
Overtreatment with drugs kills many people, and the death rate is increasing. It is therefore strange that we have allowed this long-lasting drug pandemic to continue, and even more so because most of the drug deaths are easily preventable.
In 2013, I estimated that our prescription drugs are the third leading cause of death after heart disease and cancer,1 and in 2015, that psychiatric drugs alone are also the third leading cause of death.2 However, in USA, it is commonly stated that our drugs are “only” the fourth leading cause of death.3,4 This estimate was derived from a 1998 meta-analysis of 39 US studies where monitors recorded all adverse drug reactions that occurred while the patients were in hospital, or which were the reason for hospital admission.5
This methodology clearly underestimates drug deaths. Most people who are killed by their drugs die outside hospitals, and the time people spent in hospitals was only 11 days on average in the meta-analysis.5 Moreover, the meta-analysis only included patients who died from drugs that were properly prescribed, not those who died as a result of errors in drug administration, noncompliance, overdose, or drug abuse, and not deaths where the adverse drug reaction was only possible.5
Many people die because of errors, e.g. simultaneous use of contraindicated drugs, and many possible drug deaths are real. Moreover, most of the included studies are very old, the median publication year being 1973, and drug deaths have increased dramatically the last 50 years. As an example, 37,309 drug deaths were reported to the FDA in 2006 and 123,927 ten years later, which is 3.3 times as many.6
In hospital records and coroners’ reports, deaths linked to prescription drugs are often considered to be from natural or unknown causes. This misconception is particularly common for deaths caused by psychiatric drugs.2,7 Even when young patients with schizophrenia suddenly drop dead, it is called a natural death. But it is not natural to die young and it is well known that neuroleptics can cause lethal heart arrythmias.
Many people die from the drugs they take without raising any suspicion that it could be an adverse drug effect. Depression drugs kill many people, mainly among the elderly, because they can cause orthostatic hypotension, sedation, confusion, and dizziness. The drugs double the risk of falls and hip fractures in a dose-dependent manner,8,9 and within one year after a hip fracture, about one-fifth of the patients will have died. As elderly people often fall anyway, it is not possible to know if such deaths are drug deaths.
Another example of unrecognised drug deaths is provided by non-steroidal anti-inflammatory drugs (NSAIDs). They have killed hundreds of thousands of people,1 mainly through heart attacks and bleeding stomach ulcers, but these deaths are unlikely to be coded as adverse drug reactions as such deaths also occur in patients who do not take the drugs.
The 1998 US meta-analysis estimated that 106,000 patients die every year in hospital because of adverse drug effects (a 0.32% death rate).5 A carefully done Norwegian study examined 732 deaths that occurred in a two-year period ending in 1995 at a department of internal medicine, and it found that there were 9.5 drug deaths per 1000 patients (a 1% death rate).10 This is a much more reliable estimate, as drug deaths have increased markedly. If we apply this estimate to USA, we get 315,000 annual drug deaths in hospitals. A review of four newer studies, from 2008 to 2011, estimated that there were over 400,000 drug deaths in US hospitals.11
Drug usage is now so common that newborns in 2019 could be expected to take prescription drugs for roughly half their lives in USA.12 Moreover, polypharmacy has been increasing.12
How many people are killed by psychiatric drugs?
If we want to estimate the death toll of psychiatric drugs, the most reliable evidence we have are the placebo-controlled randomised trials. But we need to consider their limitations.
