
Part three of a talk on the history of psychopharmacology given to the British Neuropsychiatric Association on February 22. It follows on from Tweeting While Psychiatry Burns and Tweeting While Medicine Burns. The final group of slides are here.
This talk was first given in Toronto on November 30, 2000 to mark the 75th anniversary of the University Dept and the 150th anniversary of the Queen Street Mental Hospital (slide 1). The Chads were still hanging in Florida while the Supreme Court tried to decide whether Bush or Gore had won. I had recently been hired by the University of Toronto, and I and a number of others had been invited to contribute to a meeting to celebrate the occasions.
I led off the program with the talk pretty much as it’s been presented here. One of the other speakers was this dude Charles Nemeroff. Nemeroff was quite happy at this point in time to be featured as the “Boss of Bosses” (slide 2). He wasn’t the boss of bosses because of any scientific or clinical contribution, of which there was none.
In line with these Mafia connotations, at the meeting Nemeroff approached one of the key people involved in my hiring and suggested that they “get rid of Healy.” According to Nemeroff later, this individual wet his pants. The University later claimed that my colleagues were disturbed by my talk and would have found it difficult to work with me. They also claimed I had said “antidepressants cause suicide” which was like crying “fire” in a crowded theater.
The talk was actually about lack of access to data, not about antidepressants and suicide. It was the plot of a book then in press: The Creation of Psychopharmacology (slide 3). Harvard University Press don’t do wild or off the wall.
My talk received the highest rating of the day by the audience, which seems at odds with later university claims. Nemeroff received the lowest (slide 4). His talk was largely an advert for paroxetine (Paxil/Seroxat) and how it was more of an SNRI than people thought, which didn’t seem particularly appropriate for the occasion, but perhaps interesting in that he seemed to be thinking about being an expert for GSK in the forthcoming Tobin trial.
Escape to New York
Nemeroff flew to New York that Thursday night. The following morning, Friday, at a Suicide Prevention meeting he told colleagues that Healy had lost his job.
Unaware of any of this, I flew to New York on Friday morning and that afternoon was a few blocks away from Nemeroff. Neither he nor I knew this. I was in Pfizer’s archives where even the loo paper was marked confidential. Articles that had been in the public domain for years were stamped confidential. But extraordinarily, this document wasn’t (slide 5).
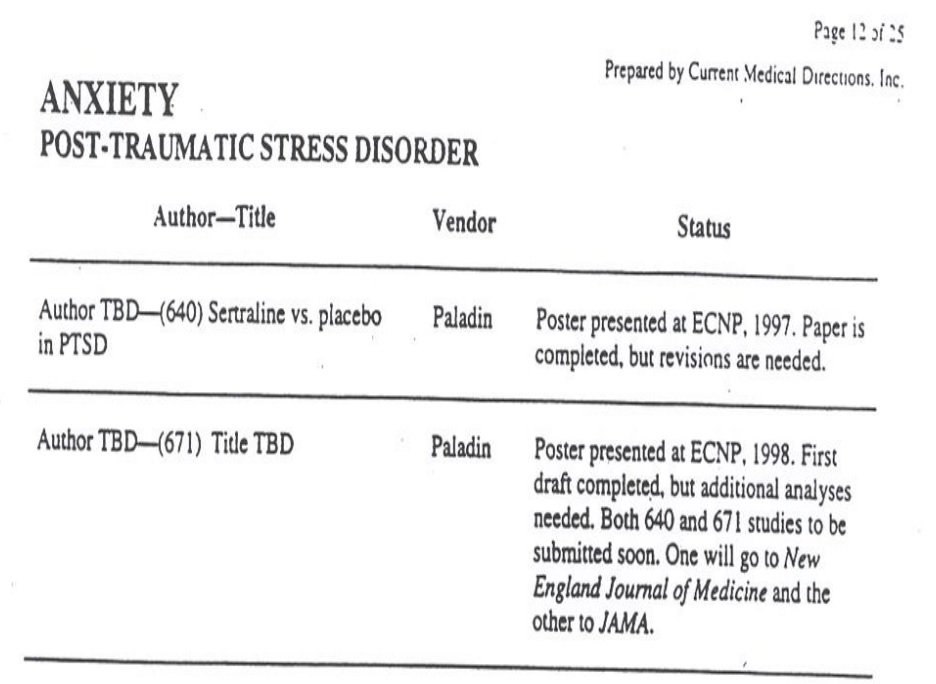
This page comes from a portfolio of articles on Pfizer’s Zoloft, covering the writing of articles on Zoloft for ingrown toenails, for anxiety, for the elderly, for the young, and how it was cheaper than older treatments that cost only a fraction of its price. This page shows you that there were two articles on PTSD being ghostwritten for leading journals. The articles were written, the journals selected — the company just had to decide on who the authors were going to be. TBD stands for To Be Determined.
