
 This is a topic that is very close to my heart and just seems to be one of those things where life leads you and you cannot really understand why certain things have happened in your life until later. Sometimes, when we get a little older – hopefully a little wiser – we realise certain things in life. One of the lessons I have had to learn is that not all people who have letters after their names are actually “gods,” or even people who have special powers to know things about us that is more important than we can learn about ourselves, about our own bodies, and our own minds. Blindly following what someone says we need to be doing for our own health (mental or physical) and well-being just because they have a white jacket on (so to speak) is usually not in our best interests. I believe it was Dr. Bernie Segiel, author of Love, Medicine and Miracles who said that those patients who took the most active involvement and who researched their own care and recovery were the ones who time and again tended to go into remission from cancer.
This is a topic that is very close to my heart and just seems to be one of those things where life leads you and you cannot really understand why certain things have happened in your life until later. Sometimes, when we get a little older – hopefully a little wiser – we realise certain things in life. One of the lessons I have had to learn is that not all people who have letters after their names are actually “gods,” or even people who have special powers to know things about us that is more important than we can learn about ourselves, about our own bodies, and our own minds. Blindly following what someone says we need to be doing for our own health (mental or physical) and well-being just because they have a white jacket on (so to speak) is usually not in our best interests. I believe it was Dr. Bernie Segiel, author of Love, Medicine and Miracles who said that those patients who took the most active involvement and who researched their own care and recovery were the ones who time and again tended to go into remission from cancer.
Let me first clarify my position on all of what I am about to say in this article so that there are no misunderstandings:
- I am not saying that people should not listen to their medical professionals, but I am saying that most of the time those who heal need to be actively involved in their own healing and research and learn as much – if not more – than their so-called “specialists.” This is the only way we can make true informed choices about our own health and well-being, and about what is right and what is wrong for us should we ever need help or “treatment” of any kind.
- I am not saying that all of psychiatry and that all psychiatrists or doctors are to blame for what has happened and what is happening in the world today. There are many fantastic doctors and psychiatrists who understand what is going on and are doing their best to help. Unfortunately there are also many who are oblivious, ignorant or even arrogant and will not listen to what their patients are telling them.
- I am not saying that people should NEVER take or be on anti-depressant medication. There certainly may be a time and a place for them, and a need when people get severely debilitated by depression, and if they become suicidal. From that point of view, one could say that sometimes these medications can save lives. However, what I am going to talk about here is the far-too-many cases where antidepressants have been prescribed prematurely for anxiety, phobias, post-natal depression, a divorce, a job loss or any other “normal” life event that causes normal human sadness and grief but then they go see their doctor and the first thing that happens is that they are offered medication.
I don’t speak about these things only as a psychologist and someone who has been interested in anxiety and depression for most of my career (and life since around 19 years of age) but also as someone who has helped hundreds of people with their anxiety and depression over the years. I also speak about these things from deep personal experience. I have written an article on Mad in America which attracted over 89,000 views since 2013. I have had hundreds of people writing to me from every corner of the world sharing their plight, their anguish, their pain and desperation to get off these terrible drugs. People in their twenties through to people in their sixties. People who has just started on them and people who have been on them for over 20 or even 30 years!
I believe that in time we will eventually see the use of some of these medications as being as insane and barbaric as we now see treatments like ECT (electro convulsive therapy) or worse, such as trepanation – the drilling of holes in people’s heads to let the demons or black bile out – that used to happen in the 19th century.
A mild panic attack at the age of 23, just after completing my master’s degree in psychology and receiving my thesis back with lots of red pen all over it, was not a good reason to be put on an antidepressant. The psychiatrist at the time said I had GAD (general anxiety disorder) and said I would feel amazing with this new drug called Ciprimal (citalopram). Anyway, that is a long story that has already been discussed elsewhere, but I will share more of it here over time.
Today, I want to really put down a challenge and hopefully start a wave of awareness and protest against a multi-billion dollar industry that is probably destroying more lives than cancer, heart disease and AIDS put together. I know that is a bold statement, and I do not make it lightly. The reason I say destroying more lives is because it is so unrecognized; not only for what these medications do that changes people forever while they are on them, but also because depression is still so stigmatized in society that no one really wants to talk about it. In some cultures they still do not believe it is real or even exists, and members of that culture or society are actually shunned if they show signs of mental distress, especially depression. Absolutely ludicrous in the world we live in today. The other reasons include the ongoing lack of recognition by the medical community (largely fueled by the big pharmaceutical companies) that there is no such thing as anti-depressant withdrawal. Whenever a patient tries to go off their medication, no matter how slow or what tapering process they may use, they will experience a withdrawal reaction just as you would from any other mind/brain altering drug. The pharmaceuticals vehemently denied this for decades, until finally forced to acknowledge something they euphemistically called “anti-depressant discontinuation syndrome”! Let’s call it what it is people; it’s a drug withdrawal issue. The patient goes back to the doctor and says they have stopped their medication, and feel anxious or depressed again. The doctor invariably says, ‘well that’s your depression coming back so you best just go back onto your anti-depressants.’
