
![]()
In a couple of weeks – on 20 March – it will be five years since my beautiful son killed himself. After fighting for justice and accountability and for a change in the way we conceptualise and approach suicide prevention for the first two years after his death, I came to understand that rather than doing this as an individual I needed to build a worldwide network of the suicide bereaved to accomplish the task – to build a group of people who wanted their children and other family members to be remembered as pioneers in suicide prevention, not just people who killed themselves.
In August 2010, my friend and fellow ‘suicide mum’ Deb Williams and I established CASPER – Community Action on Suicide Prevention Education & Research. CASPER’s goals are to provide peer support to families bereaved by suicide, to educate politicians and opinion leaders on suicide and its prevention and to support families and communities to reclaim suicide prevention from medical professionals and governments.
CASPER is a registered charity and was initially funded by the sale of my home and other assets and run on the voluntary labour of people who had lost loved ones to suicide. We had almost no money but refused to let that get in the way of doing what needed to be done. When you know a child may die if you don’t do something, you find a way of doing it. It really is as simple as that. I smile when I think of the things we did – getting free paint test pots and painting Deb’s old horse float with suicide prevention messages and driving around the streets to advertise our community education sessions, driving around the country in an unregistered vehicle with a tent in the back in the middle of winter running free workshops and building our own website from scratch using instructions from google.
I graduated with an MBA five weeks after Toran died and during my study had developed an interest in models of partnership between business and non-profits which were profitable for business and grew the work of charities.
From the beginning, CASPER made a commitment to not seeking or accepting government funding. This was important to us for three reasons. First, as a watchdog on government it was critical we maintain financial independence. Second we wanted to work collaboratively with other organisations and being in competition with them for funding was not going to facilitate that. Third we wanted business and other sectors of the community to see themselves as integral to suicide prevention and step up to play their role rather than considering that paying their taxes was the beginning and end of their responsibility to suicide prevention.
My business degree and experience as a CEO positioned me well to both produce a good case to business leaders that investing in CASPER was a sound financial decision and to engage with business leaders. A leading New Zealand entrepreneur, Mike Pero who came on board as CASPER’s principal sponsor (at the time when my life savings and the proceeds of the sale of my house was gone and we had $386 in the bank!) was the key to getting us an audience with some of our countries top business people.
My argument was simple. Communities where suicide rates are low are good for business. Dead people and families and communities traumatised by suicide do not spend money on goods and services. Communities where business is flourishing produce jobs, higher incomes, good housing and funding for social services and recreational facilities. There is a synergy that creates a win/win situation for business and non-profits who work together. Strong healthy communities support business profitability while strong healthy businesses support communities that protect against suicide.
Suicide costs $1.6 billion against the NZ economy per annum. Two hundred thousand of this is in lost productivity. The financial benefits to business of reductions in suicide rates can be quantified and financial and other resources invested in effective suicide prevention programmes can presented to shareholders as profit generating activity. Last year, CASPER received $90,000 in donations from business and far more in the donation of goods and business services including marketing, legal services, accounting and auditing services and PR.
The media was another key CASPER target. Our goal was to establish ourselves as the ‘go to’ agency for the media on stories about suicide. Rather than all comment on the subject being provided by mental health providers and pharma influenced researchers, we wanted those who have lived experience of suicide to become visible and thinking from disciplines other than psychiatry to be presented to the public. Our blend of credible research and personal stories makes good copy and it is now rare for the New Zealand media to do a story on suicide without seeking comment from CASPER.
On the front line, CASPER began connecting with families and communities. We travelled the country running free community education sessions in which we presented data on suicide in NZ, evidence that our current mental health approach to suicide is not working and research on effective suicide prevention using sociological and indigenous models of suicide prevention. We told families and communities what we who have lost our children to suicide know now, that we wish we had known before they died.
We promoted the idea that individuals live in families and communities, not in mental health clinics or parliament buildings and that families and communities are therefore the natural location for suicide prevention. We challenged the notion that suicide is a complex medical issue that only doctors can understand.
