

On July 11, the House Committee on Oversight and Reform held its first-ever hearing on childhood trauma, featuring emotional testimony from survivor witnesses, as well as a number of prominent public health experts and government officials. The hearing took place just a little over a month after the announcement of the Rise from Trauma Act, bipartisan, bicameral legislation that would fund increased services and supports for trauma-impacted children and families. (See previous MIA Report: “Bipartisan ‘RISE from Trauma Act’ Introduced to Address Childhood Trauma in America.”)
In his opening statement, Committee Chairman Rep. Elijah Cummings (D-MD-7) referred to the landmark 1997 Adverse Childhood Experiences (ACE) study, which found unaddressed childhood trauma to be linked to a number of leading causes of death in America, including heart disease, lung disease, substance use, and suicide.
Chairman Cummings added: “Sadly, I see this every day in my city of Baltimore, where far, far too many of our community’s children are suffering severe trauma, including witnessing violence, or losing parents to violence, incarceration, or substance use.”
While Rep. Cummings acknowledged the role of the Centers for Disease Control and Prevention (CDC) and other government agencies in responding to childhood trauma, he noted that “efforts at the federal level are still severely underfunded, and they do not provide the comprehensive, whole-child approach we need to combat this crisis.”
“As a nation, we have a significant economic incentive and, more importantly, a profound moral imperative to ensure that our children have the opportunity to thrive and succeed.”
— Rep. Elijah Cummings (D-MD-7), Chairman, House Committee on Oversight and Reform
Ranking Member Jim Jordan (R-OH-4) spoke on the intersection between childhood trauma and the devastating impacts of the opioid epidemic in his home state of Ohio, which has the 2nd highest overdose death rate in the country. Rep. Jordan said, “These overdoses are ripping apart families, and forcing children to cope with unspeakable grief.”
Rep. Cummings shared his own experience of being wrongly placed into special education as a child, and the impact it had on him. “This [childhood thing] is emotional for me,” he said.
The hearing opened with a witness panel of survivor-advocates, who shared moving testimony and recommendations for change. Each witness highlighted the central importance of relationships of dignity and connection in supporting them to move forward in the wake of traumatic events.
William Kellibrew, founder of the William Kellibrew Foundation, shared testimony describing the day he witnessed the murder of his mother and brother by his mother’s boyfriend, before being spared himself.
Kellibrew discussed “trying to forget” and the toll that it took on him, including a suicide attempt in the seventh grade. The turning point for Kellibrew came when he connected with a supportive, nonjudgmental therapist: “No adult had ever listened so intently to what I had to say. It was the beginning of my healing journey.”
He also shared about the pivotal and consistent role his grandmother played, as his primary caregiver and supporter, who was in attendance. Kellibrew ended his presentation by yielding his remaining time to honor her. She was met with a standing ovation by Members of Congress and hearing attendees.
“Families cannot be left to grapple with the aftermath of trauma.”
— William Kellibrew, director, the William Kellibrew Foundation

Creeanna Aviles-Rygg, survivor and activist with the parent advocacy group National Crittenton, shared her story, which highlighted the ways in which systems pathologize and criminalize the experiences of survivors. She detailed the experience of being sexually abused by her mother’s boyfriend, unable to tell her mother what was happening.
When Aviles-Rygg encountered the mental health system, her experiences were viewed solely as symptoms of “mental illness.” No one asked what had happened to her.
After years of cycling between the child welfare and juvenile justice systems, Aviles-Rygg found acceptance and connection at Florence Crittenton, a residential program for pregnant teens. “I was finally treated from the traumatic experiences I had survived,” she said. “I attended therapy sessions and learned that more than half the girls living there at the time were also survivors of sexual and/or violent crimes.”
She said, “Looking back, I feel as if I slipped through all of the cracks in the agencies that are designed to protect children from trauma.”
“I was labeled as a troubled youth, when really I just needed someone to recognize I was being hurt.”
— Creeanna Aviles-Rygg, survivor-activist, National Crittenton

Justin Miller, co-founder and deputy executive director of Objective Zero, an organization that provides peer to peer supports for vets struggling with thoughts of suicide, discussed the cumulative impact of childhood trauma and combat trauma. “After my traumatic childhood, I tried to stay numb and intoxicated all the time,” he said. “For years, I tried to stay distant to my two young kids. I had a short fuse with them. When they would cry, it would trigger old memories from war, and I would become angry.”
