
The coroner’s report on the 2010 suicide of Victoria, British Columbia teenager Freya Milne recommended expanding mental health education programs and more proactively identifying and tracking students at risk for mental health problems. In the context of the whole report, though, these final recommendations were perplexing.
By the time she was sixteen, Freya had been grappling with anxiety and suicidal feelings off and on for six years while in an accelerated school program for gifted students. She’d long been involved with psychiatrists, counselors and therapists. In mid-January of 2010, however, she suffered a setback at school and, while experiencing physical symptoms of anxiety, Freya accepted a medication for the first time – the benzodiazepine sedative clonazepam. The medication was not approved for use in adolescents, and carried warnings about unusual changes in mood or behavior and increased suicidal ideation, but the psychiatrist did not convey these warnings to Freya or to her mother. Shelley Milne soon worriedly reported to the psychiatrist that her daughter was behaving in an unusual manner, alternately paralyzed with sadness and anxiety then hypomanic. The psychiatrist, without seeing Freya, increased the dosage and twice re-filled the prescription for clonazepam. On February 2, just three weeks after beginning the medication, Freya took an overdose of codeine, loaded her pockets with rocks, and walked into the frigid coastal waters off Victoria in western Canada.

Freya’s suicide received extensive media attention, but these circumstances remained a mystery to most until the coroner’s report was released in March of 2013. Yet the report made no recommendations with respect to the failure of the treatment provided to Freya, or of the dangers of the drug given to her. Instead, the coroner recommended that the province’s schools should develop a more comprehensive “student information system” that would collect emails, meeting notes, “and anything else pertaining to a student,” and combine that with a new “flagging system on all student files where a child or youth has a diagnosed mental health issue.” In addition, the coroner recommended that mental health education “be a component of continuing education for all teachers and counsellors on an annual basis.” Basically, though the mental health system had failed to help Freya, the coroner recommended that school staff should get more mental health training, and schools should more intensively identify, flag, track and monitor students with mental health concerns.
This was so even though Freya’s case was not an isolated one. It wasn’t even the only high-profile, carefully reviewed case that year in Victoria, a community of just 80,000 people. In October of 2010, sixteen-year-old Hayden Kozeletski began experiencing intense anxiety and asked for help. A teacher took her to a hospital, where Hayden disclosed having been sexually abused. For the next two months, Hayden bounced voluntarily and involuntarily between hospitals and adolescent mental health units, received various psychotropic drugs unapproved for use in youth, and then hung herself. An inquest jury recommended intensifying mental health screening and tracking, and providing more mental health training for all professionals in regular contact with children and youth.

That same year, Victoria teen Kimberly Proctor was raped and murdered by two male peers. Her family gathered thousands of signatures and lobbied government to mandate school “threat assessment protocols” that would proactively identify potentially dangerous, mentally unstable kids and push them into counseling and involuntary psychiatric treatment. Yet court documents showed that both of the boys who killed Kimberly Proctor had been violent previously and had already been involved off and on for years with school administrators, social workers and mental health professionals.
There have been many cases in Canada and the US like these, involving suicides and homicides committed by young people who have been in mental health care. Most are complex situations with many factors involved. Even so, it raises the question: How is it that these tragedies—and clear treatment failures—are so often used as justification to expand the funding, reach and power of mental health professionals? Why are there no broader inquiries into the failure of mental health treatments, and into the possibility that common treatments may have played negative roles in these grave events? Is there some reason that the mental health system is constantly seen as deserving of more funding and authority, and evades true accountability?
The Toronto District School Board announced a four-year plan to give mental health training to all school staff to ensure mental health “is integrated into every aspect of a student’s school experience.”
