

On June 10, U.S. Senators Shelley Moore Capito (R-W. Va), Dick Durbin (D-Ill), Tammy Duckworth (D-Ill), and Lisa Murkowski (R-AK), together with U.S. Representatives Danny Davis (D-Ill.) and Mike Gallagher (R-Wis.), introduced the Resilience Investment, Support, and Expansion (RISE) From Trauma Act, legislation designed to “increase support for children who have been exposed to Adverse Childhood Experiences (ACEs) and trauma, such as witnessing violence, parental addiction, or abuse.”
The bicameral, bipartisan legislation, which has not yet been assigned a bill number, follows on the heels of a fifteen-month GAO (Government Accountability Office) investigation, with a subsequent report released in April 2019. The report does not make any recommendations, but discusses existing Federal initiatives to address trauma, and highlights key challenges facing systems in six states seeking to implement trauma-informed approaches. These include high staff turnover, lack of leadership support, lack of training for clinicians and workers, and inconsistent, insufficient funding sources.
“The weight of trauma, like exposure to violence or drug addiction, can cause emotional scars that follow a child for life. Without help, this can harm healthy development, disrupt school success, and fuel the cycle of violence and poverty.”
—Senator Dick Durbin (D-Ill), introducing the RISE from Trauma Act.
Expanding upon the GAO report, the RISE from Trauma Act is intended to increase support to the trauma-informed workforce across systems and settings, and to fund community coalitions to address the impact of trauma.
“Trauma-informed care” is not specifically defined in the legislation, but is referred to in ways that are consistent with the framework in the Substance Abuse and Mental Health Services Administration’s (SAMHSA) 2014 Concept and Guidance for a Trauma-Informed Approach document. The GAO report states that “Although trauma-informed frameworks may vary, they generally include interventions as well as a change in culture; thus if an agency or organization is taking a trauma-informed approach, it is incorporating knowledge of trauma and its effects into its policies, procedures, and practices.”
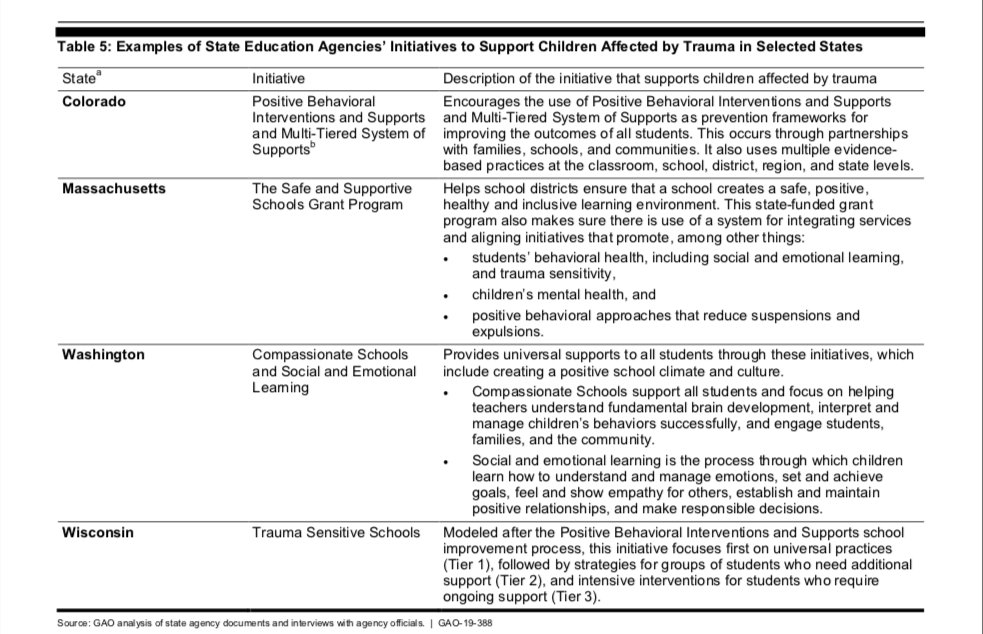
The RISE from Trauma Act includes $50 million in funding for a “mental health in schools” program. While the features of this program remain unclear, the GAO report describes efforts in six states to create trauma-sensitive schools by revamping school culture to be supportive of trauma-impacted students. And the legislation refers numerous times to section 7132(d) of the 2018 opioid legislation, the SUPPORT for Patients and Communities Act, which established a Task Force to identify best practices in supporting children and families who have experienced trauma. These best practices include social-emotional learning programs, parent-child programs, and other multi-generational approaches.
