
Recently I posted about mental health social entrepreneurship, where we can use market based principles to solve our problems accessing effective care. Some people have told me on our market design survey that they have doubted whether we should charge people for mental health care.
Click here, we’d still love to hear what you think.
Doubts about mental health social entrepreneurship:
- I think for the people who need it, paying for it may be a burden. The culture of how people with mental illness commit to paying for services would have to change
- For the people who are homeless whom I work with, any fee other than nominal would be too much. They do not have money or just enough to buy a pack of cigarettes or some food to eat. But many would gladly offer their services to pay back; their skills are many and varied.
- I do worry a bit that the concept of making peer support a “business” could make it seem cold and commercialistic (if it’s marketed heavily enough to become a well-known service); that could be a turnoff to people used to seeing free peer support services at drop-in centers, who use other funding to pay their staff.
- People with mental illness labels are often the most resistant to any sort of paradigm change, so it might really take some time for anyone able to pay to think this is a good concept; then, perhaps embrace it.
- You have to be careful to make sure it was ethically run not to make a profit beyond what’s needed to grow the business nationwide.

So, it’s time to explain some of the advantages of social entrepreneurship, to start creating the cultural change people are requesting. One of the most influential books on social entrepreneurship is called, “The Fortune at the Base of the Pyramid,” by C.K. Prahalad. This book explains how to market products to people who make less than $1 a day, who are the largest income group in the world, involving over 2 billion people. The rest of this post is summary of Chapter 1 of this book.
Making people customers creates dignity.
- This is a way that globalization can be democratized so that benefits can go to all consumers and not just the 10% of the wealthiest people on the planet that 90% of products are designed for.
- The customers get choices and attention from the private sector that were previously reserved for the wealthy. (I.e. more expensive health insurance plans involve more choice of doctors.)
- Creating choice is where dignity starts because then we view low-income people as full participants in their local economy as producers and customers, not just charity cases. Deciding, “What is good for people” is against the very spirit of co-creation.
- Organizing access to information gives people the chance to be entrepreneurs, and organizing access to credit and micro finance allows people to build equity and escape poverty.
- It lets customers choose providers instead of our current social service model where providers only choose customers closest to a desired profile.(For instance, homeless shelters only letting people in who come by a 4:00 curfew.)
- Firms must continuously innovate and upgrade their products to keep customers interested in their brands. (What if we had three respite care programs to compete with each other in a market – how fast would that growth be…)
- Competitive firms are more likely to create transparent transactions that respect the rights of individuals
- Focus on ecologically sustainable solutions
- Scalability of solutions
This last point is the most important. Right now, we know that peer support is the most effective mental health intervention according to the 2002 report on recovery from the National Association of State Mental Health Program Directors. Yet we are having trouble getting our peer support programs funded or expanded. Lets stop relying on the government which takes 50% of our incomes and spends it in ways suggested by expensive corporate lobbyists that we can’t drown out. Or the 3% of our income that goes to private charity. Instead, lets look at the 47% of our income that we can control.
SAMHSA recently awarded the Brass Tacs grants designed to scale up peer programs. There were only six $25,000 grants awarded for probably 50 applicants. Yet how much did SAMHSA spend on the Teen Screen program to help get high school kids started on antidepressants? If we wait for them to rescue us, we may be waiting a long time.
How to challenge our assumptions about buying and selling to people at the base of the pyramid:
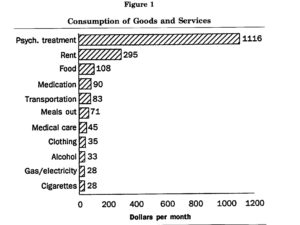
There is much dominant thinking about what poor people want or need or can or do afford. People with disabilities are the poorest of all minority groups in the United States, and people with psychiatric disabilities are the lowest of all those. Many people talk about how dirt poor we are, but when we look at our group as a total market force, we are powerful. Just by our large numbers, our latent purchasing power is huge. Paul Polak did a 1992 study on the purchasing power of diagnosed people in a community mental health center. His chart shows just how much money is spent ineffectively to “Help” us. Keep in mind that these costs were even before expensive branded psychiatric medications became the primary treatment method. Advocates in Kansas recently testified that over 80% of the cost of mental illness is lost productivity, so this chart is only the tip of the iceberg.
