
In November 2013, the journal Schizophrenia Research published a paper by Tsuji, T., et al., titled Premorbid teacher-rated social functioning predicts adult schizophrenia-spectrum disorder: A high-risk prospective investigation. Here’s the abstract:
“Social functioning deficits are a core component of schizophrenia spectrum disorders, and may emerge years prior to the onset of diagnosable illness. The current study prospectively examines the relation between teacher-rated childhood social dysfunction and later mental illness among participants who were at genetic high-risk for schizophrenia and controls (n=244). The teacher-rated social functioning scale significantly predicted psychiatric outcomes (schizophrenia-spectrum vs. other psychiatric disorder vs. no mental illness). Poor premorbid social functioning appears to constitute a marker of illness vulnerability and may also function as a chronic stressor potentially exacerbating risk for illness.”
The study was done in Denmark by a Danish-American team, as part of a large scale longitudinal developmental study. Studies of this sort are often done in Denmark, incidentally, because the Danes have a central mental health register and other data bases that facilitate the gathering of follow-up information.
The social functioning measure consisted of five items, each of which was rated on a five point scale. The total score was obtained by adding the five individual item scores. Lowest possible score was 5; highest possible score was 25. The items were:
1. The child does not seem to take part when the rest of the class is having fun.
2. The child has no friends.
3. The child is often teased.
4. The child does not actively seek friends.
5. The child seems to avoid contact with other children.
Here are some more quotes, interspersed with my comments:
“Results suggest that, even though many psychiatric difficulties are associated with deteriorations in social functioning, teacher-rated social deficits among school-age children appear to represent a marker of vulnerability specific to disorders within the ‘family’ of schizophrenia spectrum illnesses. These findings highlight the value of teachers in identifying key markers of risk such as social deficits.”
In the abstract quoted earlier, the authors acknowledge that “social functioning deficits are a core component of schizophrenia spectrum disorders.” [Emphasis added] With this in mind, it seems to me that the best and most parsimonious way to conceptualize the research finding is that children who have poor social skills will, in many cases, grow up to be adults with poor social skills. In particular, there seems to me no justification (other than psychiatric dogmatism) to conceptualize the matter in medical terms, and to impose a medical framework – “a marker of vulnerability” – on the data.
“Thus, social functioning has emerged as an important area for researchers interested in the core features of emerging psychotic illness . . .”
Here again, note the assumption of an “emerging…illness.”
“. . . results from this 48-year longitudinal record suggest that children on a trajectory toward schizophrenia-spectrum disorders demonstrate interpersonal deficits early in life, and that teachers provide valuable information regarding children’s social functioning.”
Again, note the medical language: children with poor social skills are “on a trajectory toward schizophrenia spectrum disorders.” The term “on a trajectory” also entails an element of inevitability, implying that children with poor social skills become psychotic in the same way that people who inherit the Tay-Sachs gene get the disease. Note also the identification of teachers as sources of “valuable information.”
A follow-up period of 48 years (1959-2007) is impressive in a longitudinal study, and it is likely that the findings will be afforded a high measure of credibility and status within the psychiatric community. A Google search on May 14 for the title got 7,770 hits. So the study is attracting attention.
In recent years, organized psychiatry has been actively promoting the notion of early intervention in schools and other settings for people who are considered “at risk” for acquiring a diagnosis of schizophrenia (e.g. here and here). The DSM-5 workgroup promoted the “diagnosis” of attenuated psychosis syndrome, as a means of identifying teens considered to be “at risk,” and this “diagnosis” is included in the manual as a specific example in the category: “Other Specified Schizophrenia Spectrum and Other Psychotic Disorder 298.8” (p 122).
In this general context, a simple (5-item) teacher-completed social skills rating scale is likely to have considerable appeal. For these reasons, it seems important to subject the study to some scrutiny.
Social Skills and “Schizophrenia”
Perhaps the study’s most significant shortcoming is the one already mentioned: that poor social skills are in fact the primary defining feature of DSM-5’s “schizophrenia spectrum and other psychotic disorders.” The defining features of these psychiatric “diagnoses” are set out on pages 87 and 88 of the manual, and include the following, all of which fall, I suggest, under the heading of social skills deficits:
- reduction in the expression of emotions in the face
- showing little interest in . . . social activities
- diminished speech output
- lack of interest in social interactions
- childlike silliness
- lack of verbal . . . responses
- staring
- grimacing
- mutism
- echoing of speech
- switching topics
Even delusions and hallucinations, the cornerstones of these “diagnoses,” are closely connected to social skills. A child who grows up with poor social skills is often victimized and bullied, and quickly learns that the “real” world is not usually a source of joy or reward. The subsequent retreat into a private realm is not only understandable, but in many cases adaptive.
So when Tsuji et al. discovered, through their research, that children who are rated by their teachers as socially unskilled, have a better than average chance of attracting a “diagnosis” of a schizophrenia spectrum disorder in adulthood, all that they have found is that some individuals, who are socially unskilled as children, are socially unskilled in adulthood. Poor social skills is an inherent component of the definition of “schizophrenia.” The notion that this needs to be discovered as a “marker of vulnerability” is specious and misleading.
False Positives
The study write-up is sparse in both description and data, so it’s not possible to subject the numbers to serious scrutiny. But it is clear that many of the participants who were rated poor on social skills during childhood grew up to have “no mental illness” in later life. The authors do tell us that the “. . . [s]ocial functioning scores ranged from 6 to 25 with an overall sample mean of 20.83 (SD = 3.78).” They also provide means and standard deviations for the three outcome groups.
