
Lots of funders are now doing initiatives to address health disparities. This is based on the idea that our people die 25 years younger than people without the label of so-called “serious mental illness.” But once again we have found that a project designated to help our community has gone astray without even bothering to ask our community what we need. What is a health disparity? And why does the Recovery Movement need to be included? (Or whatever we should call our community?)
I’m sure you’ve heard about the 25 year lower life expectancy already. It’s solid data, and old, from 2006. But have you ever actually read this report? It’s the National Association of State Mental Health Program Directors’ Morbidity and Mortality Report. Click the link and read it. It’s actually GOOD NEWS. It has quite a bit of good info about wellness stuff. But it also shows that small changes in wellness activities lead to big reductions in risk. Like losing 10 pounds cuts heart disease risk in half. Exercising 5 minutes a day. Cutting smoking down by 30%. People get overwhelmed at the distance from where they are to where health is perceived to be, and they don’t know that these small changes can help a lot. So this is good news.
These days there are many communities that die earlier. People in certain low income zip codes, usually the urban core, can die 12-15 years earlier than their counterparts in the suburbs. Black people, Asians, Native Americans and Latino/as have lower life expectancies. So do LGBTQ people. But those disparities are all in the 5-12 year range, not the 25 years lower that our people have. So when the Kansas Health Foundation came along with some money to work on this, we were excited!
Poetry for Personal Power has emerged as a stronger and stronger force in the last few years. We are now working in four states and we have gotten to the table more often. We are a statewide behavioral health advocacy network and peer support provider. While we started in Missouri, Kansas has been more cooperative in general because of our exposure through a fellowship program there. This time we were at the table with eight other mental health organizations as the Kansas Health Foundation grant was written. Our choice was to go in as a lead applicant or to go in as a subcontractor to someone else. We went is as a subcontractor because the funder was emphasizing “advocacy field mapping,” and we knew we hadn’t been included in that process. In other words, we knew there were pre-picked winners and it wasn’t us. We are learning that more and more funders have pre-picked winners.
So Poetry for Personal Power helped NAMI-KS write their application to this process. At that point we were collaborating with more mainstream mental health groups because the recovery movement networks in Kansas were fixated on drop-in centers and working in a closed silo, whereas the mainstream groups were more up to date, innovative, and collaborative. NAMI Kansas had invited Bob Whitaker to speak at their annual conference, and they had shown the Healing Voices movie and done a medication tapering workshop. Some of their board members were “medical-harm aware,” and they showed an interest in improving the harm/benefit ratio being delivered by their organization. We hoped that they could make progress.
NAMI Kansas and Health Disparity Ideas:
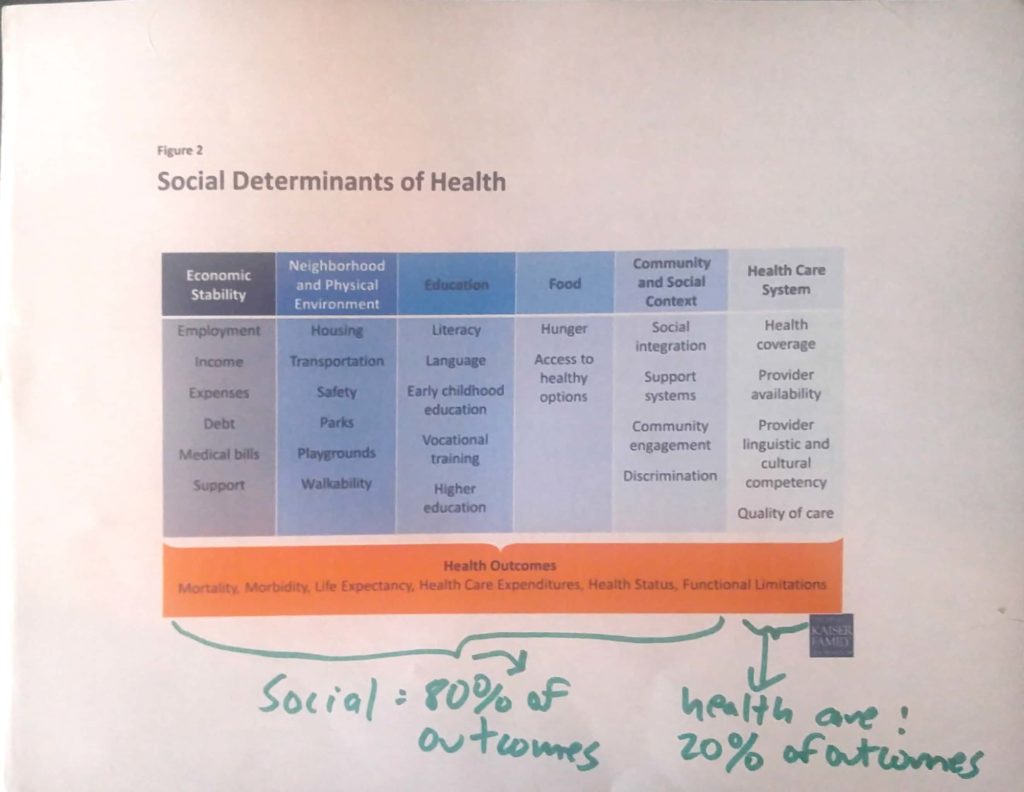
Do you understand basic concepts of health disparity? A lot of research shows that the quality of health care and people’s ability to access health care only affects 20% of health outcomes. Life expectancy is a health outcome. But the quality of the mental health system only affects 20% of life expectancy issues. The rest of it needs to be addressed at a social level:
