
I had an appointment with a doctor I had been seeing for a sleeping disorder at an outpatient clinic in a large psychiatric hospital in Montreal. My insomnia had begun a few years prior, when I stopped taking Risperdal for tics caused by Tourette’s Syndrome. I thought the insomnia was part of my withdrawal from Risperdal, yet it continued. I could not sleep without medication.
The doctor had told me that we would discuss a problem I had with a neighbour who would begin yelling whenever I entered my home. I had complained to my landlord but nothing was done. A few minutes after my appointment with my psychiatrist had begun, I was given a ‘choice’: I could either bring myself to the hospital’s ER or I could be brought there by security.
I would learn later after obtaining my medical records that I had been diagnosed with having auditory hallucinations. I was, according to doctors, schizo-affective.
After the bedlam of the ER, the calm and order of ward 408, where new patients were quarantined, was eerie.
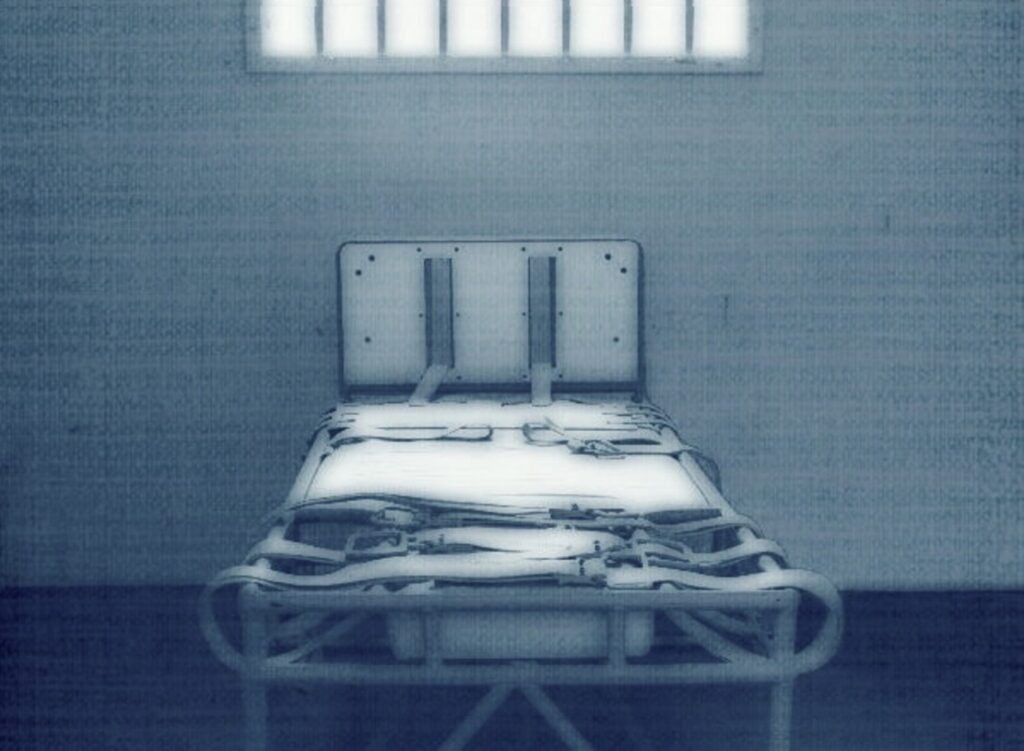
In the room opposite the nurses’ office was a bed fixed to the floor. It is fitted with restraints that can be fastened around a patient’s ankles and wrists, enabling limbs to be strapped down by nurses while security immobilizes the patient. The ‘observation room’ — on its far wall is an unbreakable window through which little can be seen.
For the new patient, the observation room is the source of intermittent yelling and anguished screams. These, he learns, end with the administering of a PRN. The room is as cold as a meat locker. Inmates are refused a blanket, the cold a valued feature for staff and part of the observation room’s chilling effect. The observation room is staff’s trump card. For a patient like myself who contests his hospitalization, containment inside its walls is an inexorable given. The only question is when.
Inmates in sanitariums were once routinely chained to walls. Medicine, we are told, has progressed since then. But a patient in ward 408 is soon disabused of this notion. Chains and other such simple and crude technologies figure still in the practice of psychiatry. The threat of their use is palpable. The fear it instills creates a bond between staff and patient, the therapeutic value of which can only be unique in medicine.
In many ways the quiet and seeming tranquility of ward 408 are a byproduct of the omnipresent fear caused by the threat of being taken to the observation room. A palpable physical presence, it hangs like a pallor over ward 408. Only the most obstinate and obtuse do not learn to fear confinement inside its featureless walls.
A new patient tells himself that only the most aggressive and violent patients are taken there. But then, of course, the full therapeutic benefit and effect of the observation room are not fully realized or exploited.
The room is unique in a legal sense. To be taken there is the same as committing a violent act. The caregiver becomes a witness for the prosecution to the patient’s crime. To escape prosecution for such crimes, committed or otherwise, is to accept unquestionably your diagnosis, whatever its clinical basis, and take your medicine, whatever the medical benefit.
Under this rough justice, perverse and sadistic staff, the guard dogs of clinico-medical privilege, are prized and protected by administrators. They, in return, may act with an impunity unknown outside the clinical environment. They are a law unto themselves.
The observation room, as a therapeutic technology or instrument, is, of course, based on sound scientific if not medical principles.
Behaviourists early on understood that punishment, when given arbitrarily and randomly, invariably induces helplessness. Indeed, if nothing you can do helps you to avoid punishment, you not only feel helpless but for all practical purposes you are helpless. For patients in ward 408, this was a familiar feeling and reinforced further the ‘therapeutic’ bond with caregivers.
A few days after my arrival in ward 408, Nurse C, my nurse for the day, told me that I looked stressed. I was preparing for a hearing in the afternoon. The hospital was seeking a court order to prolong my commitment. I declined her offer of something to relax me and returned to my writing. Nurse C left my room only to return with two security guards. I was now given another “choice.” I could go under my own power to the observation room or be forcibly taken there by security. I “chose” not to resist and walked quietly to the observation room.
The observation room quickly filled with nurses. What I now felt, though not clinically a kind of distress and better described in legal terms as a form of duress, only increased as Nurse C insisted that I open my mouth, say Ah, and swallow the medication that would be my ticket out of the observation room. As was my right under law, I continued to refuse the ‘medication’ Nurse C insisted on giving me. Finally, she put the small paper cup with the pills in front of my face. I pushed it away. I had now ‘acted out’ and ‘assaulted’ a staff member.
I was then tied by restraints to the bed. My pants were lowered and I was injected, according to the nurses’ notes, with “2 milligrams of Ativan and 5 milligrams of Haldol.”
My hearing was postponed until the next day. My reputed assault of a caregiver was entered as evidence of my dangerousness and grounds for my continued forced hospitalization.
A few weeks later I was still in ward 408. Another nurse, Nurse M, came to my room. He asked me to sit and talk with him. He told me, “The people here just want to help you.” I bolted up in my chair. The back of the chair broke a small piece of wood from the window frame above the heater.
The next morning two women came to my room with a camera. They were indignant and chastised me for my violent and destructive behavior. I told them Nurse M could support my claim that it was an accident. Despite the nurses’ report claiming that I had torn a two-by-four of wood a meter long out of the window frame, the chip in the wood was quite small.