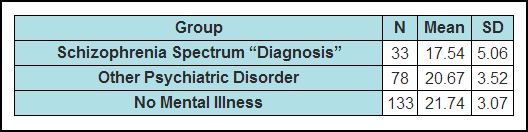
It should be noted that the above table does not appear in the text, but was created by me from data presented as run-on text in three separate sections of the paper. (Higher scores mean better social functioning)
What’s immediately clear from this table is that there is considerable overlap in the social skills scores from the three outcome groups. We can get an estimate of the range of the three groups from the standard deviations. Most of the participants’ scores will lie in the range from two SD’s below the mean to two SD’s above the mean. So we can calculate tentative score ranges as follows: (The range for all scores was 6-25, so 25 is always the upper limit.)
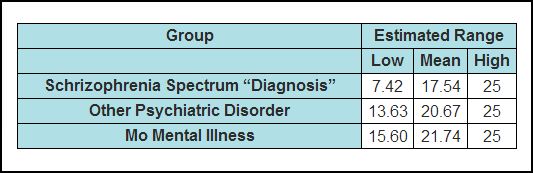
It is reasonably certain that many of the low scorers in the NMI group scored below the mean of the schizophrenia spectrum group, and yet these individuals had never been assigned a mental illness “diagnosis” of any kind. It’s not possible to say, based on the published data, what the absolute numbers were, but given that the NMI group is four times larger (133 vs. 33) than the spectrum group, it is entirely feasible that there were as many, or even more, individuals in the NMI group scoring below the “spectrum” mean (17.55) as there were in the spectrum group. Using the spectrum mean (17.55) as a prognostic cutoff would have created the prediction that these individuals were on the so-called trajectory to a schizophrenia spectrum disorder. But in fact they acquired no mental health “diagnoses” at all. So using this social skills scale, or indeed any similar scale, is likely to “identify,” and target for psychiatric treatment, large numbers of individuals who in fact were “on a trajectory” to “no mental illness.”
And there’s another problem. Of the 33 individuals who received a diagnosis of a schizophrenia spectrum disorder in adulthood, only 18 of these had been assigned a diagnosis of schizophrenia. The remaining “diagnoses” were:
Psychosis NOS or delusional disorder 8
Schizotypal, paranoid, and schizoid personality disorder 7
The authors state that their decision to group these categories together was “…guided by familial research suggesting genetic links between the disorders…” However, it is entirely possible that the grouping was done to increase the size of the high “pathology” group in order to make the association seem more robust. It is also possible that the data was pre-examined and it was noticed that a large proportion of the poor-social-skills group had been assigned these other diagnoses in adulthood.
I have no way of knowing if any data massaging of this sort happened. But the decision to group the diagnoses in this way, coupled with the sparseness of data in the write up, raises questions. At the very least, it increases the chances of a predictive “hit” by the simple expedient of widening the target.
Another troubling aspect of the “diagnosis” grouping is that the authors are not using the term “schizophrenia spectrum disorders” in the same sense as DSM-5. In particular, the authors have included the conditions known as paranoid and schizoid personality disorders, neither of which is included in the DSM-5 grouping. This, I suggest, is important for two reasons. Firstly, most readers on coming across this term in the title and in the abstract, would have assumed that it referred to the DSM-5 category. At the very least, the authors should have stated explicitly that this is not the case – that in fact, they were using the term differently. Secondly, and more importantly, the behaviors entailed in the paranoid personality and schizoid personality labels are entirely a function of social skills. It is likely that individuals who meet these general descriptors would score very low on a social skills scale at age 11-13, and this may have been a major factor in depressing the overall score of the spectrum group.
Many credible accusations of data massage have been leveled at psychiatric researchers in recent years, and in this regard it would have been helpful if Tsuji et al. had published some more numerical data. Even the means and standard deviations of the “paranoid” and “schizoid” personality groups would have been useful.
Predictive Value of the Results
As mentioned earlier, the title of the article is Premorbid teacher-rated social functioning predicts adult schizophrenia-spectrum disorder: A high-risk prospective investigation.
This, I suggest, is misleading. The social functioning risk ratio for no mental illness vs. spectrum disorders was only 1.31 (with a 95% confidence interval of 1.17 to 1.46). This does not indicate high predictive potential. To illustrate this, imagine 100 envelopes spread out on a large table; 50 red and 50 blue. A person is informed (truthfully) that half of the blue envelopes contain a $100 bill and the other half contain a go-to-jail-now card. With the red envelopes, the odds are better – 19 jail cards and 31 $100 bills. The person is invited to choose one envelope and open it. If it is a jail card, he will be incarcerated. If it contains a $100 bill, he gets to keep it. Obviously, other things being equal, he should choose a red envelope, but he still runs a 38% chance of going to jail, versus a 50% with the blue envelopes. The risk ratio for blue to red is about 1.31. So, yes, the color red does predict dollars over jail – but the potential for error (i.e., jail) is still high. Similarly, if a person were to use the five item social skills scale described in this study to predict a “schizophrenia spectrum disorder” in adulthood (odds ratio also 1.31), his prediction would be false a great deal of the time. The word “significantly” in the abstract refers only to statistical significance, and indicates that the result is unlikely to have occurred by chance. It has no bearing on the magnitude of the effect.
A more accurate title for the paper would be:
“Teacher-rated social functioning at age 10-13 (as measured by a five-item scale) is correlated modestly with acquiring a diagnosis of schizophrenia, or psychosis not otherwise specified or delusional disorder or schizotypal personality disorder or paranoid personality disorder or schizoid personality disorder, in adulthood.”
Social Skills
The great tragedy in this area is that poor social skills is an eminently remediable condition. Social skills can be taught as easily, and as readily, as counting, spelling, and playing simple games. Children, for instance, who are excessively boastful, which in later life will attract the label “grandiosity,” can be coached successfully to downplay their self-promotion and to pay compliments to others. Ordinary conversational skills such as making eye contact, admitting to mistakes, smiling, allowing others an opportunity to speak, etc., can all be coached without difficulty. Conscientious parents have been doing this since the dawn of civilization, and probably even earlier.