In British Columbia (BC), amid the deaths and subsequent pronouncements about what needed to be done to prevent such events from recurring, the provincial government launched a training program for family physicians and school staff that promotes mental health screening of all children and adolescents. Similar programs are occurring in other provinces, too, as part of a national strategy called “School Based Mental Health in Canada” that is being pushed by the Mental Health Commission, which was created by the federal government. This year, for example, the Toronto District School Board, one of the biggest school districts in the country, announced a four-year plan to give mental health training to all school staff to ensure mental health “is integrated into every aspect of a student’s school experience.” It’s modeled from a similar program in Nova Scotia led by Canada’s most prominent child and adolescent psychiatrist, Dalhousie University’s Dr. Stan Kutcher, who is also a key advisor on the Mental Health Commission. As the Commission’s report noted, all of this is in turn part of a continent-wide effort involving initiatives like the International Alliance for Child & Adolescent Mental Health & Schools, and the US-Canada Alliance for School Mental Health.
Most of the documents, lectures, and supplemental resources for the BC program are publicly available. They therefore provide a rare glimpse into exactly how psychiatrists typically educate family doctors and school staff in these kinds of programs. And ultimately, say critics, the program’s training materials provide overwhelming evidence that our mainstream mental health system is, for some undeclared reason, being allowed to continually expand its influence without any scientific accountability.
Screening more often wrong than right
According to their press release, the Practice Support Program for Child and Youth Mental Health (PSP-CYMH) is a joint initiative of the BC government’s Ministry of Health and the provincial association of medical doctors, Doctors of BC. It’s led by Dr. Stan Kutcher, along with BC Children’s Hospital’s Dr. Jana Davidson. Family doctors are being trained to conduct mental health screening tests, identify children and youth who are “at risk,” and provide specialist referrals or early intervention treatments for ADHD, anxiety and depression. Doctors are paid over $2600 to attend the 10.5 hour training and put two of their own child patients through screenings. In the past year, over 600 BC doctors have taken the program. According to a PSP-CYMH administrator, the effort is scheduled to expand this fall, with training of school staff to be more proactive “gatekeepers,” funnelling kids towards screening tests and treatments.
“The pharmaceutical industry has known for years that being involved in screening is very important,” said Cassels. “So they have put their own people on the committees that have designed the screening tools.”
Many of the PSP-CYMH education materials were authored by Kutcher or BC Children’s Hospital psychiatrists, often in conjunction with others. The whole program is touted as “evidence-based.” But, critics say, scientific problems with this program begin with the screening tools, and permeate the training materials too.
Alan Cassels, a University of Victoria pharmaceutical policy researcher and author of Seeking Sickness: Medical Screening and the Misguided Hunt for Disease, has publicly criticized the PSP-CYMH for using screening tools designed with pharmaceutical industry involvement, just like TeenScreen did. The US TeenScreen program shut down in 2008 in the wake of public protests, lawsuits, and federal investigations into its financial links to pharmaceutical companies, along with associated mounting rates of the medicating of children. Through financial disclosures in scientific journals, Cassels found that, for example, PSP-CYMH scientific lead Kutcher, author of the program’s depression screening test, was connected to at least eleven pharmaceutical companies. “The pharmaceutical industry has known for years that being involved in screening is very important,” said Cassels. “So they have put their own people on the committees that have designed the screening tools.”

The PSP-CYMH advises physicians to give mental health screening tests to all children and youth in their clinics during vaccinations and annual check-ups. “It’s the idea that you can never be too proactive,” said Cassels. However, mental health screening tests that ask children questions like if they “worry about the future,” are “nervous” around strangers, or “feel blah” a lot, as the PSP-CYMH tools do, inevitably create enormous numbers of “false positives,” said Cassels. “It’s so vague, it’s so useless. Taking any kind of range of human emotion and trying to quantify it is a mug’s game. It’s so prone to manipulation.”