The next morning, the window frame was repaired. The smell of the glue sickened me and I refused to stay in my room. My nurse, Nurse B, wrote in her notes that the windows were opened and that I was ordered to stay in my room. The windows in psychiatric wards, however, only open a few inches. Nonetheless I was told the room had been aired out. I told Nurse B. that I would not stay in my room. This was viewed as impertinent. Security was called and I was again injected with Haldol and Ativan in the observation room.
The Haldol induced extrapyramidal syndrome in me. My tremors were noted, and my inability to sit still and need to pace back and forth in the small confines of the observation room also appear in the nurses’ notes. The notes for that day are very detailed. After three pages, the letters EPS appear.
Acute akathisia is a symptom of extrapyramidal syndrome and a side effect of Haldol. The sufferer’s skin literally crawls. Waves of anxiety go up and down his body. He has restless leg syndrome. When he gets up and paces to try to calm the anxiety, he wants to lie down and relax. When he lies down, he wants to get up and pace. My EPS would continue for three horrific days.
The day I was transferred to ward 208, I had my first evaluation by Dr. P. For the first five minutes he refused to identify himself. It did not matter who he was, he told me. I had been diagnosed by four psychiatrists. He would extend my hospital stay, he told me.
He then began to yell. “You had to be restrained! You were administered repeated PRNs!”
For the next eight months, Dr. P’s yelling at me histrionically that I had to be taken to the observation room and restrained would be the sum total of our therapeutic relationship.
When my hearing in Superior Court finally came up after months of delaying by the hospital, Dr. P returned to this theme. Haldol is a molecule widely recognized for its effects on cases of extreme agitation like that I presented, he told the court. Akathisia is very rare with a first injection and the dosage of Haldol I was injected with was very small, he said, but it was possible, he conceded, that I had extrapyramidal effects like tremors or nausea. I was agitated and broke things and, in such instances, Haldol is administered and has a very quick effect, he explained.
Though Dr. P had not been in ward 408 on the two occasions that I was taken to the observation room, the judge accepted Dr. P’s claims without question and might as well have been in the observation room when the drugs were administered. In fact, I had imagined a judge, in his robes, signing the court order to inject me as nurses tightened the restraints around my ankles and wrists and Nurse B stuck the needle into my backside.
In the former Soviet Union, akathisia-inducing drugs were allegedly used as a form of torture. Haldol was used to induce intense restlessness and Parkinson’s-type symptoms in prisoners. This of course does not happen in Canada.
The question of Canada returns in my medical file.
The first time I was diagnosed with paranoia was in 2017. The doctor wrote: “Mr. Nolin denies being paranoid — he has documented crimes by Canadian governments.” (All translations from the original French are by the author.)
Four years later, Dr. P, in his ‘expert report’ presented at my hearing on forcible injection, said the same thing. “[Mr. Nolin],” he wrote, “denies being paranoid but claims to have documented crimes by the Canadian government.”
In paragraph eight of its grounds for forcible injection, the hospital gave the court my diagnosis: paranoid psychosis with a paranoid type delirium and paranoid personality. The supporting facts included a report by Dr. T, the psychiatrist I had seen at the outpatient clinic for a sleeping disorder. In the eight years I saw her, never did she mention paranoia but there it was on page twelve in the hospital’s report:
Mr. Nolin denies being paranoid. He says that he has documented crimes by the Canadian Government. He rejects attempts to restructure his thinking.
We include in our supporting documents a manuscript of 127 pages that had been provided us by Mr. Nolin. It implicates the Canadian Government in a plan to destabilize Cambodia that was responsible for many deaths.
The October 2017 evaluation says that I contacted the minister responsible for foreign affairs about my research on Canada and Cambodia and that he did not respond. The honourable minister did, however, deign to reply. He said he acknowledged my concerns, but no further action was taken.
The idea that my writing was grounds to forcibly inject me was nonetheless new to me. I had only first seen my medical file from October 2017 after an Access to Information request in March 2021. But there it was in black and white: I had had the temerity to accuse the government of being implicated in war crimes. But what indeed were the symptoms of my growing disease? I had maxed out my credit cards buying 800 pages of internal communications archived by Canadian foreign affairs on Cambodia in the 1980s. These included Ottawa explicitly agreeing to ‘sanitize’ the Pol Pot rump government-in-exile.
I shared the files with Cambodia specialists. In 2020, I shared my writing with the Norwegian embassy. Norway was seeking a seat on the UN Security Council, as was Canada. A former Quebec premier, Jean Charest, had visited New York to solicit votes. The Canadian Prime Minister, Justin Trudeau, visited Africa to this same end. Canada’s bid for a seat on the Security Council was rejected.
I do not know if my research influenced the UN Security Council vote against Canada. Perhaps not. But what I do know is that I was effectively tortured in an attempt “to restructure my thinking.” As Dr. T and Dr. P testified in Superior Court, the fact that I persisted in my research is attributed to my age. “Delusional disorders,” like my reputed ailment, the court was told, are not as susceptible to treatment as the hallucinations of schizophrenics. This is because I reputedly suffered from a certain ‘rigidity’ and the mistaken belief that forcible injection was “an affront to my autonomy.”
The day before my hearing in Superior Court, a pharmacist in ward 408 came to my room. I told her about my doubts about the panoply of drugs that the hospital was looking to inject in me. She explained how Abilify would correct all this. Holding out her fists, she said that they were like synapses that were too far apart. This resulted in negative associations. Abilify would bring the fists together and better associations would result. I was making inappropriate associations. Like Polygrip, Abilify would fill the gap between my synapses. I would be smiling again.
The idea that such crude methods and technologies as forced drugging and the observation room can “restructure” someone’s thinking is not new. As Critical Psychiatry has exposed elsewhere, class war between the haves and have nots is nowhere more evident than in a psychiatric ward, whether it is in the former Soviet Union or in the United States and Canada. The very identity and personhood of those who question the underpinnings of society are crushed and broken in the observation room. It is an instrument of an untenable status quo. Dissidence becomes both a disease and a crime where cure is indistinguishable from punishment. A hospital becomes an adjunct of the penal system where those guilty of crimes without victims — crimes of thought — are committed and imprisoned.
Incredibly, the doctors in my case stated explicitly and in no uncertain terms what they were doing. But was my treatment an anomaly? Are such abuses systemic? How many others have had their spirit broken by such means but have left no record?
For a psychiatric patient like myself, to ask such questions is to tempt fate. The observation room is where those who ask uncomfortable questions receive their answers — in no uncertain terms — and are isolated and silenced. To be taken there is to understand a terrible truth about a brutal society and its ‘caregivers’ — that the new order is imposed by the same means as the old; and that to question this order is indeed ‘insanity.’














We have to eradiate the mental health system and eradicate the idea that people need that.
Report comment
Thanks for the comment. I am not sure what you mean by “eradiate the mental health system.” Perhaps it is a typo. If you meant eradicate, I agree but where to start? By contesting one’s diagnosis and hospitalization? Through the courts and the complaint system?
Report comment
Joshua,
I do not want to necessarily eradicate the mental health system.That would be a serious overstatement. As a young man I benefitted, particularly from the year I spent in group therapy at the Reddy Memorial, a Montreal hospital that no longer exists. I was helped by the psychiatrists, psychologists and nurses that worked there. I continue to benefit from what I learned there and certainly would not want such institutions to be “eradicated.”