Unfortunately, however, in the present time this kind of teaching often doesn’t take place. While children who can’t count or read attract lots of remedial attention, the lack of social skills is somehow seen as an inherent defect that doesn’t lend itself to coaching. Social skills are often conceptualized, even by teachers, as an integral part of “the child’s personality,” or as indicators of “deeper” problems, rather than skills that can be acquired, practiced, and cultivated in the normal way. Children with deficits in this area are often sent to the mental health center, where they acquire various “diagnoses,” and are given the false and disempowering message that they are sick. The Tsuji et al. study will lend unwarranted credence and support to this practice, in that it will be used to promote the notion that these individuals are “on a trajectory” to a “schizophrenia spectrum disorder,” and that this “trajectory” can be altered only by timely psychiatric intervention.
It is also the case that some people, children and adults, don’t want to socialize. They prefer their own company, and often excel in various non-social areas. The present drive towards “early intervention” will pathologize these individuals, and will draw them into psychiatry’s disempowering and destructive net – for their own good, of course.
Authorship
Although Thomas Tsuji (a sixth-year grad student in the UBMC Department of Psychology) is shown as first author, it is clear the Jason Schiffman, PhD, is the principal investigator. Under the heading “contributors,” the article states: “Dr. Schiffman formulated, conducted, and/or oversaw the study design, data analysis, data interpretation and manuscript preparation.” Dr. Schiffman is also listed as the “corresponding author,” with an address at the University of Maryland, Baltimore County (UMBC). You can see his UMBC bio here. His listed research interests are: “Early identification and treatment of youth at risk for psychosis. Reduction of stigma against people with serious mental health concerns.”
Some of Dr. Schiffman’s recent research publications are also listed. Here are two quotes from these studies:
“Brief self-report questionnaires that assess attenuated psychotic symptoms have the potential to screen many people who may benefit from clinical monitoring, further evaluation, or early intervention.” (here)
“The validation of attenuated symptoms screening tools is an important step toward enabling early, wide-reaching identification of individuals on a course toward psychotic illness.” (here)
Dr. Schiffman is also on the staff of the Center for Excellence on Early Intervention for Serious Mental Illness. This agency was created last year by a $1.2 M grant from the State of Maryland as part of the state’s response to the problem of mass shootings in schools and other locations. The center is headed by Robert Buchanan, MD, a professor of psychiatry at University of Maryland. Dollars for Docs indicates that Dr. Buchanan received $34,520 from pharma in the period 2009-2012. Information on the Center’s activities to date is sparse, but I did find two Baltimore Sun articles about the Center. The first article, titled New Maryland mental health initiative focuses on identifying and treating psychosis by Jonathan Pitts, was published on October 21, 2013. Here are two quotes:
“Research has shown those who eventually develop psychosis have often exhibited early warning signs, clues that give family members, teachers, health-care providers and others a chance to intervene early, if only they know what to look for.”
“The Clinical High-Risk program will be contacting schools, houses of worship, law enforcement and other communities that come into contact with youth to promote public awareness about such signs, Schiffman said, and clinicians will be available to provide testing and offer treatment options.”
The second article, written by Jean Marbella, was published on March 21, 2014. It’s titled UMBC study among efforts to increase awareness of mental illness. Here are some quotes:
“‘Many of the folks who need help get lost somehow,’ said Jason Schiffman, an associate professor of psychology at the University of Maryland, Baltimore County who is heading the study. ‘There are so many kids and young adults who slip through the cracks.'”
“Schiffman has long been interested in early intervention and de-stigmatization programs for those suffering mental health problems, but more recently, his work is benefiting from a new focus on the role such illnesses may have played in some shootings.”
And perhaps most telling of all:
“‘As a society, if we normalize the seeking of help,” he said, “people are more likely to seek that help.'”
There is it: psychiatry for all. A “diagnosis” for every problem and a pill for every “diagnosis.”
Summary
And so it goes. Psychiatry, reeling under an ever-increasing barrage of criticism, has taken nothing on board with regards to its spurious concepts and its destructive treatments. Instead, it has hired a PR firm to polish up its image, and is actively cultivating the media and the politicians, with a view to embedding its concepts and practices more deeply into the legal and social fabric of our society. It is also exploiting shamelessly the public concern about the mass murders to promote its own expansionist agenda, indifferent to the stigmatizing effect that this will have on millions of innocent, socially isolated teenagers..
A great deal of their present effort is directed at two main themes: integration of psychiatry with primary care (a mental health worker in every GP’s office), and early intervention. Watch out for media infomercials on these topics in your local newspapers, and for bills on these topics in your statehouses. And please speak out. Early intervention is just a catch-phrase to sell more drugs to children and to destroy more lives.
* * * * *
Disclaimer
In critiquing a paper like Tsuji et al., it is difficult to avoid using psychiatry’s terminology. My use of the terms “schizophrenia,” “schizoid personality disorder,” “schizophrenia spectrum disorders,” etc., should not be taken to imply any endorsement on my part of the validity of these concepts. On the contrary, the central theme of my website is that these terms have no ontological or explanatory significance, and are nothing more than loosely defined labels which psychiatry uses and promotes to legitimize the prescription of psychiatric drugs.
This article appears on Philip Hickey’s website
Behaviorism and Mental Health











Hopefully, one day soon, the study of genomics is going to bury these dinosaurs. Here’s a great article— http://www.psmag.com/navigation/health-and-behavior/the-social-life-of-genes-64616/
It’s long, but it tells great stories about research into gene expressions. It starts with bees. Here’s an excerpt from the part, near the end, about research in human psychology:
“Kaufman laid both the kids’ depression scores and their SERT variants across the kids’ levels of “social support.” In this case, Kaufman narrowly defined social support as contact at least monthly with a trusted adult figure outside the home. Extraordinarily, for the kids who had it, this single, modest, closely defined social connection erased about 80 percent of the combined risk of the short SERT variant and the abuse. It came close to inoculating kids against both an established genetic vulnerability and horrid abuse.