Miller related a story of calling the VA to disclose that he was suicidal. The VA’s response was to place him on hold and give him an appointment two days later. The turning point came for Miller when he connected with the “alternative, warrior-led, holistic” Save a Warrior (SAW) project. SAW exposed Miller to the ACEs research for the first time. “During SAW is when I realized I was repeating the cycle with my children, and then decided it was time to break that cycle,” he said.
“It is going to require a culture shift for us to see a difference. People need to quit feeling ashamed or embarrassed about their trauma. By not talking about our trauma, it gives that event power over you.”
— Justin Miller, co-founder and deputy executive director, Objective Zero

Heather Martin, executive director and co-founder of The Rebels Project, a nonprofit formed to support survivors of mass trauma, testified about her experience as a survivor of the 1999 Columbine High School shooting.
Martin described how difficult it was for her to transition from high school to college in the wake of the tragedy. She tearfully related a time when she tried to advocate for herself with a professor. “I still had to write my final English paper about school violence or fail the class — even after confessing that I had been at Columbine. I failed that class.” She eventually dropped out altogether.
Martin’s healing process began a decade after that horrific day. “I reconnected with people who knew what my struggles entailed. As a result of these renewed connections and acceptance I felt when returning for the anniversary, I went back to college.”
Today, as a high school English teacher, Martin uses her lived experience to support students who have survived trauma, noting in her testimony: “Schools need programs that teach children how to build resilience, how to use coping skills, and how to practice self-care.”
“Teachers, and really anybody in the education field, need to be educated on trauma-informed instruction, what that looks like, and what that means.”
— Heather Martin, executive director and co-founder, The Rebels Project

Rep. Ayanna Pressley (D-Mass), whose office partnered with Chairman Cummings’ to hold the hearing, said, “It is all interconnected. Violence begets violence, and trauma begets trauma. And so many families and communities like my own are passing along, unfortunately, the legacy of intergenerational trauma.”
She added, “In order for us to work on it, we have to first speak on it. But one of the things that I think stands in the way of our speaking on it is the stigma and the shame that survivors carry, when it is not your shame to carry.” Rep. Pressley expressed her gratitude to the survivor panel, adding: “I am sorry that you have to weaponize your pain in order for this ‘survivor tribe’ to be seen and to be heard.”
“It’s so important that this work be survivor-led.”
— Rep. Ayanna Pressley (D-Mass)

Following the survivor witness panel, which received an unusual standing ovation from the chamber, a second witness panel of public health experts and government officials convened.
Dr. Debra Houry, director of the National Center for Injury Prevention & Control, testified on behalf of the CDC. Trained as an emergency physician, Houry related a story about a toddler she once saw in the ER for fever and cough. While treating him for pneumonia, she said, “I almost missed the multiple rib fractures he had on his chest x-ray. It became clear he had suffered trauma over a long period of time.”
Houry said that the CDC is using data, such as the Behavioral Risk Factor Surveillance System (BRFSS), to prioritize prevention and response efforts for communities most impacted by trauma and ACEs. She referenced a number of promising public health programs and approaches, including the CDC’s Essentials for Childhood framework, which equips states and communities with tools and strategies to prevent child abuse and neglect.
“By focusing on prevention, and building the resilience of our communities, we can meet the immediate needs of those already affected, reduce the long-term effects of trauma, and prevent trauma.”
— Dr. Debra Houry, director, National Center for Injury Prevention Control, CDC
Dr. Christina Bethell provided testimony as director of the Child and Adolescent Health Measurement Initiative (CAMHI), and as a board member of the nonpartisan advocacy group, the Campaign for Trauma-Informed Policy and Practice (CTIPP). She added: “I am also a person with lived experience of the majority of childhood traumas mentioned in the ACEs Study.”
Bethell referred to the high prevalence of ACEs in the U.S. as a “synergistic epidemic.” She explained: “We can’t deal with what ails us unless we also deal with the long reach of trauma, and proactively promote relational health, emotional and stress regulation skills, and all of the factors essential to health and well being.”
She noted that systems too often “diagnose, medicate, and treat the illnesses that are often very predictable outpicturings of unhealed trauma, without any awareness of their origins, the biologic drivers… or the possibilities for healing.”
Bethell’s recommendations to the Committee included “immediate shifts in federal-supported programs and services that can perpetuate trauma unwittingly.” She called for building “a national ‘caring capacity’ that is trauma-informed.”
