
Suicide rates decreased steadily from the mid-eighties until the new millennium in the USA and, on average, in Organisation for Economic Cooperation and Development (OECD) countries.1 In Europe, suicide rates decreased until around 2007 in most countries.2 Parallel to this drop of suicides, prescriptions of SSRI’s, the new generations of “antidepressants,” gradually increased. This led to numerous publications arguing that the negative correlations between antidepressant prescription rates and suicide rates was evidence that antidepressants are likely helpful in reducing suicide because they can alleviate symptoms of depression, one of the major risk factor for suicide.
Authors of these papers often had financial or other ties to the pharmaceutical industry (e.g., Ulrich Hegerl, Göran Isacsson, John Mann, Zoltan Rihmer).
In 2004, a kind of shock wave hit mainstream psychiatry when the FDA released the black box warning about prescribing antidepressants to children and youth. Not long after, Robert Gibbons and others published a now widely cited paper, based on data from 2003 to 2005, reporting that the black-box warning led to a reduction in the prescribing of antidepressants which was associated with an increase of suicides among young people.3 However, although the article was published in the high-ranked, peer-reviewed American Journal of Psychiatry, the statistical analysis and the related conclusions by Gibbons were quickly shown to be in error; there simply was no increase of suicides associated with the decrease of antidepressant prescriptions (see Jureidini, 20074 and Stone, 20145; see also Robert Whitaker’s report).
From 2000 onwards, suicide rates in the USA started to rise again (among youth around 2007). In most countries in Europe, suicide rates stopped declining or even increased again starting around 2007. However, antidepressant prescription rates steadily increased from the mid-eighties until today. As a result, the association between increased antidepressant rates and reduced suicide rates has faded with each passing year. Even worse for mainstream psychiatry, if you look at the past 10 years, antidepressant rates are associated with increased suicide rates.
Yet, as this has occurred, there has been, in our opinion, a strange silence. There has been a lack of research updates on the trend of increases in suicide rates as prescriptions of antidepressants have risen. And what about research reports on the long-term outcomes of the FDA black box warnings? Two papers pointed out that suicide rates did not increase as a result of the black box warnings in the United States and in Canada (Rhodes, Skinner, McFaull, & Katz, 20136 and Stone, 2014), but these papers were also “silenced” in psychiatry, since they were much less cited (9 and 36 times, respectively) than the Gibbons et al. paper that was cited 569 times (citation-frequency assessed via Google Scholar on August 12, 2018).
Other attempts to show that the FDA warnings led to increased suicides (Lu et al., 2014,7 cited 115 times) have also been debunked (see comments to the Lu article and Philip Hickey’s blog “Suicidal Behavior After FDA Warnings” here on MIA).
This silence about increasing suicide and antidepressant rates, and the silencing of studies that disproved harmful effects of the FDA warnings, was interrupted by at least two noteworthy incidents that demonstrate some deep-seated form of “evidence-resistance.” First, Robert Gibbons simply kept on claiming that the black box warning led to an increase of suicides (LA Times, Feb. 06/2012). Second, a research group around Zoltan Rihmer published a paper in 2015 about suicide trends and antidepressant prescription rates in Hungary, but only used data up until 2006, excluding the time span afterwards when suicide rates increased again (Otuyelu et al., 20158). This way, they of course could prove that increased antidepressant prescriptions came along with reduced suicide rates. No word about the restricted time frame or the increase of suicides in recent years in the limitation section of the paper. They even claimed that their results were an indirect proof of the harms of the FDA warnings (of course citing the debunked 2007 Gibbons et al. paper). They said that, since there was no related warning in Hungary, antidepressant prescriptions kept on rising in young people whereas suicides kept on falling. Otuyelu also cited another paper that “proved” the harms of the black box warning (Katz et al., 20089), despite opposing evidence available at that time (Rhodes et al., 2013).
