
In a new article in Nature Communications, researchers claim that “ketamine can reduce harmful drinking by pharmacologically rewriting drinking memories.” But their results were much more nuanced—and nowhere near as positive. In fact, the group that did not receive ketamine had lower levels of alcohol use throughout the study.
Ravi K. Das led the research at University College, London. The researchers based their experiment on a memory-based theory of how problematic drug use develops. In that theory, memories of the rewards associated with drug use are triggered when a person sees the drug, causing them to desire more of it.
 Because memory is theorized to rely on the N-Methyl D-Aspartate receptor system in the brain, Das and his colleagues thought that ketamine, which also affects that system, might have a potential use. They theorized that if someone received a ketamine infusion just after having their alcohol memories triggered, the drug might block the biological system that enables those memories to take hold.
Because memory is theorized to rely on the N-Methyl D-Aspartate receptor system in the brain, Das and his colleagues thought that ketamine, which also affects that system, might have a potential use. They theorized that if someone received a ketamine infusion just after having their alcohol memories triggered, the drug might block the biological system that enables those memories to take hold.
To simplify, this theory is that ketamine might cause short-term memory loss. However, the researchers did not directly test this notion. Instead, they wanted to test the whole idea—that a ketamine infusion might reduce problematic drinking.
To test this theory, Das and the other researchers collected 90 participants (men and women), all of whom were heavy beer drinkers—although none of them had a diagnosis of an alcohol use disorder, and none of them were seeking treatment for alcohol use.
The participants were split into three groups. One group received a ketamine infusion and an alcohol drinking task (the rewarding memory); another group received ketamine, plus a fake memory task (orange juice instead of alcohol); the third group received a placebo infusion (not actually ketamine), but the real memory task.
The study was single-blind, which means that the researchers were aware of whether a person received the drug or placebo. The gold standard is to use a double-blind design so that the researchers are less likely to inadvertently bias the results.
The researchers found that, on average, the group that received both the ketamine infusion and the alcohol task improved much more—they were drinking far less than their baseline levels. But all three of the groups did better over time, and the group that received the ketamine infusion and the alcohol task was doing worse than the other groups at almost every time point. They were drinking more than those in the group that received ketamine and an orange juice task, and more than those in the group that did not even receive any ketamine at all.
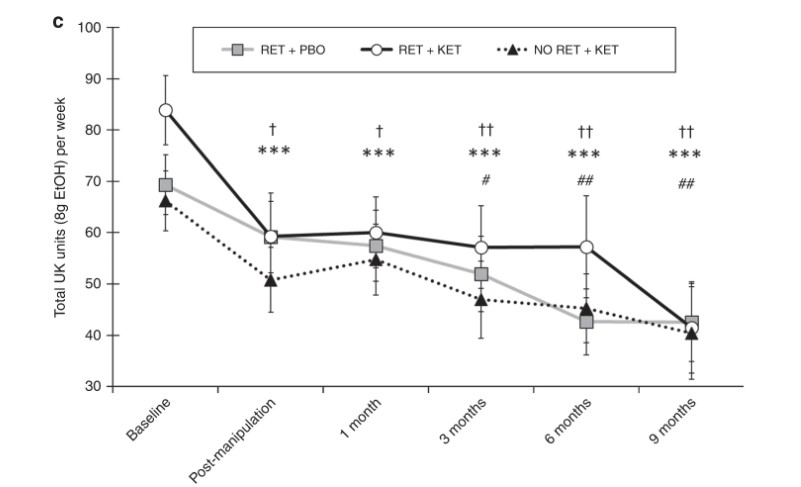 This table shows that the group that received ketamine and the alcohol memory task (RET + KET) began the study with an unusually high amount of drinking compared to the other two groups. You can see that RET + KET are, on average, drinking higher total units of alcohol at almost every time point. By the endpoint of the study, all three groups are, on average, drinking about the same amount of alcohol.
This table shows that the group that received ketamine and the alcohol memory task (RET + KET) began the study with an unusually high amount of drinking compared to the other two groups. You can see that RET + KET are, on average, drinking higher total units of alcohol at almost every time point. By the endpoint of the study, all three groups are, on average, drinking about the same amount of alcohol.