Or, to phrase it as Cole might, the lack of a reliable connection harmed the kids almost as much as abuse did. Their isolation wielded enough power to raise the question of what’s really most toxic in such situations. Most of the psychiatric literature essentially views bad experiences—extreme stress, abuse, violence—as toxins, and “risk genes” as quasi-immunological weaknesses that let the toxins poison us. And abuse is clearly toxic. Yet if social connection can almost completely protect us against the well-known effects of severe abuse, isn’t the isolation almost as toxic as the beatings and neglect?”
An adult who knows how to have a conversation with a child to find out what’s going on with them and letting the child know that someone cares— is that too much to ask? Any effort to find out what is “wrong” with the child as if there were nothing that would make a child have difficulty socializing and adapting but mental illness, is madness itself. Why aren’t these adults—- you know— adult? What color is the sky on their planet? Do they remember what it was like to be a child? Have they never suffered anything that might make them recognize and understand states of grief, shock, fearfulness, neglect, or any other unpleasant to miserable states that didn’t strike them out of the middle of nowhere, but were actually rooted in a real loss or deprivation?
Do they not know anything about being human? Who are these robots?
Report comment
Wileywitch,
I agree. All “mental illness” problems are ultimately understandable, and remediable, in terms of ordinary human interactional dynamics. On the other hand, spuriously medicalizing these problems is almost a guaranteed recipe for making everything worse.
Report comment
It’s called epigenetics and it’s a thriving area of research. Epigenetic changes can be written and re-written over the course of an individuals life and passed to their offspring.
In any case, there is already good evidence that most if not all “psychiatric disorders” have a dominant social component. We are social species and when we lack meaningful relationships it creates all sorts of problems. There is no pill for that…
Report comment
Dr. Hickey, I can find many ways to continue lines of reasoning through the topics in these helpful rundowns that you present.
For one thing, it is not hard to find scholarly or technical papers that admonish against the dogmatic conception of disease for “mental illness”. But then in research papers, as if all questions regarding freedom and power are moot, and the logic of naming and locating psychiatric diseases was implicit in the physiological make-up of human beings, the discussions from front to back assume that nothing can go wrong, not with dogmatic conceptions, not with subjective discriminations, not with live and unruly disputation that worsens with the quick and dirty arbitrations of biomedical psychiatry.
Report comment
Travailler-vous,
Yes. One could literally write volumes about every facet of this matter.
Report comment
Dr. Hickey,
As usual, another great article exposing the fraud of medicalizing typical human behavior depending on one’s environment as “mental illness.”
I am very impressed by your take on the problem of poor social skills that can begin in one’s youth and dog one throughout one’s adult years. You wisely point out that bullying at school can be a cause of such seemingly poor social skills when it is difficult for one to want to collude with and enable one’s own oppressors or seek further companionship with them. Often, teachers instigate or collude with such bullying through ignorance or malice. Also, dysfunctional families or what Daniel Shaw calls “traumatic narcissists” can destroy a child’s esteem and confidence while modeling horrible communication and lack of social skills.
http://www.amazon.com/Traumatic-Narcissism-Relational-Subjugation-Perspectives/dp/0415510252
Since you say that poor social skills can be taught, changed, improved and give some great examples without blaming or humiliating the victims, I was wondering if you can recommend some of the best books or other resources in your opinion to help one improve their social skills and confidence in social interactions. The reason is that somebody I care about recently said they feel alone and isolated because they never had/have good social skills. Like you, I said social skills are learned and not ingrained at birth, but since there is such a glut of books of the Dale Carnegie type, it’s hard to know what is the best approach as a “non-expert.”
I am an avid reader of your very enlightening and refreshing web site and articles/comments at MIA too though I don’t always comment to avoid the “repetition compulsion” in my outrage against the biopsychiatry/Big Pharma cartel.
I especially appreciate the fact that you pull no punches and call a spade a spade with regard to the biopsychiatry/Big Pharma cartel.
Report comment
Donna and travailler-vous you reminded me to thank Dr. Hickey, thank you. It’s refreshing— alarming, but sober. Thank you, Dr. Hickey, for speaking up for the children and taking the “adults” to task for their little word games.
Donna, that book looks fascinating and too expensive. Having grown up with a traumatic narcissist or sociopath, to be more exact, I found a lot of great help with counseling from psychiatrists and psychologists in the eighties. We did a lot of work on “the tapes”—- the internalized voices of sick parents. I also worked on it myself for a year outside of counseling with mindfulness until I finally stopped beating myself up with the words and toxic projections of my trauma-inducing parents. At times I was absolutely floored by the things I was saying to myself. No wonder I felt so sh***y sometimes. I completely divorced that side of my family when I realized that there was no way to relate to them without being a pawn in their psycho-drama and playing the family scapegoat who was supposed to ask them to forgive me for what they’d done to me.
A book called “The Gentle Art of Verbal Self-Defense” helped me a lot way back when. I’m thinking I should order another copy and review it all. It’s harder to deal with people socially when those tapes are playing. It’s hard to tell when one is being bullied when one is bullying one’s self. With some practice, it becomes easier to spot and deflect bullies around and inside us so that social situations aren’t so loaded and stressful.
There was a time when some people in psychiatry/psychology said that victims of sexual abuse “seek out” abuse, as if it took a lot of dedication to find a person who would sexually assault them or their child(ren). I’m pretty sure that what happens is that people who were raised by one or more sociopaths have had to turn the alarms off because they had to in order to psychically survive an inescapable situation and threats of more and worse harms for defending one’s self. Predators have an uncanny ability to spot and test people whose alarms aren’t working. Being raised by a sociopath/narcissist messes up boundaries in such a fundamental way that restoring one’s own dignity and integrity (once out of harm’s way) requires re-parenting oneself with kindness and patience.
