
Open Dialogue* has created a great stir since its public introduction to the United States two years ago through Robert Whitaker’s book, Anatomy of an Epidemic, and Dan Mackler’s film, “Open Dialogue.” This enthusiasm has been particularly marked in Massachusetts. This is partly due to the presence of Professor Mary Olson of Smith College. Prof. Olson is the only certified trainer of Open Dialogue in the US. In 2001, she spent a year as a Fulbright Scholar at the University of Jyvaskyla where she met Jaakko Seikkula, one of its developers and a faculty member. Already teaching dialogic-systems ideas, she teamed up with Jaakko to do a study of Open Dialogue (Seikkula and Olson, 2003). They have continued to collaborate since (Olson, Laitila, Rober & Seikkula, in press). She is planning a pilot study of this new approach at U. Mass. Medical School. Further, this past year, Mary established The Institute for Dialogic Practice in the Pioneer Valley (with Jaakko Seikkula, Marku Sutela, and Peter Rober) and began teaching a yearlong course on Open Dialogue to 28 peer and non-peer providers. Advocates, a community mental health center in Massachusetts, is sponsoring 15 of its staff to attend the training. In addition, the peer-run Recovery Learning Community of Northeastern MA has been conducting introductory workshops. Though developed and practiced by professionals in Finland, this approach is extremely appealing to peers with lived experience of recovery here in the US (in our movement, there is growing dissatisfaction with the term “consumer,” because of its passivity and commercial connotation, so we are using “peer” or “person with lived experience”).
So why has Open Dialogue gained an almost viral appeal, especially among peers? One reason is the extraordinary outcomes reported in Western Lapland, Finland, by the group of practitioners. During a 20-year period utilizing this approach, the frequency of schizophrenia in that region went from one of the highest in the world to one of the lowest (Seikkula, et al, 2006). These results were achieved by using a community-based, social network approach for young persons experiencing their first psychotic episode. I think, however, more than the treatment aspects, it is the philosophy underlying Open Dialogue, which is most appealing to persons with lived experience. In fact, Dr. Jaakko Seikkula, one of the developers of Open Dialogue, has emphasized that it is a philosophy, not a program.
This distinction between a program and a philosophy may seem esoteric to we Americans who seem to focus on reproducible, manualized protocols. In contrast to most professions, we with lived experience have had a deep mistrust of programs such as PACT (Program in Assertive Community Treatment), which insist on fidelity to a single model. In fact, a long-term approach called PACE (Personal Assistance for Community Existence) (see Fisher and Ahern, 2001 for a comparison of PACT and PACE) and an acute approach called emotional CPR (www.emotional-CPR) have been more appealing to peers because they are based on the principles of recovery of a life. I think that an approach based on principles rather than programs is more appealing to those of us going through recovery because it allows us to exercise agency and experience empowerment. It is my conclusion that empowerment as reflected in having a voice in the decisions affecting one’s life is the most important element of recovery. Programs and protocols, on the other hand, intrinsically prevent the recipients from developing agency and empowerment.
Dialogue has slowly been gaining presence in the US in other ways. At the very time that professionals in Finland were developing Open Dialogue, peers started using a dialogical approach in the US to improve communication between groups having difficulty understanding each other’s world-views. I personally was engaged in a series of such dialogues sponsored by the New York Office of Mental Health (Blanch, et al, 1993) between professionals with lived experience and psychiatrists. SAMHSA has also carried out a series of such dialogues (www.samhsa.gov). David Bohm an eminent physicist, conducted a series of dialogues in the 80s to help all concerned gain a deeper understanding of the implicit levels of reality (Bohm,1996).
So what is the philosophy at the heart of Open Dialogue? The principles of dialogue date back to Plato, Martin Buber, and Paolo Friere. I believe the essence of dialogue is the creation of a space between people for free, mutual, and creative generation of new thoughts. According to the Finnish psychologists, psychosis is the result of a person retreating into monologue, or their own world. I can relate.