Based on this portfolio of articles, we were later able to show that heading toward 100% of articles in the peer-reviewed literature on on-patent drugs are ghostwritten. In 100% of cases there is lack of access to the data. This is true across medicine. It applies to respiratory medicine, neurology and cardiac medicine as much as to psychiatry.
What it means is that, for instance, the NICE guidelines — which are based on these articles — are junk. Complete and utter junk. But increasingly our trainees and everyone else are trapped by guidelines like these. We will lose our jobs if we don’t adhere to them. This is what has led to the opioid epidemic in the US.
Tweeting
A few days after I gave this talk, I was informed that I had lost my job — I wasn’t a good fit and the department would lose money.
Over the last sixteen years, when visiting the US I have been struck by what can only be called a Medical McCarthyism. Everyone in healthcare is scared to open their mouths. While the average American is probably still more prepared to stand up for themselves than the average European, when it comes to doctors it feels at times like the land of the craven and the home of the slave. Just last week, however, the President of Royal College of Surgeons in Britain made a case that medicine in Britain is heading exactly the same way.
Pretty soon after this talk, the worry has to be that most of us in the US, UK and Europe are going to lose our jobs — at least, going to lose the kind of jobs many of us thought we were taking up when we entered the field.
If the drugs are as effective as we are told and as free from side effects as we are told, you can replace high-cost prescribers with nurses, pharmacists, and pretty soon with robots. This is in fact happening quite rapidly.
In the 16 years from 1952 to 1968, the world changed in astonishing ways. In the 16 years since I first gave this talk, it seems to have changed almost as much again.
So when some future historian, a very few years from now, looks back at this period and wonders about the senior figures in the field — the Jean Delays (slide 6), in the UK they will have Sir before their name — will they say it was a time when the field’s significant figures tweeted while psychiatry burned?














Great article David; thanks for your honesty.
Report comment
Berserkers are apparently at the gates of the psychiatry empire. “Anybody got a flammable substance, and a match?” You can tweet to your heart’s content, but some downfalls are sweet. Unfortunately, I don’t see it coming yet, however, perhaps, eventually. 20 % of the population can bring down a much smaller figure, and through doing so, facilitate their own liberation (as well as improved health). You mention a medical McCarthyism, but psychiatry isn’t medicine. At least, it can’t prove that it is medicine. Generally speaking, it’s injury. 400 years of confinement are too many. There are a lot of dupes out there, aren’t there? Maybe it’s about time we woke them up. Yeah, that’s right. Burn, baby, burn!
Report comment
David,
It would be interesting to know what experience/s turned you against excessive pharmacology and made you so different from many of your peers. Any comments?
At any rate, keep up the good work!
Best regards,
Mary Newton
Report comment
I expect for David, as for me (another psychiatrist exceedingly cautious regarding medication excess and deeply interested in the state of the “evidence” and how drugs actually work) – the answer is something along the lines of being an old-fashioned doctor, more concerned with the patients i’m helping than with my wallet, and taking informed consent and ‘first do no harm’ seriously. David’s generally too busy to respond to post threads, but would consider himself scientifically and medically conservative- and the present state of the field anything but. Warm wishes, rob purssey http://www.mindfulpsychiatry.com.au
Report comment
Not sure about the “first do no harm” aspect. Healy promotes and administers ECT which is Craniocerebral trauma and ALWAYS causes harm/brain damage.