Our history of corporate domination has given us good reason to mistrust capitalistic or private sector approaches to problem solving. We may instead have more confidence in governments to do what is right, despite the public sector’s record on increasing disability in our communities. The dominant logic is hard to give up, which is one of the reasons people often appear to vacillate in their beliefs. People know where we have to go, but letting go of their beleifs and abandoning their “zones of comfort,” is extremely scary. It’s also extremely hard to get off disability once someone has that committed income. It’s easier to keep a bird in hand, no matter how inadequate, than take a chance on the three birds in the bush.
How mental health social entrepreneurship can create new treatment models:
There is great hope ahead with trying new approaches, and I’ll let more voices from our customers surveys speak on this:

- I haven’t had much time to think this out. Except I know I feel better paying for something of value. Talking can keep emotions from escalating to the point where there has to be police intervention. THAT is worth a lot of money!
- I think people need to pay something although initially it may be difficult, until they feel more in charge of their lives. It is one way to really value giving service if one volunteers. Since volunteering is work, one is utilizing skills and can feel good about further developing such skills and paying in this way.
- Great idea. What it is worth is immeasurable. What folks can afford to pay varies greatly according to specific circumstances and moments in time. There needs to be supplemental donations from businesses, donors, or those recipients who can afford it so that no one is turned away if at all possible.
- For consumers able to pay, this could give a sense of dignity/self-sufficiency instead of the patronized feeling that could come from being a charity recipient. People with self-respect and a work ethic don’t want to be charity recipients and might be depressed about having to be.
- If you could generate enough revenue you would indeed remain free to say/do what you wanted to.
- People like me, who have overall been disillusioned and/or mistreated by the “medical model” system could really respect and gravitate to your philosophies and services, seeing it as a potential source of hope and healing that might not exist elsewhere.
- Volunteering to your cause (especially as peer specialists) could help mobilize consumers who aren’t doing much. This also could send the message to society that people can and do recover from mental illness; said message increases societal understanding and decreases stigma.
- Interesting. I like the “sweat equity” approach, especially if people move into the supporting role through it, creating relationships of mutuality. Consider, also, barter in the form of products, art, etc. that people receiving support can offer. I can think of times in my life when I could only offer poems, but they were darn good poems.
- Great idea, especially to help people understand their worth, get them used to being around others in a work setting, and getting them out of the house (something I struggle with still!)
Thanks so much to all who helped with our survey.


 / patient Advocacy")











This is the idea behind calling us CONSUMERS. I am not and never will be a consumer of Focred treatment. It is a total and utter insult to me to call me a consumer. NO ONE can consume mental health services. They are forced onto you, there is no choice and no control. Until you outlaw forced treatment nothing else will change.
On top of that, people don’t need money to pay for services. Within the disability community it is very common throughout the world for people to have personal budgets allocated to them. They are allocated a set amount of money and they are required to spend it broadly on disability related needs. Checks are done to ensure it is not spent on things that most people are required to subsidise themselves, like food, shelter, clothing, transport, etc. IF a person is unable to catch public transport, they could fund PART of each trip from the subsidy. If they could not go on a holidy without a carer they will fund a carer to go with them and/or fund part of a trip for people with disabilities. The simple reality is that we could very very easily give people budgets and allow them to choose for themselves what they wanted to do. But NO ONE will EVER do that in mental health. First they believe that we have no idea of what we need and secondly most people are very unlikely to spend it on what they want us to spend it on. Very few people would even choose to spend it on peer support services. Many people find them incredibly insulting and useless. They are the best of what is offered, but not what we would choose. We use them as we have no choice and they are sure as hell better than ECT or being unconcious on medication.
Research shows they would choose exercise classes, diet advice and cooking classes, counselling, massage, outdoor programs, etc, and above all else they would choose to do them all in the mainstream and not access specialist mental health services. At present if they are allowed those things they do them in special mental health programs. Apparently these people are too deranged to be in the real world.
Report comment
This is the idea of “self-directed care.” It’s used a lot in the development disability community and has been used some in mental health. The places using it find what you say, that people spend it on wellness and job development instead of endless medical care. It saves a lot of money and improves outcomes in the places it’s been used.
I agree with you, this service needs to be 100% voluntary. It also needs to be a low enough price that it’s not a huge burden to anyone to participate. I’d love to have you click our survey to tell us what that price might be, to talk to someone for a bit who’s been through much of the same experiences as you. You could search by state, psych labels given, people who know how to come off meds, age, or shared hobbies, or any number of other variables to find someone with very similar experiences, then just meet up with them or give them a phone call.