When I was experiencing retraumatization from an unsuccessful love relationship and deadening research, I retreated into complete monologue. I was so disappointed by the world of our war on Vietnam and mechanistic descriptions of behavior, that I stopped speaking altogether. I was hospitalized in Bethesda Naval Hospital and was mute for over a month. Medications did not touch my refusal to speak. In fact they caused me to retreat even deeper. I only felt safe to emerge from my monologue when a corpsman, the lowest ranking member of the team, and I developed a nonverbal language of our own. We created a dialogical space between us, which has been described by Dr. Peter Rober (Rober, 2005; Rober lecture, 2012) as “a space into which life can come.” This is the space that I believe our peer movement has been creating on a national scale through advocacy for recovery. Our collective lived experience has taught us that the essence of recovery is being able to live a free and fulfilling life in the community – a life in which we are the authors not the subjects of our destiny. I would call this approach creating dialogical recovery space, which enables our life to come more fully into our lives.
These liberating life forces of dialogical recovery, however, face heavy resistance from the dominant, narrowly applied medical model. The medical approach as practiced by my father and his generation of doctors was more respectful of the patient’s participation in their healing. Without the high-powered medical technology, these humble doctors would say that doctors dressed the wound, but the person’s own powers healed the wound. I am not opposed to modern technology and medications used sparingly. In fact, penicillin, partly through my father’s research, saved my life when I was a year old. But present day health care professionals have the arrogance to think that they cure illnesses. Whether in mental health or physical health, medications can help relieve distress, but the healing ultimately must be through the coordinated agency of the person’s whole mind/body self. In mental health, this arrogant attitude leads to the imposition of a single story of so-called “chemical causation” of emotional distress on the whole society and the conviction that only a medication program is needed to correct this imbalance. I believe this model of so-called reality is perpetuating monologue, and thereby is keeping many persons in distress in their own world. I call this dominant explanation of emotional distress the “monological medical model.”
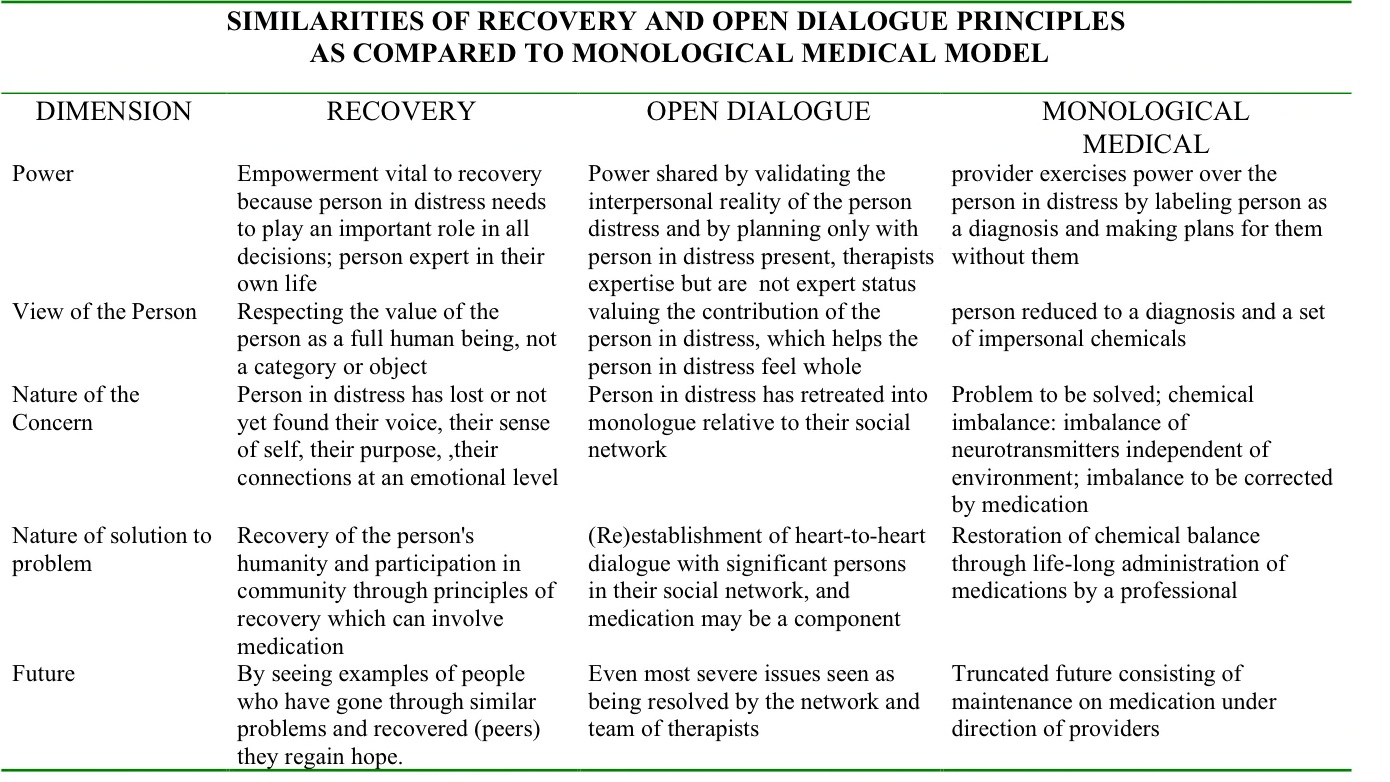
