

On April 20, 1999, the mass shooting tragedy at Columbine High School signaled the beginning of a rising tide of violence that America has not yet figured out how to stem. News media coverage following mass shootings has overwhelmingly named serious mental illness (SMI) as the causal factor, despite the fact that research has not found that to be so.
The most-widely cited research conducted by Swanson et al found that only 4% of violent behavior towards others can reasonably be attributed to SMI; in other words, 96% of American violence is due to factors unrelated to diagnosis.
A 2014 study in the American Journal of Public Health analyzed a random sample of 25% of news stories on SMI and gun violence published in the national and regional news from 1997 to 2012. During this time period, the study found that “‘dangerous people’ with SMI were more likely than ‘dangerous weapons’ to be mentioned as a cause of gun violence.”
A subsequent study published in Health Affairs last year found that public associations of schizophrenia with violence rose “significantly” from 1996 to 2018. By 2018, over 60% of survey respondents associated schizophrenia with dangerousness, and as high as 59% supported coercive treatment.
The study’s authors concluded: “These findings reflect political discourse, not scientific data, and could lead to policies that would be ineffective and misdirect the search for the underlying roots of violence.”
Questioning the Dominant Narrative
On February 3, the Coalition for Smart Safety and the Consortium of Citizens with Disabilities (CCD) co-organized back-to-back briefings in the House and Senate to provide background and education about the pervasive myth linking gun violence and mental illness.
Comprised of leading local, state, and national disability rights, civil rights, education, mental health, and privacy organizations, the Coalition for Smart Safety formed last year “with the shared goal of affirming that mental health disabilities are not predictors of gun violence and should not be the focus of gun violence prevention proposals.” CCD is the largest coalition of national organizations “working together to advocate for federal public policy that ensures the self-determination, independence, empowerment, integration and inclusion of children and adults with disabilities in all aspects of society.”
Despite the nation’s laser focus early last week on the final days of the impeachment trial, both briefing rooms were packed with staffers and advocates. On the House side, the briefing was presented in conjunction with Reps. Grace Napolitano (D-Calif), and Jim Langevin (D-RI), both members of the House Gun Violence Prevention Task Force. The House briefing was livestreamed by the National Parent-Teacher Association.
An identical briefing followed on the Senate side, presented in conjunction with the offices of Senators Richard Blumenthal (D-CT), and Bob Casey (D-PA).
Mental Illness Low On List of Causal Factors
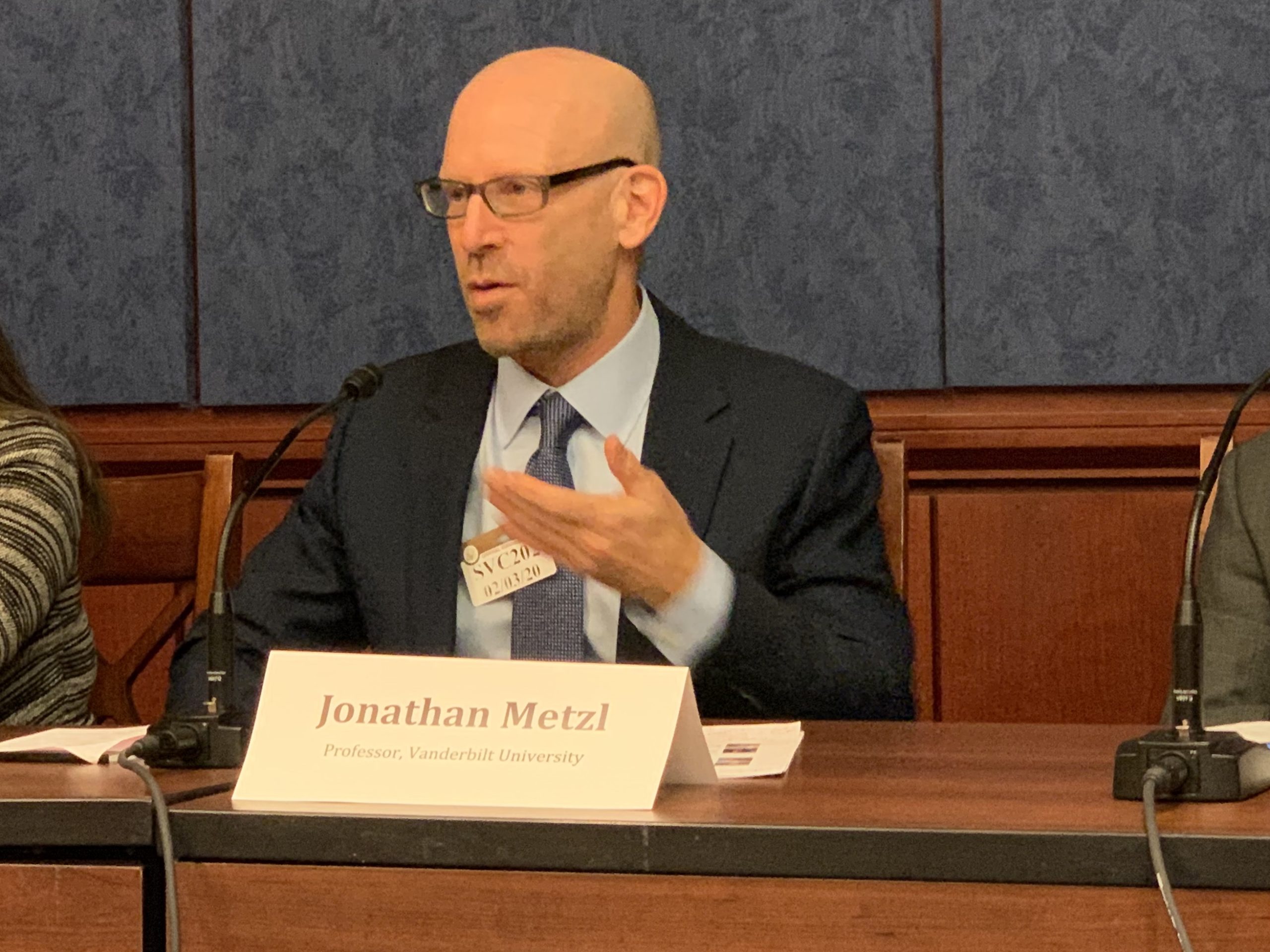
Jonathan Metzl, author, psychiatrist, and director of the Center for Medicine, Health, and Society at Vanderbilt University, provided an overview of the research evidence on gun violence and mental illness. Metzl, who is also research director of The Safe Tennessee Project, a nonpartisan gun safety organization, and a frequent media commentator on mass shootings, said that in the aftermath of the Sandy Hook tragedy that “every time there would be a mass shooting, there would be some politician who would basically say, ‘This isn’t a gun problem. This is a mental illness problem,’ followed by a seemingly endless slew of media saying, ‘This disorder caused the mass shooting.’ I kept getting asked the question, ‘Does mental illness cause mass shootings?'”
