
Two years ago, I read Robert Whitaker’s book Anatomy of an Epidemic. Little did I know then that I would get to work with him on the issues that unite us. Since Autumn of 2018, I have been working on the Swedish site which now joins the other global affiliated sites: Mad in America Hispanohablante, Mad in Asia Pacific, Mad in Brasil, Mad in Finland and Mad in the UK. It is with great pleasure that I announce that Mad in Sweden launches today, March 16th, 2019.
The number of people in Sweden experiencing mental ill-health has increased dramatically in the last couple of years. Society’s efforts to address mental health are often characterized by great legal uncertainty and dominated by a biomedical view of human distress. Many feel that this road will, ultimately, lead to more distress and not meet society’s needs.
Psychiatric diagnosis
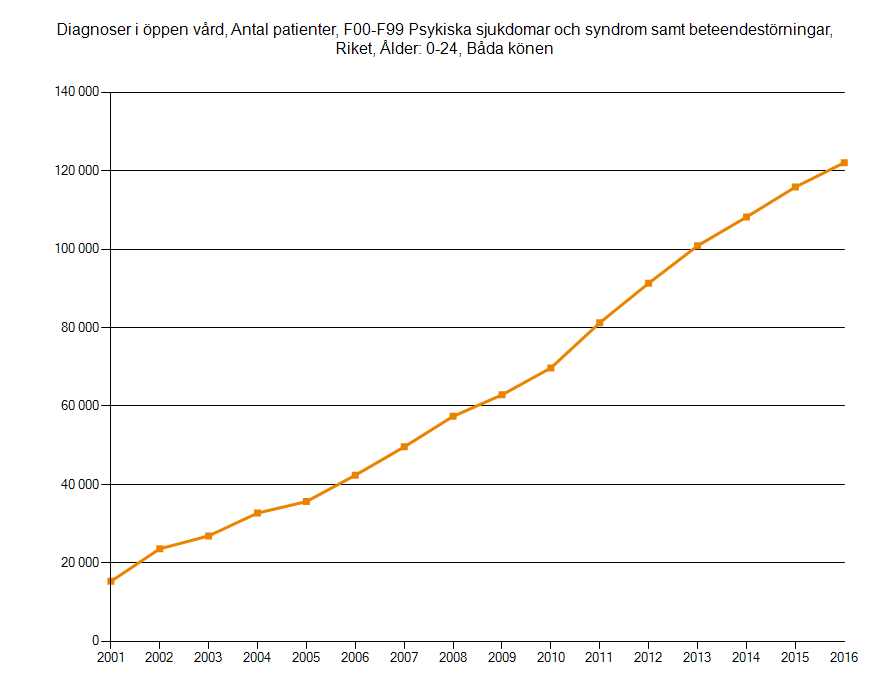
In pace with the rapidly increasing reports of poor mental health, the number of people receiving a psychiatric diagnosis has also increased sharply. It seems clear that diagnostic inflation is having a profound impact on vulnerable children and young people. In outpatient care for children and young people aged 0-24 years, the number with a diagnosis has increased several hundred percent since the beginning of the 21st century.1
The diagnoses that have increased the most during recent years are depression and anxiety disorders. Even neuropsychiatric diagnoses such as ADHD and autism have increased significantly. The same applies to other diagnoses, as evidenced by increasing use of antidepressants and other psychotropic drugs.2
While the National Board of Health predicts continuing increases in both psychiatric diagnosis and prescription of psychiatric drugs, the diagnosed ‘mental illness’ among Swedish children and adolescents also tends to be prolonged. According to the National Board of Health’s report, “The development of mental illness among children and young adults,” those children and young people who are diagnosed with depression or anxiety disorder, and those who are cared for in specialized mental care, end up with long-term mental illness and continuing needs for psychiatric care and psychiatric drug treatment. Even the risk of suicide attempts and suicide is significantly higher for this group of children and young people than for the rest of the population.
Although alternatives to both psychiatric diagnosing and the often inevitable psychiatric medication exist, these are rarely mentioned in the public narrative. Thus the vulnerability and social exclusion of the children and young people is reinforced along with the unsustainable influence of the biomedical view of human distress and suffering.
