

The first time I met Martin Harrow was after he gave a presentation at the 2008 meeting of the American Psychiatric Association. At one point he grew annoyed with one of my questions, and I am reminded of this today, following his death on February 21, because it helps illustrate the extraordinary courage and intellectual curiosity that it took for him, and his long-time collaborator Thomas Jobe, to persist in their research that told of antipsychotics worsening long-term outcomes in psychotic patients.
That day Harrow had presented the findings from their 2007 paper on 145 patients in their Chicago Followup Study. Theirs was the best longitudinal study of outcomes for psychotic patients in the antipsychotic era, and they had reported that the recovery rate for schizophrenia patients off medication was eight times higher than for those who stayed on the drugs. You might think, given the importance of this finding, that Harrow would have been asked to present in a large room, and given a full hour so that the audience could ask the obvious questions. This was a finding that belied everything that psychiatry—and the conventional history of psychiatry—held true. But instead, his presentation had been assigned to a small room, and if I remember correctly, he was given only 20 minutes, as he was one of three speakers for that period. The setting was quite telling, for it told of a profession eager to ignore and dismiss his and Jobe’s findings with little more than a wave of the hand. Yet, in his talk, Harrow spoke boldly about their bottom-line conclusion.
“I conclude that schizophrenia patients not on antipsychotic medication for a long period of time have significantly better global functioning than those on antipsychotics,” he declared.
This was a more definitive statement than had appeared in their published paper, and after his talk, as Harrow prepared to exit the stage, I raised a question that immediately aroused his suspicion . . . about me.
In their 2007 paper, Harrow and Jobe had stated that it was the “good prognosis” schizophrenia patients who were more likely to stop taking antipsychotic medication, and this difference in prognosis was the reason for the much higher recovery rate for those off antipsychotics. It wasn’t that antipsychotics worsened long-term outcomes; rather, their study showed that not all schizophrenic patients needed the drugs long-term. That was the clinical implication of their study.
He reiterated all this in our brief conversation, and then I raised a final question. There was a table in their paper that made it possible to compare outcomes for those with milder psychotic disorders at baseline who stayed on antipsychotic medications to schizophrenia patients who got off the drugs, and in this comparison, it was those with milder disorders who had the worse outcomes. Given that schizophrenia is a more severe diagnosis, didn’t that raise the possibility that the drugs, on the whole, had a negative long-term effect?
“Who are you with?” he snapped.
He had reason to be wary of such a question. Harrow was a psychologist and Jobe a psychiatrist, and they had published a finding that was heretical to mainstream beliefs, and everyone knows what happens to heretics in medicine and science, and this is particularly true for heretics within psychiatry. If they are lucky, they will be ignored and politely shunned, but more often, they are in some way ousted from the fraternity of their peers. And now I, with my question, was urging Harrow to go even further out on that heretical limb.
I could see the synapses in his brain firing at that moment: Was I a Scientologist? If so, his answering that question would have made his professional life all that more difficult.
I explained who I was, and the reason that I was curious about the question. I was writing a book that sought to explore this question: How do psychiatric drugs affect long-term outcomes? He relaxed and then, in something of an off-the-record manner, told of the difficulties that he and Jobe had already experienced.

The most prominent psychiatric journals had all rejected their 2007 paper, and finally they published in a second-tier journal, the Journal of Nervous and Mental Disease. The impact factor for this journal was less than two (which tells of how often articles in the journal are cited); the American Journal of Psychiatry has an impact factor nine times as high. And while they believed in their “good prognosis” explanation for the difference in outcomes, Harrow also noted that you had to be careful with your conclusions if they upset conventional wisdom. He didn’t use the word “spin,” but the implication was there: researchers had to soft-pedal the implications of such data if you wanted to get past peer review and into print.
Thus, his moment of annoyance with me is revelatory for this reason: It tells of how Harrow and Jobe, when they published their 15-year findings, had already moved far out on a limb. Their 2007 report had been widely ignored within the field (hence the small room), and if they went any further, they could expect more of the same: isolation, dismissals of their work, and difficulty finding funds to continue their research. If they cared about their careers, they would close the book on their longitudinal study, or at least provide no further report on the impact of antipsychotics on long-term outcomes, and move on to topics that wouldn’t be so upsetting.
Yet, what did Harrow and Jobe do? They had been surprised by the 15-year results of their study, and soon they climbed out further on that limb of heresy. They set out to investigate whether antipsychotics could, in fact, worsen long-term outcomes, and with every new paper they published, their challenge to psychiatry grew.
The conventional history of psychiatry tells of how the introduction of antipsychotics into asylum medicine kicked off a psychopharmacological revolution, a great advance in care. This was the narrative that psychiatry touted to the public and governed their thinking and clinical practice, and yet for the past 15 years, Harrow and Jobe, as they explored every nook and cranny of the data set from their longitudinal study, presented a different truth to consider.
The analogy to draw here is a grand one: think of Galileo upsetting the apple cart in the 17th century with his pronouncements that the earth revolved around the sun and the reaction of the Catholic Church, and you can get a sense of how profoundly their work challenged psychiatry’s conventional beliefs and practices.
Both Harrow and Jobe are now gone, as Jobe died last March. To fully appreciate their work, and to see how they “followed the data,” which is the defining behavior of good scientists, all you need to do is follow the trail of their research subsequent to their 2007 report.
A Record of Research
The conventional wisdom is that antipsychotics reduce psychotic symptoms and the risk of relapse, and therefore they need to be taken continuously. In this paper, Harrow and Jobe specifically countered that wisdom: They reported that “[schizophrenia] patients not on antipsychotics for prolonged periods were significantly less likely to be psychotic and experienced more periods of recovery.” In addition, the patients not on antipsychotics were less anxious and had better cognitive functioning.
In this paper, they first addressed the merits of relapse studies. They noted that the World Psychiatric Association, in a section on pharmacopsychiatry, had set forth the conventional understanding: “Antipsychotic treatment has a significant impact on the long-term course of schizophrenic illness and can significantly facilitate recovery.” But, Harrow and Jobe wrote, most of the increased risk following drug withdrawal is in the first six to ten months, which then recedes. This could indicate that the high rate of relapse during this period was, in fact, a “medicine-generated psychosis” due to the “buildup, prior to discontinuation, of supersensitive dopamine receptors.”
In short, the high relapse rate was likely due to drug-induced changes in the brain, as opposed to a return “of the disease.”
Next, they revisited their own “good-prognosis” explanation in their 2007 paper for the better outcomes of the off-medication schizophrenia patients. This was the explanation eagerly accepted by mainstream psychiatry—this was just a matter of patients with a more severe illness staying on the drugs. But Harrow and Jobe now cast doubt on their own explanation. While many in the good prognosis group who got off antipsychotics had favorable outcomes, they wrote, there were also good prognosis patients treated with antipsychotics for prolonged periods that “did not show favorable outcomes, suggesting early prognostic status is one important, but not the only, influence on long-term outcome.”
Finally, and for the first time, they explicitly raised the possibility that antipsychotics do long-term harm. “How unique among medical treatments is it that the apparent efficacy of antipsychotics could diminish over time or become ineffective or harmful? There are many examples for other medications of similar long-term effects, with this often occurring as the body readjusts biologically to the medications.”
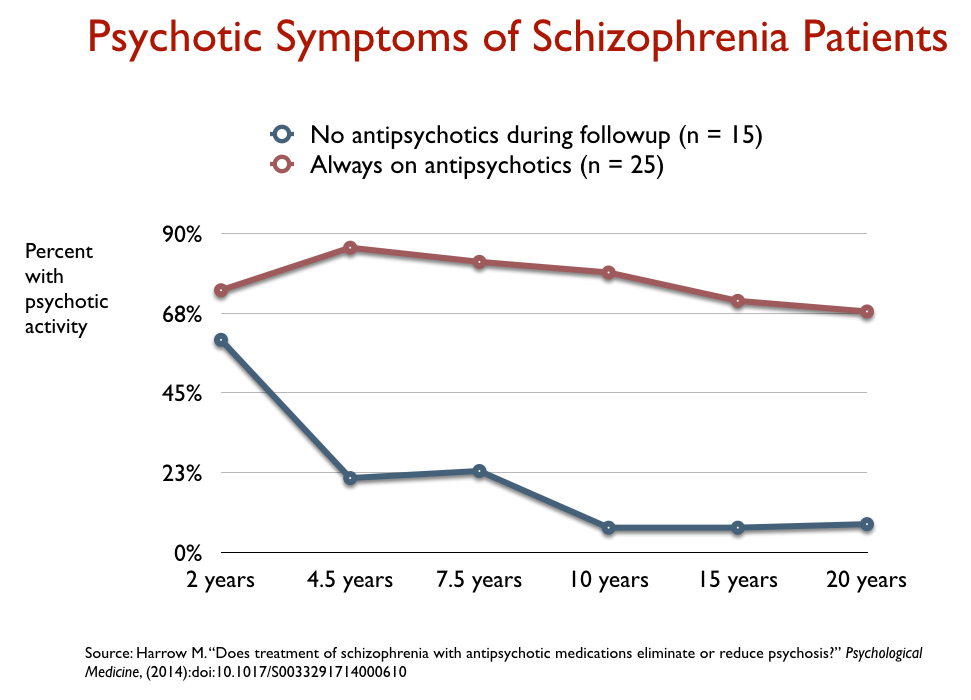
In their study, Harrow and Jobe could identify three sets of patients: those who were medication-compliant throughout the 20 years (on antipsychotic medication at every follow-up), those who got off antipsychotic medication by year two and stayed off the drugs throughout the 20 years, and those who were sometimes on medication at a follow-up assessment and sometimes not. In this paper, they sorted through their data to compare outcomes in those who were either medication compliant or always off medication. This provided a clearer picture of the long-term impact of the drugs, as it removed patients who used the drugs sporadically.
They reported that 70% of those who continuously took antipsychotic medication were actively psychotic at four of the six follow-up assessments. In contrast, patients off prescribed antipsychotics showed significantly less psychotic activity. “After the first few years,” they concluded, “antipsychotic medications do not eliminate or reduce the frequency of psychosis in schizophrenia, or reduce the severity of post-acute psychosis.”