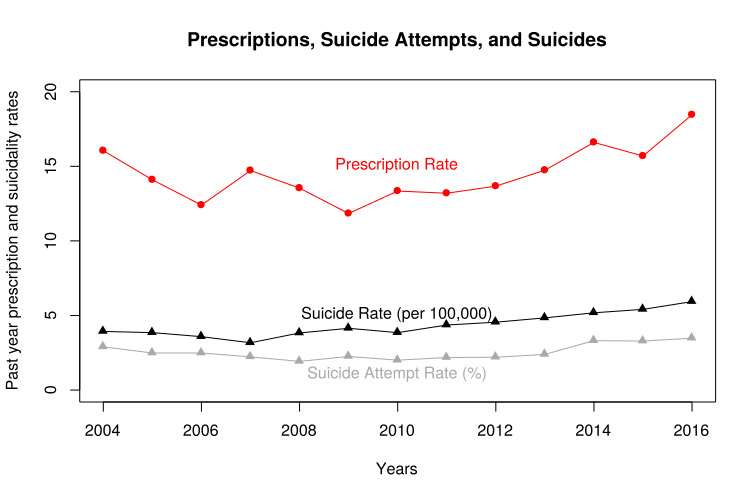
All of this is the background to our recent research on this topic. Recently, when we became aware of a newly published paper in the Journal of the American Academy of Child & Adolescent Psychiatry that analyzed trends of suicidality and mental health utilization of young people in the US, we wondered why the authors did not also include the results for prescriptions rates, despite that data being available.10 However, since the data was in the public domain, we were able to investigate the association of the suicide attempt rate with drug prescriptions for mood disorders (most likely antidepressants) among adolescents for the years 2004 to 2016.
Our analysis was rejected for publication by the Journal of the American Academy of Child & Adolescent Psychiatry and by JAMA Psychiatry. We were finally able to publish the paper in Epidemiology and Psychiatric Sciences (Plöderl & Hengartner, 201811).
Unfortunately, variables for years prior to 2004 could not be compared to later years, but with the available data we could still explore changes in the rate of prescriptions and suicide attempt rates following the FDA warning. The data is based on the annual National Survey on Drug Use and Health, a nationally representative survey among the US population. Past year major depression was assessed with a structured interview, and participants were asked if they had taken prescribed medication for their mood problems in the past year. We used this as a proxy for use of antidepressant medication. Prior suicide attempts were also assessed. This suicide attempt variable seemed to be a valid indicator of past year suicide risk, since it correlated high with the yearly suicide rates of the same age group (r = 0.75, p < .05).
Our analysis revealed that the rates of prescriptions, suicide attempts, and suicides decreased in the years following the FDA warning in 2004 but started to rise again in recent years. This is also confirmed by large and statistically significant correlation coefficients. Obviously, this contrasts with the assumption that the FDA warning led to an increase of suicidal behavior. On the contrary, it seems that reduced prescriptions lead to a reduction in suicidal behavior. It also indicates that the FDA warning had no enduring effect, since prescriptions to youth are on the rise again.
The usual interpretation by mainstream psychiatry is that our findings are an artefact: young people attempting suicide are more likely to receive mental health treatment, and this produces the found association. This explanation, however, does not fit with the fact that our findings apply both to adolescents with and without a major depression diagnosis. Persons without major depression are rarely suicidal; therefore, in these youths, the strong correlation between suicide attempts and antidepressant prescriptions is hardly explained by diagnosis alone. Also, antidepressant prescription rates increased before the suicide attempt rates did, as indicated via a statistical technique called changepoint-analysis.
Given the limitations of our study, it is important to look for replications. Indeed, our findings are similar to that of a study by Gupta, Gersing, Erkanli, & Burt (2016).12 By using patient data from psychiatric settings, Gupta et al. found that antidepressant prescriptions decreased from 79 to 60% from the period before the black box warning (2000-2003) relative to the period afterwards (2004-2009). The relative risk for suicidality decreased substantially by around 60-70% as well.
