
Recently I came across a remarkable article, “From surviving to thriving: how does that happen.” The authors are Mark Bertram and Sarah McDonald, and the piece was published in The Journal of Mental Health Training, Education and Practice, Vol 10, Iss 5, 2015. The work was conducted in the vocational service department of a large mental health center in London, UK.
The authors’ purpose was:
“…to explore what helped seven people in contact with secondary mental health services achieve their vocational goals, such as: employment, education, training and volunteering.”
Here are some quotes, interspersed with my observations and comments.
“It is widely recognised that people in contact with mental health services are one of the most excluded groups in society. The causes of this exclusion are complex, multifaceted and not completely understood, but the facts are stark. Employment rates have hit their highest since records began, yet the majority of service users are unemployed (Office National Statistics, Statistical Bulletin, 2015).”
“Current critiques of the care programme approach (CPA) and the care planning process state that the work of mental health services through CPA is generally not effective — in terms of helping people achieve their goals and enhancing their life experience. There are calls for a fundamental change to the nature of the relationship between service users and professionals — with an emphasis on partnership and collaboration (Rinaldi and Watkeys, 2014).”
In fact, psychiatric care is inherently disempowering. Telling people, falsely, that they have an incurable, disabling brain disease militates against the notion that they can pursue their goals and improve their situation.
“The role of the staff is collaborative — moving from doing to or trying to fix, to helping people find their own way forward by identifying the things people are able to do and encouraging choice and control within a trusting relationship. This has been described as hope inducing and promotes well-being (Rapp and Goscha, 2010).”
“There are continuous calls for new ways of working in mental health services and knowledge from service users to be given its rightful place (Basset, 2008; Beales, 2012; Faulkner and Basset, 2012). What remains less clear in the literature is what service users are actually saying? Specifically, what do service users say are the conditions that help them achieve their goals, increase their well-being and be included?”
. . . . . . . . . . . . . . . .
The authors invited the service users at their center to come forward and be interviewed, with the objective of developing answers to the following questions:
“1. What areas of life were you struggling with prior to engaging in the peer support or vocational service?
2. What mental health services were you using and how was your mental health and well-being?
3. How were you involved in the project, what worked for you and what life changes have occurred as a result of engaging in peer support or vocational services?
Data analysis
The data were transcribed, content analysed and categorised under the key emerging themes. Validity checks involved giving the participants a copy of their interview with our interpretations. Some minor adjustments were necessary. Overall, the participants agreed that these records were accurate versions of their interview.
We then combined the qualitative data from all the interviews and through further reflection and content analysis we began to see patterns emerging — similarities between the nature and impact of people’s struggles and the types of conditions that people were saying helped them in a process of change and growth. These were listed on five pages of A4 [letter size paper] and consisted of 50 themes. To try and make the data clearer and more concise, we explored the possibility of creating images to visually represent the themes. We hired a systems designer and she was able to construct initial tree designs. We were then able to embed the themes into roots, trunk, branches and fruits.
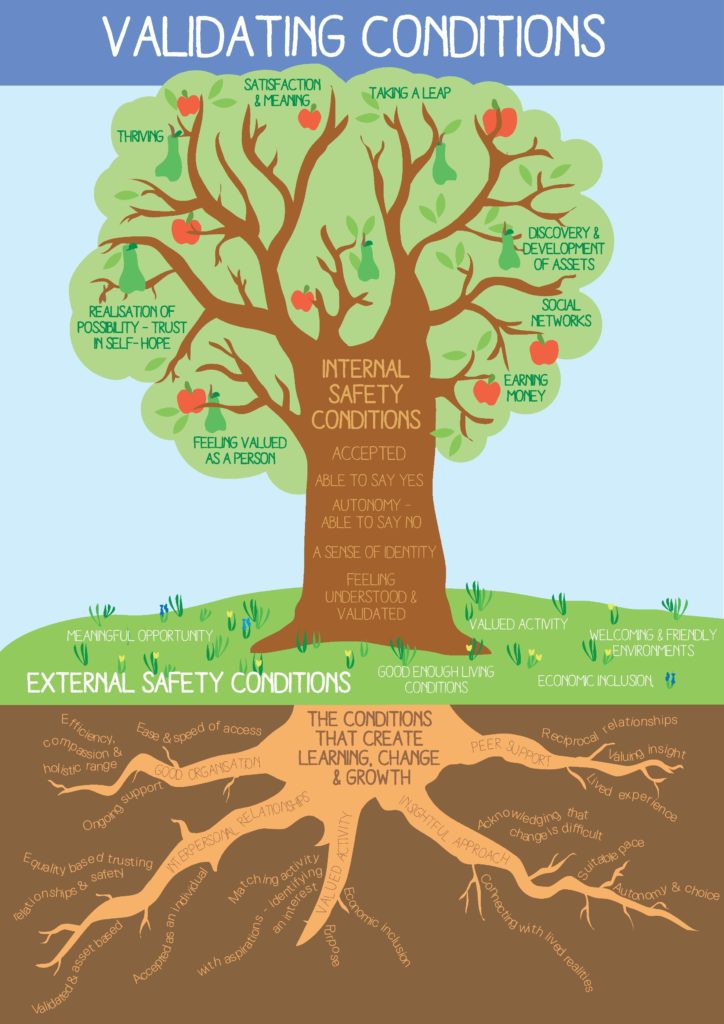
We shared these images with staff, peer supporters and service users and the response was enthusiastic and positive. People were saying these images and the themes represented their understanding of the invalidating conditions that cause distress and the validating conditions that facilitate a process of learning, change and growth. Gradually, a model of change — with all its inter-related parts and processes — emerged and this remained faithful to the insights people shared.”
Here are the tree images:
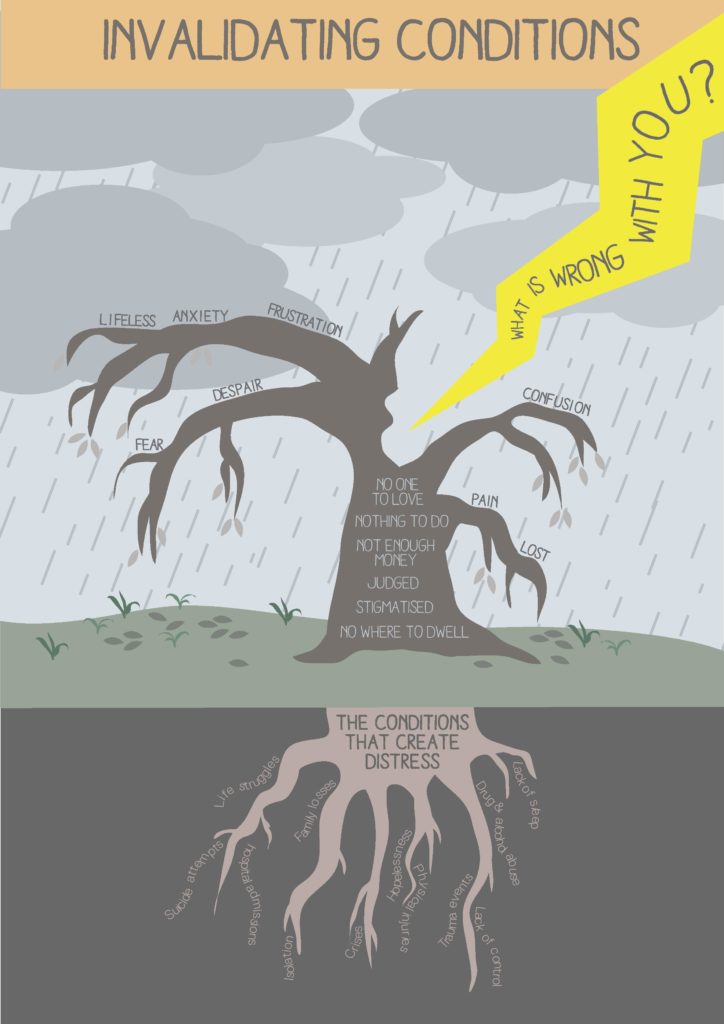
Under the heading Life Struggles, the authors pointed out:
“People were saying their main struggles with their mental health were related to problems with living and these difficult life experiences had created significant distress over a number of years. Consequently, everyone we spoke with had ended up in secondary mental health services for over five years. One person had been in services for 20 years, including 11 annual admissions to hospital. These were bleak, harrowing and painful situations that people arrived with.”