This was a finding that told of drug treatments that, over the long term, worsened the very symptoms they were designed to treat.
The relapse literature in psychiatry fails to tell how psychotic patients are functioning, particularly over the long term. In this paper, Harrow and Jobe addressed this question, and did so by comparing medication-compliant patients to those who got off the drugs early and stayed off them. They found that the off-medication group had “significantly better work functioning.”
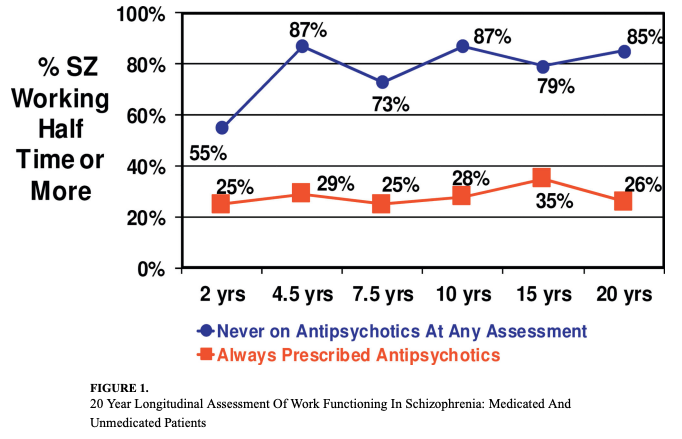
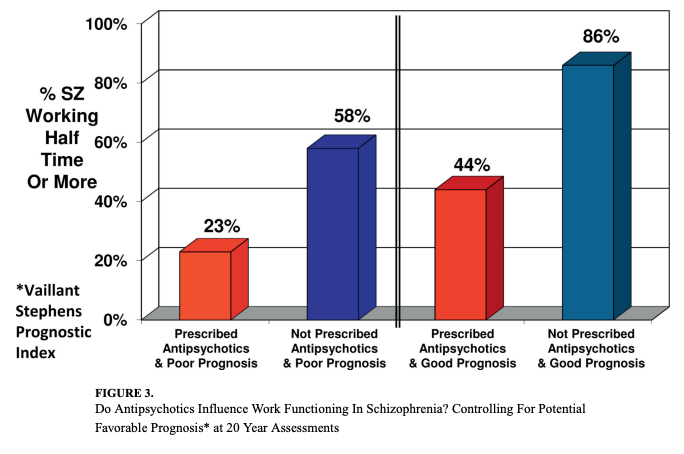
This difference in work history was true for those in the “bad prognosis” group at baseline, and for those in the good prognosis group. In fact, the work history in the bad prognosis group who stopped taking antipsychotics was superior to the work history in the good prognosis group who continually took antipsychotics.
This presentation of work outcomes provided further evidence that it was the drug treatment that was the causal factor, as opposed to a difference that arose from a difference in initial prognosis.
In this publication, they put these findings together to make the argument that antipsychotics worsen long-term outcomes. Their argument consisted of three main points.
In addition to their Chicago Followup Study, there were now seven other studies, they wrote, “assessing whether schizophrenia patients improve when treated longer than two-three years with antipsychotic medication. […] These research programs included samples studied from 7 to 20 years. Unlike short-term studies, none of them showed positive long-term results” for the medicated patients.
As for the “more severely ill” explanation for the difference of outcomes in their study, they had compared outcomes for medicated and off-medication patients in both the “good prognosis” and “bad prognosis” cohorts, and “in both comparisons, those patients not on antipsychotics for 15-20 years had fewer symptoms and better outcomes after the first 2-3 years.”
Third, there was a biological explanation for this long-term worsening: Drug-induced “dopamine supersensitivity psychosis.” Unfortunately, they wrote, “There has been a systematic failure to incorporate this finding [of dopamine supersensitive psychosis] into the risk-benefit ratio for continuous use of antipsychotics. The same applies to the possible negative impact of long-term antipsychotic treatment on work functioning; the block of dopamine receptors may indeed reduce drive and motivation.”
Once more, they responded in this paper to those who dismissed their findings as arising from a difference in the severity of illness between those who stayed on antipsychotics and those who got off. After adjusting for “confounding factors,” such as baseline prognosis and other prognostic factors, they reported that those off medication at any point during the study were six times more likely to be in recovery, and they had a much “lower probability of rehospitalization at subsequent follow-ups.”
As always, there were criticisms of the merits of this final study, which Harrow and Jobe answered with a detailed reply.
Psychiatry’s Response: Nothing to See Here
Such is the extraordinary record of Harrow and Jobe’s research. Their list of publications on this issue tells of how their own initial good prognosis/bad prognosis explanation for the difference in recovery rates did not hold up under further examination—a finding that reveals the “open mind” that governed their investigations. And, by the end, with their last publication, they had told of how long-term antipsychotic use is associated with lower recovery rates, higher relapse rates, greater persistence of psychotic symptoms, worse cognitive function, and worse functional outcomes. Dopamine supersensitivity psychosis provided a biological explanation for why this would be, and there was now a larger body of research—seven additional studies—that had found that long-term use of antipsychotics does not provide a benefit to schizophrenia patients.
I last spoke to Martin Harrow at the time of Thomas Jobe’s death, and asked him why the field remained resistant to their findings.
“There are a lot of publications. But they are not highlighted, they are not advertised. You have been very active in keeping things going, but most people ignore it because it doesn’t fit the time. It’s hard to get people to change. Most people don’t see the data, and most who do shrug it off, say it’s just chance or whatever.”
Money, he added, was an obvious reason. “Drug companies of course don’t want to think their drugs aren’t helpful after two years, this threatens their money supply, and this is one class of drugs thought to work and is very profitable . . . let’s not kid ourselves. The phenothiazines are very financially successful medications, and psychiatrists are taught that phenothiazines are the answer. That is one of the things we have to face. Our research keeps demonstrating that it isn’t the answer, and that most of the patients (after a time) have relapsed.”
Up until the time of Jobe’s death, Harrow and Jobe, together with their colleague Cherise Rosen, would meet every other Sunday at 4 p.m. to discuss their ongoing analysis of their Chicago Followup Study. Harrow was nearly blind by this time, and yet, when I spoke to him last spring, his passion for science was still at work: “We haven’t given up,” he said. “We keep going. We are still going.”
Martin Harrow: Chess Master, Mentor, and Devoted Family Man
Harrow grew up in New York City, and by the time he was 20, he was making his mark as a top competitor in national chess tournaments. He took second place in the U.S. Junior Chess Championship in 1953 and placed in the top seven in U.S. Open Chess Championships three times. He was crowned New England Chess champion in 1967, and he was particularly proud of having twice drawn games against Bobby Fisher, who became world champion after defeating Boris Spassky in 1972.
He received his B.A. from City University of New York in 1955, and his Ph.D. in psychology from Indiana University in 1961. After graduating, he joined the faculty at Yale University, and for years was the chief psychologist at the inpatient unit at Yale-New Haven hospital. While there, he developed a validated diagnostic system, known as the New Haven Schizophrenia Index, that would provide the foundation for his decades of research on schizophrenia and other psychotic disorders.
In 1973, he moved to Chicago to assume the position of Director of Psychology at the Michael Reese Medical Center and to join the faculty at the University of Chicago.
Soon he obtained a National Institute of Mental Health grant for his Chicago Followup Study. Jobe joined Harrow in this research effort after he came to the University of Illinois at Chicago in 1978.
Although Harrow may be best known for that study, he began his groundbreaking work on psychotic disorders while at Yale, and his research investigated many facets of schizophrenia, such as the nature of psychosis and thought disorders, and again and again, his findings challenged conventional beliefs. At his funeral, Rosen told of how his mastery of chess influenced his scholarly efforts.
“Marty often mentioned the fact that he had to abandon his tournament chess career to fully engage in the demands of academic psychology and psychiatry. His success in academia, which led to many professional accolades and research accomplishments that equally matched his tournament wins in chess, would at first glance appear to be an altogether separate branch of endeavor. However, when we reflect on his success to the highest level of these two extremely challenging fields, we must ask ourselves how Marty makes such expert decisions on such a regular basis. We have to wonder what secret talent Marty possessed that other remarkably gifted people may not possess.
“Having learned a few things about Marty’s childhood growing up in New York City, I began to understand one of Marty’s favorite manners of speech. This is a phrase he often uses when he makes any affirmative statement beginning with the word “should” and ending with the phrase “but maybe not” accompanied by a raising of his hand (usually his right hand) in various degrees of extension for emphasis.
“For example, in some of the academic understandings he challenged that caused the field to rethink its long-held assumptions:
- If schizophrenia is a chronic disease, it should be marked by continuous decline . . . but maybe not.
- Thought disorder in people with schizophrenia should be more severe than in people with acute mania . . . but maybe not.
- Thought disorder itself should derive from a disorder of language . . . but maybe not.
- The theory that dopamine is a principal causal agent in psychosis should follow from the efficacy of dopamine-blocking antipsychotics . . . but maybe not.
- The continuous use of antipsychotic medications should be the long-term standard of care for people with schizophrenia . . . but maybe not.
“I think what helps bring so many of Marty’s achievements is his uncanny ability to properly assess the range of possibilities flanking either side of a given event, a range that is much broader than most people would typically imagine, matched by the ability to assign an extraordinarily accurate probability distribution to those very possibilities. This talent is at work when he uses the word ‘should,’ which expresses his real-world probability assignment to the event in question, and the words ‘but maybe’ and ‘not’ which refer to the range of possibilities he has intuited that contextualize the event.”
Harrow published nearly 300 papers during his 60-year career and co-authored four books. In addition to the Chicago Followup Study, he conducted a naturalistic study of bipolar patients that punctured conventional wisdom about the merits of lithium. At the end of 4.5 years, 41% of the patients on lithium had a poor outcome, nearly half had been rehospitalized, and as a group they weren’t functioning any better than those not taking the drug. The Chicago Followup Study also included 81 patients who fell into a “manic depressive” classification, and once again, in this cohort, at the end of 15 years those who stopped taking antipsychotics fared much better than those who took such medication.
