed to not see by the State. And hey, it’s only the family of a mental patient that has been ‘fucking destroyed’, not like it was someone that matters. Well, okay I wasn’t a mental patient when this was done, unless you consider the Community Nurse lying to police and saying I was an “Outpatient” of his hospital to procure the thug services of police to force me to talk whilst stupefied without my knowledge…… you know, receiving ‘care’.
One might suggest that this is because they were dealing with the matter in a ‘quiet’ manner…. but why was this person who did these vile deeds still harming people TWO YEARS AFTER he should have been reported to the Corruption watchdog under the MANDATORY reporting provisions? (lest the person not reporting suspected misconduct commit an offense).
There is no need to report when the documents have been “edited”, the legal representatives have thrown the victim under a bus, and the victim is delivered to an E.D. for ‘treatment’ (which is a great way to terrorise others into silence I note. You wouldn’t want what was done to me done to your family kind of thing.)
The Operations Manager was quite open about her offending (as a representative of the State). Telling me when I ensured she was aware of her duty to report that “we’ll fucking destroy you”. And with the Chief Psychiatrist able to remove legal protections from the Mental Health Act (is this what they call “grandiose”? That’s what I got called for suggesting I had human rights to the Senior Medical Officer. That and whatever other slander he could fabricate with words without too much effort in his “three minute diagnosis”).
Anyway, quite happy to share the letter, from the person who “provides expert legal advice on matters of Mental Health law to the Minister”. But, I might add, who would fail a first year law course at the Mahatma Ghandi Online School of Law lol
The letter was FORGED by the Law Centre and handed to someone they KNEW had been viciously attacked and gaslighted, to cause significant psychological problems……. and let me tell you, that letter almost contributed to my death. I’m sure they feel no shame over the matter though (just following orders), the author going on to run for Federal Parliament despite these facts being known to our ‘authorities’. Just what we need, forgers and utterers in Federal Parliament instead of ‘providing access to the law to the vulnerable of our community’ with her offending..
‘Sorry, we haven’t got the resources to assist people who have been subjected to human rights abuses by the State, we’re too busy at the Audi dealership picking a colour for our new cars with the increased funding were getting from the State for NOT looking at these abuses’ You could try seeking ‘help’ from the people that did this to you? Because the “edited” documents make you into a violent psychotic drug abusing wife beater, and now that police have ensured your homeless….. well, things aren’t looking too good for you. Nothing that cant be achieved with a little bit of “editing” and gross criminal negligence.
Might be time to redo some ‘exams’ in the place our aboriginal population calls ‘University’ (ie Prison)
Report comment
Boans,
Thanks for clarifying what “spiking” means in a medical treatment.
That’s similar to what a group of researchers did to ER patients (links below). They administered ketamine to 1700 “agitated” patients without their knowledge/consent to see how quickly it works compared to Haloperidol:
“…People brought to the emergency room with “severe” agitation, as assessed by emergency technicians using criteria developed by the researchers. The study leaders apparently persuaded the IRB [Internal Review Board] that such patients could not provide informed consent, and so could be swept into the trial unknowingly.”
Thirty-nine percent of the patients had to be intubated for ketamine-induced breathing issues (compared to 4% for Haloperidol). The “participants” of the study were never informed that they had been used for experimental medical research, that they were given Ketamine during their ER visit, or that it caused their breathing issues/need for intubation.
The FDA did nothing even though the researchers had been cited for ethics violations in human medical experimentation.
It’s unconscionable & scary that practically any medical or law enforcement personnel has the authority to slap psychiatric labels on a person to prevent them from exercising their rights to bodily autonomy, informed consent, due process/legal protection, freedom of speech, thought, expression. “Chemical Imbalance” diagnoses effectively silence, disempower, & allow many medical crimes to be covered-up or legalized.
The damage from the “chemical imbalance” marketing ploy extends beyond psych med harm. It legalizes discrimination, mistreatment, & deprivation of rights. Individuals with psych diagnoses have to pay more for life insurance. They may lose their job or be locked out of certain jobs (especially military & government). It allows medical providers to dismiss patient concerns/symptoms as “psychiatric” & even refuse them treatment & testing, thus endangering the person’s health, safety, wellbeing, functioning, quality of life, & life span.
It is imperative for this lawsuit to move forward. I’m in.
https://www.medscape.com/viewarticle/975036
https://www.statnews.com/2018/10/29/er-patients-given-ketamine-powerful-drugs-without-consent/
Report comment
Wow, THAT is scary as hell! How can they experiment on people without telling them they were participants? Holy Tuskegee Institute, Batman!
Report comment
Yes, that is kind of scary.
And it is the case I believe that in Australia the idea of such a lawsuit would be laughed about. I know for a fact that the medical fraternity was provided with immunity from any lawsuit relating to the vaccinations, and the same is basically true with any other form of ‘medicine’ You could literally run a Unit 731 experiments in this Nation and nothing could or would be done about it. (see for example the lack of action in the case of Garth Daniels who we watched basically being killed)
I suppose that in some ways, it works against the State to leave such matters festering. For example I play golf with a Consul General of a large Asian country with a Consulate here in the State capital. He goes back to his country and tells them that they are taking a risk by coming here and being tourists or sending their kids as students because the State simply ignores the human and civil rights legislation? They are ‘at risk’ in such a place that refuses to right wrongs, and abuses human rights and then “edits” the facts with fraud. Maybe the reason the Canadian Embassy is so quick onto their citizens ending up in one of our ‘hospitals’? Something they know, that others don’t? I was impressed I must say.
Same goes for me sitting with the Grand Mufti and the President of our National Islamic Councils who understand the right to bodily integrity as a direct result of intoxicants being Haram. I’m sure they have a right to be informed of the risks they are being exposed to by the gross criminal negligence of those with a duty to act on such matters. The Chief Psychiatrist doesn’t recognize the protections afforded the community in the law, and removes them with a misrepresentation? Allowing not only me but also them to be ‘spiked’ should the need arise. I felt at ease sitting sharing food with these people, as we share some values in regard the tampering with peoples food and drink without their knowledge.
Even the unfair Treaty of Huddabiyah wasn’t distorted beyond recognition by the people of Mecca. Imagine them going to the Muslims in Medina and lying about the status of citizens to have them wrongfully detained and returned for ‘treatments’.
So whilst they may have “fucking destroyed” me, I think that the people watching as Bilal ibn Rabbah was tortured realised that the person who was doing the torturing wasn’t the good person they actually claimed to be. I even have a “With Compliments” slip provided as a receipt for my body by the Community Nurse as he had police throw me into a police van in front of my mother and father in law for my “potential for damage to reputation and meaningful relationships”. Glad they ensured that my potential didn’t actuate.
This not being a reason to scrap the whole Treaty, and it was after all agreed to by Muhammad (saw) who received some resistance when he stood by the agreement he had made, and returned Muslims to the people of Mecca to be incarcerated and tortured (see the Day of Abu Jandal).
So as you can see, it may be that the Muslims hearing that our ‘medical fraternity’ is enabling the ‘spiking’ of citizens with intoxicants and the lying to police regarding their status actually has a history within Islam. And whilst we have a social contract that will be honored, it might just be the case that cooperation will depend on the very black letter of the law.
Personally I would have thought resolving the matter with truth and justice foremost may have been best. But as noted in the Quran, there are many who prefer the means of fraud and slander, and who think they can conceal the truth from God. They scheme, and He schemes, and Allah is the best of schemers.
I think that KNOWING that you can rely on the people you have contracts with to perform their duty according to that contract (and it is seen that they have done so) is the best way for friendly relations to remain in place. The refusal of the Chief Psychiatrist to even recognise the terms of our ‘contract’ by misrepresenting them, is an offense to all of our people. Leaving these people in positions where they can harm others (for more than ten years now) is not really what on would expect given the serious nature of what they did, AND that they were aware that what they did was criminal. And such a shame that in more than 8 years he has simply refused to even acknowledge the facts or the truth. Or is he being ‘obstructed’ by others who stand to loose something by acknowledging the truth?
The documents are there should ANYONE care to examine them.
Thanks for the information Skeetbeet.
A side note, the “added protections” inserted into our MHA in 2014 are basically protections from those nutjob mental patients out in the community. You know, anyone that isn’t ‘them’. “Outpatients” who the Community Nurse used to have to lie to police about to arbitrarily detain and torture. That has changed, and these days Police have been procured by having a Community Nurse in the Police Station who can be called by doctor to go and get his ‘potential’ “Outpatients” for delivery to the locked ward, pre drugged and ready for interrogations.
It’s much easier to do what was done to me these days, and the community never got the Memo.
That’s what they call “added protections”. Added protections from YOU. ‘A mentally ill man was arrested today for walking through a car park where the Minister for Mental Health was. He was admitted to hospital for his injuries inflicted by police when they tried to ensure that he didn’t breathe in her general direction, and for wearing a loud shirt in a public place (what you get when police haven’t got a copy of the Criminal Code I’m afraid)…. part of the new ‘added protections’ in the MHA. Condolences have been offered to the family, and the documents “edited” to ensure clarity for the legal representatives of the man and his family. Police have stated that “it never happened” and any further enquires will result in harm to journalists families’
Report comment
SSRI class does sometime provide pain relief (wasn’t this ‘discovery’ accidental in the beginning?). People with depression want pain relief. Yes, psychiatry ought to be forthcoming, but it must wait until new news morphs into solid-seeming science, which itself always changes in time.
If one really wants to help, then stop nerve damage before it happens… broadfork (communication website).
Report comment
Bob Whitaker, thank you for another stellar article and for the call to action on putting together a class action lawsuit. I’ve written my story and my mother’s of psychiatric mistreatment and would be happy to join in such a lawsuit. How dare psychiatrists try to dismiss the notion that they ever told us we had a chemical imbalance in the brain which caused depression, anxiety, bipolar, etc. Many of us here on MIA were repeatedly told this lie and though we may not have a written record of it, we well remember the experience.
What I fail to understand is that if there is no evidence of a chemical imbalance in the brain leading to mental health issues, why do psychiatrists continue to prescribe antidepressants which then disrupt brain chemistry? And why do they support brain-damaging “treatments” such as ECT and TMS? Oh, yes, I’m all in!
Report comment
This is fantastic! Sounds like an excellent, well-thought-out plan, and with so many people who want to sign up, there is a good chance that it will work.
One thought I wanted to add.
Many people say that antidepressants work for them. My response to this that many people say exactly the same about alcohol and nicotine: having a drink or a smoke helps them to relax, to forget their misery, lifts their mood. And not everyone gets harmed in the end.
When I worked in high school and talked with my students about drinking/smoking, I often heard, “My grandpa has smoked since childhood, he is 75, healthy and active,” or “My aunt was drinking every day through her pregnancy, and the baby is healthy and is doing great,” etc.
So, yes, psychotropics — SSRI, vodka, nicotine, you name it — do help some people, without damaging them. The problem is that you never know if you are one of these people before you try.
Report comment
I was thinking about this the other day.
Thank you for everything you do!
“Dream until your dreams come true.”-Aerosmith
Report comment
Does “depression” cause hopelessness?
Have we all been led to believe this?
Or is not “depression” simply hopelessness, itself?
And is hopelessness (whether we consider it “endogenous” or “exogenous”) not always a symptom, never a disease?
Thomas Szasz (The Myth of Mental Illness) suggested that what has come to be called “mental illness” is “problems in living.”
I believe Joanna Moncrieff put it, in one of her presentations, “human suffering.”
If so, I agree.
“The human condition: lost in thought.” – Eckhart Tolle in “Stillness Speaks.”
Left to its own devices, our minds, defense/survival mechanisms, are, for the most part, anxious and depressed” as well they might be, pretty much entirely preoccupied with our physical survival/reproduction, so that “happiness” or “peace of mind is fleeting and hardly worth pursuing (thank you, Founding Fathers), whereas the joy within, peace from mind, may provide us with lasting peace.
What organic illness or injury might not cause depressive symptoms?
Which nutritional imbalances might not?
Which acute or prolonged stresses might not?
Which underlying “pathologies” might not?
“The psychiatric research community has long known that the low-serotonin theory didn’t pan out and that, in fact, the field long ago moved on to new theories about the possible pathology that gives rise to depression.”
I doubt anyone can feel more grateful to and admiring of Robert Whitaker for all the magnificent, meticulous, painstaking and uniquely inspiring work he has carried out for such a great cause.
Not least, I have admired how he has so consistently emphasized that what he is about to say is “as seen through the lens” of Psychopharmacology or of the authors of any works he is referencing – the medical model.
And perhaps this unspoken proviso was implied or intended to preface that above quotation, too?
If we blandly, carelessly, thoughtlessly or unwittingly accept that “pathology underlies depression” we have already missed the point, I think, and, I hope, strayed from Joanna Moncrieff’s own opinion, too?
Psychopharmacologists (I do love that term) may have succeeded in persuading so many folks to drug themselves primarily by persuading them/society that “Depression/Major Depression/Clinical Depression/Bipolar Depression/Double Depression/Dysthymic Disorder/Psychotic Depression” or, nowadays, “PGA/Prolonged Grief Disorder” may cause hopelessness, a sense of hopelessness, or feelings of hopelessness.
They may avoid the terms “despair,” or “sloth,” perhaps anxious to avoid drawing attention the fact that what has been seen in Judaic, “Judeo-Christian” (or, perhaps more accurately Judeo-Pauline) and other traditions as “Sin” is now largely regarded as “mental disorder” and/or personality disorder.”
To suggest that “depression” or “schizophrenia” or “psychosis” is a disease without a shred of scientific evidence to support it is absurd.
Those who have persuaded us and our justice systems and judiciaries to believe absurdities have indeed persuaded us and our justice systems to commit atrocities towards one another.
“Coercive psychiatry does not commit human rights abuse: coercive psychiatry is human rights abuse.” – Thomas Szasz.
Thanks to men and women like Robert Whitaker, Carl Jung, Thomas Szasz, Loren Mosher and Joanna Moncrieff, it seems this may soon cease.
Heartfelt thanks.
Tom.
Report comment
Very well said. The comment “Depression causes hopelessness” is an absolute meaningless sophistry. It’s akin with saying “A sore knee can cause your knee to hurt.” The attempt to make “depression” into some kind of an active, evil entity that “does things” to us is the most destructive and disempowering way one could possibly view the situation. It is the opposite of the kind of thinking that can actually help us move past feeling hopeless. It is hard to fathom how they continue to get away with these syntactical idiocies!
Report comment
“It is hard to fathom how they continue to get away with these syntactical idiocies!”
“Stupidity is something unshakable, nothing attacks it without breaking itself against it, it is of the nature of granite, hard and resistant” Flaubert.
That’s how 🙂
Report comment
Never heard that one! Thanks!
Report comment
Spot on, Steve!
Report comment
Steve, many thanks.
But I do not believe it is sophistry on the part of anyone, but rather than “they” – “we” – have all been duped into thinking we are miscreants, disordered, defective, broken, unworthy, having the wrong personalities, not being adequately fitted by Nature Herself for whatsoever purposes She intends us – exactly like the priests and clerics of old believed that they are we we sinful, and any serpents in any gardens believed the bs of which they persuaded any adams and eves: we are all equal victims of the delusion of being less than infinitely pluperfectly equipped to carry out whatever we need to do, so-called perps and victims alike, all equal, as I see it.
Then we witness works by the likes of Robert Whitaker, Carl Jung, Cervantes, Seamus Heaney, Jesus, Ridley Scott, Stephen Spielberg, Joan of Arc, or Joanna Moncrieff, and remember that we are all equal, and so must have within us that which each of those personifies, and infinitely more, at least.
“Nothing happens to anyone that he is not fitted by nature to bear.” – “The Gladiator,” and Marcus Aurelius, and every spiritual teacher, I guess?
“In all chaos, there is cosmos; in all disorder, a secret order…” Carl Jung.