Other key provisions in the RISE from Trauma Act will:
- Authorize a $17 million increase in funding for the U.S. Department of Health & Human Services’ (HHS) National Child Traumatic Stress Network.
- Create a new HHS grant program to fund community-based coalitions to address trauma.
- Incentivize flexibility for local, state, and tribal entities to pool federal grants from multiple agencies to serve trauma-impacted children and families across programs and sectors.
- Strengthen the AmeriCorps program and several HRSA health profession training programs to prioritize recruitment and programming in communities that have experienced trauma.
- Direct the National Institutes of Health (NIH) to study and report on its trauma research agenda.
- Expand existing National Endowment for the Arts programs for projects that provide “trauma-informed arts opportunities and interventions.”
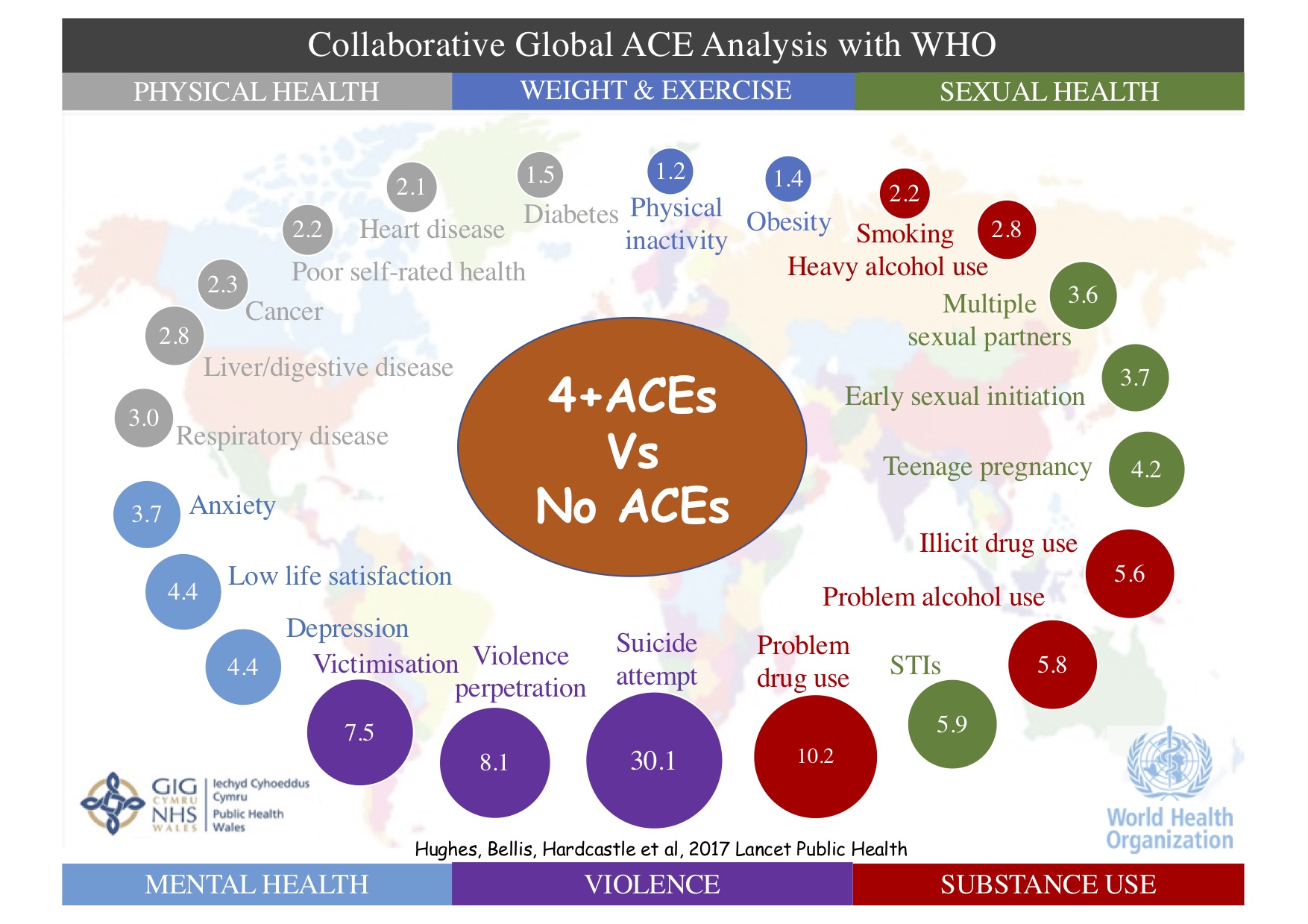
The RISE From Trauma Act was inspired, in part, by the findings of the landmark 1997 Adverse Childhood Experiences (ACE) Study. A collaboration between Kaiser Permanente and the CDC, the ACE Study surveyed 17,000 Californians regarding 10 categories of childhood adversity. The data revealed a “dose-response” relationship between the number of types of adversity and the risk of many physical health, mental health, and social outcomes into adulthood, such as addiction, mental health conditions, violent victimization, homelessness, suicide, and early mortality.
As recently noted in a Mad in America report by Joshua Kendall, “Adverse Childhood Experiences: When Will the Lessons of the ACE Study Inform Societal Care?,” in the over two decades since the ACE Study was first published, there has been an ongoing lack of political will to support the implementation of trauma-informed practices across systems and settings. Existing trauma-informed programs and initiatives have arisen largely at the state and local levels.
Yet advocacy efforts to raise attention to trauma on the Federal level have begun to gain significant traction and momentum in recent years. In 2016, the Campaign for Trauma-Informed Policy and Practice (CTIPP), a broad coalition of individuals and organizations, formed to advance ACEs science in policy at all levels of government and society.