Metzl is not unsympathetic to this gut reaction. “The aftermath of a period of mass shooting is a moment of terror, right? This idea of creating some boundary between ‘us and them,’ some kind of lingua franca that ‘only a crazy person would commit an act like that,’ is an understandable response.” He added that with a number of mass shooters, there were histories of psychiatric symptoms, adding to the pervasiveness of the myth.
However, as Metzl began to dig deeper into the data, he found that prevailing stereotypes and reality simply did not match up. “I started to list out the many factors that went into a mass shooting,” he said. “And the factors were things like the availability of firearms, substance use, recent firing from a job, trauma, things like that. Mental illness is often number 15 or 20 on the list. And so it was increasingly problematic, I thought, that mental illness was being isolated as being this one causal factor.”
Metzl’s research went even further to reveal the opposite of the “violent madman” stereotype so ingrained in public consciousness. “There was a lot of data that I thought was convincing, which was showing that people with diagnosed mental illness were actually less likely to shoot somebody and less likely to commit mass shootings,” he said.
This is partly because “negative symptoms” that can lead to a diagnosis, such as low energy, low mood, and disorganization, were actually protective factors against committing violence, because people having these experiences were less likely to be out in public, Metzl explained.
“Here was another example of the stigmatization being really at odds with what was happening in the real world,” he added.
Metzl said that psychiatrists are likely to be “poor predictors” of whether an individual will become violent, at least in part because “the population of patients that psychiatrists are seeing are less likely than a more dangerous group—the sane—to go shoot somebody else.”
For Metzl, the concern is that when people make the erroneous link between mental illness and gun violence, they are less likely to pursue solutions that address the true root causes of gun violence. Instead, they are more likely to focus on getting better at predicting who will be the next “ticking time bomb,” he said.
While Metzl did not mention it by name in his remarks, last year just such a proposal made headlines. Bob Wright, head of the Suzanne Wright Foundation and a friend of President Trump, floated a proposal to the White House called Stopping Aberrant Fatal Events by Helping Overcome Mental Extremes (SAFEHOME). According to this proposal, SAFEHOME would be part of a new agency, the Health Advanced Research Projects Agency (HARPA), modeled after DARPA, or the Defense Advanced Research Projects Agency.
With an estimated price tag of $40-60 billion, SAFEHOME is supposed to utilize tracking software to detect signs of “mental health” concerns that could portend mass shootings. But according to Jessica Baron, a tech ethicist who blogged about SAFEHOME as “pseudoscience:” “just because we have AI and machine learning that can process massive amounts of behavioral data doesn’t mean it actually works.”
Metzl concluded by stating that we as a society need to be asking much broader cultural questions about gun violence, such as “Why do we need so many guns in the first place? Why do people mistrust each other?” and “What do guns mean to the population of gun owners?”
Since the year 2013, there have been more guns than people in America, making the country an outlier among all the world’s nations.
