
Editor’s Note: Over the next several months, Mad in America is publishing a serialized version of Peter Gøtzsche’s book, Mental Health Survival Kit and Withdrawal from Psychiatric Drugs. In this blog, he discusses some final issues with psychiatry, its drugs, and electroshock. Each Monday, a new section of the book is published, and all chapters are archived here.
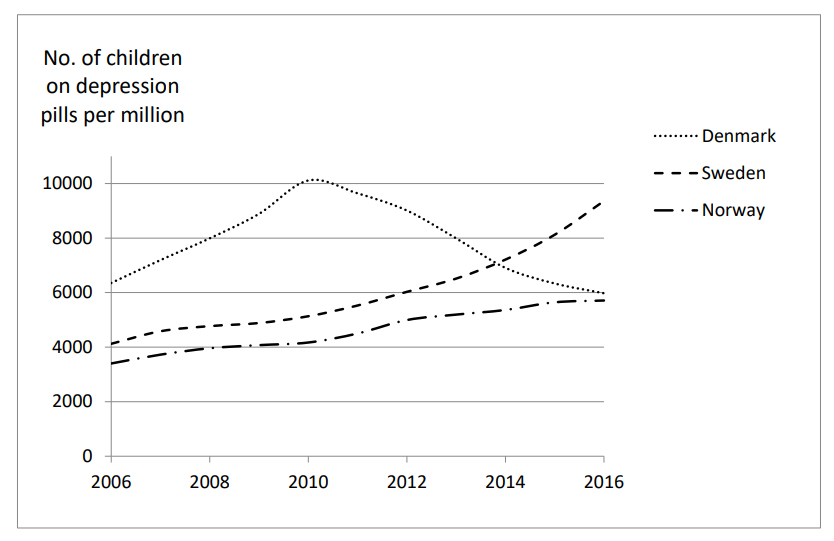
Use of depression pills for children dropped 41% in Denmark
Here comes a little glimpse of hope in defiance of the dark hole of psychiatry, which absorbs all rational thought like black holes in the cosmos absorb everything that comes near them.
It is possible to revert the ever-increasing trends in usage of psychiatric drugs if you are similarly tenacious as John Read was in relation to the UK Royal Society of Psychiatry.
Due to concerns about the suicide risk, the Danish National Board of Health reminded family doctors in the summer of 2011 that they should not write prescriptions for depression pills for children, which was a task for psychiatrists.168 At the same time, I began to warn strongly against the suicide risk of the pills. I repeated my warnings countless times in the following years on the radio and TV, and in articles, books and lectures.
It started with an interview with the managing director of Lundbeck, Ulf Wiinberg, who, in 2011, claimed that depression pills protect children against suicide. The interview took place while Lundbeck’s US partner, Forest Laboratories, was negotiating compensation with 54 families whose children had committed or attempted suicide under the influence of Lundbeck’s depression pills. Elsewhere, I have described Lundbeck’s irresponsible behaviour, also in relation to a paper I published about the interview.4
In Norway and Sweden, there have been no such initiatives. The number of children in treatment increased by 40% in Norway (0-19 years) and 82% in Sweden (0-17 years) from 2010 to 2016, while it decreased by 41% in Denmark (0-19 years) despite the fact that professors of psychiatry also in Denmark continued to propagate their false claims that depression pills protect children against suicide.169
The Danish National Board of Health had issued several warnings against using depression pills to children before 2011. I therefore believe it is primarily due to my tenacity that the usage went down in Denmark. I say this to encourage people to fight for a good cause. Despite the formidable odds, it is possible to change things in psychiatry for the better. Not much, but we must not give up the fighting.
Number needed to treat is highly misleading
It is standard in psychiatric research articles to mention the number of patients that need to be treated (NNT) to benefit one of them. The psychiatrists mention NNT all the time as evidence that their drugs are highly effective. But NNT is so misleading that you should ignore everything you read about it.