“The science requires a paradigm shift in how we think about child development, human health, social problems, and the skills and requirements for our own well-being, which we can learn.”
— Dr. Christina Bethell, director, the Child and Adolescent Health Measurement Initiative

Dr. Denese Shervington, Clinical Professor of Psychiatry at Tulane University School of Medicine, shared her lived experience as a survivor of Hurricane Katrina in 2005. “Some of those effects are still being felt by certain communities,” she said. “Today we are under threat of another flood, and I know that the people of New Orleans are really traumatized,” she added, referring to the impending advance of Hurricane Barry on New Orleans.
Shervington emphasized how important it is for the public to receive education about the impact of trauma. In her testimony, Shervington referred to In that Number, a New Orleans-based public awareness campaign which was designed to “change the negative perceptions of . . . youth suffering from trauma, and to advocate for psychological and restorative services rather than punitive juvenile justice responses.”
https://www.instagram.com/p/ByHIFRaF74s/?utm_source=ig_web_copy_link
As a result of the In that Number campaign, she notes, “local media began to frame the issue of youth violence with a landscape lens that presented a broader perspective of their lived lives — their personal traumas and community trauma.”
“I think about the need for us to inform our communities that trauma is not ‘normal.’ We can’t ‘keep it moving.’”
— Dr. Denese Shervington

James Henry, former deputy governor & chief of staff for Tennessee, discussed in his testimony how the experience of learning about ACEs permanently changed his worldview and approach to public policy. Reflecting on his own childhood, during which he was surrounded by a large and loving extended family, Henry said, “I realized for the first time, ‘Maybe you didn’t just ‘pull yourself up by the bootstraps.’ You had some help.’”
He detailed his efforts to get the Tennessee state legislature to approve recurring funding to address ACEs, including public relations work, as well as holding a statewide summit to educate policymakers about the human toll and economic impact of unaddressed ACEs. “We set out to make a difference,” he said. “We got the appropriations, we got people involved, we adopted. But we need Congress now to help us move forward with this.”
“Congress, we need your help.”
— James Henry, former deputy governor and chief of staff for Tennessee
Charles Patterson, health commissioner in Clark County, Ohio, was the final witness to testify, from a county that has been particularly ravaged by the opioid epidemic. He noted how teachers in the county are overwhelmed with the needs of traumatized children. “We’ve always thought that it was because Johnny was a bad kid, and now we’ve figured out it’s because Johnny’s living with stuff that most of us can’t even imagine.”
Patterson described a county review of drug deaths since 2015, in an effort to conduct a “root-cause analysis.” He said, “When you review a mother’s death, and then later on, you review the death of the son, and you wonder, could it have been ACEs? Could it have been the trauma that the child lived, with the mom going through drug abuse for many years, and them sitting at the kitchen table doing opioids together? It’s very sad when . . . we’ve got the data that shows us that we are seeing generation after generation.”

“Let’s make everyone provide trauma-informed care. Not everyone will see a doctor or clinician. We need everyone in the community to be able to begin to build the relationships. Because the relationships are key, and that’s where the healing can begin.”
— Charles Patterson, health commissioner, Clark County, Ohio
Following the second panel, Committee members made statements and asked questions of the witnesses for nearly two hours, on subjects ranging from racial and historical trauma, to gun violence, to poverty and homelessness, to the role of faith-based communities, to the Medicaid program.
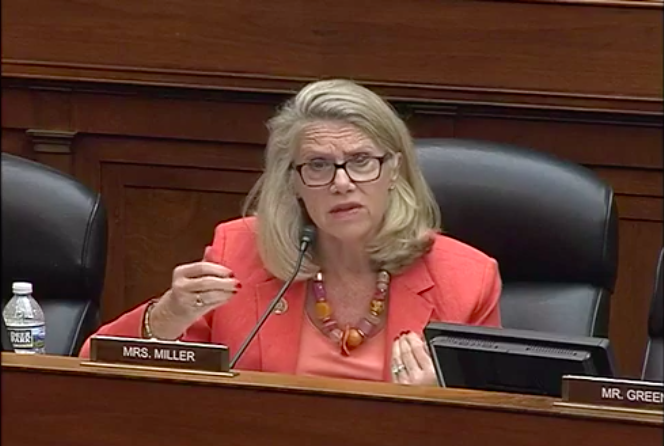
Members of the Committee shared emotional stories from their own districts about the impact of trauma. Representative Carol Miller (R-W.Va-3) shared that in her home state of West-Virginia, “ground zero” of the opioid epidemic, they are seeing “second and third generation effects.”