In the grant narrative, we wrote in the imperative to address the harms being done by NAMI Kansas in order to address health disparity:
Although direct care issues and access to care are very important, there is also much more to the issue of health care outcomes. The health care system is only the tip of the iceberg for health disparities. NAMI Kansas and the Kansas Mental Health Coalition has been able to work with other grassroots advocates that bring a long history of information about social determinants to the project. This is the Recovery Movement, or mental health civil rights movement, or self-advocates and patient advocates for people who have recovered from mental health concerns.
We went on to explain a lot more: The Recovery Movement (or whatever you call our community these days) brings a passionately different perspective to the table. Their view is equally science based. Including both the Recovery Movement views and the traditional NAMI views allows this project to dig deeply into health disparities and social determinants.
-
While disease model advocates talk about the cost of “untreated mental illness,” recovery movement advocates also talk about the cost of “treated mental illness.” Medicalization of normal emotions costs the US over $35 billion annually (Social Science and Medicine, 2010: 70, 1943). De-medicalizing help-seeking for mental health concerns addresses the two largest causes of stigma (J Psychiatry Neurosci, 2015) and the three biggest barriers to help seeking (Clement et al, Psychological Sciences, 2014).
-
While many disease model advocates talk about the need for “supporting the disabled,” recovery movement advocates say that psychiatric disability does not have to happen. Helping people avoid psychiatric disability would save an average Medicaid cost of $20,000 per year per person, a total of $307 million dollars annually in the KC Metro area alone. (KDADS presentation data 2011). These Medicaid costs don’t even include the lifetime of disability payments or the lost wages and lost creative input to our society.
-
While many disease model advocates talk about getting people in treatment, Recovery Movement Advocates talk about getting people into their community where people spend their time, through the people with whom they interact, doing the things they enjoy doing (Prevention Institute “Making Connections” 2014).
We wrote this into the grant narrative:
This project gives NAMI the chance to learn from and co-operate with other perspectives that challenge some of the basic assumptions held by NAMI organization’s leaders.
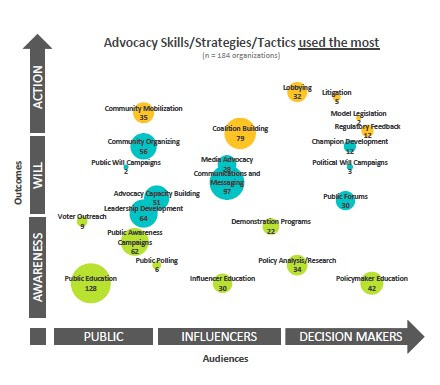
NAMI’s advocacy has focused historically on health access and the health care system; in other words, only the right-hand side of the box that affects 20% of health disparities. However, Recovery Movement advocates have focused much more heavily on social determinants like oppression, poverty, trauma, lack of education, low rates of entrepreneurship, and employment discrimination.
Remember, health access = 20% of health care outcomes. And social stuff affects 80% of health care outcomes. So “building better access to care” only affects 20% of the problem.
Also remember, there is a huge amount of data showing that the 25 year lower life expectancy is CAUSED by psych drugs. It’s caused by the loss of hope when people tell you that you might be disabled for life. It’s caused by the weight gain and the sluggishness of psych drugs. It’s caused by discrimination in the physical health care system against people with mental health labels.
Much of our community’s health disparity is caused by the very things NAMI chapters are promoting — psych drugs and psych labeling.