“Life will give you whatever experience is most helpful for the evolution of your consciousness. How do you know this is the experience you need? Because this is the experience you are having at the moment.” ― Eckhart Tolle.
“…for we are all as God made us, and many of us [sometimes rendered “and frequently”] much worse.” – Sancho Panza, with Cervantes’s whatever about Sancho’s tongue firmly in cheek, presumably, for how can any of us ever have been “made” or be any worse than any divinity of which we are an inseparable part, and always have been, with neither beginning nor end?
“No man chooses evil because it is evil; he only mistakes it for happiness, the good he seeks.” – Mary Wollstonecraft Shelley.
“PersonALity disorder?! Ya can’t have a personALity disorder! Your personality – that’s, like, who you ARE! That’s, like theee rudest thing – eh-vur!” – Our then-16-year-old Liz, making me laugh, again, even if I think we all manifest many personae, as well as being Being or Awareness, Herself, including that endless medium into which this last big bang is expanding, and much more I cannot yet begin to imagine.
When we are laughing, we get it. When we are not, maybe we simply don’t – yet: “God is a comedian, playing to an audience too scared to laugh.”
Comedy = Tragedy + Time.
Let’s keep on laughing, Steve: “God” rest you and all of us merry.
And thanks, again, Steve McCrea: I am so glad that you were just what I needed just now, to return me to right back again towards Heaney’s “From the Republic of Conscience,” from which I stray, daily.
Beir bua.
Tom.
Tom.
Report comment
Mainstrem media writes about it, because there is a crisis going on and there will be problems with supply chains. Addicted people won’t be able to get antidepressants.
Report comment
SSRIs are very widely available and have been for many years, along with a host of other psych drugs. If they worked, there wouldn’t be a crisis. (assuming you’re talking about the “crisis of mental illness” that mainstream media talks about).
A class action lawsuit would not necessarily take SSRIs off the market or cause them to be any less available than they are now. A class action lawsuit would be to get the makers of the drugs and perhaps the psychiatric establishment to acknowledge that they have lied about the drugs for decades and harmed patients. The lawsuit would be to make the drug makers and doctors give informed consent.
Report comment
“there will be problems with supply chains.”
And we saw the problems caused when the Taliban pulled up all the opium poppies in Afghanistan. We’re still trying to shut down the Meth labs that sprang up to ‘fill the gap’.
Report comment
What is needed is a RICO case here. Oxycontin was approved by the FDA and claimed to be extended relief for 12 hours which was false and that it was non-addictive and it still is on the market. It was a conspiracy to harm and many actors worked to conspire to promulgate the SSRI’s. But the problem is proving harm since the package in the pharmacy inserts that are attached to the bottles actually list all the potential and actual harm. Psychiatry is a LONG CON and there are NO medical reversals- never mistakes were made etc.
The system is set up to support, encourage and evade this type of fraud.
Report comment
Yes! I think a RICO case would be a great way to go
As to the warnings, many of us, including myself, were prescribed SSRIs in the 1990s, when there were no warnings at all. The only way they found out how dangerous the drugs are is by testing them on the public.
Report comment
I would say multiple RICO cases is the way to go. The only problem I will point out is that when college tuition is something like $200,000 per person, and then the correspondingly high salary increases you get for getting your degree are that much more rewarding compared to if you didn’t, and when the college educated population starts swelling bigger and bigger and bigger, you end up with a problem that people cannot back out of the system or choose a different occupation, the moment they find out their jobs involve criminal racketeering.
Once you invested in your medical school education, you are married to the mafia for life, basically. When people can’t back out, which people used to be able to do with respect to jobs that only required a high school education, the system is now capable of increasing the amount of criminality it requires of its participant employees, and how can they say no?
The legal system can police criminality so long as criminality is not the norm. When it IS the norm, I don’t know what they can do. They don’t have the time. The criminal racketeering that goes on today that academic institutions and corporations are involved with deliberately goes out of its way to introduce the kind of complexity and convolutedness to their schemes, so that it may not be impossible to bring RICO cases in certain circumstances perhaps. The biggest problem is the sheer number of man hours that would have to be involved, in just bringing one single case. And there are thousands of such cases, too many to count. The FBI cannot even begin to wade through it.
Let me see, how can I illustrate this. In 2010, I believe, or perhaps it was 2011, I had just started working with my second attorney on the racketeering scheme I had been a victim of since Harvard, which I had by then spent 15 years collecting evidence on, and trust me, this was a very good case and what I did was very clever. It’s an amazing legal case I mustered up. Exquisite. Something I am very proud of.
Well, around that time I have an email I wrote to one gay man I was emailing online about the matter, explaining that the number of computer files I have which are relevant now amounts to 8000 files just for the five year period from 2005-2010 alone. It would be 15000 files if I include everything from Harvard starting in 1994. However, some of these files are block files, which means each of them include hundreds of documents all saved in one file. So that’s an under-estimate. And this was all from simply doing a quick computer count on all the relevant files I had which I’d saved in various folders and marked as relevant. A quick computer count which does not separate out tons of block files which contained hundreds of different documents each.
In addition to all of that, however, I should note that the moment I started emailing the second attorney I had, I suddenly started being deluged online by huge numbers of gay men on a certain hook up site, all placating placating placating me. This was because my computer and gmail account were being hacked, so I could do nothing without the perpetrators finding out everything I did and staying one step ahead of me.
This placating of me — only after I go to that second attorney — was in such contrast to the non-stop campaign of death threats, hate mail, and harassment which same online community had been heaping on me for two years straight that I knew, this sudden contrast was very very relevant to “proving” that the (gay mafia) existed, or even if that’s not the best way to characterize it (it’s really more of a Harvard and corporate mafia run by straight male CEO’s than a gay mafia), at least it proves the gang-like pattern of behavior this community was engaging in nearly without exception. Let’s just say I had a legalistic background from before, so I knew how legally relevant these placating emails were.
So I started copying every single one of them, hitting print screen and saving to microsoft word, over and over and over again. Since, by now, the same website which maybe netted me on average two or three or at most five or ten emails a day from other guys probably was netting me hundreds of emails a day from guys, all placating me in the same way. And I saved every single one of them in a graphics file, except these were pasted to MS Word documents which quickly got hundreds of pages long and then had to be saved and then I’d start up another document which I’d say after it was well over 100 pages.
In less than a month, I wracked up maybe — I can’t remember if it was 5 gb or maybe more like 12 to 14 gb of memory. The files started taking up some ungodly amount of space, and then I simply had to stop further documentation. Because I knew if I continued it, I’d need to buy a bigger computer and I knew I couldn’t afford that.
So, by the time it would be a RICO case which the FBI might be in a position to investigate, there were probably thousands of emails from gay men online, just from a very short time period, which were suspicious enough so they all would need to be tracked down and very thoroughly investigated.
Except, I am sure, you know how the mafia works. Where one perpetrator may do something, only if it’s criminal racketeering and you investigate it, you might learn of dozens of people involved behind the scenes, for every one person who did something “overt” and in need of investigation.
Now I did all the right things which would make it easy for a government agency to investigate matters. You could say what I did was brilliant. And yet, it still would be a really really tough investigation involving extraordinary amounts of man power. Even while I carefully manipulated the perpetrators into at times making all the right explicit confessions that are easy to follow up on. Meaning, I was smart enough not only to make my situation become a legal case, but I was also smart enough to figure out how to make it so it can be efficiently investigated so as to reduce the number of man hours put into it.
Most victims don’t do the right things so they can be helped. And even if some of them do enough of the right things so they theoretically could be helped, they still can’t be helped because, well, the way investigations work, if something is too ambiguous, if law enforcement REALLY tries very very hard, as in devotes an enormous amount of time, yes they can still crack the case anyway. They are only able to reserve that kind of effort for a small number of cases like murders. Otherwise, they just don’t have the time.
Report comment
What kinds of lawsuits will work is mostly a matter of tort law, that is, precedent. So you proceed with the lawsuits that you can, and you stay ready for proceeding on the more difficult ones later. But this forum should be tracking all related lawsuits and legal precedents. This has been absent.
I write this as I am trying to follow the proceedings in CA Governor Newsom’s Psychiatric Internment law, Care Courts SB-1338.
https://www.madinamerica.com/2022/04/saving-lives-cementing-stigma-review-just-like-you/#comment-200162
The idea that someone is “mentally ill” always seems to have started with in the family. And these are the ones who clamor for official recognition that their child is the locus or original sin.
https://www.latimes.com/california/story/2022-08-04/mental-health-california-newsom-proposal-care-courts-aclu
We need laws that will protect people from being made into the family scapegoat. We need to be able to protect people like the daughter of Darrell Steinberg. And we need to be able to protect people like the aunt of Susan Eggman.
Eggman has spent her entire adult life getting the family scapegoats needled with psychiatric neurotoxins and with suicide drugs.
Eggman
https://www.youtube.com/watch?v=227f4j0bVHk
Eggman shows us how to convince people
https://www.tandfonline.com/doi/abs/10.1300/J010v35n03_04
And we need laws to protect people like Matthew Warren, youngest child of Rick and Kay, who shot himself in the head at the age of 27.
“The best doctors money could buy, the best medications, the best therapists, and the best people praying…”
^ I submit to you that very few people could have survived that.
https://www.youtube.com/watch?v=vG-IK2kXCQI
https://www.youtube.com/watch?v=7vzASWdMX5g
Joshua
Report comment
As usual, Robert Whittaker, your article is super-excellent! A class-action lawsuit sounds great, but. how do you get enough support so as to prevent all from being “cancelled” as it were in the lexicon of today. Just as I was reading this article, another news report came across the tv about how people should take care of their mental health and it seems the new ploy might be how if you don’t it affects others (i.e. those you love.) Psychiatry has grown so big and has so many friends in the media and I would say Congress, etc. too especially after the Pandemic and these increasing mass shootings, etc. this to me seems like climbing Mt Everest and I’m usually the optimist, not necessarily a realist. But still something must be done and since I trust you, Robert Whitaker and additionally, your book, “Anatomy of an Epidemic” in addition to another strange book that fell into my lap at the right time saved my life. So, please, give us all more information. I always have hope, but I do like it when the hope begins to fly. Thank you.
Report comment
Today, a pro-mental health article, “schizophrenia”.
https://www.sacbee.com/opinion/article263602568.html
Yeah this article is sad and their are problems in our system. But they are using this to promote care courts and that is not the answer.
This writer they say covers local stuff, but that probably means that she serves the real estate industry, and they are the ones who most want to intern the unhoused.
They can still do a lot more for the disabled, but not require any mental health treatment at all.
Also this quy starts fires. Should he even be out of prison?
Joshua
Report comment
I notice that after the whole exposition of how the ideology that depression comes from a lack of serotonin is exposed as not panning out, we finally get that if that were true that anti-depressants aren’t doing that. After a few weeks the brain starts to adjust, because there’s so much serotonin left over in the synapse, and the brain stops producing as much serotonin, so there’s actually less serotonin. The whole marketing blip is not even true.
(!?)
There’s also the fact that the clinical trials not only had HAD to use people that already were on psychiatric drugs to get the results they wanted and/or give them a sedative because of the akithesia effect, but had taken out people in the non control group that got better the first few weeks (they supposedly then weren’t depressed, but someone who is used to having their natural brain chemistry compromised or likes a disabled mind from anti-depressants they then are left in the trial); there’s also the fact that in some of the trials more than half the people in the control group had to leave because of side effects (this of course wasn’t counted), neither were the amount of severe withdrawal symptoms initially reported of people in the control group who didn’t get a “therapeutic” result, and had to get off of the anti-depressant: these withdrawal symptoms which could be inability to stay awake, or sleep, fevers, seizure, akithesia, a whole list of others that would take pages weren’t reported, in fact left out till further looked into; and then the long term effect where people who felt they had a “therapeutic” result couldn’t get off of the antidepressants without again severe side effects. Added to that, they knew that there were people that got homicidal or suicidal, in fact in the trials there were suicides; but not only did they aggressively cover this up, but when this was ongoing after anti-depressants were FDA approved they simply didn’t report it, and then after getting an international collective of people addicted to anti-depressants, they tried to prevent the warning label that’s current. Still one can add up how much addiction to these highly addictive “medications” played a role as to whether they were still being taken. And then we get the amount of collusion between the extreme rise in mass shootings and anti-depressants or other psychiatric drugs. That’s then used as a call to force more people on drugs, same as withdrawal symptoms, same as side effects used to get people on a cocktails of drugs. And then we have all the marketing, people just wanting to believe that they can pop a pill and fix their life; and the whole change in conception of depression, leading to paranoia against something as scary as that it’s associated with faulty brain chemistry. Something that used to go away, although uncomfortable was made out to be so scary, with added ideology as treatment, this then could be exploited, harnessed to gain a whole populace of consumers of anti-depressants and other “medications,” when in reality the medications cause disruption of natural brain functions (chemical imbalance) the disease hasn’t been proven to cause, and the drug companies more than a decade ago stopped looking for this “illusive” proof that their medications treat chemical imbalance.
THIS is what a person comes up against wanting to find answers to mental health, and those stuck in the system can’t voice the truth or possibly be found non-compliant. How many people have been “forced” on these treatments and possibly wouldn’t even be able to dare to entertain the truth, consequently? How many people actually interested in mental health, wanting to help others, got so full of ideology and propaganda that their FIRST response is to get frustrated and blame those not following “treatment” as it jars with the programming they’ve been inundated with akin to the pastel colors, butterflies and angel wings that go with such marketing? How many people have not been able to share the truth as clinicians or psychiatrists? How many people who truly could have helped others chose another job when they got gist of what’s going on? How many people have died or had their lives severely disabled because of all of this? How many people have become the brunt of superstition, gossip, demonizing and bullying because of this ideology that they are dangerous and there’s something wrong with their brain?
And it’s effected more than just “mental health” in all areas of life, anyone expressing dissent can become labeled, or be terrified of going outside of the box. Anyone acting a bit weird can suddenly be made out to be some imminent danger and assaulted with “treatments” that in reality are in collusion with the rise in violence, all because of this chemical imbalance ideology that is treated with “medications” that are proven to cause chemical imbalance in contrast to the “disease” that’s alleged to.
I’ve actually had it myself that when being honest enough about thought itself, that other people and namely a “social worker” didn’t have the ability to understand, and having delved into necessary symbolic dreamlike-spiritual areas, even knowing the next day that it was symbolic rather than “actual” (which I’m saying because symbolism can be more objective than physical reality because it involves your reflexes, your thoughts, which determine the future, and HAS TO remain intangible to the physical) but fine it wasn’t “actual” although the next day when I realized that I already was made out to be a dangerous psychotic that could become violent, for nothing more than the EXTREME paranoia of the social worker. I was lucky that I wasn’t directly involved with this brainwashed individual, so I wasn’t institutionalized; but in the working out of the symbolism and the theme regarding life that it animated (the initial idea of what I was trying to express that became symbolic: the symbolism I believed in for one day that was made out to be dangerous psychosis) although in the end the very theme that needed the symbolism it lead to what metaphysically would be called a miracle (I have the x-rays to prove it), as well as spiritual connections with people from beyond time (that I hadn’t even met yet at that moment when I was made out to be crazy, and where the very meaning of how life brings together such interactions wouldn’t have become conscious) where such themes basically give meaning to life (does life have meaning that there’s themes like in “fiction” and who we encounter in life are the working out of those themes?) and to understand it you really have to go beyond the boundaries put on what’s sane and what isn’t. And emotions that aren’t compliant with society’s limitations, or even the dream you had of fitting into that, they when allowed to beyond the discomfort give you wings rather than inhibit your life. And seriously, what lead to a miracle was made out to be dangerously psychotic. Fortunately, it got this social worker out of my life who was so off, and like a synthetic intelligence program who spun some delusional handle on anything as if there was some other devious meaning to it, spiced this up with lies to such a degree that it makes me wonder WHAT she was on.
She could have ruined my whole life had she control over it, and I was the one that was supposed to be dangerously psychotic!?