Prescription of psychiatric drugs
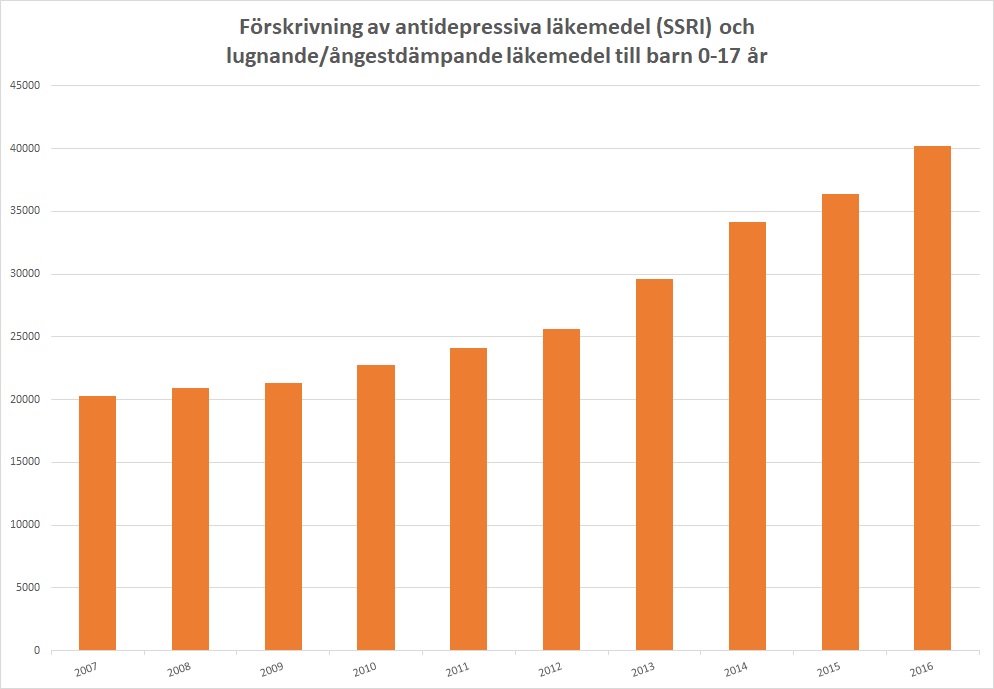
When looking at psychiatric prescribing, we see a similar story to that of diagnosis. For example, the prescribing of antidepressants and sedatives/anxiolytics to children aged 0-17 years has doubled in the last decade.3
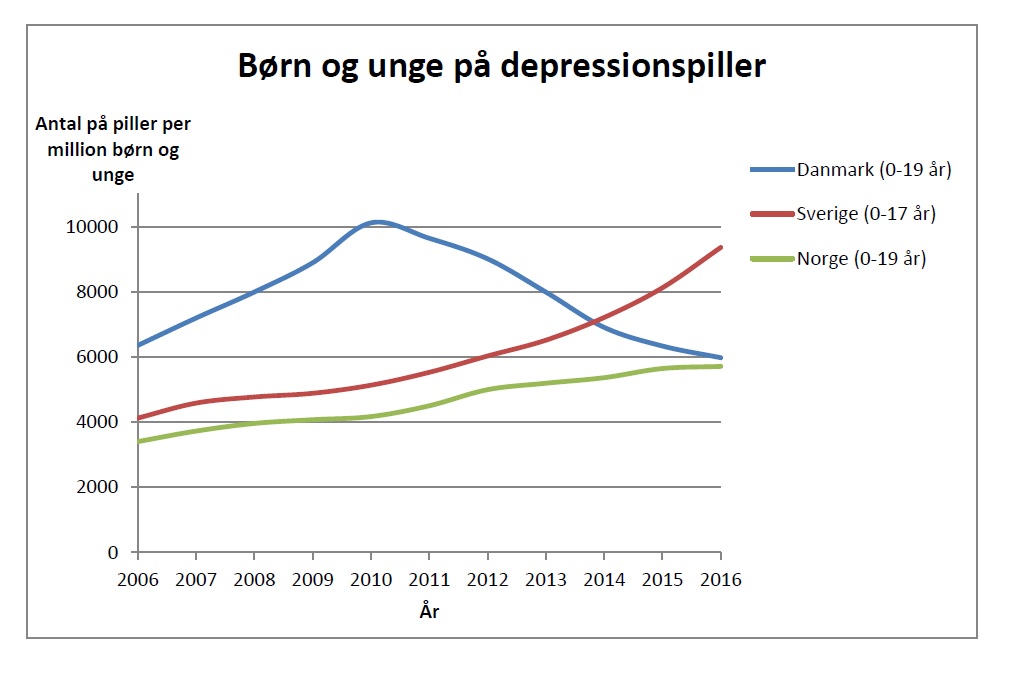
As regards the prescription of antidepressants to children and adolescents between 0 and 19 years, Sweden differs markedly from its Nordic neighbors Norway and Denmark. While prescriptions have increased gradually in Norway and decreased by almost half (!) in Denmark over the past seven years, prescription in Sweden has instead increased explosively during the same period of time.4
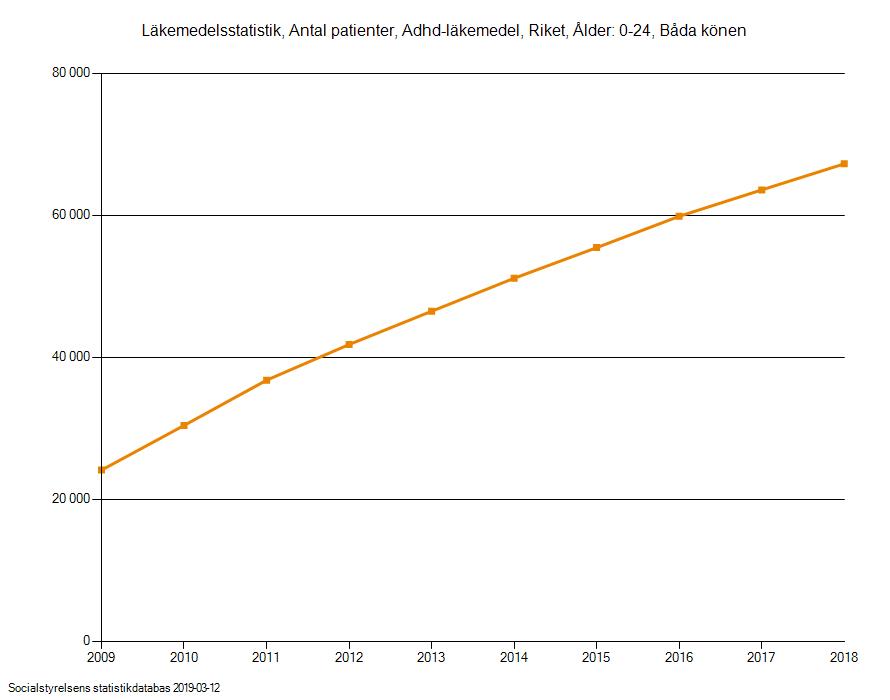
When it comes to ‘mental illness’ among young people, there are even large regional differences across Sweden.5 This also applies to the prescription of psychotropic drugs, including ADHD-drugs, where the number of patients between 0 and 24 years has increased in the last 10 years.6
What the large variations in both psychiatric diagnosis and prescription of psychiatric drugs really result from is a matter for speculation. Regardless of any causal relationships, these phenomena still leave us in doubt as to the value to society of increased diagnosing and prescribing.
Authorities’ recommendation for treatment
In December of 2017, the Swedish National Board of Health published its new national guidelines for treatment of depression and anxiety disorders. In these guidelines, which were widely criticized by a number of referral bodies, psychotropic drugs have a very prominent role in the treatment of depression and anxiety disorders.7 Of the Swedish National Board of Health’s recommendations, very little indicates that any positive change will occur in the near future concerning mental health practice in the country.
Lack of knowledge about psychotropic drugs and their side effects
In addition to the symptom-based and pharmacologically oriented guidelines, there are also large gaps in knowledge regarding psychiatric drugs and their side effects within public health care. Information for patients is often nonexistent and the prescribing is often done without any plan for follow-up, side-effect reporting or withdrawal. In the case of tapering, there are huge gaps in knowledge, which increases the risk of exposing patients to very difficult and sometimes life-threatening withdrawal symptoms.
Looking at the current state of knowledge and the practice that this generates, we can only note from the above that much remains to be done to enable us to find more patient-safe and sustainable approaches in our response to mental and emotional suffering in Sweden.
Together for a sustainable change
With Mad in Sweden we wish to contribute to this change by bringing forward alternative perspectives to the currently dominating biomedical paradigm of mental health, and to hopefully influence unsustainable mental health practice in Sweden.
