
“Without health, life is not life; it is only a state
of languor and suffering — an image of death”— The Buddha
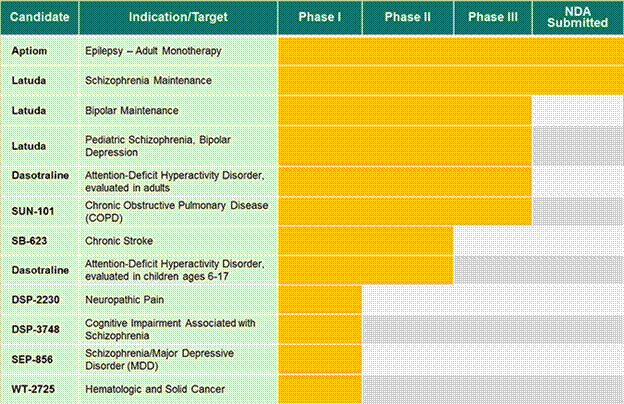
In Boston a meeting of the Massachusetts Neuroscience Consortium has just come to a close. The most recent member of the consortium; Sunovian (a Japanese drug company) has generated a great deal of excitement and has projected increased revenues over the next year. As they leave the meeting, the high-level Sunovian reps are conferring enthusiastically about success with the new investigational drug Dasotraline; an antidepressant with triple reuptake properties. Phase 3 trials are in progress for adult ADHD and testing with youngsters is well underway for the child studies (see links below for studies, and charts for trials).
Although adult studies are being done the Consortium members know that the real target for this new drug is the pediatric population; the children ages 6-17 with ADHD, Schizophrenia and early onset Bipolar symptom. There is more news from Sunovian; the phase 1 trial with Latuda on 6-17 year-olds has been completed. Sunovian is the heavy hitter in this game, as the multiple studies show (see below) and their multiple testing sites are expanding world-wide.
The other reps who attended the Consortium meeting, from Pfizer, Johnson & Johnson, Merck, Abbott, & Biogen will profit from Sunovian’s aggressive moves in the drug development world and they are pleased with the four new innovation centers in London, Shanghai, California and Boston that are poised to coordinate the efforts. It is collaboration, collusion, and competition. Business in triple time due to threats of funding cuts and new legislation that aims at financial transparencey for drug companies.
Time magazine, with its bold new article that expresses outrage at ADHD mass medication, has apparently not been read by the Consortium reps or the members of TransCelerate. The article — in a loud, compelling voice — talks about the addiction to stimulant medication, and misdiagnosing behaviors as ADHD. The Consortium members are not listening.
It is difficult to track down the centers that are doing the actual trials since the consortia have partnered with hospitals, universities and medical centers world-wide in order to accelerate the process of completing clinical trials. Thus far NYU, Cincinnati Children’s Hospital in Ohio, and Ohio State University have come up in the study literature. The studies themselves are easier to locate on-line, as the links below demonstrate, and as they advertise abundantly for recruits for their research.
We know that NYU, for example, is actively looking for children for the Autism and Temper Outburst Study, and the MRI research on 18-month-old infants (see their ad below). We also know that Cincinnati Children’s hospital is conducting research on 5- to 7-year-olds with Autism, 7- to 10-year-olds with AHDH, and 10- to 17-year-olds who meet this criterion; “Does Your Child or Teen Have a Condition that Makes Them Upset or Agitated?”
These studies appear to be identifying expected childish behaviors as dysfunctional and requiring evaluation and medication. They are, however, part of the repertoire of behaviors that emerge during a child’s developmental course.
Critical Ages and the Superhighway:
From Empathy to Memory, Through Reasoning to Maturation
The information above is critical in fully appreciating the implications of research studies on infants at critical stages of development, and the speed with which clinical trials are being conducted today. It is interesting and alarming that drug companies have focused on the 18 month to 5 year age range, and the adolescent period, as these are landmark brain-development periods in the child’s brain and emotional/cognitive development.