A recurring theme in the hearing was the need for the Federal government to coordinate a comprehensive, cross-sector response to addressing ACEs. In his testimony, Charles Patterson, the Clark County, Ohio health commissioner, said, “What we don’t need is the Department of Education saying ‘we need to do this,’ and law enforcement is going to do this, and the medical community is going to do something else. We need it to be a coordinated effort.”
Dr. Shervington agreed, noting: “It will be really helpful to communities when we have one message, almost one kind of science, about how we’re going to go ahead and heal.”
Rep. Debbie Wasserman Schultz (D-FL-23), referred back to Ms. Rygg’s testimony to highlight the failures of the U.S. juvenile justice system to identify and respond to trauma.
She added, “Why do we sanitize all of these terms? It’s hard to feel the same impact that her testimony had with the term ‘ACE.’ ACE is benign.”
Wasserman Schultz cited research finding that “half of justice-impacted girls have experienced five or more ACEs,” and that “ninety percent of youth in the juvenile justice system have at least two ACEs.”
She added that under the Trump Administration, the Office of Juvenile Justice and Delinquency Programs (OJJDP) rescinded guidance about trauma-informed reforms for girls in the juvenile justice system, and OJJDP Administrator Karen Harp said the agency is “too focused on therapeutic interventions” and has “questioned the validity of neuroscience regarding adolescent brain development science.”

“These are young people in our country that we are categorically failing.”
— Rep. Debbie Wasserman Schultz
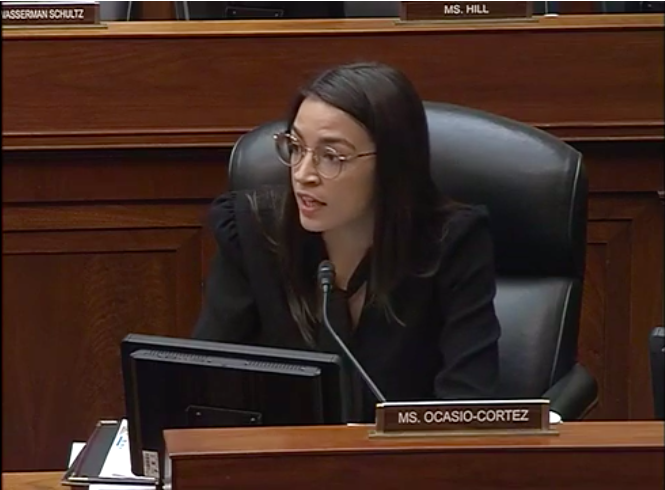
Rep. Alexandria Ocasio-Cortez (D-NY) took a moment to acknowledge the role of Reps. Cummings and Pressley in advancing the Congressional conversation, noting: “This is our first hearing on childhood trauma in the history of the Oversight Committee.”
Ocasio-Cortez asked Dr. Bethell to confirm that half of American children have had exposure to one or more ACEs, stating: “I think it’s important that we note for the record, and for all people, that childhood trauma . . . is a lifelong issue for people to live with and deal with. Which means at some point in this country, half of an entire generation will be dealing with trauma.”
“When I think about this on a macro level, we think about how intergenerational trauma is not just familial. It is cultural.” She added: “The health of our children is a reflection of the health of our nation. How we are going to have to deal with these traumas is a collective responsibility on the public policy across all of our issues.”
“This is a macro issue of national consequence.”
— Rep. Alexandria Ocasio-Cortez (D-NY)
Rep. Glenn Grothman (R-WI) asked questions about the connection between ACEs, suicide, and ‘mental illness.’ Dr. Houry from the CDC referred to a recent youth suicide investigation from Stark County, Ohio finding that “Among youth that had three or more ACEs, 30 percent of them disclosed suicidal ideation. Those who said they were using opioids plus had those ACEs, eighty percent disclosed suicidal ideation.”
Rep. Grothman asked about the percentage of American children who were currently on psychiatric medication. Dr. Bethell responded, “One of the movements we’d like to see is that before we medicate our kids and put numbers of foster kids in on Abilify, which generally can prevent them even engaging in school, first we need to assess and treat the trauma. There are so many needs, and opportunities to deal with the symptoms of mental health rather than just medicate them.”
