
In the domestic violence field, the methods employed by men to bully and abuse women and children are identified in the Duluth Project’s Power and Control Wheel, a tool developed by survivors of domestic abuse.
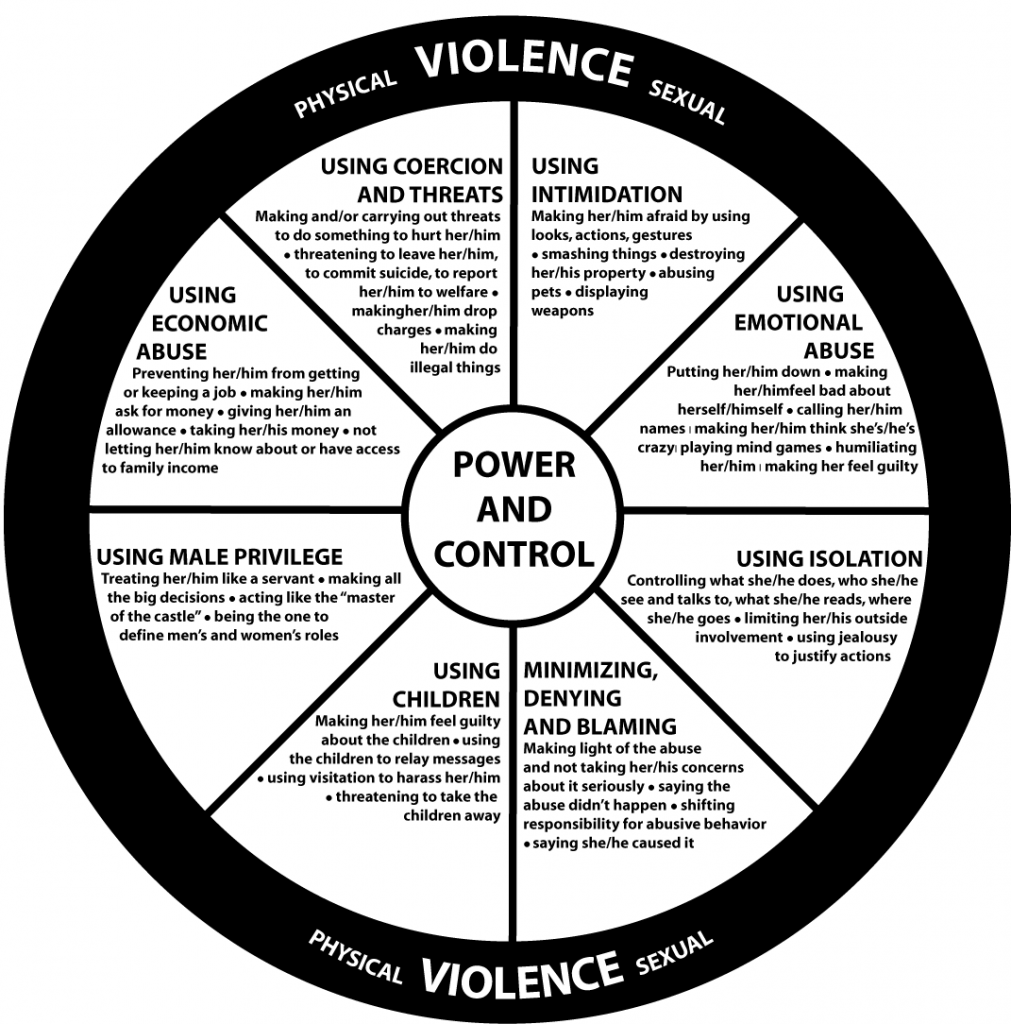
Replace male privilege with medical privilege, change a few descriptors and you have a good explanation of the ways in which psychiatry maintains its dominance over individuals and societies.
Name calling (diagnostic labelling), coercion (forced treatment), threats (removal of children, incarceration) . . . the parallels are obvious.
There is no accepted definition of bullying either in statute or general use but the elements common to most definitions include the misuse of power and influence to cause fear, distress, humiliation and harm to vulnerable people. Bullying within family, work and student relationships is generally understood as being learned and practiced within social, cultural and institutional contexts.
Arguably, psychiatry is nothing more than officially sanctioned bullying and abuse.
