
By the mid-19th century, the nascent field now known as psychiatry had begun to attempt to explain symptoms of mental distress with impaired nervous structure. Early experts tried to draw a direct link between physiology and psychology. This was the birth of the “medical model,” which compares mental illness to physical ailments and implies that they, too, can be addressed medically. This theory—which has now become the dominant paradigm for understanding emotional distress—assigns psychiatric disorders to neurological, biological, or hereditary causes.
You may think that modern psychiatry has advanced far beyond the clumsy attempts of early practitioners, with their lobotomies and insulin shock therapies. But the truth is that the basic assumptions behind those early attempts still inform psychiatry’s main treatments today. Biological-based interventions such as psychopharmacology (drug-based therapy), electroconvulsive therapy (ECT), or psychosurgery (brain surgery) are the direct descendants of treatments that are now considered inhumane and were based on guesswork that has still remained unconfirmed.
Similarities between past practices and modern psychiatry
ECT
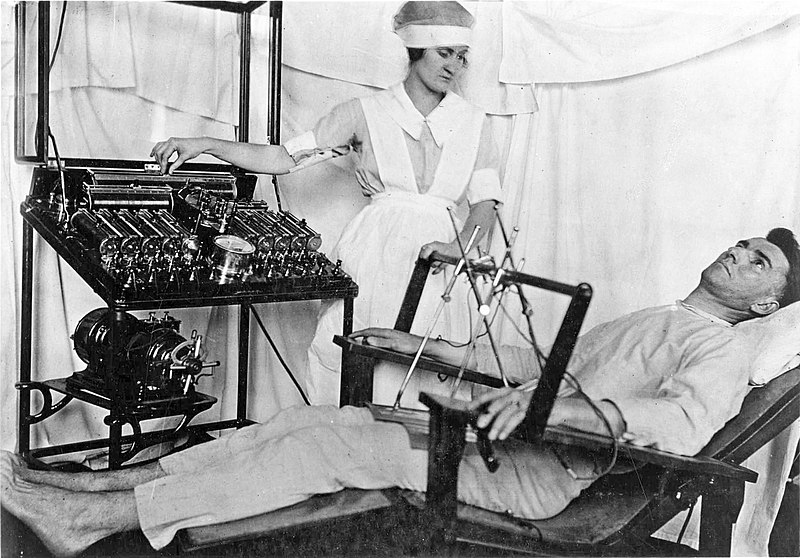
Electroconvulsive therapy (ECT) is perhaps the most obvious example. ECT has been continuously used with only minor changes since the time of the lobotomy. The purpose of ECT is to trigger seizures, which are theorized to somehow cure a depressive state. This theory has been in circulation since long before any knowledge of neurology—see, for instance, drug-induced shock therapy, which was approved by the FDA until 1982. It’s also little different from insulin shock therapy, although there the goal was coma instead of seizures.
ECT is a procedure in which an electrical current is passed through the brain in order to induce seizures. Advocates of ECT argue that it is the safest and most effective cure for major depression. However, studies have found that ECT is ineffective for reducing suicide—its main indication—and no evidence that it’s effective for depression, either. The studies themselves were of poor quality with inconsistent results.
Moreover, memory loss occurred in up to 79% of participants. Studies have also found that one-third to one-half of people receiving ECT were not given appropriate informed consent or were forced into the procedure.
The only real difference between modern-day ECT and its 1940s counterpart is that it is now administered under anesthesia as opposed to the past, which means that risk of physical harm during the seizure itself is reduced.
ECT’s target demographic today is older depressed women—interestingly, the same demographic as the lobotomy and the diagnosis of hysteria.
Psychosurgeries
At the forefront of current medical “treatments” for psychiatric “disorders” are psychosurgeries, such as deep brain stimulation and anterior cingulotomy. What separates these surgeries from the prefrontal lobotomy? They operate on the same principle—a guess as to where the supposed “disorder” is located in the brain, followed by a tool for destroying that part of the brain. The difference is merely that the lobotomy was more aggressive, destroying more of the brain.