“Suicide is not just about mental illness,” added Houry. “Often times it’s precipitated by a traumatic event — loss of a job, partnership issues, economic issues… which is why I think resiliency is so key.”
The discussion also focused on the role of social injustice in contributing to child and family trauma. Rep. Ayanna Pressley noted, “We need to be not only coordinated, but equitable” when it comes to addressing trauma. She asked Dr. Shervington, “When the root causes that often lead to trauma are so entrenched in our very infrastructure — discriminatory housing policies, health and racial disparities —how do we respond?”
Dr. Shervington said: “As public health practitioners, we have to advocate for those kind of policies that are going to look at those inequities and try to fix them. We can’t do them alone, and so we have to be in partnership with those in our communities. It has to be community-driven, how these inequities play out.”
Another theme that emerged was the need for locally-driven vs. one-size-fits-all approaches to prevent and address ACEs. Bethell said, “We need common element approaches and supports to implement them, with data, measurement, tools, and models, that then can be used by communities where they adapt and make it their own.” She added, “Unless we make it our own, nothing will change. This is relational and engagement-based.”
Several members of the Committee expressed interest in the Self-Healing Communities Model referenced by Bethell. Funded by the Robert Wood Johnson Foundation and operating in Washington state, the model seeks to “strengthen culture and community capacity by empowering communities to recognize their own ability to make change, and provide a sense of hope that what they do will make a difference.”
Bethell said, “Until the community is engaged in driving the change and working with systems that are receptive to their needs and ideas about what they need, I don’t think we’ll ever have a sustainable system.”
In an era of unprecedented rancor in Washington, the tone of the hearing was remarkably civil. In their opening statements, both Chairman Cummings and Ranking Member Jordan expressed their personal commitment to moving forward on trauma on a bipartisan basis.
“It was the most nonpartisan meeting that I’ve ever attended,” said Dan Press, whose firm provides pro bono lobbying services to the Campaign for Trauma-Informed Policy and Practice (CTIPP).
“I hope that the hearing helps lay the foundation for meaningful conversations about how we can best support our children who have been impacted by traumatic events.”
— Heather Martin, executive director and co-founder, The Rebels Project
During the upcoming August recess, grassroots trauma-informed community coalitions around the country are mobilizing to keep the momentum from the hearing going. Several groups are planning to hold roundtables and invite their representatives in Congress to learn more about the existing work happening in their communities.
Rep. Cummings is expected to introduce legislation in the coming months. “Rep. Cummings has expressed an intention not just to educate, but to come up with legislation,” Press said. “In his testimony, he talked about the need for a comprehensive approach. We’re hoping this legislation will offer a comprehensive approach to addressing trauma.”
****
MIA Reports are supported, in part, by a grant from the Open Society Foundations



For the love of all that is good in this world, and the hope for helping these kids, please don’t encourage the state to intervene in the lives of traumatized kids any more than they already do. As someone with firsthand experience of the state’s juvenile justice and child welfare agencies (and who has also heard plenty of firsthand experience from friends and colleagues), and knows the beatings, the neglect, the rape, the harassment, the drugs, and the threats of prison these organizations are all too often rife with, I can only say this is bad news. They talked the same “trauma-informed” language when I was a kid getting trauma-informed beatings, in the heart of the state’s trauma informed juvenile jail, and perved on by trauma-informed staff. Their depredations were written off as behaviors resulting the so-called Secondary Traumatic Stress they caught by being in proximity to us. Any response to childhood or adolescent trauma should not involve forcing the kid into a situation that makes them more vulnerable.
Report comment
I totally agree with Ayanna Pressley, “It’s so important that this work be survivor-led.” In other words, NOT led by the DSM believers (psychologists, psychiatrists, social workers, counselors, etc.), who’ve been profiteering off of covering up child abuse for over a century.
https://www.indybay.org/newsitems/2019/01/23/18820633.php?fbclid=IwAR2-cgZPcEvbz7yFqMuUwneIuaqGleGiOzackY4N2sPeVXolwmEga5iKxdo
https://www.madinamerica.com/2016/04/heal-for-life/
In part, because their DSM “bible” was designed as a child abuse covering up “bible.”
https://www.psychologytoday.com/us/blog/your-child-does-not-have-bipolar-disorder/201402/dsm-5-and-child-neglect-and-abuse-1
Since our DSM believers can’t bill to help child abuse survivors, they have spent decades misdiagnosing the child abuse survivors, and/or their concerned family members, when the child was VERY young when raped. Once the medical evidence of the abuse of my child was finally handed over, a psychiatrist thought the best way to help a healing child abuse survivor, who I got away from the child rapists over four years prior, was to drug him. Bye, bye lunatic psychiatrist!