Report comment
There are people for whom false medical empiricism based on assumption “build back better” or on “growth”, is a death sentence. Psyche is not a broken leg, it’s identity with certain traits. Unchanging or changeable. We call it character. And you cannot extract the identity from the psychological context and pretend that it is a medical issue. This is fallacy and claim which should not take place. Character is a character, not a property of medical empiricism of psychopats. To think that we can change people using medicine is also naive and immature – vulgar materialism of Marxists in medical disguise. Psychiatry is cut off from nature of the psyche – and who will help you if they ignore sth inside you and beyond your small ego, which is immposible to change? Who will help you, if they know better ? Their arrogance is killing people for what they are, because they have wrong assumption on the psyche, based on biological growth. Psyche is not biology – psyche runs biology. Psyche is the captain here, not psychiatry.
Report comment
Thanks for the feedback. People do change. People who suffer from compulsions or impulse control do sometimes benefit from b. mod. Delusions are reputably less susceptible to modification…
Report comment
No, he meant “e-radiate”, maybe?….irradiate? Yes, “irradiate”. NUKE psychiatry! LOL!….
The so-called “mental health system” is a BROKEN JOKE….
Sure, yes, there ARE many good people in the system, but far too many EVIL ONES…. And, it’s a system-centered system, and a process-centered process…..
Can we convert or adjust it to be a SERVICES-CENTERED system, and a PERSON-CENTERED process?…. That’s a start…..
Psychiatry can’t exist without DRUGS, and the “mental health system”….
But, some kind of “mental health system” would work just fine withOUT the pseudoscience of psychiatry….
Report comment
Involving the public in the administration of hospitals is a place to start. It has been tried in Quebec but failed because of a lack of interest on the part of the public.
Report comment
Better yet, involve the PATIENTS & INMATES, & RESIDENTS in the running of such facilities…. Treating people like the responsible adults they are, or can become, is the BEST, most THERAPEUTIC way to treat them. On small scales, in various “alternative” settings, such an approach has worked wonders. But “the mental health system” in general, and psychiatry in particular, uses a system that disrespects and dis-empowers people. And you’re correct, – the general public shares psychiatry’s view of it’s victims. They DO NOT REALLY CARE AT ALL, despite their lame protests to the contrary….
Report comment
Yes, eradicate.
Where to start? Well first of all you never accept any diagnosis and you do your best to never put yourself in a place where anyone could give such a diagnosis.
So if people approach you and seem to want to do that, tell them to go away and not to approach you again, ever.
If you are in custody, you still have the right to remain silent. You have the right to a free lawyer from the point at which you are named as a suspect. If you aren’t a suspect, they really can’t hold you for more than a few hours.
The Mental Illness diagnosis comes entirely from what people say.
1. ECT and TMS should be prosecuted as Crimes Against Humanity. For anyone holding a government issued medical license who does that to another person the penalty should be death.
2. The Psychiatric Neurotoxins should not be on the market. But even as they are on the market, for anyone who gives forced drugging or drugging of a juvenile the penalty should be death.
3. Anyone who holds a government issued medical license and prescribes the neurotoxins to a consenting adult should receive a life sentence.
4. Anyone holding a government issued medical license who tells someone that they are mentally ill, should receive a 20 year sentence.
5. We should not allow our government to be licensing any kind of Psychotherapists or Behavioral Therapists. Most of the harm they can do is the direct result of this licensing. Cutting off the licensing does not stop the therapy from happening, it just makes it outside of government approval.
6. Anyone who does any kind of therapy on a Juvenile should be required to report that to Child Protective Services from the first visit, and to keep them regularly updated. This will shut off the Fix My Kid Doctors. The triggering event for suspected child abuse should be simply that the child shows up at their office door.
7. We all have to learn to stop talking about people and creating the impression that they are Mentally Ill or have Autism/Aspergers, or of ever suggesting that anyone needs Therapy, Recovery, Support Groups, or Salvation.
And we have to fight California Governor Gavin Newsom who has long been trying to turn California into a 40 million bed mental hospital. He is now targeting the homeless, a marginalized group, and he wants to set up mental health courts in every county and to do forced treatments.
We must stop him. Start by getting the Democratic Party to nominate someone else.
Joshua
Report comment
Nah, I oppose the death penalty on principle…..Life in prison with forced neuroleptic injection would be JUSTICE SERVED to the worst of the psychiatrists….
And, until & unless they are held accountable, and FINANCIALLY LIABLE, no government should “license” psychiatry….to license is to accrue culpability & liability….
Some more good FIRST STEPS towards the absolute eradication of toxic psychiatry:
1. The A.P.A. (“psychiatric ass’n”, NOT “psychological ass’n”….) MUST cease all NEW memberships, and allow the A.P.A. to DIE OFF by terminal attrition….
2.Announce *NO DSM-6*….Let the DSM-5 END THE FRAUD….
Those 2 steps alone would bring medicine forward in time a century or more….
Yes, the state of “current” “medical science” in 2022, is in fact late 1800’s vintage….
Much newer chemistry today, and drugs, and Electro-Cution Torture, but an 1800’s mentality…..
Report comment
Joshua, people can be held on psychiatric wards without their consent for much longer than a few hours. It is not the same as being in jail – one has no right to a lawyer.
When you say: “…you do your best to never put yourself in a place where anyone could give such a diagnosis. So if people approach you and seem to want to do that, tell them to go away and not to approach you again, ever.”
But you forget that many people receive a psychiatric diagnosis when they are involuntarily committed. This happened in my case almost 10 years ago. I could not tell psychiatrists to go away and not to approach me again – in fact, if I had talked to them in this way, this would have been seen as a symptom of my “illness” and I would have been surely prescribed higher doses of neuroleptics… (I was forced to take them in the hospital, just like Phil).
Report comment
Yeah, I love it when telling them you don’t want their “help” is an indication that you NEED their “help” because if you were “mentally healthy,” you’d automatically agree with them about everything! Talk about “crazy!”
Report comment
Steve, it’s a Catch 22 — you are crazy if you don’t and crazy if you do. After I was poisoned with EPS and severe akathisia I became even warier of psychiatrists. This only further confirmed my diagnosis as paranoid.
Report comment
Quite so. It is an endless loop. Heller captured this idea so well with Catch-22!
Report comment
I had a close friend who was being abused by “the mental health system”, and she reported the abuses her landlord inflicted on her. She was not believed. She was accused of being delusional, or fabricating stories. The Court illegally evicted her into homelessness, after “child protective services” wrongly took her daughter away. Within months, her 8yr. old daughter was in the State mental hospital on neuro-toxic psych drugs. Mom left the State, and I lost touch with her. Yes, the practice of psychiatry DOES CONSTITUTE GENOCIDE….the actions of “the mental health system” do meet the legal definition of genocide against vulnerable persons. So, I validate your experiences.
Report comment
According to Allen Frances you are crazy if you think you’re sane, and worried well if you believe you are mentally ill. Why these people think they are mentally ill? Maybe because someone with an MD told them they were mentally ill, but they’re the problem for believing someone with an MD.
Report comment
I agree with both of you, it’s a Catch 22!
Report comment
Just wanted to say I appreciate and agree with what both Joshua and Bradford writes. Where i’m from(Sweden), there is almost no one with similiar opinions. At most we got people who supports (various forms of) alternative psychiatry, and so there still is the “seek professional help”, “recover” and similar crap.
