
In a new Lancet paper, researchers Joseph Friedman, Helena Hansen, and Joseph Gone called attention to how the mortality rates of Native Americans have been overlooked and excluded. The term “data genocide” describes the erasure of American Indian and Alaskan Native descendants from public health metrics, contributing to inaccurate findings and poorly informed policy and funding decisions.
In particular, Friedman and colleagues explored the exclusion of Native Americans’ data from deaths of despair-related causes. They described this exclusion as a “double moral injury,” adding:
“Not only do Native American communities have the highest rates of midlife mortality from the causes of deaths of despair, but these realities are also almost entirely missing from a set of powerful mainstream narratives about health inequalities told through the deaths of despair theory.
This erasure of contemporary Native American presence and visibility plays a role in allowing health inequalities to go unchecked by depriving extreme disparities among Native American communities of the intense media and public attention that they deserve. Such attention—when properly contextualized through consistent reference to circumstances of Indigenous disadvantage—could play a role in galvanizing desperately needed additional health resources.”
 “Deaths of despair” was a term coined in an influential 2015 study that identified the stark increase in White Americans’ death rates during midlife (ages 45-54). Unlike their Hispanic and Asian American Pacific Islander (AAPI) counterparts, it appeared as though White Americans were increasingly dying from suicide, drug overdose, and alcoholic liver disease.
“Deaths of despair” was a term coined in an influential 2015 study that identified the stark increase in White Americans’ death rates during midlife (ages 45-54). Unlike their Hispanic and Asian American Pacific Islander (AAPI) counterparts, it appeared as though White Americans were increasingly dying from suicide, drug overdose, and alcoholic liver disease.
However, Native Americans were excluded in the original and subsequent deaths of despair studies. Deaths of despair were theorized to be a trend exclusive to the White US population. From this, several explanations arose to understand factors in the US that uniquely impacted White communities. For instance, deaths of despair were connected to the opioid epidemic and White Americans’ lower educational attainment and threatened social status.
Friedman and team highlight, however, that when compared to White Americans, Native Americans’ increase in midlife mortality rates was three times higher.
“If Native American people had been included in these analyses,” they write, “increases in midlife mortality would not have been determined to be uniquely high among White people.”
Including Native Americans’ data reveals that every year population data have been available, their mortality rates from suicide, overdose, and alcoholic liver disease have been higher. Since the 2015 analysis, the death rate of midlife Native Americans has further increased. In addition, the COVID-19 pandemic exacerbated social inequities leading to an even sharper increase in mortality rates. By 2020, Native Americans’ death rates had risen to over double White Americans’ rates.
Deaths of despair have not only increased more starkly for Native Americans, but they have been higher than the death rates of White people in the US for each year analyzed. The social inequity contributing to Native Americans’ deaths appears to have been worsening, while at the same time, these trends have been concealed.
