
Editor’s Note: Over the next several months, Mad in America is publishing a serialized version of Peter Gøtzsche’s book, Critical Psychiatry Textbook. In this blog, he discusses the broadening of ADHD diagnostic criteria and the misleading and biased stimulant drug trials. Each Monday, a new section of the book is published, and all chapters are archived here.
The sections on ADHD in the textbooks can best be described as being seriously dishonest even though there was useful advice interspersed here and there.
An epidemic of ADHD diagnoses
As mentioned earlier, Allen Frances, chairman for the DSM-IV task force, noted that DSM-IV created a false epidemic of ADHD because the diagnostic criteria were too wide.116 The criteria for the ADHD diagnosis have changed with each iteration of the DSM, with each updated volume making it easier to make the diagnosis.57 Prevalence studies reflect this. The percentage of youth said to have ADHD increased from 3% with DSM-III, to 5% with DSM-IV and to 10% with DSM-5.
 The scientific literature is also dishonest, and it starts with the diagnosis. The American Psychiatric Association invented ADHD for DSM-III in 1980, and in 1998, the US National Institutes of Health (NIH) held a three-day consensus conference about its diagnosis and treatment.7:137,506
The scientific literature is also dishonest, and it starts with the diagnosis. The American Psychiatric Association invented ADHD for DSM-III in 1980, and in 1998, the US National Institutes of Health (NIH) held a three-day consensus conference about its diagnosis and treatment.7:137,506
At the meeting, the chairman asked a leading ADHD expert, Mark Vonnegut, what ADHD is, but although he talked for 2-3 minutes, he couldn’t explain it (see the YouTube video; starts after 4 minutes):507
“They cannot sit still … they are difficult and they aggravate their parents … the diagnosis is a mess but there is, there is, uhm, we all have a belief that we are dealing with a very serious core problem and that we have a diagnosis that allows us to communicate and gives us research, uhm, generates, uhm, sort of ideas for research, and I think, you know, we, uhm, I, I do, I think, part of the problem is that the profession keeps changing the diagnoses.”
Vonnegut’s ravings included that a teacher might say that a kid was two standard deviations different from the other kids in the classroom. I don’t think teachers argue this way.
Furthermore, 5% of us are by definition beyond two standard deviations from the average of everything that follows a normal distribution, but this doesn’t mean we are sick. If we measure people’s height, 5% are beyond two standard deviations from the average height, but we don’t invent some disorder for those 5% who are small or tall.
The consensus document stated that “The diagnosis of ADHD can be made reliably using well-tested diagnostic interview methods.”506 This was a huge lie, which Vonnegut contradicted: “The diagnosis is a mess.”
The document is embarrassing in many other ways. It uses 15 pages to tell us what ADHD is.506 It says that ADHD is one of the most common childhood “brain disorders” and that imaging studies have shown abnormalities in the brain.
ADHD is not a brain disorder and the brains of these children are not different from the brains of other children (see Chapter 2, Part Two).
The first page mentioned that “Inattention, hyperactivity, and impulsivity are the key behaviors of ADHD. It is normal for all children to be inattentive, hyperactive, or impulsive sometimes, but for children with ADHD, these behaviors are more severe and occur more often. To be diagnosed with the disorder, a child must have symptoms for 6 or more months and to a degree that is greater than other children of the same age.”
This is about as weak as it gets and cannot justify calling ADHD a brain disorder. There is a hilariously funny video that mocks this pseudoscience, which I strongly recommend.508
Many children qualify for the diagnosis because they are talented and therefore bored and cannot sit still in poorly disciplined classrooms, or because they have emotional problems generated by their parents.
I have lectured a lot for various audiences, both professionals and lay people, and I often expose people to the recommended test for adult ADHD (see below).7,509 Between one-third and one-half test positive. When I lectured for 27 therapists in 2022, 21 tested positive and 10 of these had a full house, which is six out of six criteria (only four positive replies to the questionnaire are needed for the diagnosis). I told them they were a great audience because some of the most interesting people I have ever met qualify for the ADHD diagnosis. They are dynamic and creative and have difficulty sitting still on their chairs pretending they are listening if the lecturer is dull.