Report comment
(Duplicate Comment)
Report comment
removed for moderation
Report comment
Joshua,
What I would want to change is the system of recourse for inpatients. I wrote to the Ombudsman after my experiences in the observation room. They refused to intervene. There are very limited recourses for an inpatient.
Report comment
Phil, I totally agree with you. When I was held on a psychiatric ward in 2012 (in Poland), I was not even informed that there was a psychiatric Ombudsman who had a duty to regularly visit the wards. I have never seen this Ombudsman and I think that his visits existed only on paper…
Report comment
Joanna, thanks for your comment. It was only after I was discharged that I finally talked to the ombudsman in any important way. All I could do was file a complaint against her with the State, her employer. As an inpatient, I did have a right to a lawyer. After four or five, paid by legal aid, I found one who took the time to know my file,which was admittedly a quite complex one. There are other resources for patient’s rights but most don’t deal with psychiatric patients. And many people on the outside don’t know and wouldn’t believe anyway what happens in a psychiatric ward if you told them. We need to get the message out. MIA does important work…
Report comment
Phil, thanks a lot for your reply. It is so disappointing that you actually had to file a complaint against the ombudsman! I am happy to hear that you did have a right to a lawyer and that you finally managed to find a trustworthy one.
You are so right in saying that many people on the outside “don’t know and wouldn’t believe anyway what happens in a psychiatric ward” – I fully agree with you that MIA is doing crucially important work.
Report comment
Joanna, it is extremely unfortunate that many rights exist only on paper. There are no consequences for their violation.
In Quebec, Protecteur du citoyen is responsible for complaints against public entities like the ombudsman. When they close your file, that leaves only the courts. A consultation with a lawyer is several hundred dollars…
Report comment
Phil, this is so depressing and unfortunately you are so right: many rights exist only on paper!
Report comment
Phil Nolin, we need to intervene with severe criminal penalties, as well as with financial consequences, otherwise this is a conversation which goes around in circles and circles for decades, and still it goes no where.
“Life in prison with forced neuroleptic injection would be JUSTICE SERVED to the worst of the psychiatrists….”
That would be cruel and unusual punishment. Civilized societies do not do that.
Only 3 categories of persons would be effected by the above:
1. Those who work with children regularly are already required to report in suspected cases of child abuse. Trying to investigate it themselves, or trying to council the people, does not constitute compliance. Failure to report is a state felony, and it is also a federal felony.
The problem is that it has not been clear how high the bar should be for suspected child abuse. The public clinics are quite good at reporting.
But the Middle-Class defines itself by not using such public clinics, and instead by hiring its own doctors. These doctors have got nonreporting built right into their business model.
If they are forced to report, then their business is finished.
As far as what happens when they report, it would likely depend on what they are able to say in the report, and on whether or not there are prior complaints. And then there will be follow up reports. If CPS feels it rises to such a level, they may do a well being check.
And why should such therapy not be supervised by an outside authority. Otherwise it is just doctors marketing to parents.
2. The Government. We should not be allowing it to license psychotherapists and behavioral therapists. We don’t license fortune tellers, psychics, or faith healers. The Government licensing is what sustains the idea that survivors are not well.
3. Those with Government issued medical licenses. They should not be able to use that license to do things to people which have no medical basis, like telling them that they have Mental Illness or Autism – Aspergers.
20 years.
And they should not be able to prescribe medicines which are only for behavioral control and suppressing people.
Life
And they should not be able to authorize forced drugging, or drugging of juveniles, or ECT, or TMS, or Lobotomy.
Death
Otherwise we have to keep arguing with them. This way we just need to dig a few mass graves.
Science and the Swastika : Hitler’s Biological Soldiers
https://www.youtube.com/watch?v=pQAdwjYc_VE
Doctors Trial
https://en.wikipedia.org/wiki/Doctors%27_trial
Joshua
Report comment
Joshua, I like your comments & ideas, and I’m glad you post here at MiA, and I hope you continue to do so. So my argument is NOT with you personally, but rather with the ideas and words you present.
When my parents took me to a psychiatrist in 10th grade, at age 15, I was given a prescription for neuro-toxic drugs, which ruined the next 20 -25 years of my life. And a bogus & fraudulent “diagnosis”. ANY psychiatric “diagnosis” is the civil equivalent of a criminal sentence of LIFE IN PRISON, WITH NO POSSIBILITY OF PAROLE. Have you EVER heard of ANYBODY who has been told they have NO diagnosible psychiatric condition. No psychiatrist would EVER say that! The staff at the local “community mental health center” regularly LIES about one of my best friends. These LIES are used as justification to ship her to the State mental hospital, in handcuffs and shackles, in the back of a Sheriff’s cruiser. She is Court-ordered to be needle-raped and pill-raped on a daily basis. She SUFFERS, and STRUGGLES, not with some bogus psychiatric “diagnosis”, or imaginary “mental illness”, but rather she suffers from the abuse, and acts of GENOCIDE comitted against her by the so-called “mental health system”. So you’re wrong, you seem young, over-idealistic, naive, and uninformed of the actual BRUTALITY inflicted by an UNCIVILIZED, BARBARIC “society”. Life in prison with forced drugging would in fact BE JUSTICE SERVED for many, if not most psychiatrists. Not all, certainly, but MANY, if not MOST psychiatrists are GUILTY AS CHARGED. Have I changed your mind with the TRUTH, Joshua?….
Report comment
Bradford, there is always a danger of false positives — of being diagnosed with a disorder you don’t have. In court, a dr. needs the opinion of a second doctor to have a patient’s institutionalization prolonged. In my experience, these assessments are pro forma. You meet a dr., say a few words and he supports your treating doctor’s diagnosis based on a five minute evaluation. If the patient was reticent to talk or wary of doctors (after being involuntarily confined and drugged!),then he is “paranoid and delusional.” This has more to do with making a brief against the patient than caring for the patient as someone who may or may not require medical care…
Report comment
The problem I see is that there is no way to ever prove them wrong. If they claimed you had high blood pressure, you could have someone measure your blood pressure and say, “See, it’s in normal range.” But with psych “disorders,” it is always a matter of someone’s opinion, and anyone with an MD gets more autotmatic credence than the average Joe, and a LOT more than someone they’ve labeled with a “mental illness.” As long as there are no concrete criteria for deciding who “has” and “doesn’t have” a “mental illness,” the psychiatrists/psychologists/doctors will always be in control!
Report comment
Steve, Yes I have seen doctors’ evaluations that speak explicitly about “control” and who controlled the evaluation. Psychiatry also shares much with the soft sciences. The personal philosophy of a physician often figures in a diagnosis. And then there is the collegial aspect where doctors are afraid to criticize a colleague. If they do, it can have legal and personal implications. A wrong diagnosis can be actionable. So there is also a question of money …
Report comment
This ‘diagnosed with a disorder’ stuff in psychiatry is nonsensical. It’s not like someone presents with a fever and an altered sense of smell and on nasal swab and bloodwork investigation, you find out they have coronavirus (which is an external infectious disease causing a problem). All they do is re-word behaviour with circular labels, and then give those labels agency, as explanations to problems. It’s a dangerous slight of hand trick. And just look at those ‘disorders’ and how they’re used. Social media provides good insight into the political and legal nature of these.