First, they usually run for only a few weeks even though most patients take the drugs for many years.13,14
Second, polypharmacy is common in psychiatry, and this increases the risk of dying. As an example, the Danish Board of Health has warned that adding a benzodiazepine to a neuroleptic increases mortality by 50-65%.15
Third, half of all deaths are missing in published trial reports.16 For dementia, published data show that for every 100 people treated with a newer neuroleptic for ten weeks, one patient is killed.17 This is an extremely high death rate for a drug, but FDA data on the same trials show it is double as high, namely two patients killed per 100 after ten weeks.18 And if we extend the observation period, the death toll becomes even higher. A Finnish study of 70,718 community-dwellers newly diagnosed with Alzheimer’s disease reported that neuroleptics kill 4-5 people per 100 annually compared to patients who were not treated.19
Fourth, the design of psychiatric drug trials is biased. In almost all cases, patients were already in treatment before they entered the trial,2,7 and some of those randomised to placebo will therefore experience withdrawal effects that will increase their risk of dying, e.g. because of akathisia. It is not possible to use the placebo-controlled trials in schizophrenia to estimate the effect of neuroleptics on mortality because of the drug withdrawal design. The suicide rate in these unethical trials was 2-5 times higher than the norm.20,21 One in every 145 patients who entered the trials of risperidone, olanzapine, quetiapine and sertindole died, but none of these deaths were mentioned in the scientific literature, and the FDA didn’t require them to be mentioned.
Fifth, events after the trial is stopped are ignored. In Pfizer’s trials of sertraline in adults, the risk ratio for suicides and suicide attempts was 0.52 when the follow-up was only 24 hours, but 1.47 when the follow-up was 30 days, i.e. an increase in suicidal events.22 And when researchers reanalysed the FDA trial data on depression drugs and included harms occurring during follow-up, they found that the drugs double the number of suicides in adults compared to placebo.23,24
In 2013, I estimated that, in people aged 65 and above, neuroleptics, benzodiazepines or similar, and depression drugs kill 209,000 people annually in the United States.2 I used rather conservative estimates, however, and usage data from Denmark, which are far lower than those in USA. I have therefore updated the analysis based on US usage data, again focusing on older age groups.
For neuroleptics, I used the estimate of 2% mortality from the FDA data.18
For benzodiazepines and similar drugs, a matched cohort study showed that the drugs doubled the death rate, although the average age of the patients was only 55.25 The excess death rate was about 1% per year. In another large, matched cohort study, the appendix to the study report shows that hypnotics quadrupled the death rate (hazard ratio 4.5).26 These authors estimated that sleeping pills kill between 320,000 and 507,000 Americans every year.26 A reasonable estimate of the annual death rate would therefore be 2%.
For SSRIs, a UK cohort study of 60,746 depressed patients older than 65 showed that they led to falls and that the drugs kill 3.6% of patients treated for one year.27 The study was done very well, e.g. the patients were their own control in one of the analyses, which is a good way to remove the effect of confounders. But the death rate is surprisingly high.
Another cohort study, of 136,293 American postmenopausal women (age 50-79) participating in the Women’s Health Initiative study, found that depression drugs were associated with a 32% increase in all-cause mortality after adjustment for confounding factors, which corresponded to 0.5% of women killed by SSRIs when treated for one year.28 The death rate was very likely underestimated. The authors warned that their results should be interpreted with great caution, as the way exposure to antidepressant drugs was ascertained carried a high risk of misclassification, which would make it more difficult to find an increase in mortality. Further, the patients were much younger than in the UK study, and the death rate increased markedly with age and was 1.4% for those aged 70-79. Finally, the exposed and unexposed women were different for many important risk factors for early death, whereas the people in the UK cohort were their own control.
For these reasons, I decided to use the average of the two estimates, a 2% annual death rate.
These are my results for USA for these three drug groups for people at least 65 years of age (58.2 million; usage is in outpatients only):29-32
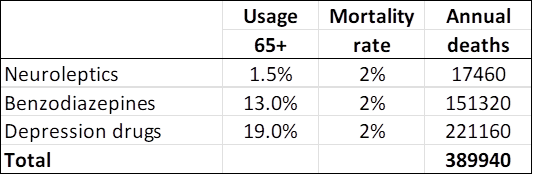
A limitation in these estimates is that you can only die once, and many people receive polypharmacy. It is not clear how we should adjust for this. In the UK cohort study of depressed patients, 9% also took neuroleptics, and 24% took hypnotics/anxiolytics.27
On the other hand, the data on death rates come from studies where many patients were also on several psychiatric drugs in the comparison group, so this is not likely to be a major limitation considering also that polypharmacy increases mortality beyond what the individual drugs cause.