Harrow moved to the University of Illinois College of Medicine in 1990, and his colleagues there, in addition to celebrating his academic achievements, tell of how he was a “kind” and generous” mentor to junior faculty. One of his colleagues, Geri Fox, posted this memory of him after attending his funeral service:
“In his role on the department of psychiatry’s promotions and tenure committee, Marty went well above and beyond the job description. He took it upon himself to mentor his junior colleagues in various specialties in the department. He was generous with his time and wisdom. The first time I visited Marty in his office, I was astounded to see him surrounded by stacks and stacks of papers from floor to ceiling. He told me that this filing system worked very well for him, and that he knew where everything was. This reminded me of Albert Einstein saying, “If a cluttered desk is a sign of a cluttered mind, of what, then, is an empty desk a sign?” Not only did Marty give my CV a careful review and provided specific helpful advice early in my career, he later shared additional advice about various retirement savings vehicles that were available within the University. These are just a few examples of how he went out of his way to be helpful to his colleagues.”
Harrow is survived by his wife of 66 years, Helen, four children, and seven grandchildren. Chess master, scientist par excellence, mentor, and devoted family man . . . such was the life of Martin Harrow.
A Voice From the Grave
Harrow’s name will not soon altogether disappear from newly published articles in academic journals. There are now several papers “under review,” Rosen said, that she and Harrow had been working on prior to his death. She and her colleagues at the University of Illinois Chicago are also now seeking to secure funding for a seventh follow-up assessment of patients in the Chicago Followup Study, an effort that she and Harrow were working on prior to his death.
“Many times during his career, Marty was a voice in the wilderness as he followed the data and findings of the Chicago Followup study that often challenged the ‘academic’ understanding of schizophrenia and other psychotic disorders,” she said. “I can only imagine that when Marty was facing an opponent in chess or debating a point with an opponent in an academic setting, or countering an established theory with longitudinal data, which I witnessed on more than one occasion, his arguments and actions tended to become more insistent, persistent, and consistent, and in this [manner], his work literally changed the way the field thinks about schizophrenia and recovery, not to mention question the need for long-term antipsychotics as standard of care in schizophrenia. His research continues to promote thought and debate in the community to this day and will continue to do such for a long time to come.”
There are many in science and medicine who were seen as heretics during their lifetimes, only to have their work gain influence and acceptance after their deaths. Rosen’s words speak to that hopeful possibility.
***
Martin Harrow and Thomas Jobe presented a Mad in America Continuing Education Course on their Chicago Followup Study, which can be viewed here.
Bob,
I think that is a very nice tribute to Dr. Harrow, his work and what seems like a wonderful life. Thank you for writing it.
Whenever I see terms like, “psychotic patients”, “schizophrenia patients”, schizophrenic illness”, “people with schizophrenia”, I can’t help but cringe.
I hate those labels.
“If schizophrenia is a chronic disease, it should be marked by continuous decline . . . but maybe not.”
“The New Haven schizophrenia index (NHSI) is an attempt to operationalize the broad DSM-II concept of schizophrenia (Fenton et at., 1981).”
Schizophrenia is not a disease; it is a psychiatric disorder.
All psychiatric disorders are creations of the APA as defined by the APA in the DSM. They are nothing more than descriptive labels for moods, thoughts, behaviors, personalities, sleep/eating patterns, etc., etc., perceived by professionals as abnormal.
The descriptions are very accurate, therefore psychiatric disorders seem like actual medical diseases.
There are many medical conditions and substances, including medications, that can cause a person to experience what the APA considers to be schizophrenia.
The system profits immensely from the fact medical professionals label patients with idiopathic problems, like schizophrenia.
Webster’s defines the word idiopathic as “arising spontaneously or from an obscure or unknown cause.”
If medical professionals treating patients with symptoms of psychosis followed the BMJ’s guidelines for Best Practice Assessment of Psychosis, there would be less “schizophrenic patients”, less “treatment-resistant patients” and more former psychiatric patients, like me.
A uniform advocacy agenda advancing best practices is greatly needed.
https://psychoticdisorders.wordpress.com/bmj-best-practice-assessment-of-psychosis/
Report comment
Thanks for this article and especially the summary of studies in the Record of Research section. I haven’t looked through the various studies yet, but just having the summary you provided here is quite useful.
To Dr. Harrow — thanks so much for your work with Dr. Jobe. I have referenced your work from time to time in the last few years. May we keep the legacy of your work alive to bring about change that is so desperately needed.
Report comment
I am not meant to drop in as I did say I am leaving, on my lingering Hoover dam prophecy. However, something caught my notice.
I am not referring to any specific “you” as I make this next comment reply but I only want to humorously play with a marvellous commonly heard mainstream phrase that this comment has brought up. It is this…
“Bring about change that is desperately needed”.
Has anyone yet noticed that everyone is fighting everyone on our shared mud ball of a planet?
People with silk robes are calling people with velvet robes fascists. People with satin robes and calling people with rayon robes fascists. People with linen robes and calling people with corduroy robes fascists. Round and round goes the accusation that all others are controlling narcissistic fascists and chants grow louder that…
“change is desperately needed”.
Every human finds themselves in this war-like grip, in this time, where “neighbour is fighting neighbour” because “change is desperately needed”.
Once Upon A Time the world had a beautiful glorious jigsaw puzzle whose picture was full of lovely artistic meanings and shapes and colours. The eye could trail freely over any of the details found inspiring in that picture therein. But one day much of the jigsaw was covered by cloth and only one part of the jigsaw was allowed to be seen. It was not your part. It was not my part. It was not some other peoples part. Before long many people grew angry about that covering up of the whole jigsaw. The people then smashed up the jigsaw’s wholeness and grabbed the single piece of the puzzle that they themselves found was “most desperately needed”. But soon all the people began quarrelling as to whose jigsaw puzzle piece was REALLY the MOST IMPORTANT piece. Each person began slandering all the other people’s puzzle pieces by saying those pieces were OFFENSIVE or UNTRUE or DANGEROUS. Until nobody could bear to fit their jigsaw puzzle piece next to any other jigsaw puzzle piece. Each piece felt like THE ANSWER to each person. THE ANSWER to how the mud ball planet SHOULD BE. Things got ugly and soon bodies began to mount up as people with other jigsaw puzzle pieces were annihilated for having a “wrong” bit of a picture, a bit too different from THE BEST BIT. One day there were nuclear warheads pointing at children who clutched different bits of jigsaw puzzle. Laws were passed where everyone on the planet would have to throw away their jigsaw puzzle piece and their children’s jigsaw puzzle piece in order to accept that ONLY ONE jigsaw puzzle piece could BE a bit LIKE THE WHOLE PICTURE or the BE a bit LIKE WHOLE ANSWER to “the change desperately needed”.
All the people had to get used to only looking at the tiny single jigsaw puzzle piece, perhaps it depicted a fragment of an industrial chimney, or a part of of bridge, or a bit of a misty scene, or an oven. “Is this now life?” cried all the multitudinous people. And they wailed “Is everyone a now deemed to be a fascist for wanting their own puzzle piece scene?”.
How can the whole jigsaw ever fit together again, groove locking to curve locking to edge locking to roundness?
WHAT “change” is so desperately needed that the end of the WHOLE jigsaw puzzle comes about? Is not the wooden breaking apart, demise of that “wholeness”, formed from billions of unique “different” puzzle scenes, a demise that becomes the worst “change” that could ever befall humanity?
These are very important times humanity is going through. There is a need to treasure your own piece of jigsaw puzzle, your own “answer” about what “changes are desperately needed”, a need to love YOUR puzzle piece exclusively…But all things in nature involve BALANCE…YOU need to nourish yourself and love your own puzzle piece or scene but also you need to bear in mind the world that nourishes you. That world is made up of billions of NOT YOU. Billions of completely different pieces of the whole picture.
All of the fighting going on at present is not being seen FOR WHAT IT IS. Few see the golden opportunity for a global aerial perspective this time offers. Instead everyone is caught up in comparing each others jigsaw puzzle piece in a foolish race to establish which piece is THE TRUE PIECE and the ONLY bit worth dying for, which really means the ONLY bit worth killing everyone different for.
Time will tell…that you cannot INSIST that all eight billion uniquely different people on the mud ball planet MUST all obey ONLY deifying your single puzzle piece. How are you going to INSIST? More fighting, fighting, fighting? Until there is not even a mud ball planet left upon which to showcase a piece of jigsaw?
The jigsaw sort of IS the planet. The jigsaw is the entirety of creation. When it all explodes to smithereens, chunks of atomized planet all shooting off in deep space, what use to you will be the single little jigsaw piece puzzle ANSWER that indents grooves in the grip of your dying palm?
Report comment
I like your title, Bob, and since “There are many in science and medicine who were seen as heretics during their lifetimes, only to have their work gain influence and acceptance after their deaths.” Let’s maintain our hope that this will be true of Harrow & Jobe’s honest research some day.
My condolences to his family and loved ones, and I am personally very grateful for Harrow & Jobe’s work.
Report comment
There can be no “Galileo of modern psychiatry.” Galileo was a scientist.
A more appropriate analogy might be to a prominent alchemist.
Report comment
Maybe more like the guy who pointed out the Emperor was, in fact, completely naked.
Report comment
I just wanted to point out something more. One of the problems with “in group” brainwashing or herd like behavior, such as with the field of psychiatry, is that it subtly impacts even those who argue with them. It’s like battered women’s syndrome.
You start arguing with them over the facts. However, you are still accepting one premise, which is: if all they say is true, that sicker patients are the ones staying on the anti-psychotics, they are still terrible drugs with terrible side effects, and “you know, I think you are capable of doing better and coming up with a better treatment than that ANYWAY.”
What nobody is arguing about is that, EVEN IF everything they are saying is true, they have the wrong defeatist attitude, and this reminds me of how Obama had his supporters chant “yes we can.” Are psychiatrists even trying to be like that?
But I know how group thinks are. If you immerse yourself in a group, even as a devil’s advocate, it’s still possible — unconsciously — to develop some of their more defeatest group thinks, without fully realizing it. Actually, my mother would often fight against that type of thinking in her dealings with other people, and I’d see her do that and turn out to be right in the end, so that makes me programmed to try to see outside the box too.