Once my child largely healed, and went from “remedial reading” in first grade, after the abuse, to getting 100% on his state standardized tests in eighth grade. My family was attacked by an insanity spewing school social worker, who wanted to get her grubby little hands on my well behaved, intelligent, healing child. Off to boarding school instead, lunatic psycho social workers.
I know where I live there are absolutely NO trauma survivor groups run by survivors, only DSM believers. And since I was proactively attacked by “mental health” workers who wanted to profiteer off of covering up the abuse of my child, for a pastor, according to medical records. Obviously, I wouldn’t be able to attend a group for parents of child abuse survivors, and explain my story of the child rape covering up crimes of our “mental health” workers, if that group is led by a “mental health” worker.
https://www.amazon.com/Jesus-Culture-Wars-Reclaiming-Prayer/dp/1598868330
https://virtueonline.org/lutherans-elca-texas-catastrophe-coming-lesson-episcopalians
And my childhood religion, obviously, is filled with child rape cover uppers as well. I’ve learned recently that mothers of child abuse survivors, who are also widows, are absolutely not welcome in the ELCA churches. But the psychologists in those churches do want to steal everything we own, according to a BS “art manager” contract I was recently handed over. The Lutherans are apparently terrified of my “too truthful,” “insightful,” and “prophetic” artwork.
So you have to be cautious of having both the child rape covering up “mental health” workers involved in such trauma informed services, and the child rape covering up religions do not want to be involved either. My childhood religion wants to maintain their “dirty little secret of the two original educated professions” child rape profiteering “mental health” and “social services” systems.
“It’s so important that this work be survivor-led.” So true.
Report comment
With the right approach Genuine Recovery is not such a difficult thing!
Report comment
I think trauma informed understanding is critical, and I commend those who raise awareness on this so I thank the writer/activist for that. I am however deeply concerned about potential unintended consequences around this, and mean no disrespect to the writer/activist through expressing constructive concern. The writer/activist is not to blame for the abuse that occurs in these systems and our culture as a whole.
That being said, child welfare agencies employ abusive tactics under the guise of trauma informed care and set children and adolescents up for further abuse by the mental health system and therefore additional and compounded trauma. The abuse of the mental health system includes psychological/emotional, physical, and sexual violence. Trauma informed care is already being coopted and perverted by this system. For instance, psychological and emotional assault occurs through gaslighting, (ie: bogus trauma related diagnoses, and subsequent “trauma informed treatment”). Sexual abuse occurs through pathologizing or demonization of human sexuality (i.e.: pathologizing of sexual/romantic preferences and expression). I knew someone who’s “trauma therapist” told her that her bisexuality was simply a manifestation of childhood trauma because she was attracted to a woman 15 years older than her. Physical assault through the gratuitous use of physically injurious chemical substances. Many “trauma informed therapists” use these “treatments” in addition to attempting to resolve trauma without providing true informed consent.
Report comment
I should clarify that it is sexually abusive when a person is forced, coerced and/or manipulated into any unwanted sexual activity. For example, a person being manipulated into a different sexual orientation (unwanted sexual activity) under the guise of trauma informed care is something that I consider to fall under the umbrella of sexual violence.
Report comment
I have also worked with foster youth, and found that the “trauma brain” trainings, rather than increasing empathy as they ought to, for some people provide yet another way to say that “his brain is broken because he’s traumatized” and use it to justify more drugging and diagnosing. What is needed for traumatized people (which is pretty much all of us!) is empathy and kindness and honesty and human vulnerability. It doesn’t matter how many trainings are done – we need to impact the ethics of the people involved such that they start thinking about how they might accidentally be harming someone rather than assuming that everything they do is magically helpful.
Report comment
Leah, I would have liked to see more in-depth reporting on several areas that you only mentioned in padding but I think need much more light.
Do you or others know the history of past government congressional and White House conferences and hearings?
There used to be a fair number. This hearing was done by the Oversight Committee! What is wrong with this?