Having a good friend to talk about social situations and possible responses means the world, too. I’m grateful for all the guidance and inspiration I’ve received from many people, from all walks of life. There is so much that can be learned and unlearned. The objectification being carried out by psychiatry and its institutional drive to medicate as many people as possible by extending the definitions of mental illness to the degree that young people can be damned for expressing what they’re living instead of what two institutions think they should be expressing because ka-ching! is FUBAR. Absolutely unacceptable!
Report comment
Hi wileywitch,
Thanks for your comment and validation of my own reality based on your own experience and input. It sounds like you’ve come a long way through much hard effort and pain while being fortunate enough to find therapists/helpers able or willing to validate your experience and support you through it. Your story is very inspiring and I agree with you that you have to do reality checks from time to time since you really have to pinch yourself when confronting the horrible tactics of the character disordered.
This is explained at the great web site, What Makes Narcissists Tick:
http://narc-attack-mirror.blogspot.com/
I agree that the book, Traumatic Narcissism, I cited above is expensive, so as much as I’d like to buy it along with many other books I am holding off with the hope a less expensive used or other copy might be available later. However, the concept conveyed by this author really floored me since though I was aware of the nasty tactics of the character disordered, Daniel Shaw’s concept of their traumatic subjugation of their victims while robbing them of their very selves and reality through many abusive, gas lighting, crazy making tactics really nailed it in my opinion unlike anyone else I’ve read.
But, you can read quite a bit about the author’s ideas by clicking the “Look Inside” feature on Amazon and you will come to a reader with a table of contents, index and many sample pages from the book that are quite enlightening in the meantime. Also, if you google the author, the book and the words “traumatic narcissism” lots of articles by and about this author, book and the concept come up, which are also enlightening.
http://www.amazon.com/Traumatic-Narcissism-Relational-Subjugation-Perspectives/dp/0415510252#reader_0415510252
One of the best books on verbal/emotional abuse in my opinion is:
The Verbally Abusive Relationship by Patricia Evans. Her follow up book, Verbal Abuse Survivors Speak Out is also excellent.
http://www.amazon.com/The-Verbally-Abusive-Relationship-recognize/dp/1440504636
http://www.amazon.com/Verbal-Abuse-Survivors-Releationship-Recovery/dp/1558503048/ref=la_B001JPCCWY_1_5?s=books&ie=UTF8&qid=1400186717&sr=1-5
Although these two books deal with marital and other male/female relationships, the complete and thorough description of most if not all verbal/emotional abuse tactics is excellent and very helpful for any type of relationship since this pulls the wool OFF your eyes to see why abusers use these deplorable tactics.
Finally, in my opinion, one of the very best books on narcissistic abusive violence is Stalking the Soul by psychiatrist Marie-France Hirigoyen who also explains this type of evil, sneaky demolition enterprise against victims of all types of relationships with family, marriages, work, etc. If you read the great reviews, much gratitude is expressed toward the author who completely validates the target of such vicious abuse while exposing the malignant narcissist’s goal of complete destruction of his scapegoat/victim since this is the only way these predators can relate to them since they are empty souls!
http://www.amazon.com/Stalking-Soul-Marie-France-Hirigoyen/dp/188558699X/ref=la_B001K178CQ_1_1?s=books&ie=UTF8&qid=1400186880&sr=1-1
Of course, as you know, there are tons of others you can find by searching Amazon and reading the reviews which are also a great source of help, information and inspiration. I’m sure you have plenty of favorites yourself because you sound very well informed in your many posts.
Report comment
Thanks for the resources, Donna.
I had all that counseling before 1991. Free counseling from grad students at the University of Texas, plus a few licensed psychiatrists and psychologists off campus who worked on a sliding scale, and even lay counseling. Took the best and left the rest, and am very grateful for having had that opportunity. Some group therapy helped a lot too. In 1991, psychiatrists I saw started wanting to put people on antidepressants right away to “make counseling more productive.”
Outside of my childhood home, most adults in my life really liked and cared for me, and I pretty much got along with everybody. I have a lot more good memories than bad from my childhood, but learning about sociopaths really opened my eyes about my stepfather and reading “World of Pain” by Doctor Lillian Rubenstein taught me that a lot of what I didn’t understand about my childhood family was part of a text book case of a certain class of working poor pathologies– my parents were “hard settlers”. We always had the cleaning house and greenest lawn in our little working class neighborhoods. Aside from my sociopath of a step-father, we did have structure, unlike the other class, which I can’t remember what Rubenstein named; but they were skid row, addicts, alcoholics, etc., who were too incompetent to hold jobs and had little to no structure and discipline in their lives.
Sociopaths rely on a small set of what are essentially baby tricks, once you recognize the patterns. They have a real talent for dressing them up so they look different each time, but they’re not, and much of what they show themselves to be is counter-intuitive. Anyone, for instance, who believes that someone who is looking them in the eye is telling the truth is ripe for the taking.
Report comment
That’s true, the tactics is really transparent when you know what to look for. I think for people who were not brought up in such toxic environment (like me) the most tricky part is to grasp that such a behaviour is even humanly possible. You always make excuses for what you see and likely what you see is anyway only a small part of reality (I remember being stunned by the fact how much my surrounding knew about the guy I was with – that’s because it was impossible for him to play the game with each and every person so he only played it in front of me and few other targets).
Report comment
May I just add there is also a lot of on-line places where one can get good information and support, like:
https://www.psychopathfree.com/
In general I’d also recommend reading Robert D. Hare.
Report comment
Hi, WileyWitch and Donna,
I actually wrote a book myself on this topic, based on years of work with domestic abuse victims. It’s called “Jerk Radar: How to Stop a Bad Relationship Before It Starts” and is basically a manual for detecting narcissists when they’re in their charm/grooming phase.
I definitely agree, abusers are the ones who seek out people who have never had their boundaries respected or learned it’s OK to say NO and stick to it. Most of the victims are not seeking anything but someone who genuinely cares about them, and these sickos pretend to be everything the victim’s always been looking for, and then pull the rug out once they’ve got them under control. It’s pretty disturbing, but there are some ways to turn the alarms back on, and that’s what the book is about.