Report comment
The field of medicine is the third largest killer of Americans today, if I remember correctly. It’s not just psychiatry that is out of control, although psychiatry is probably the worst specialty where it comes to an unholy marriage with drug companies. Medicine in general has gone over the edge with a drug for this and a drug for that. I believe that this should make us stop and do some thinking about what is going on. Everything is a disease today, at least according to the drug companies. The drug companies are doing their best to convince doctors that their main objective is to prescribe, prescribe, prescribe……Dry eyes is now a disease! Television constantly advertises “medicines” for everything; while watching the early news this morning I counted six commercials for drugs that dealt with everything from psoriasis to dry eyes to congestive heart failure to constipation due to opioids to leaky bladder to copd to allergies to asthma.
Report comment
I doubt all the deaths caused by prescribed drugs are counted. The current generation of elderly people experiences more death from falls than any other, and they are also elderly at a time when rates of prescribing falls-causeimg drugs like statins and beta-blockers have done nothing but rise for many years–at their peak now. So does a person die of a fall/head injury, or because a drug that causes hypotension and syncope caused her to fall?
If only the drugs were prescribed for actual illnesses. The bulk of the drugs taken by old people these days are meant to prevent things, or deal with the side effects of other drugs, not cure or limit genuine organic health problems.
The newest data show that lifespan has decreased for Americans, for the first time in many years. If you know any old people and know what drugs they’re on, you’ll know why,
Report comment
Great points and all too true. I worked in a large nursing home/retirement center and saw this happen all the time.
I am older and it’s a constant battle with my doctor about things that she wants to put me on, like statins. I actually fired one doctor because he told me point blank to my face that I would absolutely take the statins that he prescribed! When I said that I would not take them he actually told me that I had no choice in the matter and at that point I pointed to my feet and said, “Oh yes I do! Watch this!” I then got up, walked out of the exam room and out of his office. I refused to pay the bill for the visit where I was verbally abused by the doctor!
Report comment
eek – at least in the UK Dr’s are free – at the moment
Report comment
Good for you! I also informed my doctor that I would not take statins as well as some other “preventive” meds. he wanted to put me on based on so-called guidelines (influenced by big pharma. I’m sure) I think I had an edge on you, however, because I was a former R.N. before becoming an attorney. I am 73 and take only one med. for mild COPD (Yes, I’m a smoker). I was almost killed by psychiatrists at a time when I was suffering a severe situational depression. I had nowhere else to turn, no resources, no support network, and was desperate. I stupidly bought into their claptrap and was on numerous SSRIs for almost 8 years believing them when they said I needed them. I eventually realized that being a zombie was not living and weaned myself off. At that point, my recovery started. I have had a wonderful life since then, but my former psyche. diagnosis is still in my record and causes me problems.
Report comment
Yes but there is a important historical caveat here. Dry eyes is actually a dumbed down terminology for Syogern’s Syndrome sp? It is related to the immune system and immflamuation
. It has a high cluster for females. The term has been used for decades and was never something that any of the docs I knew got excited about. It’s an inconvenient but workable medical issue for most people. Having a elderly relative with it I know it wasn’t pleasant but not overwhelming.
Like most of these issues, I would prefer more research and exploration of nonpharma interventions. Always, always with every medical or actually human issue money and its intricate loops get in the way of good kind just merciful medical intervention.