But the lobotomy, too, was once considered the height of scientific practice at the time, and its critics were considered anti-science quacks—just as critics of current practice are now.
Interestingly, the cingulotomy was initially proposed in the 1940s and was viewed as little different from a lobotomy. While lobotomies involved severance of the connections in the prefrontal cortex through the insertion of a long needle through the eye socket, cingulotomy involves severing the circuit in the cingulate gyrus of the brain that processes emotions and regulates behavior. Current cingulotomies are performed using an electrode or gamma knife to cut or burn a half inch of the brain.
This has obvious implications on the emotional capacity of a patient. As with the lobotomy, “side effects” of this targeted brain damage include apathy, memory loss, seizures, nausea, and—perhaps obviously—intense headaches.
Moreover, the inability to understand the consequences of behavior is the most important of all the consequences of a lobotomy and by extension, cingulotomy as well. In fact, it could be argued that this is essential to the procedure. The cingulotomy is currently used in patients with the diagnosis of OCD—who are terribly afraid of the consequences of potential actions. Thus, destroying the part of the brain that connects action to consequence may leave them apathetic, but it also may remove their fears.
While the implications of lobotomy were recognized as evident human rights violations, the same has not been the case regarding the newer procedure.
The similarities between the two procedures are so eerie that they extend to the arguments doctors have used to further their cause. Despite the obvious question of ethics, psychiatrists continued to argue in favor of lobotomies through the mid-20th century. Although early practitioners openly admitted that the lobotomy wasn’t perfect, they still argued for continuous experimentation in this surgery—and against its regulation.
Consider, for example, these words from 1937:
The hypotheses underlying the procedure might be called into question; the surgical intervention might be considered very audacious; but such arguments occupy a secondary position because it can be affirmed now that these operations are not prejudicial to either physical or psychic life of the patient, and also that recovery or improvement may be obtained frequently in this way.
Another common argument was that, without advancement by research and practical experimentation, the potential benefit of lobotomies will never be understood. However, no law could help deter rare violations without restricting such experimentation. The public interest would be served only by resisting regulatory restraints and relying on the medical profession’s protocol and high discretion for patients’ safety.
A similar argument has been offered for newer procedures like cingulotomy. Doctors continue to argue that scientific progress is only possible through unbridled experimentation. This translates to the belief that it is acceptable to reduce patients to a mere statistic of “surgeries-gone-wrong” as long as it could yield interesting experimentation results.
Institutionalization
When the concept of the “asylum” was introduced in Europe it entailed a relatively moral care system of patients based on the belief that those suffering from mental illness could heal and eventually be cured if they were treated gently and in ways that spoke to the reasonable parts of their minds. This approach was entirely forgotten and radically changed with the introduction of public mental institutions.
Even though institutionalization was introduced in the early 19th century, the current era is even more rampant with human rights violations in such facilities. According to the World Health Organization (WHO), when human rights commissions toured many mental institutions in Central America and India, they discovered “atrocious and intolerable” conditions.
Many other mental institutions around the world, in developed as well as third-world countries, have similar conditions. Putrid living quarters, dripping roofs, overflowing toilets, crumbling floors, and damaged doors and windows were among them. The majority of the patients who were surveyed were dressed in pajamas or were completely naked. Many patients were seen bound to beds in tiny areas of psychiatric wards where they were left to sit, walk, or lie on the concrete floor all day. They were also constantly referred to as “inmates” rather than “patients.”
This is an obvious indication of the change in perception of people with severe mental distress. The aim of such institutions is not healing; rather, it is segregation of the “insane and untamable” from the society. Patients with mental illnesses were often treated far worse than criminals in such asylums.
The situation in India is much worse than in countries like the USA due to extreme overcrowding in mental institutions and a major lack of proper understanding of mental illness. Further, according to the study, approximately one-third of those in mental institutions did not have a psychiatric diagnosis to warrant their stay. There have been constant insinuations that mental institutions have largely been used to confine political dissidents.
