
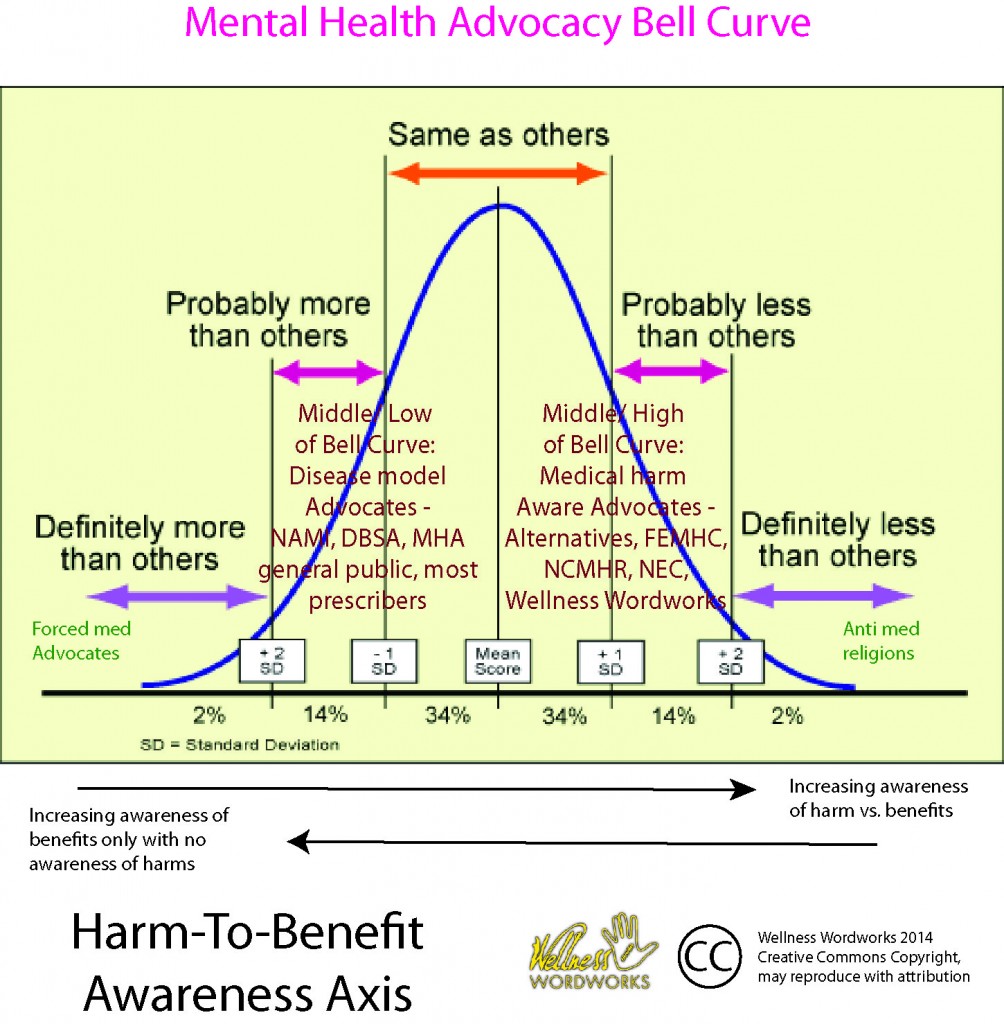
Allen Frances recently wrote a Huffington Post blog that made some good points about advocate compromise, but used some very insulting language and therefore made an inaccurate assessment of the problem. He is asking the mental health advocates to end a “civil war.” I am making the point instead, that it’s not a civil war. Dr. Frances is trying to get two ends of the bell curve together instead of addressing issues in the middle of the bell curve. In the middle, it’s people who know the science trying to educate people who don’t know the science.
Dr. Frances, like many people, is confused from the noise at the extremes from people that are flat-out lying about the science. Unfortunately, the people lying about the science have been in the ears and pocketbooks of several politicians lately, including, Dr. Murphy of HR 3717.
Here is the graphic. The four players are the forced med advocates (a tiny group), the disease model advocates (a big group), the recovery model advocates (a big group), and the anti med religions (a tiny group).
Dr. Frances says:
“There will never be any compromise acceptable to the die-hard defenders of psychiatry or to its most fanatic critics. Some inflexible psychiatrists are blind biological reductionists who assume that genes are destiny and that there is a pill for every problem.”
We really appreciate Dr. Frances’ work to challenge the DSM-5 and bring awareness to some of the medical harm in the mental health community. We appreciate Dr. Frances’ efforts to build bridges and mend fences and link communities. However, he isn’t really aware of our community’s viewpoint and challenges.
Here is a better and more nuanced look at the 5 types of mental health advocates. Dr. Frances is confusing a religious cult, which is truly against all medication, with 96% of all other advocates. Most of us just want to balance harm vs. benefit. It is true that people at the very far ends of the bell curve won’t talk. But I suspect about 96% of advocates are the middle of the bell curve on their awareness of harms and benefits. And we all do talk already. It’s only the 2% on either far end that refuses to compromise.
Dr Frances says:
“Some inflexible anti-psychiatrists are blind ideologues who see only the limits and harms of mental-health treatment, not its necessity or any of its benefits.”
Very few people in our community are anti-medication. We are pro fully-informed choice. If psychiatrists would do the work to learn the academic literature in their own field, they could give better informed choices so our advocates wouldn’t have to do work pro-bono that psychiatrists are already paid to do. So we might seem like “anti-psychiatrists,” but we are just promoting medical harm awareness.