Even if you manage to taper off the drugs there is no guarantee that you won’t experience some major withdrawal symptoms, including increased anxiety, agitation and anger, crying spells, depressive thoughts, electric shock-like sensations in your brain, vertigo, flu-like symptoms, and potentially a few others as well. What this does is often push the person to start taking the drug again to get relief from the withdrawal. If people aren’t made aware of the withdrawal they will believe – falsely – that their original “condition” of anxiety or depression is returning. I am astounded at how many doctors and psychiatrists will agree that this is the case and that the person just needs to go back onto their medication. Family and friends – having witnessed the destruction that can occur in their loved ones life when they do try to come off anti-depressants – will unwittingly be supporting the doctors’ and psychiatrists’ assessment, and encourage their loved one to go back onto their medication. And so an awful vicious cycle continues. Sometimes, unfortunately and very sadly, it can lead to the person paying some hefty prices in terms of relationships, jobs and health. Sometimes even the ultimate price of taking their own lives.
And many, in mental agony and pain, are forced back onto the same medication or a different one, and the cycle goes on and on. I believe that, unfortunately, the longer you are on these medications the harder it may be to come off them. This may not be entirely true but it seems that way, at least to me. Having said that, I have had people write to me who have only been on them for a few months, try get off, and have major withdrawal problems. Another woman wrote to me recently saying that she had started having seizures after being on a particular anti-depressant for only a few months!
One of the biggest issues we are facing is that we just do not know the real long-term damage that these drugs may be doing to people. We do know that there is a possible link to heart disease as well as many other health problems the longer people are on them, some of which I will detail later on.
People are crying out for help; Marriages are breaking down, careers are falling apart, and the quality of people’s lives is being severely compromised. I had one man write to me saying he had been on anti-depressants for 20 years, from 40 years old to 60 years old, and during that time he had lost both his parents and had been UNABLE to grieve their loss. Why? Because whilst anti-depressants may be preventing people from feeling the very negative emotions of anxiety and deep unrelenting sadness, they also prevent people experiencing the normal range of sadness and love and joy and ecstasy that others just take for granted. It is an extremely painful realisation to think that you have lost part of your humanity because your ability to feel deeply about anything has been taken away, the good and the bad. So what are we becoming then? It raises questions of what it means to be human and if emotions are taken out of the question I don’t believe we are truly living.
I know this is deeply controversial and I know that there are many who will say that anti-depressants save people’s lives. And again let me repeat that I am not disagreeing with that, but let me put forward a potential solution to this world-wide epidemic. I highly recommend that anyone who is interested in the story of how these medications began, how they developed and where they have led us should get a copy of Robert Whitaker’s fantastic book called Anatomy of an Epidemic. I contacted Robert immediately after reading his book and he asked me to write my story for his website. There are now two parts to that story online. The third part is in the making as I continue on this path. I have written my own book about my views on anxiety, depression and all the tools that I believe are the best tools available to help without needing to resort to the medications. The book covers a range of topics such as cognitive behavioural therapy, acceptance and commitment therapy, meditation, exercise, goal setting, and mindfulness practices as well as chapters on dealing with emotion and letting go of our fears.
For the majority of medical ailments and diseases, the disease was discovered and then the epidemiology (underlying causes and history) first studied and then once fully understood through medical and scientific proof, successful cures were developed. This was never the case with depression or anxiety. Experiments with such wonderful substances such as jet fuel and clothing dye led to products which were tested on lab animals and then theories were created about why the mice or rats acted in a certain way when given these “calming” drugs and then human tests inevitably followed. After that, the psychiatric community and pharmaceutical companies got involved and the rest is history. A very sad history for the human race or at least for the poor souls who have suffered because of the neglect of the primary principle of the Hippocratic Oath that all doctors and I presume psychiatrists (and alright I will include psychologists too!) would have sworn to when they qualified in their degrees: “FIRST DO NO HARM”. This has clearly and unfortunately not been the case when it comes to some of the results from using psychiatric medication in the treatment of anxiety disorders and depression.
I will always say anti-depressants should be a last resort and only used when people are being debilitated by their condition and are not able to function normally in their world in terms of working or looking after themselves and/or other people in their lives. No-one should have to be on anti-depressants for the rest of their lives. That old story that people who need anti-depressants are the same as a diabetic who needs his or her insulin is just plain and simply not true. Talk to most doctors or psychiatrists and they will most likely tell you something along the lines of: “People with depression and anxiety need to take medication just as a diabetic needs to take insulin.”