In their Conclusion section, the authors note:
“People were very clear and identified a wide range of life struggles that brought them into contact with services such as: income poverty, unemployment, trauma events, serious physical injuries, bullying, isolation, drug and alcohol problems, family losses, stigma, meaninglessness, hopelessness and a lack of sleep. It was the invalidating effects of these struggles that caused serious damage.”
This is in marked contrast to the standard psychiatric approach, which is to downplay the significance of these kinds of adverse events and circumstances, and to tell the client that he/she has a brain illness which needs to be treated with chemicals and/or high voltage electric shocks to the brain.
“However, all of the people we interviewed found their own way through and there are several important threads that bound their stories together. How people were perceived and treated was simply everything. It was the human, can do and co-productive approach within the vocational and peer support projects that shone through.”
Under the heading Recommendations:
“The evidence here reveals that the difficulties that bring people into contact with mental health services are multifaceted, but have common themes — problems with living and being invalidated. The challenge for all mental health services is to recognise and address the economic, psychological and social consequences of these life struggles. If these areas are not addressed then the demand on services will continue to increase because the direct causes of distress are not being resolved.” [Emphasis added]
How simple and clear. In my experience, people who are despondent are always able to explain in clear, simple terms why they are feeling despondent. And it always comes down to adverse events and/or abiding adverse circumstances. Psychiatry, however, self-servingly wedded as it is to spurious biological explanations, ignores this entire area, and focuses solely on “making the diagnosis.” So instead of asking open-ended questions and allowing the client to talk, they ask the questions on their inane, simplistic checklists: how often do you feel depressed?; are you less interested in doing things than formerly?; have you lost or gained weight recently?; are you having trouble sleeping?; are you sleeping excessively?; do you feel slow or sluggish?; do you feel worthless or guilty?; do you find it difficult to concentrate?; do you think about death or suicide?, etc.
And if the person answers yes to at least five of these questions, then voila, by the great miracle of psychiatric transformation, the hapless individual now has another serious problem: a life-threatening brain illness called major depressive disorder, which requires the ingestion of dangerous chemicals for life. What an unmitigated travesty!
And what a contrast to the simple, respectful, insightful, and entirely meaningful approach set out by Mark Bertram and Sarah McDonald in this paper.
“The wide range of current standardised approaches and pathology-laden practices in the mental health field need to be reviewed in the light of: the extent to which they invalidate or validate service users lived experiences.”
FINALLY
I cannot, in this short post, do justice to this paper. Besides its obvious merits, it offers a profound contrast to the drug-pushing, people-shriveling practices of psychiatry. Although the paper does not particularly promote anti-psychiatry, it does demonstrate that even people who have been drawn deeply into the disempowering maw of “mental health” can still articulate their needs, and can still find fulfillment in productive activity and self-direction.
Mark Bertram and Sarah McDonald have demonstrated that when people are weighed down by life’s adversities, what they need is authentic, validating support, not facile pathologizing checklists, and not tranquilizing or stimulant drugs.
I strongly encourage readers to study this paper and pass it along.














I have a much more jaded reaction to articles of this sort. I had a teacher once, a mental health professional, who was pushing the thriving versus surviving thing partly as a reaction to the criticism of psychiatric survivors. Thing is, given recent statistics regarding people with the most severe of labels, you’ve got less thriving than you’ve got dying in the mental health system, which remains, as pointed out, a system of exclusion.
I think to begin with you have to deal with those exclusions this article speaks of at the beginning, and nowhere do I see this being done. This would also be a matter of dealing with the power disparities that facilitate (loaded word) those exclusions. Here is the system, in other words, there is the mental health system, and, as a rule, the twain don’t meet. Your “break with reality” system is suffering, in this regard, from it’s own “break with reality”.
They are out to address the unemployment issue, are they? I’m not sure what “vocational services” means, but I know what “peer support” is all about, and it’s not about getting people out of this “break with reality” system. Ultimately, “peer support”–I don’t know–‘work’ or ‘play’–means expanding the mental health system. You’re getting more “consumers”, “chronic patients”, all the time, hire some, and you’ve got more workers to help carry the load when it comes to your growing patient population. The most radical experiments are the ones least likely to succeed, and the course of most “alternatives” here is to grow closer and closer to the traditional “forced treatment”, adjust them to “normalcy”, system.
