
In their recently published article in Journal of Psychotherapy Integration, a team of international researchers led by Christopher Hopwood propose how the novel hierarchical taxonomy of psychopathology (HiTOP) framework can innovate psychotherapy. With this new framework, Hopwood and his team attempt to improve the clinical utility of diagnoses, connecting clinical and research interests in a way that previous taxonomies have not done for psychotherapy.
In recent years, a variety of alternative diagnostic systems have sprung up in reaction to the limits of the Diagnostic and Statistical Manual (DSM) that dominates in mental health services. Naturally, these new systems have problems of their own. For example, the National Institute of Mental health (NIMH) has developed the Research Domain Criteria (RDoC) to search for biomarkers of “mental diseases.” There is a concern that a focus on biomedical explanations will undermine institutional support and funding for psychotherapy research and training in favor of drug development.
In response, the authors anticipate that the fields of psychopathology and psychotherapy will move towards multidimensional and integrative approaches. HiTOP is a model of a psychiatric diagnostic system that its proponents argue that it is a more empirically driven and dimensional classification system, compared to the current categorical ones (i.e., DSM, ICD) that they feel is constrained by clinical authority and tradition. HiTOP principles are proposed for improving psychotherapy practice and research to promote more clinically useful psychopathology models that allow for more synthesis between diagnosis, clinical conceptualization, and treatment.
“HiTOP conceptualizes psychopathology as continuously distributed rather than as binary categories. With respect to the interrelations among variables, HiTOP groups psychopathology constructs based on their empirical relations to one another in a hierarchical factor structure, whereas expert-based models organize psychopathology constructs based on their presumed phenotypic similarity,” the authors explain.
“Given that evidence is incomplete regarding the structure of psychopathology, particularly at the lower levels of the hierarchy, the HiTOP structure is an evolving model undergoing continuous empirical refinement.”
 They mention that some of the major issues mental health professionals have with these dominant paradigms. For example, the co-morbidity of disorders within a person as patients more commonly present with multiple diagnoses create difficulties with generalizing findings from psychotherapy clinical trials tied to a single diagnosis.
They mention that some of the major issues mental health professionals have with these dominant paradigms. For example, the co-morbidity of disorders within a person as patients more commonly present with multiple diagnoses create difficulties with generalizing findings from psychotherapy clinical trials tied to a single diagnosis.
Heterogeneity is also a major issue in that people diagnosed with the same disorder may be more different than they are similar. Psychotherapists often need to do further clinical formulations because categorical diagnoses do not offer much to direct more effective and personalized treatment.
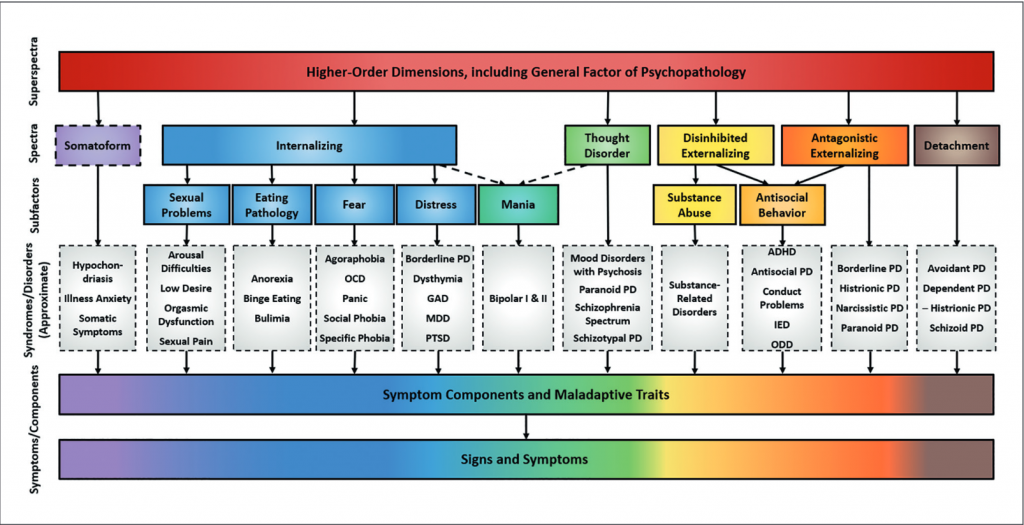
The authors outline the six levels of the HiTOP framework:
- “General psychopathology factor” or “super spectra” indicates nonspecific clinical severity and is related to all forms of psychopathology.