Why? Because, supposedly, just as it is a lack of insulin causing the diabetes, similarly, it is a lack of serotonin that causes depression and anxiety. However, a closer look at the research shows that this is just not true, and has never been conclusively proven. The research that the pharmaceutical companies rely on to prove the deficiency theory is usually paid for by the pharmaceutical companies themselves. Important bits of information are either adjusted or ignored altogether such as the fact that in some of the trials, there was no clinically significant difference in serotonin levels between the depressed and non-depressed people. Another issue is that for the FDA in America to pass a drug it only needs to show it has been effective within a few weeks and there is no systematic follow-up as to how these patients fare of the longer term. Do their lives continue to improve and do they stay happy and well? Unfortunately, most of the time the answer is no.
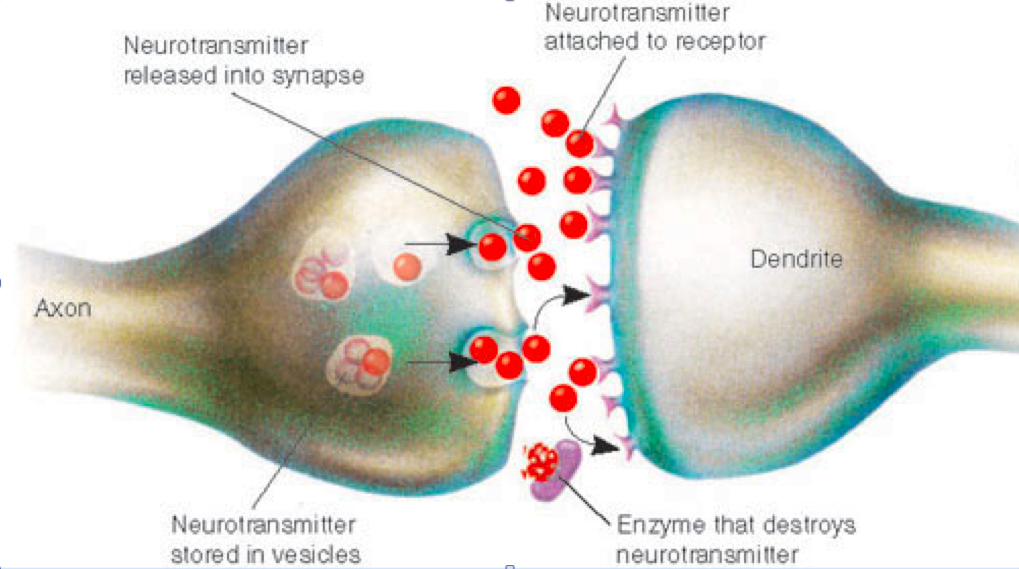
Let me add a caveat to that as well. I am not saying that serotonin doesn’t play a major part in how we feel, and it is well-known to be the mood chemical in terms of helping us feel happiness and joy. But, many people don’t really know how an anti-depressant actually works. What it does is effectively blocks the “re-uptake” of serotonin in the brain which basically means that when you have a thought, your brain sends an electrical signal between two neurons. In order for the two neurons to communicate chemicals are released in a tiny micro gap between them. Chemicals float across the gap and connect to receptors on the other neuron, and off the signal goes. Now, if there is not enough of the chemical getting through, some of what is left in the gap is taken back or reabsorbed into the first neuron. Add in an anti-depressant and what it does is block or stop the re-uptake of the serotonin chemical (hence the drugs are called SSRI -selective serotonin re-uptake inhibitors). With more serotonin available in the gap – more floats across and fires the signal off for happiness and joy etc.
Wonderful isn’t it? And that’s all we needed to know right? Pop a pill and problem solved, you’re happy again. Or are you? As the years have gone by and more and more side effects and issues has arisen over time with people taking the drugs, we are learning more and more that is just isn’t that simple and that playing around with the brain and the body’s chemistry can have some debilitating and life altering impacts. Some of these include:
- lack of libido
- loss of motor control and facial tics (I had one client come to see me who had been put on such high doses of Zoloft for so long that she had an embarrassing and highly distressing condition of legs and arms shooting out uncontrollably whenever she tried to relax!)
- increased anger and irritability
- difficulty accessing emotions both positive and negative
- delayed or lack of ability to orgasm (leading to major issues in marriages and relationships)
- ongoing and sometimes even worsened anxiety and depression whilst being on the drugs
- major problems with trying to stop taking the drug even when the actual situational factors that may have caused the depression have long since passed and people are now ready to go off and resume their lives and just want to be who they were before they started taking the drugs
- major problems with short term memory (this was even detailed as far back as 1999 in Dr. Joseph Glenmullen’s book Prozac Backlash)
- issues of the drugs just ceasing to be effective – known as the “poop out” effect (unfortunate terminology) – which is basically when the drug just stops working. And so people are moved from one drug to the next in an endless human experiment. I am sorry to say this but psychiatry is about as close to a science as black magic at this stage in our understanding of how the brain works.