Even in the US and UK, however, where living conditions in psychiatric institutions are much better, the lack or even violation of consent is prevalent. United Nations guidelines state that informed medical consent is a categorical right for everyone. However, in complete contrast with other branches of medicine, there is a complete disregard for consent when it comes to mental health; especially regarding institutionalization.
Due to the lack of delineated laws on the role of consent in mental healthcare, it is generally legal to force a patient to be institutionalized regardless of whether he agrees or not. A common trend in India is a person being institutionalized solely at the request of family members. This has often been used as a ploy to gain an upper hand in property or other familial disputes. There is absolutely no consideration of whether the person consents to be institutionalized or not.
This is an absolute violation of human rights that has been disregarded by public debate and psychiatry at large.
Adverse effects of gross medicalization
The medical model’s linking of physiology and mental health promotes ignorance of the role environmental factors play in this regard. It has time and again been shown that the distressing experiences labeled as depression, anxiety, etc. are inexorably linked to trauma. In fact, perhaps obviously, stopping traumatic experiences has been demonstrated to resolve emotional distress.
The strong nexus between environmental factors and mental distress is widely accepted in psychology and counseling. Trauma-informed psychotherapy, for instance, is a mainstay of the psychology field. But psychiatry sees things differently.
Instead of providing trauma-informed care, psychiatry—and the medical model at its foundation—relies on gross medicalization of patients. Although the evidence for this model’s success is limited (for instance, in 49% of antidepressant trials, the drug was no better than the placebo; long-term outcomes are also worse for people taking the drugs), it is widespread.
This completely separates the psychological state of a patient from social/environmental factors that may affect it. The medicalization of mental illness refuses to acknowledge the varied psychological consequences of different social issues. It aims at a “one size fits all” approach that tries to categorize individuals into distinct compartments of mental disorders solely based on common symptoms and ignoring the root cause.
But without addressing the social cause of distress, it is impossible to assuage it. For instance, in India, only when the oppression faced by the scheduled castes is addressed can the trauma of that oppression be mitigated. Unless we address societal factors, we cannot appreciate the different psychological implications and address them according to their distinct natures. The influence societal factors have on mental health means that mental distress should be revaluated as psychosocial distress rather than “illnesses.” They should not be put in the same category as physical illnesses.
Conclusion
Medicalization of mental health has led to not only to ignoring social factors in mental health, but also egregious human rights violations. Just as it has in the past, psychiatry has found ways to bypass rights in a more subtle manner. Constantly claiming the progression of scientific knowledge and implying that treatments have radically changed cannot hide the fact that the foundations of current treatments are no different from the unethical and horrific interventions of the early 20th century.
When analyzed closely, ECT, institutionalization, and other mainstays of psychiatry are replete with instances of human rights violations just like their predecessors in the past. This issue can only be addressed when psychiatry is no longer perceived as the primary method of intervention for mental distress. Only then will the veil over it be lifted.
Social intervention—which offers a more individualized approach without pigeonholing an individual’s symptoms into strict categories—needs to become more prevalent. This requires refocusing the approach to mental health to the cause—working to address inequality, injustice, and childhood trauma—as well as providing trauma-informed healing practices.














A lot has changed. They have become much more dangerous and powerful.
The governments have to do something, but then we won’t find the bodies
stacked under old institutions, so no evidence.
No they are littering the countryside, their families uprooted and displaced.
Report comment
Psychiatry has had a long battle with itself to find and justify its place alongside actual medical professions which were founded on and supported by scientific knowledge. When you, for example, claim that poor sleep and poor eating are both symptoms and causes of an “illness” (depression) then don’t be surprised why you have become the laughing stock of the medical and scientific community.
The Royal Australian and New Zealand College of Psychiatrists – https://www.yourhealthinmind.org/mental-illnesses-disorders/depression
Report comment
This is something that must be repeated in MIA.