- “Major spectra” reflect personality dimensions (internalizing, thought disorder, disinhibited externalizing, antagonistic externalizing, detachment, and somatoform.
- “Subfactors” group together diagnostic variables such as fear, distress, and mania.
- “Syndromes” are similar in principle to DSM-5 disorder categories.
- “Components” include homogenous symptom clusters and narrow maladaptive traits like insomnia or callousness.
- Finally, the spectrum’s base contains signs, symptoms, and maladaptive behaviors such as compulsive checking.
 HiTOP being conceptualized as trans-theoretical adds to its advantage as the field of psychotherapy is often thought to be fractured among different schools of thought. The authors offer suggestions around bringing about a potentially mutually beneficial relationship in integrating HiTOP with treatment principles from three major clusters of therapy types identified by the authors: common factors, cognitive-behavioral (CBT), and relational therapies.
HiTOP being conceptualized as trans-theoretical adds to its advantage as the field of psychotherapy is often thought to be fractured among different schools of thought. The authors offer suggestions around bringing about a potentially mutually beneficial relationship in integrating HiTOP with treatment principles from three major clusters of therapy types identified by the authors: common factors, cognitive-behavioral (CBT), and relational therapies.
However, the authors caution that HiTOP is not interested in mapping specific techniques in these clusters to specific model variables.
“The presence of transtheoretical common factors in psychotherapy and a statistical general factor of psychopathology should support integrative approaches to practice and research. That is, psychopathology and psychotherapy researchers should focus more on clarifying why so many different problems seem to co-occur, and why so many features of psychotherapy seem to be effective for treating people regardless of their specific problems,” the authors note.
“In addition, research aimed at ascertaining the degree to which general factors in psychopathology and psychotherapy have something in common would be useful.”
The common factors model includes treatment elements like expectancy (i.e., placebo), therapist and client effects that influence psychotherapy’s effectiveness across approaches. The authors propose studying whether common factors reduce specific symptoms through their impact on the general factor of psychopathology. In understanding the nature of the general psychopathology factor and its elements, HiTOP could provide an evidence-based explanation for why different treatment approaches tend to produce similar therapeutic effects.
CBT focuses on skills training, cognitive restructuring, and exposure based on learning theory. It has been historically aligned with the DSM, studying treatments through randomized controlled trials (RCT) that focus more narrowly on shifts in the symptom level of a diagnosis.
With a recent emphasis in CBT on trans-diagnostic practice, HiTOP provides CBT ways to expand to a wider range of psychopathology beyond the ‘internalizing’ spectrum. This is done by focusing on finer dimensions of psychopathology not clearly defined in most categorical diagnoses (e.g., types of compulsive behaviors in OCD). From CBT, HiTOP could benefit from incorporating learning theory into understanding how the environment influences the expression of psychopathology at the different levels of the hierarchy.
In relational psychotherapy traditions, such as psychodynamic therapy, there is an emphasis on the relationship between therapist and patient as central to healing, with such techniques as transference interpretations and improving mentalizing. HiTOP could provide ways to summarize the complexity of a person’s problems in a more focused manner.
The authors see psychodynamic approaches providing HiTOP with attention to conscious and unconscious aspects of personality and psychopathology that could improve assessment, such as expanding from verbal report-based measures relying on conscious knowledge (e.g., MMPI-3) to more performance-based measures (e.g., Rorschach Inkblot Test). Psychodynamic perspectives also provide a developmental perspective to HiTOP and inform the relational aspects of how the social environment reinforces, maintains, or alters psychopathology.
“Clinical utility studies suggest that clinicians and researchers tend to find dimensional models more useful than categorical models. However, such research has focused primarily on personality disorders. The hierarchical organization of psychopathology variables in HiTOP facilitates a comprehensive approach to the assessment of both pretreatment functioning/diagnosis and treatment outcomes for all of psychopathology.”