Statistics from the Centers for Disease Control and Prevention list these four top causes of death:33
Heart disease: 695,547
Cancer: 605,213
COVID-19: 416,893
Accidents: 224,935
COVID-19 deaths are rapidly declining, and many of such deaths are not caused by the virus but merely occurred in people who tested positive for it because the WHO advised that all deaths in people who tested positive should be called COVID deaths.
Young people have much smaller deaths risk than the elderly, as they rarely fall and break their hip, which is why I have focused on the elderly. I have tried to be conservative. My estimate misses many drug deaths in those younger than 65 years; it only included three classes of psychiatric drugs; and it did not include hospital deaths.
I therefore do not doubt that psychiatric drugs are the third leading cause of death after heart disease and cancer.
Other drug groups and hospital deaths
Analgesics are also major killers. In USA, about 70,000 people were killed in 2021 by an overdose of a synthetic opioid.34
The usage of NSAIDs is also high. In USA, 26% of adults use them regularly, 16% of which get them without a prescription35 (mostly ibuprofen and diclofenac).36
As there seems to be no major differences between the drugs in their capacity to cause thromboses,37 we may use data for rofecoxib. Merck and Pfizer underreported thrombotic events in their trials of rofecoxib and celecoxib, respectively, to such an extent that it constituted fraud,1 but in one trial, of colorectal adenomas, Merck assessed thrombotic events. There were 1.5 more cases of myocardial infarction, sudden cardiac death or stroke on rofecoxib than on placebo per 100 patients treated.38 About 10% of the thromboses are fatal, but heart attacks are rare in young people. Restricting the analysis to those aged at least 65, we get 87,300 annual deaths.
It has been estimated that 3700 deaths occur each year in the UK due to peptic ulcer complications in NSAID users,39 corresponding to about 20,000 deaths each year in USA. Thus, the total estimate of NSAID deaths is about 107,000.
If we add the estimates above, 315,000 hospital deaths, 390,000 psychiatric drug deaths, 70,000 synthetic opioid deaths, and 107,000 NSAID deaths, we get 882,000 drug deaths in the United States annually.
Many other commonly used drugs than those mentioned above can cause dizziness and falls, e.g. anticholinergic drugs against urinary incontinence and dementia drugs, which are used by 1% and 0.5% of the Danish population, respectively, even though they do not have any clinically relevant effects.1,2
It is difficult to know what the exact death toll of our drugs is, but there can be no doubt that they are the leading cause of death. And the death toll would be much higher if we included people below 65 years of age. Moreover, from the official number of deaths from heart disease, we would need to subtract those caused by NSAIDs, and from accidents, deaths by falls caused by psychiatric drugs and many other drugs.
If such a hugely lethal pandemic had been caused by a microorganism, we would have done everything we could to get it under control. The tragedy is that we could easily get our drug pandemic under control, but when our politicians act, they usually make matters worse. They have been so heavily lobbied by the drug industry that drug regulation has become much more permissive than it was in the past.40
Most of the drug deaths are preventable,41 above all because most of the patients who died didn’t need the drug that killed them. In placebo-controlled trials, the effect of neuroleptics and depression drugs has been considerably below the least clinically relevant effect, also for very severe depression.2,7 And, despite their name, non-steroidal, anti-inflammatory drugs, NSAIDs do not have anti-inflammatory effects,1,42 and systematic reviews have shown that their analgesic effect is similar to that of paracetamol (acetaminophen). Yet, most patients with pain are recommended to take both paracetamol and an NSAID over the counter. This will not increase the effect, only the risk of dying.