Using research and experience we produced the following two models – one showing what causes suicide and the other what an environment that protects against suicide would look like.
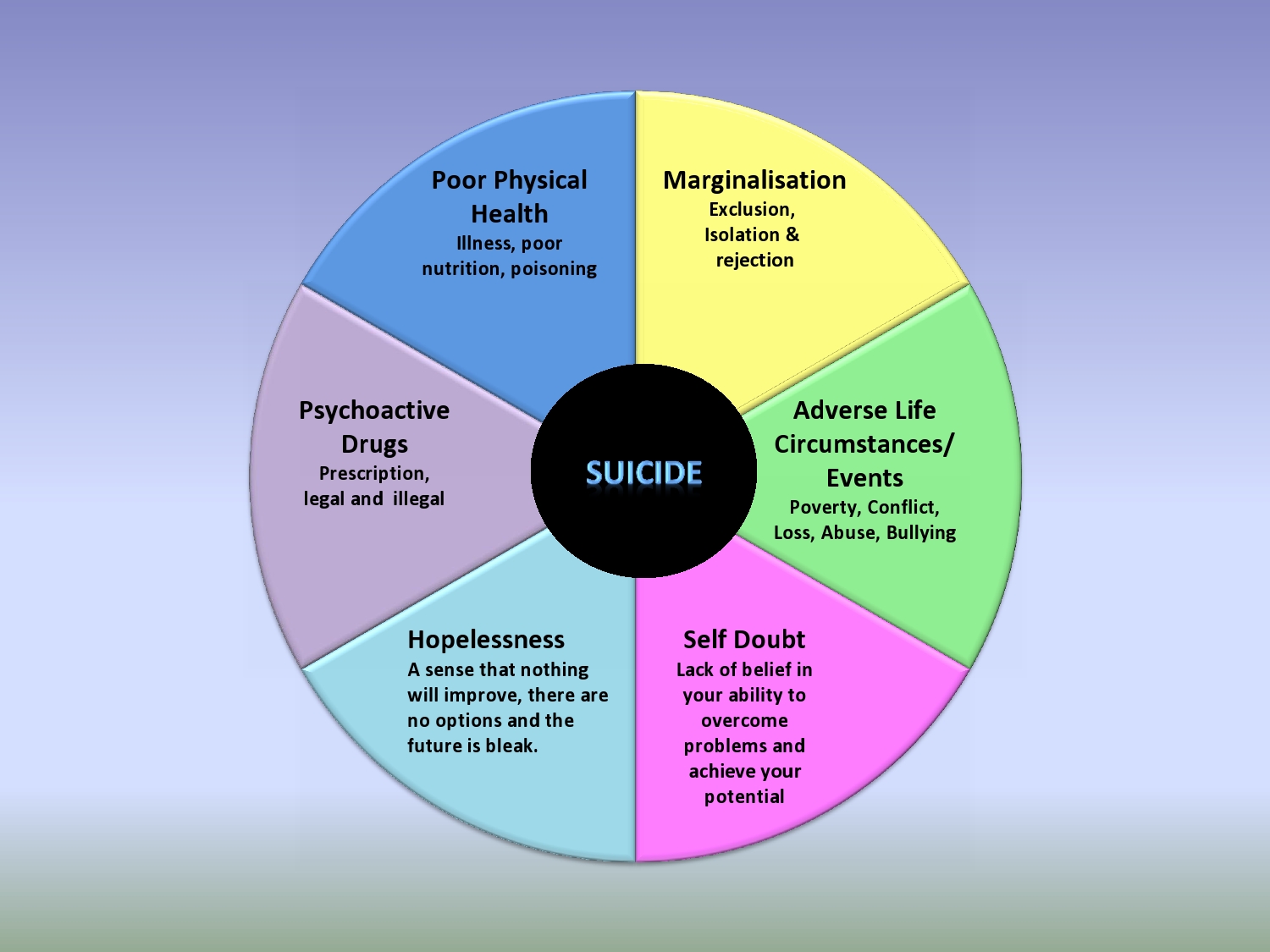
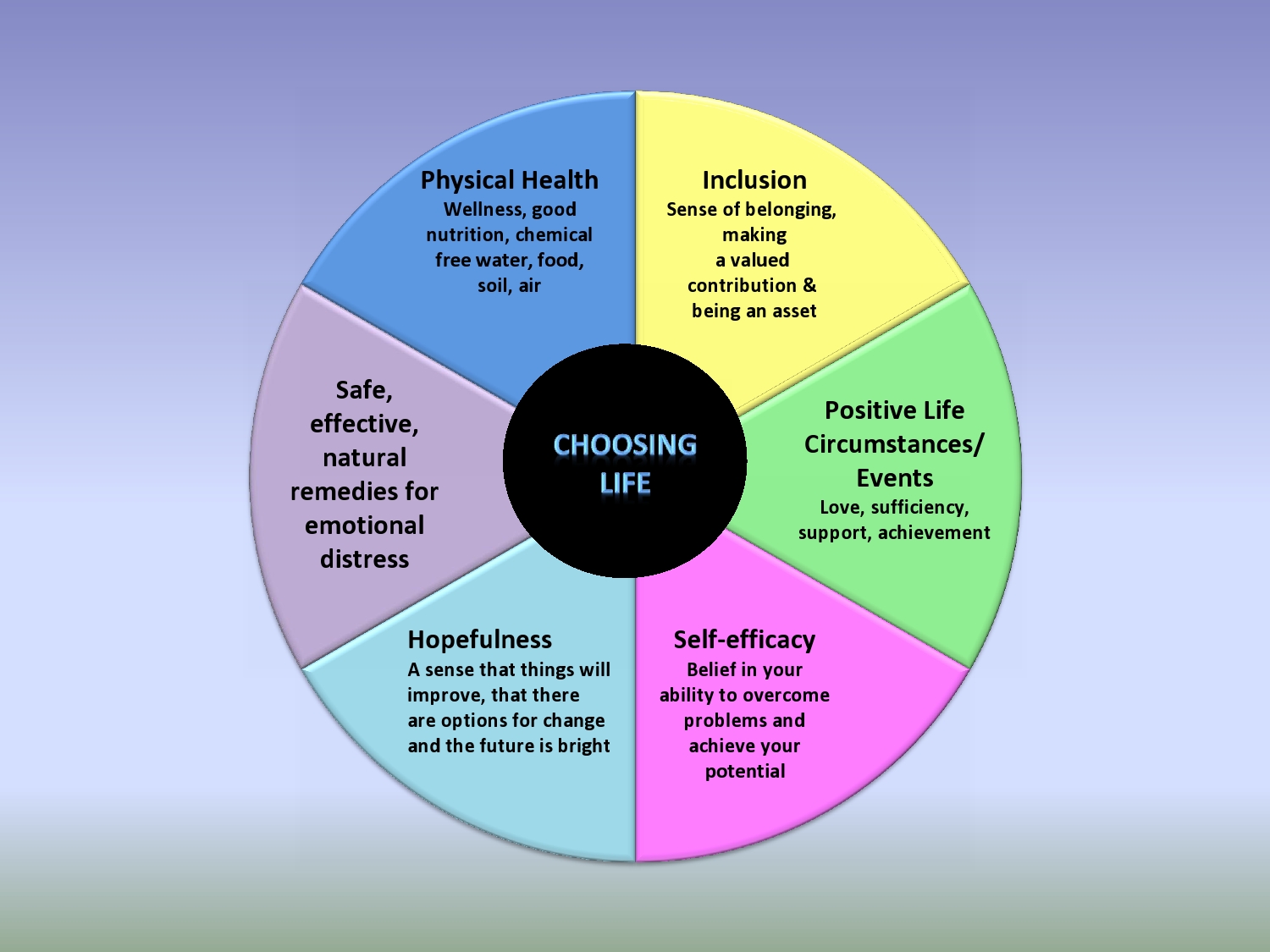
We worked with families and communities to audit themselves and identify where they needed to target their suicide prevention activities but also promoted the idea that suicide prevention, rather than being an activity or a programme is a way of living with and relating to others. It is about kindness, compassion and concern. It is about suspending judgement and offering support. It is about valuing everyone in your family and community and letting them know you value them. It is about making sure that everyone has a sense that they belong. Simple really and no white coat or prescription pad required.