The ‘critical psychiatry’ implies that there is a system somewhat elaborate enough to be warranted criticisms and benevolent enough to be corrected instead of being simply uprooted.
The blunt truth is that psychiatry, for all its existence, never ceased to be a crude and ignorant crook that people enabled because of the various illusions and benefits they get from it.
Its not a modern and flawed cathedral, and never ceased to be a grotesque hut of horrors.
It is sad and even scandalous that so many ‘critics’ make it, willingly or not, more respectable that it is.
Psychiatry, at its core paradigm and effect, is just a turd.
On a side not, this article sadly missed the opportunities of citing drugs as a category. There is no advance since the early XX century barbiturates, or even opium.
Thats the proportion of the turd.
Report comment
Neuroleptic drugs were described by psychiatry as a “chemical lobotomy” until lobotomies were recognized for what they were. This earlier description was accurate in the sense that these drugs cause brain damage to everyone taking them.
Psychiatry when not denying/ignoring the science often claims that this brain damage is helpful. Benzo type drugs, “antidepressants” cause dementia/brain damage as well.
Lobotomy equaled giving people brain damage and calling it medicine.
Psychiatric drugs equals giving people brain damage and calling it medicine.
Maybe someone else can give the term for psychiatry saying people “lack insight” and are too stupid to know that brain damage is good for them.
Report comment
First; with all due respect to the author: the title: “How far psychiatry really come? Historical Practice versus Modern-Day Psychiatry.” is at best an “oxymoron” at worst, a question-mark. Second, and I believe Willoweed noted this: there was no mention in this article of the us of neuroleptic drugs or any of the drugs these psychiatrists prescribe. Considering that this is the treatment modus operandi of these psychiatrists, why was this omitted from the article? This is tragically telling. In my opinion, the fact that this drugging of their patients was left out of the article reflects that psychiatry has essentially gone nowhere, but backwards, way backwards. But, then how can something truly progress forward when it is illegitimate and an out and out fraud that makes “snake oil salesmen” look like real doctors and places the proverbial used car salesmen above the common petty criminal? Please, there is no difference from the past except that they use “Chemicals” (“drugs”) to do what the lobotomies and other surgeries and treatments did in the past? No difference. No progression. All a waste of not only time and money, but good human beings who could make contributions to society to make it a better place. But, why make society better, because it would be these psychiatrists out of business? Huh! Thank you.
Report comment
(Duplicate comment).
Report comment
olaveivind 55 year
The voice intones, “you’ve just had a heavy session of electroshock therapy, and you’re more relaxed than you’ve been in weeks. all those childhood traumas, magically wiped away…along with most of your personality.” – The orb «Alles ist Schoen», from the mini album Pomme Fritz.
Report comment
If I were to write an article it would be titled I’m So Bored With Mental Health. The Mental Health business is primarily concerned with selling “Mental Illness”. Think…Lobotomy, ECT, harmful drugs, endless talk, etc. Maybe this “Mental Illness” is a product I don’t really need (and by that I don’t mean “luxury”). Mental Health, on the other hand, is an abstraction. The only people who need Mental Health are those deemed to be Mentally Sick. When you don’t buy Mental Illness, you’re already there (i.e. mentally healthy). Of course, given guardians, ECT, radical brain surgery, bleeding, endless talk, etc., wising up can be a difficult undertaking. Any of those out there who aren’t wise to the system yet have my deepest sympathy. I hope you can come through it relatively intact, and by that I mean I hope you can manage to leave the system, and not in a body bag.
Report comment
Psychiatric “diagnosis” is a self-fulfilling prophecy. It works just like a placebo. When people are told they have a terminal illness they get miserable because of it. Just like when they are told and believe they have an ill brain and will be mentally ill for life they get miserable.