The researchers interpret this finding to mean that ketamine is successful—this group improved more over time, after all. But this finding is what would be predicted by chance.
One statistical phenomenon that occurs by chance is called regression to the mean. In that phenomenon, groups that start at an abnormally high (or low) point on any scale are more likely to return to the average over time. For instance, let’s say an event occurs—like a wedding, or a holiday celebration, during which you drink much more than usual. You are most likely to return to your regular drinking amount afterward. And that’s what we see here.
The researchers do acknowledge this:
“We cannot rule out regression to the mean as a contributing factor to the observed reduction in alcohol consumption.”
However, the researchers assert their belief that regression to the mean is not responsible for their results, calling that common statistical phenomenon “highly unlikely.”
The researchers write that “The subsequent, lasting clinical benefits observed suggest that this one-session intervention approach should be pursued in the future treatment of alcohol-related disorders.”
****
Das, R. K., Gale, G., Walsh, K., Hennessy, V. E., Iskandar, G., Mordecai, L. A., . . . & Kamboj, S. K. (2019). Ketamine can reduce harmful drinking by pharmacologically rewriting drinking memories. Nature Communications, 10(5187). DOI: 10.1038/s41467-019-13162-w (Link)














I have a friend that’s in Alcoholics Anonymous and he says that if a person stops drinking and life stays okay then that’s good. But if a person stops drinking and they find other problems begin to cause trouble then this is something the AA could help them with.
Report comment
We can find other biases in this study.
Hawthorne effect: “is a type of reactivity in which individuals modify an aspect of their behavior in response to their awareness of being observed.”
Social desirability bias: “is a type of response bias that is the tendency of survey respondents to answer questions in a manner that will be viewed favorably by others.”
Classical conditioning: “refers to a learning procedure in which a biologically potent stimulus (e.g. alcool) is paired with a previously neutral stimulus (e.g. aversive social situation).”
At least some parts of the experience was designed to maximize the Hawthorne effect and the social desirability bias by classical conditioning.
“Baseline and post-manipulation (i.e. Day 1 and Day 10) cue reactivity was assessed via ‘liking’ and ‘urge to drink’ ratings of a set of beer (N = 7), wine (N = 3) orange juice (N = 4) and soft drink (N=2) cue images, as described previously12. The experimenter first opened a bottle of lager (Pilsner Urquell) in front of the participants and poured 150ml into a half-pint glass. This was placed on the table in front of the participants and they were told that they would drink this beer when instructed to by on-screen prompts, but that first they would rate a series of images for pleasantness(liking) and their effects on urge to drink(wanting) the beer in front of them. All ratings were made verbally on a scale of -5 (extremely unpleasant/ greatly reduces urge) to +5 (extremely pleasant/ greatly increases urge) and noted by the experimenter. Images were 400×400 pixels, presented centrally on a computer screen, in a random order, for 10 seconds each. Following completion of the rating, participants were asked to rate their current urge to drink the in vivo beer (anticipatory urgerating) and how much they Conducting the cue reactivity/alcohol reinforcement task on Day 1 and Day 10 both provided a metric of clinically-relevant changes in the hedonic and motivational effects of beer and maximised the expectancy of receiving beer during the Day 3 reactivation procedure, thus generating a prediction error (PE) when the drink was withheld on Day 3.
The alcohol MRM (RET) and Control (No RET) Memory Reactivation Procedures took place on Day 3 and used sub-sets of stimuli from the cue reactivity /alcohol reinforcement task. For MRM retrieval (RETgroups), these were four images of beer and for No RET+KET, these were four images of orange juice. All participants also rated two ‘soft drink’ images of cola and coffee. Participants in MRM retrieval conditions were told they would repeat the image rating and beer consumption task from Day 1. Again, a beer was opened and 150ml poured into a glass placed in front of participants. They then rated four of the beer cue images (designated ‘beer retrieval’ images) and the two soft drink images, along with their ‘urge to drink’ and anticipated enjoyment of the in vivo beer. The drinking prompt screens then began, but the final prompt read ‘Stop! Do not drink’.”