And we were there for bereaved families. Not as counselors or service providers but as human beings who had shared the nightmare of suicide and would never expose them to judgement or rejection but be there in whatever capacity they needed. We match the families who contact us with families who have lost the same family member, whose dead loved one is a similar age, gender and ethnicity and who died by the same method. Our volunteers are trained to assist families in making decisions about autopsies and toxicology testing, to help deal with police investigations, to support families to prepare their cases for inquests and other enquiries and to provide practical help. Shopping, supervising childrens homework, making meals – whatever they need. We also of course provide an opportunity for people to become involved in suicide prevention – to give their loved one a legacy and to give themselves a reason to carry on living.
We also support families who have not experienced suicide loss but who are dealing with the suicidality of a loved one and are scared they may join our group.
We run a sibling network for children who have lost brothers, sisters or close friends to suicide.
We meet with politicians and government official and medical/mental health professionals but frankly, we don’t put a huge amount of effort into changing the views of these people. We believe our efforts are better directed to creating a model of suicide prevention that is so superior to the current model, that mental health clinics and antidepressants become obsolete. We believe that educating the community so that voters ask the right questions of their elected representatives and see suicide prevention as a key election issue is the path to change in government policy. We do however provide a voice for the 65,000 New Zealand families bereaved by suicide when legislation and policy are being developed that impact suicide and the families it affects.
We work hard. It is physically and emotionally draining work. But it is the job our children left us with and we are their mothers and fathers. This is how we continue to parent our children after their deaths and none of us can imagine doing anything else.
More information about CASPER is available on our website at www.casper.org.nz and our facebook page www.facebook.com/Caspercommunity














God speed! I’m certain you are saving lives and your son would be proud.
Report comment
Thank you. Many of the families we work with have said they do not believe their child would be alive today if it wasn’t for the support and information we provided. I just wish Toran was one of the ones who had survived.
Report comment
This is a wonderful enterprise and a model for other communities around the world. What especially struck me is Casper’s challenge to the notion that suicide is a complex medical issue that only doctors can understand. This segregated (medical ownership) thinking is true for so many areas of mental health. We need to bring the understanding down to how we live and relate to others, as you so wisely explain.
Report comment
I know! Discussions of ‘proximal’ and ‘distal’ factors, Axis 1 diagnoses and all the rest only serve to disempower families and communities and make them feel out of their depth. Interesting that a few decades ago when children being sad or scared or worried was seen as something to be addressed by families, our youth suicide rates were pretty low.
Report comment
I wish I would have had somebody to talk to when my son tried to commit suicide. It left all the family in a terrible turmoil and badly traumatised with no psychological help whatsoever.
On the other hand I owe a lot of gratitude to the police, the ambulance people and the A&E doctors and nurses who saved his life.The young psychiatrist who came and talked to me and gave him some medication to calm him down was a lovely person too.
Sadly things changed once he was out of danger. The authorities sectioned him, medicated him with antipsychotics against his will and caused him untold trauma. It took him years to get over the “help” he was metted out afterwards
Report comment
So sorry this happened to you and your son Alix. Hope your son is doing ok now. You can always contact us through our website or on [email protected] if you need any support or information of just someone to listen. We have families in countries other than NZ who can provide support too.
Report comment
I love the graphics! Makes too much sense. Have the “authorities” in the mental health system gotten upset with you yet for grouping their wonderful magic pills in there with the illegal drugs? I have to imagine there are some who would find your presentation extremely threatening.