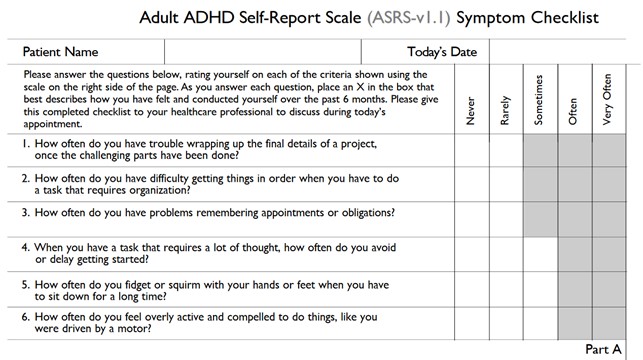
When I tested my wife, she also scored a full house. Once, when we discussed the silliness of psychiatric diagnoses, I subjected one of my daughters and her boyfriend to the test. My daughter scored five, like I did, and her laid-back boyfriend whom I would never suspect would be positive, scored four. So, we all got a bogus diagnosis that should land us on narcotics on prescription (amphetamine or amphetamine-like compounds).
My little exercise makes people realise how foolish and unscientific psychiatric diagnoses are. If you don’t test positive for adult ADHD, then try a few other diagnostic questionnaires for other disorders, and you are likely to get one.
I do not deny that there are people with symptoms labelled ADHD that we can help to get a better life, but the big mistake is that psychiatrists tend to equate help with drugs.
Psychoeducation and psychotherapy or drugs?
The advice in the textbooks was highly inconsistent, sometimes even within the same book. Some texts praised psychosocial interventions while others praised drugs, with loads of false claims.
The focus was predominantly on drugs. One textbook chapter demonstrated a total subjugation to the biological model.17:620 Its authors, both psychiatrists, noted that there is no evidence that cognitive behavioural therapy works on the fundamental “neurologically conditioned core symptoms” in adults with an ADHD diagnosis but that therapy should be offered in the form of general psychoeducation and training in practical and social skills as a supplement to medical treatment. They claimed that there are only a few large studies of psychotherapy and that they all have methodological problems. The reference for these remarks about psychotherapy was a whole book written by one of the two authors, psychiatrist Marianne Geoffroy.
But there is actually a review of 14 trials of psychotherapy, and it showed an effect on core symptoms, in contrast to the textbook statement.510
When I published my first psychiatry book in 2015, Deadly Psychiatry and Organised Denial,7 there was enormous media interest all over the world because I had documented in detail why psychiatry is a disaster area. It was very threatening to mainstream psychiatry, and two weeks after it came out, Geoffroy wrote in an industry supported throwaway magazine that I used public funds to publish private, non-scientific books, which she compared to Scientology books.8:23
She claimed that I scared citizens suffering from psychiatric disorders away from getting relevant treatment (which means drugs). I complained about her libellous misinformation, and a tribunal concluded that she had violated both the ethical guidelines and the collegiate guidelines from the Danish Medical Association and had used a language that was totally beyond the borders of a decent debate about healthcare issues.
I mention this because Geoffroy’s below-the-belt reaction is typical of the way psychiatrists react in the public debate when they have no counterarguments and perceive their opponent as being dangerous for their interests.1,5,7,8
The textbooks direly warned of the consequences if ADHD is not treated with drugs. It was claimed that untreated ADHD can increase the risk of poor educational course, risky behaviour, crime and drug abuse; that there are effective treatments, primarily in the form of drugs;19:107 and that several follow-up studies suggest that stimulants protect against drug abuse.19:291
Another book claimed that drugs reduce the risk of developing drug abuse, traffic accidents, and committing crime.16:475
A third book, the one with no references at all, also mentioned the risk of drug abuse and crime, and that children might not get the education they could otherwise get, and it said that studies suggest that treatment can counteract this.18:224 This book mentioned psychoeducation, support, training, and rules for adults diagnosed with ADHD and claimed that the vast majority experience a good effect of the medicine and that venlafaxine may also be effective.18:229 None of these claims can be substantiated (see below).
A fourth textbook wasn’t any better. It said that medication is central and that many benefit from it.17:618 It noted that a Cochrane review raised doubt about the effect of methylphenidate because there was substantial bias in the trials,511 but added that many clinicians and patients say that they have a positive experience that methylphenidate works, which is indisputable.
So, clinical experience is all we need, right? If that is the case, then why bother to do trials? Did it ever occur to the psychiatrists that some patients say they like the drugs, not because they work, but because they are speed on prescription that makes them high?