Instead I have a deeper understanding of life, where miracles are allowed.
And don’t do this! Don’t sit and groan about something that makes you think it gets in the way of your ability to function, when in reality, would you look at it clearly it’s nothing but sane compared to the straight jacket of limitations you’re supposed to believe is what you need to find your way: your way in what? WHAT subset of fabricated beliefs are you supposed to be imprisoned in, where everyone is holding onto them to such a degree that their lack of logic needs you to feel there’s some loss when you find you’re not inhibiting yourself in such a fashion to take part in this @#$_(#$()#$%*#$%(#$)%(). EVEN when you don’t know why you did that. It’s OK. It’ll make sense in the end.
Report comment
Another excellent article and summary. Another result of using SSRIs has been the massive increase in bipolar diagnoses. Maybe this is for another day.
Report comment
I have very little respect for the bipolar diagnosis these days.
Do you know that Harvard University tried to get me fraudulently diagnosed bipolar? All so they could invent a pretext for refusing to investigate my claims of misconduct against the then organist at Harvard and some of his students?
See, I had this talent at the pipe organ that made it so many teachers said I was probably one of the best in my generation at it. Meaning I was better than all the other organists at Harvard, even though I was a student. And not just a little bit better. A lot better. There was no comparison.
Guess what other organists did? It was just one problem after the other after the other. I was forced to quit a job playing the organ at Harvard due to intolerable working conditions. But then, other students started doing things like rope me into agreeing to give performances, and then not tell me the right pieces I’m supposed to practice or play until the very last minute. One told me “I only want you to accompany these four pieces” at first, only to then tell me, less than a week before the performance, “actually, I need you to accompany ALL 21 pieces of this work.”
It was just one thing after the other after the other like that. I had low self esteem due to not having the most supportive family, so actually what happened was that the things I tolerated for very long without formally complaining were actually quite outrageous. Most other people would have complained long ago and I didn’t because I had such low self esteem. However, eventually the antics of the organ world at Harvard got so outrageous and over the top that I finally do officially complain.
Harvard literally corruptly arranged for their doctors, who had previously insisted I was not bipolar, to suddenly insist I was bipolar. And my official complaint against the organ world at Harvard was the proof of my insanity, they said. And that meant they were not obliged to even investigate my claims in the first place.
Of course, they knew that such an investigation would show up very serious wrong doing detrimental to Harvard’s reputation. Not only that, but I’m gay and Harvard arranged for a large portion of the gay community to harass me and ostracize me on behalf of Harvard, so that years later, I’d still have gays come up to me who shouldn’t have known me from Atom and accuse me of being “crazy” in a manner that was obviously linked to my experiences at Harvard.
Or, in some cases, they would harass me in subtle ways which were sneaky but just a repeated pattern of sneaky nasty behavior engaged in over and over and over again. Until I’d eventually get fed up and confront them on it. And they’d suddenly accuse me of having a mental health problem the moment I did. It was as if Harvard was a kind of mafia.
I started documenting much of the behavior, and have an enormous amount of computer files on it. However, in one instance, a somewhat indiscreet gay man ended up kind of summarizing, very accurately, the systematic abusive behavior from the gay community, which can be traced back to my problems with Harvard. But, already, you can see here the abuse and corruption of the mental health system in all of this.
It also became true that, when it eventually came to rape, cops refused to help me, and they made reference to this same “mental health excuse” that everyone else started making in conjunction with abuse of me, ever since Harvard got their docs to suddenly impose a bipolar diagnosis on me for asking for an investigation into the misconduct of other organists.
Also, if you see this series of emails I post, from one “JPBoy” — notice how he says “hundreds of guys know about you” and I correct him and say that I think it is 1000’s. I was right.
https://pbase.com/damian1974/jpboy_about_justin_who_was_then_age_23_but
I eventually hire a lawyer to deal with these matters, and was almost murdered with rat poison, which was an incident staged by NYC cops, and if I’d died of it, they were planning to do faked forensics in a manner similar to what happened in the Matthew Shepard “hate crimes” case where a fake narrative was imposed to cover up the antics of the gay crystal meth scene, and everyone pretended the perpetrators were straight. In my case, after the rat poison gets into my system, someone comes into my hotel room, breaks my laptop in half and trashes it. But police were going to pretend I’d done all that myself in some kind of psychotic rage.
And they probably were going to arrange for me to maybe fall off a balcony and hit my head or something – this as a way to cover up what was a whole series of brutal crimes carried out by gay men with the blessing of the police and mental health system. Or, rather, which police and the mental health system had COLLUDED with.
The perpetrators wanted to be able to somehow portray me as a difficult person who flies off the handle and goes into all sorts of psychotic rages, all so that the hordes of gay perpetrators could all go lie and say they had a difficult time with me, I was so difficult, etc.. People at Harvard could have then gone and explained that, all the problems I had had there was because I was that difficult too.
Well, it all didn’t work because, as a result of some kind of fluke, I got only a tiny portion of the rat poison/warfarin dose that was intended. So after the person who trashes my hotel room leaves, I escape in my jacket and underwear … The hotel clerk at the front desk refuses to call the police on my behalf so I have to run to another business to call the police. They instantly take me to the hospital and they all knew it was warfarin and they treated me for warfarin overdose without having to ask me a single question about any kind of symptoms.
Basically the same “system” that had colluded to try to murder me had to then go and save my life after I was seen escaping the hotel room in the middle of January in my underwear. Because if they had let me die of warfarin poisoning, there is no way they could have faked it so as to make it look like anything but a murder. Too many witnesses saw me running outside. And they could not cajol me back into my hotel room, only to have me fall off a balcony or something. It would be like, if I’m running out of the hotel in my underwear, if it isn’t a crime, at the very least I need medical attention. Well, they can’t have me dying in the hospital, you know. That’s not according to plan. So they had to save my life instead.
What you have here, though, is the police and mental health system acting as a kind of criminal gang. However, no one can accuse the police and mental health system of doing that. The very accusation would be used as “proof” the person making the accusation suffers from schizophrenia. It’s a really bad problem. But, see, after experiencing THAT from the system, I really do not have much respect at all for current diagnostic categories like bipolar.
Report comment
Thank you Robert Whitaker. Such is the intensity of injury, morbidity and mortality imposed on both those suffering extreme emotional distress, and those who have no psychiatric condition whatsoever, but in whom inappropriate psychotropic drug prescribing has caused AKATHISIA which has been misdiagnosed as SMI (Serious Mental Illness).
“The court also set forth a standard whether this legal obligation had been met”:
“What would a reasonable patient want to know with respect to the proposed therapy and the dangers that may be inherently or potentially involved?”
With regard to SSRIs/SNRIs ‘antidepressants, I would require to be advised that AKATHISIA is a common adverse drug reaction. I should be warned that this is not simply ‘restlessness’ but that my family MUST look out for crescendo AGITATION, for a writhing tormented inability to be still because of intolerable pain and suffering. That this suffering may be so unbearable that I might tear out my hair, eye lashes and body hair whilst being unable to try to convey to them what is happening to me. I have to be warned that my family MUST insist that any doctor addressing this iatrogenic emergency MUST be told that THIS IS AKATHISIA. In my experience, they may not/will not know what it is. I am then vulnerable to a ‘diagnostic’ label for life such as ‘psychotic depression’ resulting in detention (Medical Kidnapping) and forcibly given further psychotropic drugs leading to cascade iatrogenesis and a catalogue of fantasy psychiatric diagnoses. I should be warned that if my (medical) family tries to challenge this tragedy, they will be ridiculed and treated with contempt; That I will become so injured by their drugging that the person I once was will never be seen again.
I would like to be told that at best, SSRIs/SNRIs are very weak ‘antidepressants’, but extremely powerful and effective anti-libidinous drugs, causing a specific (non-depression) form of sexual dysfunction: PSSD which may last for years, perhaps for life.
There will not be much time left now for the prescriber to explain that psychotropic drugs have been reported to cause mitochondrial toxicity, metabolic syndrome, diabetes, hyper-prolactinaemia (hence gynaecomastia) and other endocrine pathology.
Both my family and I MUST be warned that these drugs cause changes in emotions, feelings and behaviours including emotional blunting, disinhibition, suicidal ideation and risk of violence to self and/or others.
How could I give valid informed consent without this information? If I were to be given enough information upon which to base a decision equating to real, valid informed consent, my response would be: thank you for your honesty Doctor. I have no wish to take any such medication.
This further post rekindles hope that something may be achieved to reduce the tragedy of psychotropic drug ADRs. Thank you for your courage and for your lifetime commitment to this cause.
Report comment
So well said! I agree one hundred percent.
I would add that these drugs should no longer be prescribed to children. No one who is under the age of consent should be given psychiatric drugs as children are incapable, due to not being of age, of giving informed consent. Just like they’re not able to drive, or vote, or consent to sexual activity. And since the child is the one being made to ingest the drugs, I don’t think that a parent/guardian should be qualified to provide informed consent on the child’s behalf. Maybe if the parent wants to take the drug first for a long period of time, then they will have a real understanding of what that drug does, and then they will be qualified to provide informed consent on behalf of their child. I would say the period should be at least a year of being on the drug in question.
Report comment
I agree. I am very grateful to Robert Whitaker’ for his moral courage, personal integrity and for using his journalistic brio to report on what does not get a hearing in the mainstream media.
I’m from another jurisdiction. A class action is a lovely idea. I doubt it will happen. As another poster said it would take an army of public interest lawyers and and a lawyer’s main and in fairness legitimate concern is how and when are they going to be paid. Who is going to fund it? Most psychiatric patients live at subsistence level.
The American Psychiatric Association and the pharma companies that would presumably be jointly sued will have access to the best lawyers that the pharma companies can buy. They will have access to legal firms who have armies of junior, trainee and support staff that can spend months compiling the necessary research with which to shut down the plaintiffs even before the matter gets to court. It would take an enormous amount of resources to advertise for potential plaintiffs and take the necessary depositions and there is the unfortunate fact that psychiatric patients will struggle to present as credible witnesses due to having been diagnosed with a psychiatric illness and therefore lacking capacity.
I see that there have been lawsuits taken against the pharma companies and that the courageous lawyer Jim Gottstein risked criminal contempt of court charges to leak damaging information about how Eli Lilly was illegally marketing the drug to the elderly and children. But at the end of the day Eli Lilly settled the case and was allowed to plead guilty to a misdemeanor for its illegal and dangerous marketing of Zyprexa to dementia sufferers. The US court system seems to allow pharma companies to settle by paying negligible fines and in the Zyprexa case they were allowed not to acknowledge any civil wrongdoing.
In the US I understand there are non profit public interest organisations that conduct impact oriented litigation such as Jim Gottstein’s Law Project for Psychiatric Rights (whose web page says that it is currently inactive pending funding), the American Civil Liberties Union, The Lawyers’ Committee for Civil Rights Under Law and Lambda Legal Defense and Education Fund. I understand there is an Office of Consumer Litigation who was a party to the Zyprexa case.
There is an Consumer Protection Branch aligned to the Department of Justice that would presumably be the body to take a case on. Is it likely that the Consumer Protection Branch would agree to take on a class action against the pharma companies for misleading advertising given that the court system in the States seem to side so often with the corporate world. Would any of the other bodies have the teeth, money or even the belief to go up against the pharma companies and the American Psychiatric Association in a lawsuit?
The US now has a Supreme Court that is predominantly made up of ultra right wing judges that side with industry. As recently as June 2022 the State Supreme Court of Washington sided with Eli Lilly in refusing to recognise an exception to the learned intermediary doctrine in direct to consumer advertising. I note also that the US courts have dismissed several applications for class certifications against Eli Lilly for injuries sustained by Cymbalta starting in 2014 with the last dismissal in 2017. In fact as far as I could ascertain from the attached link from drugwatch, every single claim for injuries sustained against that drug by individual plaintiffs have been thrown out by the US courts (https://www.drugwatch.com/cymbalta/lawsuits/). That does not give one confidence that a class certification would either be allowed or would be successful in the courts.
I note that Robert Lustig in his book ‘The Hacking of the American Mind’ writes that the US court system tied itself to corporate interests with the election to the US Supreme Court of Lewis F Powell a lawyer who acted previously for tobacco companies. Between 1976 to 1980 in a series of cases in which Powell seems to have written the majority judgment, corporations were allowed unrestricted lobbying rights (Buckley v Valeo – 1976), unfettered corporate advertising (State Pharmacy Board v Citizens Consumer Councill 1976) and allowed to say whatever they wanted publicly without being held liable (Central Hudson Gas and Electric Corp v Public Service Commission 1980).
Even if class certification was allowed and made it to the courts, would it get a fair hearing in the American judicial system as it is currently constituted?
Report comment
Thank you for this information! It is indeed sobering. I was somewhat aware of all of the Cymbalta lawsuits being repeatedly dismissed…which says a lot. I’ve probably been on and off 35 or 40 different psych drugs, and Cymbalta is in a class of its own in terms of the suffering it can cause.
I think in some ways what Psychiatry has done is the perfect crime. There is no way for someone who has already been deemed a mental patient, as you point out, to prove or even convince a majority of people from the general public, that their suffering and symptoms were caused by the drugs they were prescribed (without being given informed consent) and not their “inherent mental illness.”
Report comment
Hi KateL
Yes I was on Cymbalta too for four years until I was told to get off it more or less immediately as my liver enzymes and cholesterol were dangerously raised. I am off it a few years now but the withdrawal period was dreadful.
One can only live in hope that eventually the truth will come out – it did about barbiturates and benzo’s.
Report comment
There are no “psychiatric rights.” If you are being psychiatrized your humanity is being violated and those who pretend that “rights” can be obtained via legalities are being misleading, and are perpetuating psychiatry’s false raison d’etre.
Report comment
YinYangn
So true. My state’s mental illness disability rights handbook is 50 pages of meaningless fluff that allows legislators to brag & pat themselves on the back for “allowing” people with psych diagnoses to have “equal” rights. It’s a sham. I don’t have equal rights. The few rights I do have can be over-ruled on a psychiatrist’s whim.
Report comment
I have been gobsmacked by the ability to deny victims of crimes the right to legal representation.
Consider that the Community Nurse who made me into an “Outpatient” before calling Police to have them force me into a forgone conclusion interrogation (a ‘verballed’ confession) was clearly committing an offence.
The hospital becomes aware of the long list of offending that followed and they then have Police retrieve the documents proving those offences (and human rights abuses including acts of torture), and the legal representation I did have is removed to make things a little more difficult for me.
The “edited” documents now show the narrative that the hospital wants to be true, and everybody goes about their business.
I mean I get it if this was what our politicians were complaining about in North Korea (see Otto Warmbier) but to find out that it is being done in your own back yard AND that the ‘legal representatives’ who are supposed to be a protections against these abuses’ are nothing more than SHILLS?
Turning up with the proof that police failed to retrieve only makes matters worse in the end, because the long list of people who have been negligent after contacting the SHILLS now have something to worry about. They might get marched past the piles of corpses left behind in the wake of their negligence.
Not that they ever seem to think they will be held to account. How could they when witnesses are threatened and the hypocrites who claim to be ‘defenders of our rights’ turn and run at the first sign of trouble?
Don’t look, then what you don’t know can’t hurt you. And if you do look, you can always turn your back on the ‘Jew’ because no one else is actually going to help them anyway right? Not when the police tell you to say “It never happened”
So whilst I admire the legal system and the right to representation in other places, the States where I live have the ability to rewrite the laws which appear to provide protections (without Parliamentary approval. And i’m sure there are doubters about this, who maintain their doubt rather than examine the documents) , to ensure that any criminal or human right abuse’s “never happened”.