At the age of 18 months, a child is growing rapidly and excitedly exploring the world around him on his own two feet (with mother close by). He or she can babble a few words and he loves to throw things on the floor and pour his milk out on his tray. He’s beginning to solve problems. His brain is developing rapidly and critical connections are forming that will enable him to solve the big life problems that he will encounter later on. Perhaps more importantly than this he is beginning to test separation from his caretaker and, he is starting to recognize that he is a distinct individual. One of the key developments at around 18 months is the emergence of empathy.
When an infant is securely bonded to a caretaker and is the recipient of love and support he or she recognizes the feelings of other people and experiences these feelings within himself or herself. The onset of empathy is the true beginning of human connectedness and of the emotion that underlies healthy human relationships. For children in this sensitive and wonderful age range a traumatic event such as separation from a loved one or abuse will leave lasting scars. Events that would not appear to be devastatingly traumatic to the adult; such as loud arguing, hospitalization of the child or parent, a new and scary environment may be the kinds of experiences that interrupt or even damage the delicate developments that are going on within his brain.
The 3-year-old child is experiencing another landmark in brain development; this is the onset of auto-biographical memory a critical emergence as it enables him to remember himself in past situations. It is the recollection of personally experienced past events and It forms the basis and framework for our emotions about people, situations and ourselves
At the age of 5 or 6 years the child is undergoing another growth spurt physically and in the brain domain. Relationships come into play here and kids are learning how to reason, to calculate and to express themselves. There is an overproduction of synaptic connections at this time that will be pruned back during the adolescent period. For the 5 and 6 year old, these connections enable the youngster to test out different solutions to life problems.
The adolescent years are a critical phase during which extensive maturation is going on within the domain of the prefrontal cortex. This area is responsible for working memory, organization, planning and regulating mood. This area is in growth mode and there is “pruning” of under used connections that is occurring throughout the brain. This rapid production balanced by discrete elimination of synaptic material is critical for all later brain development.
What are the Diagnoses Being Tested and What are the Drugs?
The disorders that the drug companies are zealously targeting in very young children are; ADHD, Autism-spectrum disorder, Temper Outburst Study, Early Onset Bipolar Disorder, Schizophrenia and Depression. These diagnoses elicit fear in the hearts and minds of parents. These diagnoses will ignite that fear and the search for treatment or a “cure” will begin.
The testing itself involves medication and MRI studies (on the 18-month-olds) The drugs are Risperdal, Depakote , Ritalin, Latuda, the new drug Dasotraline, and one that is “not approved by the US Food and Drug Administration.” This last study is for children ages 10-17 and is entitled “Does your Child or Teen Have a Condition that Makes them Upset or Agitated? Are they on an antipsychotic Medication? ”
The reader can investigate side effects for the above medications; they are too numerous to list. These medications have unknown long-term effects on the body and brain and this is especially significant in light of the age of the population and their vulnerability to disruptive life events. For the 18-month-olds we need to remember that the MRI involves sedation, placement in a tunnel-like machine, and no food or water for a specified period of time.
In an article on the CNBC website, “Is There a Cure for Pharma’s Innovation Problem?” the urgency and threats to big pharma are summarized as a lack of subjects for research since trials have shifted from animal to human studies for “ethical” reasons, the new transparency regulations, the expense of doing the research and the fact that the FDA is overwhelmed with paperwork for the studies.
The article continues with the comment from the president of TransCelerate that the collaborative efforts of the drug companies are part of a solution to these problems. This writer begs to differ with this view given the test subjects, along with the medications they are being prescribed, and the rush to drug development that is occurring. TransCelerate has a loud voice, and media attention that will only be countered if many individuals who have the best interest of youngsters at heart speak louder than the companies do
To frame all of these research studies in a scientific context is a difficult task since the jury is still out on the question of whether symptoms of “psychiatric” disorders are to be found in an unbalanced brain, in the chemicals that fuel brain processes, or in something entirely different. A recent article reported in the U.C Davis Journal states that research is uncovering an immune system link to autism. Similarly, a 2012 New York Times article explored the link between autism and the immune system. If this is the case — or part of the case in regards to autism, as the articles points out — the mother’s immune system may be a domain for further research before and during pregnancy.