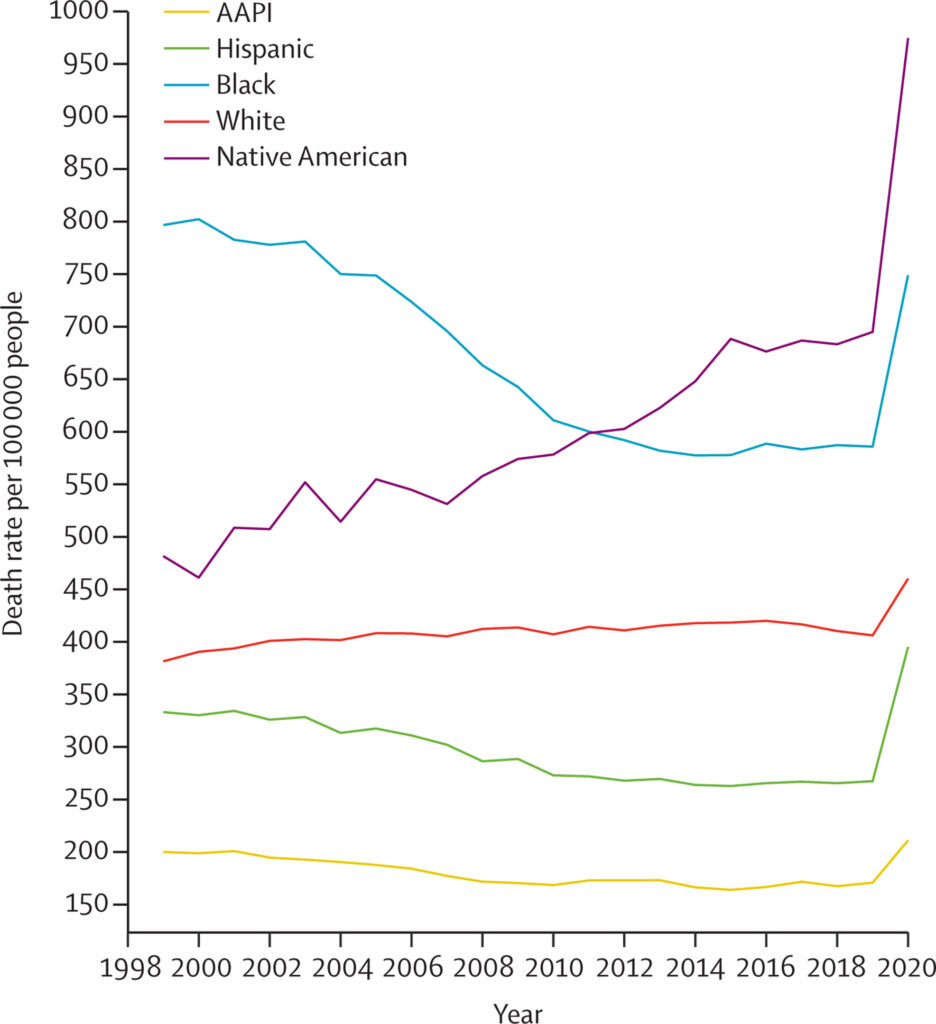
In addition to data about Native Americans, the researchers bring attention to the increase in Black mortality rates, which occurred at a higher rate than White mortality rates during the same period.
Deaths of despair have been misunderstood as only a White American problem.
“The narrative of overdose, suicide, and alcoholic liver disease as White American problems—tied to economic disinvestment from working-class White areas and related loss of social status—has reached widespread prominence as an explanatory framework in academic and popular press literature,” Friedman and team write.
“Yet this core idea of the uniqueness of White people being at greater risk to these causes of death was only made possible by the erasure of data describing Native American mortality.”
Given the prominence of these data, how is it that Native Americans have been consistently excluded from deaths of despair analyses? Friedman and colleagues highlight the importance of exploring this discrepancy:
“Narratives that center poor outcomes among White communities must be assessed critically, as they have historically overlooked and ignored higher rates of economic, social, and health inequities among minoritized populations in the USA.”
They highlight that “Indigenous data genocide” is commonplace, tied to the pervasive exclusion of Native American communities. As public policy decisions are increasingly decided using data, the exclusion of data “extends a long and shameful history of government-sanctioned erasure and data genocide of Indigenous People in the US.”
When data genocide occurs, social inequities remain hidden. Outcomes of this exclusion include ongoing underfunding and inaccessibility of the services that may remedy inequity.
Friedman, Hansen, and Gone proposed several guidelines to prevent the exclusion of data moving forward.
First, during data collection, Native Americans should be categorized and enumerated rather than labeled as other or excluded owing to small sample sizes. In so doing, Friedman and team caution against stigmatizing interpretations and recommend careful analyses, and Native American leadership, to reduce the risk of propagating misleading findings.
Second, Native American concerns should be centered in research collection and sharing processes to mitigate the risk of continuing exploitative research practices. They recommend privileging Native-led research endeavors and consultation processes and offer specific recommendations:
“Most relevant for national surveillance efforts, Native American leadership could be accomplished via Tribal consultation to establish a national Tribal data access and protections policy, investing in and partnering with Tribal epidemiological centers for rapid data response and dissemination; partnering with a small number of larger Tribal communities for sentinel public health data collection and dissemination (with concrete local benefits for Tribes), and partnering with urban Native American health programs for Native-led data gathering, linkage, and analysis.”
Finally, Friedman and the team underscore the importance of recognizing that health inequities are multifaceted and structural. Therefore, they are not so easily explained by any one factor or one solution.
One consequence of centering White Americans’ experiences is chronic underfunding and inattention to the diverse and complicated contexts that surround deaths of despair, especially in minoritized populations.