If these drugs are truly the answer to anxiety and depression, answer me one little question: Have you ever been tested for a serotonin deficiency? Have you ever gone to a doctor and had a test that came up with a result saying yes indeed my friend you are deficient in serotonin and this much medication will correct the problem and you will be A okay for the rest of your life? No? Why not? Because it is extremely difficult to measure serotonin levels in the brain and body. As far as I am aware, the only way to measure serotonin levels is through your cerebral spinal fluid and even that is not a direct measure of actual levels as it is more about what is wasted or taken away by the body and then doctors would guess from that how much you have. How would we even know what the “correct” amount of serotonin would be for each individual? The medical community, only in recent times, has identified that serotonin not only resides in the brain but it resides in the stomach too. So we are playing around with people’s brains, people’s minds, and people’s quality of life in ways that we just don’t fully understand. My very real and serious concern is the impact this is having on the lives of millions of people all over the globe.
My own further research found that there are natural products that can actually help the body produce more serotonin naturally, rather than artificially increase the levels with dangerous drugs with major side effects and extreme difficulty in ever stopping them. These supplements include the well-known ones like St John’s Wort, which is the most-prescribed in Germany as they are one of the few countries trying to avoid the overuse of anti-depressant medications. Others include the natural amino acid called 5 HTP (5 Hydroxy-tryptophan). This is the basic building block that your body and brain use to make/create serotonin and dopamine. Why aren’t doctors and psychiatrists trying these methods first along with all the other known methods of relieving anxiety and depression such as exercise, meditation, yoga, counseling, CBT, ACT etc.? This is just a sampling of potential natural methods that can and absolutely should be tried before medication is indicated.
Whilst I am certainly not saying that I am an expert in the field by any means, I do believe that there are some things that the medical fraternity and government health authorities should be taking into account in terms of the prescribing of anti-depressant medications.
Here are some important questions all doctors, psychiatrists and government health authorities should be asking themselves before the prescribing of any anti-depressant medications:
- Does this patient have a psychological condition that is severe enough to warrant psychiatric drugs that may alter his or her personality, relationships, career and quality of life in general?
- If so, is this patient mildly, moderately or severely anxious or depressed? How do I know this? (In my opinion and this is in agreement with Dr. Joseph Glenmullen’s conclusions in his book – only those who are severely affected by anxiety or depression should be put onto these medications and even then for only 4-6 months until they are able to resolve their psychological issues with a therapist).
- Have I informed my patient of the 4-6 week period of adaption that may cause some significant distress to the patient and that they may need an additional anti-anxiety medication to assist with the increased agitation and anxiety until the anti-depressant “kicks in”?
- Have I warned my patient that they are more than likely to experience difficulty withdrawing from the anti-depressant, and that they will need to taper very slowly off the drug and possibly switch to one of the longest-acting anti-depressants, such as Prozac, in order to successfully come off the drug?
- Have I warned my patient that he or she may experience any or all of the following:
• Decreased libido.
• Delayed orgasm/failure to achieve orgasm.
• Increased agitation/anger.
• Difficulty accessing his or her emotions and thus ability to empathize with others.
• Potential memory loss if taken for a period of years due to the chemicals effect on the hippocampus in the brain (the brains memory site).
• (…and other side effects that I have already been mentioned earlier) - Have I arranged to follow up with the patient and his or her counsellor to assist them in getting off the drugs as soon as possible once the patient is feeling better and has resolved the primary situational and psychological issues that led to the anxiety or depression in the first place?
The sad reality is that many doctors do not even know that a patient can experience withdrawal reactions. I had a client come to see me with his wife once, extremely worried about the fact that he had been experiencing electric shock-like sensations in his brain and legs, as well as vertigo, after suddenly stopping an anti-depressant. I asked him if he had discussed coming off with his doctor and he said he had and that his doctor had agreed he could just stop taking them. When I informed the patient that this was a normal reaction and that he needed to either try to handle it – as he had not been on them for very long so it was likely he would be fine – or to go back to a lower dose and taper off, the look of relief on both their faces was amazing. He told me he thought he was either going mad or dying!
There should be much stricter controls over when a person is given these drugs and who gives it to them. There should be a formal assessment of how depressed a person really is, using a valid and reliable depression tool such as the Beck Depression Inventory and not a 10-question form filled in at the doctor’s office while the patient is in tears and feeling at their very worst. Obviously, if the person is reporting suicidal thoughts and appears to have some ideas of following through, some immediate action must be taken including letting the patient’s family know, and potentially getting an acute care mental health team involved. Starting anti-depressants for a patient such as this may be the very thing that is needed, but, once again, I question for how long? Forever? Who takes control to oversee how the patient is fairing in a few weeks, months, or years, and then assists them to taper off when the time is right? I believe this is a very important missing link in our health system, not just in Australia, but around the world from what I have gathered from the hundreds of people who have written to me over the past 3 years.
As I have mentioned, there are many tools and techniques that can be learned to help people get better and stay better, many of which I have detailed in my book along with descriptions of exactly what I believe anxiety and depression are and how they differ from stress or situational anxiety and low mood.