Perhaps this is a light at the end of the tunnel. Is this a shift of attention away from the brain and towards other systems (including life itself) that contribute to the emotional suffering of young and old alike?
In the words of our esteemed colleague Dr. Michael Cornwall;
“The safety of our children is a sacred obligation we strive to preserve. Anything or anyone that harms them becomes the object of our distrust and potential wrath. I want to raise the possibility that psychiatry, for all its accomplished champions like Thomas Insel of the NIMH, may have forgotten the elemental fear people feel for the safety of their children. If psychiatry becomes perceived as a consistently increasing threat to our children, then are its days as a monolithic social institution numbered?”
* * * * *
Below is information for those who wish to investigate the studies and research in more detail:
Cincinnati, Ohio Children’s Hospital
NYU Child Study Center in New York
Ohio State University clinical trials information
Massachusetts Consortium information
Pediatric ADHD information and Sunovian use of Dasotraline
General information on Sunovian











This is horrible how they are trying to market more drugs to kids. As has been stated so many times, this research has nothing to do with what is good for people; it is only the drive for profit. Maybe there should be a section on MIA about how to protect your child from inappropriate psychiatric intervention.
Two comments:
Regarding the following, “the jury is still out on the question of whether symptoms of “psychiatric” disorders are to be found in an unbalanced brain, in the chemicals that fuel brain processes, or in something entirely different,”
Perhaps the jury is still out among some poorly trained psychiatrists and drug company representatives. But I think many people intuitively understand that emotional distress (“symptoms”) requires interaction with the environment over time, usually traumatic or anxiety-provoking interaction. It’s this process that results in brain chemistry disturbance. Without ongoing brain-environment interaction, nothing would happen. That’s one reason why medications are so ineffective over the long term, because they are not relationships and cannot affect complex brain-environment interactions in a transformative way.
And as for this part, “The disorders that the drug companies are zealously targeting in very young children are; ADHD, Autism-spectrum disorder, Temper Outburst Study, Early Onset Bipolar Disorder, Schizophrenia and Depression. These diagnoses elicit fear in the hearts and minds of parents. ”
It’s too bad these “disorders” elicit such fear, because they are only projections from psychiatrists’ minds onto children. If more parents realized that emotional distress cannot be concretized or reified into diagnoses, that emotional distress should instead be understood as existing along a continuum of severity and as amenable to change and cure, they would be less worried. It is almost like a sick joke that something like Temper Outburst would be considered a disorder. How stupid and profit-driven are the psychiatrists that fabricated that?
Understanding the non-validity of diagnoses would also undermine the basis for using drugs to treat emotional distress, and would empower parents to say no to drugs.
Margaret, I’d add that sometimes semantics are important. I guess that you probably don’t believe in the validity of these diagnoses as concrete illnesses: if this is correct, I encourage you to say so alongside discussing “disorders” in the drug companies’ terms, as writers like Philip Hickey do.
Furthermore, calling something “autism spectrum disorder” is confusing. If something exists along a highly variable spectrum and involves subjective behaviors or lack of behaviors, it isn’t a disorder in the classical sense of a medical illness which is consistent from person to person. A disorder has sharp boundaries, and autistic traits/behavior can exist in innumerable variations and severities, without a clear boundary demarcating where a disorder stops and normality starts.
Report comment
Thank you for your continued efforts in bringing to light and fighting against this Orwellian nightmare of relentless psychiatric drugging of children!
Report comment
I appreciate your support. It gives me the energy to pursue this.
Thanks again
Report comment
Thank you for your comment; I will follow through with the good advice!
Just a heads up for you the latest research studies are not only using non FDA approved drugs, they are using Latuda (a sunovion best seller) that is not recommended for more than 6 weeks (on teens in the clinical trials) and one study gives kids a spoonful of “cough syrup). I think the actual targets of the drug companies are the parents who are so fear-driven and miss informed that they are expected to line up for these new meds, (toxic chemicals I should say) . Parents aren’t stupid but you are right, many psychiatrists are ignorant and worse they are profit-driven and without any moral compass.