Of note, the relative risk for homicidality and other violent events was also reduced around 60-70%. These findings are exactly what would be predicted by the outcomes of randomized controlled clinical trials. In these trials, young people using antidepressants had higher rates of both suicidality and aggression, compared to those taking placebo.
With our study results, as with all such correlational data, it must be mentioned that causality cannot be inferred, and there are other strong arguments regarding why such data must be interpreted with caution. However, as stated above, our findings are in line with those from randomized controlled trials, where young people taking antidepressants indeed had higher rates of suicide attempts and other forms of suicidality (Healy, Le Noury, & Jureidini, 2018;13 Sharma et al., 2016;14 Stone et al., 200915). Put together, these data strongly suggest that antidepressants can cause suicides and aggressive behavior.
Disturbingly, our study and others reveal that the black box warning is now ignored in many countries, since antidepressant prescription rates for children and youth are on the rise again (Bachmann et al., 2016;16 Otuyelu et al., 2015). This increase is happening despite increasing certainty that antidepressants are rather ineffective and most likely cause suicidal behavior in young people.
It seems that the current strategy in mainstream psychiatry to deal with the problematic evidence base is to recommend fluoxetine, because it was reported as being the most effective drug with no increase of suicidality (Brent, Gibbons, Wilkinson, & Dubicka, 2018;17 Cipriani et al., 201618). Again, problems with these studies and the excess of suicidal events under fluoxetine in the trials continue to be ignored. As with other reports critical of antidepressant prescriptions, these inconvenient findings are not properly acknowledged. As a result, mainstream psychiatry will continue to claim that antidepressants effectively reduce suicide risk, despite compelling evidence to the contrary.














Thank you for this informative article Dr. Ploderl and Dr. Hengartner.
When it comes to Pharma Psychiatry there is a lot of ignoring research that doesn’t support the popularly accepted theories. This is not the only branch of medicine/science where this occurs, but it may be the worst.
Report comment
Thank you so much Martin Plöderl & Michael P. Hengartner – this is superb!
And yet, will it make a scrap of difference? Mainstream Psychiatry’s refusal to accept the years of data on this goes well beyond “evidence-resistance.” To this day, lead psychiatrists use Gibbons et al to justify spreading out-and-out fiction to the media. For instance, in July 2017 Prof Carmine Pariante put out a statement that… “we know very well that every time an alarm reduces the rates of prescription for antidepressants, suicide rates increase, including in adolescent and young adults.”
Prof Pariante is fully supported and endorsed by the Royal College of Psychiatrists, and he is trusted by journalists because of his expert status and reputable credentials bestowed on him by the Science Media Centre. Last year I pursued a serious official complaint against the SMC about Pariante’s statement. Here’s what happened…
http://www.auntiepsychiatry.com/red.aspx?ha=smc
Report comment
Dr. Charlatan has written numerous scientific papers in support of the discipline of iridology. He is fully supported by the College of Iridologists where he earned his advanced degree. The journalists trust him because he is an expert in the field of Iridology and has many credentials and awards from the Center for Phrenologists, Iridologists, and Alchemists.
A little academic incest going on at this mutual admiration center? 😀
Report comment
Thank you for this interesting link. Prof. Pariante seems to be really a hard case of “evidence resistance”
Report comment
Prof Pariante is just trying to keep the plates in the air long enough to calm down the current furore and get to his next job.
The methods he uses could have come from an MBA Marketing course. If the case against you is overwhelming, pick small areas where you can claim a win. (a) So he picks one item out of the depression scale, and although that is riddled with publication bias, claims a win. This one doesn’t seem to fool anyone.
(b) If the response curve is bell shaped, then at the end of bell must be some people who respond. Apart from the obvious jokes, he ignores the placebo effect. This one has people scratching their heads long enough to move on to the next topic.