This is pure classical conditionning. Alcohol consumption is associated with an unpleasant social situation, frustration, and public exposure by the “experts”.
Although the experiment has resulted in “favorable” results, it is likely that it has above all (re)demonstrated the effectiveness of classical conditioning and social pressure in reducing alcohol consumption, or at least, the declaration of alcohol consumption.
Other biases can be found in the detailed description of the experiment.
For example, 27/30 of the placebo group and 60/60 of the ketamine group guessed which group they were in. Therefore, this experience is almost open label.
SUPPLEMENTARY INFORMATION
Report comment
I find it interesting that the group that received both the ketamine infusion and the alcohol reward task had a much higher baseline of drinking than the other two groups. I suspect this is the biggest reason that group had the most improvement over time. They had the most room for improvement. I’d find it very hard to believe that this group wasn’t specifically cherry picked for that very reason and it underscores the need for both double-blinding and random assignment of participants. Great reporting, Peter!
Report comment
I’m so easily consumed by the information that in one way or another, the study itself would impact me. Just being aware would cause me to either think of drinking more, or cutting back, depending on what else is happening within me.
If before the study I played with the idea that perhaps I should drink less, that would possibly have an effect. There are so many variables.
I don’t understand studies at all, especially at an academic level, and I don’t trust most of them anyway.
Besides, beer is probably cheaper than Ketamine…..I hope the Ketamine group didn’t get hooked on the Ketamine 🙂
Report comment
This seems similar to the medical delusion that dangerous, mind altering antidepressants are “safe smoking cessation meds.”
Maybe, since the medical/pharmaceutical industrial complex wants to make legal vices, medically illegal. In other words, the medical/pharmaceutical industrial complex has turned the legal behaviors of smoking cigarettes and drinking alcohol into “mental illnesses.”
This desire on the part of the medical/pharmaceutical industrial complex to turn legal vices into “mental illnesses” should be announced to the public? If for no other reason, than none of us mere humans are perfect, including the doctors?
Report comment
And the irony is, they are now starting to prescribe more and more “medication” to stop people drinking. Drugs to stop taking drugs. What could go wrong?
Report comment
Someone Else, Steve.
If doctors and shrinks had wanted to, they could have shut down the industries of dangerous habits. There are enough of them, enough money and power to do that along with politicians and lawyers.
They complain about the costs to health services, but take no action except to create drugs that are not safe. For governments to allow production and sales of highly toxic and addictive substances is not right. They seem to want control over people and if they really wanted to, could have shut down these companies.
But somehow it benefits everyone in the long run. Hospitals need sick people, we have people who need jobs. If not for sick people, what will all the hospital employees do?
Freud himself was an addict, psychiatry and therapy are founded on his own neurosis. He sucked on that cigar like a mommas breast (as per his theory) He also availed himself of a death, which allowed him to escape the final suffering.
If mental illness exists, it exists within psychiatry and might very well look like the very people who diagnose.
Everything within the DSM is starting to overlap, describing the human condition as an illness.
Many moved as they say, away from Freudian thinking. This is false. Everyone including his dog borrows from the forefathers of navel gazing that projected onto others the maladies they themselves were confused and preoccupied with. There are now thousands of drugs, thousands of therapies. Therapists and their followers posting on forums, in disguise, to try and sell their thinking.
It is the Avon of society. What better gimmick than to assume things about the brain and sell it as a speciality.
Report comment
Psychiatry=projection.
Physicians, heal yourselves.
Report comment
Yes. Must be those shadow selves.
Report comment
Can you say god complexed? And medical greed run amok?
Report comment
I’m reminded of Mrs Terrain in Brazil whose “complication has had a slight complication” lol
https://m.youtube.com/watch?v=_-gJrmIL5BE
The choice between the “knife man” and the “acid man” when selecting who to do your face lift can be quite crucial. Poor Mrs Terrain ended up a pile of offal in a coffin and minus a lot of money for the services of Dr Chapman. I’m sure that Terry Gillam was a closet anti psychiatrist after watching this movie lol
Report comment