Mad in Sweden will be administrated in collaboration with FAP – Föreningen Alternativ till Psykofarmaka (The Association Alternatives to Psychotropics), a national politically and religiously independent non-profit association, whose mission is to contribute to improved public health in Sweden. It is an honor for me, both as chairman of FAP and as responsible publisher/editor-in-chief of Mad in Sweden, to be part of a global network of people who, together, want to reform society’s efforts in the mental health arena.
The need for alternative perspectives to today’s biomedical and pharmacologically oriented paradigm of mental health has never been greater. As the United Nations Special Rapporteur on the right to health, Dainius Puras, points out in his 2017 report: “The world needs a revolution in mental health care.”8 9 Mad in Sweden wishes to contribute to the debate and be part of that revolution.














Lasse, Congratulations on the launch of the MIA Sweden site! It is heartening to see that “rethinking psychiatry” is alive, well, and expanding in Sweden. Lycka till !
Report comment
There are a plethora of healing paths far and away from anything bio and psych mainstream which many of us have discovered as we healed from psychiatric debacle. Debating it is an academic exercise and helps no one who is suffering in the trenches. It’s a matter of educating oneself in and applying different ways of thinking which already exist worldwide.
Chinese medicine and the study of yin/yang (masculine/feminine) energy balance in the body is universal truth and based exclusively on the nature of being human. Trauma is energy, as is healing, as is love. Nature is about balance for ease in evolution.
Report comment
Should society be “providing” “medical treatment” for it’s social problems? That is the multi-billion, going on trillion, dollar question.
“The number of people in Sweden experiencing mental ill-health has increased dramatically in the last couple of years.”
Replace the word Sweden with the word world, and you might just have something there. No wonder Mad In America, Inc. is expanding, too.
The 17th century Trade in Lunacy has evolved into a less lucrative (unless you think pharmaceutically oil’s well that ends oil’s well) but actually more sustainable 21st century Trade In “Mental Illness”. One might wonder why, but I don’t. Obviously, any Trade In “Mental Health” is not going to pay off. Also, you’ve got your release valve for the state when it comes to social issues with this detour and diversion (kinda like a perpetual motion machine).
In the psychiatric realm, the alternative medicine angle (pseudo-science anywhere else) is booming because of the fraudulent nature of the entire business.
Keep going.
Report comment
Social issues will be alleviated as individuals (and, in turn, societies) align with nature. Science will either eventually prove this if it wants to, or some may continue try to keep truth away from the public and keep it to themselves, so they can continue to collect more and more money for more and more “research,” or what have you–maybe a nice big house, exotic travel, high rent office space, state-of-the-art technology, etc.
What’s changed is that people are now more awake and savvy, so we’ll get the information one way or another. We don’t really need the ivory tower perspective any longer. It is neither practical nor grounded in reality, and I think most people realize this by now.
Life simply is, and it creates as it flows. The evidence is everpresent, we do not need scientific proof of this. Life abounds, it is inherently abundant clearly, as we hear, see, feel, taste, and/or smell on a daily basis. Experience is the teacher and guide, unique to each of us.
Report comment
I wish you well in your efforts Mr. Mattila.
Report comment
Glad the word of the fraud of psychiatry is spreading the globe. Best wishes, Lasse.
Report comment
Will Mad In Sweden subject all comments to pre-screening like MITUK?
Report comment
Hi Lasse, congrats on your hard work and wish you success in going farther than you knew possible.
Thanks Robert, MIA.
Report comment
Congrats, I hope it draws a lot of people.
We need to wonder IF “mental illness” “increased”, or did “diagnosis”?
Psychiatry loves this question as their answer I can guess. Almost all answers are guessable, counterarguments are often guessable especially in that field.
They would say that it is not that MI has increased, but rather that the experts have “identified” more, that the other “experts” years ago missed. Also they use the argument of “early identification”….
Of course, we know better. There are not more people MI, in fact you can prove this theory by sending ANYONE to a shrink. They will not let people escape without a label. Guaranteed.
If a shrink went to a shrink, he also would get a label.
The DSM is what is the trap. You can literally catch the whole world with it, because it is non sensical.
The disorders are made up in the brain of shrinks who then turn around and make it fit as loosely as possible.
Report comment