Technically, NNT is calculated as the inverse of the risk difference (it is actually a benefit difference), which is very simple. If 30% have improved on drug and 20% on placebo, NNT = 1/(0.3-0.2) = 10. Here are the main problems:
First, NNT is derived from seriously flawed trials, with cold turkey withdrawal in the placebo group, insufficient blinding, and industry sponsorship with selective publication of positive results and data torture.
Second, NNT only takes those patients into account that have improved by a certain amount. If a similar number of patients have deteriorated, there would be no NNT, as it would be infinite (1 divided by zero is infinite). For example, if a drug is totally useless and only makes the condition after treatment more variable, so that more patients improve and more patients deteriorate than in the placebo group, the drug would still seem effective based on NNT because more patients in the drug group would have improved than in the placebo group.
Third, NNT opens the door to additional bias. If the chosen cut-off for improvement does not yield a result the company’s marketing department likes, they can try other cut-offs till the data confess. Such manipulations with the data during the statistical analysis, where the prespecified outcomes are changed after company employees have seen the data, are very common.4,51,101,184
My research group demonstrated this in 2004 by comparing trial protocols we had acquired from ethics review committees with the trial publications. Two-thirds of the trials had at least one primary outcome that was changed, introduced, or omitted, while 86% of the trialists denied the existence of unreported outcomes (they did not know, of course, that we had access to their protocols when we asked).184 These serious manipulations were not described in any of the 51 publications.
Fourth, NNT is only about benefit and completely ignores that drugs have harms, which are much more certain to occur than their possible benefits.
Fifth, if benefits and harms are combined in a preference measure, it is not likely that an NNT can be calculated because psychiatric drugs produce more harm than good. In this case, we can only calculate the number needed to harm (NNH). Drop-outs during trials of depression pills illustrate this. Since 12% more patients drop out on drug than on placebo,114 the NNH is 1/0.12, or 8.
The UK silverbacks did not take any of these flaws into account when they claimed that depression pills have an impressive effect on recurrence, with an NNT of around three to prevent one recurrence.182 It is not surprising that patients want to come back on the drug when their psychiatrists have thrown them into the hell of acute withdrawal by suddenly substituting their drug with placebo. As only two patients are needed to get one with withdrawal symptoms,57 there cannot exist an NNT to prevent recurrence, only an NNH to harm, which is two.
Nor can there exist an NNT in other depression trials, as the difference between drug and placebo in flawed trials is about 10%,4 or an NNT of 10, which is far less than the NNH. For example, the NNH for creating sexual problems is less than two for depression pills.
Similar arguments and examples can be produced for all psychiatric drugs. Thus, the NNT in psychiatry is bogus. It doesn’t exist.
Electroshock
As this book is about drugs, I won’t say much about electroshock.4 Some patients and psychiatrists say it can have a dramatic effect. This could be true, but the average effect is less impressive, and if electroshock were effective, people wouldn’t need to receive a long series of shocks, which is usually the case. Furthermore, the shock effect doesn’t last beyond the treatment period, and electroshock “works” by causing brain damage, which is scary.4
Once, I was asked at a meeting what my view was about a woman who was so depressed that she could hardly be contacted but asked for a glass of water after an electroshock. I said that since this was an anecdote, I would reply with an anecdote. I was once asked to look after a newly admitted man, an unconscious alcoholic. As I needed to rule out meningitis, I tried to insert a needle in his back to tap cerebrospinal fluid for microscopy and culture. It was very difficult to get in and I hit his bone several times. All of a sudden, the drunkard exclaimed loudly: “Bloody hell, stop stinging me in the back!”
Had I caused a miracle with my needle and cured the guy? No. Odd things happen all the time in healthcare. Could I have woken up the deeply depressed woman with my needle? Who knows, but why not?