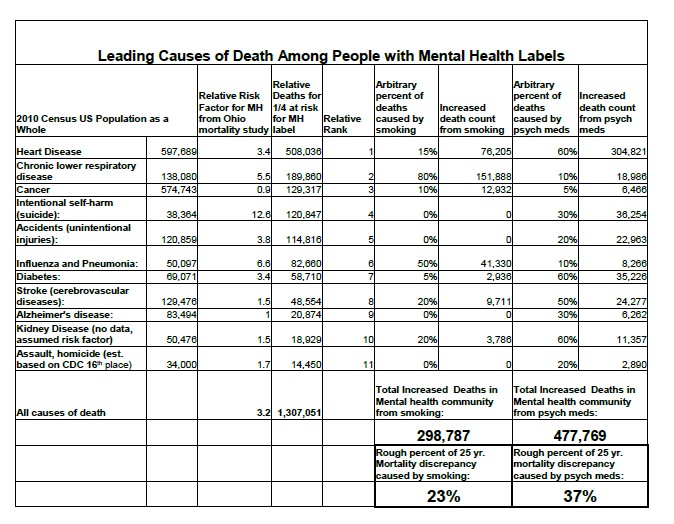
People have been doing research on social determinants for a long time. Here’s a breakdown I made to compare the impact of smoking (which many funders will address) versus the impact of psych drugs and the disease model (which few funders will address). The source for this data is explained in each column: coming from the Ohio mortality study referenced in the NASMHPD morbidity and mortality report. For the heart attack data, you can see more detailed calculations on my previous MIA Carrie Fisher blog post.
So how did our project go astray in Kansas? First of all, NAMI Kansas cut the above portion out of the final grant narrative. They just said, “Poetry for Pesonal Power is nontraditional.” They took out any text that committed them to learning to move beyond the disease model. Then they wrote the grant budget vastly different than we had requested. Their CEO makes $66,000 a year according to their 2015 990 form. Their project director for this grant was budgeted for $45,000 a year. But they budgeted zero dollars to pay advocates for their time even though many of us live in poverty and/or freelance for a living.
The next huge problem was that NAMI Kansas hired a person as “communication director” that didn’t even know how to run social media. Like, he didn’t even have any personal accounts, let alone any experience managing business accounts. Or developing websites or managing databases or running HTML email sending services or anything else demanded by this project.
Then NAMI Kansas stopped making decisions on the project. We kept offering suggestions that got ignored. The Kansas Mental Health Coalition got ignored. It became clear that the project director wasn’t even working on the project that much. We had a final conversation where it became clear that their project director had no understanding at all of health disparity. And knew nothing about the Recovery Movement or the “medical harm aware” information explained above. We tried to inform him of this information and he accused our advocates of being “mean” for expecting him to know something about this information. NAMI voted to cut Poetry for Personal Power out of the grant, we appealed to the funder, and the funder didn’t want to hear anything at all from us.
Their excuse was, “Well, the first year was only capacity building.”
And we said, “You can’t build capacity to solve health disparity without looking at the problem.”
But then their second year plan didn’t even mention health disparity once either, so they’ll have to come up with a new excuse for that.
And, to take some blame myself, I got really really angry at seeing this project get so sidetracked. I got really offended that after all the education work I have done with NAMI Kansas, to help them update their science, it was simply dismissed as “snipping and criticism.” I am very sad to think of all the people that could recover from “mental illness” or completely avoid “mental illness” who now don’t get access to this information. I’m reading a book on conflict and I went nuclear too fast because this stuff really matters to me. Next time I will be better about explaining expectations, setting up boundaries, and outlining processes for resolving conflict.
But this hurts. When people are dying 25 years younger, I know names, faces. Eddie Taylor, he came with me last time I needed help. Les Luthie, he gave me a ride home when I stranded myself in Wichita after Al Henning died by suicide. Then Kevin Kenny, he helped me out the night I went to jail. Helen De Witt, she invited me to her apartment one time. This is NOT ABSTRACT TO ME. I have been to too many funerals.
So now what? If you care about health disparity? If you actually want to work on why people with mental health issues die 25 years younger? If you actually want to listen to grassroots advocates? And funders keep ignoring our community’s needs?
How grassroots advocates CAN work on health disparity:
1. You can make a donation to Poetry for Personal Power. Just use the PayPal button on the right-hand side of our website http://poetryforpersonalpower.com/.
2. Join our launch of the Recovery Movement Health Equity Facebook Group.
3. You can promote the Making Connections for Men’s Mental Health white paper, it’s one of the best documents on mental illness prevention. Many physical health prevention projects exclude mental health because they believe it’s not preventable — this report counters that argument somewhat.
4. You can keep advocating for resilience, prevention, wellness, and social approaches to mental health. Eric Maisel interviewed 100 of these interventions here and you can read through their program descriptions.
5. You can ask funders to observe best practices or better approaches to making funding decisions. For one thing, STOP requiring mandatory coalitions — it chokes out grassroots advocates. Share these 10 problems and 10 solutions for behavioral health funding.