I just know that I’ve done a number of things in the countryside in the white mountains of New Hampshire to get over PTSD, brain injury, and all sorts of other stuff. And I’m insightful about my brain. Maybe people labeled as Schizophrenics could do what I’ve been doing. And perhaps in a social context as with the soteria project. They walked WITH THEM, didn’t they? I think the schizophrenia issue is tied somehow to malfunctioning of parts of the brain used in the fight-flight response, and walking through the woods outdoors in nature probably will “reset” it somehow. People hallucinate if left long enough in sensory deprivation chambers. Maybe modern society IS different enough from nature so it’s like a sensory deprivation chamber to schizophrenics. Maybe modern building materials are bad. In terms of what light rays or frequencies they systematically block, and for millions of years we evolved in environments where all frequencies of light were blocked pretty evenly, anytime we were inside or outdoors.
Anyway. Bottom line. I just think of Obama’s supporters who chanted “yes we can.” Anti-psychotics are terrible. But EVEN IF THEY HAD WORKED, psychiatry should have looked for others solutions anyway.
Psychiatry’s WORST OFFENSE is that they refused to look for alternatives EVEN BELIEVING anti-psychotics worked against symptoms. And then they try to force detractors to accept the premise that, if anti-psychotics genuinely work against symptoms, we should stick with them and not try anything better. And bogging down the conversation that way.
And what’s their excuse? “Oh no, we can’t. It’s impossible.” Well, guess what? Human beings invented the cell phone. Computers. All sorts of amazing technological stuff. All psychiatrists should have taken the position, on anti-psychotics, that “they may work, but even if they work, they are so bad that we need to find a better alternative and fast.”
We have mass incarceration of how many black men, and what did they do that was anywhere near as harmful as that negative defeatest attitude? We should not under-estimate the sheer amount of damage that can be done to society merely through a pessimistic negative defeatest attitude like that. And someone should say that to psychiatrists. “You have a defeatest attitude, and you know what? How about we call THAT a mental health condition in its own right, and how about we say this makes you a danger to yourself or others?”
And, I note, it’s important to argue with psychiatrists about the facts, definitely. But it’s also important to rise above those petty arguments and just tell them: “you know what, I don’t care about those details, you need to find something better than anti-psychotics anyway, or you’re worthless. And if you aren’t even. trying, then there’s something very wrong with you.”
I just note, also, I think of the sickest schizophrenia patients staying on anti-psychotics for decades, and I just feel so sorry for them, so sad for them. Because I know the damage being done them and I also know, they could be helped, and nobody is trying to help them. I really do feel sorry for them and, indeed, I feel hurt to think about it and I have to deliberately avoid thinking about it too intensely, in order to protect myself from feeling a certain sense of deep sad regret over “what might have been” for so many people, what their lives could have been.
Maybe the worst thing about psychiatry is how they have brainwashed themselves into being completely devoid of that type of compassion or empathy, and have gotten caught up with greed instead. And they don’t know how bad they are because they all got brainwashed, little by little, as a group.
Is that kind of compassion I feel a “salt of the earth” value and they think they are important people who have evolved above it?
You know what? Although I have tons of problems with Christianity which is terribly corrupt, we are completely missing, now, the part about morals. And that is a really bad problem. And, yes, Christianity became corrupt and there are many reasons to want to throw out much of it. Oh, and when I mean morals, I’m not talking about sexual puritanism but, instead, about the kind of thing regarding compassion for other human beings.
Actually, the sexual puritanism part of Christianity is part of its anti-compassion. As, after all, humans are sexual beings, and puritanism also tries to force us to repress that positive side of humans interacting with each other sexually. But, that same kind of repression is also, in some ways and sometimes — not all the time — a form of lack of empathy too. Which I am going to say is IMMORAL. And when I talk about morals, I’m talking about something other than the super ascetic and stringent “Christian morals” stereotype.
I think now of the principle of Karma, what goes around comes around and what you put out in the world eventually comes back to you, ten fold. I think that should happen to the psychiatric community, and many others who have gone down similar wrong paths. This is not forgiveness, notice. Actually, that’s another problem with Christianity as its developed. Where forgiveness has been substituted with the notion of being an enabler for evil — where you have an excuse for being a coward and can say, instead, that you are “nice” and want to go easy on people who are doing wrong, out of “compassion.”
Do we need to “forgive” psychiatrists who destroy others’ lives? Sure, you forgive them — in your own mind — all the while doing everything you can to remove their abilities to harm other people. And that may well involve sometimes not being nice and sometimes not saying only lovely and nice words.
Report comment
“He followed the DATA and FINDINGS of the Chicago Followup study that often challenged the ‘academic’ understanding of schizophrenia”.
If he was following DATA and FINDINGS he was being academic. If he was following DATA and FINDINGS was he letting PEOPLE with PERSONAL EXPERIENCE of SCHIZOPHRENIA SPEAK for THEMSELVES? To truly get away from academia there needs to be a move away from arguing WITHIN science about science’s scandals and instead a prioritizing of the SOVEREIGNTY of the PERSON’S LIVED EXPERIENCE. This means that some people diagnosed with schizophrenia may be believed when they say THEY FEEL that they do NOT have that condition and some people diagnosed with schizophrenia may be believed when they say that THEY FEEL they DO have that condition. FREE CHOICE to believe as you do believe gets railroaded by scientific academia, and railroaded by the ACADEMIC arguers about scientific academia. You do not need a sheild and lance of DATA or FINDINGS to listen to peoples LIVED EXPERIENCE. If you are coming at people with a once removed suspicion that their OWN EXPERIENCE cannot be trusted and believed emphatically then you give them no voice but the voice that you think SCIENCE, whether old science or argued new science, says they should have.
I am in complete agreement that poison will always be a source of additional illness. I am in agreement, having myself years of LIVED EXPERIENCE of being on medication, that antipsychotics are vile. I hope no antipsychotics pass the lips of any more people. But my hope is only MY hope. It may not be what someone “different” from me wants as THEIR free choice. I hope to end the global production of alcohol. It destroys lives and especially the lives of children. Antipsychotics seem to me to be as bad as alcohol at wrecking lives.
But I doubt that I will EVER say that I believe MY SCHIZOPHRENIA is not that but is something else. I do not care how much DATA or FINDINGS a NON SCHIZOPHRENIA sufferer passes my way. DATA is not a more FOOLPROOF descriptive of MY PERSONAL HELL.
I am more than capable of describing what troubles me first and foremost by myself in any way I deem suitable to my choice of description.
I am not saying this any of this with annoyance but merely a desire to clarify my own perspective.
It seems to me that there is a hurry in the world at present to answer old scientific bombast with declarations of fraud on old science’s part, a blanket assumption that absolutely everything that was ever gathered by way of LIVED EXPERIENCE within old science’s searching must be now refuted as sham. The phenomenon of voices, hallucinations, delusions, are being, it seems to me, reappropriated and made over as being perfectly “normal”, caused perhaps by enduring enough trying circumstances. For some people voices, hallucinations, delusions may very well be THEIR normal. For others such intense torment, of a level few could withstand without suiciding, is a level of suffering that is NOT THEIR normal at all. I reserve the basic human right to call my “not normal for me” precisely SCHIZOPHRENIA. This does not mean I need a psychiatrist or want horrendous medications or treatment. If tomorrow I call my LIVED EXPERIENCE “jungle vine malaise”, or the following week I call it “Tibetan singing bowl vibration ailment”, or next month “trauma”, or next year “evil psychiatrist hypnosis”, then these preferences about how I define what ails me are also under the auspices of my free choice. I can do without yet more and more DATA or FINDINGS seeming to attempt to muffle MY OWN creative definition of what FEELS “not normal” FOR ME.
The world, it seems to me, kind of is ironically missing this opportunity to put ALL science and academia SECONDARY to each unique individual’s FREE CHOICE to follow old science or new science or no science at all. There is prevallent elsewhere these days online a counter attacking impetus to battle old science by using its same sublime, detached, cold steely logical verbal weapons, ones that old science invented, to arrive at CONSENSUS truth. But this battle just swaps one tyrannous CONSENSUS for another one. The bane of humanity is its CONSENSUS CERTAINTY. It becomes…
“I know you even more than you know you”.
I would say that on a transcendental and existential level, where the nature of the fabric of reality, at subatomic particle sizes, is itself “UNKNOWABLE” through the electron microscope, THERE IS NO CONSENSUS “TRUTH”. What in God’s name do people ever mean by the concept of absolute truth? Proof and more proof and more proof is often sought to arrive at “truth”. To which the LIVED EXPERIENCE of the odd or wildly unique individual is dis-proved and denounced and ridiculed.
Each human perceives reality “differently”. A shaman perceives the stars and clock time, that reality, “radically differently” from Western Europeans. There are many deviations from CONSENSUS “TRUTH” that offer abundant harmless free choices to believe whatever accords with each individual’s own LIVED EXPERIENCE.
When one person’s lived experience is used to silence or dismiss another person’s lived experience, perhaps by using religion or politics or science in an effort to establish “consensus opinion” all the stars and all the time come with an instruction manual. A new “this is how you should think” quasi DSM to replace the old “this is how you should think” DSM.
Some people, and I am NOT referring to MIA articles here, just other venues online, seem to want to rub out schizophrenia as way of mocking old science’s reverence of that diagnosis, but in doing so they might minimize or dismiss or rub out some of the authentic LIVED EXPERIENCE of the people who REALLY DO suffer hideous voices, hallucinations, delusions and so on. Mocking old science in a specifically data amassing CONSENSUS “TRUTH” weilding way, which is another academic science way, runs the risk of mocking the crippled.
There seems now in the world an almost evangelical keenness to tell the crippled to take up their bed and walk. I have said it before…
“The ill have a right to FEEL ill”.
I am very glad this man was a HERETIC. I also am a HERETIC. Any community will find BALANCE by including many different and sometimes opposing HERETICS. The moment a community thinks it has its consensus opinion all worked out, as your man found out in old psychiatry, is the moment a community closes to freedom of choice.
When we need data “first” to prioritize establishing the voices of the ill, we are not listening at all, we have left old science only to enter back into it via the enticements of its academic revolving door.
But just to end on a confusing note…why I support the right of this article to be aired is because the decision to align one’s belief to DATA and FINDINGS and academic science…IS ALSO a WONDERFUL FREE CHOICE.