It is my mission to continue to talk about and help people with these and other issues in terms of living the best life they can, having the greatest quality of life mentally, emotionally, physically and spiritually. As a wise author once said: I am not saying to you that I am on the top of the mountain, all I am saying is that I have been climbing it a bit longer and I can hopefully point out some of the pitfalls and pathways that you may be encountering as you climb too.
To those of you who are struggling out there, know that you are not alone, there is a growing number of people speaking out about what has been happening to them and more people learning alternative ways to get better and stay better. I would recommend joining up with sites such as Surviving Antidepressants as well as keeping abreast on what is happening on Robert Whitaker’s Mad in America.














Agreed on most things except I think you’re too tentative and apologetic in your approach, such as defending yourself against someone’s possible accusation that you are being too “extreme” before you even start. But actually the “bold” assertions you believe you are making are standard fare at MIA, and I don’t see anything here that MIA folk would consider particularly new or extreme. I’m saying that as a good thing, i.e. to help you feel comfortable about thinking freely here without fear of being punished or fired.
Report comment
David, I agree with Oldhead. I actually feel that you are being way too timid, almost like you are apologizing for the sometimes continuing use of psych meds.
For myself I have never and would never use tobacco or street drugs, even marijuana. I have consumed alcohol, but it was decades ago and only occasionally. And it was also because it was promoted in those social environments, and I never really approved of that anyway. I don’t do it now because I see more of the trouble it causes, and so I see that it is necessary to take a firm stand. And I would never accept psych meds. Even if they attempted to administer them by force, it is very unlikely that they would succeed.
People say of for example marijuana that I don’t know it’s benefits because I have not tried it. Well I see that as an absurd argument because it knows no bounds. And besides, meditation, prayer, exercise, and tantric sex are plenty good mood alterants for me; and used well I feel very constructive. I see what marijuana does and it is the opposite of what I want.
In some other places people have called me a buzzkill, and I wear that label with honor knowing that those who call me that could never even imagine how much of an understatement it is.
One’s own experience is political, and psych meds, and I feel psychotherapy, are designed to suppress experience. So I am totally opposed to them.
I know that the bulk of the population does not yet see it this way, but I feel that as familial child abuse is exposed and the perpetrators start being held accountable, rather than the survivors sent to therapy and recovery, that this will change.
Nomadic
Survivors of the Middle-Class Family
http://freedomtoexpress.freeforums.org/survivors-of-the-middle-class-family-t243.html
Save this link in an email to yourself!
Report comment
Thanks Oldhead. Appreciate the feedback. Noted !
Regards
David
Report comment
I agree that the euphemism “discontinuation effects” should be called “WITHDRAWAL” because that’s exactly what it is. I would further suggest that the “poop-out effect” (an even more horrific euphemism) should also be called by its proper name: TOLERANCE. We need to clearly establish that there is NO essential difference in effect of these drugs to any other psychoactive drugs, including street drugs. Anyone with training in the area knows that cocaine, amphetamine, heroin, etc. all create TOLERANCE because they increase the presence of a particular neurotransmitter, and the brain/body reacts by DECREASING that same transmitter’s production and pruning off of receptors for that transmitter, a process long known as “neurological down-regulation” in the field. The drug becomes less effective because the brain adapts. Similarly, longer-term WITHDRAWAL effects are not just the result of the drug leaving the system – they are also caused by the fact that the brain’s down-regulated state doesn’t work well when there are normal neurotransmitter levels around. It takes the brain time to readjust, and it’s not clear if full readjustment happens if the person has been using a long time.
Why would we imagine that these same processes don’t happen just because a drug is prescribed????
—- Steve
Report comment
“It takes the brain time to readjust, and it’s not clear if full readjustment happens if the person has been using a long time.”
Steve, I like all that you say here re withdrawal effects. From my experience of having withdrawn after 20 years of psych drugs, there were many things going on at once that created all sorts of new neural activity and pathways, including actual issues coming up that had been suppressed by the drugs. Cells are changing and adjusting all over our bodies, not just our brains. It’s quite disorienting, to say the least. All I can call it is ‘a journey.’
The longer we are on them, the more stuff can pile on because we’re really not making core shifts. So all of that needs time to surface and process on multiple levels, including cellular. That’s a lot of energy. And at the same time our brains and other organs are changing and shifting. Multiple adjustments are happening on a body and mind level.
And I was very active in life on these drugs and interacting all the time, going to school, working, having a relationship. A lot did, indeed, pile on as the years went by, all the while my system was slowly and systematically breaking down, unbeknownst to me. Became an internal train wreck after 20 years.
Regarding “full readjustment”–it’s been 14 years since I took my last psych drug of any kind, and what followed for years was kind of epic, really. I had no idea what to expect, and I basically followed this thread as each step appeared. It was the only option that had any hope and light attached to it, all visible roads would doom me, undoubtedly.