“Anti-psychiatry” is like the N-word in our community. That’s a word that Dr. Frances’ community uses to feel good about ignoring our input, when there are at least 10 good reasons that our community knows more science. Mainly because it’s life and death for us, and we have more time on our hands and less risk to learn and talk publicly about new stuff.
Dr. Frances says;
“I have spent a good deal of frustrating time trying to open the minds of extremists at both ends — rarely making much headway.”
That is because the extremists on one end, the forced-med people, are not scientists; they are propaganda artists. And Dr. Frances confuses mainstream advocates on the other end with extremists. Mostly because we are angry at watching our brothers and sisters die, so our language is strong. So I am making that point that if Dr. Frances can’t tell the difference between medical-harm aware advocates and anti-medication religions, then he has not yet talked very deeply to our community.
For instance, here is an open letter to Allen Frances asking him to stop phrasing everything as an illness. The Hearing Voices community says that over 75% of people who could get a schizophrenia label recover spontaneously without any kind of treatment at all.
This is similar to the addiction community where 75% of people who could get an addiction label recover without any kind of treatment at all. In both communities, the long-term outcomes literature shows that people who do get “treatment” actually do worse.
For schizophrenia, the very short version is that antipsychotics actually cause psychosis by increasing the number of dopamine receptors in the supersensitive state. Now, this is in the aggregrate, in the long term. So some people will like and benefit from their treatment. But they are statistical outliers, not the foundation upon which public policy should be made.
Dr. Frances says;
“Fortunately, though, there are many reasonable people in both camps who may differ markedly in their overall assessment of psychiatry but still can agree that it is certainly not all good or all bad. With open-mindedness as a starting point, common ground can usually be found; seemingly divergent abstract opinions are not so divergent when you discuss how to deal with practical problems.”
The Hearing Voices blog linked to above already dealt with that “practical” list of suggestions from Allen Frances that wasn’t so practical after all. It turns out that the disease model of emotional distress has a lot of limitations and dangers than even Dr. Frances is not aware of yet.
Dr. Frances says;
“And finding common ground has never been more important. We simply can’t afford a civil war among the various advocates of the mentally ill at a time when strong and united advocacy is so desperately needed.
“Mental-health services in the U.S. are a failed mess: underfunded, disorganized, inaccessible, misallocated, dispirited, and driven by commercial interest. The current nonsystem is a shameful disgrace that won’t change unless the various voices who care about the mentally ill can achieve greater harmony.”
Well, the thing is, most emotional distress is not an illness. Calling it an illness is not a great way to help most people. Therein lies the difference. It’s not a civil war, it’s one view of science vs. another view of science.
In the middle of the advocate bell curve are medical-harm aware advocates that see that sometimes emotional distress is caused by life experiences. It could be past trauma experiences, lack of social connection, poor job fit or career goals, grief, loss of hope, spiritual emergency, or drug use, poor nutrition, lack of sleep, lack of exercise, or traumatic brain injury. Screening out this list of things is actually the ONE thing that all type of advocates agree on — but it rarely, if ever, happens in real life.
Dr. Frances says;
“Here is the cruel paradox: Those who need help can’t get it. We have half a million severely ill patients in prison for nuisance crimes that easily could have been avoided had they received adequate treatment and housing. Sleeping on a stoop, stealing a Coke, or shouting on a street can get a person arrested. Once arrested, not being able to make bail and/or not fitting in well with jail routine leads to prolonged incarceration and, too frequently, crazy-making solitary confinement. The U.S. today is probably the worst place and worst time ever to suffer from a severe mental illness.
“Meanwhile, those who don’t need psychiatric medicine get far too much: We spend $50 billion a year on often-unnecessary and potentially dangerous pills peddled by Big Pharma drug pushers, prescribed by careless doctors, and sought by patients brainwashed by advertising. There are now more deaths in the U.S. from drug overdoses than from car accidents, and most of these come from prescription pills, not street drugs.”
Agreed. The problem is well stated.
Dr. Frances says;
“The mess is deeply entrenched because
- There are few and fairly powerless advocates for the most disadvantaged
- The commercial interests are rich and powerful, control the airwaves and the politicians, and profit from the status quo; and
- The mental-health community is riven by a longstanding civil war that distracts from a unified advocacy for the severely ill.
The first two factors won’t change easily. Leverage in this David vs. Goliath struggle is possible only if we can find a middle ground for unified advocacy.”
This analysis is flawed because
- There are many medical-harm aware advocates, with much power, but Dr. Frances is confused between our mainstream of advocate community and the people at the ends of the extremes.
- The commercial interests pretty much just lie about the science and the status quo basically lets them, despite the fact that every single psych med category has now been busted for illegal marketing, and
- It’s not a longstanding civil war, it’s a propaganda battle. There are people who just basically make stuff up, and right now they have a lot of money and they are very loud. But the mainstream of advocates are people who know the science trying to educate people who don’t know the science. When Dr. Frances calls our mainstream community “anti-psychiatry,” he is ignoring a vast pool of science that shows very serious concerns with the current paradigm of mental health care.
Dr. Frances says;
“I think reasonable people can readily agree on four fairly obvious common goals:
- We need to work for the freedom of those who have been inappropriately imprisoned.
- We need to provide adequate housing to reduce the risks and indignities of homelessness.
- We need to provide medication for those who really need it and avoid medicating those who don’t.
- We need to provide adequate and easily accessible psychosocial support and treatment in the community.
“The arguments occur over the extent to which medication and coercion are necessary, and over who should get how much funding to provide what type of psychosocial support to which people.