Most tragically, leading psychiatrists all over the world do not realise how ineffective and dangerous their drugs are. A US psychiatrist, Roy Perlis, professor at Harvard, argued in April 2024, that depression pills should be sold over the counter because they are “safe and effective.”43 They are highly unsafe and ineffective. Perlis also claimed that depression drugs do not increase the risk of suicide in people older than 25, which is also wrong. They double suicides in adults.23,24
Perlis wrote that “Some still question the biological basis of this disorder, despite the identification of more than 100 genes that increase depression risk and neuroimaging studies showing differences in the brains of people with depression.” Both these claims are plain wrong. Genetic association studies have come up empty-handed and so have brain imaging studies, which are generally highly flawed.44 People are depressed because they live depressing lives, not because of some brain disorder.
References
1 Gøtzsche PC. Deadly medicines and organised crime: How big pharma has corrupted health care. London: Radcliffe Publishing; 2013.
2 Gøtzsche PC. Deadly psychiatry and organised denial. Copenhagen: People’s Press; 2015.
3 Schroeder MO. Death by prescription: By one estimate, taking prescribed medications is the fourth leading cause of death among Americans. US News 2016; Sept 27.
4 Light DW, Lexchin J, Darrow JJ. Institutional corruption of pharmaceuticals and the myth of safe and effective drugs. J Law Med Ethics 2013;41:590-600.
5 Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA 1998;279:1200–5.
6 FAERS Reporting by Patient Outcomes by Year. FDA 2015;Nov 10.
7 Gøtzsche PC. Mental health survival kit and withdrawal from psychiatric drugs. Ann Arbor: L H Press; 2022.
8 Hubbard R, Farrington P, Smith C, et al. Exposure to tricyclic and selective serotonin reuptake inhibitor antidepressants and the risk of hip fracture. Am J Epidemiol 2003;158:77-84.
9 Thapa PB, Gideon P, Cost TW, et al. Antidepressants and the risk of falls among nursing home residents. N Engl J Med 1998;339:875-82.
10 Ebbesen J, Buajordet I, Erikssen J, et al. Drug-related deaths in a department of internal medicine. Arch Intern Med 2001;161:2317–23.
11 James JTA. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf 2013;9:122-8.
12 Ho JY. Life course patterns of prescription drug use in the United States. Demography 2023;60:1549-79.
13 Gøtzsche PC. Long-term use of antipsychotics and antidepressants is not evidence-based. Int J Risk Saf Med 2020;31:37-42.
14 Gøtzsche PC. Long-term use of benzodiazepines, stimulants and lithium is not evidence-based. Clin Neuropsychiatry 2020;17:281-3.
15 Forbruget af antipsykotika blandt 18-64 årige patienter, med skizofreni, mani eller bipolar affektiv sindslidelse. København: Sundhedsstyrelsen; 2006.
16 Hughes S, Cohen D, Jaggi R. Differences in reporting serious adverse events in industry sponsored clinical trial registries and journal articles on antidepressant and antipsychotic drugs: a cross-sectional study. BMJ Open 2014;4:e005535.
17 Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA 2005;294:1934–43.
18 FDA package insert for Risperdal (risperidone). Accessed 30 May 2022.
19 Koponen M, Taipale H, Lavikainen P, et al. Risk of mortality associated with antipsychotic monotherapy and polypharmacy among community-dwelling persons with Alzheimer’s disease. J Alzheimers Dis 2017;56:107-18.
20 Whitaker R. Lure of riches fuels testing. Boston Globe 1998;Nov 17.
21 Whitaker R. Mad in America: bad science, bad medicine, and the enduring mistreatment of the mentally ill. Cambridge: Perseus Books Group; 2002:page 269.
22 Vanderburg DG, Batzar E, Fogel I, et al. A pooled analysis of suicidality in double-blind, placebo-controlled studies of sertraline in adults. J Clin Psychiatry 2009;70:674-83.
23 Hengartner MP, Plöderl M. Newer-generation antidepressants and suicide risk in randomized controlled trials: a re-analysis of the FDA database. Psychother Psychosom 2019;88:247-8.