A Societal Belief That Is Just “Completely Wrong”
Josh Horwitz, director of the Coalition to Stop Gun Violence (CSGV) which develops and advocates for evidence-based solutions to reduce gun injury and death, admitted that he had once believed in the link between mental illness diagnosis and mass shootings. After bringing together experts who showed him the data, he now feels that the idea of mental illness causing mass shootings or violence in general is “just completely wrong,” adding: “I’ve had to change my thinking about it after about 23 years of doing this.”
Horwitz explained that gun violence is complex and multifactorial, encompassing interpersonal and intimate partner violence, suicide, police violence, and accidental deaths. Therefore, there is no one cure. As far as policymaking at his organization, Horwitz no longer gives the mental illness link any credence. “I don’t spend any time on that,” he said.

From an epidemiological perspective, Horwitz noted that if there are nearly 45 million people in America diagnosed with a mental illness in any given year, the likelihood that any one person in this group would use a gun to commit a homicide is extremely small.
“Thinking about screening 45 million people for things that they are not a risk for is a gigantic waste of resources,” Horwitz said. “When we think about stopping gun violence, focusing on people who are less likely to be violent makes zero sense, and it’s also incredibly stigmatizing.”
“What we need to do is focus on the real risks of gun violence,” he added. Known risk factors unrelated to psychiatric diagnosis or disability include alcohol or drug misuse; a prior history of violence; being male and young; and a recent relational, social, work or financial loss.
While alcohol and street drugs are commonly associated with an increased risk of committing gun violence, psychiatric medications were not mentioned at the briefing and are rarely included in media or academic discussions of mass shootings. Yet psychiatric drugs, most notably antidepressants, have long been associated with an increased risk of violence in a percentage of individuals, with several mass shooters having taken such drugs. As early as post-Columbine in 1999, psychiatrist Peter Breggin warned about a possible connection, as one of the shooters was taking the antidepressant Luvox at the time.
Author and sociologist Anthony Ryan Hatch, who wrote about psychiatric drugs and interpersonal violence in his book Silent Cells: The Secret Drugging of Captive America, told Mad in America last month: “I think that more research needs to be done to try to figure this out. Because this combination of widespread societal psychotropic drug use and the mass availability of weapons is creating a situation where far too many of us are dying and being injured. Although it’s very difficult for me to say that A causes B.”
While Horwitz acknowledges that there is no singular cure for gun violence, his organization has been focused on a specific set of policy reforms: “extreme risk protective orders” (ERPOs), also known as “red flag laws” or “gun violence restraining orders (GVROs). As of this writing, such laws have been passed in 17 states and the District of Columbia.
ERPOs have been implemented in a variety of ways. Some laws discriminate on the basis of psychiatric disability and diagnosis, and some focus only on non diagnosis-specific risk factors. New York’s 2013 SAFE Act is one of the earlier and more controversial ERPO laws, as it requires mental health professionals to report on individuals who are “likely to engage in conduct that would result in serious harm to self or others, regardless of whether a legal firearm is implicated,” even though mental health professionals are typically poor predictors of violence.
“Think of a domestic violence restraining order, except it’s available to any family member,” Horwitz explained. “That family member can say ‘my loved one’s at risk’ because of evidence-based risk factors of violence: past acts of violence, threats of violence, drug or alcohol abuse, impulsive anger.” He added, “The studies are pointing in the right direction that these laws that are focused on the actual risk factors, rather than mental illness, are saving lives.”
“We have to stay focused on the facts.”
Kelly Vaillancourt, director of policy and advocacy with the National Association of School Psychologists, shared her concerns about mental health services in schools being touted as the solution for school shootings. “If we’re really going to be serious about tackling the issue of gun violence, we have to stay focused on facts,” she said. “To conclude that a child or an adolescent who is exhibiting symptoms of depression or anxiety is more predisposed to commit an act of violence does nothing but perpetuate an incorrect stereotype.”
“What we absolutely have to move away from is the notion that we provide school mental health services because kids with disabilities or kids who have a mental illness are violent,” Vaillancourt said.
Vaillancourt mentioned her organization’s concerns about policies that profile students on the basis of disability or diagnosis. “It is completely inappropriate for schools to be using any kind of profile to say, ‘Oh, you’re a student with a disability, therefore you must need these types of services.’ Or, ‘you’re a student with a mental illness. Therefore, we automatically assume that you pose a threat of violence.’”
One example, not specifically referred to by Vaillancourt, is the “school safety” policy implemented in Florida in the wake of the Parkland shooting, which sparked controversy over a requirement that students disclose past referrals to mental health services when registering for public schools. Writing about this law for the Center for American Progress (CAP), Azza Altiraifi and Valerie Novack warned: “This policy will disproportionately harm marginalized students, especially those who may exhibit aberrational behaviors as a result of a disability but who pose no actual threat.”
Vaillancourt said that her organization is hearing about such discriminatory policies being enacted around the U.S. “I strongly encourage those of you that are in communities where you’re hearing this is happening to do everything you can to stop it. Because that is not how we should be addressing school mental health.”