Then just pay a little bit DIRECTLY to that person for their time. You aren’t paying a mental health center at all, just another peer who really needs a job. Or some people who don’t want to charge money to help other people can deliver the services for free if they want. That option will be available, too.
Report comment
I don’t think that people should be focused on getting “care” so much as getting their lives back. And I don’t think that another person can do that for someone. Maybe people don’t need more services. Maybe they need jobs. Maybe they don’t need “peer support”. Maybe they have to get away from a “community” that talks about “wellness” and back into the regular world. Just because someone else has been labeled as having a “mental illness” doesn’t mean that you’ll have anything whatsoever in common with them. This whole peer thing doesn’t sound right to me. Better to find yourself than rely on others to constantly “support” you. If we stop thinking of ourselves as being in another category, if we reconnect with the larger world instead of “services”, we will start to get our lives back.
Report comment
Dear Corinna,
I have enjoyed your posts so far, and I applaud you for your activism. I also happen to think that peer support services are a great thing, and support your drive to make them more readily available to folks who would like to access them.
… all that being said, I must warn you that citing Prahalad’s work as the template for your vision of “social entrepreneurship” severely damages your credibility. I have read C.K. Prahalad’s book all the way through(have you?), and while Chapter 1 can sound deceptively nice, there’s some truly horrible stuff buried in the case studies, and in his other writings as well. This man is not out to empower anybody or anything except his own wallet. He aims to create consumers out of a class of people that lives OUTSIDE of that paradigm at the moment, to suck them into the consumerist philosophy of “never enough, never satisified” … and to get them to expend their limited resources on planned obsolescence instead of sustainability.
In this article of Prahalad’s, he applies his BoP [bottom of the pyramid] philosophy to the selling of fairness creams in India. A quote from Prahalad:
Beyond such benefits as higher standards of living and greater purchasing power, poor consumers find real value in dignity and choice. In part, lack of choice is what being poor is all about. In India, a young woman working as a sweeper outdoors in the hot sun recently expressed pride in being able to use a fashion product — Fair and Lovely cream, which is part sunscreen, part moisturizer, and part skin-lightener — because, she says, her hard labor will take less of a toll on her skin than it did on her parents’. She has a choice and feels empowered because of an affordable consumer product formulated for her needs.
Apparently, it’s empowering for a street cleaner to buy a product that a.) doesn’t work, but b.) promises to make her fair and lovely like the White imperialists that rape(d) her country of resources and created the urban squalor she lives in?
And that’s the fundamental problem with the whole BoP/”doing [monetarily] well while doing good” idea: are we offering people something that is truly of value and relevant to their lives, or are we simply lassoeing them into the same consumerist trap that many of us have fallen into? Are we “empowering” them by offering them a new product, or glossing over the root causes of their sufferings with a quick fix that will make us a few bucks? Because the “opportunity” to partake in something frivolous or downright unhelpful or even imperialist (and to trade your hard-earned resources for it) is not particularly empowering, in my humble opinion, if the root problem remains.
Report comment
ALT,
I am not so into beauty cream either, and I’m aware of the claims that some sunscreen ingredients cause cancer. I have not investigated whether or not the reduction in cancer rates from using sunscreen is greater than this or not. Right now there are so manly inaccuracies in health care messaging that I’m mainly focusing on mental health messaging. I agree that a “lightening cream” is a pretty racist product.
However, there are other products in Prahalad’s book like prosthetic limbs and eye care that might be less morally offensive to people who object to capitalism itself. I agree that capitalism has caused many problems, and this is mainly because corporations are currently judged purely on their monetary return to shareholders.
A social benefit corporation, however, according to Mohammed Yunus’ definition, does not make any return at all to the shareholders. Instead, it’s judged by it’s contributions to the well-being of customers, employees, community, and other stakeholders. Six states in the US have a B or benefit incorporation law standing, and certification is available that rigorously checks the impact on all these groups.
Other products have been provided using social entrepreneurship to allow a much bigger expansion and service area: clean water, sewage recycling, generic medications, vitamin fortified yogurts, therapy that does not rely on expensive professionals, and social services provided by community members that solve root causes of poverty.
Of course, this is why I am doing an extensive pre-launch investigation of our model and our product. Social entrepreneurship is a difficult concept to explain to many, but good programs produce very transparent results and numbers.
We won’t be able to expand effective programs by relying on handouts from charities and governments. Conversely, services that are so expensive that we must rely on handouts are probably way too complex, labor intensive, and outside our regular communities to be effective.