Report comment
More on Nemeroff from Marcia Angell’s “Drug Companies & Doctors: A Story of Corruption” (2009)
http://www.nybooks.com/articles/2009/01/15/drug-companies-doctorsa-story-of-corruption/
I quote her verbatim:
“Perhaps the most egregious case exposed so far by Senator Grassley is that of Dr. Charles B. Nemeroff, chair of Emory University’s department of psychiatry and, along with Schatzberg, coeditor of the influential Textbook of Psychopharmacology.2 Nemeroff was the principal investigator on a five-year $3.95 million National Institute of Mental Health grant—of which $1.35 million went to Emory for overhead—to study several drugs made by GlaxoSmithKline. To comply with university and government regulations, he was required to disclose to Emory income from GlaxoSmithKline, and Emory was required to report amounts over $10,000 per year to the National Institutes of Health, along with assurances that the conflict of interest would be managed or eliminated.
“But according to Senator Grassley, who compared Emory’s records with those from the company, Nemeroff failed to disclose approximately $500,000 he received from GlaxoSmithKline for giving dozens of talks promoting the company’s drugs. In June 2004, a year into the grant, Emory conducted its own investigation of Nemeroff’s activities, and found multiple violations of its policies. Nemeroff responded by assuring Emory in a memorandum, “In view of the NIMH/Emory/GSK grant, I shall limit my consulting to GSK to under $10,000/year and I have informed GSK of this policy.” Yet that same year, he received $171,031 from the company, while he reported to Emory just $9,999—a dollar shy of the $10,000 threshold for reporting to the National Institutes of Health.
“Emory benefited from Nemeroff’s grants and other activities, and that raises the question of whether its lax oversight was influenced by its own conflicts of interest. As reported by Gardiner Harris in The New York Times,3 Nemeroff himself had pointed out his value to Emory in a 2000 letter to the dean of the medical school, in which he justified his membership on a dozen corporate advisory boards by saying:
Surely you remember that Smith-Kline Beecham Pharmaceuticals donated an endowed chair to the department and there is some reasonable likelihood that Janssen Pharmaceuticals will do so as well. In addition, Wyeth-Ayerst Pharmaceuticals has funded a Research Career Development Award program in the department, and I have asked both AstraZeneca Pharmaceuticals and Bristol-Meyers [sic] Squibb to do the same. Part of the rationale for their funding our faculty in such a manner would be my service on these boards.”
Report comment
Marica Angell on Nemeroff: “Perhaps the most egregious case exposed so far by Senator Grassley is that of Dr. Charles B. Nemeroff” from Drug Companies & Doctors: A Story of Corruption by Marcia Angell January 15, 2009 at http://www.nybooks.com/articles/2009/01/15/drug-companies-doctorsa-story-of-corruption/
Report comment
I somehow think this vid is relevant. It is called: George Monbiot on Neoliberalism: “A self-serving racket.”
https://www.youtube.com/watch?v=UuMntvVwwWM
Report comment
http://fibroawareness.info/clinical-research-finds-neurontin-lyrica-death-sentence-new-brain-synapses/
Neurotin andLyrica speed brain decline faster than any known substance…. Still heavily prescribed for withdrawal.
Report comment
Yikes
I was prescribed Neurotin as part of the ‘cocktail’ of drugs my former shrink prescribed for my mythical ‘chemical imbalance’.
Might have something to do with the PAWS I’m dealing with now these last 3+ years.
But who knows? And who the F*** cares?
Report comment
Well, I guess David, since we’d rather not alter the brain with poisons, as you suggest, we’ll have to we’ll have to turn to Electroconvulsive SHOCK Treatment won’t we, and burn it out. Have you considered a job with CORE, Charles Kellner’s group, at Duke University – the centre for ECT `research’ in 2017 – the centre for delusional psychiatry, at least some are delusional, others are ruled by the profit motive.
After all this is the treatment so admired by you that you wrote a book extolling its effectiveness and safety. The book that was funded by the Scion Natural Science Association, Dr Max Fink’s (the grandfather of shock) private family foundation funding research favorable to ECT. Dr Fink promoted ECT for over 50 years. He made promotional videos for shock machine company Somatics, and published books and articles denying any adverse effects of ECT, though paradoxically was often quoted describing its brain injuring potential. Guess you missed that.
Report comment