As far as being able to focus, function, create, and be happy with how things are going, that did come back to me, after having sat in a pool of anxiety and other issues for a while. My brain felt totally scrambled of course and I was emotionally raw, but normal functions eventually came back and my emotions regulated. A lot to that shift, but that’s it in a nutshell.
Although my brain did change considerably, because I learned new things and began to address life in a different way than I had. My values, beliefs, experiences, and perspectives changed radically–as did my relationships and the quality of them–so whatever occurred with my brain from drug use to withdrawal to finding my center, I’m sure it does not look like it looked before, it has changed.
What it adapted to was my heart and spirit–the real me, not the me that was created from trauma (negative self-beliefs, non-deservedness, “I am bad” etc.)–so that is a different perspective than I had before, hence, a different brain, and definitely a different reality and life experience. Naturally, that feels a lot better to me, more relaxed and clear. You can imagine how chaotic it was during and just after 20 years of psych drugs, 9 on that last year. Messy doesn’t begin to describe it.
I’d use the word “transformation” rather than readjustment. Although there is certainly a lot of healing to do, which in this case, would be radical core change–but back to our selves, and that may be unfamiliar. Another adjustment to make after coming off psych drugs. Who the hell am I?
Report comment
Thanks Steve. Very much the way I feel about it.
Appreciate the time taken to comment.
All the best
David
Report comment
A little history. The SSRI’s got their start as a treatment for OCD, back when the only one was a tri-cyclic antidepressant with the generic name clomipramine and the trade name “anafranil”. Prozac was the next one, and because depressed folks are frequently tormented by repetitive obsessive thoughts, some “genius” decided the drug might be useful as an antidepressant. It worked for that, whereupon the pharmaceutical industry came out with a slew of them to dodge the patent on Prozac (which probably was created to dodge the patent on anafranil.
Report comment
I remember a whole slew of tricyclics — wouldn’t Elavil be one of those?
Report comment
Yes. It was less likely to lead to hallucinatory episodes than other members of this family and the earlier MAO inhibitors, which were notorious for turning depressed patients into full- blown hallucinatory psychotics.
Report comment
Hi BC
That’s something I wasn’t aware of. Thanks for pointing that out. It’s just madness what has been done. The nerve to play with people’s lives in this way.
Regards
David
Report comment
Absolutely, I agree antidepressants are being given to way too many people, and without informed concent (mine was given by a PCP, and called a “safe smoking cessation med,” so I had no clue prior to taking it, that it even was a mind altering drug). And it is shameful the medical community claims it is unaware of the common adverse and withdrawal effects of the antidepressants. In my case the common symptoms of antidepressant discontinuation syndrome:
https://en.m.wikipedia.org/wiki/Antidepressant_discontinuation_syndrome
Were misdiagnosed as “bipolar,” despite the DSM-IV-TR specifically stating this was a misdiagnosis (and these ADRs were misdiagnosed as “bipolar,” “depression caused by self,” and “paranoid schizophrenia” by two paranoid PCPs, a psychologist, and two psychiatrists within two weeks, according to my medical records – so much for the validity or reliability of the DSM disorders). And I was heartbroken to learn, from reading “Anatomy,” that over a million American children were similarly misdiagnosed as “bipolar,” due to the common ADRs and withdrawal symptoms of the antidepressants and ADHD drugs.
And my research has found that today’s “bipolar” drug cocktail recommendations:
http://www.mayoclinic.org/diseases-conditions/bipolar-disorder/basics/treatment/con-20027544
Which include combining the antidepressants with the antipsychotics is already medically known to make a person “mad as a hatter” / “psychotic,” via a known drug interaction issue called anticholinergic toxidrome.
https://en.m.wikipedia.org/wiki/Toxidrome
And I do have proof in my medical records that psychiatrists can not distinguish the central symptoms of anticholinergic intoxication syndrome:
http://www.drugs.com/interactions-check.php?drug_list=2330-1540,1744-1113&types%5B%5D=major&types%5B%5D=minor&types%5B%5D=moderate&types%5B%5D=food&types%5B%5D=therapeutic_duplication&professional=1
From the “classic symptoms of “schizophrenia” or “bipolar.” But this is because the only difference between the central symptoms of poly pharmacy or neuroleptic induced anticholinergic intoxication syndrome, and the positive symptoms of the theorized “schizophrenia,” is “hyperactivity” vs. “inactivity.” And the neuroleptics do make all humans ungodly tired.
But this means that starting millions of people on the antidepressants, especially since the PCPs and psychiatrists claim to have no idea of any of the adverse effects of the psychiatric drugs, and since they are seemingly unable to even read the warnings within their own scientifically invalid DSM “bible,” is extraordinarily unwise. Unless the goal is to make millions of people ungodly sick, for their entire life, for profit.
But, of course, this is the opposite of the promise made by doctors, to “first and foremost, do no harm.” Thanks for speaking out about the harms of the antidepressants, David.