Well done! I’m so impressed that you have the motivation and skills to accomplish so much with so little resources. Thanks for sharing your success, and I hope your organization continues to thrive.
— Steve
Report comment
Thanks Steve. We find our diagrams give families and communities a place to start when they are identifying things they can do to keep their members safe. Rather than being told to look out for depression and focusing on ‘fixing’ a person, they look at the environment and work on altering things that are giving rise to emotional distress. This gives people a set of concrete actions and a sense of control.
Definitely not popular with our Ministry of Health or mental health professionals although we are working with some sympathetic psychiatrists at the moment and have the support of some mental health professionals who see the lack of results with the current approach.
In the end, Toran didn’t leave me with the job of being popular so I don’t let it bother me too much.
Report comment
I can’t remember who said it, but I’m reminded of the quote, “Well-behaved women rarely make history.” I’m glad your not afraid to shake them up!
It is interesting that our biology and genetics is the one thing that we have almost no control over, and yet that’s where all the energy goes. The environment is what we DO control, and yet we act as if it has no impact. There are SO many things that can be done to help someone with feeling depressed, anxious, suicidal that have nothing to do with their bodies. And there are even physiological things we can do, like sleep, exercise, nutrition, etc. that have an impact. Drugs seem like the very last thing you would do when all else has failed. I find it hopeful that you are working effectively to change that focus to the things we actually can control!
— Steve
Report comment
Thanks Steve. I so agree with everything you say and only wish that what seems so obvious to us – work on those things amenable to the most change – was obvious to those who have set themselves up as the experts in suicide prevention. Changing brain chemistry might be lucrative but it is also lunacy!
Report comment
Wow.
Wow!
What wonderful work!
Duane
Report comment
Thanks Duane 🙂 Appreciate your enthusiasm as always.
Report comment
Maria,
I like the graphics so much I would like to use them. Are they copyrighted? Is there a process to use them as part of Suicide Prevention activities here in the States?
Thanks for all you do,
David
Report comment
Hi David. They are in the process of being copyrighted but we are happy for anyone to use them as long as CASPER is credited.
Report comment
That’s seems more than fair. Thanks Maria.
Report comment
Maria,
Great work! Wow… What you’ve developed is, far and away, the *best* Suicide Prevention program I’ve ever heard of (and, really – it should go without saying – *much* better than anything any government or government-assisted Suicide Prevention program shall ever provide.)
Medical-coercive psychiatry drove me to *very* seriously contemplating suicide, 25 years ago…
Never, prior to being introduced to psychiatry, had I ever been at all suicidal.
After I successfully got away from psychiatry and its ‘meds'(nearly 24 years ago), I *never* again felt suicidal.
Thus, nothing in the news, these days, is more disturbing, to me, than the many headlines indicating, that top leaders, in my government (here, in the U.S.) are increasingly dedicated to initiatives, which would ‘screen’ supposedly ‘at risk’ kids, in their schools – and send them into the ‘mental health’ system (which is, of course, dominated by medical-coercive psychiatry).
Your son is very well-honored by all that you’re doing, in his name.
More power to you and your organization!
Respectfully,
~Jonah
Report comment
Thanks so much Jonah. We don’t think for a minute we have all the answers, just that we are asking some of the right questions.
I find nothing more frustrating that seeing the media and policy makers unquestioningly accepting the claims of biological psychiatry. Having to read constantly that “90% of those who kill themselves have a mental disorder” from opinion leaders who have not even looked at the ridiculous research behind that claim, drives me mad.
Its interesting that in NZ,a very small percentage of those who kill themselves have been diagnosed with a mental disorder and the government’s own research shows a direct causal link between increased prescribing of antidepressants and increases in hospitalisation for serious suicide attempts but that government insists mental health ‘treatment’ is the answer to suicide prevention.
Thanks again for your kind words.
Maria
Report comment