
The Finnish Psychological Association held a meeting in Helsinki on 1 Sept 2014 titled “Mental Health and Medicalization.” I spoke at the meeting and four days later I sent a letter to another speaker — psychiatrist & professor Erkki Isometsä. Professor Isometsä replied: “I will respond to it in detail within a few days; I will also ask Drs. Gibbons and Mann about your comments, as I would like to hear their thoughts about your criticism, too. I suppose you don’t have anything against me forwarding your comments, do you?” I replied: “I don’t mind that you consult with Gibbons and Mann about my letter. Science benefits from debates and discussions of methodological issues, so I believe we all learn when we debate the issues.” On 28 Oct, I wrote to Isometsä: “as I have not heard from you, I just wish to inform you that I might put up my letter to you on my website.”
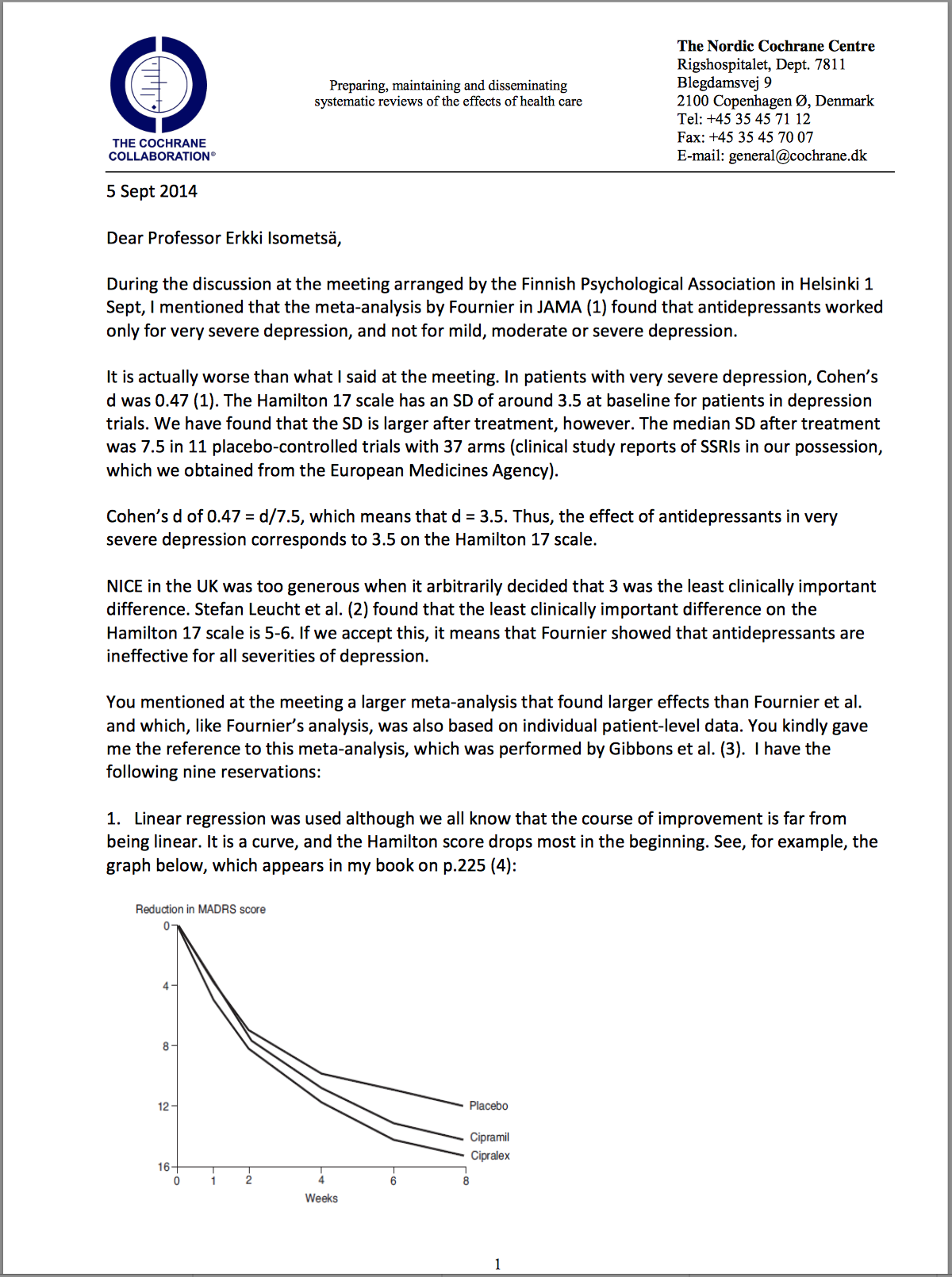
Open Dialogue is a succesful Finnish concept for treating patients with schizophrenia that builds on the remarkable results obtained by Loren Mosher, who was once the chief of the Center for Studies of Schizophrenia in the US National Institute of Mental Health. The third speaker at the meeting, professor Jaakko Seikkula, University of Jyväskylä, spoke about the Open Dialogue approach in acute psychosis under the title: “Returning to employment with less medication and hospitalization.”