“We can all agree that too much medicine is being prescribed by the wrong people to the wrong people and for the wrong indications. Eighty percent of all psychiatric medicine is prescribed by primary-care doctors after very brief visits that are primed for overprescribing by misleading drug-company advertising. Many psychiatrists also tend to err by being too quick to write prescriptions. Anti-psychiatrists err in the other direction, thinking that because they have personally done better without meds, no one needs them.”
I (personally) agree with the above, but why confuse the mainstream advocates with extremists at either end? This shows a real lack of awareness of the various advocacy communities.
Dr. Frances says;
“I think reasonable people can agree that we need to reeducate doctors and the public that medications have harms, not just benefits, and should be reserved only for narrow indications when they are really necessary. It is ludicrous that 20 percent of our population takes a psychoactive pill every day, and it is equally ludicrous that anyone should be sent to jail for symptoms that would have responded to medication if the waiting time for an appointment had been one day, not two months.”
Agreed.
Dr. Frances says;
“Coercion is an even more contentious topic, but one that also has a common-sense common ground. When, more than 50 years ago, Tom Szasz began to fight for patient empowerment, freedom, and dignity, the main threat to these was a snake-pit state hospital system that warehoused more than 600,000 patients, usually involuntarily and often inappropriately. That system no longer exists. There are now only about 65,000 psychiatric beds in the entire country, and the problem is finding a way into the hospital, not finding a way out.
“Anti-psychiatrists are fighting the last war. Psychiatric coercion has become largely a paper tiger: rare, short-term, and usually a well-meaning attempt to help the person avoid the real modern-day coercive threat of imprisonment. Decriminalizing mental illness and deprisoning the mentally ill should be an appealing common banner. And when you discuss specific situations, there is much more common-sense, common-ground agreement about when psychiatric coercion makes sense than when you discuss this hot-button issue in the abstract.
“Finally, there is the inevitable competition for scarce resources that causes conflict between professionally run mental-health programs and those based on recovery. The fight for slices of the pie gets particularly fierce when the pie is far too small to start with and is forever shrinking.”
Dr. Frances has missed the point. We are not fighting to get a piece of the mental health system pie, we are fighting for good science, for the application of the best and most effective treatment methods that would help the most people in the long term for the least amount of money. We are fighting for complete recovery. We are fighting to promote a way out of disability, a way to free our people from the disability industrial complex. We are freedom fighters – we have found a good life beyond the slavery of medications that cause more harm than good, from diagnoses that cause more harm than good.
We have found our way to the promised land of recovery and now we want to bring our family and friends into the new world of life beyond labels. What worked for us is not unique – the literature backs up that there is no difference between people who recover and those who don’t except that someone believed in us. We know we can hold the flame for other people, and we do.
We are fighting for the very lives of our brothers and sisters. We are fighting for our lives, still, many of us. Because this battle is so lopsided against us, we fight for ourselves every day, too. So we ask Dr. Frances to listen again, keep listening until he can actually hear us through our rage and our pain and our despair and not being heard again and again when we know the cure.
We know how to help people that experience emotional distress. We know how to solve the problem. Our battle is that people don’t listen to our solution.
Our battle is not to get part of the pie. We want to make the whole problem go away, and we know how.
Dr. Frances says;
“The common ground here is recognition of the fact that one size does not fit all. We need all sorts of different psychosocial support systems, because different people have different needs and tastes. We should be joining together to grow a bigger pie, not fighting for slightly bigger slices of a shrinking one.
“Rome is burning, and no one seems to be doing much about it. The ivory-tower institutions (like the professional associations and the National Institute of Mental Health) and the more grassroots organizations need to put aside differences and focus common advocacy on two goals that all can share: helping our most disadvantaged regain freedom and dignity, and taming the rampant and careless overuse of medication.”
These last two paragraphs are true, too. We are glad Dr. Frances came to our film festival to hear our people. But, next time, maybe he can hear beyond the surface of anger and pain, to hear into our knowledge of data and science and recovery.
Maybe next time Dr. Frances wants to build a bridge between communities, he can ask for our help to make an assessment of the actual problem instead of calling our community the problem. Because we know that our community actually holds the solution. So that way, if Mr. Frances keeps talking to us, then maybe we could solve the problem together.











If ‘mainstream mentality’ cannot hear the voices of those outside of their construct of reality, then perhaps the education and dialogue would be better served if aimed at everyone who is simply looking for guidance about how to best address extreme stress for themselves. After all, I don’t know anyone who hasn’t been thrown off kilter by life stressors. Right now, psychiatry/psychology is the default, because that is has been the propaganda programming from education and media. We’ve soaked it in all too well, as a collective.
If Rome is burning (which I agree, it is), then I think it’s best to walk away from the fire and build a new city with this new expanded awareness that has been so skillfully and passionately brought into reality by radical advocacy.
Of course, one can try to fight the fire, but personally, I feel that would be futile and a waste of energy. From where I sit, it is a raging inferno with a life of its own at this point.
Our personal resources of energy could be allocated more efficiently to a receptive audience, rather than one so rigid with resistance, with no subjective first-person experience whatsoever regarding the depth of what many of us have experienced, not to mention the amazing recoveries and healings so many of us have achieved, are achieving, or are well on their way to achieving. I’d say that this is what gives this movement its unique power. We do know exactly what we’re talking about, because we’ve been through it and back. To me, that defines the parameters of ‘expertise.’
Report comment
Corinna,
Your article here, not to mention your massive body of work, comprises an embarrassment of riches for me. I will try hard to digest fully your thought and references, as long as it takes.