The Senate and White House Administration ain’t hearing nothin! And the press as well.
Second- one needs to look at every Republican member on committees such as these. Not because I am against the old Republican Party but now many Congress folks are funded by NRI and other not so benign entities. Rep. Jordan also has a history that should be explored as well in terms of possible knowledge of abuse.
A History of Florence Crittenton would be helpful for folks to see how not all agencies were always always awful,. I worked there part time and it was before chemicals were given Carte Blanche to children and adolescents in the system and the program had its strengths.
Report comment
All of this is interesting. Distressing and a bit hopeful at the same time. There was very little mention of sexual abuse in spite of Sandusky, Catholics, and epidemic sex trafficking, let alone rapes, long term childhood sexual abuse and incest. I agree that this absolutely needs to be survivor led or they will be wasting money, doing the same BS that’s always been done and leaving children and adults worse than they had been if this isn’t done right. I endured years of childhood sexual abuse plus several other “ACE’s” growing up. I had very few teachers take an interest in me and many treat me badly even though I did mostly well in school and was responsible. It was my fault I was being bullied because I “didn’t get along with others”. Many teachers basically bullied me as well. I was quiet and sullen, so I’m not sure how blamed me and became part of the bullying. I thought about suicide every single day. There were many years of hospitalizations beginning in my 20’s. I was yelled at by Drs who didn’t care why I was there. Including why being strip searched while suicidal was traumatic since nobody asked or cared. They literally left me on my own to cry for hours right after admitting me. Drs didn’t care that I was allergic to a previously tried psych med because it was the one they wanted to put me on. Or that I had an eating disorder and therefore didn’t want to be put on MAOI’s. One “doctor” said I didn’t want to be in them just so I could eat pizza with friends. Once I wasnt allowed to talk to my hospital social worker while there. This meant I was keep “hostage” an extra week while I used the pay phone to find a partial program, which was required for my release. A director wouldn’t let my medical Dr talk to me even though she had releases. Many therapists have NO idea what they are doing. Even when they know what I’ve been through it’s all “talk therapy” which only deals with coping with daily living. Without any real help, let alone looking at any underlying cause. I’ve always had to fight for myself in the system and they saw that as one of my problems – being non-compliant as opposed to advocating for myself even though I was so depressed I couldn’t even muster up enough feelings to do this with anger or attitude. A year ago I was transferred to a therapist after four years of asking to see her. She finally consented, but made no promises. She went drill sargent all over me at my first appt. Telling me (with much attitude) expectations, that she could only promise to see me once a month, etc. When she was done she got right in my face and half yelled, “Are you sure you still want to see me?” I smiled, looked her straight in the eye and said, “Absolutely”. I had no idea she was a trauma therapist. She saw me a month later and realized I seriously wanted to get better. We went from every other week to every week. I thank God that after almost four decades since the last abuse episode as a teen, I have a specialist who knows what she’s doing, cares very much, and has helped me tremendously even in such a short period of time! It’s going to take several years, but I now have hope. The only person I’ve been able to find who understands trauma is Diane Langberg PHD. ALL kinds of trauma due to working with abuse survivors, refugees, Rwandans, people affected by natural disasters, poverty, etc. She ought to be on any team working on these changes along with survivors leading the way. I pray for current and future generations that these people do everything they can to “get it right” and truly lead the way to making a difference as opposed to offering hope while doing nothing or even making things worse.
Report comment
Leah, good work. I’m glad somebody got to the bottom of the initial hearing. What interests me is that noone at AltCon19 knew of it, even a person on the Committee, nor did the go-to from Tennessee. We were like, “… WHY DIDN’T YOU TELL US ABOUT THIS EARLIER?!”
Why didn’t they?
I am keenly interested and committed to seeing P2P and Peer Workforce (CPS and Endorsements, 2019) be embedded into all/any forthcoming proposed legislation for TIC, Recovery in MH, SUD and Trauma.
I will be on calls as scheduled.
Thanks again.
Kindly,
Jen Padron, Ed.M, CPS
Report comment
Please see my expose article on the cyber school I worked at. Here is the link: https://www.madinamerica.com/2019/07/inside-online-charter-school-labeling-kids-disabled-for-profit/
All the kids I had worked with were traumatized due to bullying at their former schools. This was ignored by the behavior specialists across the board. One of the school personnel even suggested the families were “lying” about the past. I did not think so. Wow they really wanted to silence me.
Report comment