Report comment
I just note, in a comment above which is now under moderation, I point out how I think schizophrenics should try doing the outdoor exercise and mountain climbing that i am doing to help my ptsd and brain injuries. And I’m insightful about my brain and I just know or feel this would help schizophrenics. Of course, I’m not schizophrenic myself so I guess I can’t say I know for sure. But I’m probably right about it.
Though, of course, you know what? Maybe I’m not fully right about it, or I’m only right about it for some people but not others. But what if the social environment and culture of the mental health field were such, so that everyone who was passionate and enthusiastic about me and had creative ideas like I have, about “what could be” or “what might be true” were welcomed and others responded to them not by shunning them but by getting excited about it too and volunteering their own ideas?
Guess what? Even if I don’t have the answer. Or don’t have the full answer, if the culture were the type that would welcome my way of thinking and open minded enthusiasm and passion, enormous progress would be made, one way or another.
By the way, did you know, I have been investigating some of my photographs and trying to analyze what I’m doing mathematically with them, and they show I have both this amazingly precise memory but also out-of-this-world visual processing skills, making me something of a savant.
I discovered that I had this gift with schizophrenics — well, only three of them, — where I would touch them and they told me I’d made their voices go away.
I don’t like divulging it because it sounds kind of weird. But, that’s what they said I did, and I assume they were not lying. I think my visual skills as shown in certain mathematical precision I have in the way I frame the photographs I take may somehow exploit quantum mechanics in the brain somehow or may have something to do with how quantum mechanics manifests itself in the brain. And my visual processing skills would make me very anti-schizophrenic somehow.
Or, no, maybe it’s like a part of one’s brain evolved to harness quantum mechanics, but it needs certain sensory stimuli from nature in order to develop such skills. Deprive the brain of such sensory stimuli and it will try to learn anyway and learn wrong.
Actually, I also have a gift in music too, as you can see here.
https://www.youtube.com/watch?v=sS2QU2yIm2Y
Study me enough, and it’s not so far fetched.
Maybe it was something about the rhythm with which I moved when I touched them. On the head. That did something. A bit like the Mozart effect.
Anyway, I think schizophrenia has something to do with quantum mechanics in the brain. And maybe tied to a brain skill that is actually very useful to us, but only if its developed right.
Report comment
Excuse me if I have read your comments as being pointed at my comments. Your comments may well be for general discussion. I do apologize if that is the case. But from my paranoid schizophrenic reading you seem in a hurry to fix my paranoid schizophrenia. That is very caring of you. I have no doubt your motives come from a considerate place within.
However, I have been in a few hospice settings or at the bedside of the terminally dying and it caused me to wonder at my own hurry to fix the dying of their dying. I believe my own motive for being a “fixer” of their suffering was tangled up in my own need to ease my own suffering instead, my suffering feeling that THERE IS NOTHING I CAN DO.
Humans are not comfortable with thinking that sometimes there is nothing they can DO about life or death or nature. It brings anxiety to feel the paralysis of POWERLESSNESS.
A victim will always cause in an observer a moment of the experience of awful awful awful POWERLESSNESS to DO a magical CURE. The observer may then goad the victim to NOT BE A VICTIM, just so that the observer can feel EMPOWERED again.
An offering may come from the observer, perhaps a gift, or a stock positive affirmation phrase, or a magical new pharmicological medicine, or an operation, or a bear hug, or a best seller self healing book, or a series of athletic workouts, or a year long membership to a political party that says all victims are made victims by political oppression, or a cd of meditations to scenic visualizations, or catchy tunes that give uplifting vibes, or homemade nourishing life changing soup, or the name of a top notch therapist, a family therapist, a Jungian therapist, a rational therapist, a seaweed therapist, a door slamming therapist, a nervous therapist, on and on and on come offers to fix the victim.
Meanwhile the victim understands all about POWERLESSNESS since they have to get into bed with it every hour of the day. They have to get real with abject helplessness. As the dying do. The lonely lonely dying, who know there is no fix but death itself.
Most mature schizophrenics know that THERE IS NOTHING anyone can offer or DO. Which is why when someone says that much, it comes as something of a relief. It is always a huge relief to have a compatriate in the POWERLESSNESS. It makes life less lonely to have someone there to commiserate that yes there is NOTHING can be DONE…this becomes an all embracing holding. Hopelessness is horrible but acceptance is not horrible. There is a fine line between these states. I have had experience of being told to hurry up and DO something about my suffering, my powerlessness, my victimhood, my dying of schizophrenia. This sometimes became a form of victimizing the victim for enduring their torment or trying to just accept it, accepting there is NOTHING can be DONE. The victim gets blamed for the HOPELESSNESS of their predicament, as if they can CURE it by THINKING properly. Suddenly their suffering is due to “wrong thinking” or a “bad perspective”. This is not that different from days of yore when religious priests would tell people with epilepsy to stop thinking in sinful ways of thinking. The offers come as curative salvations. But who is the fixing really curing? I say all this because psychiatry has turned this offering cures into a full time production line. In doing so it has often not helped the victims of hellish hallucinations and delusions and voices to try to move into the gentleness of acceptance, and find peace there.
Nature, as you are wonderfully aware, is wonderfully accepting of whatever state we are in. This acceptingness becomes “a kind of transient lovely cure” for an hour or a day or a week. I walk often in nature and I do often feel revived by the way nature does not try to “rub out” my POWERLESSNESS but holds me most tenderly in it and unites me with all the other rather accepting and POWERLESS mortal creatures within nature. I feel companionship there, by every tree and bird and flower, befriended in my hopelessness, and this befriending BECOMES a kind of hope. A hope that despite my inability to “get rid of” my schizophrenic torment I am sort of not all ALONE in my pain and POWERLESSNESS. Nature finds a way to BE with me, BE with me as victim, rather than DO lots of fixing stuff to me.
Healing can be a bully. Psychiatry has discovered this a little late in the day. It became a society wide manner of “getting rid of” victims’ POWERLESSNESS by DOING lots of sciency things to victims to stop them being uncomfortable locuses of grief and dying and anxiety for society. Society hates confronting helplessness even less than helpless individuals do. So society hygenically tidies away the helplessly wailing birthing mothers and the helplessly sobbing lonely dying. As if its offensive and ungrateful towards professionals and their tidy offers if a victim remains unhelpable. If being a genuine victim marks you as offensive and ungrateful you probably begin to long for the peace of death.
Please do not misconstrue me here. The very human impulse to ease another person’s suffering is itself utterly natural and good. It comes first and foremost from love. It is just that through wobbly empathy this impulse can also come from a wish to stop one’s own anxious suffering from having to find ways of mending the victim. This swapping from attending to the victim’s suffering and then attending to one’s own suffering from helplessness to get the victim all smiling again can burden the victim with a message that their helplessness is an inconvenient truth.
Love will always come as gifts and trinkets and cd’s of nice music and shawls and bowls of soup and great ideas for how to miraculously heal fast and encouragements to get out into nature. Love is love and love is good.
I listen to anyone who comes out with an offer of what might bannish my schizophrenia. Sometimes fellow schizophrenics come out with the best notions of what to DO, such as place a blue thread in a small box and wear it whilst sleeping or do drumming on saucepans and lids. All very shamanic, but mostly fellow schizophrenics just BE with me. We just BE. It is so very soothing.
You spoke of how psychiatrists keep give give giving antipsychotics. I know only from my own experience that the suffering involved in constantly having hallucinations made me often DEMAND antipsychotic cures. EVEN after finding out that they shorten life spans. On a bad day life feels like it is going to end in a day IF nothing is DONE to ease suffering immediately. There are schizophrenics who have rather mild or even pleasant hallucinations but there are many who live with severe schizophrenia with hourly torture. Yes, the pills make it much worse, in my own experience, but I know that there IS a placebo resurrection that lasts a month or two upon imbibing a NEW HOPEFUL PILL. That placebo upliftment can give just enough stamina to help a victim of schizophrenia not suicide. They pop them pills and go back to psychiatrists for a follow up appointment and near kiss the ground the psychiatrist walks on for “saving” them with that “offer”. Then three months later it becomes clear the pills did not work, and so a NEWER antipsychotic is desperately DEMANDED of by the victim. Another placebo lift occurs. Each placebo lift confering HOPE to the psychiatrist that they can DO something to ease the victim’s and their own anxious suffering. On and on it goes. Until psychiatrists look like healing bullies insisting on offers of pharma cures being tried…because several patients in a placebo false dawn loudly and emphatically say they feel improvements on them.
Report comment
Hmmmmm. Have you tried weight lifting to get your leg muscles very strong, and then done something like mountain climbing intensely, going up a whole mountain and I would think areas with lots of cold streams and running water that splashes off rocks have the biggest psychoactive effect.
See, there is walking through nature gently. Then — well, when large leg muscles are exercised a lot from mountain climbing, say, the muscles produce chemicals that do have an impact on your brain.
I would say that, rather than a calm walk through nature, an intense walk or climb that exhausts your whole body and your brain — where, once you’re done, you go home and go straight to bed and are so exhausted that you end up spending not only the rest of the day in bed but the whole following day in bed too, that’s how much you have to rest.
That kind of really intense mountain climb has effects on the brain comparable, I would say, to electric shock therapy. To make it more intense, you can sometimes go do it like interval training. Run up an especially steep part as fast as you can, then rest, then run up again.
Actually, I have or had a neurological pain syndrome, and mountain climbing did help it a lot. But, one thing I noticed was, when the pain syndrome was still much worse than it is now, let’s say I had pain in one part of my body that just wasn’t going away. Doing an extra long extra intense mountain climb would completely wipe that pain away. Non-intense nature walks wouldn’t do a thing. But, here’s the thing, schizophrenia is similar to a pain syndrome.
I suspect the super intense mountain climb might help. Actually, it not only exhausts the brain but impacts how the brain prioritizes brain activity. Because the brain does have energy conservation issues. Actually, it makes sense that exhausting oneself by walking really intensely in a mountain climb like that might reprogram the brain into stopping the hallucinations or whatever.
Because you are providing the brain with something of a real live external challenge it needs to overcome, that way.
Report comment
Have I tried this? Have I tried that?