The final speaker was William Kellibrew, director of the Office of Youth and Trauma Services with the Baltimore City Health Department, which has helped to train thousands of city employees, community leaders, organizations in trauma-informed approaches.
Kellibrew shared his personal experience as a survivor of a gun violence tragedy that claimed his mother and brother. “It shaped the rest of my life,” he said. He spoke of being misunderstood by teachers and bullied by other students for staring out the window and for other behaviors he developed in the wake of the traumatic events.
Searching for news reports of his family tragedy a decade after the fact, what struck Kellibrew was a report in the Washington Post that described him as having witnessed the shooting but as being “unhurt.” Kellibrew said, “It actually crushed me 10 years later to know that that was the report about my experience. I was far from ‘unhurt.’ I was devastated.”

Kellibrew has learned through his life and work that “healing and recovery are possible.” He emphasized that “managing and struggling with mental health challenges is not a death sentence, or something that we should be afraid of. Nor should it prohibit us from living our best lives. What prohibits us from living our best lives is when we lack the support, and we’re attacked with labeling and stigma about who we are.”
He concluded that for young people who have survived traumatic events, “getting support as fast as we can to go ‘upstream’ and address some of the challenges is important, but (surviving a traumatic event) certainly isn’t a predictor of violence. I’m sitting right here with you.”
Kellibrew added: “I’m just glad to be part of a framework that says that these things aren’t connected in the way that people are connecting them.”
Debunking the Master Narrative
During the panel discussion, Jonathan Metzl mentioned that as someone who often engages with the media as a commentator, he has begun to notice some improvement in how mass shootings have been reported over the last decade. “I remember when I first started this, I would get asked questions like ‘What’s the diagnosis of the shooter?'” he said. “Another one I remember was: ‘Is Asperger’s linked to a higher risk of mass shooting?’ I do think we’ve gotten much more nuanced about this as a society.”
Metzl referred to the racialized dimension of the media and public rhetoric around mass shootings, which also has gotten more attention in recent years. “There’s a politics to which kinds of mass shootings get called ‘mass shootings caused by mental illness,’ and which ones get dismissed as ‘gang-related’ or ‘drive bys,’ (which is) just kind of an easy shorthand for ‘urban violence.'”
Discussing the media stereotype of the mass shooter as a “white mentally ill loner,” he explained how it “plays into all of these kinds of historical stereotypes about whiteness and intellect and factors like that. And it leads to calls to stop these kinds of shootings. But particularly when the victims are from communities of color, it never gets called ‘mental illness.’ It’s very quick shorthand for ‘there’s nothing we can do about it because it’s not a disorder of the brain, it’s a disorder of the neighborhood, it’s a disorder of the culture,’ or things like that.”
Metzl added, “There’s a long history of what gets called ‘mental illness’ being divided along racial lines.”
He also noted that a narrow focus on changing the media narrative may miss another important aspect of this issue. “The media is also reporting on gun laws. So I think part of the issue is that it’s not just enough to tell the media to do a particular thing. It’s actually linked to pushing for more responsible gun laws.”
He added, “I think that in a way, the media here sometimes deflect from the judiciary here, and what kinds of laws are being implemented.”
The latest Federal legislation to link SMI and violence is S. 2690, Sen. John Cornyn’s (R-TX) Restoring, Enhancing, Securing, and Promoting Our Nation’s Safety Efforts (RESPONSE) Act of 2019. The RESPONSE Act was introduced into Congress last fall following two back-to-back mass shootings in Cornyn’s home state of Texas last August. Cornyn’s legislation focuses on access to mental health treatment, including involuntary treatment; increased surveillance of America’s schoolchildren; and greater collaboration between mental health and law enforcement authorities. The bill currently has seven Republican co-sponsors.
The RESPONSE Act is similar to former Rep. Tim Murphy’s Helping Families in Mental Health Crisis Act, bipartisan mental health legislation introduced in 2013 following the Sandy Hook tragedy. Until Murphy resigned from Congress in 2017, the Republican Congressman and psychologist from Pittsburgh appeared in the press after every mass shooting, blaming people with SMI for gun violence. Murphy currently serves on the board of directors of the Schizophrenia and Related Disorders Alliance of America (SARDAA).

Maria Town, President and CEO of the American Association of People with Disabilities (AAPD) served as the moderator for both briefings. “We need to make sure we’re actually centering the voices of people with psychiatric disabilities in these conversations,” she said. “That speaks to making sure we’re telling the whole story.”
Town added, “All too often, you hear from everyone else but people with psychiatric disabilities.”
Correction: The original version of this article stated that the briefing was also held in conjunction with Senator Patty Murray’s office, but that was in error.
****
MIA Reports are supported, in part, by a grant from the Open Society Foundations
Everybody on here knows it’s psych drug toxicity. So long as we have BS after more BS and young people on this crap – their drug metabolising enzymes can’t cope – it will continue.