In 2017, CTIPP developed and circulated a policy brief on the intersection between opioid addiction and traumatic experience, which heavily influenced conversations on the Hill. That same year, CTIPP successfully lobbied for the inclusion of trauma-informed provisions in H.R.6, the SUPPORT for Patients and Communities Act, opioid legislation signed into law by President Trump in October 2018.
Last year, CTIPP played an instrumental role in influencing members of Congress to form a bipartisan Trauma-Informed Care Caucus, with the mission to “increase awareness in Congress of Trauma-Informed Care (TIC), the science-based treatment framework used to address the root causes of major public health issues in the U.S.”
Dan Press, a Washington, D.C. attorney whose firm provides pro-bono lobbying on behalf of CTIPP, said: “Three years ago, when I first started lobbying on trauma, I’d mention it to Hill staffers, and just get a blank stare. Last year was the first year that there was legislation focusing on trauma. This year when you go out talking to offices, everybody gets it. You see Senators mentioning trauma in their prepared remarks. It’s now an issue that seems to have caught fire.”
The RISE from Trauma Act was introduced amidst a climate of ongoing public outcry caused by the Trump administration’s 2018 “zero-tolerance” policy separating refugee families seeking asylum at the U.S. border. The “zero-tolerance” policy was decried by a variety of groups, including the American Psychological Association (APA), highlighting the long-term traumatic impact on children and families, many of whom were already fleeing violent circumstances in their home countries.
Even after the Trump administration issued an executive order revoking the policy in June of 2018, the APA cited concern that the executive order would further jeopardize the health and well-being of asylum-seeking families, by allowing for their incarceration longer than is permitted by current law.