“The assessment approach should help the clinician identify the specific regions of the HiTOP model that are most relevant to the patient’s presenting problems. The flexibility of HiTOP allows the clinician to focus on different levels of generality and type of problem. The clinician would then apply the intervention that is most likely to work, based on the HiTOP characterization of the client’s clinical concerns.”
As psychotherapy research on treatment principles has demonstrated common strategies that are effective for a range of disorders, HiTOP could shift treatment focus up from the level of specific disorders to broader variables in the hierarchy. Since its multidimensional nature, HiTOP also would require measuring a range of outcome variables in treatment research, rather than just measuring symptoms of a disorder.
As a framework for studying individual differences, HiTOP is thought to help study therapist effects on treatment outcome and explore the zones in the hierarchy where particular therapists are more successful.
The article ends with a case example of how HiTOP conceptualization could help the therapist improve their approach to the patient. However, the authors also acknowledge difficulties in implementing HiTOP as proposed, including traditional divisions of different psychotherapy schools and the categorical model’s entrenchment in the health care system and third-party reimbursement.
****
Hopwood, C. J., Bagby, R. M., Gralnick, T., Ro, E., Ruggero, C., Mullins-Sweatt, S., Kotov, R., Bach, B., Cicero, D. C., Krueger, R. F., Patrick, C. J., Chmielewski, M., DeYoung, C. G., Docherty, A. R., Eaton, N. R., Forbush, K. T., Ivanova, M. Y., Latzman, R. D., Pincus, A. L., … Zimmermann, J. (2020). Integrating psychotherapy with the hierarchical taxonomy of psychopathology (HiTOP). Journal of Psychotherapy Integration, 30(4), 477–497. https://doi.org/10.1037/int0000156 (LINK)














No, because Psychotherapy is about earning a living, and ‘Mental Health’ Recovery is Straightforward.
Report comment
Forgive my ignorance, but this all largely reads as a bunch of psycho-babble to me. Since I’m pretty certain that I agree with you, that the DSM “bible” belief system is wrong. And I’m pretty certain the major issue with most of those who have been mislabeled with the psychiatric DSM disorders, by both the psychologists and psychiatrists, is that the vast majority of them, are child abuse survivors.
https://www.indybay.org/newsitems/2019/01/23/18820633.php?fbclid=IwAR2-cgZPcEvbz7yFqMuUwneIuaqGleGiOzackY4N2sPeVXolwmEga5iKxdo
https://www.madinamerica.com/2016/04/heal-for-life/
And all this systemic psychological and psychiatric, systemic, child abuse covering up, is all by DSM design.
https://www.psychologytoday.com/us/blog/your-child-does-not-have-bipolar-disorder/201402/dsm-5-and-child-neglect-and-abuse-1
So, perhaps rather than proposing new weird, and unproven, psychological theories, for explaining the systemic “invalidity” and serious problems going on within both the psychological and psychiatric industries, psychologists should be properly addressing the common sense problems within your industries? Which are that both your industries are systemic child abuse covering up industries. And these systemic crimes have led us all to now living in a satanic “pedophile empire.”
https://www.amazon.com/Pedophilia-Empire-Chapter-Introduction-Disorder-ebook/dp/B0773QHGPT
Report comment
Hi Javier,
Are you familiar with the UK’s Power Threat Meaning Framework (PTMF)? It makes so much more sense to me than this HiTOP framework, which feels somewhat like rearranging the chairs on the deck of the Titanic.
But the PTMF, developed with core involvement from some heavy hitting survivors, seems to ask the right questions:
What happened? (Imagine that! I have yet to find a person who had been diagnosed in a hospital–or anywhere?–be asked this!);
How did it affect you?;
What sense do you make of it?;
What did you have to do to survive?;
What are your strengths: and
What is your story?