“Distress”, too, always conjures up the image of the maiden in distress for me. Usually, this maiden is counting on the efforts of a knight in shining armor to rescue her from the harassment of some villainous character or another. There is also the situation of the wagon train being circled by native Americans, I think they called them ‘savages’, and praying to catch the clarion call of a bugle in the distance expanse. In my case, I’m not prone to see the mental health system as a knight in shining armor or the cavalry. Quite the reverse. The ‘alternative’ thing, too, here is evolving more into an adjunct to the tradition system than into salvation from it, at least, to my way of reckoning.
We discuss this or that approach, and while we are doing so, the population of people in treatment, what is it? 1/5 of the population in the USA, approaching that in other places, goes up by another .01 %. Those .01 %s add up eventually. What do we do then? Hire more “peer support” mental health paraprofessionals? Really? I’d seriously consider sending the mental health system a get-well soon card over this contagion, but…I don’t think it would do any good in the long run. What is the problem? The truth is out there in the world, not hiding from it, and I don’t think people are helped by seeking permanent sanctuary from it. People are basically alike, in the main, and it is only the mental health system that creates this false sense of difference between one and the other.
Report comment
Frank,
Thanks for this.
As you know, my primary position is that psychiatry is fundamentally rotten and destructive, and that the mental health system is the primary instrument of their activities. For this reason, I had some qualms about show-casing the work in question, but ultimately the notion of validating people vs. the opposite, and asking people what they might find helpful vs. telling them to take drugs, seemed important enough to warrant attention. This was particularly the case in that most of the people involved either stopped or reduced their use of psychiatric drugs.
I think Mark and Sarah showed that people who had been severely repressed by the psychiatric system for many years, far from being the victims of an incurable disease as psychiatrists tell us, were able to articulate their needs/desires, and achieve objectives, not with the help of some hi-tech “medical breakthrough” (such as smart pills, brain shocks, magnetic stimulation, etc.), but merely by being treated with respect and dignity.
On the broader front, I don’t believe that psychiatry, or the mental health system, can be reformed in any meaningful sense of the term. But I think it is possible for some individuals who work in the system to help some individuals escape the system. And the way they go about this is useful information.
Best wishes.
Report comment
I’d say great if I thought it would mean more people exiting the system. I’m more inclined to think it is just another program. The rhetoric, in other words, is bound to clash with the reality. You’ve got a lot of people colluding with psychiatry as a rule of thumb. Psychiatrists are among the top dogs in the system. If more people were actually tapering off psychiatric drugs, then maybe more of them would be able to function on their own. I’m not sure it is anything more than an option, occasionally taken, in this circumstance. I just worry that what is described in the PDF might be more apt to expand rather than to contract the system. I do imagine, although I could be wrong, that some things are not quite so bad in the UK as they are in the states. As you say, if it does help some individuals escape the system, that would be a very good thing indeed.
Report comment
Philip Hickey,
i liked your considerations of that article from: Mark Bertram & Sarah McDonald. Is the basic-basic, evident for the “victims” (that do not want to be victims).
Despite the damages being obvious (for the victims),… the whole psychiatric industry (and the rest of the parasites), is based on those feet of clay.
Yes, is worth reading the PDF.
The trees of the PDF (that are copied at this blog), are substandard, child-like. My advise to Bertram & McDonald is ask to do that “tree diagram”, to someone who is worth his/her salt.
The “artwork” at MIA… is also low grade (sorry for those who took the time/ effort to do it, but is my opinon).
No need to descrive why is weak art… you get it, or you dont.
Report comment
AntiP,
Thanks for coming in.
I’m no expert on artwork, but I thought the contrast between the two trees was compelling.
Report comment
Philip Hickey, hi 🙂
English is not my language, lets see if i can explain explain this…
If “compelling” is understanded as: “to exert a strong, irresistible force…” My opinion is: no is not, other will do better.
I did read the 12 pages PDF of Mark Bertram & Sarah McDonald.
Is nice that the authors made the effort to create a visual image of a important stand of the article. And they hired a designer that used colored trees (instead of the more common black and white linear diagrams).
The idea of using 2 types of trees is good (had potencial, if well used). Is not a new idea to use trees to explain a idea (has been used for many years).
But the execution of both drawings could be much better.
At the PDF says: “Graphic design (Trees) Sophie Walker”. The trees are so amateur-like that i thougth the authors did the trees themselves…
……………
Lets see:
The tree of the “invalidanting conditions” is at page 9 of the PDF.