Psychiatrists often say electroshock can be lifesaving, but there is no reliable documentation for this claim, whereas we know that electroshock may kill people.4 Furthermore, it can lead to severe and permanent loss of memory, which leading psychiatrists fiercely deny can happen,4,23 even though it is well documented that electroshock leads to memory loss in most patients.4,185-187
I find it totally unacceptable that electroshock can be enforced upon patients against their will, because some patients will die, about 1 per 1000,186 and others will suffer from serious, irreversible brain damage.4,23
- You should not take psychiatric drugs. The only exception I can imagine is a seriously disturbed acute situation where you may need to get some rest.
- If you are lucky and have a good psychiatrist who understands the fallibility of psychiatric diagnoses and that drugs or electroshock are not the solution to your problem, continue talking to this doctor.
- Don’t accept electroshock. It is not curative, and some patients are killed or suffer serious and permanent brain damage that reduces their memory and other cognitive functions.
- If you, after having read all the foregoing, believe psychiatry is evidence-based and that psychiatrists generally know what they are doing, and that you therefore want to consult one you have never met before, I wish you good luck. You will need it.
To read the footnotes for this chapter and others, click here.













After all, one day,
psychiatry becomes like an hourglass that just flows out like sand and most psychiatrists will realize that they have been fooling around with God’s creative power, just like aliens!
55 years – olaveivind
Report comment
Psychiatrists understand one thing. – Whatever evil they have committed, everything will remain unpunished. They have no reason to understand anything else.
Report comment
I didn’t know that asking for a class of water after being electrocuted meant “mental illness” was improved. If someone were to piss in someone’s mouth they’d probably also ask for a glass of water afterwards. Psych denies all harms, or even pretends harms are helpful (brain damage, memory loss, sedation, cognitive impairment, weight gain) while they insist that someone asking for water after being electrocuted means electrocution helps people.
Report comment
Yes, this property of psychiatrists is not only to destroy a person, but also to call the damage caused as help.
Report comment
Really folks — if “mental health” needs this many chapters of instruction on how it is to be “survived,” doesn’t it make sense to just stay as far away from it as possible?
Report comment
However, not everyone is allowed to “stay away”. Don’t forget compulsory psychiatry.
Report comment
True, for sure. But I believe this article is directed to those who do have a choice.
Report comment
I notice of articles aimed at saving those who have no choice left at all – is not visible at all. Which in my opinion is not right and too cruel.
Report comment
Thank you so much, Peter, for all your truth telling. I know so well, it has caused you to be attacked, because my truth telling has also caused me to be attacked and censored. I’m so grateful for all you do. Please keep speaking the truth, for those of us who are being prevented from speaking the truth.
Report comment
I second that, and this is your best book yet.
Report comment
Hi Peter – do you have a graph showing trends in suicide rates in the three countries, as that is what is claimed to be the reason to start depression pills?
Yes I appreciate your work over the years – I think it was some of your work which convinced me basically never to initiate prescription of depression pills (I like this term) as a GP in Australia – only for people already on them. Also due to your work I have never had a mammogram myself, though still do refer patients as part of the KPIs of my workplace – but don’t push them unlike other screening tests with more evidence behind them. It seems like the tide is starting to turn at least in the UK and some EU countries with regard to use of depression pills and with increasing understanding of harms and significant withdrawal side-effects in 50% plus on users.
Report comment
BBC News – ‘My doctor prescribed rambling for lockdown anxiety’
https://www.bbc.co.uk/news/uk-scotland-edinburgh-east-fife-56919166
It seemed to work!
Report comment
Nothing like a prescription of “common sense!” Though as Tim McCarver once remarked, if it were all that common, more people would have it!
Report comment
Peter your articles are very much needed by parents and parents to be. And GO DENMARK health for trying to, making the effort to protect it’s children!
If it is not okay to drug kids in one country, it must be so for all countries.
And you are correct, one would need a hell of a lot of luck to find a good psychiatrist.
Long ago when I asked two doctors if they knew of a good shrink, one being my friend said, “they are crazy, and I only know one that I like, but only on a personal basis”. The other, being my GP said, “you can’t use the word “psychiatrist” and “good” in the same sentence”, after which she continued to discuss the issue at length.