The following table shows the similarities in the principles of the recovery (Ahern and Fisher, 2001; www.SAMHSA.gov) and the principles of Open Dialogue philosophy. The table also shows how much the monological medical model contrasts with these other sets of principles:
See table:
In conclusion, I would suggest that the shift to a recovery-based community healthcare system could be greatly facilitated by the adoption of a dialogical recovery philosophy. This would mean an infusion of dialogical principles into all facets of daily living. This might be best carried out through the engagement of all the members of society in various sized dialogues, covering a variety of topics of great concern. In the healthcare field, for instance, we need much more dialogue between persons who have lived experience with mental health, substance use, and physical health issues, psychiatrists, and medical doctors. This much sought after integration of these separate fields is best done by the person suffering gaining a sense of their own agency. Once the person gains a voice in their life, they can carry forth genuine person centered, whole health planning.
* I use the term Open Dialogue broadly in this article to encompass both the specific practice in Tornio, Finland and adaptations of Open Dialogue in other areas of the world, which technically speaking are dialogical practices. I have used Open Dialogue to include both practices because the US audience is much more familiar with Open Dialogue than dialogical practices. Also it is beyond the scope of this paper to explain the details of the Open Dialogue practice. Therefore, I have focused on the principles of Open Dialogue, which are similar to those of dialogical practice.
References:
Ahern, L., and D. Fisher. Recovery at your own PACE. Journal of Psychosocial Nursing 39:22–32.(2001).
Blanch, A., D.B. Fisher, D. Walsh, and J. Chassman. Consumers/survivors share insights about recovery and coping. Disabilities Studies Quarterly. Spring issue.(1993).
Bohm, D. On Dialogue. New York: Routledge. (1996).
Fisher, D., and L. Ahern. Personal assistance in community existence (PACE): An alternative to PACT. Ethical Human Service and Sciences2(2): 87–92 (2006).
Mackler, D. Open Dialogue. Video on DVD, can be obtained through the National Empowerment Center, www.power2u.org.
Rober, P. Family therapy as a dialogue of living persons. J. of Marital and Family Therapy. 31:385-97. (2005).
Seikkula, J., Aaltonen, J., Alakare, B., Haarakangas, K., Keranen,P., and Lehtinen, K. Five-year experience of first-episode psychosis in open-dialogue approach. Psychotherapy Research. 16:214-228 (2006).
Whitaker, R. Anatomy of an Epidemic. Crown Publisher, NY. (2010).