24 Hengartner MP, Plöderl M. Reply to the Letter to the Editor: “Newer-Generation Antidepressants and Suicide Risk: Thoughts on Hengartner and Plöderl’s ReAnalysis.” Psychother Psychosom 2019;88:373-4.
25 Weich S, Pearce HL, Croft P, et al. Effect of anxiolytic and hypnotic drug prescriptions on mortality hazards: retrospective cohort study. BMJ 2014;348:g1996.
26 Kripke DF, Langer RD, Kline LE. Hypnotics’ association with mortality or cancer: a matched cohort study. BMJ Open 2012;2:e000850.
27 Coupland C, Dhiman P, Morriss R, et al. Antidepressant use and risk of adverse outcomes in older people: population based cohort study. BMJ 2011;343:d4551.
28 Smoller JW, Allison M, Cochrane BB, et al. Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women’s Health Initiative study. Arch Intern Med 2009;169:2128-39.
29 O’Neill A. Age distribution in the United States from 2012 to 2022. Statista 2024;Jan 25.
30 Olfson M, King M, Schoenbaum M. Antipsychotic treatment of adults in the United States. Psychiatrist.com 2015;Oct 21.
31 Maust DT, Lin LA, Blow FC. Benzodiazepine use and misuse among adults in the United States. Psychiatr Serv 2019;70:97-106.
32 Brody DJ, Gu Q. Antidepressant use among adults: United States, 2015-2018. CDC 2020;Sept.
33 Centers for Disease Control and Prevention. Leading Causes of Death. 2024;Jan 17.
34 Drug overdose deaths. Centers for Disease Control and Prevention 2023;Aug 22.
35 Davis JS, Lee HY, Kim J, et al. Use of non-steroidal anti-inflammatory drugs in US adults: changes over time and by demographic. Open Heart 2017;4:e000550.
36 Conaghan PG. A turbulent decade for NSAIDs: update on current concepts of classification, epidemiology, comparative efficacy, and toxicity. Rheumatol Int 2012;32:1491-502.
37 Bally M, Dendukuri N, Rich B, et al. Risk of acute myocardial infarction with NSAIDs in real world use: bayesian meta-analysis of individual patient data. BMJ 2017;357:j1909.
38 Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005;352:1092-102.
39 Blower AL, Brooks A, Fenn GC, et al. Emergency admissions for upper gastrointestinal disease and their relation to NSAID use. Aliment Pharmacol Ther 1997;11:283–91.
40 Davis C, Lexchin J, Jefferson T, Gøtzsche P, McKee M. “Adaptive pathways” to drug authorisation: adapting to industry? BMJ 2016;354:i4437.
41 van der Hooft CS, Sturkenboom MC, van Grootheest K, et al. Adverse drug reaction-related hospitalisations: a nationwide study in The Netherlands. Drug Saf 2006;29:161-8.
42 Gøtzsche PC. Big marketing hoax: Non-steroidal, anti-inflammatory drugs (NSAIDs) are not anti-inflammatory. Copenhagen: Institute for Scientific Freedom 2022;Nov 10.
43 Perlis R. The time has come for over-the-counter antidepressants. Stat News 2024;April 8.
44 Gøtzsche PC. Critical psychiatry textbook. Copenhagen: Institute for Scientific Freedom; 2022. Freely available.











A much needed article and I just wanted to mention Dr. Peter Breggin, author of “Toxic Psychiatry” and “Your Drug May Be Your Problem”. He has done excellent work on this issue for years.
Report comment
Human research on the toxicity of psychotropic medications is either imprecise (observational studies) or unethical (clinical trials).
What about animal testing? It allows accurate results to be produced in an ethical manner, regarding the chronic use of psychotropic medications.
Report comment
Animal testing is disgusting.
Homeopathy works wonders. It actually cures the causes of depression, psychosis, anxiety and all the rest.
The WHO says homeopathy is the second most widely used system of medicine in the world. It’s amazing, so very different from Western medicine or even herbalism.