Report comment
As the mobilizing wheels of the psychiatric branch of the Therapeutic State turn with military like organization and precision across the planet the people and their children caught like deer in over bright headlights isolating each individual within a family , while all are being collectively attacked with the sophistication of robber baron round table think tank strategies, trojan horse presented to us as the urgently needed health solutions of the “new world order” with the implication that this is an offer that can’t be refused. And yet we must refuse , our guts scream out , and win out over our fear, and like any wild animal protect our young against the predator. But we must organize and do it together with enough precision or guerrilla action to dismantle the nightmare they wish to drape over us and somehow make it fall back over themselves.
Report comment
Yes, yes and yes again, you put it so eloquently and we have the energy, we have the moral principle, we have the guts what we need is a strategy. We are all being bullied and they truly believe we will stand for this offensive behavior. But then psychopaths and sociopaths truly believe that they will never be caught and that they are entitled to do what they do. This is their weakness, their greatest Achilles heel, but we are bringing the information to light, we will shake their tree until the drugs fall off and rot.
Report comment
The drug companies won’t be doing this on their own, they’ll need medical and official assistance. They’ll also need the help of the public relations and media industry. Unfortunately, these people are easily bought.
Report comment
Correct! I have some of that data now, the partnerships, the sites where the testing is done, even the universities that are helping with the research. I will put the info in the reader’s hands and we can at least see who is involved.
Report comment
I agree with both the writer of this blog and Michael Cornwall’s statement as well that if parents in general (who probably make up the majority of our society) come to realize the threat to themselves and their families that the multinational drug corporations pose, there might be some great steps forward in the fight of all decent people against the destructive power of psychiatry.
I have to say also that I think the amazing critical article about drugging children in a recent issue of TIME magazine is a development our movement should be encouraging.
Our human rights movement needs to reach out to new allies, and I can’t imagine better allies than the parents of children targeted by drug companies, to be treated as profit centers instead of human beings. We have ignored the abuse of children, like the cases of Rebecca Riley and Justina Pelletier. I don’t know why this came about, but I think we have to pay more attention to what happens to kids snatched into the system.
“…(the) psychopaths and sociopaths (who run the mental illness system and own it) truly believe that they will never be caught and that they are entitled to do what they do.” Yes, and it’s our job to make sure they answer for their crimes.
Report comment
Thank you, Margaret, for speaking out against the psycho / pharmaceutical industries’ horrendous crimes against children. And, Ted, I agree, pointing out psychiatry’s crimes against children is very important. I’m heartbroken 13% of American children have been diagnosed with the bogus ‘ADHD’ label. If I recall correctly the psychiatric / medical community at one point (2010, or so) had approximately 7% of American children (mis)diagnosed as ‘bipolar,’ largely due to Biederman’s antics and DSM-IV-TR misdiagnoses of adverse reactions to ADHD drugs and antidepressants. And John Read’s research proves the most common trait of all ‘schizophrenia’ patients is child abuse or adverse childhood experiences. Plus, children suffering from symptoms of child abuse are, if I recall correctly, six times more likely to be diagnosed as “psychotic,” than children not suffering from symptoms of child abuse. And the ‘gold standard’ treatment for ‘schizophrenia’ is known to cause both the negative and positive symptoms of ‘schizophrenia,’ via both neuroleptic induced deficit syndrome and the central symptoms of anticholinergic intoxication syndrome, and likely more ways I haven’t happened to find in my research yet.
GROWN ADULTS NEED TO STOP DEFAMING AND DRUGGING INNOCENT CHILDREN!
Report comment
‘Schizophtenia’
It’s not the genuine crisis that needs worrying about this can be resolved (believe it or not) and overcome. It’s the nasty medicalisation that steals the persons life away.
Report comment
For lack of a like button…Well said!!!