Just thought I’d mention it, as it seemed very relevant to your observations.
—- Steve
Report comment
Hi Steve,
Thanks for letting us know about your book, Jerk Radar. I will check it out and from what I’ve learned from your many great posts, I am sure it is filled with much wisdom, compassion, empathy and great advice that anyone can use, especially women without the necessary training/boundaries.
As I’ve told you before, I have always appreciated your kind, empathetic, common sense and honest comments here about the perils of biopsychiatry.
I’ve admired your efforts to bring up your kids with so called “ADHD” symptoms with a nondrug approach that recognized their uniqueness as human beings.
I also appreciated your frequent validation when I cited many articles, books and experts exposing that abused women and children suffering trauma symptoms are now routinely stigmatized as bipolar, which I think is evil and heinous to do since it retraumatizes, blames and scapegoats the victims while aiding and abetting the abusers with more power, which is all too typical of biopsychiatry. Dr. Carole Warshaw, Psychiatrist and Domestic Violence expert exposes how psychiatry causes huge harm to abuse, trauma victims with bipolar and other bogus stigmas for their trauma symptoms in court, custody, asset and other battles when dealing with abusers that I’ve cited several times at MIA.
I’ve had the misfortune of having to rescue loved ones from this nightmare and succeeded at great cost.
I have appreciated the fact that you have acknowledged that in your counseling work, you have seen the bipolar stigma applied to abuse/trauma female victims all too frequently.
I have written several posts at MIA recently exposing those like Nassir Ghaemi doing all in his ill gotten power to expand the bogus bipolar fraud epidemic ad infinitum while refusing to acknowledge any social, relationship, abuse, bullying, mobbing, environmental and other typical causes of the post traumatic stress INJURIES now covered up with the latest bipolar fad fraud taking over the former borderline insult stigma for abused women suffering from Complex Post Traumatic Stress injuries exposed by Dr. Judith Herman, author of the classic, Trauma and Recovery.
What makes Ghaemi especially pernicious is that he deliberately uses known traumatic events to falsely claim that if the victim has any reaction, she has bipolar!!! He perpetrates every Big Pharma lie including that iatrogenic injuries from SSRI’s including mania uncover the victim’s bipolar, which is such an old Big Pharma ploy it would be laughable if not so deadly! Dr. David Healy exposes that Mitch Daniels, a Big Pharma CEO, came up with the great ploy to blame the victims’ so called mental illness for every iatrogenic, nasty drug effect, drugs that don’t work (treatment resistant…) and other typical psychopathic schemes to literally get away with murder. Ghaemi is also eliminating a requirement for mania or hypomania in such absurd labels as bipolar V, VI, ad infinitum he proposes!! Even over eating is now being considered bipolar due to its impulsive nature per a study I just read that screens for comorbid bipolar and borderline along with the eating disorder in a brief test. Do you believe this?? Needless to say I am very upset and worried about the fate of our children and humanity as biopsychiatry continues its fascist, destructive agenda even though the DSM and their bogus stigmas like bipolar have been proven and exposed to be totally invalid junk science even by Dr. Thomas Insel, Head of NIMH. So, obviously, the purpose of biopsychiatry has nothing to do with health or well being of any kind, but rather, the opposite as is all too clear now and has been since its beginnings as agents of social control in the guise of medicine. I cited a post by The Last Psychiatrist, who exposed that the real nefarious purpose of Ghaemi and cohorts is to eliminate most if not all depression “diagnoses” and convert them to bipolar now that SSRI’s are coming off patent and neuroleptics still make billions that can better be pushed for bogus bipolar now as so called “mood stabilizers,” a term invented by Big Pharma, as exposed by Dr. Healy that has no meaning whatever in terms of a medical term nor do neuroleptics “stabilize moods.” They are just chemical straight jackets that have the same horrible effect on all per Dr. Joanna Moncrieff, Dr. Grace Jackson, etc.
Since this horrific expansion is just another evil ploy to push more of the brain/body damaging neuroleptics still on patent, I hope you will continue to speak out about this horrible menace since it places the abuse victims in all the more danger and at the mercy of all the abusers in their lives at work, home and the community at large only to be further betrayed, abused and retraumatized by the so called mental health system, courts, etc. The fact that they are preying on toddlers and babies in utero in addition to the elderly shows this profession has no shame or conscience in my opinion given that these drugs are well known to cause massive damage to the brain and body and early death by about 25 years on average with far worse effects on children and elderly.
Actually, I have read that many of the character disordered target strong, successful women to charm, devalue and discard to exploit what they can and enjoy their great victory of destroying them with impunity as a greater challenge. Of course, as Dr. Robert Hare points out, we all have our weak spots and vulnerabilities and malignant narcissists/psychopaths are very good at ferreting them out and exploiting them without mercy. Dr. Hare admits that even experts like himself and Dr. Reid Meloy can still be conned by these predators regardless of their expertise, so he warns not to blame yourself since these predators will do this with anyone and they are apt to have a trail of lots of victims in their wake. However, he also points out in his book, Without Conscience, that depending on one’s background and boundaries one woman at the first sign or trouble will walk out and never look back while some become perpetual long suffering, martyr wives dealing with abuse, cheating, etc. So, I think coming from families that violated boundaries and engaged in other abuse/assaults on esteem certainly make women and people in general more vulnerable to these “snakes in suits, ” title of another of Dr. Hare’s books.
Dr. Frank Ochberg, Psychiatrist and trauma expert, has a great article on spousal abuse at his web site, The Gift From Within. He also points out that often the original betrayal and abuse came from one’s family of origin making one more vulnerable to abuse, so there won’t be much help there:
http://www.giftfromwithin.org/html/spousal.html
One of the great benefits of books like yours is that women are often taught to doubt themselves or allow themselves to be pressured to act deferential to men, so they ignore red flags and their gut instincts unless they are very clear about what constitutes boundary violations and danger. Guy deBecker’s book, The Gift of Fear, is great in terms of coaching women and people in general to be aware of danger signs like a man’ s refusal to hear your “no,” excessive charm/flattery, gas lighting insults like “you’re too sensitive if you object to their controlling and other inappropriate behavior and other red flags.