There are currently no provisions in the RISE from Trauma Act that would specifically address the trauma recovery needs of refugee families impacted by U.S. immigration policy. Ira Cohen, director of issues and communications with the office of Congressman Danny Davis (D-IL), a co-sponsor of the RISE from Trauma Act, said: “To the extent that any policies have led to an increased amount of trauma, it is fair to say that the need for this legislation is greater than ever.”
****
MIA Reports are supported, in part, by a grant from the Open Society Foundations



{kind=link}
First, I’m really leery about providing more money for the government to get into our nation’s schools through “mental health” programs. Second, I don’t see how doing so is not going to lead to more labeling and drugging of school children. “Trauma” may provide an excuse for more labeling and drugging, but getting people out of the “trauma informed” system then becomes a little more problematic and difficult. A bigger system means an expanded system, both on the part of “the traumatized” “patient/consumers”, and the “treating” staff. My sense is that this bill, if passed, is likely to lead to more rather than less medicalization of school children, and that is something that I could not, in all honesty, support. Generally, I just see this as another liberal policy maneuver to fix matters by spend, spend, spending, and I think those spending efforts, rather than correcting anything, are likely to result in more and more of the same. This is especially true when this is a matter of putting the “mental health” system in our nation’s schools, just as it would be if they were doing the same at places of business.
Report comment
I don’t think that it’s possible to be truly “trauma informed” as long as you are relying on the DSM-driven standard “mental health” system. The only “trauma informed” thing to do is to erase everything people claim to know about “mental illness” and start over from scratch, and rebuild from the viewpoint that the people who have been traumatized are the ones who actually know what they need.
Report comment
I should add, the concept of “mental illness” would itself have to be trashed as job one, because it is most definitely NOT “trauma informed” to tell someone that their understandable reaction to being beaten, sexually abused, or otherwise oppressed is a “disorder” that needs “treatment!”
Report comment
I see competing approaches at work here, the only problem is that the more the “highly critical” approach competes with the conventional approach, the more entrenched the conventional approach actually becomes. You’ve just got two schools of thought competing for business, and business, the business of labeling and drugging people, is the problem. The farther away you get from them, the more the two schools of thought resemble each other. I don’t think sob stories really explain anything as sob stories are less a matter of selling stories, and more a matter of horrors that we’d want to see diminished. You don’t, I want to emphasize, diminish such horror stories by making a business, and therefore careers, out of them. You diminish such horror stories by attacking any such business, and the horrors that come with it, itself. This means acknowledging that a shrinking “mental health” system, “trauma informed” or otherwise, would be progress over a perpetually expanding system. I’d challenge the system, in a sense, to…Oh, how do you say? Oh, yeah. “Wither away”.
Report comment
That sounds like the best solution…for this entire system to just stop existing. If only it would collapse under its own weight.
It was suggested to me a number of times by treatment providers that “trauma work” would be available to me once I was stable in their eyes. Being stable meant…accepting the borderline diagnosis, being compliant, taking the drugs as prescribed, and the like.
There was never going to be any trauma work. It was a long con.
If we know what trauma is, then, yes, better to stop it from happening in the first place than to add a trauma informed veneer to the current system. If we can see that a policy is creating trauma, better to focus on changing the policy rather than put more money into a broken system.
Report comment
I’m leery too Frank.
Know what would make me celebrate? A bill requiring the bureacrats and Rx drug dealers to leave our kids alone.
Never trust the Mental Illness makers. Especially when Big Brother has got their back.
Report comment
Well it is a start though I have concerns.
Before policy there should have been and or a White House Conference on both Adult and Childhood Trauma, Congressional Hearings on Trauma to be real one would need to highlight First Nation Peoples Trauma, African American Trauma caused by institutional and non institutional racism, Trauma from Sexism, Tbe effects of Moral injury trauma due to First Responders and Safety and Protective Forces primary and secondary and tertiary trauma, the Trauma of Incarceneration All Systems ——see Charles Dickens writing about his travel to America and he knew trauma and incarceration,
Intergenerational Trauma, the Trauma of Sexism and much more.