For now, I just have to say, we are so lucky to have you on our side. I spent so many years thinking no one understood. But you do!!
What a relief and what a long unlooked for blessing.
Thank you so very much, from the bottom of our crazy hearts. You and so many authors here steal from me the sense of isolation. You have stolen from me my loneliness.
Please keep stealing more!
I hope that you can feel the groundswell of gratitude your writing invites.
It is beyond price.
It punctures time and space
With insight.
I don’t think we can ever
repay You.
Maybe the best
We can say
again and again
from
The dark places we
Inhabit
Thank You!!
You give us hope
You give us light.
It’s cold here,
I’ll never be able to say
How much warmth
Your words bring.
I know I’m
Repeating myself
I don’t care
True gratitude
Is worth repeating.
Report comment
Thanks for the nice thoughts and the poem. Here is a poem about the positives of being outside consensus reality. What people call “psychosis.”
https://www.youtube.com/watch?v=PfBKa9EpMzI
Report comment
A final thought.
As someone with a major mental illness.
You bet I need help.
I want so badly to return to
The person I used to be
Or even some
Semblance
Of functionality.
Give us real treatments
Not a scary gauntlet
Of
Russian roulette.
I would seek the
Help
If it was real help
In a
Hot
Minute.
Report comment
Just wondering why you want to return to the person you used to be? That person wasn’t working. A new person was called for.
Report comment
Maybe she wants to be the person she was before she was traumatized, diagnosed, then discarded.
Report comment
I don’t understand why some people in our movement act as if Dr. Frances is to be taken seriously as some kind of ally. Yes, it’s fine he criticized the DSM 5, but he openly said he was doing that because he was trying to prevent his profession from shooting themselves in the foot.
I think the way DSM 5 discredited psychiatry is just fine.
A “civil war” takes place when people who should be on the same side fight each other. Our human rights movement and Dr Frances are not on the same side. This is nonsense.
Further, I think it is a big mistake for us to be afraid of the label “anti-psychiatry” the way it is being used by Dr. Frances and E. Fuller Torrey. I am anti-psychiatry because I oppose psychiatry’s damaging practices. Nothing weird there. We are actually letting psychiatrists define anyone who opposes what they do as (almost) having some kind of mental illness. In no other area of politics could one side get away with this. As usual, psychiatry has no good arguments to justify what they do. Instead, they try to define anyone who opposes them as beyond the pale.
To some extent, I think they may be succeeding in getting this non-argument accepted in a lot of places. But does our movement have to accept this as well? This is senseless.
Report comment
YES! Ted!! thank you so much for saying what I believe is the bottom line here.
If ant-psychiatry=
*pro-truth,
*pro-science,
*pro-human rights,
*pro-justice,
________________
then call us all anti-psychiatry!!!
Psychiatry as it stands is completely anathema to truth, science, human rights and justice!
It is seriously upsetting to see this previous editor of the DSM start to try to blend in with activists, etc. by denouncing the current DSM and suddenly warn everyone about psychiatry. As if he wasn’t behind many years of deadly treatments. He now shrugs his shoulders about his past and instead distracts us and points everyone to the new DSMV. How many people died or were irreversibly harmed because of his unscientific and invalid work. Lest we forget.
Enough said.
Report comment
You are right NewPC. Frances is greatly responsible for the epidemic of ADHD bologna that we’re fighting now. He even admits to having helped create this epidemic. He says he’s sorry but it’s a little too late now for that. I for one do not want to sit in a circle, hold hands with him, and sing Kumbaya. Sorry. I won’t do it.
I too stand in the antipsychiatry camp and I do so proudly as one person who knows that many psychiatrists have more issues than the people who are their supposed “patients.” When the two “best” psychiatrists in the hospital where I work will not discuss, openly or behind closed doors, the WHO studies, Courtney Harding’s studies, or the studies of Harrow, or Whitaker’s two books, I have little respect for the profession. They know that they are wrong and they refuse to talk about any of it. All these two will say is that they and I have “large areas where we disagree with one another.” At this point it’s more honest for me to stand in the antipsychiatry camp.
Report comment
My concern is that the perception is different, that anti-psychiatry is perceived as anti-science. This is why I prefer the term “medical harm aware advocate,” because then it point clearly to both the cause and the solution of the problem.
Report comment
Ted,
I agree.
Francis is worried about the death of his own profession.
Nothing else.
Duane
Report comment
This and Alex’s comment is a good point and also the way I used to feel. After the Carter Center symposium I decided to just ignore the professionals and go it alone. http://www.madinamerica.com/2012/11/carter-center-social-inclusion/
After all, we can help one person who wants help in the time it takes to help 10 people who don’t want help.
But in the meantime, in the last two years, I’ve had a spiritual emergency, traumatic brain injury, and 34 re-concussions including two this week that delayed my response to your worthy comments here.
In that time, my personal spiritual guidance has been to sell “mental illness prevention” and “graduating a need for services” to the mental health providers. I am not clear on why I’m supposed to do this or how.
Your guidance may be difference if you have such. Your path may be equally valid, to continue protest approaches and to continue to raise awareness and fight injustice and speak truth to power. All approaches are useful. There are many types of advocates.
Report comment
He came to the MIA film festival?
He is engaging with these issues.
This is a huge sign that MIA and this movement is having an impact.