One look at the following discussions is enough to make you gag with revulsion:
In the interests of not getting my reputation destroyed, please note that I have NEVER been labelled with this psychiatric ‘diagnosis’/label/categorisation. This post is merely to explain what psychiatric categorisations, irrespective of what they are, are like:
Readers are welcome to visit some of these threads:
1.) What is the most effective way to deal with a slander campaign from a Borderline Personality Disorder ex?
2.) Have you ever been widely slandered by a person with Borderline Personality Disorder? How did you handle it?
3.) Is is best to cut someone who has BPD out of your life?
4.) Why are people with BPD so hated?
In the 4th link, Nav Ng who says he’s been abused by a ‘BPD woman’ writes pretty clearly:
“BPD people:
For God’s sake don’t start any relationships without warning potential partners of your condition. Kindly don’t inflict your misery on the rest of us.
And don’t ever bring a child into this world, it is worse enough already with the rest of us suffering from your lot being let loose in society. Consider sterilising yourself, if you have any empathy left.”
Now, each of these people write about their experiences with certain abusive and difficult people. But note that none of them simply say that: that they have had abusive people in their life. They shoehorn the term ‘Borderline Personality Disorder’, a defamatory and tautological psychiatric categorisation into the picture. And individuals in mental health have the audacity to say that these categorisations are ‘just like diabetes and cancer’. They are absolute bastards for saying so. Forgive my language, but calling them bastards is very mild compared to what they do. They deserve it.
People should always get justice from unwarrantedly abusive people. But not on the basis of psychiatric categorisations. Rather it should be based on actions and mitigating circumstances.
This is clearly a function that psychiatry provides. To do away with unwanted individuals, not simply in terms of their actions or behaviour, but rather on the basis of the psychiatric categorisations applied to them. It always provides a useful function to label the opposite party with some kind of a ‘disorder’ for this purpose. In those same links I provided, you’ll find people put under the BPD categorisation argue with people trying to disprove their position about people with BPD. None of these guys realise they’ve been massively duped by people more powerful than them when they sought out help in vulnerable situations. They’re in the ‘it’s all science’ phase of their lives.
For all the abusive individuals placed under these categories, think of how many people whose lives have been ruined by abusive individuals got placed in these categories.
It is perfectly legitimate for people to ask to be not labelled with ANYTHING in the DSM. It’s a legitimate defensive response. Unfortunately, I do not think you can get legal justice from people who have MDs in Psychiatry when they do that.
Members of the public and mental health workers have gotten used to mockery, condescension and gaslighting in terms of ‘it’s common for these people to deny their illness’ types of statements.
I have also had severely abusive people in my life. But I hate these categorisations and what mental health workers do to people MORE than I could ever hate what these abusive people have done. I want justice too. But on the basis of behaviour and actions alone, and not psychiatric categorisations.
I do not care what a person has done. He/she might have stomped on the heads of ten 6-month old babies, crushing their skulls and making their brain ooze out like toothpaste. A person might have set an entire village on fire. A person could have gaslighted a victim into madness. In such cases, their victims should get justice based on the behaviour of these perpetrators. NOT on the basis of supposed ‘diagnoses’ of this nature.
Note: MIA team, please provide a text-editor on this website. This way of writing is very cumbersome. I have to manually type the syntax for hyperlinking, for making words bold, italic etc.
Report comment
Think of how many already hurt people psychiatrists and psychologists have (even inadvertently) re-hurt and marginalised from society by psychiatrically labelling them, only for those people to be gaslighted into oblivion and anonymity. Into a corner with no escape. It’s truly disgusting. They are perverse. I don’t care how much they smile on social media or YouTube, or how nice they are to their families, or even if they are ‘kind’ to vulnerable people in vulnerable situations, if this is what the end result of their actions is.
Report comment
Also, just to mention: I am so grateful for this website and the whole team on here. It must have been even more horrendous than it is today, for people trapped in the mental health system and gaslighting families/people before such places. No place to tell your truth or truth in general, like it is.
Report comment
Sorry I missed your reply last week! You are correct. Court-appointed attorneys are another JOKE. Despite their SUPPOSED role, their ACTUAL role is to create the appearance of representing the oppressed “mental patient”, while actually facilitating their involuntary servitude. The practice of psychiatry is in fact unconstitutional….
Report comment
Joanna wrote, “people can be held on psychiatric wards without their consent for much longer than a few hours. It is not the same as being in jail – one has no right to a lawyer.”
Yes you are correct. Though I believe that there is some variation state to state. And these practices are completely unconstitutional. But this is the core problem with the Psychiatric System, that you have less rights than a criminal suspect.
I would still say though that the earlier you can cut them off, run them away from you, the better. And when they do gain power over you it is still mostly based on what you have said, so the less said the better.
Once they have their hooks into you, I know that there could be costs to even saying nothing.
We still need to educate people to build political opposition to the mental health system, and also so that if faced with it, people will have the best chance of survival.
And this is all the more important now as CA Governor Gavin Newsom is targeting the homeless, a marginalized group which has already be devastated by the mental health system. Newsom wants to set up mental health courts in each county and to impose forced psychiatric procedures.
I think the best is just to educate people as to how there is never any good in the mental health system, and so you are always best in fighting it as you feel able.
We need to come to understand that this is a state of war. As I see it, it started with the social Darwinism of the 19th Century. It continued with the Nazi Party and its eugenics and philosophical doctrine, and it has been resurrected in the service of Neo-Liberal Capitalism.
So everyone is supposed to self-actualizing and getting on in the world. If they are not, then they need to submit to their crisis line counselor, their social worker, their therapist, or their minister. And if that is not enough, then there are drugs, and then things like ECT, TMS and Lobotomy.
And this does support war around the globe, just as the Nazi Holocaust and Eugenics programs supported war.
I am impressed Joanna with your clarity.
Joshua
Report comment
Joshua, thank you for your kind words, I really appreciate them! I agree with you – a psychiatric patient has less rights than a criminal suspect, though the situation can be better or worse depending on the state or country.
I fully agree with you that the earlier one cuts them off, the better! This is what I have done myself. I am now trying to get a disability pension because I don’t have any other form of regular income, but I will never agree to use psychiatric drugs.
What you say about the CA Governor is terrifying, just like any other attempts to force the “mentally ill” to take psychiatric drugs…
I think that there is some good in the mental health system – as an example, people may need a relatively safe place when they are having suicidal thoughts or when they are severely psychotic. Sometimes a psychiatric ward becomes such a place… My brother spent some time on a psychiatric ward because of suicidal thoughts. He did not have to take any drugs and was not diagnosed with a mental illness.
I definitely agree with you that there are obvious links between eugenics, including Nazi eugenics, and today’s mainstream attitudes towards the “mentally ill”, as well as people with intellectual disabilities.
I like the way you describe the current situation: “So everyone is supposed to self-actualizing and getting on in the world. If they are not, then they need to submit to their crisis line counselor, their social worker, their therapist, or their minister. And if that is not enough, then there are drugs, and then things like ECT, TMS and Lobotomy.”
I would add that in some countries like mine the “mentally ill” are expected to submit to psychiatrists, but are not protected from extreme poverty and hunger even if they do submit to them. The system does not care about them and its callousness is horrifying.
As the Polish scholar Stanislaw Kowalik rightly pointed out, the fact that vulnerable people find it increasingly difficult to obtain any help from the authorities actually constitutes a form of extermination.
Report comment
We should have Universal Basic Income, no needs test, everyone gets it.