Seems kind of brilliant to me. Read a summary here https://openexcellence.org/introducing-power-threat-meaning-framework/
With respect,
Grace
Report comment
If being called schizophrenic got you a sumptuous tree lined drive leading up to a five hundred million dollar home set in seventy three acres of pristine, fertile land dotted with cottages for your many friends and a star shaped heated pool with a revolving palm tree bar and a feature waterfall tumbling into a deep indigo lagoon ably stocked with tropical fish..perhaps eight billion people on this planet would form a very very very long long long queue in the hope to be called schizophrenic. With reference to this article I think it does not matter much what words you use to describe some’s need, only simply that you endeavour to respect the need where possible. You could call psychosis “big distress” or “misery” or “purple pineapples syndrome” it does not get you past the really hard task of merely enabling the person to get more comfortable, regardless of what words you use to “define” the fellow before you. I have long suspected that “specialists” of “people” have a problem taking people at face value. They seem ever wont to magically “work” on them, or “transform” them, or “mould” them, or otherwise make them the raw clay to their life’s purpose. It gets called “a relationship” and really that is ALL it actually is. There is no hocus pocus theoretical underpining itching to make the relationship “a specialist” relationship, like “an illicit” relationship” or “a saviour relationship” or “a sado masochistic relationship”….it is just an ordinary boring muddled human relationship with good aspects and rubbish aspects. When people start doing “specialist” styles of relationship I think of rainforest tribes and quite what they might make of those. Yes, indiginous people do cavort with the drama of “roles”, where there may puff or chant an “expert” of leaves, a “doer”, if you like, but the “done to” is not expected to be a docile recipient, since docility and complience would be a dire sign of something being woefully very wrong indeed.
Anyway, I am growing bored with my own comment now and my dinner smells delicious…..
Report comment
It seems HiTOP may be a more scientific way of classifying different types of “symptoms” into categories than the DSM. But like the DSM, it assumes psychological experiences are “symptoms” (i.e., manifestations of a pathological condition) and totally ignores the history and context in which they occur. No matter how much success the authors have in scientifically mapping various types of “symptoms,” their framework can never be useful in actually understanding a person’s psychological experience or of any use to therapists who attempt to understand their clients as people whose psychological experiences are reactions to what has happened in their life and the meaning they make of it.
I agree with Grace that the UK clinical psychology Power, Threat, and Meaning framework makes so much more sense than HiTOP. The UK framework was written mainly by practitioners who want to be able to understand and help real people. The HiTOP framework is written mainly by American academics who don’t see clients and are incentivised for publications and research grants.
Report comment
I HAVE SCHIZOPHRENIA. I prefer you to call me by my chosen definition not yours.
Report comment
Waste of time. The “model” fails to alter the most basic and incorrect assumptions of the DSM, namely, that a “clinician,” by virtue of some level of training and education, can look at someone’s behavior, mood, or thinking and objectively determine if there is something “wrong” with them. It doesn’t matter how you slice it, we’re substituting human judgment for actual scientific observation and attributing “medical” legitimacy to someone’s biases and opinions based solely on what kind of degree or training they have. As long as we pretend that we are “diagnosing” a “mental illness,” it doesn’t matter if we use HiTop or the DSM or the ICD or a dart board, we’re wasting a lot of energy categorizing what kind of iceberg hit the Titanic instead of trying to keep the ship from sinking or getting the passengers to the lifeboats!
Report comment
Here is an analogy. Imagine we apply the DSM symptom-based approach to medical symptoms. The DSM framers would invent syndromes such as sore throat disorder, cough disorder, fever disorder, difficulty breathing disorder, chest pain disorder, rash disorder, etc. These disorders would be grouped together in sections based on the framer’s clinical judgment – for example, difficulty breathing disorder would be found in the respiratory disorders section.
Then HiTOPS comes along and says we can do better. Symptoms such as sore throat are dimensional, not categorical. And the DSM way of grouping disorders together relies on expert judgment, so we can group them together empirically which is more sciency. A coalition of HiTOPS academics produces a new model of medical symptoms. There is a higher-order factor of “general medical symptoms,” and several lower order “major spectra” such as respiratory symptoms, cardiac symptoms, pain symptoms, movement symptoms, and so on. Within these spectra are DSM-based disorders such as cough disorder and sore throat disorder (which are often comorbid). What an improvement!