Report comment
I agree, too, Fiachra. And truly we need the psychiatric industry to get out of the business of profiting off of turning child trauma or abuse victims into “schizophrenics” with their neuroleptics / antipsychotics.
Report comment
I agree with the assertion that children are being overly medicated. I also agree that, in many cases, children are being medicated for things that are within the normal range of child behavior. This is a truly despicable thing that must stop.
But I know well many parents of children who have been labeled “mentally ill,” and I know well their children. Most of these parents seek out medication for their child (or have it pushed on them) because of behaviors that are *well* outside what would be considered normal.
We do not have to call these children mentally ill, but we certainly need to acknowledge that they and their families are struggling. These parents choose medication because they are presented with few other options.
Medication is not the answer for these children. But these families also do not need to be told that their child’s behavior is normal. They need options that are safe and effective for their child and their family, options that work to alleviate whatever stressors is triggering the behavior in the first place. That is what will allow these children to became healthy adults who stay out of prison and psychiatric hospitals.
Report comment
Excellent article.
Having just spent two months working in an elementary school, I must say – as a longtime advocate for safer prescription drugs (having lost my son to Zyprexa) – that I was shocked by the amount of polypharmacy as well as the bold way in which a few teachers pushed parents of “busy” little pre-school boys to look into drugs. One particular note – it is not just psychiatrists prescribing. Many pediatricians are perfectly happy to whip out their prescription pads.
The topper was today, when the long-time, sensible principal told me that some of the parents get their children diagnosed so that they have a source of psychotropic drugs for themselves – they push for higher doses for their children so that they can siphon them off for their own “highs”…
Report comment
The first time I heard of drugging of children was when I volunteered in high school ata summer camp for the developmentally disabled. One child was said to be on “speed”. He was extremely active and definitely was out of the normal range. I was shocked. In my journey in the social services field. I did work at a group home for adolescent females. None were drugged that I was aware of. It was the beginning of cutting coming out as an issue. When I was a professional graduate level Social Worker I was involved with a case of an acting out adolescent only on the weekends with an open wound that required at that time hospitalization. He was bored bored bored especially on the weekends when Child Life workers were not on.He had no family that was able to fill in the weekend gap. The ortho surgeon had the great plan to send him to the adult floor with a psychotrophic. I tried my best to fight that plan to no avail. This was the beginning of our descent into medicating preschool children.
That was early to mid 1980’s.
Later on my child need specialized surgery that required a choice between that doc and another. I refused to let that doc treat my child.
If you read works of the 1950’s and 1960’s there was an emphasis on therapeutic milieu without drugs. Still bad stuff went on but no drugging. Fritz Redl did good work and is worth a read. There were others in that timework that listened to the stories of children. I doubt many CEO’s of child social service agencies are even aware of their names or that they existed as professional and caring therapists.
Report comment
It certainly appears that parents have to be vigilant in raising their kids these days. There’s just so many things to keep a real close eye on beyond even the psychiatry nonsense.
Vaccinations, weirdos in the education process (gender crap etc), possible polutants everywhere, making sure diet is good etc etc.
Report comment
Margaret, Your article is very effective for representing the moments of empathetic connection beyond your description of it. I got inspired by the careful restatement of the facts of this awakening to sense of self in respect of other minds and reasonings than will necessarily in every regard FEEL for this newer, little person’s own one. That demonstrative approach makes it easy to turn to your own life history and reflect on the true regard in which you know of empathy as serving you, and as coming to mean the right way to resilience only as some hard won insights bring its ultimate value into perspective. Many things here connected to the original developments of Bob Whitaker’s critique of psychiatry here, too, it seemed, and extended the relevance of the opportunity to learn from the comments to your article. Specifically, the general mood of criticizing patients and teachers and families for “denying facts of disorder” on the one hand, and then coaxing them into denial about the loss of control over normal life choices with coercive arrangements for administering drugs and extending treatment plans to infinity. Refusing to acknowledge the totally experimental nature of these monolithic treatment protocols just is not professional “helping”.
Report comment