Report comment
It’s true that this has been shown to be the case over and over in these events. But that can’t be the only factor. There are millions of kids on these drugs and the vast majority don’t flip out in this manner. Many more, as a proportion, simply kill themselves. But there’s no doubt this is an important factor that could be eliminated if we could get all to realize what a fiasco these drugs really are.
Report comment
Marijuana сould treat dementia and causes anti-drug psychosis = psychiatry diagnoses in such people dementia praecox aggravated by drug addiction. It seems like someone forgot to close the faucet in the bathroom..
Report comment
If we are going to go by the premise that everyone can explode, which everyone or might we say almost everyone has the potential for, then do we drug everyone? With the same drugs that have been proven to make people explode?
No matter what spin we give this issue, it is not sensible, rational or factual.
We have ALWAYS killed, the ability to do so is hardwired. If we think that drugging young men to prevent this, I suppose then it narrows down a capable army for self defense?
When someone orders a killing in the middle east and it causes deaths to civilians, and the result is escalation in violence, even though the killings had nothing to do with immediate threat or defense of territory (which we are wired for)?
Use whatever argument you want, national defense? But was it imaginary defense? Based on a potential drummed up in the mind?
Sorry, but we cannot justify most killings unless someone dragged us into war, in which case we are in kill mode, and the effects of being forced to participate in killings that were not the plan of the killer himself are well documented.
The results of killing are often “mental illness”, or “addiction”. It is much more convenient for governments to hide their atrocities behind booze.
It is nothing for a world leader to kill people, he does not even feel regret for the civilians. And we the public are wedded to the ideas that it is all in the name of territorial defense.
The crap people get away with and not have it called “mental illness” is incredible.
It has been the great diversion to pull something called “mental illness” into the failings of us as sapiens.
Report comment
It is true that we and the media have focused on a few spectacular incidents when the truth is that “mass killing” is rampant throughout the world and has been for centuries. It is obvious that most of us continue to have little or no understanding of this or any real idea of what to do about it.
Report comment
The financial aspect of this gun violence debate is usually missed. The notion that the world is overrun with dangerous lunatics ready to fly off the handle is a godsend to manufacturers, because they can use it to promote an arms race with yourself, with themselves reaping all the financial benefits. An interesting corollary to this notion is that there should be no prior examination to see why the would-be gunslinger wants a firearm, nor should there be any restriction on the kinds of firearms available over the counter, including the ownership of automatic weapons (and rocket launchers?).
Report comment
Thank You Leah – this is very worthwhile news.
Coronavirus kills Chinese whistleblower doctor –
https://www.bbc.co.uk/news/world-asia-china-51403795
“….A Chinese doctor who tried to issue the first warning about the deadly coronavirus outbreak has died…”
American Doctor Warns –
“…As early as post-Columbine in 1999, psychologist Peter Breggin warned ..”
https://breggin.com/prozac-like-drug-luvox-taken-by-eric-harris/
“…about a possible connection, as one of the shooters was taking the antidepressant Luvox at the time…”
Medical Journalist Warns –
https://www.madinamerica.com/2018/08/suicide-in-the-age-of-prozac/
“….Here are just a few of the headlines that have appeared:
“The Neglected Suicide Epidemic”—The New Yorker
“The Unseen Epidemic”—Baltimore Sun..”
Renowned Psychologists Daughter Warns –
https://nationalpost.com/news/the-doctors-here-have-the-guts-to-medically-detox-someone-mikhaila-peterson-on-her-fathers-condition
Report comment
Was like Tssssh face forward look at this.
I mean I actually breeding interest in reading this report as opposed to looking it over and doing so skimming.
Report comment
I don’t think it takes an intellect to come to the conclusion that trying to deal with crime, and using MI as a target, is actually targeting the most vulnerable lol.
But let them knock themselves out, because the ‘problems’ go so deep, back to the beginning of a ‘sapien’ brain, so even if they tried to get rid of it genetically, the modern psych countries might see themselves without a defense system.
It is just so silly, so ludicrous of a project that even those involved in spreading gossip must realize that to tackle it based on the lies of psychiatry and general populace, will expose psychiatry even more.
I think psychiatry is most likely not on board anyway and most likely don’t want to be involved in such mass projects?
Report comment
Yes, psychiatry is not interested in finding the answer; only the next “solution” they can sell to a bewildered public.
Per my data, the problem goes much deeper than the development of the brain, as that’s not the actual locus of the mind. An answer does lie in the field of the mind, but not as psychology or psychiatry currently define it.
Report comment
Thanks to those who are trying to expose the truth. And I will just add that given the reality that “the prevalence of childhood trauma exposure within borderline personality disorder patients has been evidenced to be as high as 92% (Yen et al., 2002). Within individuals diagnosed with psychotic or affective disorders, it reaches 82% (Larsson et al., 2012).”
Meaning the vast majority of those labeled with the “mental illnesses” are survivors of violence, not perpetrators of violence. Absolutely, the lies about “mental illness” causing violence need to be exposed.