Open Dialogue is also essential in science. I therefore have published my letter to Isometsä here as well as on my own website, although I didn’t succeed in starting a dialogue.
* * * * *
Interview with Peter Gøtzsche:











This I am sure is important, but almost impossible to understand for someone for someone who isn’t completely immersed in the subject.
Report comment
The techie bit, all about statistical interpretation, is indeed hard to understand Ted. But the comments that anti-depressants are only effective in very severe depression and even that is in doubt in the first two paragraphs and that they probably have no true effect at all in point 9 are damning on thier own.
A multinational industry that is sweeping the world with pills that according to Peter are useless and known to be damaging. No reputed pro drug commentator wants to engage with this analysis.
Pretty damning if you ask me
Report comment
The technical representation is complicated. I think the argument is that the antidepressants are useless (or worse than useless).
Report comment
Yes, he has.
My understanding is that the analysis not only debunks the statistical underpinning of the studies questioned as lies and manipulations, it also addresses the fact that even were the methods valid, all the drugs could achieve is a clinically insignificant change in a depression rating.
AND they have been shown to increase suicides and (they carry black box warning to this effect).
So….in reality, these drugs are better at causing suicides than they are at fixing depression.
…AND the people who conducted the research know it and so won’t come out and debate the issues Dr Gotzsche raises.
Report comment
And if you look at the hundreds of millions of prescriptions in European countries you’re talking about a very expensive medical confidence trick.
Report comment
I can sum it up: anti-depressants are no better than placebos but with serious side effects and people who claim otherwise turned out to be fraudulent pharma lapdogs doing bad science.
Report comment
Sometimes it is important to confront researchers who consider themselves “experts” with the weaknesses or occasional frauds embedded in their own methods. Though I am not a medical researcher, I am technically trained in experimental design and basic statistics. From that background, I would say that Peter Gotzsche’s analysis is quite devastating to people who perform research on antidepressant meds, out of a pre-existing personal agenda to validate medication effectiveness.
I would hope that Professor Isometsä responds to this article with similar depth and scientific rigor. That does not appear to have happened thus far.
Report comment
Letter sent 5 September – a promise to reply in a few days. No response.
Peter put this on his webiste on the 28 October and now on here.
Worth pushing around I’d say.
Like on NAMI and other similar organisations facebook pages perhaps?
Report comment
Well said, Richard
Report comment
Hi Peter
There is no such thing as the illness of “schizophrenia” and diagnosing someone like this finishes them off. I became well and returned to work as a result of cutting drugs and switching to psychotherapy. The nondrug solutions proved sucessful in the longterm.
I got your book “Deadly medicines. . .”. It’s a fantastic read, and I would recommend it to anyone.
Report comment
Thanks so much for the post. I was curious that the variance/standard deviation increased after Rx relative to before. Michael Thase, an apologist for the industry, always says that the results of drugs are dramatic in some. I always wondered about the variance needing to be larger in the treated group for Thase’s claim to be true. Apparently, the variance is larger. But, does this fact invalidate the use of the statistic? What a mess.
With regard to the serotonin argument, Chris Lowrey finds that the serotonin neurons in the raphe actually entail multiple circuits. One of these circuits, through the caudal dorsal raphe causes learned helplessness and depressive behavior. Even the theory is ridiculous.
Report comment
Jill, It’s probably just gobbledygook.
Report comment
Jill: Could you please cite the study by Chris Lowrey ?
Report comment
A good amount of sound research data points to the link that serotonin (and tryptophan) enhancement leads to “learned helplessness and depressive behavior” and a host of other adverse effects such as brain degeneration, stress hormone release, inflammation, compromised blood circulation in the brain, high blood pressure, cancer, etc – see: http://www.supplements-and-health.com/tryptophan-side-effects.html
Report comment
Actually there is not much truth to what you write. Learned helplessness is a concept arising from animal studies conducted by psychologist Martin Seligman. It refers to a situation where one cannot escape from a frustrating situation, like caught between a rock and a hard place. Learned helplessness signifies the relationship between an organisms and its environment.
Inflammation and increased stress hormone release are a result of acute or chronic stress, distressing life events, childhood traumas, low socio-economic status, overweight, insomnia among others. These are factors that precede any form of depression or its medication. Inflammation and stress hormone release are involved in many illnesses that have nothing to do with depression or its medication.
Report comment
If you go to google scholar and put in Chris Lowrey’s name, many articles will come up. You can download many of them.