Gaving went nuts with the COVID precautions and his daily press conferences. Back then I said, “He is trying to turn CA into a 40 million bed mental hospital with his grandstanding and gaslighting.”
There is no good in the Mental Health System. People need to develop their own emotional reserves.
If someone feels that they need to talk about something or need a safe place to chill out okay. But that is NOT the mental health system.
You don’t talk to psychiatrists, psychotherapists or social workers.
We need to develop other kinds of institutions or our own.
Thanks, Joanna and I wish you well.
Report comment
Joshua, I do like the idea of a Universal Basic Income. However, it is obvious that there are many people who don’t need such a guaranteed income. People who have well-paid jobs, people who own houses/apartments they can rent etc. don’t need such an income, unlike the poor.
I agree with you that people should develop their own emotional reserves, but it is difficult for many people. You say: “If someone feels that they need to talk about something or need a safe place to chill out okay. But that is NOT the mental health system.”
But unfortunately it can be very difficult or even impossible to find such a (relatively) safe place in our societies… Even if a person has loving family members, they are not always able to cope with the situation, especially if the person does not trust them.
A family member can’t stay awake for 24 hours in order to protect someone from a suicide attempt; and he or she is not always able to fully focus on the person who needs help.
As to finding someone to talk to, again it is not always easy. There are people who are isolated; there are people who don’t feel able to talk openly about their problems to family or friends.
Family members or friends can also give very bad advice to those who are suffering. Finally, they are often too busy with their own lives… I was able to help my brother during his crisis (during his stay in the mental hospital and after his release) only because I don’t have a job.
For all these reasons I don’t think that mainstream mental health institutions and professionals are completely unnecessary. In some cases they can literally save someone’s life…
Of course I agree with you that psychiatric survivors should develop their own institutions, but there are many obstacles, including the lack of funding and all kinds of internal disagreements.
I, too, wish you the best!
Report comment
We need to look for emancipation, and we need to teach emancipation, from the mental health system.
Joshua
Report comment
Joanna wrote:
“Universal Basic Income. However, it is obvious that there are many people who don’t need such a guaranteed income. ”
Joanna, the idea of Universal Basic Income is that there is no needs test. Everyone gets it, no need to apply. You get it whether you want it or not. This was originally Thomas Paine’s idea, which he called, Citizenship Pay.
This is very different from Guaranteed Minimum Income, as that is just an expanded welfare.
Once you have a needs test, then it becomes like welfare where the stigma is extremely high and our entire politics revolves around stigmatizing the recipients. If one person is getting a needs tested benefit, then the entire state of Arkansas goes ballistic.
To make this work I say that you need to have 3 other things. And then the net cost of this to public coffers is zero.
Andy Yang said it would cost annually $3.2T, but then you would redeem $1.4T by being able to eliminate other programs. But he was not talking about it necessarily enough money to live on.
I say that it does need to be enough money to live on, like say $2k per month. And so it would cost more like $8T annually, and you would redeem $1.4T.
The money recirculates. 1/2 of the money goes to those below median income. So what will they do with it? They will spend it. So long as it stays with people who spend it, it recirculates while taxes nibble away at it so that it is available for the next payment.
But the other 1/2 of the money goes to those above the median income. And they use it to further inflate the securities and real estate markets. And then wealthy people usually are so because they have tap roots which run deep into our socio-economic strata so that all money spent enriches them. And that is not the purpose of UBI, fattening the fat.
Making UBI payments expands the economy, keeps the money in circulation. If you want to be able to sustain this you have to have taxes to take back what gets used to inflate the securities and real estate markets. So you have to have progressive income tax, and likely a wealth tax too.
The time of highest economic growth in the US was in the Eisenhower-Kennedy era, when the top federal income tax rate was 90%.
Then Kennedy knocked it down to 70%. Then Reagan took it down to 40%. Then Trump took it down to 37%. Most of our social and economic ills come directly from the Reagan tax gut.
In the social democracy’s of Western Europe, it is more like 55% or 60%.
But we have much broader military commitments around the globe. So most people feel that going back to 70% would be right.
Now to make UBI work though you still have to take care of people’s other needs, the kind of things which usually cause them financial problems.
So we need to have a strong public housing offering. These would be towers built on the rail public transit lines. In Europe they call these Urban Transit Villages, 10 to 40 acres, and starting 6 stories down for the train station and parking.
These would rent at a board established fee, say it could be 1/2 the UBI benefit. This board established fee public housing takes the place of rent control. Rent control is very hard to enforce and it causes its own problems. So with public housing, which should be able to operate at a profit, we will drive the slum lords out of business.
Never make this public housing needs tested. Anyone can live there. If you have to ration it, then make it age tested, but never needs tested.
Building, operating, and maintaining these would be some of the best jobs around.
One question has always been, do you assume car ownership. I would say that at this point, if someone has UBI only long term, then they probably won’t want to own a car.
All services are in the lower floors, and these are not just for residents, they are for everyone.
Then we also need Medicare for All and Free College with College Debt Forgiveness.
Having these four things makes for a material paradise on earth.
And running our current Work Ethic Squirrel Cage costs our society vastly more. We have had a gross surplus productive capacity since the 1870’s. And the cost of this has been extreme deprivation and large scale war.
Most people will still want employment and other income, just to win the admiration of friends and family. The Work Ethic always was a capitalist over coding.
With UBI, more people will be able to have paying employment and profitable businesses than would otherwise.
Joshua
Report comment
Joanna, usually the idea that someone is mentally ill begins with family members.
https://www.amazon.com/Sanity-Madness-Family-Routledge-Classics/dp/113868774X/ref=sr_1_1?keywords=sanity+madness+and+the+family&qid=1649971509&sr=8-1
While someone may wish there were a safe person that they could talk to, this really never exists.
You talk to comrades, those fighting shoulder to shoulder with you in the struggle for justice.
Right now Ukrainians are fighting for their lives and for their country. Suppose they just said, “I need to talk to my therapist” or “I need to talk to my support line.”
And talking to these people is giving up critical information. Doing so will limit your range of future actions.
Joshua
Report comment
Joshua, yes, I know that there are such toxic family members – this is very sad.
You say that people should talk to “comrades” who are fighting for justice, but unfortunately only some people are lucky enough to have such “comrades” when they are going through a mental health crisis. Groups and networks of people critical of psychiatry exist only in some countries.
I did not know anyone with similar experiences when I was going through a psychotic episode and after my release from the mental hospital. I later joined an online community for people diagnosed with “schizophrenia”, but virtually everyone in this community believed that people with this diagnosis should be on neuroleptics. I was actually attacked by many members of this community because of my own approach…
Another problem is that only some psychiatric survivors are “comrades” able and ready to offer friendship and support to others. Today’s societies encourage people to see themselves as isolated individuals and unfortunately many survivors are not immune to this trend. Some currents of pop psychology encourage people to fully focus on themselves, their own emotions and needs while completely ignoring the emotions, needs and problems of others.
I have often noticed that psychiatric survivors can be very self-centered, convinced that their personal stories are completely unique and uninterested in other people’s lives and problems. In some cases I have seen a pattern where a person takes it for granted that as a psychiatric survivor s/he deserves others’ attention, compassion, time and energy, but is too self-centered to really notice other survivors. Such people can even get very callous and hostile towards other survivors – they clearly don’t see them as comrades.