And testing is done on fairly healthy humans, not on puppies or other animals.
-Linda, author of “Goodbye, Quacks – Hello, Homeopathy!”
Report comment
Good article and ending ‘People are depressed because they lead depressing lives’. People may also be depressed because of thought patterns, relations with others or memories of childhood. Ultimately it is the life they lead.
Medical practicioners offering medication because they themselves will profit from giving out a certain drug is no more advanced than a tribal Witch Doctor dispensing a potion they have concocted.
You are right when you see that Doctors do not realise the effects of the drugs they give out. Maybe Medical schools should make students/junior Dr.’s take the drugs they will be prescribing !!
Report comment
Interesting
Report comment
what’s the first?
Report comment
Medication associated and as true cause of death- is ignored side effect, when a drug company sells a drug.
As seen in drug withdrawal by manufacturer, most antidiabetic drugs causes more deaths. This includes insulins- one brand of insulin is withdrawn from market recently. As a physician I have observed many deaths due to hypoglycemia in insulin users- especially elderly diabetics. All such drugs cause fluid retention and congestive heart failure as well.
NSAIDs causes renal failure and patients end up on dialysis and death.
Report comment
There’s no doubt Americans are over medicated and that drugs cause deaths, with psychiatric drugs being among the worst. But there’s no research that proves drugs are the leading cause of death. That’s because a person’s death may have numerous causes with the drug being only one factor In addition, a toxic drug may eventually kill someone, but the patient may have succumbed to their illness sooner if they hadn’t been taking the medication. I’m not convinced, for example, that statins, blood pressure medications or diabetes medications are completely safe, but they’re supposed to extend lifespans. Maybe they do or maybe they don’t, but that’s the argument for them.
One other point, people, such as those with dementia or a terminal illness, may be medicated to keep them comfortable even if the drug may shorten their lifespan.
Report comment
Fair.
Report comment
My life was destroyed by a drug that gave me PSSD (permanent side effects) and now i want to die everyday.
Report comment
Great article, Doc. Unethically designed trials are rife within all fields of medicine. The regulatory agencies not only permit them, but enable and endorse their findings as well. Publication standards are a joke, and the world’s health authorities have lost legitimacy. Dementia research and cancer therapies stand out as particularly egregious. To say we have lost the way is a severe understatement; the system is beyond reproach. May god help us all or may we join hands and stand up to the corrupt system of profit driven healthcare.
Report comment
I agree
Report comment
I would like to see the meta-analysis on the studies done to confirm this statement. At the very least, it is entirely too broad a brush and vague. Leading cause of death in what cohort? If you look at the CDC and NHI statistics this is not included. Is it a conspiracy?
Report comment
When a VHA psychologist two weeks ago asked if I wanted “mental health” care,
I replied, “No,” while waving off the questioner with my hands.
I then said, “I can’t tolerate any more poly-pharmacy, and I will not go back to my (chemical ) abusers.”
In psychiatric wards, I was forced to take multiple medications, and I felt I was being pharmaceutically raped because when I asked, “what is the drug you’re giving me, ” the reply was, “It’s what the doctor ordered.” I replied, “I know that, but what is the name and type of this drug?” The orderly replied, “You won’t get out of here unless you take it.” -PTSD flashback
It’s one thing to be sexually raped while serving in the Navy, but it’s unacceptable to be forced (raped) to take a drug when a veteran has a documented history of military sexual trauma.
All my doctors were ignorant that they were causing my PTSD to worsen. Unfortunately, too many psychiatrists are drug pushers.
-JL Reoch
Report comment
I had insomnia so badly and for so long (despite all kinds of therapy etc.) that I wanted to kill myself. Drugs saved my life, as they enabled me to sleep and feel 100% better. Maybe I will die sooner, but I would already be dead without them.
Report comment
Are you willing to share with us what drugs you were prescribed that saved you by successfully treating your insomnia? I was recently diagnosed with hyperthyroidism after being diagnosed with insomnia and hypertension. I currently don’t take any psychiatric medications.