Just as with other forms of bullying, psychiatric bullying is minimised through victim blaming, defensive posturing and self justification by those who practice it. The victims of schoolyard bullying are blamed for being over-sensitive, bringing the abuse on themselves by their behavior and needing to toughen up. Bullies are excused for knowing no better, not intending to cause harm, not understanding the impact of their actions and being victims themselves. Some even justify bullying as toughening people up’ and therefore being in the best interests of the victim.
Similarly, psychiatrists argue that their victims exaggerate their feelings of distress and experience of harm, are treated the way they are because of socially unacceptable behaviours and need to become more resilient. Psychiatrists would argue they do not intend to cause harm, humiliation and distress, are just doing what they have been taught to do, don’t believe their ‘treatments’ and attitudes cause harm and are themselves the victims of abuse by violent, abusive patients. They argue that forced incarceration and treatment are in the best interests of the people subject to it.
Not a lot of difference between schoolyard bullies and those in psychiatric hospitals then.
I was interested to read recently a review of a debate held in 2004 by the UK Royal College of Psychiatry on the topic Bullies Should be Pitied and Not Feared.
According to the paper, those in favour of the motion argued that understanding the adverse circumstances that create bullies should lead us to pity them and that rather than blaming individuals, we should pay more attention to the roles that communities can play in either condoning or combating bullying.
Those against argued that fear is an appropriate reaction to a behaviour that is unpleasant, injurious and wrong particularly where the consequences for victims range from “anxiety and depression to post-traumatic stress disorder and even suicide,” that the ‘fight or flight’ reaction is an entirely appropriate response when an individual is being bullied, and that pity gives the bully positive attention which may reinforce the bullying behavior and encourage victims to become bullies.
Child and Adolescent psychiatrist Anne York, who argued against the idea that bullies should be pitied, claimed that bullies bully in order to gain unwarranted attention and respect, and that any pitying of such behaviour is highly inappropriate.
She argued that giving bullies this recognition may result in them ending up in positions of national or even international responsibility, making us all potential victims of bullying.
Imagine. Bullies in positions of national and international power.
According to the review’s authors, the audience of adolescents who were pro the notion of pitying bullies at the beginning of the debate found the arguments against that position so persuasive they voted to reject the motion by the end of the debate.
Interestingly, the review also tells us that the one issue on which both side of the debate agreed is that all schools should have anti-bullying policies in place.
It is not uncommon for psychiatrists to agree that the practice of psychiatry contains elements that are coercive, distressing, humiliating and harmful. Would they therefore agree that, as with schoolyard bullying, all institutions in which people are at risk of encountering psychiatry should develop and implement anti-psychiatry policies?
Around the world, governments have insisted that schools develop anti-bullying policies which could be adapted and developed into anti-psychiatric bullying policies. Taking elements of policies available on the internet, from a range of educational institutions, workplaces and advisory bodies such as the NZ EEO Trust, I offer the following as a model anti-psychiatric bullying policy for any forward thinking mental health institution.
Model Policy To Address Psychiatric Bullying, Harassment, or Intimidation
Introduction
Sometimes regarded as “treatment”psychiatric bullying and harassment can no longer be considered as such. During the past two decades, the often devastating effects of psychiatric bullying and harassment have evidenced themselves on the well-being of consumers and the climate of mental health facilities. Pharmaceutical and medical device advances of the last ten years have unwittingly provided another outlet for bullying and harassment, ‘biological psychiatry.’ Its message enters homes and communities and the resulting effects extend into every aspect of society. Incidents of psychiatric bullying, harassment, and intimidation have caused increasing concern among health professionals, children and young people, parents, and public officials.
Definition of psychiatric bullying
This policy adopts the definition of harassment and bullying provided by the NZ EEO Trust:
Harassment can be defined as any unwelcome comment, conduct or gesture that is insulting, intimidating, humiliating, malicious, degrading or offensive. It might be repeated or an isolated incident but it is so significant that it adversely affects someone’s performance, contribution or work environment. It can include physical, degrading or threatening behaviour, abuse of power, isolation, discrimination, sexual and/or racial harassment. Harassment is behaviour that is unwanted by the recipient even if the recipient does not tell the harasser that the behaviour is unwanted. Bullying is ongoing unreasonable behaviour which is often intended to humiliate or undermine the recipient but is not specifically unlawful.[1]
Mobbing is a particular type of bullying behavior carried out by a group rather than by an individual. Mobbing is the bullying or social isolation of a person through collective unjustified accusations, humiliation, general harassment or emotional abuse. Although it is group behavior, individuals can be held accountable for their role in mobbing.