If I say I live near a mountain that I regularly go up someone might say it is maybe not a high enough mountain. If I say I have done ten massive house moves in the span of fifteen years, physical excercise that absolutely decked me for weeks and caused me sleep in oblivion for days someone might say I really need to do twenty big house moves to get the proper level of excercise that would bannish my demons. Perhaps I ought to be sent down a coal pit or put to work in a quarry to “cure” me of my schizophrenia. And maybe if that don’t work then someone can call me lazy for not shovelling rocks fast enough or not scaling mountains often enough. Perhaps I could wear pyjamas while I process gravel in a quarry. And if voices continue to pipe up unwelcomely then I could be told it is ALL MY FAULT for not being a GOOD cripple, the sort who TAKES UP THY BED and walks up the lofty peak.
I say all this with humour my friend. I appreciate that you are giving a kind and generous offer. You are motivated to heal. There is nothing wrong with what you, or anyone else, advocates as a best bet for how to cease suffering. The more ideas we bring the table the better. But each idea may help one schizophenic but leave another unchanged. Does that mean that the unchanged one is deliberately refusing to be fixed? Blaming the ill for remaining stubbornly ill is a risk inherent in ANY healing offer. We do not blame the heart attack victim for having a horrible coronary arrest EVEN IF it is quite clear the jaunt up a mountain might have brought them a better view in which to sit and devour their MacDonalds. We do not blame the horribly suffering cancer patient for not taking their free radical vitamins often enough. Mental torment has always been easy for the onlooker to blame on the sufferer of such torment. Healing offers can play a part in entrenching the myth of the perperually fixed human, and the myth of the insolent lazy healing-refuser.
I am not at all saying your very good idea of mountain climbing is not great. It is a wonderful idea. What I do know from experience though is that when on antipsychotics a person typically cannot move their limbs even when they long to. Muscle rigidity IS A THING for that population, as is heart failure, as is obesity that is caused NOT be over eating but by the way pills kill the metabolism, even upon excercise. It is not that easy to just don a pair of shorts and running shoes when dying of the effects of antipsychotics. If the general public thought that all it took to master schizophrenia was a daily marathon, the effects of muscle rigidity and heart failure and obesity would soon ALSO be blamed on the poor schizophrenic who simply could not run a mile without dangerous breathlessness.
I am not saying your idea is not good, because it IS a good idea. BUT I know for my own experience that such extreme physical exertion DID NOTHING to stop my hallucinatons. It did not mend my schizophrenia. What it did do, and this is important, is it let me live a better set of visceral experiences than if I had just sat watching day time television all day. But nice experiences did not cure me, after twenty years of having had millions of very nice experiences.
You mention excercise as changing brain chemistry. I have seen schizophrenics run up stairs, hurl furniture around, fight with motor vehicles, physically throw themselves around for hours on end, all quite excercised and yet still they would say they feel horribly tormented by voices.
But yes…not ALL schizophrenics are identical. Many may be “improved” by treks in wild mountainous regions. I think it would be great if you maybe founded a way to take a group of schizophrenics on such wellness retreats. I love your idea. It has medicinal healing in it. For me it would not be MY cure. All schizophrenics are DIFFERENT.
Report comment
Removed for moderation.
Report comment
“outcomes for psychotic patients ”
And where’s the stolen meaning. Intellectuals of marxisms thinks that schis is sth to get rid of.
So people want help with complex situation, with whom normalcy can’t cope, because normal people can only be happy and count money. So intellectuals who steal meaning of the psyche in the name of mental helath care (materialism preservation and wellbeing of Wall Street), give you number to show how immoral you are compared to normal goyims who serves Wall Street, and have no psyche and one god – economy. Normal people do not have psychological identity. And victims of psychiatry are victims of their ease of being. Without the image of the psyche, people with psychological issues, are seen as simply stupid non workers who disturbe the virtual order of goyim.
They should be seen as people whose psychological work is far more advanced and more difficult than normal well being of those privilleged in empty materialism with zero psyche.
People who use diagnosis only to show that you can’t work miss the point.
I don’t want be rude, or maybe I should be, but the level in thinking of post Kraepelin psychiatry, including normal people, are on imbecile level.
People still think that when someone can’t work that means he is stupid or have sth wrong with the brain.
And psychiatry is using nominalism not to show the realism of the psyche behind sb ego. This is f semantics criminal war against reality of the psychological experience.
Schizophrenia as non working label shows only wrong attitude of goyim toward psyche. It is only useless materialiststic/marxistic point of view, without the realism of the psychological experience.
—————————————————————————————–
It is easy to use nominalism to hide tremendous and REAL states of the psyche WHICH MEANS MORE AND ARE MORE DIFFICULT THAN SIMPLE WORK for system AND FOR money, isn’t it?
—————————————————————————————————
If the psyche were perceived as REAL, nominalists/normal people would be perceived as ignorants or idiots.
————————————————————————————————-
“I show you my power to humiliate you.” Antichrist will do the same with people who are using nominalism to hide the REALITY of the psyche. People who are on the privilleged minus zero level of psychological experience still think that they have a right to punish or humiliate those in state which is far more difficult than whole their economical correct life on zero level of the psyche. But the reality of psychological experience was banned by monism/ marxism, so it is not real now.
And people think that psyche is some kind of toy for marxists in medical disguise.
Things done to psyche by corrupted intellectuals are unbearable to even think of. I have a problem with normal souless people. How could you sell your soul for the needs of Wall Street and corrupted Rockefeller’s medicine? It is too late, antichrist of technocracy is the continuation of Enlightenment era egoic souless psychopathy. And it is not because psyche, it is because privilleged normal intellectuals. They are the right hand of the beast.
———————————————————————————–
You, intelectualls of mental health preseravtion – you are talking about how to get rid of psychological roots all the time, and how to create antichrist materialistic reality in which psychological reality is only a form of verbal nominalism. This is not a system for humans, since the Enlightenment Era. There’s no point in living when our psychological roots are non existent.
Economy based on false money, is not worth of the difficult and complex life of banned psychological man.
—————————————————————————————–
The rhetorics of psychiatry is beyond any kind of propriety, and there is no connection between the realism of the psyche and actions of the psychiatry or normal people. Psychiatry is talking about the psyche without the psyche itself. It is as if theology talk about God without God.
———————————————————————————–
Life among “normals” is without any kind of worth. Because there is no. They are evil.
Report comment
https://www.youtube.com/live/1x0IOcFp94s?feature=share
Heartened I am that my comment got published. All credit to the impartiality in MIA!
Just back to share the above video. First part is a dull long intro so skip to around twelve minutes in to get to the journey proper. The narrator is speaking about the topic of Time. She explores the various other ways that humans throughout history have perceived the passages of Time.
It seems to me that CONSENSUS AGREEMENT about what exactly Time is is linked to “collaborative intention”. Something necessary to build “a civilization”. Agreement insists that you will show up at the factory at seven am in order to bind to the agreement that you will be rewarded with wages.
What is agreement? Many things. But one of these things is that you agree to suspend some of ALL of your FREE CHOICES in order to SERVE the choice of another, cooperatively. It becomes perhaps “in your best interests” to subordinate your initial free choices under the prioritizing of some “group consensus choice”. But this too can sometimes feel like it is exactly your free choice to do so. You align your own preferences with group preferences. You choose to participate in the tribe or civilization.
In society you may be asked to sign up to “consensus opinion” in myriad areas, or mark yourself as an unruly outsider, a heretic. Sometimes it is very easy to see how a group’s “consensus opinion” differs from your own worldview. Especially if that group is an extreme church or religious temple or army or coven or band of renegades or polital party not resonant with any of your “free choices”.
But there are other hard to define widespread “consensus opinions” that overarch small groups and encompass them in such a manner that the widespread agreed upon consensus “truth” gets taken for granted that it IS THE TRUTH. A truth that you signal yourself as mad in IF you say you do not believe in it.
The nature of what we each perceive as TIME itself becomes one such widespread group “consensus opinion”, or “group truth”, not because anyone “knows” exactly or “truthfully” what Time is, but because forming some sort of “mutual agreement” about Time’s mechanism and experience becomes useful to “group cooperation and trade”.
But very soon “that” TRUTH, that is established by “group think” about what Time is, has an impact on your “freedom of choice” to do with your “own” Time whatever you deem necessary to your needs and free choices. Consensus opinion can be the saviour of your free choice if you couple your choice to “group aims”, or it can be the death of your free choice.
We rarely realize quite how much we are influenced by “consensus truth”. It is not that this being influenced is “wrong”. Humans ARE social creatures. Agreements mean that your choice is not always going to be front and centre. Someone else’s choice, or a group’s choice, may take presidence. But this taking presidence IS NOT THE SAME THING AS THE TRUTH. We all “consensusly agree” on what Time is, so that our shops and cafes stay open when desired, and buses and trains show up when expected, and we may become servants of that version of understanding of what Time is, but we need not cloud out the vision of more ancient TRUTH about Time. We can expand Time’s meaning to encompass broader definitions that DO accomodate more of our “freedom of choice”.
I think this is some of what the narrator (Odell) was expressing, if I picked it up accurately.
If we live under the rather draconian modern “consensus opinion” of the notion of Time, as if that mere “opinion” speaks the TRUTH to each of us, a “clock time” ordering “agreed upon” REALITY to which we must all prostrate our very lives, then it behoves us to be aware of other kinds of “establishing” THE TRUTH that similarly might box us out of our optional more “choosy” and “different” ways of experiencing the “isness” of our mortal existence.
Consensus opinions in science have become for a rather long time THE TRUTH. A forest dwelling indigenous person may have their own opinion about what the sun and moon are. Interestingly they go unchallenged by science perhaps because their worldview is so very “different” it poses no threat. A Heretic on the other hand is in close proximity to the keepers of established TRUTH and gently rocks the boat with an air of authority borrowed from that establishment. This intimate connection, of being both still “within” the “group” yet having the audacity to quibble over received TRUTH is perceived as more “dangerous” than the very “different” far out forest dwellers notion of truth. Having your “free choice” to see life as you do see it, whilst still within a larger “group consensus” is threatening to that “agreement”. But if a group can tolerate having such “traitors” to its version of THE TRUTH it becomes itself A NEW FACILITATOR of the actual TRUTH that there is no such thing as ever completely arriving at THE TRUTH.