Report comment
Yes I agree with you Ted, Allen Frances is not a friend and not necessarily an ally. He came to the filmfest with an arrogance that is hard to bear. He told the participants what “they don’t know”, threw around a lot of statistics and made a plea for not fighting with each other because “we are all really on the same side of things”. Instead of begging for more tolerance of supposedly good-willed psychiatrists, I think he should be thinking about exactly what it is that psychiatry might actually have to offer. Thus I asked him and the panel of psychiatrists at the filmfest the following question: What exactly does a psychiatrist and psychiatry have to offer besides diagnoses and medications that are at best, not useful, and at worse, most harmful? Frances responded with a “let’s not throw the baby out with the bathwater” argument that diagnoses are heuristically useful and medications help people too. Saying that diagnoses are “heuristically useful” simply means that doctors have created a rather exclusive language that creates the illusion of reliability. In other words, it allows them to create and throw around terms like “depression” or “bi-polar disorder” or “borderline personality disorder” or “schizophrenia” and act like they are always talking about the same thing. You know, if we were not so tolerant of people who think differently, we might just think that such an illusion is really a delusion!
A more fitting answer to my question was given by Peter Stastny, who basically said that mainstream psychiatry has nothing useful to offer a movement of reform and we should simply continue to go it alone.
Report comment
I think it is brill that he came to the film fest, that he got asked hard questions and that his response is being debated here.
This is movement growth.
Slow but steady movement growth.
Report comment
I agree totally. I believe that we need to go it alone.
Report comment
go it alone but crow when people like Allen concede lots of our points.
Then carry on and head for the next target.
Wining in this sort of war is about slowly but surely deligitamising your enemies while building a community of resistance.
Report comment
Corinna hi,
Basically, I agree with your post, and I’m very impressed by your chart, and I quite appreciate your emphasizing (in bold print) these following sentiments,
“Well, the thing is, most emotional distress is not an illness. Calling it an illness is not a great way to help most people. Therein lies the difference. It’s not a civil war, it’s one view of science vs. another view of science.”
But, why, after that (just a bit further down), do you wind up offering a couple of paragraphs from Frances and then say, “Agreed. The problem is well stated”?
You are referring there to two paragraphs by Frances, and I think the 2nd paragraph may be stated well enough, but the 1st one is very questionable, imo.
Let’s look for a moment, at that one paragraph.
Says Allen France,
About his last sentence, in that paragraph (“The U.S. today is probably the worst place and worst time ever to suffer from a severe mental illness”), I can’t help but firmly disagree, for I believe that, in the U.S., “the worst time ever to [be viewed as suffering] from a severe mental illness” was during the era of lobotomies — the 1940’s and 50’s. (Approximately 40,000 lobotomies were ‘performed’ in this country.)
And, of course, the worst place and time ever be perceived as suffering a “severe mental illness” was Germany, in the middle of that same era (during the WW2).
(We all know, quite well what happened to ostensibly “severely mentally ill” people in Hitler’s Germany.)
I know, as far as psychiatric ‘treatment’ goes, we have all kinds of horrors going on still, today, in this country; e.g., there is still a lot of coerced “brief hospitalization” (which causes far more damage that Frances is willing to admit), and their is court-ordered ‘treatment’ for “outpatients”; not for a moment do I wish to downplay the harms of such abuse.
But, in comparison to the those other times and places (especially, WW2 Germany), most individuals who today are viewed as “suffering from a severe mental illness” actually have a rather fair shot at seeing through and escaping the worst horrors that psychiatry could offer them.
Particularly, with today’s Internet, the average person can rather easily discover ‘alternate’ views of such sufferings — including ‘alternate’ forms of ‘treatment’.
And, then, I can’t help but wonder about this line one: “We have half a million severely ill patients in prison for nuisance crimes that easily could have been avoided had they received adequate treatment and housing.”
Corinna, he keeps referring to “severely ill patients,” as he’s (apparently) meaning to refer to individuals who are arguably suffering ‘psychoses’. (Personally, I’d prefer to say, rather: he’s apparently referring to extremely emotionally distressed and/or acutely confused individuals.)
Of course, it should go without saying, there should not be prison sentencing for any individuals who have committed mere “nuisance crimes” — let alone for such individuals whose emotional and psychological sufferings may be so severe that they are genuinely quite out of touch with reality; having precipitated only committed mere “nuisance crimes,” they should be treated far more mercifully.
But, I seriously question this statistic: “half a million severely ill patients in prison for nuisance crimes”
Half a million???
I would quite appreciate it if you or anyone else can help me to understand where that 1/2 million stat comes from…
To me, it seems like it must be from NAMI and/or TAC (E Fuller Torrey) and purely false propaganda.
It seems a total impossibility to me; but, I wonder, to what extent should we accept any number even close to that one (500,000) as truly reflecting an approximate of how many people, officially identified as “severely mentally ill,” are currently populating our (U.S.) prisons — and indeed for having committed “nuisance crimes” and nothing worse.
Anyone who knows more about this, please, feel free to reply.
Respectfully,
Jonah
Report comment
P.S. — Still pondering how Allen Frances claims there are “half a million severely ill patients in prison for nuisance crimes,” so I just followed a link, above, to his Huffington Post blog, that’s titled “Stigmatizing and Shunning the Severely Ill.”
It’s dated not quite three months ago.
It begins:
“400,000.” Huh?
Did the the number of prisoners with “severe mental illness” in this country jump by literally 100,000 since late July?
Again, I’m wondering: Where is Allen Frances coming up with these statistics?
Report comment
You should not say “Where?” but “Why?”
Why does he claim 500,000 people in jail are innocent? because he wants psychiatry to own the prisoners, not the law.
He and psychiatry (and pharma Co.) will get money and prestige from “helping” the ill.