I was glad to read that the situation is very similar to the time spent by Frantz Fanon (the Wretched of the Earth) in Algeria where the very same mechanisms allowed the systematic torture and murder of ‘activists’. Psychiatrists boasting of their method of working with ‘legal representatives’ to “overcome resistance” (ie breach the trust people place in them. Defense lawyers working as paid police informants? Both sides of the bread being buttered in Australia )
It may go some way to explaining why our hospital system has been rapidly degrading to providing third world ‘care’. Reports commissioned to find out who needs threatening, and what documents to “edit” rather than holding those responsible to account. Unaccountability tends to attract a certain type of person, who can see the benefits of such an environment. The possibilities for emptying wallets while police provide assistance holding the victims down and ensuring nowhere to go to complain? Yeah, I can see how that might work.
Unfortunate that even if we had RICO laws, they could be rewritten by the Commissioner to ensure that no action could be taken. Our politicians completely redundant these days, providing the smoke and mirrors for criminals, as even the flimsy legal protections the community IS provided in our laws, don’t count when you try and access them.
Report comment
I’d like to point out that, in my opinion, the social role of control over the delivery of psychotropic drugs is assumed by the physicists but it is not a therapeutic role in the strictest sense of addressing the cause of an underlying diagnosed biological process. This delivery control mission could be assumed as well by pharmacists. I think this basic confusion feeds the charlatanism in psychiatry, and also the very wrong ideology of medicine as competent and sufficient in everything human, aka the religion of medicine.
Report comment
We have all known for years that the basic reasoning behind psychiatric drugging is fraudulent and that these drugs are given for “illnesses” that do not exist. MIA was founded upon this understanding, yet years later people keep beating this dead horse as THE problem when THE problem is the existence of psychiatry, period.
Report comment
I agree with yinyang without any reservation.
Joshua
Report comment
But, how DO we get started on all this? What are the next steps? Someone reach out to me if we can start getting the ball rolling. I think things like this are a strike while the iron is hot kind of thing, and frankly I’m pretty pragmatic but I’d love to see a takedown. These people need to be stopped.
Report comment
The anti-psychiatry movement is currently moribund because people are led to believe illusions such as that lawsuits can stop psychiatry. This is catering to people’s naivete and is like thinking that lawsuits can stop capitalism (you might call it corporate greed). Only organized resistance — not for those who like to feel comfy — can effectively confront a neutralize psychiatric oppression.
Report comment
What would that organized resistance look like?
Report comment
“What would that organized resistance look like?”
I know what it won’t look like. Like one of the advertisments for their drugs lol
Mind you, this age of ignorance we seem to be going through, where the public is being increasingly stripped of resources by those who have usurped the power of the vote, and where our elected representatives are simply put in place by media moguls to do their bidding.
It’s simply not going to hold water for long. They’ve neglected the fire fighting equipment, and once a spark turns into a blaze, …… and they think the futures so bright, they gotta wear shades.
“God will remind us what we already know, that the human race is about to reap what it’s sown” The The. Armageddon Days are Here (Again)
Report comment
Organized Resistance, first refuse any cooperation with the Mental Health System of any type.
Try to put as many doctors and psychotherapists as possible out of business, and try to hold parents responsible when they are saying their child is “mentally ill” or on the “Autism Spectrum”.
Stop government money or licensing from supporting Mental Health or Psychotherapy.
Joshua
Report comment
That’s not something that can be answered in the abstract, it depends on the particular circumstances out of which the movement, or particular “wave” of the ongoing movement, arises. There has always been and continues to be an “underground” anti-psychiatry consciousness among psychiatric victims, and the most articulate and revolutionary voices of any given era have the collective moral and strategic responsibility to determine the nature of that era’s form of resistance. I know that’s pretty abstract in itself, but before pursuing any goal the goal needs to be thoroughly understood, as well as strategically and analytically sound. Otherwise you’re in danger of working against your own interests without even realizing it.
There’s nothing wrong with reformist tactics such as lawsuits as long as they are understood as such and not presented as something that will achieve “systemic” change, i.e. the abolition of psychiatry. No system will voluntarily overthrow itself, and if lawsuits could have that effect they would be outlawed. Currently the danger of winning a lawsuit or two would be that “victory” being used as a pretext for claiming, “see the system works, psychiatry can clean its own house,” and making people believe that they “won” and there’s no need to struggle AGAINST PSYCHIATRY anymore.
P.S. Remember that victims of psychiatry should put their sights not just on “resisting,” but on overcoming.
Report comment
It is not just resisting, it is being made whole, reparations. And from that there will be overcoming.
It is no accident that Mental Health has been fully embraced by the Evangelical Christian Movement. They are both based on this idea of Original Sin or Innate Moral Defect.
Freud was able to replace the religious view of fallenness because it did not accept sex. Freud said that we are all animals, so sex is okay.
But what Freud did not understand is that sex is merely a portion of a larger need, public honor. And public honor sometimes requires violent retribution.
So our society uses psychotherapy to keep people compliant by talking them out and talking them down.
Joshua
Report comment
Start here
https://www.presidency.ucsb.edu/documents/special-message-the-congress-recommending-health-program
Report comment
It is not only the Psychiatrists, it is also the parents and all other arms of government.
People will start to see the anti-psychiatry side when they see that they can vidicated by a jury and made whole again. Without law suits and civil judgements it is all just abstract principles.
And usually as long as people have access to the courts and the ballot box, they will not go outside the law. So the legal route has to be pushed as far as it can go.
Joshua
Report comment
There is something to this: my mood is not the business of my medical doctors.
My mood is not their wheelhouse. They can deal with bloods and heart & lungs & bowel & even brain – but my mood is none of their business.
Someone here said boycott is the start of power, here. I agree. But – when so many people are buying into the dominant narrative, we need PSA’s to educate, to counter the billions spent by pharma on their belief that “doctor can fix this.”
Report comment
“My mood is not their wheelhouse. They can deal with bloods and heart & lungs & bowel & even brain – but my mood is none of their business.”
You just made me a better person with that comment JanCarol. Thanks.
Boans wanders off practicing “my mood is none of their business, my mood is…….”
Report comment
What if the doctor helped you find a diet you enjoy that improved you mood? Or what if the doctor suggested some easy exercises so that nagging injury quit hurting? Of course you don’t want to talk about your mood to a psychiatrists that is only trained to prescibe and not to heal or prevent.
The sad truth is doctors don’t study the alternatives. That requires nutritionists, physical therapists, and other professions that treat the person and not just the symptoms.
Report comment
Hey LivingPast27, you kinda described a piece of the problem – and that’s the “specialisation.” My GP gets mad when my natural doctor (also an MD) finds something, GP throws a tanty and says, “Well let HIM manage that, then.”
This specialist for pain, that specialist for my throat, another specialist for my rectum, another specialist for endocrine, yet another for diet, and a physiotherapist or exercise physiologist to manage movement. . . . and on and on and on.
I’d love to have one practitioner that looked at me as a whole, instead of just a mouth, a rectum, a skin problem, or a digestive problem. . . .
And no. I don’t trust any of them with my mood. That’s my business, I have a toolkit for that which is superior to anything an MD or specialist could offer.
Report comment
Yeah, good luck with getting anti-psych PSAs on corporate media, which is controlled by Pharma. This is the sort of thing people always seem to buy into, i.e. that the system will assist in bringing itself down, but those in power have had their bases covered for a long time.
Report comment
“but those in power have had their bases covered for a long time.”
How true. The ability to “edit” legal narrative” to fit the desired outcome a major benefit to the State. The current Coronial Inquiry into the death of a child one example. S light change in the documentation, a few threats to the staff (“it never happened”) and there isn’t a chance that anyone would be held accountable.
And with the lie that their ‘treatments are effective’ and that ‘your chemicals have become imbalanced’, they can subject people to the most vile abuses, and then have them ‘referred’ for ‘treatment’ when they break down.
I’m sure the grief of the parents will no doubt justify electricity to their heads should they spot the “editing” during proceedings and ask their shills…… I mean lawyers to do something about it. Show the video again and make them leave the court for this bit.
When the cure for torture is torture, and they can’t see why there might be a problem, best they are left to their own ‘devices’.
And how easy is it for ‘them’ to simply ignore the facts and evidence? Simple, ‘flag’ the ‘problem’ as an “Outpatient” and give them the ‘treatment’.
And what worked best of all in my situation (and I’ve no doubt in many others) was to maintain the lie. DESPITE knowing it was a lie. Commonly called uttering, except when the outcome depends on the lie.
Spending the forged $100 note despite knowing it was a forgery? Using a forged statutory declaration produced via an act of torture and then writing “The reasons listed on the Form 1 are considered to be reasonable grounds”? Same offense (though the consequences are much more serious when the Chief Psychiatrist is doing it and people are being harmed as a direct result), but when you are above the law (and in fact actually rewriting it to remove the protections afforded the community with no need for Parliamentary approval), not a lot anyone can do about your gross criminal negligence right? The concealment of the other offences by the failure to do due diligence, and check the facts. See for example the way the failure to provide unedited documents to the Law Centre was dealt with in ‘his’ letter.
Which would explain the reasons no one wants anything done about the ‘pathway’ to the ‘unintended negative outcomes’ (a Euthanasia Act “with more than a 100 protections” Non eof which are effective once the documents are “edited” before an independent legal representative can examine them.).
Minus the ability to ‘outcome’ your mistakes, there would be a shift in power back to the people. And we can’t have the ‘Outpatients’ (that is anyone who isn’t an Inpatient) being protected by the law. Where would they be if they couldn’t ‘spike’ people and subject them to acts of torture, belt them over the head with the chemical kosh and electricity, empty their wallets and destroy their families, and then “edit” the documents and call it medicine?
People might start asking inconvenient questions and expecting answers. Such people need treatments and there needs to be ways to get them that treatment when they need it which is……. when they try and access the protection of the law from criminals and corrupt public officers.
The response to trying to make a complaint about torture from the State? “get treated’. Yeah, they have a lot of respect for the Conventions they ratified (including the Optional Protocols). There is no means to make a complaint, even when the attempt to “edit” the documents and remove the problem from existence has failed. “Who else has got the documents?”….. and knows the State is covering up arbitrary detentions and acts of torture with ‘outcomings’? Like the bird said “Ewwww That can’t look good”
The door to a complaint has been welded shut, and no one ever gets the opportunity despite the Articles of the Convention. You will be swallowed up by ‘mental health services’ and be like the children who were being raped by Priests……. silenced for 40 years to ensure the perpetrators “character flaws” aren’t seen as crimes.
And once the lie has been told that you are an “Outpatient” despite the facts showing otherwise, it simply becomes a matter of how to get you to ‘take your medicine’. Makes a nice little training exercise for some of the young uns.
Report comment
The deception and harm perpetuated by psychiatry has carried on far too long as business as usual. This thorough, compelling presentation by Robert Whitaker is much needed.
It’s clear after psychiatry labels someone “disordered” the person is no longer afforded any credibility or much respect. The dehumanization of the ‘labelled’ allows psychiatry to continue ignoring or dismissing the voice of the harmed. Those who died from adverse effects of psychiatric treatment as my brother did, are permanently silenced. Very thankful to Robert Whitaker and MIA for the dedicated, courageous and humanitarian work to try bring more awareness and justice.
Report comment
I’ve found that psychiatrists often get avoid directly using the chemical imbalance lie my simply saying the drugs are “safe and effective”. The research has proven over and over again that this is a lie as well. I think unless we are able to legally hold them accountable for these damaging, life ruining lies, they will continue to peddle them in any form they can get away with to keep patients “compliant”. After 20 years of suffering this kind of “treatment”, and watching so many of my friends in the SMI community suffer and die, I am disgusted, disheartened and furious that this is still accepted as being just the way things are, as if a status quo of extreme suffering and early death is acceptable.
Report comment
“I am disgusted, disheartened and furious that this is still accepted as being just the way things are, as if a status quo of extreme suffering and early death is acceptable.”
I think the turning point for me was the passing of a Euthanasia Act. There was something about the way it was done (after failing to have forced sterilizations of children without parental consent passed) and which appears to be a defense against what is about to occur.
Of course it is an ‘internal matter’ and like the Chinese, keep your noses out of our business. Only ‘we’ understand the problem, and ‘we’ can’t discuss it with the plebs because they wouldn’t agree to what needs to be done.
The bleeding liberals in the United Nations making the crimes of public officers the responsibility of the State? (and all the while allowing the sexual assaults’ of women to be covered up, and whistleblowers destroyed) There’s going to have to be a ‘wall’ between the people doing the ‘assisted dying’ and those turning a blind eye. We do of course have Himmler’s diaries as a ‘play book’, and the problem created by Josef Hartinger and the ‘assisted dyings’ at Dachau. How did they get around the same problem?
Must admit, I hope I’m never in a position to say “i told you so”. and if it wasn’t for a doctor without the stomach for it rudely interrupting my ‘outcoming’ (and then “editing” of the documents) I wouldn’t be around to not say “I told you so”…… if that makes sense lol
You get desensitized to it from what I’ve seen in the locked ward. Abu Ghraib being a good example of how quickly you can turn humans into animals with a little ‘role confusion’. Hence the chaotic and always a crisis situations which seem standard for mental institutions. They are deliberately designed to be that way, in a Gruen Effect kind of way. It sort of looks like a hospital, but there’s something about it which ……..
Report comment
You know what would be a really good idea to do?
Have a study done which lists the causes of death of those prescribed certain psych meds. Take, for instance, diabetes, but also take the added obesity rates and project deaths by heart disease or cancer or whatever.
As opposed to old age.
You might want to do this for some of the blockbuster atypical anti-psychotics like Zyprexa, known to cause lots of obesity and diabetes.
But here is where you want to get some really good mathematicians to calculate the increased revenues derived by the cancer industry, heart disease industry, and diabetes industry, all due to the prescriptions of anti-psychotics.
Let me ask, how much did zyprexa cost per year, when it first came out? Was it something like $10 a pill or $10 a day? So perhaps that comes out to $3650 a year? Profits realized only for 20 years per patient, and then price goes way down as a generic. That would be $73,000 for the original drug company, over the lifetime of that one patient.
Oh wow, look at this:
https://www.ajmc.com/view/ajmc_10marnicholswebx_e86to93
“The total mean direct medical care costs for patients with established cardiovascular disease (CVD) were $18,953 per patient per year. Cost estimates varied widely, however, depending on the presence or absence of other health conditions.”
Oh wow. That’s six times higher per year than the direct cost of prescribing a patient zyprexa for 20 years. But I suspect zyprexa would raise heart disease rates far more than even the corresponding rise in obesity, by itself would.
Let’s say 20 percent of zyprexa patients get heart disease — coronary artery disease, I mean — and they wouldn’t have gotten it but for taking zyprexa, then the Heart Disease Industry should be counted as having realized even more increased revenues than Eli Lilly did.
My mother outright told me that elite Wall Street investors will network with institutions like Harvard, studying the effects of newly released blockbuster drugs like zyprexa, specifically for the purpose of getting an “inside edge” to the market. E.g., if zyprexa is going to cause a huge increase in heart attacks, they figure it out long before anyone else does, working with institutions engaging in unethical involuntary human experimentation — often using identical twins for that purpose — and here is where they add insult to injury. If they learn that a drug like zyprexa is bad, will cause very serious long term health problems, and should be taken off the market, they usually will cover up that knowledge, so they can experiment with various insider trading schemes designed to exploit, for profit, this secret knowledge they have about a product, which they expect nobody else will become aware of for decades.
But think of the carnage. These crooks are knowingly condemning large sectors of the population to health problems they know will happen, so they can profit from it. I find that part terrible.
Report comment
These are some excellent calculations!
Report comment
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3973179/
This is an interesting comparison of the costs of Zyprexa compared to lithium by analyzing insurance claims. Zyprexa was wonderful drug to experience but just like other substances it is difficult to say the benefits outweigh the harms.
Diabetes and Parkinsons are just not worth the benefits.
Report comment
Sorry, I had to chuckle when you used the term “outweighs” in reference to Zyprexa! I think in this case the risks LITERALLY outweigh the benefits!