When that happens something else must ascend to take the place of the hunt for THE TRUTH.
Something like LOVE.
To be able to LOVE requires valuing curiosity and wonder and not assuming…
“I know you even more than you know yourself”.
(Ive given myself a headache with my own comment. Someone stop me rambling on and on. I need help….)
Report comment
….of course there is nothing “wrong” with wanting to be part of a stirring magnificent “group consensus opinion”. It confers to a person a sense of belonging and identity. Joining a “consensus opinion” can feel healing of a former wound of being refuted over sentiments held dear. It is gratifying to have cheerleaders. It is a boost to jaded morale to sign up to a big “consensus opinon creator” group such as in a religion or philosophy or politics or science. One begins to blur the exhilaration of healingly “belonging” with a sense of moral or intellectual “rightness” and this starts to seem identical to THE TRUTH. “Consensus opinion” brings order and this reduces personal insecurity about the unfathomable nature of wild truth.
I go on about the vital need to align with one’s own individual “freedom of choice”, to optimize wellbeing, but for many a bond of “belonging” to a collective of religious or scientists or political thinkers IS often their own fine “free choice”, for all of the above reasons and more. A “consensus opinion group” may peddle THE TRUTH as they see it and another “consensus opinion group” may rear up and try to dismantle that first group’s TRUTH with its own take on THE TRUTH.
There really is nothing “wrong” with choosing to be “belonging” to a “consensus opinion group”. Take your pick. There are millions of the damn things. We believe this. We believe that. It gets like finding cosy niches or depositories in which to more structurely nestle your existential madness. Having “an opinion” is a basic human right. And so is forging your “opinion” to a cluster of opinions within a “consensus opinion group” a basic human right. There is no harm in having “opinions”. They are NOT the same thing as outward acts of BULLYING, even though any bully may trumpet “opinions” as if these are the ONLY sacred TRUTH to which all must kneel.
One can grow very fond of a particular affirming “consensus opinion group” and start regarding the people within it as even more essential than family. When the group’s TRUTH seems to take a knock there can marshal a compulsion to DEFEND the “consensus opinion group” as if defending one’s very own self. But often these loyalties are subconscious or hidden and instead the DEFENDING is all about DEFENDING THE TRUTH.
In DEFENSE of THE TRUTH more stuff needs to get poked at externally as being NOT TRUE. Maybe inspirations in other “consensus opinion groups” such as the indigenous forest dweller’s notion of the sun and the moon. Everyone knows the sun and the moon are spherical cosmic bodies in space. Everyone knows the sun and moon are flat discs like the flat Earth. Everyone knows the sun and the moon were hung there by Great God. Everyone knows the sun and the moon are a leopard and a swan. Everyone knows the sun and the moon are a trick computer simulation made of pixels. Everyone knows the sun and the moon are Nasa carparks filmed fraudulently.
Everyone knows what lunar madness is. Everyone knows what lunar madness is not. Arguing arguing arguing over “consensus opinion”. It is okay to argue too. It is fantastic fun to. No harm in it. No harm in thinking yourself to be the ONLY person possessed of THE TRUTH. It can be thrilling and diverting. But none of this is the same thing as outward BULLYING. People often think that in order to get rid of bullying they have to wrestle with THE TRUTH. Drop the TRUTH to its knees until it says it is very sorry for getting it all wrong. This requires coming up with a fresh competing TRUTH, an even TRUER TRUTH, one that will obliterate other “free choices” of what to believe is TRUE, about the sun and the moon and lunar madness. But this deriding of other people’s “freedom of choice” to believe whatever they will can BECOME a form of BULLYING if it overshoots merely remaining a good natured arguement, about what we each individually feel we know of the sun and the moon and lunar madness.
Having a feeling, a thought, an opinion, even a consensus opinion, and even to uphold received science or bicker anew at it, as if being a denizen of what is absolutely true, are all lovely choices we can avail ourselves of.
It is outward behaviour of BULLYING that is the vast problem.
BULLYING often arises within a person when that person is not allowed to hold their own feeling, thought, opinion, consensus opinion, or true for them viewpoint, but rather is taught that what is within their psyche is dangerously unacceptable according to a dominant “consensus opinion group”. The person then cuts off from their deep awareness of their own “free choices” and instead becomes a benumbed ventriloquized spokesperson for certain dogma. MORE supposed TRUTH.
Regimes thrive not on feelings, thoughts, opinions, consensus opinions, all of which harm nobody, but on the chilling absence of the “freedom of choice” to, as an individual, fully enjoy the above.
I heard singer Lisa O’neill say in a video concert that apparently Nina Simone was once asked what she felt “freedom” would be like. Nina answered…
“No fear”.
Report comment
I heard Martin Harrow speak at an ICHR (International Consortium on Hallucinations Research) conference in Chicago in 2016.
I was impressed by how he asked the questions that challenged conventional ‘wisdom’ and pursued them with integrity and commitment in spite of resistance from ‘the profession’.
He mentioned this idea specifically – the fact that others in the profession vilified him for simply asking different questions and taking the exploration of answers seriously. And that this has affected the resources and money he had access to. What a shame.
Although it seems obvious ‘why’ this happened… in that there is AN explanation based on greed and power and money… I am still to this day mystified and surprised that ‘the profession’ of psychiatry is unable to rise above the politics and public mis-perceptions and demonstrate thought leadership in their own field.
That to me is what I saw in Martin Harrow that day at the conference – thought leadership.
He presented many perspectives… both questions and answers… and a rationale supported by data for the conclusions he had reached. He had made an effort to challenge his own confidence in those conclusions, thoughtfully . He understood how people might challenge his work and had clear responses to address them.
He was inspiring.
Report comment
It says a lot that Harrow, who before his research was very much a mainstream researcher, was vilified for simply presenting the results of his research. It goes to show the lack of integrity pervading the psychiatric industry, and the lengths to which their leaders will go to stifle any attempt to undermine their cash flow, regardless of the truth of the data presented.
Report comment
https://youtu.be/JvSHD_n3Lyg
…again a point of clarity.
I am NOT against a principle of anyone availing themselves of any “consensus opinion group” scientific body or field that purports to have the TRUTH of DATA. Although I do observe that with regard to “consensus opinion” on covid vaccines, and antipsychotics, that “yesterdays” watertight, irrefutable, scientific DATA had both of these seem like wonder cures for everyone so at risk. DATA can do this thing of conveying an impression that every human body is identical, as if mechanistically made in a factory. That supposed TRUTH can then be used by bad actors to rub out your own LIVED EXPERIENCE. Until it gets like there between what symptoms your body is coming out with and your soul’s ability to express your experience of the body you reside within there is a mistrust, a suspiscion that you are a LIAR about DATA DISCOVERED TRUTH about your very own one of a kind body.
Today’s TRUE vaccine or TRUE antipsychotic “scientific” weilded DATA becomes tomorrows revealled wishful thinking. This occurs ALL THE TIME in science. As your man Harrow seems to have noticed. The memo is “consensus opinion” and “science” are not always reliable forms of THE TRUTH about individuals or other things in life. NO “consensus opinion” IS!
That is because THE TRUTH is always a moving unfolding elaborartion that will never be completed. A blanket assumption that all bodies work the same way gets rapidly overtaken as thousands of bodies say they have been left damaged. Or a blanket assumption that nobody is healed by a twig or a leaf or crystal or a book is rapidly overtaken as thousands of bodies say the twig bannished all their bodily afflictions. “Consensus opinion”, because by its very nature of being given to groupthink and therefore blanket assumptions, is just not that great at listening to “individuals”. Who get called LIARS when they say they FEEL they really have “this” or LIARS when they say they FEEL really have “that”. Armed with lots of scientific research and data and truth of a blanketty order there is no room for individuals to express their LIVED EXPERIENCE as fed by THEIR OWN GUT FEELINGS….that TRUTH.
Old timey science has been called out on this by antipsychiatry. An antipsychiatry that damns old timey science for not pitying the truthful talker with their own LIVED EXPERIENCE that FEELS that old timey science has done them a mischeif. But rather than champion each individual’s basic human right to hold their own “opinion” of what is the matter with them…EVEN IF this aligns with an increasingly unpopular old timey science…antipsychiatry seems to do what old timey science does, which is box individuals into blanket assumption DATA, as if…yet again…that is THE TRUTH that is SUPERIOR to LIVED EXPERIENCE.
Both psychiatry and antipsychiatry battle each other in the bloody arena of science. Both are very fond of “consensus opinion” found in science.
Science may derive some of its DATA from batches of peoples LIVED EXPERIENCE but because it churns out yet more DATA this then gets used to hush unwelcome LIVED EXPERIENCE elsewhere from apparent LIARS that challenges this new notion of THE TRUTH.
DATA, SCIENCE, THE TRUTH, are all todays speculation until tomorrows fresh DATA, SCIENCE, THE TRUTH becomes deeper revealled, by an electron microscope or a James Web telescope. The search for THE TRUTH is merely a process of watching nature’s endless infinite strip tease. There is NO getting to the naked TRUTH. And to call any individual a LIAR for coming out with their preferred notion of what FEELS TRUE to them is to subordinate the individual BENEATH “consensus opinion” science, as if science is always going to be BETTER MOUTHPIECE for their own FEELINGS.
When a “consensus” religion, or politics, or science, not of my free choosing, purports to KNOW ME….infinitely MORE….than I KNOW ME….I am called a LIAR by these and deemed a threat and MY OWN LIVED EXPERIENCE is declared NOT TRUE and I am given NO VOICE.
Science alone won’t get us all to a beautifully respectful, tolerant, loving humanity.
The video clip is a marvellous gladiatorial scrum where a politician braves using DATA to joust former pharma/government DATA. Or uses new science to rebuke old timey science. He uses the LIVED EXPERIENCE of vaccine harmed to add to gathered new DATA. He uses new science to box clever with old science. As befits the constantly evolving scientific process. New DATA rubbishes the FOOLPROOF old DATA. This is all brilliant and necessary for science.
It is just that DATA is NOT ME.
It is fine to align with “consensus opinion” found in any religion or any politics or any science.