If , on the other hand, as in front of parliament, he is faced with a gullible audience, he goes flat out with “all the studies….working on the core of depression…no doubt about it….”.
Report comment
How can he be stopped? Any ideas?
Report comment
To be honest, he and others on the SMC will be hoisted on their own petards. For example, the statements they made via the SMC in February 2018 to try and mislead the public simply incriminate them in dishonesty.
“compelling evidence for efficacy” Glyn Lewis
“confirms that they are safe and effective” Carmine Pariante
“puts to bed the idea antidepressants don’t work” Prof Anthony Cleare
“confirms existing evidence that antidepressants do work” Prof Allan Young
“much more effective than placebo” Prof David Taylor
Not one of them would attempt to defend these statements and are probably regretting they made them.
Just a quick reminder, the effect size for Prosac in the meta-analysis to which they are referring was a clinically invisible 0.24, and all the UK’s first choice antidepressants fell below NICE’s minimum threshold of 0.30. I think they have a case to answer.
Report comment
To Everybody , I’m not certain how to definitely stop Prof Pariante but I think this should get him pissed off . Bear with me . Many people have seen this others have not. In 1975 the great comedian John Belushi did some comedy skits as a samurai warrior in very unusual occupations . His character was based on the performance of the great Japanese actor Toshiro Mifune in Yojimbo . For example do a search John Belushi Samurai delicatessen , and John Belushi Samurai dry cleaners .
Now with a little imagination any one who is able could create countless comedic skits of Samurai Anti-Psychiatry Shop . Anything ,like various neuro-toxic pills ,snake head staff logos , shock machines , DSM books ,etc associated with psychiatry could be dealt with by the Samurai shop owner as various people bring in their particular request and why , to have a psychiatric object cut into pieces by the Samurai anti-psychiatry shop owner , in very funny comedic skits. These could be lots of short films for YouTube or even a feature length movie . Maybe a real Japanese sword expert with a sense of humour could play the main character or anyone else. Maybe Auntie Psychiatry might also want to cartoon a whole new book with these skits . I do think film , the Skits on YouTube and/or elsewhere might take off and get millions of views. Anyone out there Feel free to use this idea for the purpose to at the very least help take psychiatry’s power away or even better , to help send psychiatry sooner into the dustbin of history. Who knows maybe a place in MIA could also be set aside for these filmed skits where those who wanted to could write and refine them together .
Report comment
Psychiatry is not based on reason. It appeals to people’s emotional needs for security, relief from guilt, chronic misery from life problems, and low self esteem…it DOES help all undiagnosed folks feel good about how “sane” they are. And it makes them feel safe because they can protect society from all the Evil SMI.
The answer? Ridicule shrinks. Make them into villains, buffoons or both. Online skits and ebook stories. Satirical/troll sites. Shrinks’ credibility is based on discrediting and demonizing others. Discredit and demonize them till they become laughing stocks and no one listens to their lies. Psych lies only have power if you believe in them. Like voodoo curses.
Report comment
Thank You , to the writers of this Blog.
Here’s the link to John Belushi samurai delicatessen as an example and continuation of my last comment .
https://vimeo.com/154855749
I also agree with Rachel777 ridicule shrinks !
Report comment
Long ago, in Michigan, a Gertrude Black, MD regularly used mega B1 when treating suicidal ideation on a schedule of a 500mg initial dose, plus 100mg every hour thereafter until the ideation faded (I’d also suspect a long-term maintenance follow up). Naturally, her patients never told their local shrinks (this was back in the days when doctors could go to jail for using vitamins in large doses in their practices).
Report comment
I’m low in magnesium, iron, B12, D3, and other stuff. I don’t know if this caused my depression and anxiety–I was always trying starvation diets as a teen because adults told me no one could ever love a fatty.