Report comment
Excellent truth to pitch in with…
Report comment
Jonah, you are right on this. I should have examined his paragraph closer. I was getting tired. I know jails like to label people so they can give them behavior control meds. Also, my one friend tracked down a bunch of data in Missouri showing jails were billed for 60 minutes of therapy but only delivering 5 minutes. Corporate racketeering stuff.
The funny story on this is that the jail lobby mafia sent a couple big ex-cons in a high dollar car to beat up my friend, Edward. Edward said the tipoff was when the ex-con said, “Why are you messing with US,” plural.
The dude starting smacking Edward, who was still walking with a cane after an accident falling out of a tree with a chainsaw when he was pruning at 3 am during a high energy [manic] phase.
Edward just smacked the dude back with the cane, expert like, and said my all time favorite come-back line. “Well, if I’m going to the ER today, you are going to come with me.”
The mafia dude left. That one jail contractor lost the 2 million dollar contract. I’m sure by now someone else picked it back up and resumed the BS.
Report comment
To let your comments show to a larger audience, why don’t you all comment on Francis’ blog in Huffington post. It is still open for comments with only 2 very small comments. Huffington post gets 200 000 000 visitors pr month and many read Francis’ blog.
Report comment
done it, thanks for the suggestion
Report comment
Huffington post is not displaying comments.
On my home computer I did leave a comment on Huffington post. If I go back it shows up.
BUT today I used the public libraries computer and discovered my comment is not displaying.
Report comment
Re:
“anti-med religions”
They’re not meds, they’re drugs.
It’s not a religion, it’s a legitimate concern.
Duane
Report comment
I think what I’m trying to say here is that we do not need to try to join the two extremes of the bell curve as Francis suggests.
In fact, we ought to be grateful for the very few on the anti-med curve, such as Dr. Peter Breggin – who has done more these past 60 years than any other human being alive. –
http://breggin.com/index.php?option=com_content&task=view&id=192&Itemid=94
Duane
Report comment
Hello Corinna,
You say
“The Hearing Voices community says that over 75% of people who could get a schizophrenia label recover spontaneously without any kind of treatment at all.”
However reading the open letter what is said is:
“In adults, around 75% begin to hear voices in association with a specific trauma, loss, or situations that make them feel powerless”. Is this the 75% that you are referring to?
In regards to recovering without medical treatment the open letter says :
“Significantly, it is well documented that there are many people who hear voices with the diagnosis of schizophrenia who have recovered successfully without long term medication use”.
Is there any evidence demonstrating that 75% of people with the diagnosis of schizophrenia recover without medical treatment?
Best wishes,
Russ
Report comment
“Is there any evidence demonstrating ” http://www.apa.org/monitor/feb00/schizophrenia.aspx
Harding’s study in The American Journal of Psychiatry (Vol. 144, No. 6, p. 718-735) showed that 62 percent to 68 percent of those former back ward patients showed no signs at all of schizophrenia. “They just didn’t have them anymore.”
Report comment
Sorry, I mislinked that link. It’s this article. Send me an email and i will send you the whole PDF if it’s behind a pay wall.
http://informahealthcare.com/doi/abs/10.3109/09638237.2011.562262
Report comment
Corinna,
I appreciate what you do and the time you obviously put into making people aware of various issues. But you really get this one wrong, on several counts:
You put ‘anti-med’ (it would seem ‘anti-psychiatry’ would also pertain) in the same league as pro-force, (just different ends of the ‘extreme’ spectrum), by insisting that both sides are lying about the science.
Really? When has Dr. Peter Breggin or ISEPP lied about science?
It seems to me that consent has been tried, and has fallen short, because lives keep getting ruined. FULLY informed consent is what is needed.
And compromising about the use of force has no place in any type of dialogue with those in the meddle of the bell curve; because ending the use of force does not need to be decided by popular vote, or referendum, or a platform with NAMI or DBSA.
That subject has already been addressed in the Constitution. We just need to make sure it gets respected, even if it means bringing some law suits against many of those at the far end (force advocates) along with those who support force in the MIDDLE of the bell curve (ie, leadership of NAMI mommies).
Duane
Report comment
My definition of “anti-med religion” is anyone who says there is absolutely never a benefit to “treatment.” It’s false science just as those who insist there is absolutely never any harm during “treatment.” I classify both ISEPP and Breggin with “medical harm aware.” They both admit some benefit to “treatment” in very rare cases.
I agree fully informed consent is needed. I have not finalized my opinions on forced treatment. 98% of treatment is “voluntary,” or would be if people could make real choices. So yes, Frances is right that arguing about 2% is a paper tiger, if this was an isolated isssue. But he doesn’t understand that the people arguing about the 2% are using it to make a whole bunch of bullshit false claims that confuse people when making decisions about the 98% of “voluntary” mental health care.
Report comment
I’ll stick with Breggin and ISEPP. Both are pushing for *fully* informed consent. We don’t have such consent at the present time. We have an (almost) monopoly, where “treatment” (conventional variety, with labels, drugs, ECT, and lockdowns) are anything but therapeutic. And this treatment, although not always done by force, is often done with deception.
I don’t care to see our community reach out to Frances or any other person in the status quo. I want to see the conventional system replaced (not reformed). So I suppose you could place me in the ‘extreme’ category. IMO, extreme conditions call for extreme solutions.
Duane
Report comment
I think, for instance that neuroleptics ought to be used as an absolute last resort, for extremely short periods of time. And that a person who has signed an advanced directive, against taking neuroleptics deserves to have it honored.
If the mental health community and judicial system want to argue this point, then the person with the “mental illness” has a right to a trial, with representation from a LAWYER (not a social worker).