There are also survivors who actually look down on people they see as “really” mentally ill. I remember a very ironic situation: when I said to a person that I had experienced hallucinations and delusions, she replied something condescending, implying that unlike her I was “really” mentally ill. The irony of the situation is that this person was the one who kept talking about how distressed and miserable she felt and who expected compassion from others…
It was obvious to me that this survivor had internalized the belief that anyone who has ever experienced hallucinations and delusions is mentally ill and that there is something shameful about being mentally ill. Yes, unfortunately many survivors do internalize the beliefs of the mainstream society on “mental illness”!
Report comment
I also know a person of privilege who had a hallucinatory experience, and was “diagnosed” as “bipolar” and discriminated against in their work and other settings for this label. It was interesting to note that this person claimed that they were “misdiagnosed” and were having a “spiritual awakening,” but continued to believe there were “real” bipolar people out there, only she wasn’t one of them. This person’s emphasis was on proving she was not “one of them” instead of identifying the labeling process itself as opening the door to very real and serious discrimination and abuse, which of course anyone labeled “bipolar” would likely experience, regardless of the reason for their label being attached. I understand why this happens, but I think it shows how hard it is to arrange a sense of “comradeship” when the entire process is so fraught with danger for anyone participating as a “client” or “patient.” When people are scared and isolated, they tend to search for a way to save themselves, and the plight of others may not occur to them until well after the incident, or in many cases, it may not occur to them at all.
Report comment
Steve, this is very true. Many distressed people focus on their own situation, on saving themselves and only themselves. Of course this is unsurprising…
Sadly, many people never stop saying that they are unlike the “really mentally ill” and cutting themselves off from them. As you said, they don’t see that the real problem is the labeling process.
It is not at all easy to create a sense of solidarity between psychiatric survivors, especially between those who are privileged in some sense (e.g. socioeconomically) and the others. People diagnosed with serious mental illnesses are disproportionately poor and I am sure that in the case of middle-class and upper-middle class people the desire to cut oneself off from the “really mentally ill” is partially linked to prejudice towards the poor.
Report comment
Joshua, regarding what you said about Ukrainians fighting for their lives and country: I am absolutely not saying that people can’t cope with their problems and emotions without a therapist or a support line!
I don’t personally have and have never had a therapist. I have coped with my problems and emotions in other ways. To be honest, I think that psychotherapy is hugely overrated and that many paid therapists cleverly exploit their clients and deliberately try to make the clients emotionally dependent on them.
However, people can go through situations with which they are unable to cope. Let’s not forget that many people do take their own lives… I do see it as a tragedy, unlike some psychiatric survivors.
Ukrainians who fight together for their country are in a completely different situation than people going through a mental health crisis. An individual going through a mental health crisis often feels painfully, terrifyingly alone and rejected by other people. When people are together experiencing the same situation at the same time, they can and often do support each other.
Finally, when a person is severely psychotic, simply talking to friendly people is not enough. I did talk to a few friendly people during my psychotic episode, but my hallucinations and delusions did not stop.
A severe psychotic episode is a radically different experience from e.g. a bout of depression. The mind functions in a different way during such episodes – e.g. harmless things may seem terrifying, a person may strongly believe the most horrifying things without even a shred of evidence etc. This type of psychosis is a very difficult experience and may even be traumatizing.
Report comment
Joanna, so long as we have people who defend the existence of the mental health system, then we will still have it and more people will be fed into it.
Joshua
Report comment
Joshua, a mental health system does not have to mean forced drugging, stigmatizing diagnoses etc.
As I have been saying in my earlier comments, there are many people who are not lucky enough to have a well-functioning support network. There are many people who are isolated, who don’t have real friends or who find it difficult to talk about their problems to their friends or family members.
It would be wonderful to live in a world where everyone going through a mental health crisis has loyal friends and comrades who can always offer him/her support. Unfortunately we don’t live in such a world… This is one of the main reasons why mental health issues are now so frequent.
When my brother suddenly started having suicidal thoughts, me and my other family members did not even know about it. In fact, pople can hide their most painful problems from those who can offer them support.
There are also situations when talking to someone friendly is not enough for a person going through a serious mental health crisis – a severe psychotic episode is a very good example of such a situation.
Report comment
Joanna, there is no such thing as a “Mental Health Crisis” because there is no such thing as “Mental Illness”.
People can though be pushed to the breaking point, they can loose it. I guess the worse is a nervous breakdown. But this is still not a “Mental Health Crisis” or “Mental Illness”.
The party will need to pull back from those things and people that are pushing them over the limit. And they need to do this before they do anything destructive. And then likely they will need to make some major life changes. Often these changes will be in the areas of marriage and career, but there are other things too.
They might want to talk to someone, but the safety of this is always dubious. The best is if they can learn to fight back. And you gain comrades by the way you conduct yourself in the stresses and injustices which you are already facing. No one is worth of being called a comrade when they are submitting to abusers. And of course what the abusers want is for you to end up in the mental health system, and to believe that the therapists are your allies. And the abusers want you to believe that your own pain is your own fault.
Joshua
Report comment
Thank you everyone for the comments. Much time and thought has been put into your comments. I don’t know where to start.
There is always a possibility of “solidarity” among psychiatric survivors. Evidently, from what you write this possibility has limits. Nonetheless it exists. The common cause you have found in your comments is a case in point.
As to the comments on pharmacotherapy, I am told by doctors that my bipolar II causes me to be an imposition on others. The cure for this, they tell me, is more neuroleptics. And of course the solution to world peace, for these doctors, it would seem to me, is also neuroleptics.
It is well known that psychoactive drugs are overprescribed and that diagnoses are so broad today that almost anyone can be diagnosed with suffering from some form of mental illness. But what are the prolonged effects of all these drugs? At the best they cause metabolic syndrome. At the worst, people can endure years of akathisia and other substance induced horrors.
The cost and benefit of pharmacological treatment is often decided not by the individual but by the courts. We are told that the evidence must be overwhelming to compel a court order for forcible injection but often such rulings are based on little more than opinion. The defendant has broken no law. There are no victims. It is his “potential” that is in litigation. It is as if you find yourself before a parole board but have committed no crime. If psychiatry is evidence based, there is little to support the contention that such hearings protect anyone. And the costs to those who bear the brunt of such judicial discretion can be incalculable.
All the comments — even with their differences — suggest to me a kind of solidarity and give me the hope that psychiatric survivors can find a sympathetic ear. I have found that in your comments and it is appreciated.
My earlier replies were incomplete insofar as I did not say that it is possible obviously to file a complaint against a physician with his deontological society. That is one more route that is open to psychiatric survivors.
Report comment
Call for personal stories-
Hi Phil,
I am a blogger writing from personal experiences in the psychiatric world. I love your story. I have been on psychiatric drugs for 30 years. I have attempted to stop them in the past and experienced withdrawal. The last time, was very bad and I checked myself into the locked psychiatric floors of my local hospital. I stayed for 5 days and was released to my family with an appointment for electroconvulsive therapy and more meds than I went in taking.
You can read my entire personal story on Mad in America’s website and listen to it on Courageously You podcast with Tara Bixby.
Today I am looking for writers to guest blog for my initiative, Stories of Psychiatric Drug Users, with a focus on side effects and withdrawal symptoms.
I am openly inviting black, indigenous, people of color, lesbian, gay, bi-sexual, transgender, and queer individuals to share their voices.