The people around them then treat them as mentally ill resulting in stigma, discrimination, stress and social difficulties. There is less motivation to change aspects of ones life because doing so won’t fix a chemical imbalance. Instead of partaking in pleasurable or productive activities the “mentally ill” are told to go to therapy where this self fulfilling prophecy is reinforced. Talking with friends or family results in a response containing “take drugs” and “seek help.”
The mental illness industry lies to people to make them feel powerless and hopeless and uses that fear to make people dependent on them. This goes so far as addicting people to deadly, cognitive impairing drugs that worsen outcomes. The most effective step out of this cycle is to recognize that in the medical and biological sense “mental illness” isn’t real. People struggle to do this because they’ve been manipulated to think the only way suffering can occur is if it is a brain disease. They think it is insulting if you don’t tell them they have inferior brains.
Report comment
Willoweed: What you say is tragically correct. In fact, the psychiatrists and their buddies want to make you think your suffering is good. Also, the horrifying thing is when you go see them you don’t have a brain disease, but they convince you that you do; then they give you their drugs, reinforce those drugs with therapy and other stuff they come up with (I say come up with because that’s not like using one’s creativity at all) and then, guess what, your brain becomes diseased or the better words are damaged or injured. So, you go in their offices-healthy-they convince you, you’re sick–they give you drugs, etc. because they say you are sick–then you get sick from the drugs. And the cycle continues. The only way to save yourself is to get off the drugs and walk away from them (renounce them). Of course, that might be easier said than done. But, it is possible. And, when you do that– no matter the suffering (withdrawal) and then, later, adaptation to living with this brain damage, you will be free of their terror. Just don’t get yourself caught up in that evil again. That’s all I can say. Thank you.
Report comment
Removed for moderation.
Report comment
Great article with a thoughtful conclusion:
“Medicalization of mental health has led to not only to ignoring social factors in mental health, but also egregious human rights violations. Just as it has in the past, psychiatry has found ways to bypass rights in a more subtle manner. Constantly claiming the progression of scientific knowledge and implying that treatments have radically changed cannot hide the fact that the foundations of current treatments are no different from the unethical and horrific interventions of the early 20th century.
When analyzed closely, ECT, institutionalization, and other mainstays of psychiatry are replete with instances of human rights violations just like their predecessors in the past. This issue can only be addressed when psychiatry is no longer perceived as the primary method of intervention for mental distress. Only then will the veil over it be lifted.
Social intervention—which offers a more individualized approach without pigeonholing an individual’s symptoms into strict categories—needs to become more prevalent. This requires refocusing the approach to mental health to the cause—working to address inequality, injustice, and childhood trauma—as well as providing trauma-informed healing practices.”
Report comment
I am not sure how to put this; sometimes, I get took the wrong way. From some of the reading, I have been doing, it appears that psychiatry is “making a killing” out of shaming peoples into false diagnoses, when, hidden inside those very false diagnosis are very probably our natural gifts and talents when they don’t try to drug and therapize all these people, they could use these natural gifts and talents to make the world a better place. Of course, sometimes, people get shamed at the friend and family level or over social media, now. That kind of shaming can lead some to the psychiatrist and his or her bag of drugs and therapies. It is a definite tragedy that they are doing this; because, yes, it hurts the “patient” and probably the “patient’s family” but it also hurts the very world in which we live. I guess this is the tragic millstone psychiatry must bear into eternity. Thank you.
Report comment
“hidden inside those very false diagnosis are very probably our natural gifts and talents when they don’t try to drug and therapize all these people, they could use these natural gifts and talents to make the world a better place.”
That is exactly right. It is a crime against humanity for this very reason.
Report comment
This article by this young student from India is a good synopsis of what continues to be wrong with this “profession.” None of this should be news to us.
The younger generation still wants to get this right. This young woman plans to study criminal (forensic) psychology. And I know another woman here in California about the same age who also wants to study this subject. I hope they know what they are getting into! This is the legacy of Robert Hare, Stanton Samenow, and some more recent others. It is a rough and unsettling subject. The focus is on psychopathy, as it rightly should be, I suppose. And while I think these people are on the right track, their intellectual boundaries make attaining their goal more difficult, if not hopeless.