A Blue Ribbon Panel Or White Paper or Rainbow Two Year nationwide Listening Sessions and then a Third Year report with professionals and non professionals involved.
These activities should be funded by the Big Pharma Industry who deliberately and willfully let greed versus ethical considerations run their business plans.
Also any companies or financial entities or other profit or nonprofit groups that have indulged in deliberate malfeasance.
That or have a Nuremberg type of Trial.
Policies and legislation no matter how well entioned will far apart fast if not backed up by a system wide learning and nationwide outing of the corruption that had almost destroyed our country.
Kudus for trying but dialogue before planning.
Report comment
My opinion is not directed at the author, but at the topic. I want to make clear that I think the nature of “Trauma-Informed Care” is literally bass-ackwards. What is TIC?
“The intention of Trauma-Informed Care is not to treat symptoms or issues related to sexual, physical or emotional abuse or any other form of trauma but rather to provide support services in a way that is accessible and appropriate to those who may have experienced trauma.”
And this is why, of all the state models, only one mentioned families. This “trauma-informed” approach seems to still be focused on altering childrens’ behaviour to get them through the educational system. (A 50 million investment in mental health services was the first clue!) This article mentions health care resources multiple times as well as a school-based clinic. I have read nothing that mentions treating the family situation, and that seems to be because that is intentionally not part of trauma-informed care.
Speaking as someone who has a high ACE score, the most traumatic part of my childhood was not the physical, sexual, or emotional abuses that took place. Nor the violence I witnessed. The most traumatic part of my childhood was the intense focus paid to my “bad” behaviors, the sympathy and support given to my parents for all they had to “cope with”, and the dismissal of my (and my sister’s) reports of said physical, sexual, and emotional abuse. And the way I read it, trauma-informed care means exactly more of this. No focus whatsoever on the issues causing the trauma, but instead responding to the effects of trauma in social and educational service settings.
I want to be able to applaud efforts at being more trauma-informed in terms of understanding a child’s behaviour, but I fear that legislation intended to help children by devoting more resources to disadvantaged children’s mental health in the school environment will merely cause more kids to end up in the psychiatric system instead of in the penal system. I don’t view a school to psychiatry pipeline as an improvement over the school to prison pipeline.
You cannot address the issues that happen in the family and community in a school health clinic – either via therapy or drugs. This focus on the child is inappropriate and harmful, frankly, because it doesn’t address the root causes. A truly trauma-informed approach would start in the community and in the home to address the issues that kids are experiencing at the source, whether that be witnessing violence, experiencing violence, having food or shelter insecurity, changes in caregivers, or just being severely neglected. One thing I know is that kids don’t get to an ACE score of 8 like I have without failings both in and out of the family and social institutions. Severe trauma doesn’t happen accidentally and there is no number of school health clinics that are going to do more than put a bandaid over a hemorrhaging wound.
Lastly, like many organizations that purport to lobby on behalf of marginalized groups, the board CTIPP is made up of mostly white people, and entirely of professionals. How many of them personally identify as having experienced severe childhood trauma? How many of them have been in foster care or lived in dangerous, violent neighborhoods, or were used as sexual playthings, or were beaten by their caregivers? How many of them have anything more than an academic knowledge of what they’re promoting? You sure don’t get the impression from their bios that they are anything more than SJWs talking over the voices of marginalized people who have experienced these things and have a solid understanding of the kinds of changes necessary to create whole, healthy communities, families, and kids. So I’ll say it loud and clear: Nothing about us without us! Targeting children for behavioral alteration by promoting more mental healthcare in educational settings while having no intention of addressing the root cause of their distress and is immoral and harmful.
Report comment
Fantastic post!
Report comment
I agree with Steve of course.
One thing about that whole “nothing about us without us” — while valid in principle, many things said and done “about us” would be equally invalid if we were suckered into participating. So it’s more like “nothing about us period unless we agree it should exist In the first place.”