Psychiatric bullying, harassment, intimidation and mobbing includes any behavior by a mental health professional or group of mental health professionals which insults, demeans, humiliates, distresses, coerces, intimidates or harms a consumer. It includes, but is not limited to:
- Unwelcome diagnostic labelling
- Involuntary incarceration
- The use of restraints and seclusion
- The forcible administration of drugs or other ‘treatments’ including ECT, DBS and other invasive processes dressed up as treatment by the use of innocuous acronyms.
- Threats designed to coerce compliance including threats to remove children, take proceedings under mental health legislation and breach confidentiality
- Verbal abuse
- Use of subjective assessments which damage self esteem, reputation and future prospects
- Victim blaming
- Coercion, threats and intimidation
- Economic abuse including the prescribing of expensive medications which have no efficacy and cause harm, insurance fraud and the abandonment of patients who have no financial means.
- Discrimination on the basis of personal characteristics and ability to function.
Appointment of Anti-Psychiatric Bullying (APB) Officer
The organisation shall appoint an anti-psychiatric bullying officer who is independent of the organisation and has completed training from an accredited psychiatric services consumer group.
The APB Officer will have the power to receive and investigate complaints without restriction. Full access to documents, records, files, CCTV footage and any other materials required to fully investigate complaints will be provided to the APB Officer on request. The organisation will ensure the APB Officer is provided with any support required to conduct interviews with complainants, witnesses and those accused of bullying, harassment or intimidation.
The APB Officer may make recommendations for change, initiation of disciplinary proceedings or victim compensation.
Reporting Psychiatric Bullying
Anyone who is a victim of, or who witnesses, psychiatric bullying should report it immediately to the APB Officer. Those reporting bullying should be assigned a support person to assist them to file a complaint, to explain the investigation process and to provide practical and emotional support for the duration of the process.
Bullying should be investigated whether a formal complaint has been received or not.
All reports will be acknowledged and investigations commenced within 24 hours.
Bystanders
As bystander support of bullying and harassment can encourage these behaviors, mental health insitutions must prohibit both active and passive support for acts of harassment or bullying. The staff should encourage staff and other consumers not to be part of the problem; not
to pass on the rumor or derogatory message; to walk away from these acts when they see them; to constructively attempt to stop them; to report them to the designated authority; and to reach out in friendship to the target.
Training should be provided to staff on how to respond to bullying and harassment incidents. Posters and pamphlets should be provided to in waiting areas and information packs to all consumers which encourage them to report any bullying or harassment they witness. When bystanders do report or cooperate in an investigation, they must be protected from retaliation with the same type of procedures used to respond to bullying and harassment.
Disciplinary Action
All criminal actions must be reported to the police. All breaches of professional codes must be reported to the medical council.
Investigations will determine, on the balance of probabilities whether bullying, harassment or intimidation has occurred.
A report will be provided to the complainant on the findings of the investigation and on disciplinary action being taken.
Now obviously this is not a comprehensive policy. It is not intended to be. Rather my purpose is to highlight the way that mandatory policy development has changed thinking and operating in response to schoolyard and workplace bullying.
Policy sometimes follows a change in thinking, but equally often it is developed as a tool of thought leadership and cultural change. Without strong leadership on preventing bullying, the ritual humiliation and abuse of children and employees would in all likelihood still be seen as an inevitable occurrence that shouldn’t be taken too seriously.
While the practice of psychiatry is governed by vague codes of rights which lack any specificity around rights to respect and safety, a culture of failing to recognize or respond to abuse will prevail. I believe that the overwhelming evidence of psychiatric abuse means those who are engaged with mental health services should be extended the same rights to protection against bullying, harassment and intimidation as are extended to others. I believe mental health institutions should pro-actively institute such policies but that governments should mandate their development.
An anti-psychiatric bullying policy would contribute to the establishment of a culture of respect, safety and accountability and make psychiatric abuse more visible and therefore more open to public scrutiny.