Report comment
Excellent, Peter. It is disgraceful what is going on and highlighting the questionable data analyses is spot on.
After 25 years in neuroscience I found that when people started playing with their data in the ways you describe, they were ‘forcing their way’ to significance. They were committing scientific fraud. There was a lot of that going on.
The researchers should be forced to show the raw data is there are questions being posed. Ultimately, their data is seriously affecting people’s lives and possibly increasing deaths, i.e. increasing suicide. They should consider the responsibility they have when ‘playing’ with their numbers and having a drug appear on the market.
Report comment
And what about the drug pushing initiative (53 million prescriptions per year in England). Where’s the money?
Report comment
and not just suicide as an effect – there are many bad effects of so called anti-depressents
Report comment
Stir the brain soup….. see what happens…..stir some more…..see what happens next…..kick it….. see what happens…..repeat…..
Report comment
I surely appreciate both Open Dialogue and Peter Goetzche but I am not happy with the concept “schizophrenia” aince the diagnosis itself is very weak, and there are still no common sense about what it means. So I would suggest that we are very careful when using such wordings. Another thing I would like to highlight is that the concept Open Dialogue is sometimes a bit “vague”, and as far as I know we are many people all over the globe who have known for ages that it is important to talk to and not about others, and also that listening to the other one is the abolutely first step to take if a meeting will take place. But it might be that P G means OD in relation to research about how the team in Torneå meet people in acute crisis?
Report comment
Erkki Isometsä has probably been too busy since winning, subsequent to your meeting, a pan Nordic prize for services to science! For his lengthy career, conducting high quality research in mood disorders and, especially, for his work in developing depression and bipolar treatment guidelines in Finland. It probably won’t surprise you that these are heavily weighted towards physical treatments.
Gibbons, R.D. , for the record, has too many conflicted interests, that I’d advise one takes anything he says with a large tablespoon of salt.
Report comment
Just a couple of words about the “Open dialogue” method. It was originally developed in Turku, Finland while I was a resident. Most of us were enthusiastic about the project. But later it became a lot of trouble. Most of the staff were relieved when the method was stopped. There were some suicides and serious suicide attempts. In general the patients were hospitalised for many months to years. It was never a method that used no medication. High doses of benzodiazepines were used (e.g. 20-25 mg of lorazepam) instead of antipsychotics. In general the patients were unable to kick of the benzodiazepines for years. At the time the model was called integrated treatment of psychosis indicating combination of individual therapy and family therapy. I was one of those who was enthusiastic but from my point of view it was heading for a disaster.
In the Open Dialogue method benzodiazepines are also used in high doses. The study they made of the project was of weak quality but most of all the researhers concealed cases of suicides during the study period. Currently, the Keroputaa hospital area in Finland where the method is used has the highest suicide rate among schizophrenia patients in Finland.
The method is by no means unique. It is like incorporating motivational interview routinely in the treatment, which is more than you get in most hospitals. In Australia they have done a better job also research-wise
Report comment
“There were some suicides and serious suicide attempts.”
Is there any data available for that?
“High doses of benzodiazepines were used (e.g. 20-25 mg of lorazepam) instead of antipsychotics”
The paper says “During the first 3 weeks, benzodiazepines were used in the event of need for medication and, after this, if there was no progress in the psychotic symptoms or in the social behavior of the patient, neuroleptic medication was considered”. There is no mention that people were left on benzos for longer, is that a manipulation? The paper also suggests a decrease in hospitalization time – are you also accusing authors of manipulation here?
“In Australia they have done a better job also research-wise”
What do you have in mind?
Report comment
Antero, your writing seems quite polished. Maybe it’s not just “you” who is writing out there. In any case, for instance you say:
“Just a couple of words about the “Open dialogue” method. It was originally developed in Turku, Finland while I was a resident. Most of us were enthusiastic about the project. But later it became a lot of trouble. Most of the staff were relieved when the method was stopped.”
“In the Open Dialogue method benzodiazepines are also used in high doses. The study they made of the project was of weak quality but most of all the researhers concealed cases of suicides during the study period. Currently, the Keroputaa hospital area in Finland where the method is used has the highest suicide rate among schizophrenia patients in Finland.”
For instance, you don’t make sense if the “method” was stopped or not. First, you were relieved when the “method” was stopped. Then you tell that the area where the “method” is used “has the highest suicide rate among schizophrenia patients in Finland”.
Report comment
The first paragraph refers to the project in Turku, where the researchers focused on psychosocial methods and antipsychotics, but not on the fact that the doses of benzodiazepines were high and for a long time (which was evident to everybody working at the clinic in late 80´and early 90´s. It was marketed as a “medication free treatment”. That project resulted only in one paper (by Lehtinen et al. in European Psychiatry 2000). I think, however, the conclusion that it is not necessary to start antipsychotics routinely to all patients is sound. Traditionally the doses of antipsychotics used were in Finland low on a much lower level than in US or Europe.