It was also claimed that placebo-controlled studies have shown an effect of central stimulants in 70-80% of the children,19:289 and that 50% of adults have significant positive effects on the core symptoms, compared to 75% in children and adolescents.16:475 These claims are meaningless, as the percentages are before-after observations from a treated group, with no placebo control.
It was claimed that methylphenidate reduces hyperactivity and impulsivity in adults with an effect size of 0.50-0.56 and increases clinician-assessed global functioning with an effect size of 0.87.16:475 These large effects are also wrong (see below).
Trials of ADHD drugs are biased to an exceptional degree, even by psychiatric standards. A review of 43 studies in children, of which 34 were randomised, showed that very few of the reported adverse drug reactions were called serious, although many children dropped out of the studies precisely because of serious adverse drug reactions.512
Many of the trials have been carried out by the same small group of Harvard psychiatrists who have numerous financial ties to the drug makers. And most trials are flawed by design in the same way, e.g. by including only patients that have tolerated the drug, and often also only patients who improved while on the drug. The industry calls this an “enriched design.” I call it a design that makes the industry rich.
Most systematic reviews of the trials are therefore also biased. Two Cochrane reviews per-formed by my former employees, who paid attention to the flaws, found that every single trial ever performed was at high risk of bias, both for trials in children,511 and in adults.513
An earlier Cochrane review from 2014, of immediate-release methylphenidate for adults, showed positive effects for hyperactivity, impulsivity, and inattention, but the trials were short-term and biased.514 The results varied so hugely that I would not have performed meta-analyses on these data. Most worryingly, the authors could not even determine if adverse effects were not discussed because none occurred, or because the data had not been collected. The review was so bad that the criticism we and others raised led to its withdrawal from the Cochrane Library.515
My research group found that also the drug agencies’ reporting of harms can be highly unreliable.513 In the British drug agency’s review, “psychosis/mania” was reported to occur in 3% of patients treated with methylphenidate and in 1% of those on placebo. The 3% estimate is 30 times higher than the 0.1% risk of “new psychotic or manic symptoms” that the FDA’s Prescribing Information warns about. We even encountered discrepancies within the regulatory documents.
We observed huge differences across trials that could not be explained by trial design or patient populations, e.g. decreased libido on methylphenidate was experienced by 11% in one trial versus only 1% in a pooled analysis of three other trials. As quality of life was measured in 11 trials but only reported in 5, where a tiny effect was found,513 it is reasonable to assume that quality of life worsens on ADHD drugs, which is also what the kids experience. They don’t like the drugs if asked while their parents are not in the room.
In 2022, my research group published a systematic review of extended-release methylphenidate in adults.513 We found that every single trial had a flawed design and there were many other flaws. A medical student involved with our research was shocked when he saw this; he had never imagined that clinical trials could be of such poor quality, with many missing patient-relevant outcomes. He wondered, for example, why blood pressure measurements were missing when we know that stimulants increase blood pressure and that many people die from high blood pressure.
We used proper methods and could not confirm the large effects described in the textbooks. We included 24 placebo-controlled trials of extended-release methylphenidate for ADHD in 5066 adults. We also included documents from six drug regulatory agencies covering eight of the trials. We rated 20 trials at high risk of bias, primarily due to unclear blinding of participants and investigators, attrition bias, and selective outcome reporting.
All trials were impaired in at least one of three design characteristics related to generalisability, e.g. by excluding patients with psychiatric comorbidity or by including only participants with a previous positive response to stimulants. We rated the certainty of the evidence as very low for all outcomes.
For the primary outcomes, we found that methylphenidate had no effect on days missed at work and a minor effect on self-rated ADHD symptoms, effect size -0.37 (-0.43 to -0.30). Methylphenidate improved self-rated quality of life slightly, -0.15 (-0.25 to -0.05); investigator-rated ADHD symptoms, -0.42 (-0.49 to -0.36); and ADHD symptoms rated by peers, -0.31 (-0.48 to -0.14). These confidence intervals did not include the large effects of 0.50 to 0.87 claimed in a textbook, see just above.16:475 Methylphenidate increased the risk of several adverse effects.
We concluded that the benefits and harms of extended-release methylphenidate are uncertain.
***
To see the list of all references cited, click here.