Of course the “meds” sapped my body of nutrients too. Years on neuroleptics have really sapped away my magnesium and other good things. Oddly enough, the psych folks banned vitamins. Those are bad for you. Lol.
Report comment
The psych folks banned you taking vitamins because nutrients are bad for them, not you. They’d have to learn new techniques, new approaches and that their attempted persecution of the late A. Hoffer, et. al. was riddled with ignorance. They’d also have to trust patient reports and become bereft of drug company perks like “conferences” at warm weather resorts during the winter because they didn’t prescribe enough of their “angel’s” drugs.
Report comment
I think this is an “epidemic of psychiary,” as Szasz put it. My guess is its rooted in the woes of late stage capitalism.
Report comment
A bunch of rich, powerful “doctors” afraid of becoming obsolete when the truth prevails. And a society of wooses who consider emotional pain not just intolerable but an aberration. Plus the shrinks can prevent mass shootings and suicide with their Psych Magic. They provide the sheep with a sense of security–unfounded though it is.
Ever read the play An Enemy of the People by Ibsen?
Report comment
i don’t think most people are -permitted- to have the same emotional range as in years, generations past. obey authority at school–or else! suffering is for losers! know your place! who, in this day and age, has time to cry? time to reflect? i mean…i do, which…oddly enough, is one of the “perks” of being a “mental patient” (under very limited circumstances…”play the hand you’re dealt,” basically…).
its also worth noting that psychiatry has been thoroughly deconstructed, debunked, the works. Mental Health, Inc. is not growing and taking over our schools, our homes, our minds because its “treatments” are effective or even all that tolerable…
society needs psychiatry, especially in an era in which inequality has grown internationally, the costs of any sort of education that -might- lead to job stability and upward mobility have sky rocketed, and religions have lost their hold over our spirits and souls…which might explain the incredible number of M.Divinity people in secular mental health, inc. and the booming industry that is “Christian counseling.”
This is…I believe the phrase is “disenchantment of the world,” what happens when modernization saps us of our humanity, one way or another.
Report comment
Yes psychiatry has been thoroughly debunked and discredited…but no one off this site seems to know that. Everyone I talk to believes in the chemical imbalance “metaphor” without any question because they saw it on a drug commercial. And TV wouldn’t lie.
Googling articles by the American Psychiatric Association is way too HARD man! And you gotta read them too. They use those real big words. Double plus ungood!
Idiocracy meets Brave New World with a little 1984 thrown in if you get out of line by thinking too much.
Report comment
“Idiocracy” omg Rachel, I love your wit!
That is exactly what we have right now, an idiocracy.
Report comment
Not my idea. There’s a movie by that name. 🙂
Report comment
Rachel exactly. To convert people away from the belief in psychiatry is EXACTLY like questioning people about their religious beliefs. Neither one can be proven, or proven to do no harm, and people DO know, they just don’t want to let go of what they have been taught. The people I talk to don’t believe in psychiatry, they just don’t want to admit it. It is difficult not to believe in a hell, when you have been told there is. And when one questions hell, one wonders what other aspects of the bible are not true……it is this that many people do not want to do, the examining of a system. But they do not with absolute faith believe, some do, but the majority of people simply don’t want to make a decision one way or another. Come on, psychiatry itself knows LOL
Report comment
I have experienced a reasonable facsimile of Hell between my ears.
Courtesy of the Church of Psychiatry.