As to the project in Northern Finland, the sale of benzodiazepines is high and according to those who worked there and were disappointed, the case was similar to that in Turku. Also patients sent to state mental hospital from that region had high doses of benzodiazepines. What may be true to some average cases may not be true to other cases. The study reports are not actual papers on intervention outcomes but more reports of what is the theoretical background (prof. Alanen´s project, Tom Andreassen´s thinking, Bakhtin etc). The sample is too small to draw any conclusions. There are many other short-comings additionally. So, we do not know on the basis of the paper about much else than you state above and that is not enough. In comparison to the national statistics. Moreover, the treatment models used are rarely transferable elsewhere as there are local background factors and enthusiasm.
The length of hospitalisations went down in all of Finland and the mean is currently 10 days in acute psychoses. Family interventions are also in use in most of Finland. What is positive in Keroputaa´s treatment is the fact that psychosocial interventions are carried out by same teams whether the patient is in hospital or outpatient care, and the are incorporated comprehensively, which is not the case somewhere else. But there have been development projects elsewhere in Finland and have been ion some respects a bit more innovative which have not been in the focus of attention internationally.
I do not think that they would have manipulated the data regarding medication. It is more a question of poor reporting and lack of critical analysis. As to the suicides, it is an intentional concealment. Why this has happened, I do not know. We will hear about this later this year from a leading Nordic researcher on mortality in psychoses in the Nordic countries.
In the end, all psychosocial/psychotherapeutic methods seem to lead to comparative results and the theoretical background does not exceed that of treatment allegiance and the so called general factors.
Other projects using heavily psychosocial methods are e.g. the OPUS-project in Copenhagen and Early Psychosis teams in Australia.
Report comment
Thanks for your comments with perhaps some new perspectives or data on this issue. Watching the international hype around Open Dialogue, I’ve thought it’s almost certainly oversold. I was “treated” in a Helsinki state hospital for “psychosis” and “schizophrenia” by another “ex-Open Dialogue psychiatrist in Oulu”, and I can tell that was also a most horrible experience which entirely destroyed my life. Well, to be honest, she didn’t start it, but neither was she very willing to fix the issues with false diagnoses, etc.
{code}
I do not think that they would have manipulated the data regarding medication. It is more a question of poor reporting and lack of critical analysis. As to the suicides, it is an intentional concealment. Why this has happened, I do not know. We will hear about this later this year from a leading Nordic researcher on mortality in psychoses in the Nordic countries.
{code}
OMG, more propaganda from Tiihonen, I presume?
Report comment
“I do not think that they would have manipulated the data regarding medication. It is more a question of poor reporting and lack of critical analysis. As to the suicides, it is an intentional concealment. Why this has happened, I do not know. We will hear about this later this year from a leading Nordic researcher on mortality in psychoses in the Nordic countries.”
Perhaps we’re seeing cohort studies from Jari Tiihonen on this topic. Previously, he has published cohort studies to support use of two concurrent neuroleptics (but not benzo), clozapine, injections, etc. Let’s see if I’m pre-cognitive.
Report comment
“But there have been development projects elsewhere in Finland and have been ion some respects a bit more innovative which have not been in the focus of attention internationally.”
Can you be more specific? How do they differ from OD?
Report comment
Also, from what I’ve seen in and about the public mental health services in more Southern parts of Finland… It’s more coercion, injections, etc. Patients get a cup of coffee if they get an injection. Active promotion of injections from the top psychiatrists. Etc. I have no clue where in Finland things in public psychiatry are actually getting *better*… it was horrible in there.
Report comment
Antero,
I’m sincerely sorry about those posts I made above. I had some bad experiences in public Finnish psychiatric system, and sometimes – especially when I’ve had wine – I start to rant about these issues. I will try to behave better from now on.
In any case, I think your posts about Open Dialogue were some of the more interesting ones I’ve seen on these forums in a long time. I’ve thought that Open Dialogue is perhaps even too much idealised internationally. It’s true that it is created for the needs of a certain local area and culture, and it probably can’t be very easily just transferred to other areas. The studies are maybe not very high quality. As you say, there are other systems out there which may perform as well or better for certain purposes. One of the big reasons for the international interest in OD is because it was featured in the last chapter of Robert Whitaker’s book.
I’m still somewhat interested in the short term use of benzodiazepines instead of neuroleptics in acute crisis. Maybe I’ll comment about it later on.
Report comment
By the way, you can find slides and video about this meeting of Gotzsche and the Finnish culture here, provided by the “Finnish Psychological Association”. I don’t know the true English name of this association, but it is the general association for all psychologists. Anyway. Here’s the videos:
http://www.psyli.fi/media/tapahtumia
Report comment