Report comment
When “we” are a ‘business’, sometimes the answer is to ‘get out of the business’ so to speak. When your “we” are an expanding category of so-called “sick” people, even abused and oppressed people, maybe some doctor would be better off in another field of study rather than that of “us”. Perhaps, and that statement is also true when applied to many of “us” as well.
Report comment
So Oldhead you never had a shrink say, “I don’t know what’s wrong with you. You look perfectly healthy. But your behaviors/thoughts/mannerisms/tone of voice bug me. So I’m going to lock you up and experiment on you with a bunch of mind altering drugs. Been ‘tested’ by the place that manufactured them. No conflict of interest there.
“Nobody knows what the long term results of these drugs are. Or even how they work. But I’m sure they work cause Yolanda, that hot babe of a Pharma rep offered me warm doughnuts–and further…office calls–if I try this out on a lucky consumer.
“So how bout it? You don’t want poor old Doc Quackenbush to go doughnutless would you?” 😀
Report comment
Your comments are staggeringly articulate!
Report comment
“Provide $50 million in funding for a ‘mental health in schools’ program.” This is a mistake, we need the “invalid” and “unreliable” “mental health” workers OUT of the schools. The “mental health” industry’s DSM “bible” was debunked as “invalid” six years ago, but they’re still using it. And the DSM does NOT allow the “mental health” workers to bill for helping child abuse survivors.
https://www.nimh.nih.gov/about/directors/thomas-insel/blog/2013/transforming-diagnosis.shtml
https://www.psychologytoday.com/us/blog/your-child-does-not-have-bipolar-disorder/201402/dsm-5-and-child-neglect-and-abuse-1
And since the “mental health” workers regularly force treat people, which in and of itself, is traumatic. The right of the “mental health” workers to force treat people needs to be taken away. Force treatment is traumatic.
And both the psychologists and psychiatrists have had as their primary actual societal function, for the past century, covering up child abuse, not helping child abuse survivors. As the mother of an abused child, I have medical proof of this in medical records.
Our “mental health” workers deny child abuse happens, misdiagnose the child abuse survivors, and/or their concerned parents, and poison them with the neurotoxic psychiatric drugs. And this is a systemic problem, according to the medical and historic evidence.
https://www.indybay.org/newsitems/2019/01/23/18820633.php?fbclid=IwAR2-cgZPcEvbz7yFqMuUwneIuaqGleGiOzackY4N2sPeVXolwmEga5iKxdo
https://www.madinamerica.com/2016/04/heal-for-life/
I do have a suggestion, however, we should start arresting, convicting, and imprisoning for life or chemically castrating the child molesters. Today, if you report that medical evidence of the abuse of your child was handed over, you get told by the police to go talk to a psychiatrist. CPS won’t look into legitimate cases of child abuse, if the abuse occurred outside the home, preventing CPS from stealing the children. We need our government officials, and their “mental health” minion, to start punishing the child molesters, and stop poisoning the child abuse survivors.
But, instead, our government officials are partying with the convicted, but set free, child molesters. Upside down and backwards, America.
https://www.youtube.com/watch?v=siCsVQTbpkI
Report comment
Like CatNight, I also have concerns about this.
Glad it is being talked about, glad MIA has reported on this. But my concern that this will lead to more therapy and recovery, as well as more reification of the Good Family.
Hoping to hear more and waiting to see.
Report comment
Oh Illinois, the land of 6,963 units of government- Maybe one day policies will be made that actually help prevent the violence, crime, drug cartels, and gangs from taking over in the first place.
Report comment
IL is a very corrupt state, unfortunately. I remember, when I was young, and told Europeans I was from Chicago. They’d point their finger like a gun, and say “bang, bang,” in reference to Al Capone. What’s the IL joke? “Vote early and often.”
And how many IL politicians have landed in jail? Most, eventually. And what’s really sad? Today, the IL medical system has been completely corrupted, as at least somewhat exemplified by this now FBI convicted, sicko doctor.
https://www.justice.gov/usao-ndil/pr/oak-brook-doctor-convicted-kickback-scheme-sacred-heart-hospital
But note, he’s not even American, he’s a foreigner who came to Chicago to destroy America from within.