Report comment
Hi someone
Wow, sorry to hear about all of that. Just shocking the number of disagnoses that happen. And that leads to the whole issue of the DSM being the “bible” of what is considered to be normal. Great book called “saving normal” by Allen France’s who actually oversaw the writing of the DSM Iv – revolting against all the new categories being created to capture more levels of abnormality. Very soon we will be classified as mad because we choose to wear funny coloured clothes or choose to laugh at too many jokes.
Report comment
And being put into an antidepressant for smoking cessation is just pure madness. That dr should be struck off the register
Report comment
That combination of antidepressant and antipsychotic drugs reminds me of the result of treating belladonna intoxication (e.g. jimsonweed, fly amanita) with antipsychotic drugs and having the emergency room and everything and everybody in it trashed by a berserk patient.
The guys who dreamed that drug combination up should have read RG Wasson’s hypothesis that the Viking berserkers of the European dark ages worked themselves into their frenzies by chowing down on (anticholinergic) fly amanitas until they were ready to rave.
Report comment
“One of the lessons I have had to learn is that not all people who have letters after their names are actually “gods,” or even people who have special powers to know things about us that is more important than we can learn about ourselves, about our own bodies, and our own minds.” I agree 100%. A caveat? Not every person with lived experience has special insight either. “Expert” is a cheap label.
Report comment
Since the author practices in Australia, it would be interesting to learn what effective alternatives would be readily available to Australians if antidepressant use were to be reduced by half. Since 2000 Australia’s rate of anti-depressant use has doubled and it is now the second highest in the OECD. Would Australians be able to access high quality non-medication treatment from a therapist well versed and successful in the treatment of depression?
Report comment
Not sure exactly what was passed/changed, but I know a few years ago they were talking about changing the mental health treatment options to allow for 12 (I think it was 12 with the option of another 6) psychological appointments or up to 50 psychiatric appointments to be handled by medicare. But just like America and other Western countries the emphasis has increasingly moved away from social/psychological/environmental towards biological/medical. Heck, in 2012 the Mental Health Bill proposed for Western Australia even promoted sterilization for children (aged 12 and older I think it was), though I’m fairly sure the eugenical sterilization clause was removed after massive public outcry (I live in WA and went to 3 of the public meetings for the Mental Health Bill to oppose it).
As for what type of non-medication options are available, it’s typically the same as other Western countries with regards to therapy (CBT, psychodynamic, counseling, etc).
Report comment
Looks like you have your answer below. :))
There is a fair amount of support here. It’s 10 sessions a year in terms of government rebate for each psych session but it depends on how much the psych charges too. There are more and more apps coming up to help people and there are more people being able to access help through free chat help lines and phone services but this obviously doesn’t replace the benefits of face to face counselling with a trusted therapist.
Thanks for the comment.
Report comment
If depression is the result of not enough serotonin in a person’s system why is it that people who had their serotonin levels reduced on purpose did not become depressed?????? There were experiments done where they lowered peoples’ levels of serotonin to see if depression followed and nothing happened. They did not get depressed.
As far as I’m concerned SSRI’s and all the other “antidepressants” are a rip off, plain and simple. I don’t think they do what they’re supposed to do at all and if they “work” at all I think it’s the placebo effect taking hold. I know that some people claim that their lives were saved by these damned drugs and that’s just fine and dandy for them if they want to say that, but I don’t really believe it.
I took huge doses of Effexor for a number of years and all it did was numb me to my emotions and feelings and turned me into a damned zombie. I didn’t care if I lived or died.
The other thing that I wonder about all the time is this; serotonin is a regulator that is found all through our system. The stomach has probably the largest amount of serotonin of all the places it’s found. What are SSRI’s doing to other parts of our bodies where serotonin is found, other than in just our brains. I can’t imagine that they are just affecting the serotonin in our brains and no where else. To me this would be like saying that when shock treatments are used that the electricity only effects the bad cells in the brain ( I actually heard a psychiatrist say this one time). These toxic drugs have to be affecting many parts of our body other than just the brain itself. Is this why we get all of the so-called “side effects” like sexual dysfunction and all those other wonderful things?
Report comment
I think the numbing effect IS what they do. I think for some people, who are hyper-concerned with what other people think about them or whether they are measuring up to some outside standard, a small degree of numbing feels good, because they’re able to say, “Who cares what my mom thinks? I’m going to do what works for me!” But for others, numbing itself is probably very uncomfortable, and for a small but significant number, it becomes dangerous, because they no longer care about the consequences of their actions and are now willing to do things that they previously only fantasized about, like running an airplane full of passengers into a mountainside or shooting up a school or shopping mall.
Calling them “antidepressants” is, indeed, a huge fraud. Perhaps they should be called “numbing agents” so people who are taking them will know what they’re really getting into.
Or perhaps they simply shouldn’t be prescribed by doctors at all.