Imagine the innovation in assessment and treatment this new HiTOPS system will produce! I quote the article cited in Javier’s article: “The assessment approach should help the clinician identify the specific regions of the HiTOP model that are most relevant to the patient’s presenting problems. The flexibility of HiTOP allows the clinician to focus on different levels of generality and type of problem. The clinician would then apply the intervention that is most likely to work, based on the HiTOP characterization of the client’s clinical concerns.”
As they say in Australia, yeah…nah. It is as useless to understand psychological experiences purely at the “symptom” level as it is to understand medical diseases at this same level. And it’s also philosophically wrong to construe psychological experiences like feeling sad, worried, bored, irritable, etc. as “symptoms.” It’s long past time to retire the symptom-based approach of the DSM and HiTOPS. But researchers continue to be incentivised for using these systems in their publications and grants, and practitioners are incentivised for using these systems in their work, and the entire educational framework of psychology and psychiatry is based on accepting symptom-based diagnosis as valid. The entire system is f$%&#d. The fact that symptom-based diagnosis is invalid and harmful is an inconvenient truth, best to ignore it when there are jobs to be had and money to be made.
Report comment
Excellent analysis!
I always figured the best assessment tool was to ask the client what s/he felt was troubling them, and then ask what they would like to see be different in their lives. Then ask them what barriers they saw to making that happen. Depending on what they said, there would be a whole lot of different things they could do to move in the direction they wanted to. No “clinical judgment” or “diagnosis” or “spectrum disorders” required!
Report comment
I applaud what you are saying here Steve. And sorry to latch on like a sticky label. Im just munching my rice cake and scrolling in a coffee break and there you are, sounding eloquent again. I like what you say in this comment very much. You exemplify what it means to be non judgemental. This is the spirit of acceptance. But as I am writing this, is it? When I meet someone I am abuzz with sensory input from my several senses. I perceive their body odour, their tone of voice, the wealth or poverty of their attire, their knees, their tendency to click their pen, all kinds of things, and it is a given that they perceive me in such a way also. We drink each other in. And in that process most people cannot stop their innate tendency to assess, which means judge. Is this person sad, safe, wild, loyal, vindictive….on and on it goes like a fluid reconnoitre that periodically adjusts if something surprising occurs. I have exprienced all kinds of non judgey people and I adore them and aspire to be that way. However, I have met one or two who were a bit cloak and dagger and concealing their judgeyness in a way I have found alarming, more than if they did the thing kids do when little kids boldly state outright what they think of you. I had a counsellor for a time who oozed acceptance and this I found more like she was doing a taking thing than a giving thing, like she had read a book on how to do the technique of benevolence on clients and was loving me but it seemed to be coming from a place of her own need to see herself as more loving than her colleagues. It did not feel like it was genuine acceptance. I could be wrong about that. I do whole heatedly agree with what you yourself are aiming to create. You come from a place of integrity, I can tell.
For me, I want a counsellor to accept that I need my diagnosis. There are a number of reasons for that but probably the biggest is that my schizophrenia has been for me a life of unending hell. It has felt like being in my own personal Belsen and being hourly marched to the gas ovens. I want to call that hell a stunning name. A weird name. A ghastly name. An outageous name. And even a beautiful name. A triumphant name. A bastard of a name. A mythic battle of a name. A kickable name. A shoutable screamable name. A name I can blow snottily into a wept out tissue. A gangster name. A fuck off name. A pop star name.
I dont want to call my Belsen hell…..”trauma”.
A tea at the vicarage name.
But you know, Im a bit screwed up. I mean much of the Belsen stuff is because I am persecuted by a voice who orders me to think a certain way, speak a certain way, even now as I try to write this I am being orderd not to. And that voice often tells me I have to say I am schizophrenic when I would rather read a book. It is a bit like a tyrant that takes over. So I am very much approving of what you say and that nobody should be saddled with a description of them that they do not like the sound of. I am all for nobody having to say they are something they do not feel in their heart or being that they are. But equally I think if someone wants to have a certain way of describing who they are they should also have that free choice. And neither should be “name shamed” because of their free choice. Because when people deny anyone their free choice, whether they want to call their condition poverty, or whether they want to call their Belsen hell schizophrenia, people become what people are trying to remedy, people become the shadow side of judgement.
Imagine a Jew getting led yet again to the showers for the fiftieth time that year and finding an activist there near the sliding door saying “do you mind not calling yourself a Jew, it offends the Alaskans”.