Report comment
I share the concerns of CatNight, Kindred Spirit, Frank Blankenship, and PacificDawn. All of them brought up really good points. But Catnight suggested a built in solution which resonates with me. Take steps to innocolate this modest initiative (17 million for ACES v.s. 5 billion in big Pharm funding is a drop in the bucket but we will take it!) lest it get swallowed up in layers of federal and state bureaucracy or co-opted by big Pharma front groups. “Policies and legislation no matter how well intentioned will far apart fast if not backed up by a system wide learning and nationwide outing of the corruption that had almost destroyed our country.” CatNight suggested a Nuremberg Trial. I doubt society is ready for that type of restorative justice but even nationwide listening sessions would be awesome if they were organized by survivors, not treatment providers, in other words, experts by experience, not experts by training. For a good model, see the wonderful ‘truth and reconcilation’ circles organized by Rethinking Psychiatry. HERE http://www.rethinkingpsychiatry.org/2017/02/05/truth-reconciliation-march-1/
Report comment
And of course at least most if not all of the interventions are inevitably going to be or involve psych drugs, brain damaging, sometimes life-destroying, and certainly capable of traumatizing psych drugs. (especially regarding psychiatric hospitalizations and custody battles over refusal to drug a child or a child’s insistence not to take them because of the harm they’re experiencing; oh wait, it’s just kids being silly because ‘kids don’t like medicine, pooey!’ )
And if you think I’m exaggerating;
http://bonkersinstitute.org/medshow/kidtime.html
Or more accurately, “must assaulting your child from the inside out, with damages they may never recover from, and damaging the most important organ in their body always involve a game of tag?”
Report comment
Is it not absurd on its face to ask or expect the very system that foments such widespread trauma as the cost of doing business to then turn around and provide the solution?
Report comment
It’s not absurd, it’s called the “Hegelian Dialectic.” And it is how our so called “mental health” workers, who are the “omnipotent moral busy bodies,” controlled by our run amok government, operate.
Report comment
Well Germany and the Allies did have the trials and there were massive educational programming. Scores of elementary schools were named for Sophie Scholl and Kathy Kollowitz. Corrie Ten Boom a Dutch Reformed Christian spent time in internment for helping out the Jewish folks in the Netherlands. Miep G. the same for the Frank Family. And yes they missed the genocide of the disabled and homosexual communities- the testing phrase learned from the Eugenic movement in the states and other countries.
Soviet Russia had generations of all sort of pogoms. Which leader did which? Do which groups- changed with the decade. And any tyrant at any time look under the rugs and there it all is.
But the trials did happen. Read Hannah Arndt.
The Slave Trade in America – the North played a silent partner role.
It ain’t never gonna be perfect but something needs to be done.
The legislation though probably well intentioned – so many folks don’t know what they don’t know not best practice.
Call your legislatures and do something. Check out the opioid action at the Met. They did it.
Report comment
Psychiatry is “trauma denial”; “trauma informed care” is dishonest. A trauma is a distressful experience of a distressful environment; in contrast, psychiatry implies that a trauma is a distressful experience of an otherwise friendly, supportive environment. Psychiatry denies trauma from bullying, discrimination, poverty and sexual assault by advocating that victims “recover” from their legitimate fears while their environments remain dangerous and hostile. Psychiatry similarly denies trauma from child abuse and the sorrow of war by advocating that victims “recover” from their distressful experiences while the community ostensibly ignores its reality.
Report comment
Trauma Inflicting Coercion.
Appropriately called TIC. And they’ll have tics aplenty along with seizures, tardive psychosis, morbid obesity, akathisia, and diminished IQ. All children being groomed for lives of isolation and physician induced disability so these Dr. Mengele wanna be’s can try cruel pointless experiments on them.
Pardon me while I go off and cry.
Report comment
^^^^^^ I agree with Rachel777
Report comment