I figured because they were doctors, they would be personally able to recommend one, but instead I was warned.
More physicians should do so. After all physicians are supposed to care for our health and so they should be honest.
Report comment
“….I began to warn strongly against the suicide risk of the pills…”
The logic I believe behind these “pills” is that they CAN cause suicide – but that they PREVENT more suicides.
I’m not so sure – because from my own experience I did request in writing that drugs I had taken be warned against and I described Akathisia fairly well in my historical letter – but doctors lied to me about my protection. And many years later present day doctors also covered up on behalf of these doctors.
My historical doctors had been promoting the drugs via Research papers even after I had warned them about the Suicidal risk.
Ultimately my ADR Warning Request letter had the University Hospital Stamp on it, My historical Record Summary minus any ADR Warning had the University Hospital Stamp on it. The Historical Doctors False Reassurance Letter had the University Hospital Stamp on it. And a subsequent 1998 Research Paper Recommending the Suicidal Drugs as reliable also had the University credentials attached to it.
The Suicidal Drugs (Fluphenazine) were eventually removed from the market (circa 2015) after 60 years usage due to “Reliability of Supply Problems”.
.. My Historical Records 1980 – 1984, had described me as a “Dreadful Schizophrenic” – but I recovered fully in 1984 as a result of STOPPING Fluphenazine – NOT as a result of taking Fluphenazine.
Report comment
There is actually no data supporting the idea that “antidepressants” reduce the likelihood of suicide. Rather, the data indicates the opposite – that people are MORE likely to kill themselves after starting “antidepressants.” Yet somehow the idea that “antidepressants save lives” still lives on.
Report comment
The ‘Neuroscientists ‘ are killing the vulnerable – just like Dr Shipman and Nurse Beverly Allitt were…
Dr Shipman
https://en.m.wikipedia.org/wiki/Harold_Shipman
Beverly Allitt
https://en.m.wikipedia.org/wiki/Beverley_Allitt
…but they’re getting away with it.
Report comment
It’s either people admit they killed people by telling them to take drugs or rationalize how the data is wrong and continue giving people the drugs. Denial is a powerful thing especially if it’s denying the harm you caused.
Report comment
Too true Willoweed,
In my case the University Hospital I had attended actively doctored my records – so that I could potentially be killed.
Report comment
Many people who’ve gotten ahold of their psych records note how they are filled with misinformation, and insulting diatribes. I don’t know how common that is but I wonder if an effective way to get people to stop holding their psych as a well intentioned informative expert is to have them get ahold of their records. Don’t even have to phrase it as anti-psych can just say “seeing your entire records can help facilitate improving your mental health.l
Report comment
.
Report comment
Dear Peter,
I appreciate the information you have shared with us. What about the people who are not given the choice to reject the drugs? I for one had my civil rights taken away from me and my medical care choices were given to my mother. I had to take the drugs and pretend they are working to avoid worse treatment like electroshock. I am not at the point where I can perceive the drugs doing damage to my motor skills but the psychiatrist won’t budge and won’t let me off the olanzapine
Report comment
According to the Congressional Research Service there is no law in the United States that requires the American Psychiatric Association to even try to restore the mental health of its patients. The APA is free to choose whatever approach they like – and, clearly, what they like is the approach that brings them and their business buddies, the drug companies, the highest profits. Drugs aren’t designed to cure anyone – just suppress symptoms. Mental healthcare is mainly an attempt to turn patients into lifelong customers of psychiatric goods (drugs) and services (talk therapy). I used the orthomolecular approach, acupuncture, and homeopathy to cure my loved ones so I was happily able to kick the psychiatrists and their nasty drugs out of our lives. Best thing I ever did. Linda, from Youtube “Linda Van Zandt’s Mental Health Recovery Channel; Facebook “A Dose of Sanity;” and author of The Secrets to Real Mental Health (about orthomolecular treatment)
Report comment