For a million kids going through hell some of them wont want their diagnosis but some of them shall. I know for myself that it is very helpful at this time in my life to shut up the awful bogeyman in my head by really concentrating and telling him “You are only schizophrenia, go away!”. As you may know, one of the worst things about schizophrenia hallucinatons is you cannot, simply CANNOT believe it is just an illness, since the nightmare figment feels horribly real every five minutes, and because of that disbelief you want something extraordinary to fling at it, something almost mystical sounding, to save your actual real life, and the word “trauma” isn’t gonna do that for kids at their wits end. The whole world IS TRAUMA. We are all awash with TRAUMA. Everyone and everyone’s friends have had trauma. It is all over the place. But hardly anyone of those billions of variously traumatized people will be having to go to bed tonight with two excruciatingly tight hats on their head to stop the insufferable torment of an invisible monster who wraps and coils into their pondering to the extent they dare not think at all incase Belsen happens on the barb of a feather of a thought.
Report comment
You write very powerfully! And I appreciate your comments very much, and your kind words for me as well.
I think the only REAL way to be non-judgmental is to understand that we are ALL judging all the time, and to become AWARE of and acknowledge one’s judgment, to the degree that one is able to view those very judgments themselves objectively enough to set them aside and not put them onto the other person. It is difficult to describe, but I do believe it is most definitely possible to accomplish, at least enough that the person we are dealing with doesn’t feel they are being judged and sees that you are able to hear what they really are saying instead of what you think they ought to say or mean.
I am reminded of a quote from the Princess Bride by your closing paragraph: “Live IS pain, Highness. Anyone who tells you different is selling something.”
Report comment
Dear Daiphanous Weeping,
Your post took my breath away.
I have had the experience of being in the gas chambers, but for me it was Auschwitz and only once (this lifetime), and it ended with dying and death all around me. No, actually, it didn’t end there. That part was almost serene, an acceptance and still a connection to G-d. Instead, it ended with my body scooped up and fed into the furnace, at which time my soul started screaming and screaming and screaming.
I cannot imaging having to go through that hourly.
What I’m getting is that it’s not the name you mind. It’s the torture. And if the name can help quiet the torment even for a few minutes, you have a right to it and demand (hope? request? expect?) not to be name shamed. That, at least, is free choice. And you want a counselor–and a community?–that authentically accepts this.
Also, that the word trauma stands for something so universal it becomes like repeating a word over and over until the meaning dissolves. The texture, range and depth and soaring height of your experiences deserve to be named their many forms in a way that is true and alive for them and you, from moment to moment. All of those shimmering, terrifying, magical names.
Thank you for sharing so astonishingly closely. I don’t know who you are or where you live, but I feel like you have reached out your hand, open, palm out, and I am moved to reach mine out to meet it.
With a full heart,
Grace
Report comment
How beautiful of you Grrace to bring on the bandages. Aw, what a lovely soul you are. And I am in awe of anyone who has been through Auschwitz. I am not sure if you experienced the actual geographical Auschwitz or the sort of portable one that psychosis does, the one that makes a facsimile of the huts and puts into the being you are, and your several senses that would be perceiving the sights and sounds and smells and horror of the real muddy environ, an evocation of terrifying cruel people. Either way I honour your endurance.
Your comment has blown me away as I sincerely never expected it. I try to write not for myself but for others, though I use my passion to empsthize with them if I can. I am also though aware that my many chatty comments have stirred up alot of mental activity in my brain as I go through the philosophical twists and turns of this voyage of learning and sharing. It is all good. Though I must today retreat from mulling on everything activism. Just today. Ive just moved house and my brain is in a spin. Im sure the reaching out will find the fingertips. Let me just for today give you something rewarding for you being so compassionate and commiserating. It is in recognition of the torture you and I both know is unspeakable, it is my “serene” silence.
(I am new to MIA and not sure of how anything is done here. I feel sure we can maybes email one another. Though I probably wont be able to be prolific at this time because I have an elderly dementing mother to look after. She thinks I am fourteen and in need of a blazing row.)
But you know…
“only love can set us free”.
Report comment