{kind=link}
I was at a conference recently where this bloke from a Quaker therapeutic community was explaining the principles of therapeutic communities, one of them was tolerance (of weird behaviour I guess?) and another was democracy, specifically consensus decision making. There were a few others. I flippantly said to a friend that it sounded like the way the Occupy movement was run, and I wondered if participating in Occupy London, or anywhere else, would be, “Therapeutic?”
Only if your contribution to the daily meeting was fully appreciated and considered and not shouted down or ignored is my guess.
To be considered as an equal partner in any relationship is the essence of mental well-being, in my humble opinion. And mental distress so often comes from being bullied, abused and ignored. So I can see why the practice of Open Dialogue, where the voices of the distressed are once more fully considered and bought back into there proper place in the relationships of their family and social network, is so effective in relieving distress.
That Peers (and I presume by this you mean what in this country are called Peer Supporters) are being trained in this is truly inspiring and a welcome contrast to the lacklustre training I recently received that was so obviously designed by a service provider (all diagnosis categories and which drugs are the relevant treatments plus a bit of really basic counselling skills – it was shallow, demeaning and yuk).
Report comment
John, Thank you for your interest. Yes we want to enable peers to learn the most respectful, least stigmatizing approach to mental health I have found, instead of being trained in the medical model. The IPS model of Sheri Mead shares some principles with Open Dialogue, such as mutuality and sharing of power.
Report comment
I have been promoting Open Dialogue approaches since 2006. My heart and experience is closer to Jungian approaches but I feel the world is more open to hearing the voice of Jaakko Seikkula. Besides, in the end, it doesn’t matter how people recover, it just matters that they do.
See also: http://spiritualrecoveries.blogspot.com/2006/05/dr-jaakko-seikkula-dialogue-is-change.html
Report comment
Dear Spiritual Emergency, There is much that is spiritual in the Open Dailogue approach, but as you say the world is readier to hear from Jaakko Seikkula.
Report comment
I have seen these therapeutic dialogues and communities in action, in my life also. Incidentally I came across this beautiful Ted talk of a therapeutic community of unexpected kind: http://www.ted.com/talks/lang/en/ramona_pierson_an_unexpected_place_of_healing.html .
There is not only a healing of individuals, there is healing of families, groups and societies. Thank you Daniel for a wonderful piece.
Report comment
Hrannar, Thank you. Yes healing communities is ultimately the most important goal. I will look at the talk.
Report comment
Dan, your blog was so inspiring as was my recent discovery of the Open Dialogue approach to healing extreme emotional distress. Thank you for starting this dialogue here on Mad in America.
As a mother, a professional and a spiritual seeker, dialogue has long been at the heart of my approach to healing and guiding myself and others to create authentic relationships and community.
I have studied Marshall Rosenberg’s Non-Violent Communications approach and participated in Gregory Kramer’s Insight Dialogue retreats. As powerful as these experiences have been, I must confess that I didn’t think that this same process could be effective with someone in extreme emotional distress, dissociating, hallucinating.
You mention that the Open Dialogue philosophy or approach is much more accessible and credible to those with lived experience. I would suspect, in part because it can embrace mental diversity and because it nurtures and empowers those with the weakest voice (the person in distress).
In Insight Dialogue, one of the most important aspects of the dialogic process is the recognition that truth is emergent. That the interaction of two human beings, in real relationship, creates a kind of magic that transforms not only the speaker but also the listener, so that dialogue often unfolds in mysterious ways, not as predicted or scripted. As truths emerge, are they are met and responded to with an open-minded but grounded awareness. It seems that this fluid moment-by-moment context allows for and invites change, trust, shifts in perspective, common ground. Nothing solid other than a shared commitment to seeking understanding. No need for labels or diagnoses only healing.
The big question perhaps is not “does it work?” but how could a dialogical approach work on a systems-wide level when our current mental health care systems are somewhat calcified and overly reliant on replication, rules, quantitative measures, and efficiency in “processing” human beings. The 15-minute psychiatric med checks mirror the 15-minute primary care visits (actually, I believe the average face time with a primary care physician is 7 to 10 minutes).