Report comment
SA I could not agree more with you. I spent decades floating around so called peer support services and all I found was that they reinforced this idea that I was different and that I didn’t belong in the world. I didn’t need another person who had supposedly been through what I had been through telling me how to get better, or supposedly giving me hope. What I needed was the wider community showing me hope. EVERY time I have spoken to ANY peer support worker or the like I have simply been told if you just do what I do you will get as good as I am. WRONG. I am me. There is no person the same as me. And I don’t want anyone the same as me. I am me, a full unique person just the way I am. I should be loved and valued for being me. I still have huge levels of symptoms, but I REFUSE to live with a label, and I refuse to be part of services. In fact I’ve been kicked out of services because of my beliefs and banned for life from them all!! I have spent over 10 years doing everything anyone said I should do to “get better”. Very little of that was medical, most of it was so called peer or rehabilitation services. I am still not “better”. I’m now simply focusing on what I’m good at and enjoying the things I can do. And what do I find that by simply being allowed to be me and being allowed to do the things I enjoy, instead of sitting around waiting to “get better” I am actually better than I have ever been. Doing nothing did not help me. Attending services didn’t help me. Meeting up with so called like minded peers didn’t help me. Being in the real world doing real things did help me. Peer support MAY work for some, but it sure as hell does not work for me. We all want to know that we are not alone. We all want to know that someoen else has gone through what we have gone through, but NO ONE wants there whole life to be that. The whole reason people are not getting better is because NO ONE allows them to get better. They are stuck in service land until they are better. They are told they have to be better until they can work, go to school, or do any number of other things. NO ONE tells a blind person they can’t do anything until they are better. NO one tells a deaf person they have to get better before they can do anything. No one tells a person in a wheelchair they have to get better. And no one says it to someone with intellectual/development/learning disabilities (different countries use different terms). Have any number of other conditions and we support people to be fully functioning members of the community WHILE they are disabled. Suffer a so called mental illness and everyone needs to FIX you!! We also know from the research by the World Health Organisation that doing nothing is better than what we currently do. In fact if we do nothing at all the chances are people will naturally get better. If is our need to fix people that makes them sick. And while so many rehabilitation and peer support services go on about how they are different, the simple fact is they are all doing the same thing and telling us that we need to ‘get better’.
In terms of other disabilities, it is not just those labelled cognitively impaired that have these budgets and they are not always self dirceted. Different places do them in different ways. What happens in your country and in particular your community is not what is happening elsewhere. This came about because it was what other groups were doing. In particular people with physical disabilities were demanding it. They wanted to choose there carers, choose where they lived, etc. People who are totally blind can not do everything totally alone. They can learn to do many things and learn to get around and there are many things that can enable them to live independently. With a kitchen adapted for them, with talking scales, thermonetors, etc, they can learn cook, etc. They can learn to clean. But they still need help at times. If they have a supportive family that may be enough for them. But not everyone has that. They can’t get ALL bills and stuff in braille and so often need someone to come and read mail for them, at least once a week. They need someone to take them grocery shopping, etc. People with an Aquired Brain Injury can learn many things but they can have varying levels of disability and again need varying levels of support. Not everyone can direct that support. BUT that doesn’t mean that support cannot be directed at them. Supported decision making is not simply about allowing the person to control everything, many can’t do that. And many are so called profoundly disabled and unable to communicate in any meaningful way. They cannot direct there care. That does not mean that they are retarded and that we should just do things to them. It means we listen to there body language, we listen to what they are trying to tell us and we look and consider what they enjoy doing and we start doing more of that with them, instead of just shoving them in day programs.