Not meaning to minimize the incredible harm done to folks by the massive weight loss and other health insults caused by these horrible “atypical” antipsychotics. There’s really nothing funny about it – it’s a systematic criminal act!
Report comment
Yes, well I think a common saying in the mental health industry now is, “what you said was crazy, and I am not going to dignify what you have to say with any kind of answer other than: take your medicine, take your medicine, take your medicine …. til you are as fat as a house.”
Report comment
Yes, dmscholm. Highlighting the costs of the drugs plus the burden on the healthcare system & economy due to severe health problems & disability is crucial.
Have you read The Zyprexa Papers by Jim Gottstein? The government decided to take a big cut of the victims’ lawsuit winnings when they realized how much they had to pay out for Zyprexa-related disability & health care costs. And, due to US entitlement policies, the victims had to spend their lawsuit winnings within a year so they wouldn’t lose their public assistance (food, housing, healthcare) because having money in the bank makes them ineligible for these.
Report comment
More redundancy masquerading as enlightened social justice.
The basic fraud of psychiatry is its claim to be a branch of medicine; drugs are merely fraud-within-a-fraud. The fraud of psychiatric neurotoxins/”medications” is that they exist period, and that psychiatric drugs are being prescribed for non-diseases.
The idea that there is anything “anti-psychiatry” contained in this article is seriously flawed as well. The function of such a lawsuit would be merely for psychiatric victims to squawk and complain about psychiatry in an effort to “improve” it, rather than organizing to abolish it.
Report comment
I should add that it’s a sign that the Left is dead (at least for now) when the person most responsible for disseminating anti-SSRI info these days is Tucker Carlson.
Report comment
Re: Above — check out
Tucker Carlson: You Are Not Supposed To Notice That Psychiatric Drugs Are Driving Young American Men Insane ?
https://www.realclearpolitics.com/video/2022/07/06/tucker_carlson_are_you_surprised_young_american_men_are_going_nuts.html
Report comment
‘Es got a point.
I’ve never heard of Tucker Carlson, and in fact thought it was a food additive but …. had a listen and he does make some very good points.
Particularly about the spend on advertising versus research and development.
The media is to democracy what the bludgeon is to the totalitarian State (Chomsky) huh? The laws are in place to use force should there ever be a crisis as a result of the drugs being cut off. In fact, people where I live are just coming to terms with how many of their rights have been removed by stealth…. see the loss of housing rights for example.
I guess the one question I have about it though is why is it a gender specific thing? Should we ban access to the drugs for males?
I can see an expansion of the ‘industry’ if they can come up with a drug for people withdrawing from the drugs that does the opposite of what they say it does. That is, makes the withdrawal symptoms worse rather than better. But i’d be getting some of the guns back first. Either that or take a sabbatical in one of the properties bought with the money form the drugs….. you know, the Bahamas or some such tax haven. Come back when the shooting is over sort of thing. And someone pleeeeeease make sure the Nuclear Power plants are secured before they head off on holidays.
I’ve been giving financial advice to the people at the Golf Club. Buy shares in guns and drugs. No need to get involved in Colombian cartels, you can do it on the stock exchange. Some guys get a license to do it, and some don’t. So you get people like Manuel Noriega trying to set up shop. Or the likes of Ariel Castro trying to get in on the psychiatric hostel business without a license.
Stay legal I say, and get your accountant to help out with the drug distribution and gun sales.
Seriously though, the guys got a point, and like the gun situation, it looks like it’ll end in tears.
Report comment
I must note that Chomsky essentially called for the un-VAXXed to be cast into the hinterlands away from “civilized” society to fend for themselves, he’s a disgrace to his own name, and has permanently stained his legacy. Talk about totalitarianism. Hypocrite codger.
Report comment
I like the quote from Chomsky, I have no idea what is in his heart. I still singalong to Michael Jackson on the radio, but have no idea if the allegations are true or not.
Hypocrisy IS the greatest luxury.
“The problem has never been our political logic
But the way we enact it
We can imagine a perfect society
But can’t maintain a decent relationship
The failure found in the luxury, not in the hardship”
Disposable Heroes of Hiphoprisy
Report comment
You’ll never agree with everything someone else believes. If your only beef with Chomsky is that he disagrees with you over Covid vaccination, that’s a weak reason to disavow him entirely.
Report comment
Re: Chomsky — It’s as if Mother Teresa at the end of her life called for branding children with the sign of the cross — that would stain HER legacy no matter what, right? Same here.
Report comment
I definitely noticed that. The left leaning media, if they even report on the latest news of psychiatry fraud, find ways to dismiss it or mock it (and they always have to include bs remarks in their “reportage” like “of course psychiatric medications have been life-saving for many…” as if that’s something that’s just agreed upon). I used to consider myself a liberal but no more. I don’t care about causes trumpeted by people who don’t care about me or my basic rights. The left does not care about mental patients. They believe in human rights for everyone, except those who’ve been diagnosed as mentally ill.
Report comment
It is always a requirement to say “We know psychiatric medications can be life-saving for some” or something of that nature. Otherwise, your comments are instantly dismissed.
Report comment
I don’t think the media is a matter of left or right as much as it is the advertisers threatening to pull their advertisements from legitimate sources of information. Is Tucker Carlson really considered are reliable source? He may be right on this one but people are able to brush it off as another part of the cult.
Report comment
You got it right. This is NOT a left/right issue, it’s an issue of economic power and investment. Neither party will sign off on something that their contributors will freak out about because it loses them big, big bucks! Carlson is willing to put this on because he is famous for spitting in the face of anyone he wants to, and he’s tolerated because his comments are considered so biased as to not be believable. Mainstream media will not cover this kind of thing or will minimize or spin it somehow, because they depend on the same contributors who own our representatives.
We need to ditch the left-right axis. We need to replace it with the greed – integrity axis. People on the greed end of the axis should not be supported by anyone, regardless of party. Unfortunately, that doesn’t leave a whole lot of representatives left on the integrity end!
Report comment
“We need to ditch the left-right axis. We need to replace it with the greed – integrity axis. People on the greed end of the axis should not be supported by anyone, regardless of party. Unfortunately, that doesn’t leave a whole lot of representatives left on the integrity end!”
This reminded me of a picture I saw once of a ‘panhandler’ sitting with a sign saying “Why lie, it’s for Beer”. Now THAT’s integrity lol
Report comment
Gotta love it! Maybe he should start a new political party, the “It’s For the Beer” party? Probably get a lot of followers!
Report comment
It actually IS a left-right issue, except all the “leftists” are right wing too.
Report comment
An interesting way to put it! Can’t say I can argue with you. We have center-right and right-right and crazy-right in this country for the most part. What would be a soft left-center in Germany is considered a wide-eyed radical in the USA!
Report comment
Got to say at least the Americans had the nutz to tell the Brits to go fuk themselves, unlike the ‘colonies’ such as Australia.
I like the idea that ‘our’ government is jumping in on the baiting of China. And lets see where it goes when they get ‘left’ in the lurch. Might just find they are no longer “economically viable” lol
Report comment
I posted the Tucker Carlson link to my page at Surviving Antidepressants, and got messages telling me I had done a bad thing, that Tucker Carlson is SO HATED by 50% of Americans, that even if the message was good, I shouldn’t have posted it. I did a bad thing – our society is so striated and divided, that people can’t even hear as message if it comes from the “wrong” side. Hmph.
Report comment
Tucker Carlson is a smug, middle-brow halfwit who occasionally says something that’s not incredibly stupid. There are always other, better sources than Tucker Carlson. I mean, c’mon. Seriously.
Report comment
I’ll stop listening to Tucker Carlson when someone else takes up the baton and discusses these evil drugs. Right now, he’s the only MSM talking about it.
Report comment
COMMENTING AS MODERATOR:
Tucker Carlson and/or Fox News are not the topics of this conversation. Everyone’s had their say, now let’s get back on topic.
Report comment
And except for those who refuse the (totally failed) COVID “vaccine.” (Unfortunately there are still some victims of psychiatry who think there’s a difference depending on which drug you are being forcibly injected with. Psychiatrists are wrong, Fauci is a hero. Puke.
Hail Pharma!
Report comment
The so called mRNA COVID vaccine was a total failure. We must get it off the market.
Joshua
Report comment
And the issue of “side” effects is only beginning to emerge.
Report comment
“The so called mRNA COVID vaccine was a total failure.”
Huh! Where is the science to back up this statement?
Yes, vaccinated people can be infected with Covid, but the vaccines have literally saved MILLIONS of lives across the planet.
There is clear evidence that vaccines (and certain drugs) prevent serious Covid disease, reduce hospitalization, and YES, reduce the overall number of deaths by a significant factor.
And this success of the vaccines has NOT been offset by any significant amount of serious side effects.
Richard
Report comment
POSTING AS MODERATOR:
Let’s recall that this thread is on “psychiatry, fraud that the case for a class action lawsuit.” I am not allowing further discussion of COVID on this thread, as it is far off topic. We all know it is controversial, and both sides have now been stated, so I’m calling a stop to further back and forth on this, because experience says that this will be unproductive and will escalate to hostility.
Thanks to both of you for your viewpoints.
Steve
Report comment
The relevance was the analogy of so-called leftists opposing the right to refuse “vaccination” to “leftists” who turn a blind eye to psychiatric oppression.
Report comment
JanCarol, funny you should mention this now. Meghan Murphy just posted a similar refrain on her blog yesterday. Different topic, of course, but did you know that 39% of Tucker Carlson’s audience are Democrats? It’s worth a read. She makes your point perfectly.
https://meghanmurphy.substack.com/p/if-feminists-want-to-be-heard-they
Report comment
The “left-leaning media” has been bought out by the psychiatry/big-pharma people. Just see the ads on their tv shows and hear them speak of how psychiatry or whatever saved their lives or someone they know and there is no shame speaking to a therapist. Blah… Blah… Blah… Just so you know, the left, the progressives, the socialists or whatever are no friends to anyone who feels that psychiatry has harmed them. Thank you.
Report comment
As I’ve said many times, the “right” isn’t friends to anyone who feels psychiatry has harmed them, either. They get money from the same pharmaceutical and insurance industries, who are happy to paper both sides of the aisle with warbucks. Looking to the current political parties to support this movement will lead to nothing much worth discussing. They will both be dragged kicking and screaming to any real resolution, because it will mean tweaking the noses of people who have lots of money and power and make big campaign contributions!
Report comment
Steve is correct.
Report comment
Well, the way it works, while the right is beholden to large corporate interests like Big Pharma, bad psychiatry which disables and marginalizes and creates permanent dependency on drugs as well as permanent dependency on welfare services such as public housing or group homes, all of that creates steady professional jobs not just for psychiatrists but for those professionals who run all of the “affordable housing projects” those disabled people live in.
These are all political patronage jobs handed out by the Democratic Party. And, the way the machine all works, it’s absolutely important that the number of political patronage jobs stays steady and doesn’t shrink. Their system is completely incompatible with any kind of mental health system that actually has people get better.
Let me just say, I know something about the paranoia the system has regarding the potential shrinking of political patronage jobs in such areas as affordable housing. They are obsessed.
Similarly, nobody talks about this but, while Republicans might have the tough on crime rhetoric, Mass Incarceration creates HUGE numbers of political patronage jobs for the Democratic Party.
Although I do believe prisons also creates political patronage jobs for the Republican Party as well. Whereas the mental health system is far more imbalanced in terms of creating political patronage jobs for the Democrats only.
However, our system of mass incarceration along with the mental health system for the poor, both kind of go together and ally with one another. How many prisoners get put on those debilitating psychiatric drugs?
Left wing opponents of Mass Incarceration go on and on and on about how “so many prisoners are mentally ill, we are incarcerating the mentally ill, that’s terrible.” However, I think prisons are pushing drugs on prisoners solely on behalf of the drug companies and not always appropriately.
However, prisons are cheap and house prisoners efficiently. Left wing liberals want those prisoners to be taken out of prison, be declared mentally ill, and then housed in affordable housing projects with mental health services, all of which is probably two to three times more expensive PER PERSON, but that would create how many more political patronage jobs for the left, for them to do that?
Thus, even the opposition to Mass Incarceration is a little bit too wedded to the greed of the whole — well, there is this whole academic corporate complex and the “college degree leads to a high paying job” guild.
Colleges, in order to justify their tuition, need to ensure they can place all of their graduates in decent paying jobs.
Bloating the mental health system is a way to do that. And prisons, by the way, are not such decent jobs. Thus, the political patronage jobs of the prison system do not go to the same crowd of people as political patronage jobs in the mental health system.
Blue collar and lower class people probably without college degrees work in prisons. White collar and more upper middle class people work in the mental health system.
It may be the case that “the system” prefers to house people who are difficult in prisons, and people who are easier to manage in the “mental health system.”
One thing I am aware of, from living in Cambridge, MA and knowing about the politics of the affordable housing lobby is that “affordable housing” in liberal cities is designed primarily to create political patronage jobs for liberal professionals. And these liberal professionals are not the nicest landlords either. They do not treat the tenants very well at all. And they have a sense of entitlement and do not want to deal with anyone who is “difficult.”
Thus, the most needy people are excluded from affordable housing, because they would be regarded as “too difficult.” I remember hearing two decades ago that, in Cambridge, MA, the ideal “affordable housing” inmate was often something like a white woman from a wealthy family who has perfect credit (perfect credit absolutely essential and non-negotiable for tenants of these affordable housing projects) who has decided to quit her job and pursue her calling as an artist.
But, the thing is, affordable housing projects are part of the “nice jobs” program former students are promised after their parents paid an arm and a leg on college tuition. With that kind of money being paid in tuition, it is a requirement that these professionals be coddled afterwards. Part of that is ensuring they never have to deal with mentally ill or other “needy people” who might be regarded as “difficult.”
So I do think you might have some sort of “cross-over” where the prisons often are used to house the mentally ill who are “difficult” and who the spoiled rich kids employed in the “mental health system” don’t want to have to bother with. And since their parents paid that much in college tuition, they are entitled to get their money’s worth for what they paid for in their college degrees.
Report comment
After the past two years are you saying the “left” does NOT embrace Pharma?
Report comment
“The left does not care about mental patients. They believe in human rights for everyone, except those who’ve been diagnosed as mentally ill.”
Which is everyone who doesn’t think the way they do. My ‘Union’ quite prepared to support the use of ‘mental health services’ as a means to attack any whistleblowers, and run back to their ‘slavemasters’ with information for a pat on the head and a few ‘hush puppies’. Sychophants.
Report comment
Yin Yang,
Sorry to break it to you but Mother Teresa was a con woman who has long been exposed for being gleeful over children suffering and dying in her care homes in India. She was exposed first by Christopher Hitchens and later by Hemley Gonzalez and his organization Responsible Charity. Her mission was investigated for child trafficking and whole documentaries have been produced on it.
Chomsky is an actual saint in comparison.
Report comment
Not contesting the Mother Teresa stuff, but I think you get my general idea.
Report comment
I think it’s important to elucidate how many people have become collateral damage for the few who have supposedly been “saved” by psychiatry. This hasn’t become “real” enough. We need major motion pictures showing what’s really happening on a large & small scale. Individuals stories & also movies showing the corruption, lies, & greed especially in the APA, FDA, government officials, politicians.
Perhaps a movie about the APA? Their history of torture, abuse, eugenics, racism. Their inner workings & ties to the drug companies. Most people are unaware that much of our mental health “care” is based on a few people hashing things out in a room during the DSM voting committee circus. These few people hold the power to fundamentally alter countless lives & determine who’s in & who’s out in society through their diagnostic classifications. (Hmm, any votes on which movie stars should play the DSM voting committee?)
Thalidomide was pulled from the market relatively quickly. Society was shocked when they saw images & videos of those deformed babies. Our injuries aren’t visible in this way. We need to make it real to them. They need to see it. To feel it. To be heartbroken & disgusted & enraged. One Flew Over the Cuckoo’s Nest stirred the public’s rebellion against psychiatry in the 70’s. Although, for me, it did not fully capture the brutality of the inpatient experience & ECT procedure or the devastating aftermath of this type of trauma, violation, & injury on a person’s life.