—- Steve
Report comment
Have you watched the video in Phillip Hickey’s post today. It poses an interesting hypothesis that these things are being used to structure society so that we will quit worrying so much about the inequities and unfairness of so many things that are going on and instead we will numbly go about our jobs and family life kind of like robots Spitzer talks about how the DSM and psychiatry has overmedicalized and pathologized normal things about living and speculates that this may happen at levels of 20 to 30% of people. It’s really interesting and supports what you say here about the numbing effect. This numbing effect comes in handy for corporations and big business and government and many other organizations.
Report comment
True words! The psychiatric worldview removes all responsibility from the power elite for social conditions and blames anyone who is unhappy or protesting by “diagnosing” them with not supporting the status quo. Remember “Brave New World” and Soma? “A gramme is better than a damn!” Prophetic.
Report comment
It’s actually kind of frightening. Fiction becoming reality right in front of our eyes; if we aren’t too blind to see it.
Report comment
Why would the SSRIs expand other wise – its got to be a conspiracy.
Report comment
There is even a sleep-inducing drug whose trade name is (or was) “Soma.” I found it quite chilling!
—- Steve
Report comment
If they actually call it Soma what do you think the odds are that it was named by someone who had read Brave New World and didn’t get it?
Report comment
“I think the numbing effect IS what they do. I think for some people, who are hyper-concerned with what other people think about them or whether they are measuring up to some outside standard, small degree of numbing feels good…”
Yes, and it hides the fact that this person is attached to what others think, which is inherently disempowering and self-alienating.
Good healing would focus on detaching from what others think or from society’s standards (which are no measure of health and well-being, as we all know), and guiding that person to feel comfortable in their own skin and on their own path, regardless of outside judgment. Healing self-judgment is powerful healing and brings tremendous changes, because only then can we feel our own light and create from that.
Anti-deps or any numbing agent only embeds this dependence on approval so the low self-esteem and lack of independent thinking never shifts. This serves no one to any positive end, other than those wanting only to control others for the sake of their own wealth, prestige, and power. In the meantime, people are walking around completely dissociated from themselves, thanks to these drugs, and that creates only chaos, which I think is evident.
Report comment
And I believe that this is what is referred to as textbook “vampirism.”
http://www.drlwilson.com/articles/vampirism.htm
Report comment
Alex,
If a person doesn’t think about “the other people” they disappear.
Report comment
Fiachra, yes, that is a great point. That is empowering, we have control, here. Where we choose to focus is what we are creating in that moment. So if we shift focus, we can “un-create” the first thing and create another thing. I think at the core, change is that simple. To my mind, it’s just a matter of following the path of evolution.
Report comment
Of course, I agree. Losing connection to others is tantamount to losing our humanity. It’s never a good thing to reduce someone’s empathy for others. Leads to bad ends, like mass murder in some cases!
—- Steve
Report comment
Hi Stephen
Fascinating study !
Well again proves that we are not really sure that it is serotonin that is the issue. Certainly agree that we don’t know how much the drugs are impacting other areas of the body and brain but we can certainly get an idea with regards to reported side effects such as sexual dysfunction, memory issues and lack of emotional depth.
I truly hope that more people become aware of their choices and seek alternative help before they decide to start with anti depressants.
Report comment
Why would you give these drugs to someone who is “seriously depressed” or suicidal?! Do you really pretend to believe they work? Or would you just be another person desperate enough to do harm to help somone? The fact of the matter is that if anti-depressnts worked at all, especially in these so-called really serious cases, the US suicide rate would have dropped dramatically ever since doctors had these drugs for use. But in fact since the 1950s suicide success rate has decreased only slightly (it varies yearly) and was exactly the same in the 1960s. None of which proves anything except that whatever these drugs do, they decidedly do NOT REDUCE suicides or the rate at which deoressed people kill themselves, which seems to me to be not only the gold standard, but pretty much the one standard that ought to make or break them as useful. But doctors go on prescribing them like candy and writers who purport to be against their use insist that they remain useful in these most dire of cases. Well, if so, i would need some proof! So far i ain’t seen any.
Report comment
I am certainly very uncomfortable when any client of mine decides to start taking anti depressants. I don’t prescribe them. I’m not allowed to as a psychologist and thank god for that. I just try to give them all options short of having to taking them and outline the possible side effects and long term problems they may experience plus the difficulty with coming off. It’s then up to them whether they decide that they will go ahead.
Report comment
If anti-depressants, so-called, worked at all, especially in “really serious” cases, the US suicide rate would have dropped dramatically ever since doctors had AD drugs for use. But in fact since 1950 the suicide success rate has decreased only slightly (it varies yearly) and was exactly the same in 1960 as in 2015. None of which proves anything except that whatever such drugs do, they decidedly do not reduce the rate at which depressed people kill themselves, which seems to me to be not only the gold standard, but pretty much the one standard that ought to make or break the reputation of these chemicals as useful.
Report comment