We also know that even with people who are profoundly disabled and need carer’s 24/7, the community is more likely to accept them if it is just them and a carer. Of course we have adult day programs and we take them out in groups, to the movies, the pool or the like. Everyone moves away from them and lets them through. No one tries to interact with them. Take them there one on one with an individual carer and people are much more likely to interact with them. We also know from ALL areas of disabilty that the untrained and the totaly inexperienced are generally the best carers we have. As soon as someone is trained they act as though they know everything. If someone has had an ABI and then recovers they go in as a carer and tell people what to do so they can get better like them. People with families who have experienced something treat them as they treat the family member. Only when people have no idea of anything do they tend to accept people as they are and consider what they need. Why should those labelled as mentally ill be any different at all. I don’t need some so called self proclaimed expert, whether by experience or by training. I just need the average person down the road to accept me as me. And from experience, when I started interacting with the average person down the road, instead of listening to what everyone was telling me, I began to interact with people and I began to get better. I also fail to see how ANYONE can set up anything to connect people who are like them, we dont’ even know what we are connecting people on. As for diagnosis. At last can’t I had 37. Which one do you want to me to search on, or should I search for all of them at once. I should add that ALL of those 37 are CURRENT. I meet the FULL diagnositic criteria for each and everyone of them. And if I consider people with the diagnosis, yes to some degree I’m like them, but I have an extra 36 to add to the fun. Since there are no two people in the whole world with the exact same symptoms of schizophrenia I fail to see anyone can possibly let someone know what they are going through. Mental illness is not like anything else. These are not real conditions in that we can say this condition really exists. They are simply lists of symptoms and those symptoms change all the time, by nothing more than a vote. No one has a vote to decide what the symptoms are of any real medical condition. It is up to people to decide if they do or do not want to believe in a diagnosis. It is up to people to decide if they do or do not want peer support. What annoys me the most is that people either take what the system offers or they go without. It does not matter how much you fit outside the square you are, it does not matter how much of an amoloy you are, when it comes to mental health you are required to be a square peg in a round whole. And while most people will have some level of roundness and fit in slightly better, some of us are so far from the norm, that our edges could not be more square if I tried. While individual budgets are a relatively new thing in my country, for over 60 years in ALL areas of disability there has ALWAYS been some level of brokerage funds for those that do not fit the norm, are were just so far away from any standard service that they needed something different. And yet in 60 years of mental health they are pushing for people to be more and more the same than ever before. And of course from my perspective what I see is worse and worse and worse outcomes. I have seen fad’s in all areas of mental health in my journey with the system and NONE of them have ever shown anything of value to me. They all do exactly the same thing. Tell us that this is the new thing and this will save us all and this will some how fix us all. Why should this be any different. How can anyone know me better than me. And yet that is exactly what you are claiming that someone who has shown a few behaviours similar to me, can somehow know me better than I know myself, and they can tell me how I can get better. HOW. If the top doctors and scientists in the world can’t do it, why can a total stranger, who has no education and no nothing. They have not lived my life, they have not lived through my trauma’s, and they do not have my diagnoses, as they may have similar things, but they are not me. I am me and I am perfectly OK as I am. I personally am sick and tired of being told that I am defective and that these so called consumer experts know how to fix me. What I see happening in the peer services is no better than the clinical services are. They are just doing it in different ways. They may not force electricity through my brain, may not force me to take toxic medications, but they are no less harmful in my opinion. The psychological torment they put me through is worse than the medical treatments. At least with the medical treatments I am so sedated I can’t move or think. I am sick and tired of being told by peer workers that I need to get better. Exactly what is better. You tell me I’m not better, and say it is a personal decision, but then insist that I am not better and need to get better. Better to you is me being you, but WHY. WHY is what your doing right and what I’m doing wrong. And how are you better and I’m not.
Report comment
SA and Belinda, my thought is to find people like you who are mental health “escapees”, complete graduates from services to share their stories with a little reimbursement for their time or the chance to volunteer, whichever you prefer. This is slightly different that the “obedient consumers” that mental health centers sometimes recruit to be peer specialists.
If someone contacts a supporter on our site that acts superior or all-knowing they’ll be free to leave a poor review score just like on Amazon. People can choose whoever they want to talk to based on what part of the profile interests them. People can find help for medication withdrawal, employment, spiritual needs, help getting undiagnosed, or building physical health (the number one most requested service.) 74% of people said they wanted face to face interaction, and 54% said they wanted to spend time with shared hobbies, out in the real world.
Our job is not to get people into the mental health system, it’s to get them out.
The best way to do this is to help people find their own natural supports, like PTA meetings, sports clubs, gardening groups, church, activism, whatever works for you, as an individual. People who are heavily entrenched in the system often have lost these. Our primary customers are people with only 1-2 unpaid people in their lives who will listen carefully to them.
Most people using this online forum are beyond this place and are more likely to be our potential staffers, people who can list a profile and earn money any time they might already be online doing something. Or volunteer, if that will create the most mutual interaction and you are willing to do this.
Report comment
I for one would have been glad to find support from someone who had been through the hell of compulsory mental health care when my son came out of hospital, physically and mentally paralysed by antipsychotic meds. Doctors refused to help and I searched high and low for pracical help and advice how to get him safely off those drugs and back into normal life- Someone who didn’t believe in the “mental illness” malarkey. I was glad I found Will Hall and Peter Breggin on the Internet. A live person to talk to would have been even better.
Report comment