We can do even better than this now. We need numbers. We need this to become a household name, a hot topic, part of our vernacular like abortion & racism. Something so ugly & real that people can’t look away. It must extend beyond the psych survivor/psych advocate community. The “average” person needs to see that, with the expansion of diagnostic classification & forced treatment laws, they too are are risk of being subjected to psychiatric enslavement & mutilation.
I also have a vision for an art exhibition in a big city where survivors can display work related to their experiences in the mental illness system. Perhaps in Washington DC near the APA’s headquarters 😉
Any opinions, ideas?
Report comment
When the Chief Psychiatrist can rewrite the laws to cover up what were criminal offences, and fail to report to the Corruption watchdog because ….. well, we covered it up so why bother?
Significant to note that since this time, the laws have been ‘amended’ to give ‘us’ “added protections”. Now, best you don’t look at what they mean by “added protections” but in brief;
teenagers can ‘consent’ to ECT, and doctors can not be held accountable for any damage done. ie no litigation threat which was a concern…… so they got ‘protected’.
The ‘little problem’ with arbitrary detentions, that is, the protections afforded the community by the law under s. 26 of the MHA has now been removed. Any Community Nurse now using police to have people snatched form their beds has been resolved. In fact, these guys are now working from Police Stations, where the ‘treatment’ and ‘coercive methods’ being used which tend to result in the need for the trauma to be ‘treated’ can be made ‘on the run’. No need for those pesky “reasonable grounds” given their paranoid delusions (or ‘suspicions’ if you like) are all the grounds they need. Consider the use of “suss laws” with the ability to force drug anyone you are ‘suspicious’ of? They’re bad enough when police get such powers, but with a needle full of brain damage, for an incompetent the likes of the ‘verballer’ I met? It really does bring psychiatry down a notch when Community Nurses are giving ‘diagnoses’ and prescribing the drugs before they even leave the hospital to meet their “Outpatient”.
https://www.youtube.com/watch?v=oZ9UQKBUrsg&t=3s
The “concerning aspects” of this detention, no longer a concern given it is the ‘illness’ of the man which is now the issue, and not the cause of that ‘illness’. Formed by the waiting Community Nurse and off to the E.D. to be put into an induced coma until he stops whining.
Added protections for Police by making their ‘referrals’ not based on anything other than a ‘suspicion’ (as opposed to the one where they need a reason other than I want him to stop screaming when I crush his fingers, or apply the tazer to his testicles).
And then there is the subtle changes to the laws relating to mandatory reporting to the corruption watchdog. That really was a problem for those doing cover ups as ‘principle authorities’, not wanting their ‘internal problems’ being examined by an outside ‘independent observers’. Having to report torture and kidnappings in writing must have made them cringe. No longer necessary, and the prison term for such non reporting has been removed I believe. Given the comments by our previous ‘leader’ (whose concealment of acts of police torture was part of his downfall once the video was released) that the Corruption watchdog was now “redundant” and shouldn’t be investigating public officers………has come to fruition with the rather long winded amendments to the Act. A ‘paper trail’ showing a removal of accountability, and “added protections” for those engaging in human rights abuses.
A “zero tolerance” policy if you like, that is zero tolerance of anyone trying to access their human rights or the protections afforded by the law…… which, as we know, the Chief Psychiatrists rewrites according to his requirements WITHOUT THE NEED FOR PARLIAMENT. Is the community aware they have no right to legal representation when public officers commit offences against the community? I’d suggest this is a bigger myth than the ‘chemical imbalance lie, that you have a right to legal representation.
They can ‘patch’ the problems later by invalidating the report of the U.N. which stated quite clearly that Australia’s mental health laws ARE a violation of human rights, and MAY constitute acts of torture (without a confession, it could never be proven… so keep your mouths shut doc). The benefits two fold, because the public is stripped of their rights and legal protections, and they think they have received “added protections”. No need for acts of gross criminal negligence by public officers coming across acts of torture and kidnappings (not to mention the ‘unintended negative outcomes’) having to report anymore.
Euthanasia Act?
This is straight form Himmler’s diaries (see the problem caused by Josef Hartingers report into the deaths at Dachau, and the ‘governments response to their ‘problem’. Bury the facts and change the laws to make it lawful…….and then the killings started again), and the public blissfully unaware that it has been done. The stealth model has actually been quite effective.
At last, carte blanche, and they should be able to ‘get the job done’. Which unfortunately seems to be taking a little longer than expected……and it looks like our hospital system is in an absolute mess but ……. maybe added powers?
I mean really, what is there beyond carte blanche and zero accountability? And a public more afraid of their local police than any ‘terrorist’ or ‘mental patient’. The obvious justification for the removal of ‘our’ rights.
Can’t defend these rights on my own, and these people obviously place no value in them…… until the boot is on their heads, and it’s their families being “fucking destroyed” for trying to exercise what they no longer have, that is a right to complain about being tortured (article 13). And I note the use of a document KNOWN to have been produced using an act of torture being used by the C.P. to defend the unlawful detention (Article 15)….who cares about such bits of paper when your being waterboarded, they scream for their mothers not the United Nations. Ask the Community Nurse who I note is STILL torturing people to this very day as a direct result of the negligence of others.
This then becomes STATE SANCTIONED TORTURE.
So my refusal to speak to a private clinic psychologist (with a Masters degree no less) about a family conflict results in the exposing of the State sanctioned torture program ….. and i’m surprised that none of y’all want to look? I really have lost my mind, of course you wouldn’t look, you’d end up in the ‘cells’ with the rest of ‘us’.
Report comment
I also make note here of the dilemma for the State caused by Article 10 of the Convention against the use of Torture.
It may be claimed that the Community Nurse wasn’t aware that what he was doing was enabling acts of torture?
In which case the State has been negligent in their ‘training’ of him under that particular Article which states that;
1. Each State Party shall ensure that education and information regarding the prohibition against torture are fully included in the training of law enforcement personnel, civil or military, medical personnel, public officials and other persons who may be involved in the custody, interrogation or treatment of any individual subjected to any form of arrest, detention or imprisonment.
2. Each State Party shall include this prohibition in the rules or instructions issued in regard to the duties and functions of any such person.
How many public officers believe they can ‘spike’ citizens with date rape drugs and then subject them to hours of interrogations and ‘acute stress reactions’ (ie beatings, and ‘mock executions’ which are considered ‘coercive methods’ where I live as they are not ACTUALLY going to execute you, just they make you think that, ergo not torture by definition (Combined with the ‘spiking’ which is a physical assault, different matter. Hence the need to conceal the crime) See Article 1 for the ‘loophole’) and it doesn’t break the rules?
I know 1 that does. And he is providing ‘care’ for the families of others to this day. Glad y’all are happy with that. And they do reports as to why people are killing themselves after walking out of this ‘hospital’? Why bother, it’s kind of obvious, but I guess someone has to do the “editing”.
Now the “guidelines” do seem to cover these acts of torture, and I would suggest that the State has a defense in that they have made it very clear to this Community Nurse that he isn’t allowed to torture citizens.
But what if he were to inform us that they are actually enabling him in the acts and that was why he felt he could laugh at me when I said I was going to have something done about his vile conduct? Perhaps the reason the Operations Manager felt she was justified in threatening my family and “fucking destroying” me? Not like anyone was going to step up and say “this is wrong”…… though I note someone said they didn’t have the stomach for the ‘resolution’ and rudely interrupted that in the E.D. Though a need to retrieve the documents proving what I am saying was necessary before providing the Law Centre with the fraudulent set….. and then the letter from C.P.
Consider the consequences of them thinking the documents had been retrieved, and then they turn up in a Police Station, showing the cover up? Of acts of torture and well….. the other stuff no one believes anyway because “they wouldn’t do that”. Rock solid defense that is.
Knowing the State was ‘protecting’ the Community Nurse from any form of prosecution for his acts of torture, and criminal conduct in the production of false documents? I mean, who would have thought police would be out trying to retrieve documented proof of such vile acts to ensure that the criminal wasn’t prosecuted? Placing a ‘flag’ on the complainant for an automatic referral to the criminals so they could resolve their ‘little problem’ with a needle full of ‘care’? Such mercy being shown by these people huh? Particularly considering they were the cause of the damage in the first place with their unlawful use of force.
Class action lawsuit. I’ve got the documented proof of the wrongdoing of these people, and putting it in front of a lawyer is like throwing Holy Water over Dracula, and tying him to a sunbed. They wouldn’t touch it, and their life depends on that in Australia. They have been well told not to be ‘zealous’ when it comes to mental health claims, given the ‘benefits’ to the State from such human rights abuses. Ask our ex Treasurer why he had to flee the State when Police were chasing him to do a ‘referral’. Seems some people were ‘in the know’ as to what the consequences of upsetting the wrong people was (ie the Minister for Mental Health)
Report comment
I was reading about getting one’s psychiatric records. Pleasebe aware in many states and places in the US, the only way you can see your records is if you read them in a protected, secure room with a designated employee of the clinic sitting beside you. And there are probably other rules involved, too. Just so you know. That is what I was told upfront many times when I was in the process of obtaining services or a change in services from the clinics of which I was a “patient.” Thank you.
Report comment
Do you know what psychiatrists are taught to do regarding patient records? They are taught to write the records in a manner not to maximize accuracy but instead to minimize the chances of a successful lawsuit. Don’t expect medical records to be accurate or even reflect what the doctor personally believes about the patient.
Report comment
Sometimes the records aren’t even the right patient. As a preteen they had me confused with another patient and would argue with me when I resisted being given his treatments. At one point they gave me his EEG and him my ECG. The doctor thought I was going to have a heart attack from the meds and never realized what I meant when I said ‘it wasn’t my heart.’
Report comment
“As a preteen they had me confused with another patient and would argue with me when I resisted being given his treatments.”
Police here delivered an aboriginal man to the hospital, and they insisted that his refusal to answer to the name of an escaped patient was his illness. They then force drugged him with that patients drugs and he ended up on life support in the E.D.
But, as our Minister said when asked about the report regarding the nearly 50% of women reporting being sexuality’s assaulted in the locked wards……”You can’t listen to them, they’re mental patients”.
If they tell you your Jesus, you’d better bloody accept that lol.
Obviously not a problem when the hospitals can “edit” the documents relating to his ‘treatment’, and threaten and intimidate the witnesses. And as discussed, i have made note of the ability of the Chief Psychiatrist to rewrite the law as required. He will end up owing them the price of a new Porsche for his treatment by the time they’re finished lol
Report comment
I believe you could do a class action lawsuit. But remember that such a class action lawsuit would be not just a lawsuit but a P.R. debacle for psychiatry and Big Pharma and certain parts of mainstream academia as well. Except, that’s just what’s needed to spur on the maximum amount of change for the better possible.
With that in mind, I strongly recommend such a class action suit to name Harvard University prominently if it can. Harvard is one of the biggest names in the world so such a class action suit would get so much more press if it targets Harvard University as well.
Many attorneys might refuse to take the case in the first place, simply saying that they know it’s better for their careers to stay on the good side of Harvard. I don’t know — how about starting up an association of psychiatric patients who were victimized who can be one of the plaintiffs in such a lawsuit? Where there are regular monthly meetings members can go to, where they attend in person, and the sociability drives the whole dynamic forward.
Lawyers are more willing to take cases if they know there is an active association that regularly makes the news who will endorse their good name even in the face of attacks due to them going up against the establishment. Hard to explain but, the way the media works, they are partial to organized groups who they can regularly rely upon for sources in a practical way which makes their jobs easier to get done.
What about including, for instance, the bought-and-paid-for invention of “child bipolar disorder” by Harvard professor Biederman? If you think Prozac is bad, wait until you hear about the anti-psychotics. Far worse mental straitjacket. And putting children on them? I’m horrified.
Honestly, he’s destroyed their lives, of so many children who were put on those drugs. It’s criminal. Except the parents can’t sue because they needed the welfare money in the first place and can be accused of being bad parents to have let it happen.
And, as for the kids put on anti-psychotics who are now adults, there is not enough evidence out there showing just how much the anti-psychotics permanently disabled them, made them so they will never be normal and never live normal lives, so as to help them sue. That is a problem. I strongly suspect that one of the things academic institutions do for the drug companies is simply to agree to avoid studying an issue in the first place, especially when they strongly believe that conducting such studies might expose major corporate donors to legal liability.
However, let me ask. Is there any group out there which could DO the class action lawsuit? It’s not good enough simply to write an article about it. You have to find a group willing to take it on.
Report comment
First you need to define a “class” that would be acknowledged as such by a judge, such as “those people who have been harmed by misleading claims that emotional distress is caused by chemical imbalances and that drugs can correct these imbalances.” Then you would need to find people who would be acknowledged as spokespeople for that class.
Report comment
Because so many “nice” and “respectable” upper middle class white professionals jumped on the “chemical imbalance” bandwagon, they can’t be sued as they are like those “too big to fail” banks.
Report comment
https://en.m.wikipedia.org/wiki/List_of_largest_pharmaceutical_settlements
Most of these drugs are part of the ‘bipolar cocktail’ that is a prerequisite for the ‘treatment resistant’ form.
These are not civil cases, they are the result of the drug companies pleading guilty to criminal acts.
Report comment
A class action would be strategically very clever. It would get lots of news coverage and put the APA on the defensive and highlight links with Big Pharma.
Report comment
Absolutely
Report comment
Another front? Action against NPR.
NPR should not be allowed to misue tax dollars of any amount to mislead the public and contribute to public health problems. Presently, NPR gaslights the American public by broadcasting a Big Lie: that no Americans suffer psychiatric harm under the current biomedical model.
NPR should be forced through public and congressional pressure to tell the full story of psychiatry. All labels are based in bias without scientific test. And the rest. No “chemical imbalance” etc. Sunshine laws!!!!!!!!!!!!!!!!! Generations of so called care givers mistrained.
Use a media campaign aganst NPR as a spring board for class action suit.
Report comment
You mean National Pentagon Radio?
Report comment
I think it is NeoLiberal doctrine which is pro-Psychiatry, Psychotherapy, and Recovery.
Thomas Insel calls these Mental Health Workers.
We have vast labor surpluses, and so creating jobs is used to oppose environmental needs.
So hiring on these Mental Health Workers takes pressure off of the labor market, but it also sets up a cadre of voters.
More and more, poor people, the unhoused, drug addicts, and criminals are being portrayed as “mentally ill”. And then the number of Fix My Kid Doctors continues to grow.
We have to just find ways to take these people down.
Everyone knows that the idea that someone is “mentally ill” starts within the family. If family members stood with someone, the White Coats would not have a chance. It is only after someone has been ejected from family and clan that they are prey for the mental health system.
As Sacramento Mayor Darrell Steinberg is a big part of the CA plan to place the unhoused in psychiatric internment, I’m pointing out that this is exactly what he had done to his 13yo daughter.
https://www.madinamerica.com/2022/04/saving-lives-cementing-stigma-review-just-like-you/#comment-200535
Joshua
Report comment
You are so right about the too many lousy families of America. I blame Jesus culture. Even when families aren’t Christian.
Report comment
The Born Again Christian movement and the Mental Health Movements have always been quite close, both based on their own version of original sin. But now they are seamlessly fusing.
https://hope4mentalhealth.com/
It is also there in the concepts of Recovery and Healing. And from where I sit there is regular evidence of government collusion, direct and indirect.
It is also in the neo-liberal doctrine, which is perfectly happy to sacrifice some people labeled as mentally ill so that we don’t need to go to no needs test public housing and universal income. After all, that would severely undercut the real estate industry in its economic harvesting.
Joshua
Report comment
Psychiatry will adapt to serve the interests of whatever group is in power. That would be the neolibs right now, but this is not exclusive.