I recently saw sociopathy defined as learned psychopathy. By implication, the sociopath could be “re-educated” and returned to a non-criminal life. This has been accomplished in many prisons, according to reports I am aware of. The psychopath remains the tough nut to crack for this society. He is always taking over the systems we design to restrain him! And this is what we have seen with psychiatry.
Report comment
The idea that psychiatry has advanced, become legitimate, or science-based, or more compassionate/humane,… That it’s goals and procedures are any different than they were at any point in the past…an idea which seems to be widely accepted in the public sphere: this idea makes psychiatry that much more dangerous.
Whenever I hear or see the messaging, “if you feel suicidal, depressed, anxious, blah blah blah…don’t be afraid to ask for help. There is help available” I want to shout, “Do be afraid to ask for help. Be very afraid.”
Report comment
My daughter then aged 32 had just recovered from a 3 months long depressive episode and was having more difficulty sleeping. She had been taking Ambien for over two years prescribed by her psychiatric PA and he added some Tegretol and Seroquel in the guise of helping her sleep. Well, when those additions didn’t result in more/better sleep my daughter began to panic afraid she would become manic.
I should have talked her out of seeking a hospital stay on a psych ward. She had been on one of those three times before: her junior year of college, the following year at about the same time (July 4th) as the previous year-both those admissions were involuntary and occurred during so-called manic episodes on campus. Her 3rd admission was voluntary because she wanted to get off her Ativan dependence.
She thought the psych unit could prevent another manic episode and voluntarily admitted herself. She made the mistake that cost her her life. When the psych resident and staff recognized she wanted a say in her care including whether she be given “meds” they switched her to involuntary commitment. They forced her to take Zyorexa and Lithium, and then took away Zyorexa and replaced that with Risperidone (I told them Risperidone made her zombie-like on her 1st psych admission 10 yrs earlier and I was ignored). I and her dad watched helplessly as she became twitchy and unable to hold eating utensils. This all took place in supposedly the best public hospital in North Carolina. When I begged her physicians to stop the Risperidone and Lithium I was told she’s “not rigid” so she”ll be alright. They also refused to get a cardiac consult for her tachycardia.
Patients have no rights when they get on the psych unit. Parents who know their children better than anybody are ignored or placated enough to keep quiet.
Jill died 2 weeks after she admitted herself falsely believing our current in patient mental health system could help her. There were no lawyers willing to help me get her out of the hospital and after her death no lawyers wanted to take the case but one.
In North Carolina, in cases like Jill’s the lawyers have to find a similar institution willing to review the “psychiatric care” Jill received. The consulting psychiatrist deemed the “care” jill received met the “standard of care”. Therefore there is no justice for my daughter. I had 2 years from the date of her death to seek justice and time ran out.
I want the in patient psych unit to change. Prisoners are treated better than in patient psych patients. How do I go about bringing change to the psych unit experience for the people who are suffering?
Report comment
Wow, that is a horrible story! I am so sorry you have had to deal with this level of abuse and idiocy!
I really believe the only way any of this will change is when it starts costing them more money than they are making. We need some kind of class action lawsuit where psychiatrists and drug companies and hospitals and insurance companies (especially insurance companies!) have to pay for their errors in big money.
My sincerest condolences on your loss.
Report comment
The fight to restore sanity to this planet has been a long and difficult one. I still hope that sanity will prevail in the end. But we have a lot more to learn about how to restore sanity to an individual or a society. It seems obvious that a sane society must be composed of sane individuals.
Report comment
Peanut, This is heartbreaking and maddening. I’m so sorry for your loss. Your daughter Jill did what she thought was right, what we are all repeatedly told is right — to seek help, to trust in the doctors and the system. Her trust was betrayed in the worst way. It sounds like you and Jill’s father, did everything you could to support and protect Jill from a system that is so inhumane and consequence-blind. It isn’t right. My sincere condolences.
Report comment