The tree of the “validanting conditions” is at page 10 of the PDF.
1) The contrast is between the fonts of the words (and the background) is weak. That can be measured (but is very obvious). Amateur mistake.
2) The font used does legibility no favours. The fonts of the main article is fine (despite small, but that is normal at scientific articles). But at the 2 drawings of the trees have weak fonts, small fonts, bad contrast front vs background, and uses many different directions of text (with no need, i may add… as the text even makes curves!).
3) The choice of colours of the pictures of the trees (both background & text), reminds vintage pictures, with fading colours. Silly.
4) The space used by the pic is not fully used for the best legibilty. Is not optimized,
As a result… at a normal monitor, seeing the pdf to fit the width. Is very hard to read the words of the trees, due to: 1)2)3)4).
If the PDF is zoomed to 300%, the tiny words can be read. But it should not been needed. Even then (at 300%… reminds me the words/letters the facebook requires to type before a person can seen the page (are difficult to read).
And no, i am not promoting myself. I dont do trees 🙂
……………
As for the PDF of Mark Bertram & Sarah McDonald… i wish they had more statistics.
And Philip Hickey… if you want to see what a good artwork is… try this video of Hans Rosling:
Title: “Hans Rosling’s 200 Countries, 200 Years, 4 Minutes – The Joy of Stats – BBC Four”. duration: 4 minutes and 47 seconds.
https://www.youtube.com/watch?v=jbkSRLYSojo
……………
The person that done the trees could use Hans Rosling ideas… of using volumes/ position, related to the importance of the “words”.
Example: the tree of the “validanting conditions”, has a regular size apple called: “earning money” (rigth side, down). Yet… at the top rigth there is apple… the biggest one… with no text associated. Or is “taking a leap” associated… and bad posicioned?
Anyway what is more important? “Taking a leap”? Or “earning money”/ “having a job”?
We need jobs! We need oportunity to work! We need independance!
Surely much more than… “to leap”… ?
Thanks for reading.
Report comment
AntiP,
And thank you for the pointers on the artwork. I’m sure that Mark and Sara will be reading them carefully.
Best wishes.
Report comment
I read the pdf and to me this stuff seems useful. If I’d had support around what happened to me, instead of being asked what was wrong with me or being talked at, it would have helped.
Report comment
Misfitxxx,
Thanks for this.
Report comment
On a related note — Phil, maybe you would be the one with the knowledge and experience to write a manual about how to “pass” a depression screening, i.e. the right way to answer trick questions designed to get you on the fast track to drug dependency.
Report comment
Oldhead,
Thanks. I’ll give it some thought.
Report comment
The PDF in the above post’s link is addressed to service users. They sometimes call themselves consumers in this country. How does a person become a service user/consumer? Sometimes it is through psychiatric incarceration miscalled hospitalization. After the exclusion of incarceration, there really isn’t an open armed inclusion, as if anybody thought there would be. I don’t advocate for service using/consuming. I don’t see doing so as surviving if it is the mental health (mis)treatment system that one would be surviving. Survival, in my view, is outside of that system. I advocate non-compliance with treatment plans, that is, I advocate rejection of the mental patient role. With using/consuming it is usually drugs that are being used/consumed along with other types of would be assistance rendered. Drugs are another form of captivity, but they aren’t the only other form of captivity. There was talk in the above PDF of people discharged from their treatment teams. That’s another form of captivity, and it doesn’t end there. So long as people use/consume mental health services there will be mental patients. Hmm. How inconducive to so-called mental health is that? A mentally healthy person, after all, is a person who doesn’t consume/use such services by definition. I rest my case.
Report comment
This article really sums up the difference between helpful or unhelpful interventions: do they validate or invalidate the experiences of the people needing help? Do they bring hope or destroy hope? Do they move people toward feeling more capable or less capable? Too bad the world of psychiatry will never pay any attention, because empowering people doesn’t pay well enough!
Report comment
Steve,
Yes. Psychiatry will never get it, but it threatens their very existence as a medical specialty.
Report comment
Beyond Survival?
Well always beyond survival is going to mean righting that which is wrong. Maybe at first all one can do is survive. But after that, one should try to find comrades and to right the wrongs.
So as this is supposed to be a civilized society, redress and vindication will have to occur in either the criminal or the civil courts.
So we should be tracking legal precedents and supplying people with lawyers.
Report comment