Report comment
Yet another example of why people should no longer trust their medical professionals :
“Huge numbers still registered at practices have either died or moved away… but GPs receive £151 for each one despite a crackdown pledge”
http://www.dailymail.co.uk/news/article-6098431/Scandal-3-6million-NHS-ghost-patients.html
When a patient dies in the UK, the GP medical records should be returned to Primary Care Support England. Would hope people could check here, but I doubt you could trust that either:
https://pcse.england.nhs.uk/services/gp-records/accessing-medical-records/
Report comment
I had to go for my three month check up with my GP this week. She’s always trying to get me to take statins and have colonoscopies and get a cardiologist and I always tell her no to all of that. This week she added in something new. Are you depressed and do you want an antidepressant. I just sat there staring at her until she looked up from her computer and actually looked at me. Then I started laughing and said that antidepressants would be the very last thing I’d ever consent to take since they were the very thing that caused all of my problems and got me into the “hospital” in the first place! I told her it would be a cold day in hell before I took those devil’s tic tacks. I think my imagery was lost on her since she’s a Hindu but it made me feel better anyway. She and I have never talked about my “diagnosis” since she’s the third doctor I’ve had since going to the clinic. The first one knew about it but it’s never been mentioned since. But all of a sudden out pops the question, “Are you depressed and do you want antidepressants?” I laughed and told her to never ask me those questions again. Case closed.
Report comment
This week in Stat News – yet more calculated misinformation being circulated by eminent academics… how can they live with themselves?
“FDA’s continuing use of ‘black box’ for antidepressants ignores the harms of this warning”
https://www.statnews.com/2018/08/29/fda-antidepressants-black-box-warnings-harms/?utm_content=buffere9b87&utm_medium=social&utm_source=twitter&utm_campaign=twitter_organic
Report comment
Reminds me of a scene from a sit com.
“How do you sleep at night?”
“On piles of money with beautiful women.”
Report comment
Beautiful fake science from Stephen Soumerai (Professor of population medicine, Harvard).
He shows a 40% reduction in youth antidepressants in the 18 months following the first warning, in one US state, Tennessee, in 2003.
And connects it with an increase in youth suicides in the USA from 2004 to 2016. So, apples and pears, and at different times too. We clearly aren’t supposed to notice that 18 months in one state in 2003/4 is not the same as 12 years for the whole country.
It gets worse. His graph shows a 25% increase in youth suicides from from 2006 to 2012 in the US. In that period, for the US, antidepressant prescriptions in children and adolescents actually INCREASED by 25% (Christian J. Bachmann, 2016). Professor Soumerai, the increase in youth suicide you cite is correlated with MORE antidepressants, not less.
Report comment
@ConcernedCarer: “Beautiful fake science from Stephen Soumerai (Professor of population medicine, Harvard).”
They will stoop to anything to get that ‘black box’ warning removed.
“Professor Soumerai, the increase in youth suicide you cite is correlated with MORE antidepressants, not less.”
Here are his contact details to put this to him directly…
https://www.populationmedicine.org/node/227
Report comment
I believe suicide in the young has many causes. They are raised in a very hectic world, with high demands made on them, it is utmost unhealthy of an environment. From high demands of schools, parents, video games, instant messaging, socio-economic factors and the availability of psychiatry. I believe combined with the existing environment and resulting stress and how psychiatry makes the young/people in general believe that it, the stress is somehow abnormal. Psychiatry never names the ills of a society but rather tries to enforce people to tolerate it. When kids have stress to label that stress as a problem, condition, or disease, only creates more hopelessness. Psychiatry is the most useless and in fact harmful to a person’s sense of self. No one is ever told that it is okay to have “suicidal feelings”. No one is ever told that the words “I feel like killing myself”, are simply words that say, I don’t know how to cope. They are words that people often insert when they have no other words, when it gets so overwhelming. To medicate those feelings or words with pills that actually bring/cause the tension and body sensations, nervousness and anxiety on top of what was already there, will often bring a person to do exactly the thing they were not really planning to do. Then psychiatry hides behind the original distress as being the cause, not the fact it was exacerbated by their diagnosing and pills. We live in a stress inducing time and have psychiatry make those stressors into MI. They ensure that people will feel sick. Psychiatry is responsible, because they do not contribute ANYTHING at all to ever make people feel that their feelings are not an illness. I would rather risk my kid, than send them to a shrink, than have them buy the ideas and cocktails, because the risk of not sending them has better outcomes.
Report comment