Report comment
I agree. The intent is pretty much sociopathic. Whatever gets the power and money is what they’ll do. They will serve communism, fascism, corporate capitalism, state-controlled capitalism, even anarchism, as long as they can gain the power and money they wish to compile. This is true of most industries, of course, but in this case, the scope of the damage done is so vast, and the insult to human self-determinism so blatant, and the lack of accountability so complete, I think it is a special case of extreme danger to the survival of any system which allows its participation.
Report comment
Let me start by saying I was a victim of a criminal scheme involving abuse somewhat tied to the mental health system. Even while, also, the perps may have had ties to September 11th as well. Well, by now I’m very sure they did.
The interesting part was, I knew or understood before that I was a victim of a warfarin overdose, which by some fluke was way smaller than they intended, so I was able to flee the hotel room and it was a disaster for them, for what they were planning.
But I failed to understand the full story because it was so scary, I got memory repression syndrome over it.
Well, after enough recovery from the ptsd, I looked back over emails I sent to a lawyer right after.
It turns out they had put a grenade on the bed as well. And then, well, after remembering the grenade, I had this weird feeling that I thought they were planning to come back and use gasoline as well. And why?
Well, I have a document that shows someone who was definitely a perp/criminal viciously attacking me over something — unfairly, of course — but then going further and suddenly making this weird statement “you take a can of gasoline and put it behind your back as if you didn’t know that fire burns.”
My twin brother had been misdiagnosed with “persecutory delusions” of parental neglect. And my back area really did have deteriorated disc that was worn due to over 22 years of writhing in pain from a muscle spasm that could easily have been fixed, and my parents refused to take me to a doctor for it.
I am a pipe organist. Other Harvard organists harassed and tormented me for years until I finally complained. And then Harvard arranged for me to get the same diagnosis as my brother — kinda sorta in this somewhat sleazy sketchy way — all as an excuse to cover the matter up.
Meanwhile, top Boston area hospitals got involved in covering up what should have been a scandal in the mental health system, making them all criminally complicit.
Also, it sounds like they were involved in sep 11th and used psychological torture as a way to cause memory repression syndrome over some of the information they told me about — deliberately — regarding September 11th. This part is interesting but Harvard even had one man tell me that Harvard really had perpetrated sep 11th via remote control flying the planes into the building using computers. And later evidence/info I got also pertained to sophisticated computer audio synthesis capable of faking a muslim crime via very convincing sounding faked audio recordings. And over the phone stuff — calls to peoples’ relatives.
Interestingly enough, after dropping out of Harvard, I did go to the Department of Homeland Security to try to feel them out regarding what I could come forward with, and it’s as if they already knew the truth and I was met with extreme hostility. If my parents retaliate against me for talking about what I know, the govt will not protect me and will not help me in anyway shape or form. If my parents even go so far as to cut off all funds and make me homeless, will the govt STILL not intervene in even that? The answer was, no they won’t, and the guy literally said “then you will be homeless.”
So I was forced to get a job first. Well, I ended up steered to an insurance company, which didn’t pay enough. However, here is a big problem. If corporations had perpetrated Sep 11th, in hopes of starting up a war in Iraq and Afghanistan, which would serve as a pretext for them to be able to do unethical medical experiments — I was told in robotic cancer surgery, by a Harvard math grad — then any exposure of the truth by me would result in an investigation putting blame on lots of corporations.
What does this mean to the insurance industry? 3000 families of dead WTC victims able to sue lots of deep pocketed corporations for “loss of consortium” amid very bad publicity, so the settlements would all have been very high. And this would all have been underwrited by the insurance industry. And they would have been the ones required to pay all the damages.
But, also, the truth would have exposed corruption in the psychiatric system, which could also have been impetus for enormously sized class action lawsuits, all involving liability for hospitals doctors and pharmaceutical companies which was underwritten by the insurance industry.
The interesting part of this whole scheme is, I now conclude that Harvard wanted me to know about their and corporate america’s involvement in Sep 11th just a little bit, so there would be just enough evidence on my computer, albiet sketchy, so as to potentially implicate corporate america badly enough so the insurance industry would have a big financial motive to get involved.
And then the insurance industry would try to cover it up. And that’s exactly what the company I was working for tried to do. And the so-called “rat poison incident” was intended to be passed off as a “suicide bombing” terrorist incident which, if it had succeeded, would have caused a fire killing lots of other people, not just me. But the placement of the grenade was to be in my back area to help destroy scar tissue and evidence of deteriorated disc.
And they’d pretend I’d done it to myself, and also pretend that was “proof” I was crazy.
Prior to that, they’d arranged for me to be in situations where I was victimized criminally or otherwise hurt in a way to make me complain, all the while crooked individuals fed me fake stories regarding the perpetrators, which I’d repeat to others or quote. But they intended to deny it so as to make me look like someone who was “crazy” and who made up fake stories about people who rejected me. Or something like that.
And this happened over and over again. One example. In the insurance company, the mother of this 19 year old guy who was also working there, and who was pretending to be gay and attracted to me possibly, makes sure I overhear her on the phone, telling someone else that he’d been admitted to Westpoint Military Academy. Something I repeated to others — only to later find out it was totally false and she was lying.
Again, they were going to deny that she’d said that, and instead pretend that “this is the illness” and that was proof I was crazy.
So that takes care of the Sep 11th references in my email account. A crazy man making up crazy stories. An accusation which would have worked had they pretended I’d gone crazy and done a massive suicide bombing at the Chelsea Hotel in NYC. I believe they also planned to do something with respect to deleting tons of evidence on my computer, literally crafting a whole entire fake paper trail to super impose on the truth — where I was tragically bullied in extremely horrific ways for a very long time. Raped, brutalized, and years of psychological torture. Evidence of which would have been destroyed if I’d been burnt up the way they hoped for.
But one more interesting twist. Not long before the failed rat poison incident, one gay man I hooked up with told me that “they” — the establishment or whoever — actually plan to soon phase out neuroleptics (and maybe SSRI’s) but he focused on neuroleptics. A plan to phase them out. And I asked why. And he said that everyone knows they are ineffective, but also they have such terrible side effects that compliance is a big problem, even aside from questions of effectiveness. He didn’t say what would replace them. Oh wait, maybe I asked what would replace them and he said they have been researching all sorts of other potential alternatives and some have been found to be very promising.
And I remember getting very excited and saying “maybe I can use my situation to help.” And he just did not answer. Pregnant silence. I do know that light therapy was an area of research, and they’d been doing unethical medical experiments on me in that arena, and also on children. Developing children. It’s possible modern building materials are a problem which inhibits proper developing of parts of the brain, leading both to myopia and eventual depression. Except, they would have wanted to cover up prevention techniques in favor of profitable treatment.
Even worse, I believe the technology — mathematical technology — exists and existed long ago so we could have had very cheap energy from nuclear fusion long ago. And they blocked that because, for various economic reasons, it would have cut into corporate profits AND academia’s endowments very dramatically. But that’s the kind of thing that would have allowed cheap enough energy so building materials would allow the right light rays in, for developing brains, both to prevent depression and myopia as well.
I do think they wanted to use me to raise awareness since I was really beautiful and talented so they could say it was such a shame — and mute the outcry over all the deaths to others by insisting “it was an illness” and then “now we have new ways to help” and even say the issue was “non-compliance with psych meds” because the current meds were so bad.
Doing it the terrorist way would have mollified corporations worried about bad lawsuits. How do you market a new product without bashing the old one and encouraging lawsuits? Also, there is a big problem regarding over diagnosis of schizophrenia, bogus diagnosis of schizophrenia, often to cover up crimes. We don’t want to raise awareness of that, not so long as we are a regime based on making money off over consumption or coerced consumption or coerced consumerism.
The five fold black-white schizophrenia diagnosis disparity was never mentioned in Rob Whitaker’s book. And that was quite an oversight.
Let me note, the mental health issue is just the tip of the iceburg. The current academic corporate complex is a bad system and bad in every way, not only mental health.
The problem is the forced sedentary nature of their economic model. You go to college and study alone indoors sitting down for how long? And then do the same at the job you get afterwards. Much mental and physical illness is a result of that and the best ways to help cure such problems would be to abolish academia or abolish expensive secondary schooling, and change the economy so it has the kind of flexibility that would allow us to all live much healthier lives in the first place, which would amount to prevention. And, also, we have a terrible culture as well. Americans don’t treat other Americans well.
The system feeds upon itself too. The poorer they are with prevention of illness, the more money they make treating illness.
We need a radical medical and economic revolution, and what they were planning was probably somewhat better mental health treatment, but which would have preserved their hegemony and their $$$$$$$. Also, ANYTHING would have been better than the current regime of psych drugs and neuroleptics. The bar is set so low, they can turn themselves into heroes by advocating something still very mediocre but just a little bit better. Rather than be called out as villains, for having supported that kind of evil in the first place.
Report comment
As someone who has studied non violent direct action campaign strategy I think a class action would make perfect sense.
What is needed however is an organisation to take it on and develop a strategy alongside that to organise those harmed by antidepressants and others interested in the issue to push the issue in other ways.
Report comment
I am very happy to see that Robert Whitaker will be participating as a presenter at the SPARK THE CHANGE – 2022 CONFERENCE in Syracuse, NY, hosted by a nonprofit I am very fond of, It’s About Childhood and Family, Inc.
The two-day symposium brings together presenters with very interesting backgrounds sharing many positive motivational programs for parents, educators, clinicians and childcare providers.
As someone who has experienced being misdiagnosed with a psychiatric disorder, the crippling side effects of psych drugs, the stigma of being labeled “mentally ill”, the financial losses of psychiatric treatment, along with seeing psychiatric treatment completely destroy the lives of so many including members of my immediate family, I do understand the appeal of creating a formalized complaint of wrongdoing and going through the legal process by which a court of law will hopefully make a favorable decision based on the alleged wrong of telling a false story.
It does seem like it would be a complex and costly process that will take many years to resolve.
I have experienced personally and have witnessed situations in which attorneys profited considerably off of individuals needing legal assistance for matters involving “mental illness”. In some situations, it was just quick and easy money for the attorney and the client overpaid for services with money they had to borrow.
For me, it is sickening to know the manufacturing of “mental illness” is probably even a more profitable industry for attorneys and for-profit correctional facilities than mental health professionals.
Whenever I hear about a class action settlement, I often wonder who makes out the best, the parties who suffered the actual harm, or the attorneys on both sides trying to make arguments on their client’s behalf?
The 2000 movie “Erin Brockovich” was based on a 1996 case that ended with a $333 million settlement on behalf of more than 600 plaintiffs.
Masry & Vititoe, and two other law firms received 40 percent of the settlement ($133.6 million), and Erin Brockovich received $2.5 million as part of her fees, victims received $196m, roughly $300,000 each. According to reports, many victims received $100,000 or less.
When I consider the many different factors involved in advocating for individuals labeled “mentally ill”, the problems they face and who is right, who is wrong, I think of the 2005 heated debate between Tom Cruise and Matt Lauer as an important example. This argument truly demonstrates the schizophrenic nature of mental health advocacy itself.
Although Tom presented an anti-drug argument based on facts, and Matt did not dispute those as being false, Matt’s pro-drug argument was based on the experience of knowing individuals who claim to benefit from taking psych meds. It is an argument in which both sides are correct.
I have also met many individuals who claim psych drugs/psychiatry/ECT/forced treatment “saved their life” or the life of their loved one. I do not think it is right to discredit their individual experience of claiming benefit, as I would not want anyone to discredit the harm that I claim.
In my opinion, Tom’s argument only became weak when he was asked by Matt as to what he felt the alternatives to psych drugs were and his reply was only “exercise and vitamins”, which does work for some situations, but certainly not for everyone.
I think the lack of awareness among pro-psychiatry advocates, and even prescribers of psych drugs, on what the alternatives are, keeps organizations like NAMI pushing for an agenda of forced treatment and keeps doctors prescribing, while turning a blind eye towards the great harm being done.
An insightful comment I came across in was written by a psychiatrist I know from Syracuse, NY and was published as a Letter to the Editor in a 1985 issue of the American Journal of Psychiatry, entitled, Homelessness Not a Mental Health Problem.
file:///C:/Users/17273/Documents/Homelessness.pdf
In his concluding statement, Dr. John Tanquary wrote:
By excluding “legitimate” psychiatric treatments, an alternative to psychiatry is created. This alternative could substantially erode the power base of psychiatric authority in this country.
I think among the general public and media professionals, psychiatry is viewed as an optional treatment, and unless having experienced it, most do not consider psychiatry to be a power base of authority. Even though pharmaceutical commercials state harmful side effects, I don’t think most people believe psychiatric drugs can induce more harm than good, including suicide/homicidal actions. Our lawmakers, along with many involved in advocacy, consider “mental illness” as a public safety issue and forced psychiatric treatment as a necessary, beneficial service that will improve a patient’s life, so it is a good thing to force them to accept psychiatric services, regardless of what they want.
I think the lack of awareness among our lawmakers and pro-psychiatry advocates on what the alternatives are, keeps organizations like NAMI pushing for an agenda of forced psychiatric treatment, while turning a blind eye towards the great harm being done.
I believe that creating a greater awareness among consumers and their advocates on alternatives to psychiatric treatment and fighting for the consumer’s right to access those treatments, is the most effective way to erode the power base of psychiatric authority in our country.
Our country and private research efforts spend an enormous amount of money on psychological and psychiatric research that seems of absolutely no value, while so many small organizations work diligently on shoestring budgets to provide resources that improve a person’s ability to overcome or avoid being in our broken mental health care system and a victim of forced psychiatric treatment.
In my opinion, there is an urgent need of help in our country, and we need to all work together with integrity and focus to bring forward the many proactive solutions and alternatives to psychiatric treatment that already exist.
We can all be part of a class action to spark the change in our everyday life and our community.
Report comment
Although I am (still) an attorney, I don’t have any experience with class action lawsuits, so I can’t say how this one might work out. But it is very clear to me that, no matter how this proposed suit will fare in the courts, if we make sure that the general public hears as much as possible about this, it will be a big step forward in taking away the power of psychiatry, which is more of a very profitable cult than a real medical specialty. The more the public sees psychiatry as it really is, a destructive force in our society, the sooner psychiatry will have its power taken away. What was done to me was over sixty years ago, way past the statute of limitations, so I can’t be a plaintiff, but I will urge everyone I know to be part of this lawsuit if they can.
Report comment
Dear Ted,
I hope that you are in good health and thank you for your life-long commitment to advocacy.
I don’t think most people in our society realize the power psychiatry, and other mental health professionals actually have, as well as what forced psychiatric treatment involves.
It is important to consider, how do we define this power, who does this power impact directly, and why has our society entrusted psychiatry, and other mental health professionals, with so much power?
In my opinion an important issue is:
Does the Diagnostic and Statistical Manual of Mental Disorders create a class of people who can be legally deprived of many rights, including the freedom to contract?
Unlike any other class of people, individuals diagnosed with mental disorders can be legally forced to contract the services of the providers, including the very providers who diagnosed them with the mental disorder.
I think it is important to differentiate between patients who are forced consumers verses those who willingly seek and freely contract mental/behavioral health care services/treatment/products and are satisfied consumers.
The Court’s decision in Wyatt v. Stickney 325, F.Supp. 781 (M.D.Ala. 1971), determined that patients have a “constitutional right to receive such individual treatment as will give each of them a realistic opportunity to be cured or to improve his or her mental condition.”
Yet, patients under coercive psychiatry are usually treated with an unscientific one-size-fits-all drug treatment plan that forces customers to purchase and ingest pharmaceutical products that are known to make a patient’s mental and physical condition worse, cause death, or cause the patient to commit crimes, including homicide.