This is an area where a large part of the bell curve gets it wrong.
And I see no room for compromise, unlike many of those in the larger parts of the bell curve, ie conventional shrinks and NAMI mommies.
Duane
Report comment
Duane: Richard Lewis recently suggested that maybe someone could say yes or no to benzodeopines. At one point in my life I was burning the midnight oil. Maybe all that was needed was a couple of good nights sleep.
Report comment
@ chrisreed,
As down as I am on conventional shrinks, I wouldn’t want for a moment to see adults lose their right to make their own medical decisions.
I think, if an adult is fully informed, they should be able to make these decisions. Even when they do not appear to be very wise decisions (some would call them ‘stupid’ decisions).
I don’t look toward any MIA writer/reader to get “approval” for my own medical decisions. In short, I could care less about any writer/reader’s opinion about the “safety” of taking benzodiazepines for a couple of days.
Duane
Report comment
‘98% of treatment is “voluntary,” or would be if people could make real choices. So yes, Frances is right that arguing about 2% is a paper tiger, if this was an isolated isssue. But he doesn’t understand that the people arguing about the 2% are using it to make a whole bunch of bullshit false claims that confuse people when making decisions about the 98% of “voluntary” mental health care.’
Corinna,
Maybe I’m misreading you, but you seem to be saying that “the people arguing about the 2% [forced psychiatric ‘treatments’] are using it to make a whole bunch of bullshit false claims.”
Are they all doing so, really, you think? (I don’t think so…)
As I am one who argues that forced psychiatric ‘treatments’ — especially, in terms of forced drugging, forced ECT, forced psychosurgery and other neuro-invasive ‘treatments’ — are truly de-humanizing procedures that function mainly as a convenience for psychiatrists and for “hospital” workers and for concerned family members of “involuntary patients”; such ‘treatments’ create, at best, “patient” subservience that may create a temporary sense of ‘peace’ in the psychiatric ‘ward’; but, such ‘treatments’ are ultimately abusive, terribly humiliating; they represent a unique form of personal defilement (ostensibly designed to help “patients”) that rivals the indignity of any form of rape and cannot, imo, ultimately be justified.
Anyone can be far better treated by other measures — non-violent measure…
So, I see that you say, of yourself, “I have not finalized my opinions on forced treatment,” that’s fine. But, I question your saying “I agree fully informed consent is needed” — because any forced and/or coerced ‘treatment’ puts an instant end to the possibility of informed consent.
If you haven’t already done so, I highly recommend studying David Cohen’s great MIA blog post, of just a few days ago (October 21, 2014) “It’s the Coercion, Stupid!”
http://www.madinamerica.com/2014/10/coercion-stupid/
Respectfully,
Jonah
Report comment
No you are not alone in your opinion. And yes, 98% of treatment is voluntary because they sit you down while they fill out the paperwork and tell you that if you sign yourself in, you can always leave, but if you don’t you will have to go before the judge who will see your refusal as a sign that you needed help. From personal experience, that isn’t peace. That’s fear. Example: dinner is over and silverware counted by six, but at one, a fog horn is sounded and all the lights come on, everyone is ordered out of the beds, and to take off their clothes. One staff member says she hot so they open all the blinds and the doors, and the staff that walk by outside can see us. (ages 14-17) We are told a fork was missing at six, beds are stripped, we are all forced to assume the position for a full strip search, while the staff make comments about our bodies, followed by showers without shower curtains just like we use the toilets without doors and have to have someone approve it before we can flush. we aren’t allowed to put our clothes back or keep our towels on because someone might hide the fork again.. We sit in silence for hours. Finally, I got called up to the staff desk. They really didn’t like me in the beginning because I wouldn’t tell them what they wanted me to. I had nice things so they said I was a hooker or that I was in love with my dad… fun. I don’t remember what she said to me anymore, but when I walked away I heard them talking about the new shift coming in. The one girl asked about the fork, but the one who loved to torment me, I heard her say, oh, I never lost it. I just wanted to kill a few hours until shift change.
Report comment
@ acidpop5,
One who reads your words can only, at best, begin to imagine how scarey and infuriating (and, I imagine, confusing) it must have been for you to have been forced to live in such an environment, as you’re describing…
But, for me, above all else, your story is infuriating to consider.
That is in part because I am the parent of a young woman, an adolescent, 17 years old; and, as I was, at age 21, ‘held’ against my will, by psychiatry, to be stuck with neuroleptic-filled IV needles and tagged with psychiatric labeling, I have unforgettable recollections of harrowing experiences, being ‘psychiatrized’ (including further, similar experiences, over the course of a couple years’ time).
Those were terribly traumatizing experiences; and, so, there’s nothing now (nothing whatsoever) that could possibly stop me from protecting my daughter against being ‘treated’ by psychiatrists. She will never wind up in a psychiatric “hospital” (as I did) — at least, not as long as I live and breathe…
And, what you’re describing is another kind of ‘treatment’ facility, I don’t know if it was called a “hospital,” but it was a place for kids, that could only exist, because of the so-called “diagnoses” that psychiatrists provided…
I presume that place still exists.
And, yes, I certainly recall you explaining in MIA comments previously, that your journey, as a ‘patient’ of psychiatry, began when you were a very young woman.
I am reminded of what you explained previously, by my reading of your story above — and can’t help but shake my head now, having read these further recollections you’re providing — feeling the immense travesty of it all.
Especially, as I read your story in the context of the blog post, by Dr. Allen Frances, which has been brought to our attention, by Corinna, I am struck by a sense of that travesty — and how it goes ignored…
(I wonder, is it possible that Dr. Frances — who was the lead author of the 4rth edition of the DSM — knows nothing of the existence of places, such as that which you’re describing?)