Finally, given your long career in therapy if I understand correctly, I’m sure you’ve seen it all and that your book would be especially useful. Thanks for pointing it out.
I’m posting a link to Amazon for your book, Jerk Radar, and I see that it’s gotten many five star reviews, which is a very good sign about its quality and helpfulness.
http://www.amazon.com/Jerk-Radar-Abusive-Relationship-Before/dp/1592997406
Report comment
Psychiatry is an ally of sociopaths.
It has aided and abeded two generations in my ex’s family. First his grandfather who sexually abused his kids and grandkids got away with it unscratched while a girl in the family tried to commit suicide and spend years in “treatment”. I was supposed to be the second one and only narrowly escaped – the guy knew very well what he was pushing me into, as he good proper training watching his abused sister being re-victimised.
Report comment
“I have read that many of the character disordered target strong, successful women to charm, devalue and discard to exploit what they can and enjoy their great victory of destroying them with impunity as a greater challenge.”
Also true. The guy I was with had a history in targeting women who were attractive and smart and turning them into emotional wrecks – the history I sadly only learnt after the fact. He also used them as proxies to push his own career (same as valuable men who did things for him out of kindness and were very much surprised he took all the credit).
Report comment
Psychiatrist couldn’t spot a psychopath if his life depended on it unless he is one himself, which I believe happens all too often. I was in a relationship with a real sociopath and they only people who failed to notice it were the “professionals”. They kept looking into what is so wrong with me that they completely failed to see what was going on. Somehow all my horrible mental illness went away as soon as I was rid of this asshole and his gaslighting and social isolation.
I’d have been better of if I went for advice to my colleagues at work who knew this guy.
Report comment
Donna,
Thanks for coming in. The family can be an enormous source of support for children, but, as you point out, can also be a negative experience.
I don’t really have a book recommendation. There’s an interesting list here – you might see a title that fits the need. I think the critical point is that everybody is different. The fact that your friend recognizes that there is a social skills deficit is a huge first step. When I was in practice, the next thing we’d try to do was identify a specific skill that the person felt he/she lacked, e.g. how to just chat; what to do with one’s hands during a conversation; how much eye contact to make; etc.. Usually the “solutions” are not too difficult once the problem has been identified and articulated clearly.
Report comment
From my experience social skills develop themselves if someone is provided with a good company. I’ve always thought about myself as having poor social skills, yet I have many great friends and social support that never stops to amaze me.
I think the only problem is when a child comes from the background where they learn not to trust and seek contact with people – it’s then very hard to unlearn these defences, especially given the fact they are in many cases useful.
The key is to learn how to identify the people who are worth giving a chance and not waste it on assholes who exploit you. That is by far the most important social skill.
Report comment
I taught social skills at a residential school K-12. The Boys’ Town’s “Teaching Social Skills to Youth” was the program we used. Another helpful book is Lavoie, Richard (2005-08-15). It’s So Much Work to Be Your Friend: Helping the Child with Learning Disabilities Find Social Success . Touchstone. Kindle Edition. One of the many strategies that Rick offers is called the Social Skill Autopsy. Using this technique, an adult assists a child to improve social skills by analyzing social errors together and designing alternative strategies. This technique also works well in examining and identifying behaviors that contribute to positive social interaction.
Lavoie, Richard (2005-08-15). It’s So Much Work to Be Your Friend: Helping the Child with Learning Disabilities Find Social Success . Touchstone. Kindle Edition.
Report comment
RISN,
Thanks for coming in, and for telling us about your work. One of the great tragedies of the mental health system is that the illness model has pushed social skills training aside, when so often it is precisely what is needed.
Report comment
Phil, this is truly a brilliant analysis that is devastating to the basic premises of the article. Essentially, the study at best suggests that we should teach social skills to kids in their school years, which, as you note, should be obvious to anyone with half a brain.
I have made similar arguments about ‘ADHD.’ It is commonly bandied about that ‘ADHD’ children are more likely to commit delinquent offenses as teens and drop out of school early. Well, we’ve pre-screened these kids for impulsivity. Most criminal activity in teens is impulsive in nature, so should it surprise us that kids who are impulsive as kindergarteners are more likely to be impulsive as teens? We’re also pre-screening for every behavioral variable that make kids less likely to be successful in school. And then we are impressed when it is announced that the kids who we know don’t fit in well in school are more likely to drop out? Of course, it adds insult to injury that the so-called ‘treatment’ for ‘ADHD’ does nothing to change either of these variables.
Also similar to this report, the vast majority of ‘ADHD’ kids don’t become delinquents and do graduate from high school, just not as big a percentage as the mean. And plenty of non-diagnosed kids drop out and commit crimes as well. Having an ‘ADHD’ diagnosis is actaully a very poor predictor of whether someone succeeds in school, even when we have pre-screened to include only those who are bound to find school more difficult to tolerate. And of course, at no time do we spend the slightest energy figuring out what environments might work better for these kids, or teaching them the skills to survive in a standard classroom environment.
You’ve done a great job of highlighting how the scam is conducted. Unfortunately, it’s subtle enough that it’s hard for the layperson to detect, and when enough letters are attached to the author’s name, sufficient complexity causes the average person to shut down and simply assume that these guys must be smarter than me and therefore must know what they’re talking about.
Thanks for the fantastic deconstruction!
—- Steve
Report comment
Steve,
You write: “…the study at best suggests that we should teach social skills to kids in their school years…” And the tragedy is that this even needs to be said! Something that would have been obvious to our grandparents and earlier generations is now being overlooked because psychiatry is using scare tactics – relabeling these skill deficits as “symptoms” with dire warnings if appropriate “treatment” isn’t sought.