“To address unparalleled mortality from an overdose, suicide, and alcoholic liver disease, we suggest properly funding the chronically underfunded Indian Health Service; devoting resources to tribally controlled, evidence-based, and culturally grounded substance use treatment programs; and investing deeply in housing, employment, health care, and other community resources that address the upstream drivers of premature mortality.”
The researchers conclude:
“Large investments are needed in Native American communities to address centuries of dispossession and impoverishment—maintained today through systematic exclusion and public erasure—toward community-driven, self-determined initiatives that will preserve Indigenous futurity.”
****
Friedman, J., Hansen, H., & Gone, J. P. (2023). Deaths of despair and Indigenous data genocide. The Lancet (Online First). https://doi.org/10.1016/S0140-6736(22)02404-7 (Link)














Removed for moderation.
Report comment
A solution suggested back in 1984 from the head of “the most successful private company ever in Australian history”
https://www.youtube.com/watch?v=h-RV9reCDbY
Jump forward to 2016 and the State government was suggesting the forced sterilization of children without parental consent in the Mental Health Act. Not that it was going to be done based on race, that was just going to be coincidental.
Mind you, if you read the Kennedy Royal Commission into Police corruption we had the methods psychologists developed for Guantanamo Bay long before they started ‘coercing’ suspects at Camp X Ray. I’ve been wondering lately about ‘chemical waterboarding’ given the way people have been being involuntarily euthanised using a cocktail of benzos and morphine (along with blanket Do Not Resuscitate orders)? And in these times of environmental responsibility saving water is a good thing right?
There may be some subtleties to be worked out regarding dosages etc, but that shouldn’t be difficult given the ability to have police snatch test subjects from the community (just tell them they’re “Outpatients” and to prepare them by causing an “acute stress reaction”).
And of course there would be no avenue for complaint given the Police don’t have a copy of the criminal code and will return the complainant to the people who tortur…. I mean provided them with ‘healthcare’.
Even better that the Chief Psychiatrist is enabling arbitrary detentions by ignoring the protections afforded by the law, and considers the whole community “Outpatients” (care to see his letter?)…. the silly Community Nurse forging documents for him to utter with when the laws don’t even count? That’s taxpayers money he is wasting committing offences the police have to waste time covering up for him. The Community Nurse obviously aware of the legal protections that the Chief Psychiatrist is ignoring and thus neglecting his duty to the community on?
Still, it’s a young country. A place where the criminals get rehoused, and their victims get a lethal dose in an Emergency Dept, and get called crazy when someone rudely interrupts the process, and most importantly has Police retrieve the documented motive for the attempt to euthanise.
Big mistake that (not actually retrieving the documents before sending the “edited” version to the Law Centre. Never leave the victim with the proof of the “editing”), though not a real concern given they have methods of finding out “who else has seen the documents” and can steal your laptop to find out who you have communicated with….. and might have figured out what you’ve been saying isn’t an illness but the truth. They can then have their families threatened by police too (as they did to the psychologist who refused the police referral’ when I turned up with the documents a second time…. “your not meant to have these. I can arrest you for that [my own medical records Senior Constable?] And then refer you for nothing more than attempting to access the protection of the law…. that’s called a “hallucination” and requires ‘treatment’)
We can’t have the community knowing people are being snatched out of their bed by Police thinking they are “Outpatients” when they (a) haven’t got a psychiatrist or (b) haven’t been referred by police on “reasonable grounds” (though the Community Nurse did ask police to conceal his kidnapping for him with a referral POST HOC, and was declined by a cop with integrity. Is that the funniest thing you’ve heard this week? lol) Poor guy had gone to the trouble of torturing me to forge his statutory Form and then the cop refuses to make it all lawful for him?
Though when any complaints are being snuffed while police look the other way, why worry now? Euthanasia, even involuntary, is a ‘good death’.
https://www.youtube.com/watch?v=_03uXQiz6eY
waaaaaa If you’d have seen his face when they interrupted him….. still, it really was the only way to know how they were doing these ‘jobs’. The ‘Abraham test’. And well, he is good at his job AND has the stomach for it, just requires some training in being a little more restrained in who he is snuffing in the E.D. No ‘jobs’ for cartons of beer okay?
Report comment
It when despair is all used up and there are no more ways to acknowledge the great overwhelming anguish and pain that death cometh.
Report comment