It just may not be ME. And if it is not ME does that rule out MY OWN LIVED EXPERIENCE as just the lying mutterings of a madwoman?
Does DATA now prove me an unreliable mouthpiece? Does DATA now prove me INSANE for my FEELING that I do suffer from unendurable schizophrenia?
My view…my own quirky LIVED EXPERIENCE might not be popular but when did “unpopular” mean “untrue”? Oh yes, since and for all ETERNITY. As the unpopular-in-psychiatry’s-circles Mr Harrow found to his cost.
Report comment
We certainly are not given eternity. It was pleasant to know more about the life of Martin Harrow. When reading someone’s text online I easily forget that there is a real person there somewhere who walks and talks and does his simple daily things. Until one day he is gone.
Non personal writings like studies make everyone look extremely cold. It is a sign of a great mind to be able to change opinion when there is enough evidence that everyone else is wrong. Truly a man like Galileo. I did not know how harsh and progress preventing the peer reviewing process can be. It should be for finding new knowledge together. They say as a phrase that the scientific method is not perfect, but still the best we have. But that peer reviewing process seems to be its’ Achilles heel with room for improvement.
In Donald Duck stories and drama movies if there was a scientific breakthrough every scientist would listen to that person and cover him with praises. If there are studies that contradict the physics standard model they end up not only in science magazines, but also in newspapers. But well, maybe a small 20 minutes presentation and getting an extremely important study published in a small magazine were still great moments for that chess master Harrow.
Time flies. World goes on and every greatness crumbles to dust as a temporal. When life is not easy, the view area narrows and shrinks only into personal suffering. Still, the final moments of almost any of us are likely even more horrible than that. Maybe Harrow would know. In his final moments did his history of research matter anything to him anymore? It scares me a lot. No matter how nicely we try to treat others and no matter how perfect and hard working we try to be, the rules of life are not kind ones.
Report comment
SYMPATHY is so powerfully healing that each person tends to keep it only for themselves, as if it is like a finite currency in a bank account that once spent on someone else will mean there is none left for number one. But actually the capacity to feel sympathy comes from the capicity to FEEL all kinds of emotions. If you can feel sympathy for someone you can “feel” enough “feelings” to include your own self in that wrap around hug.
Instead these days people sidestep giving sympathy by giving “healing”. This being the healer is attractive as it allows you to be “better than” the sick, more sorted, more together, more experienced, more full of answers, more of a shrewd judge of character, more reasonable, more enlightened, more of a puppet on a string. Healing can often become about “doing” a marvellous miracle technique “to” the “done to” idiot who knows nothing of how to alleviate their dire predicament. You can be a healer who never has to feel sympathy or never feel any feelings at all. Indeed, medicine is all about being a flinty emotionless doctor who martyrishly “gets rid of” their luxury of feelings in order to be a paragon of perfectly executed functions and practical actions. Medicine has that version of self sacrificing heroism. It is very stirring and attractive. And new healers have appropriated that rather grandiose “know all” way of helping the suffering. But chucking the sick a method or technique or yoga blanket or pill box or meditation cd…in other words…a “doing” thing…may not be “being” with the sick in a “feeling” way, a feeling of sympathy.
When my sister was dying of cancer I found myself sitting in a Spiritualist church. A medium came up to me at the end with a message from my late father. The message was about my dying sister. The medium said to me…
“Your father says give your sister a bit of sympathy at this time…a bit of sympathy”.
I recall blushing in anger. How dare anyone tell me that I did not care enough!
But the anger was an indication that the medium had touched the raw. I was guilty of “avoiding” feeling sympathy for my dying sister. I was guilty of feeling nothing at all. I was guilty of being completely numb. I could not take on any more sense of helplessness to DO something. I could not stop her dying. So I edited out that she even was dying. Instead I called myself brave for sending her lots of varieties of “healing”. I posted to her emolients and music and cheery cards and bestseller death defying books and rare teas and bells and crystals and names of celebrity healers who knew all. I would check up on her from afar to make sure she was dedicating herself to “the healings”, as if it would be HER FAULT if she skipped chapter ten or did not rinse the crystal in mountain dew first…exhausting exhausting exhausting offers of healing that were really my exhausting closings of doors of denial. A denial that she was more or less a goner. A denial of my own “feelings” in response to her “feelings”.
Children are brimful of sympathy. Children offer no healing. Children “be with” you in whatever sad state you find yourself in. Animals too do not offer healing but they definitely BE sympathetic. Children and animals are unafraid of “feeling” overwhelmed emotions like sadness. Grown up humans have been taught that emotional overwhelm means death.
My sister died surrounded by lots of objects of healing. Cold dead wellwishing objects.
It is a fate that awaits us all. The lonely place of being so mortally unhelpable that people cannot bear to face you.
Report comment
https://www.youtube.com/live/eDuy2Kx2HlI?feature=share
I doubt anyone will watch to the epicentre and finale of this video.
It is not a comfortable watch. But…is MIA for comfortable? Was Harrow for comfortable?
Ah, but there are no comfortable perspectives on this.
Over a decade ago I predicted the covid pandemic emanating from China. I have been here on record as predicting five meteor stikes and a massive global tsunami. I have predicted the rise of a totalitarian Regime. I have predicted the blowing up of the Hoover Dam. I have predicted a global change to the calander. I have predicted the ignoring of climate scientists who know that climate change is upon us and going to cause such weather chaos that it will be difficult to grow food. I have predicted heating in the southern part of the globe yet an Ice Age in the north. I have predicted the shut of ocean gyre streams called AMOC. I have predicted water wars. I have predicted gang warfare grinding ordinary living to a halt. I have predicted as a main prediction that the globe’s women are going to be openly castigated.
In a world where all eight billion unique individuals all have difference and all have different answers…There are NO easy answers. Looking for The Answer via Consensus Opinion is a distraction away from the uncomfortable reality that every human is different. Consensus Opinion moves humans away from the ancient adage “Live and let live”. Consensus Opinion becomes a war horse.
Violence cannot be a form of freedom. Violence can only be the antithesis of freedom.
Report comment
https://youtu.be/1dEYaCxR0RI
A soothing song for a sense of loss.
Did Harrow know such loss?
“Poor you. Battling every day to press upon the world your wondrous dream. Without your dream the world seems lost”.
These thoughts were within me today. I said them to myself after I had yet again spent a few hours telling my local friend of my dream for the world. But after a long while he communicated back to me that he already knew of all that I spoke of and he said he already had picked through the ins and outs of my dream and he said had already used bits of it for his dream but only as a polite favour, he implied that really he felt a bit indifferent to my dream.
I have been here before. Spending long whiles telling a single person of my dream. One person. Hours and hours of painstaking effort at elaboration. Only in the end to find them sloping away, flippantly.
Dreams are essential. We need our dreams. The dream of improving things is a very fine phenomenon in human experience. I am not negating the importance of dreams at all. They are vital to wellbeing. Human healing requires them.
Jesus did not stand with his back to the land of the multitudes whilst he gazed over a cliff towards the oceanic distant horizon, muttering his dream to only one shell on the shelly shore. He appealed to an audience. Humans are ever wont to self-actualize. Humans also like to appeal to an audience. They have a need to endlessly make an impression from the moment they wake up until the moment that they collapse into a pit of unrefreshing slumber. To not create a ripple of a thrill about a dream has the human bowed in despondency, as if to not make an impact on multitudes is a sign of abject failure. The dream must be fussed over by many or the dream dies, or so it seems. And so countless people have a feverish need like an urgent thrumming heartbeat in their chest to self-actualize every hour of the day by declaring the importance of their dream to everyone, even to thousands. Everything else takes second place, nourishment, rest, joy. The dream almost becomes a nightmarish burden to carry and sell. It becomes a relief to set it down, into the listening ears of those with seemingly rapt attention. Except nobody is listening. Nobody wants the dream. They give it a fair hearing, interrupted with their nitpicky criticism, but after an airy sigh of boredom they decline it. Away they go, deafly. As deaf as a shell on a beach that cannot even decipher the whisper of the wind. It comes as a sense of blushing foolishness to any budding activist to have spent all day speaking of a treasured dream to perhaps “only” the one shell that this does not equate to making an impression on the world. Why is the planet not yet being saved by your dream?
So I heard an inner voice say this to me…
Were you facing the wrong way? Should you be looking around for the crowd? Far better to speak your dream to an audience of only real shells on the beach. Far better to make no difference to them at all, and make no difference to the wind, and make no difference to the sun and the moon. For why strive to make a difference to what in nature is already perfect? Why want to “change” one shell, or see the seizing of one solitary shell as not quite activism enough? Does the whole carpet of the seashore, of billions of deaf shells, not seem quite lovely as it is? And is the multitude not also like a shelly shore, of jumbled diverse dreamers? What exactly are you trying to change?
If you want to self-actualize do not fret that you waste your precious time in scattering your dream to that which will not listen. Perhaps be relieved nobody is listening. For why want to alter what is already beautiful…the one deaf shell, or many shells?
By knowing that a dream is often best when it changes nothing, since all is as it is, you allow everything to stay what it is and what it wants to be…just as true love seeks to change nothing of the beloved…
and in this way rather than preaching your dream…
you become the dream.
Report comment
I continue to be impressed by (and admire) your pioneering and robust work – fabulous. You opened my eyes in 2002 –- I had already weaned long term sufferers from psychotic symptoms off their meds, on the general medical grounds that the fewer pills the better – and it had worked.
It still amazes me that though one of the leading UK journals, Psychosocial Medicine, did publish the punishing graph you repeat – this still had zero impact – what a travesty.
What I would like to add is that my researches lead me to suppose that mental illhealth is where your ‘intent’ gets mislead. It is strictly analogous to leg disease, where your legs won’t do what you intend them to – put the organ right, and carry on with your life as you wish it to be.
‘Intent’ however is even more fishy than ‘schizophrenia’. But it is vital. And what these dreadful drugs do is weaken it – my motto is – empowering intent detoxifies psychoses – an even bigger mountain to climb – but so what?, if it’s right, then it will emerge.
Thank you for your splendid persistence – may we see the fruition of all your sterling work, sooner rather than later . . . . .
Thanx
Bob Johnson Monday, 10 April 2023
Report comment