Best wishes.
Report comment
The Psychiatrist that diagnosed me, was painfully inept at conversation, wore wide tweed trousers several inches too short for his legs, and had starey eyes. He was not the kind of person you would want living next door to you.
Report comment
Sounds like the guy who first diagnosed me. He never looked at me once during the fifteen minutes I spent in his office. He sat bent over as he scribbled on his little note pad. He finally asked me how I was doing, without looking up. I told him I was not doing well at all. He asked why, without looking up. I told him that I’d received word the day before that my only sister had been murdered. His response: “How interesting.” I then proceeded to tell him that it felt like the entire world was coming down around me on my head and he finally looked up at me and screamed: “That’s stupid!”
And this is the kind of maladjusted people who are allowed to wield such great power over peoples’ lives. Disgusting.
Report comment
One who was “diagnosing” me was personally offended by my perceived high intelligence. He also tried to convince me that I think I am better than anyone around me and basically a narcissist. When I got irritated with it and sarcastically laughed at some of his ideas I later read in my records that I displayed “laughter unfitting to the situation” and suggested I could have symptoms of psychosis.
Another one tried to convinced me I was abused by my family and when I failed to meet his expectations and didn’t agree with him, he turned 180 degrees and said that I was loved to much (basically meaning I was a spoiled brat). He also said that all my friends are not really my friends but they pretend so because they are scared of me or something.
Report comment
Fiachra,
That’s an interesting observation. Within the framework of orthodox psychiatry, such factors don’t matter. All he has to be able to do is “diagnosis mental illnesses,” and prescribe “medications.” In reality, however, I think most people expect a little more in the way of social engagement from a helping professional.
Report comment
Thanks Philip
A lot of Psychiatric staff themselves, are sheltered people with strange ideas about the real world.
Report comment
Donna, Steve, and Wileywitch–Actually, in an classic anthropology text Ruth Benedict wraps up her comparative documentation of three diverse cultural groups–small and surely more disappeared by now–with a critical discussion of psychiatry. This was pre-WWII, I think. Patterns of Culture.
Reading it beyond the day has its own instructive value, too.
In the social sciences, conclusions can get more attenuated than the specific researcher portray. Yet with the more fully recognized fact of the value judgments guaranteed to attach to all attempts at objectivity in historical and economic analyses, and so on, I see the validity of Ms. Benedict’s work as more conprehensible. The book is not long and the last chapter may exist on a PDF somewhere, of course.
(I am just waking up, and so very term paper-y as far as words go.)
Report comment
reduction in the expression of emotions in the face
showing little interest in . . . social activities
diminished speech output
lack of interest in social interactions
childlike silliness
lack of verbal . . . responses
staring
grimacing
mutism
echoing of speech
switching topics
The psychiatrist who diagnosed my daughter had many of these characteristics.
Switching of topics when I questioned his judgement, and lack of verbal responses, sometimes by not showing up the meetings or returning my calls. When I questioned the use of neuroleptic drugs, he definitely was grimacing. I think he is on a trajectory to a psychotic illness.
Report comment
madmom,
Definitely at risk!
Report comment
“A great deal of their present effort is directed at two main themes: integration of psychiatry with primary care (a mental health worker in every GP’s office), and early intervention. Watch out for media infomercials on these topics in your local newspapers, and for bills on these topics in your statehouses. ”
An absolutely horrifying future to imagine. I guess our only hope now is that with so many victims having been harmed by them and more of them becoming aware of it that an increase in psychiatric services leads to an increase in person-to-person conflicts related to it. Hopefully it finally pushes the victims over the edge.
Report comment
Jeffrey,
Thanks for coming in.
It is horrifying. But right now I fear that they are winning the media war. There were four major articles on “mental illness” in our local paper in the past week. All four pushed the standard themes: early intervention; need more meds; jails full of “mentally ill” people; “untreated mental illness” is costing the nation billions of dollars; and, of course, “A lack of mental health care is at the core of many of our most vexing issues, such as gun violence and school shootings.”
We need to keep speaking out and exposing their propaganda for what it is.
Best wishes.
Report comment
That’s exactly why I feel that any hope for the future lies in psychiatry victims being pushed too far. Mental health workers in my area have it easy considering that they don’t have to put up with me because I, like most victims, avoid them the best that I can. If they keep pushing this expansionist agenda then one day they will find themselves face to face with many of their victims, and will be begging to make them go away.
Report comment
Jeffrey,
Yes. And in addition, they will some day have to face the fact that their “treatments” have effectively disabled so many people.
Report comment
JeffreyC
I think this is why people like Thomas Insel are pulling away from the chemical model – because the drug damage is becoming obvious. The drug companies have spread their net to capture the broader population, and have created long term illnesses in the these people.
This demonstrates that psychotropics can turn anyone into a long term psychiatric patient.
Report comment
I’m sure this is excellent work, adding up how the numbers don’t.
But beyond that, it’s quite wrong to put a child somewhere it has no choice on it’s own to seek different avenues (a different school, a different setup for learning etc.) and then when the child is uncomfortable decide to see whether it later on in life is put into a diagnosed illness there’s no proof exists, as it is defined. Along with further taking away choice.
Report comment
1. The child does not seem to take part when the rest of the class is having fun.
2. The child has no friends.
3. The child is often teased.
4. The child does not actively seek friends.
5. The child seems to avoid contact with other children.
How can you even make any assessment based on these points as scored by the teacher? I was a child who would have scored very highly on this scale in primary school and very poorly in secondary school and it had little to do with me on my own and everything with the kind of social environment. I’d also score on this scale entirely differently at school and outside of it.
Psychiatry is amazing with these checklists – they constantly ignore the context, the timing (how you feel now and how you felt 2yrs ago may be totally different, yet they are fine diagnosing a “life-long” personality disorder based on the current short-lasting situation). Ehhh…
Report comment