Please contact me at http://www.lifewithantidepressants.com if you would like to contribute. Thank you
Report comment
Joanna wrote:
”
… a mental health system does not have to mean forced drugging, stigmatizing diagnoses etc.
As I have been saying in my earlier comments, there are many people who are not lucky enough to have a well-functioning support network. There are many people who are isolated, who don’t have real friends or who find it difficult to talk about their problems to their friends or family members.
It would be wonderful to live in a world where everyone going through a mental health crisis has loyal friends and comrades who can always offer him/her support. Unfortunately we don’t live in such a world… This is one of the main reasons why mental health issues are now so frequent.
When my brother suddenly started having suicidal thoughts, me and my other family members did not even know about it. In fact, pople can hide their most painful problems from those who can offer them support.
There are also situations when talking to someone friendly is not enough for a person going through a serious mental health crisis – a severe psychotic episode is a very good example of such a situation.
”
Joanna,
Of course the mental health system does not have to mean forced drugging, but it is always predicated on the idea that the reason for one’s suffering is to be found within themselves. So if a person is angered because they are being kept in a state of slavery, they might see a therapist. And that therapist will help them to recuperate from their displeasure about being kept in a state of slavery.
If we go along with this, then there will always be drugging, and the threat of forced drugging, and the threats of ECT, TMS, and Lobotomy for the more extreme cases.
Most of the time the idea that someone is “Mentally Ill” starts within the family. And usually our friends and acquaintances are not adventurous people who would be able to offer any kind of support if we were to find it necessary to challenge what is usually taken forgranted.
There is no such thing as a Mental Health Crisis because there is no such thing as Mental Illness.
It is true that people can find themselves in emotional overload and can say and do strange things. I guess the worst is a nervous breakdown. But this is still not a crisis in Mental Health. Mental Illness is a myth.
One might have various thoughts. But they need to develop their own emotional resources to handle them.
But having strange thoughts does not mean that one is having “problems” or a “mental health crisis” or that they are “mentally ill”.
It does not mean that they should be in a psychiatric hospital ward. Those kinds of hospitals should not exist.
People may need time out, or a safe place to disconnect from things and from people that are causing stress for them. But the mental health system is not at all such a safe place.
Joshua
Report comment
regsiteredforthissite, the “kindness” shown vulnerable people by psychiatrists that you speak of is of a very particular kind. Someone in need, someone who is vulnerable, can mistake the “interest” shown by a clinician as genuine, sincere, authentic. But it is often a ruse, a means to an end. It is only when you obtain your medical records and read a psychiatrist’s observations that you can fully appreciate the character of that interest.
For someone who is isolated, the interest of a clinician in their thoughts on something, their feelings about something that compels and preoccupies them, can be welcome. It can even be felt as a kind of validation or vindication. This was once known in more innocent times as the “talking cure.” But now it is often just the prelude to the invocation of the evaluative authority of the clinician. What is said in the context of an assumedly private medical appointment becomes grounds in a court record — grounds for an invasive procedure and forced drugging.
The transference a patient experiences in his relationship with a physician is very real. It is well known that stomach ailments can return after the patient no longer sees their gastroenterologist. An astute psychiatrist exploits this transference. The patient that does not understand the implications of this for him — the legal contingencies that devolve from this “therapeutic” relationship — labours under a delusion.
Report comment
Yeah, I know all this.
Report comment
regsiteredforthissite, I learned it the hard way
Report comment
Unfortunately, we all do, and for many it’s too late by the time they do.
Report comment
That is why, if you notice my original comment, I used the word “kindness” in quotes. Unfortunately, I think writing on this place is making little difference in the real world. I doubt even 1% of mental health workers read this place. Most disgusting practices which are taking place under the guise of mental health treatment continue to happen. The least they could do is at least be honest about it. It doesn’t take much for them to say: “yes, our psychiatric categorisations can damage your life”, “yes, our drugs can make you worse than you were or be as bad as your original issues”, “yes, our profession is often used by people with less than good intentions to gaslight people”, “yes, it is wrong of us to say that a lot of the issues that our chosen profession deals with are not like cancer or diabetes which have nothing to do with your character, conduct or sanity”, “yes, there are simpler and better solutions where we could do things which are more tangible: like provide financial assistance etc. to people than simply turn them into psychiatric patients”.
Even that’s not happening. A large chunk of patients are no better either. They treat them like gods at their own peril, not even realising what’s happening to them. Their problems make them weak, and their need to rely on the mental health system makes them doubly weak. The latter applies (or has applied) to us as well.
We are failures too. We have criticised the mental health system but we haven’t been able to find a solution for people who suffer from problems (without which no one will believe us). A psychiatrist with a prescription pad or a psychologist, no matter how wrong he is in his approach, has, on an average, more power and value than us. It is my dream in life, first to get better myself, and then to at least help just one person escape this mess. To provide someone the real world help I did not have, and the knowledge I gained too late. Whether I will ever be able to accomplish this is a different matter. But I don’t want this desire to take me down the rabbit hole of becoming a psychologist or a token peer worker in some mental health institution like so many before me.
Report comment
Correction: “it is wrong of us to say that a lot of the issues we deal with are* like cancer or diabetes, which have nothing to do with your character, conduct or sanity”
Report comment
registeredforthissite, you say that we are “failures” because we “haven’t been able to find a solution for people who suffer from problems” and because a psychiatrist or psychologist has “more power and value than us”.
I find this extremely unfair. I believe that people who suffer don’t have to take psychiatric drugs and this is what I have always said to other people. I was often attacked or simply ignored.
Let me add that I personally NEVER saw psychiatrists as gods. I never wanted any psychiatric “treatment”, I was involuntarily committed and forcibly drugged.
Why do you think that a psychiatric survivor who is unable to convince other people to stop believing in psychiatry should feel like a failure?
People who have a lot of power in a cruel, inhuman and grotesque system are not in any sense better than people who have much less power in this system. I am also wondering what makes you say that psychiatrists or psychologists have more “value” than psychiatric survivors…
Psychiatrists and psychologists are usually much more respected than psychiatric survivors because of the nature of the world we live in, a world which stigmatizes and humiliates psychiatric survivors and which highly values people with medical degrees and well-paid jobs.
Why should we feel like failures only because we are unable to change the minds of millions of brainwashed people who believe in psychiatry? We can change our own lives and – if we are lucky – the lives of some other people.
Every person who bravely resists a cruel system is not a “failure”, no matter how poor and isolated this person is.
Report comment
Bradford, sorry about your friend. I didn’t know the meaning of gas-lighting until it was done to me. Incredibly, it was systemic and I encountered it everywhere. It took over my waking life. I was continually told that what I was living was not real and that I had imagined it all. Everyone from the orderlies to the doctors took part in this. You have to live it to believe it. I was completely isolated. I am only beginning to be able to talk about it now. Thank you for your comment. There is solace in knowing that you are not alone. Again, I am so sorry for your loss.
Report comment
Sorry, but it is a FACT that psychiatry is a fraudulent pseudoscience. Prove me wrong? You can’t…..
Report comment
Glad you’re out of that horrible place. Have been to placed like that myself. They’re not places of healing, but abuse, invasion, and violation.
Report comment
Kayla, thanks for the feedback. I invite you to read my blog on Mad in the UK (Medical Gaslighting of Patients with Akathisia, published September 6, 2022). It continues my account of my hospital stay and court hearing.
Report comment