Maria,
Thank you for such a comprehensive and rationale look into how psychiatry practices bullying. I think you are right on target, and hopefully your good thoughts will sprout further, and lead to change in a practical sense.
However, I would just like to add a reflection that is personal to me, in relation to your point that “Arguably, psychiatry is nothing more than officially sanctioned bullying and abuse”. Admittedly, my point is outside the scope of the objective of your fine article; however I feel it is a point to make.
I see the bullying and abuse by psychiatry as criminal behaviour because they know well that serious harm and death is a very real outcome of their “policy”. They have access to well documented evidence which demonstrate how many of their practices are actually acts of reckless criminal negligence that have caused irreversible serious harm and death.
I hope my point highlights why a challenge to their bullying and abuse is even more urgent, so as to hopefully prevent further acts of reckless criminal negligence.
Thank you for raising this very important discussion.
Best wishes
NewPC
Report comment
I couldn’t agree with you more. The New Zealand police are currently reviewing the evidence in relation to my son’s death as I have submitted it constitutes manslaughter. I’m waiting for the police to complete their review and advise whether they are laying criminal charges against the psychiatrist. Cross your fingers for me 🙂
Report comment
Nice piece, Maria, and I too hope others will see the importance of ending the blatent human rights abuses, that typify forced psychiatric “treatment.” Psychiatry, as it’s practiced today, is really nothing other than state sanctioned bullying, torture, and murder, for profit (and to cover up other egregious sins and easily recognized iatrogenesis).
Report comment
I love your piece. Sadly things are rarely that straight forward in real life and some times it must be difficult for a psychiatrist to decide what is the right thing to do. We are only human. Once my son recovered – and he could have been easily dead had I not found him in time – I went to confront the psychiatrist who failed to answer my calls for help. I expected him to apologise but to my surprise the poor man started falling apart in front of my eyes and believe it or not I felt sorry for him and thought: you could really do with some counselling yourself and thank heaven I am not in your shoes.
Report comment
I wonder how many of them are truly introspective and self-reflective enough to even come to the point of admitting that they need help? They are the “experts” after all. I suspect that very few of them could even come to admit that they need help. I’ve dealt directly in my own life with four and though three of the four would be considered good people, I believe that only one, maybe two, of the four could admit something like this. I work alongside a large number of psychiatrists in a state hospital. IMHO, very few of them are even willing to accept their humanity and work out of that for the people place in their care. I do believe that most of them are into bullying because they feel that they have the right to treat people like this because they’re the experts. I can count on one hand the number of psychiatrists that I consider to be true healers and doctors and I deal with a lot of them on a daily basis.
Report comment
Hi Alix
I accept totally that people make mistakes and psychiatrists are no different from anyone else in that respect. What I’m concerned about is that many standard practices in psychiatry are nothing more than abuse and many psychiatrists routinely engage in abusive practices for which there are no challenges and no accountability. Making mistakes is one thing…deliberate abuse is another and that’s what I think needs addressing.
Report comment
Almost every film in which a psychiatrist appears he is presented as an evil doer! And not by some accident or misperception on the part of the script writer or novelist. For example, the Millennium Trilogy–Girl With Dragon Tattoo. What sort of person typically becomes a psychiatrist? Similarly one might ask about attorneys. Professions offer a path to power over people. They can easily become corrupted as has our legal system. And of course the medical system. In fact in America corruption has become all the rage. America is now a corrupt society. Starting with that fact which is painful but the case, we have a big job ahead of us in order for America to even survive. We are like a house that termites have taken control of and are in great danger of collapsing. Lies will not work anymore. Like the VA hospitals the truth starts spilling out into the public. Time to clean up America and to leave to other nations their own destines. We can start in our own homes in our own lives.
Report comment
Thank you for a thought provoking article Maria.
My belief is that the state can not possibly deal with the bullying of mental health workers, as they are the people who created the environment for it to occur.
What they can do is drug the victims into submission.
It would be a unique wayof dealing with domestic violence, drug the person being abused and return them to their abuser. Let’s hope the state doesn’t realise how much could be saved.
Report comment
I agree. The state has too much vested in keeping patients vulnerable and afraid to have any interest or ability in the empowerment of those involved in the system. Demand for change would need to come from the public and be driven by those of us who have been harmed. Sadly the myth of the violent, irrational mental patient who is a risk to society and the myth that psychiatrists are practicing evidence based medicine serves to make the average person on the street comfortable with human rights abuses within psychiatry.