I appreciate your valuable information.
Thank you.
Report comment
Hi Jane,
it’s best to go have a sleep study. Sleep is complicated and a lot of things can go wrong, requiring a lot of different treatments. So what’s needed for one person is not necessarily what’s needed for the next.
Good luck,
BC
Report comment
I think cancer drugs cause death. you did not include chemotherapy drugs in your genius study.
i am sure, untreated, cancer patients would live longer, at least by your perverted logic
Report comment
Chemotherapy is covered by Peter C. Götzsche in this article: https://www.scientificfreedom.dk/2023/02/04/should-i-get-chemotherapy-for-cancer-probably-not/
Report comment
Everything he said here was fact based, and well cited. Your inability to deal with facts is what perverted logic is all about.
Report comment
Interesting
Report comment
As I read this article, I thought about the aging populace around me (over 50’s).
Was that thrombosis from an NSAID? How would we ever know?
When the psychiatry scales fell from my eyes, I thought about 20-30% of the population as drugged, and when they complained of heart, digestion, fatigue, and – yes, still mood – issues – I couldn’t help but “blame the drug.”
But it’s not just this one and that one. In drugs, I think of it as exponential when you combine them. 1+1=10. So when you’re on 6. Egads.
Report comment
I remember when a Dr. would consult a pharmacist before he wrote a prescription lots of times.
The pharmacist might make the pills right there at the drug store. Now instead of valuable medical training a lot of it is replaced with Dr”s. learning about medications or ‘pills’. They use a cookie cutter chart for all.
Not surprising when one considers that all the major hospitals and HMO’s and all the pharmaceutical companies are really owned by BlackRock.
This country -and the world-deserves to have drugs made by a non profit research and drug making company that only get rewarded financially for cures. They could have the brightest from good Universities helping with the research.
Right now it profits drug companies in no way to find cures-just the opposite. BioTech, Moderna, Pfizer makes $66.000 a minute on covid vaccines alone.
Isnt it food for thought that a vaccine that takes 5-15 years to make was made in 5 months?
Report comment
The Medical Mafia would not prevail without The Media Mafia covering up for it. Thank you for your beautiful heart for humanity, and for sharing your research.
Report comment
“Most tragically, leading psychiatrists all over the world do not realise how ineffective and dangerous their drugs are.”
Psychiatry needs to be banned from allopathic medicine.
Report comment
I suffered from major depression for 40 years, after which I engineered my own remission and became a CPhT in Pharmacy.
Given these experiences, I offer a few observations:
1) My depression was not caused by having a terrible life, it existed despite wonderful circumstances. It did make it difficult for me to enjoy the wonderful aspects. I find this to be a common observation amongst other depressed individuals I have known.
2) The concept of epigenetics is not addressed, but it is crucial. Combine genetics with
epigenetic influences
alterations of the microbiome
food sensitivities
environmental irritants
issues with the lack of nutrients, vitamins and minerals or the inability to used them properly -particularly b-12, folate and b-6, and
any issues with the cytochrome p-450 enzymatic pathways
and you create a recipe for depression.
3) Neuro-metobolic approaches recognizing the role that dietary approaches can play in reducing schizophrenia are being piloted in residential settings across the country. In addition research on circadian rhythms and on the RCCX genetic cluster show promise
I’m no fan of antidepressants but I am no fan of a one-dimentional approach confusing situational depression with endogenous depression.
Report comment
Lori, your insight into the genesis of depression that many can experience should be explored by researchers, because their continuous quest to find the next chemical elixir for the biomedical industry to manufacture for people to consume is a waste of taxpayer monies.
Personally, I would like to see a decrease in the escalating use of depot shots of antipsychotics because antidepressants could become the next wave in injections.
Thank you Lori!
Report comment
Excellent synopsis of a widespread public health crisis. Indeed if all the numbers could be aggregated, it would seem likely that pharmaceutical drugs are likely the leading cause of deaths in the US.
Report comment