Thank you for inviting us to explore this approach more deeply…
Report comment
Thank Jennifer, I am eager to learn more of Insight Dialogue.you
Beautifully describe a truth that emerges when two people
share their humanity or Ubuntu as it is called in South Africa.
Report comment
Have just finished reading this article, Dialogical Recovery from Monological Medicine. I must say I find myself a bit confused. On the one hand, I find myself really grateful to hear dialogic concepts being so heartily endorsed in connection with the peer mental health movement by a leader of Dan’s status and stature. There couldn’t be a more critical issue, or a more fitting leader to advance these concepts.
At the same time, I must say that I feel terribly saddened to see no mention of Shery Mead in his article. Shery is perhaps the pre-eminent pioneer of peer-based dialogic approaches to mental health and community-building not only in the USA, but also worldwide. Shery started working on this approach long nearly 2 decades ago, before it was barely even a blip on the radar of anyone else in the peer mental health movement. Moreover, Shery single-handedly developed, implemented and popularized the dialogic, community-building approach that is now so prevalent worldwide in peer mental health circles.
Quite possibly, there is something I’m overlooking. But, at this point, I have made my best effort, and still don’t see much that’s new in what’s being advanced in this current article that Shery hasn’t already been talking about for over a decade. I would welcome information or insights that others may have to shed light on what, to me, feels like a painful omission of the contributions of one of our most dedicated and long-standing leaders in the peer mental health movement.
Thank you for your consideration of my comments
Report comment
Neglected to mention that Shery’s approach is called “Intentional Peer Support” (IPS). Also wanted to credit New Zealand disability rights activist Chris Hansen with playing a critical role, with Shery, in refining the theory and practice of Intentional Peer Support and in popularizing the model with a world-wide audience.
Report comment
Sarah, I greatly admire the work of Shery Mead and Chris Hansen
and others who teach Intentional Peer Support. It is dialogical
and reinforces the truth within this approach. I like to bring together
The best that our movement creates and show how they resonate
With the human spirit.
Report comment
It is about time the whole world saw that all we need is to go back to treating a neighbor like a neighbor.
Report comment
Thank you again Dan for your great contribution to evolving a a vision of health and recovery based on principles of human caring and compassion.
How different it feels to be in a dialog about one’s needs when we are in distress or madness than to be on the recieving end of a monologue! The contrasts between PACT and Pace highlight this clearly too.
Bless you for your vocation as doctor and comradeship as peer.
Report comment
Mike, Thank you for your support. I feel that human caring and compassion are the basis of my work and yours. Though the forces of greed and coercion are strong, I agree with Martin Luther King, Jr., who said he could see over history that the arc of humanity was moving towards justice. We need to keep strengthening the bonds between those of us who can see the life force grow within our dialogue of caring and compassion. Then we can truly weave a bright tapestry to embrace our children and grandchildren. I believe, that within each human being, there is a need and a wish to grow a fuller life. This is the part that I try to resonate with, even in those whose fear constrains their life and causes them to constrain those close to them.
Report comment
Dan, your words move me and make me feel hopeful our grandchildren will have a more just and compassionate world to thrive in.
Your inspired additions to the emerging Mother Bear Community Action Network’s mission statement, are helping to pave the way for a better future now for children and families.
Report comment
This conversation helps clarify a connection between dialogue and
empowerment which is a crucial element in recovery. In my experience
much of emotional distress comes from the trauma of feeling your voice and very
existence do not matter. If contact with most people reinforces this
nausea of not being, then the safest place to be is deep inside oneself
which appears as monologue. It seems then the most crucial element
in open dialogue is the relationships which empower through creating
a dialogical space between the person in distress and their social network.
Intuitively our movement based on lived experience, has been facilitating
individual and collective recovery by strengthening our voice. Emotional
CPR (www.emotional-cpr.org) is based on these principles. I will develop
these ideas further in my next entry.
Report comment