Although, I do agree, disseminating the truth that the antidepressants can cause violent and suicidal behavior does need to be made clear to the public.
But the fact that the DSM “mental illnesses” are not scientifically valid diseases also needs to be made clear to the general public.
https://www.nimh.nih.gov/about/directors/thomas-insel/blog/2013/transforming-diagnosis.shtml
And the public needs to be educated as to the reality that the psychiatrists/psychologists/doctors are murdering 8 million people a year, based upon their scientific fraud based DSM stigmatizations, and no doubt with the psychiatric neurotoxins.
https://www.nimh.nih.gov/about/directors/thomas-insel/blog/2015/mortality-and-mental-disorders.shtml
Who are the real villains, the people who are made violent or suicidal with the psych drugs, or the doctors who are murdering 8 million people a year?
Thanks again, to those who are trying to expose the truth. But what an annoyance to reality it is, that we live in a country where our government officials have as a goal, “We’ll Know Our Disinformation Program Is Complete When Everything the American Public Believes Is False.”
Report comment
There are no such things as all the MI diagnosis. There are such things as having not many tools or the right tools to deal with distress. The distress causation is real, the causes just don’t effect everyone, or cause only slight discomfort in some. And in this way, one might say that all those arriving at distress or less than optimal function are really from the get-go on an ADD, ADHD etc spectrum. It is the most obvious thing that we are not all born the same, nor develop the same.
The inability to include non sameness, itself can lead to discomfort, anxieties. Also many kids get physically bumped on the head.
The obvious is that if born ‘sensitive’, it can go on to create a number of ‘symptoms’. Thing is, no one knows where they are, how they formed, or even the needed aspects of them in that individual.
It is completely nuts to ‘treat’ these ‘disorders’, but it is even nuttier to give any of these differences in behaviours or coping names, labels. (yes even not coping, is coping)
IF, IF psychiatry dealt with each individual without looking at them as disordered (all their diagnosis are disorders) If they held the idea that all these disorders have a place, and that the behaviours that a person finds upsetting within this very structured world could be worked with, without labels, or without expectations of reaching some normal that the shrink has in mind….possibly we could respect the practice of psychiatry.
As it is, a ton of people know they have something, that their brains have difficulty, yet cannot go to a shrink because of what a shrink stands for.
I think there might be a few super intelligent ones. Some that might suggest a “forest school” for a kid that has “ADD”…although, few would ever do so because if that leaks out to peers, they become suspect.
There are a lot of batshit crazies in psychiatry. Crazy as in cultish minded, no intellect to peer into the possibility that minds and brains survived despite huge genetic differences, and we can’t just randomly castrate minds.
I sometimes want to slip into sadness, well almost on a daily basis, because when I look back on my many years, I know myself better than anyone ever could. I DEFINITELY “had” something, YET, the problem lies in the “had”, or “has”. And the “had” or “has” is the sole reason I can’t go to a shrink.
First of because there is nothing that could have been or can be done, and second, the “had” or “has” is the biggest insult to one human to be told by another. Because we are describing the being of a person.
It would be my biggest thrill to sit with a shrink and despite my many difficulties, be seen, feel like, that him and I are the same, that no one needs a label, and that the ‘thing’ that one is there for, is not some disorder, but that some of the crap the brain does might indeed be a tad upsetting, especially when in comparison to what we think of or represent as norm.
It is the greatest Hoax to present brains as abnormal, when what they really are is DIFFERENT. And in that sense, we are all normal.
The manner in which the criteria, the labels, the idea of abnormal, the chemicals etc are presented is just such a fallacy, that one can only warn people.
YET there is such potential for growth. IF ONLY shrinks could pry away from their narrow views, and work with their brothers and sisters towards the goals that they see as being helpful.
Always, the client is the leader and keeper of what he desires to feel best.
Report comment
As I like to say, species survival depends on genetic diversity. We need a range of “phenotypes” in order to get the work of our society done. We’re in big trouble when we start deleting certain presentations because they are inconvenient or uncomfortable to confront for those in the seats of power.
Report comment
Yes-I wonder how many people realize that Hitler and Mussolini gave us the A-bomb, by persecuting physicists out of their countries because the scientists were racial inferiors.
Report comment
I believe that mass shooters cannot be psychoanalyzed because the cause of their behavior is beyond our understanding of psychology.
Most shooters fall within the realm of normality which means that anyone can be a shooter or as Hannah Arendt said, anyone can behave like Eichmann because there was nothing pathological about him. He said he was “just following orders”. You have many people in the military and law enforcement who “just follow orders” believing that doing so is normal just like Eichmann did. We ought to realize that killing another human being reflects that we still have much to learn on what it means to be human. It seems as if our mental health researchers are also unaware that being normal is not normal and that it needs to be studied in depth.