Report comment
That is the problem: no matter how many statistics you throw at people they always go back to “but there are crazy schizophrenics who hear voices and want to kill everyone”. There seems to be no possibility of constructive discussion until we’re all bogey men.
Report comment
Thats exactly the problem. Indifference to psychiatric bullying because of stigmatisation. Criteria for involuntary commitment is disgracingly abused. It’s grave and imminent danger, but theyll force you in for ventilating online. Abusive psychiatrists have waged a war against patients freedom complicit with lawyers judges nurses police. There has to be a rebellion against psychiatric soul assassination.
Report comment
Some years ago, a friend of mine posted that if you called a a domestic abuse hotline and reported that your spouse was forcing toxic drugs, isolating, humilitating, threatening and/or doing physical harm, listing many of the abuses which are done in the name of “treatment” but substituted “the spouse” for “the psychiatrist,” you’d be advised to go to a shelter. I think comparing domestic violence to psychiatric abuse and endangerment makes some excellent points and might even be useful in educating those who have not been harmed by the system, but I think our best hope is in creating better alternatives than the mh system and not put more energy into trying to fix a broken system to keep it going.
Report comment
Abuse is abuse, it doesn’t really matter where it happens. But when it comes to abusers there are two types: people who do it as a self-defence mechanism and people who are sociopaths and enjoy creating misery and playing with others feelings and very lives. It may not be always very easy to tell the difference from the outside perspective. A friend of mine is a judge and frequently encounters this problem: people who are domestic abusers but who are victims themselves, who have addiction problems etc.. In cases like that it often makes sense to give them some chance for therapy and social intervention which will help them resolve their issues. Also sometimes situations escalate so much that it’s hard to entangle who’s the original abuser – it’s like asking fighting kids “who started?” But of course there are also clear cut cases with typical sociopaths standing there with a smirk and playing the poor victim card after they’ve abused the shit out of everyone around. It takes a lot of intuition, empathy and real life experience to get to the truth and find the best solution.
Report comment
Psychiatrist that’s harassing me I sociopath that enjoys creating misery and playing with feelings and ruining lives. Unable to get rid of my harasser, all the rage of having to endure the harassment encouraged by system with nowhere for, I collateral threatened and harassed wrong targets because the rage got refuneled somewhere. WHY WONT SHE BACK THE FUCK OFF I GOT A NEW DECENT PSYCHIATRIST NOW.
RENAUD TREMBLAY [email protected]
Report comment
” Appointment of Anti-Psychiatric Bullying (APB) Officer”
Sound great but in practice it’s probably going to be as useful as patients’ advocacy…
Report comment
I’ve been psychiatrically bullied for 13 years. The soviet system in Québec coerced me to a harmful practician to which i never consented. I want her to get off my fucking case, enough damage has been done, everyone complacent here. Any outside authorities can help? CIA, FBI, for international psychiatric violation rights, torture?
She’s terrifying, uses system to involuntary commit as revenge for attempts to get rid of psychiatric torture practices. Help
Report comment
This is ridiculous they blame us for haveing emtions but they allowed to have emtions we put Up with constant bullies, instead of medicating them they medcation us to take our soul and motivation,XTR Psychartic Bullies you would have to go to united nations human rights Commission,
Report comment
Psychiatry itself is pure gaslighting of the people, so that they’ll believe the fake democracy.
Every nation on Earth claims to be a democracy; but the people do not consent to their government, since they cannot overrule it, as consent requires.
So psychiatry gaslights them for their cognitive dissonance, telling them that they’re just mentally defective.
This way, dictators can remain in power, and enslave the people under the false belief that they are free; while gaslighting the problems caused by cognitive dissonance between this dogma, and their own experience of reality.
Meanwhile, any who resist the enslavement, are subjected to political abuse of psychiatry “for their own good” using the power of the state, and its puppet-academia and medical professions– and their empowerment and control by the state.
So understanding this problem, requires a fundamental understanding of political sophistry in which we live, and the historical background by which an elite minority seized power over everyone else.
It’s explained full here at https://qr.ae/pst4jg
Report comment