Our society turns a blind eye to the lack of psychiatric consumer protection and the fact many prescription drugs can induce homicidal actions, as was the case of Ryan Ehlis who was acquitted of the murder of his five-week-old daughter Tyra. The criminal case was dismissed after psychiatrists for the prosecution and defense agreed that the prescription medicine he was taking for ADHD, Adderall, was responsible for the tragedy by inducing a temporary psychosis. The unbelievable response from the drug company published in a USA Today headline was, “Despite the slaying, Adderall remains a safe and effective drug for controlling attention deficit-hyperactivity disorder, or ADHD.”
In a later civil court case, the United States Court of Appeals, District Court of North Dakota, affirmed the lower court’s decision to dismiss a lawsuit brought by Ehlis against Shire for $100,000. Ehlis contended Shire knew Adderall could induce psychosis and failed to adequately warn of the associated risks and side effects. The court ruled the “learned intermediary doctrine” barred the claims of failure to warn. This doctrine provides that a pharmaceutical manufacturer has a duty to warn a physician of the risks involved with a drug, and the physician acts as a “learned intermediary” between the manufacturer and the patient. “Thus, a warning to the physician is deemed a warning to the patient; the manufacturer need not communicate directly with all ultimate users of the prescription drugs.”
How many parents killing their own children because of taking Adderall does it take before this drug is taken off of the market?
Isn’t just one enough?
Tragic cases like Ryan’s, Rebecca Riley’s and Gabriel Myer’s make the news, yet go unnoticed by so many in our society and the harm continues.
If we consider the facts presented by Robert Whitaker for a class action lawsuit against psychiatry in the matter involving depression and the chemical imbalance hypothesis, I am wondering about certain aspects including:
– if the class of plaintiffs would be limited to; individuals who were diagnosed with depression, told their depression was caused by a chemical imbalance, were prescribed an antidepressant and suffered harm from the antidepressant?
– if the class is limited to just patients diagnosed and treated for depression, how many were actually treated under psychiatrists, or were most treated by other providers?
– how many in this class would represent patients under forced psychiatric treatment? or would the majority be those who voluntarily accepted mental health care services and treatment for symptoms of depression?
– would this matter include pharmacists and retailers who sell antidepressants, treatment facilities that provided antidepressants and marketing/advertising mediums for antidepressants?
– if insurance companies, including Medicare/Medicaid, paid for the antidepressants, does this matter involve insurance fraud?
Report comment
Hi mariamangicaro,
you seem to have quite a grip on the legal aspects related to these drugs.
In Australia the State governments are enabling the covert drugging of citizens to incapacitate them and make taking them into custody easier. The ability to ‘plant’ items on them once icapacutated making the arbitrary detentions appear lawful….. however.
There was a case of a man who claimed to have been ‘spiked’ in this manner (known to be being authorised by the State by allowing fraudulent documents to be prepared post hoc to conceal the criminal nature of the offending) who then poured gasoline over his children and set them on fire.
There would be a defense for his action if he were allowed access to unedited documents showing that he had been drugged without his knowledge. Obviously such access would be denied by the State and the documents “edited” to ensure his conviction.
One of the issues I see with the matters you describe above is that there is no consideration of those people (later to become ‘patients’ after the documents are “edited”) who are being drugged without their knowledge with these date rape drugs for the convenience of public officers. Later concealed by a doctor writing a prescription for them and making them their “Regular Medications”.
And maybe the U.S. isn’t as ‘progressive’ in these matters as Australia, after all as was shown in the Kennedy Royal Commission, we had the ‘advanced coercive techniques’ being used in Guantanamo Bay available to the most junior of police back in the 1980s. Cattle prods and simulated drownings greasing the wheels of justice.
Police being forced into ‘medical supervision’ with ‘referrals’ done to mental health to extract information the obvious solution to satisfy the bleeding heart liberals who don’t have the stomach for what needs to be done. These days it’s the ‘spiking’ with date rape drugs and causing ‘acute stress reactions’ that are clearing the path to ‘confessions’ and ‘justice’ (along with the use of lawyers as paid informants. See Lawyer X, Nicola Gobbo The breaching of confidentiality at mental health services after chemically koshing citizens a concern though not one ever being voiced by anyone other than the victims)
So what about those being drugged without their knowledge? Or doesn’t it happen? (the famous defense offered by the community here when they refuse to examine the proof. “they wouldn’t do that”)
Report comment
Hi Boans,
Thank you for sharing this information.
I think most people take the attitude of “they wouldn’t do that” because they don’t understand there may be profit involved.
Perhaps the profit might be connected to the privatization of mental health facilities and prisons in Australia?
“There are four private companies operating prisons in Australia: Serco, G4S, GEO Group and MTC-Broadspectrum. Just these four companies combined will be paid $613.28 million annually by the Western Australian, New South Wales, Victorian and South Australian governments.
Elsewhere, the Human Rights Law Centre (HRLC) has campaigned strongly against private prisons for several years.
Senior lawyer at the HRLC, Monique Hurley, says private prisons can often see “profits trump respect for human rights”.
“Human rights do not end at prison gates, and governments shouldn’t try to shirk responsibility by caging people in private prisons,” Hurley told VICE.
“Private prisons are run off a business model where their existence depends on locking more and more people up. Instead of enabling private companies to profit off people’s punishment, governments across Australia should be focused on reducing the number of people being funneled into prisons in the first place.”
Report comment
Hi mariamangicaro,
yes, my brother worked as a manger of the sex offender treatment unit for more than 25 years, so i’ve sort of kept up with the methods of ‘treatment’.
I did actually speak at some lenght to the Speaker of the Lower House outside some offices in the city regarding the fact I had been kidnapped and tortured. His advice was to have a ‘one pager’.
It seems that i’m pretty much at that point.
Two people (one a psychologist with a Masters degree, the other my estranged wife) conspired to have me tortured and kidnapped. And they basically succeeded in this by having mental health services believe I was someone ‘patient’, and all they needed to do was to get me to talk (via an act of torture) and then have me transported unlawfully by police on a forged Form to the hospital. At that point the Senior Medical Officer could call the psychologist and she would release my medical records which she had access to at a Private Clinic (unlawful but, try doing something when your dribbling in a cell). Together they came up with a means of making my referral appear lawful.
I was then examined by a consultant psychiatrist who could find nothing wrong with me and released me after 7 hours.
The documents showed that I had been subjected to human rights abuses, and criminal conduct on the part of the Community Nurse, Senior Medical Officer. So they needed to be concealed form me and any legal representation I may have.
I spoke to lawyers and they attempted to obtain the unredacted documents they were entitled to, and I make an FOI application (which I had dealt with as a public officer) and received some ‘redacted documents. Only after it appeared that the lawyers were going to be informed of the ‘spiking’ did I actually obtain that part of the documentation (the procurement by police as a result of the lie told about me being an “Outpatient” remained concealed. A known offense under our Criminal Code)
As you can imagine, there was some concern on the part of the clinic psych regarding her involvement in the human rights abuses (advising my wife to ‘spike’ me with drugs she knew I didn’t take) and the criminal conduct such as conspiring to stupefy and commit an indictable offence etc. And me wandering around with the documents trying to have police do something about these offenses.
What she wasn’t aware of was that the police were never going to take the evidence/proof of their own involvement in acts of torture and kidnapping. But she was obviously concerned enough to have her husband (a psychiatrist) arrange to have me snuffed in the E.D. Dead men tell no tales.
Problem being my wife had spoken to someone who realised what they were likely to do, and he was waiting when they were about to inject me with what is called a ‘hotshot’ (cocktail which results in the side effect of stopping someones heart)
Once interrupted in that little bit of naughty, with police holding off on the taking of the proof of the offending, those who had arranged the ‘sting’ could then have police retrieve the documents I had, and complete the cover up by providing the lawyers with a set of fraudulent documents and what they call an “edited” legal narrative.
This being the point that the State here is concealing acts of torture with “editing” of legal narratives, and the production of forged documents to create the illusion of lawfulness (see for example the forged prescription for the drugs I had been ‘spiked’ with to conceal a known criminal offence, and enable acts of torture).
Whilst the attempt to have me killed in the E.D. may seem a serious matter, personally I’d be more concerned that there are people “editing” documents to conceal not only the original human rights abuses and crimes, but other offences which they have allowed to go to the critical point and then interrupted.
It is noted in the Criminal Code that just because there was no chance of a crime succeeding, doesn’t meant the offence hasn’t occurred. They knew they would be interrupting the attempt…… but then left the people who committed such serious offences to maintain their positions in our ‘healthcare’ system?
That is, until I turned up in a Police Station with the documents they thought had been retrieved, and they then weren’t sure as to who else had the documents, and paranoia struck deep (considering there may be consequences for the concealment of such matters given “no superior authority” where matters of torture are concerned)
What it has exposed is that the State is enabling the “editing” of legal narratives to conceal some serious criminal matters, AND human rights abuses. And that those with a duty to ensure that something is done about those matters (lawyers, ‘advocates’) can be told to actively attack their own clients for the benefit of the State. Who after all would find replacing a psychiatrist who has the stomach for the stuff they are “editing” out of existence with their fraud, difficult. He shouldn’t have to worry about his wife (with a Masters degree no less) doing ‘remote’ detentions and arranging for citizens (and clients of the Private Clinic and University) to be tortured and referred once they open their mouths to be ‘verballed’.
It’s not that they aren’t torturing people in my State, they are just getting it done with assistance of mental health services and then concealing the vile acts as being ‘healthcare’. And if you read Article 1 of the Convention against the use of Torture, this is as simple as a Community Nurse lying to Police and telling them that a citizen is his/her “Outpatient”. Then “Anything Goes”. And access to the protection of the law is denied because ‘patient’.
It should be a concern for the whole community but …… crickets. Even the Statutory body whose role under the Act is to protect human rights will ‘unread’ documents to ‘unsee’ what they don’t want to see. I don’t suppose they would want Police knowing that they were on the list of people who HAD seen the documents.
Profit maybe (not that any of these criminals will ever see inside a cell with police providing material assistance with their offending. Those places held for aboriginal children who stole a packet of colouring pencils from Piggly Wiggly), but in this instance it was more ‘political’. My anti psychiatry views and thoughts on ECT expressed to a Private Clinic psychologist whose husband is a Shock Doc also had a lot to do with it. Might be best that anyone who refuses such ‘treatment’ (at great cost) due to valid arguments be taken out. And with a State government prepared to “edit” documents relating to arbitrary detentions and torture (never mind the events at the E.D.) I don’t think the “added protections” are really functioning the way they suggested to the community.
Without the documents, there would be no reason to even consider what I am saying. The fraud sent to the Law Centre would stand, and I would be a nutjob. With them there is a clear motive for what I am alleging, and probable cause to investigate but …….. would police want to investigate the little arrangement they have had with mental health services which has enabled them to obtain information via human rights abuses such as torture? Might be best they don’t take the evidence/proof and claim there was “insufficient evidence” and the “it might be best I don’t know about that”.
The Human Rights Commission doesn’t deal with allegations of torture, and Lawyers for Human Rights don’t actually do anything to help anyone who has been tortured……and given the ‘system’ you wouldn’t normally get to make a complaint, mainly because you’d be receiving ‘forced treatment’ for your ‘illness’ or become another ‘unintended negative outcome’.
The whole Convention worth absolutely nothing to these people. No threatening of witnesses? Police had the psychologist I spoke to afraid for the lives of his family, and trying to find out who else had the documents so they could then threaten them also. Threatening my wife to retrieve the documents so they could send the fraud to the lawyers? ‘refouler’ in the E.D.?
I’ll close with a quote from Marcus Aurelius which I hold to be true. It has been the concealment of truth, or the pursuit of that concealment which has done untold harm to me and my family. Thus possibly the reason the ‘authorities’ care so little about the value of my life and would allow it to be taken for political convenience.
“If anyone can show me and prove to me, that I am wrong in thought or deed, I will gladly change. I seek truth, which never yet hurt anybody. It is only persistence in self-delusion and ignorance which does harm”
Report comment
Yes but, actually, it isn’t just about private prisons. That’s a partisan thing, to target private prisons as bad all the while overlooking public prisons as bad.
Republicans distribute political patronage jobs via private prisons and Democrats via public prisons. You need to take on the special interests on both sides.
Also, Democrats have a lot of jobs going on in the social services sector too. All those college grads in psychology need jobs tending to the children of dysfunctional homes who have problems because their fathers are in prisons. Get it? The do gooders? They are leaching off dysfunction too and we never talk about it.
Report comment
I’m not an SSRI user, but would help any way I can. Newly retired… still have space for a large project. Writer/editor/project Mgr
Report comment
Yes. Please help Carlene. Thank you
These drugs kill. Kill hope. Kill life. People don’t care about mental patients but everyone is becoming a mental patient. Maybe people should start caring?
Thanks for wanting to help Carlene. You’re smart.
Report comment
I was put on Prozac soon after it came out, for depression that a Dr. diagnosed without taking much personal history at all, and was told at that point that I would have to be on it for the rest of my life.
I was too depressed and insecure to speak aloud what the voice in my head was saying: how could you possibly know that, when this drug has just come out and there’s no substantial body of research on long-term effects/results? He also explained that I had a chemical imbalance. I spent the next thirty years on and off of Prozac. I was told repeatedly that if I went off it would no longer be effective, and that I would then have no other recourse, and would be permanently, forever depressed without hope of relief. He was kind of right, in a way, although not the way he believed. I look back now at the arrogance of that doctor and am freshly outraged on behalf of my younger self.
What he didn’t mention ask about or suggest (perhaps the 15-minute appt time had something to do with this) was my diet, exersize, meditation, or therapy. Or any other ways of dealing with depression than popping a daily pill. This was the same shrink who at one point changed my diagnosis without telling me. Much to my surprise.
Thus began a thirty-year journey into and out of an identity based on a limited and cavalier, and I believe inaccurate, diagnosis of mental illness.
I have now been off all anti-depressants for about 5 years. I will never go on them again. I have learned other ways of coping with feeling bad–much more effective ones–that don’t mean I can’t orgasm, or have feelings other than flat ones.
Standing up to the rhetoric of the psychiatric/pharma industries, esp when dealing with friends and family who are seeking and may have found some relief in anti-depressants is difficult. I certainly don’t want to rain on someone else’s parade. But when the parade is marching into quicksand, it’d be nice to give them a heads-up.
Report comment
I’m very disappointed in this article. You didn’t mention the adverse effects of Psych drugs. Yes it’s important to say they don’t work. But people get chronically and terminally physically ill from these toxins.
I have people telling me that they feel better on these. I say that’s great that you feel better but it’s probably a placebo effect. And that would be fine if these drugs weren’t so harmful. But they are killing people 20 years before their peers not on psych meds.
I myself am chronically ill from these toxins. My friend is dying from kidney failure as I write this.
Why did you leave this out of your article Robert?
Very disappointed.
Report comment
When we moved to Kentucky for career advancement, I did not get beyond the probationary period working as the Planning Manager for Louisville’s Office of Economic Development. In the 9th month of experiencing this city, then a man on Prozac would realize a mass shooting at Standard Gravure. Recently the City has come under a consent decree from the U.S. Justice Department with Louisville as a result of the history of racism along with the death of Breona Taylor. However, if one reframes the civil rights discussion across the categories of race, sex, creed, gender and disability, the ability to modulate to the last is not afforded the same degree of discourse and equal and economic respect.
My question is “Why has our struggle not yet called for the Inspector General(s) of the various Federal Cabinets to investigate the issues that are both common and specific that result in our premature deaths?”
While one can account for numbers, the real costs not understood in how to why to account must be afforded a voice in the courts, if not the public discourse.
Report comment
Count me in where do we sign up?
Report comment
I just saw this article, as a result of Linda’s comment being sent to me. I am just starting to read this very long post. Can anyone tell me if there ever was a lawsuit brought of the kind Bob Whitaker seems to be advocating? If there should be one, I would like to be involved, as I as still an (inactive) member of the California State Bar, and when I was still practicing, most of my work was about trying to protect the rights of psychiatric inmates. I know this article goes back a ways, but it is still very relevant.
Report comment