Surely, many young people are still being ‘treated’ as you were ‘treated’ by psychiatry, and many are being ‘treated’ as I was…
Yet, in that October 20, 2014 Huffington Post article, Dr. Francis explains,
Perhaps, too many times, in my MIA comments, I’ve mentioned that I was first ‘held’ by psychiatry after frisbeeing a number cheap plates at my parents’ garage door. Here, one more time, I mention that, such was the ‘incident’ that led to my ‘treatment’ — only to insist, that: Yes, I regret having thrown those dishes, but I threw them at a garage door — not at any person; and, I wish I could ‘only’ have been talked to, by someone who could have listened to me, back then.
And/or, if literally no one could have come to my aid, by ‘just’ listening to me, I wish could have had my day in court — instead of being convinced to meet with an E.R. psychiatrist…
Despite all of Dr. Francis’s fear-mongering, concerning the dangers of jails, I would have much preferred to be jailed (as opposed to meeting a psychiatrist).
Of course, there may have been a danger of meeting a psychiatrist in jail; s/he could possibly have ordered me forcibly drugged, there; and, that would have been a horrible fate, I’m sure; but, had I ‘only’ been promised my day in court, I would have happily risked jail time, in awaiting that day.
I could have avoided so much trauma that way (so could my family and friends have avoided much trauma).
Sorry to have gone on this way…
It’s good to see you again posting comments relating your own experiences with psychiatry…
Respectfully,
Jonah
Report comment
Rather than try to draw the larger portions of the left and right sides of the bell curve together, it seems to me it would make more sense to simply tell people the truth:
“Side effects’ is a drug company marketing term to imply a minor problem. In reality, these effect are main effects and serious. Despite the names given to these drugs, such as anti-depressant, anti-anxiety, and anti-psychotic, they are not smart bombs that attack depression, anxiety, or psychosis. They have a shotgun effect on your entire body, not just your brain. How they specifically work is not known to medical science. That is why they have many bad effects. These effects range from the minor (headache, dizziness, tingling), to the moderate (sexual problems, confusion, trouble sleeping), to the severe (brain damage, diabetes, suicide). When multiple drugs are prescribed, the danger becomes even worse.” – International Society for Ethical Psychology and Psychiatry (ISEPP) –
http://www.psychintegrity.org/content/files/Drug_Brochure_PDF%20%281%29.pdf
” In the long run, all psychiatric drugs tend to disrupt the normal processes of feeling and thinking, rendering the individual less able to deal effectively with personal problems and with life’s challenges. They worsen the individual’s overall mental condition and produce potentially irreversible harm to the brain.” – Peter Breggin, MD
http://breggin.com/index.php?option=com_content&task=view&id=187&Itemid=93
Duane
Report comment
I think we’re in agreement on the psych drug stuff. http://wellnesswordworks.com/psychiatric-medication-effectiveness/
As far as coercion, I did read David Cohen’s blog but I don’t like to call readers stupid. Also, I don’t think he addressed all the issues. I’m not an expert in the forced med area and don’t plan to become an expert soon. So I won’t dissect his blog point by point. Our movement does enough wrangling about this so leave me out of that discussion, please.
Report comment
To clarify, I think anyone who is being honest will admit to making some less than wise decisions. I wrote the book on stupid decisions in my 20’s, back in my drinking days.
I think we all deserve to have the *freedom* to make both good and not-so smart decisions. We live and learn.
Duane
Report comment
You know, I’m not even fighting for good medicine anymore. At this point, I just want to be seen as a person. I want people to understand that just because a diagnosis was made, that didn’t automatically rob me of my intellect and my individual goals. How can someone claim that he is speaking in the best interest of people he easily dismisses to something much less than human? I can’t imagine that we view the quality of my life on similar grounds.
Report comment
@ acidpop5,
Just because a diagnosis was made, you didn’t automatically get robbed of your intellect and individual goals.
Or your *worth* as a human being.
(Just thought it might be nice to hear it… from a fellow human being).
Duane
Report comment
I appreciate the thought, but it wasn’t my intention to sound like I doubted it these things. Doctor Francis description of the mentally ill he speaks for was demeaning and dehumanizing. More importantly, the way everyone but us get to chime in on what treatment we require makes us seem unimportant. The diagnosed doesn’t mean we stop being incredibly bright and creative people, it means, over time, all that is still there, our minds ate making the connections, but the medications just trap is in our own heads with all those thoughts and the inability to live any of them. Quality of life shouldn’t be judged on the fact that the patient is currently compliant. I also want to remind people considering mandated outpatient and impatient treatment, I know its easy to forget those patients are people with dreams and aspirations. Commitment, forced driving, monitoring… that’s not living.
Report comment
Good points.
Report comment
Huffington post (huffingtonpost.com) is either blocking or editing comments. My comments do not show up on the public city library computer.
Report comment
markps2 – Huffington post seems to be deleting comments someone or other doesn’t approve of – mine showed up, and then it was gone. Hmm…
As for tactics, we can agree and disagree but the overall picture is positive, and the movement is forward, though it feels oh-so-slow given the harm being done, the lives lost.
I take heart from the words of Howard Zinn at the May 15, 2007, Spelman College commencement. He said, in part, “The lesson of that history is that you must not despair, that if you are right, and you persist, things will change. The government may try to deceive the people, and the newspapers and television may do the same, but the truth has a way of coming out. The truth has a power greater than a hundred lies.”
Report comment