Dr. Bartlett is already on to this
“With the exception of many criminals, bullies, and other people who have already behaved violently or abusively, the majority of psychologically normal people are “sleepers”-that is, they are dispositionally inclined, when the situation is right, to aggression and destructiveness. Their patterns of thought and behavior are to be understood dispositionally, that is, in the conditional sense that, if an adequately provoking situation arises, then the behavior that results will tend to be malignant: they have a pathogenic willingness to inflict harm, which remains latent until an appropriate situation arises. Such a situation may, for example, come in the form of war, ideological conflict, unrestricted power over others (as in an inadequately supervised prison), narcissistic injury, or in many other ways. Such “adequately provoking situations” unfortunately, as we know, arise with great frequency and prevalence”
Steven James Bartlett. Normality Does Not Equal Mental Health: The Need to Look Elsewhere for Standards of Good Psychological Health
Report comment
Why is my previous comment still in moderation? And why is it that I have no access to my history of comments when I log in?
Report comment
My apologies to you and others. I’d approved a bunch of comments last night but somehow it did not process them as approved. It’s now posted. Thanks for prompting me.
Report comment
*What’s the diagnosis of the shooter?
Antisocial (hebephrenic) schizophrenia.
Report comment
Well that was far more fair and balanced than I expected, but it was still very skewed, propagandist, and a diversion from the truth. The TRUTH is that most mass-casualty school shooters have 2 things in common, – psychiatric “treatment”, and psych drugs. Starting in the 1990’s, most so-called “anti-depressants” have carried mandatory “black box” warnings about increased risk of “suicidal and homicidal ideation and behavior”. In other words, YES!, a person, especially teenaged males, on psych drugs, is far more likely to commit violent acts, including gun crimes. This is true, even if you agree that the so-called “mentally ill” in general are less likely to commit violent crimes. And consider, the article almost actually states that committing gun crimes is “normal”! And then everybody’s favorite bogeyman, “stigma” pops up! And, since the only real source of this vague and ephemeral “stigma” is psychiatrists, psych drugs, and the DSM, well, …. My, my, my, what a FINE MESS psychiatry and psych drugs have created! Even fools such as Presidential candidate Amy Klobuchar are saying there are “too few” psychiatrists, and that we need more of them!
I’m sorry there were so few voices from the survivors of the lies of the pseudoscience drug racket known as “psychiatry”…. I was taken to a psychiatrist, and given a bogus “diagnosis” and psych drugs in high school. The psychs and psych drugs ruined the best 20 years of my life. Yes, the psych drugs made me far more dangerous than I would have been without them. Thank God the only one seriously hurt was myself…. If I knew then, what I know now, I would NEVER have gone to those quack shrinks, nor taken their poison pills. And I would be much healthier and happier than I am today. I’m doing as well as I am today IN SPITE OF psychiatry and psych drugs, and NOT BECAUSE of them…. Given the pervasiveness of psychiatry and psych drugs, I’m surprised there isn’t MORE gun crime and violence….But PhRMA and the Guild of Psychiatry won’t ever let that TRUTH be spoken aloud….
Report comment
I won’t deny the role the drugs play. But the “diagnosis” itself can be alienating.
What do all shooters have in common? Isolated loners.
How do the shrinks plan on preventing people from becoming shooters?
1. Drug away their impulse control and empathy.
2. Label these people in order to alienate their family and any friends they may have.
Shut off empathy and isolate them. Couldn’t do a better job creating mass shooters if they were making a conscious effort.
Report comment
“Capitol Hill Briefings Debunk Myth Linking Gun Violence to Mental Illness” ???
How can a myth about a myth be debunked without the debunking of the original myth?
The original myth is that there is such a thing called “mental illness.” We might as well have Capitol Hill Briefings to debunk the myth linking gun violence to the Easter Bunny. Come to think of it, perhaps it is the Easter Bunny – with his nasty, big, pointy teeth (bonus points for understanding the reference) – that is responsible for all of this violence after all. It couldn’t possibly be the fault of psychiatry and psychotropic drugs that are known to CAUSE the very symptoms that they purport to cure. It must be that nefarious Easter Bunny, and his henchman, Santa Claus, the Tooth Fairy, and many Leprechauns.
As long as the myth of mental illness continues to pervade the imaginations of the vast majority of people in the United States, the violence will continue to rise, and the cause will continue to elude us. The time has long since passed when the myth of mental illness and its attendant hoaxes, such as the “chemical imbalance” hoax ought to have been driven from the public square, along with all other pharmaceutical fantasies and psychiatric chimeras.
Report comment
Where is the Holy Hand Grenade of Antioch when you need it?
Report comment
“And Saint Attila raised the hand grenade up on high, saying, ‘O Lord, bless this thy hand grenade, that with it thou mayst blow thine enemies to tiny bits, in thy mercy.’ And the Lord did grin.”
Report comment
Thou shalt count three. Thou shalt not count four, nor shalt that count two, unless thou shalt immediately proceed… unto THREE.
Five is right out.
Report comment
LOL!
Report comment
Fragging went out of style after Vietnam.