6. Keep doing legislative advocacy. States are always passing laws that help or hurt our people. Sometimes getting the right foot in the right door will make a difference.
7. Keep on trucking. First they ignore you, then they mock you, then they fight you, then you win. We lost this battle, but we are gonna come back and win the war. We will.














In my view you need a forum on here with free detailed knowledge about how to withdrawal from every class of psychiatric drug and those of us who have been through it – hopefully – prepared to offer online support, especially to those who are doing it alone or have no friend or family support, because it can be very scary, horrific, and requires an hell of a lot of fortitude and determination. Oh and by the way, I never met a GP or psychiatrist who helped.
Report comment
Thank you for the link to the 2006 research paper.
The titel and intro intriged me, yet I could not read so many pages to know who got that grant and why mental-groups didn’t.
So thank you for the link to the 2006 research
Report comment
I disagree, and I agree with what you have to say here.
The news is not so good as you would suggest. In fact, it’s still pretty dismal and grim.
I feel the 2006 report missed the point of the matter by focusing on health disparities, exercise, and diet rather than on the real problem behind this early mortality, neuroleptic drugs, specifically atypical neuroleptics. Atypicals were developed to help reduce some of the effects of the phenothiazines, most dramatically Tardive Dyskinesia. Problem is, there are metabolic changes associated with the atypicals connected with all sorts of physical conditions, any one of which can kill. People were dying earlier on phenothiazines to begin with, the development of atypicals increased this average premature mortality by 10 to 15 years. Deal with that, and these “seize control of the mind” drugs are no longer shortening lifespans. Lifestyle changes, ending smoking, exercise, and improved diet, all these would come with a diminishing of drug use. It is the over reliance on these drugs that is killing people, and any of the other health changes recommended are mainly cosmetic, a smokescreen for the industry, and a cover up of the mass maiming and murder of people that is taking place in the mental health system.
I agree in the sense that it makes no sense to spend money to disable people when you can spend money to enable them. The idea is that maybe some of these people don’t have to spend their entire lives dependent on others financially for their subsistence and survival. Much money is spent managing people on disability that could be put to better use getting them back on their feet and out of the system, integrated into society at large, with jobs and functional existences. What a waste of cash! It’s an absurd system that encourages this, and it is a system that needs to change.
Report comment
Thank you Frank. I could not agree more. Thanks also Corinna for your work and for reminding us once again about the deeply upsetting health disparities among those people who are labelled with a psychiatric diagnoses and given neuroleptics. I hope we can continue to help educate people about all the things that help people move through emotional distress, how medical model treatments cause/add to the problems and how individuals can take control of their lives beyond the medical model system.
Report comment
The graphic comparing smoking and psych drugs is a great resource! Thanks for sharing this perspective – I admire your persistence in trying to work with NAMI and other groups still invested in the medical/blame the victim model.
Report comment
There are, apparently, 35 billion reasons why the system refuses to change one iota. The people distributing the wealth from “mentally ill” people aren’t willing to let go of a dime and actually seek to increase that 35b by any means that they can. Their greed and lack of concern for the human species is appalling. If that 35 billion were used to feed, clothe and house people, strengthen communities, etc., those atop of the current “pot o’gold) would lose not only their wealth but the power that comes with it. The system operates from a twisted base where truly preventing outcomes is seen as something to be avoided. The only way to fight this is to quit being good consumers. Quit literally buying into a system that is already too powerful and uses their control to kill people. Help the people in your community however you can. Let people know that “seeking professional help” has hidden consequences. Change yourself and educate yourself so when the moment presents itself (and it will) you can tell people you opinion and back it with facts (Psyche drugs kill and this is why/how). People will get tired of being sick and tired. The facade of “mental health” complex is beginning to face some challenges. Keep the pressure up! Don’t give up!
Report comment
I agree Squash. Oldhead disagreed with my own soundbite “Psych drugs do not work!” Yet that soundbite impelled me to go outside the system to find out what my real problems were and escape the MI ghetto. A lot of people would respond well to this soundbite. For years I didn’t know there was an organized group of people against psychiatry. Just NAMI and “crazies” who wouldn’t take their “meds” because they thought the little purple elephants they saw everywhere were real. Thank God for the Internet. Without it, I might still be a Grateful Consumer, despite the overwhelming evidence that psych drugs make people crazy, keep them from recovering from psychosis and depression, and damage them in every way possible.
This is not to minimize other issues Julie Greene and others point out. But if you keep taking mind altering drugs it’s hard to think straight to take care of the other crap that keeps happening.
Report comment