Report comment
Politics wants ‘data’ where there isn’t any.
No one’s looking at themselves and the bigger constructs of society such as beliefs held that are entirely wrong. Basically, society is sick itself, badly so, and increasingly so every year.
We are all afraid, shamed, so forth as a small example.
Moreover, why are we attacking people who go to the doctor like the mentally ill (health seekers)?
Report comment
There would be no problem if the doctor knew what he was doing, but alas, psychiatrists are caught up by the discipline’s pseudo-medical model of pathological mental states, which prohibits them from even considering states that can be treated by ordinary medical means, such as heavy metal poisoning, underactive thyroid, hypoglycemia, etc., in lieu of drugging their patients into semi-consciousness.
Report comment
The public needs debriefing much more than briefing.
Report comment
Blaming the “severely mentally ill” and promising to punish (aka treat) an entire group for the crimes of a tiny minority doesn’t make anyone safer. But it provides the illusion of safety, making the public feel more secure. Just like many taking SSRI drugs have the illusion of feeling better.
Placebo effect. It’s not just a pill.
Masters of illusion.
Report comment
I believe psychiatry greatly contributes to crime, and is merely an extension of the confusion that besets people and society.
Right now the way our society is set up, is to silence it. Everyone with a murderous thought knows to keep it quiet, as that thought is deemed as abnormal. Many psychiatrist might even warn, before ‘therapy’, that anything you say, might be held against you, in the form of, it gets reported if there are concerns by shrinks.
So then, the client has the choice of being labeled and seen as dangerous, when in fact, his thoughts might just need a place to be talked about, to deescalate. Most thoughts have an underlying sense of hopelessness and psychiatry is the very practice that breeds this feeling.
Thoughts, can be distressing. Psychiatry could greatly reduce this stress by normalizing them, and to educate people about them, to show people how not to act upon each thought. And that is not to suggest mindfulness.
I think most people never divulge the things that bother them.
The more DSM labels they come up with, the more hopeless people feel, the more they get silenced.
After all, who wants a label?
The hopelessness that psychiatry itself feels, by their own discriminatory practices, IS what clients feel and is transferred over to the client.
Clients are so very unaware of what happens in therapeutic relationships. That we in fact go to the very people who preach “sickness”, “mental illness”, “chemical”, to be told we are as hopeless as we feel and thus are correct in our estimation of ourselves.
One can never redeem oneself to a shrink. THIS practice leads to absolute hopeless and combine that with meds and the ongoing despair and futility that psychiatry preaches through a “broken mind” theory and we have a perfect recipe for disaster.
No political people want to be notified by consumers. No one wants to deal with entrenched systems no matter how they fail and breed failures.
Report comment
Well that is the big exposer. When a person with anxiety, sadness and fear of life, gets a label that even courts, the medical community, and the world itself spits on. Where humans are cast out as “being different”.
And psychiatry responds, saying “yes it’s awful, all that discrimination”
and, “no, we don’t cast out, you can’t help being ill, Do you “feel” cast out”….”remember to challenge that stinkin thinkin about being cast out, it is part of your ‘illness’, it is not real”
Then they speak about stigma, the public stupidly loves this, they speak to the client about stigma, but if you feel stigma it can also be mental illness lol.
They really dislike clients that are too conscious to realize the absurdities.
“the ‘patient’ feels stigmatized, feels as if others are against him”, “patient reports being sad”.
Report comment
….ah, but NOW it’s “mental health”!…On Monday this week, I literally watched Amy Klobuchar state, “1 out of 5 Americans will struggle with *mental* *health* this year”…. In other words, I guess, 4 out of 5 Americans are fine with, and don’t struggle with, so-called “mental health”….whatever the hell THAT is!….
Report comment
I see this as an attempt by the mental health system to walk away from its responsibilities in this matter.
That we might support this flight only indicates that all our data shows that system doing more harm than good.
But these people are using the traditional paradigms for “mental illness” and “treatment” which have never worked – always been faulty. So while seemingly avoiding the disaster of letting the mental health system get even more involved in “preventing” antisocial behaviors that they know absolutely nothing about, we get nowhere in understanding why such incidents do happen or what if anything should be done about it.
I think that when a person points any kind of deadly weapon at another person when the other person is unarmed and shows no violent intentions, that person has gone temporarily insane and may be about to commit murder. We don’t expect any system, particularly the current mental health system, to be able to predict when such events might occur. Probably, good top-notch police work could do more to prevent such disasters than any sort of “teen screen” fiasco or similar “preventative intervention.”
But that’s only because the police understand criminals better than most of us do.
If we all understood the dynamics of these events much better, not only would the current mental health system no longer be run by psychiatrists, but we’d be on our way to solving a lot of other societal problems, too. What this points out most clearly to me is the gross lack of understanding of these events by the people who should understand them quite well.
Report comment
I prefer invisibility to being “outed”. That way, I’m able to say sensible things without attacks on how daft I must be.
Report comment