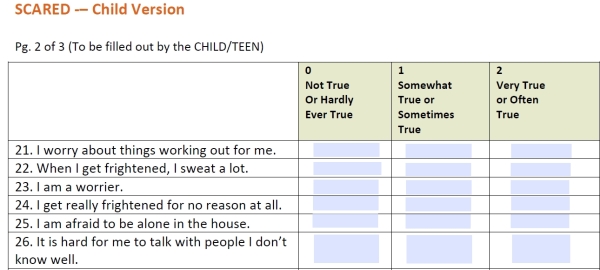
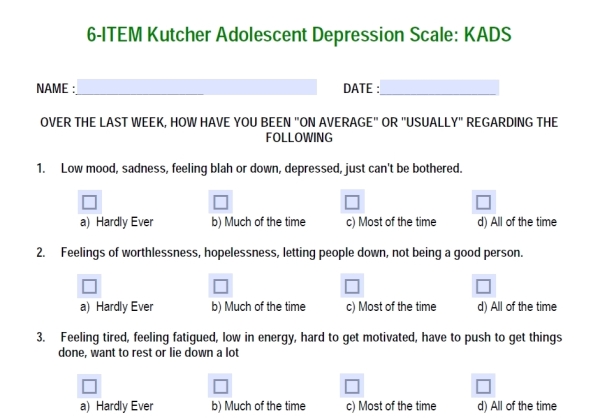
The PSP-CYMH training materials state that the Screen for Child Anxiety Related Disorders (SCARED) has demonstrated “excellent” sensitivity and specificity. In the scientific literature, though, it’s clear that, even assuming that as many as 10% of children and youth actually have an anxiety disorder, SCARED will still typically determine that about three times as many kids have anxiety disorders. Similarly, Kutcher’s “Kutcher Adolescent Depression Scale” boasts that this tool has “sensitivity and specificity rates of 92% and 71% respectively—a combination not achieved by other self-report instruments.” A 2011 exchange of letters in the Canadian Medical Association Journal shows that these kinds of numbers mislead even many physicians and mental health professionals who don’t understand the mathematics of screening for relatively low-incidence conditions. What is not clarified in the PSP-CYMH materials is that, using a common assumed rate of depression in youth of 4%, Kutcher’s test will be wrong seven times as often as it’s right; that is, if 1,000 youth are screened, 279 will be “false positives” for depression. Cassels pointed out that a high score could mean that a child is “possibly depressed,” as Kutcher’s rating scale states, but it could just as likely be a measure of how crowded a child’s classroom is, how much he cares about environmental problems, or how vulnerable his sense of himself is to manipulation by suggestive test language. Cassels said mental health screening programs are therefore known for overloading our already over-taxed mental health care systems with people who aren’t even asking for help.
“I can say pretty definitively that we don’t have the evidence that can show that kids who are screened ultimately do better than kids who are not,” added Cassels. “We know that the screening tools will increase the use of psychotropic drugs; that’s the outcome we’ve been able to actually measure. As far as whether those kids ultimately do better, are more successful in school, more likely to graduate, have happier, more successful lives, we can’t show that at all.”
Cassels is not alone in his criticisms. In the June 2013 Canadian Medical Association Journal, the Canadian Task Force on Preventive Health Care stated that they “did not identify high-quality evidence of the effectiveness of screening for depression” in adults, and recommended against doing any depression screening in primary care settings. The Task Force also said that they “remain concerned” about the potential harms from the high rates of false positives and consequent unnecessary treatment, labeling and stigma, and lamented that they could find no studies examining these potential harms. Similarly, in 2009, the US Preventive Services Task Force found no evidence to support screening children for depression, and also recommended against screening for depression in adolescents unless they had ready access to non-drug therapies. The US Task Force couldn’t find a single trial that had assessed whether screening improved mental health outcomes in children or adolescents. In 2014, the US Task Force concluded that all suicide screening was unreliable and “the current evidence is insufficient to assess the balance of benefits and harms.”
“Kutcher was a co-author of one of the most fraudulent, scandalous mental health studies in the last fifty years,” said Cassels.
Despite those findings, the PSP-CYMH training materials instruct doctors to use screening scores to guide medication adjustments. If a child is taking 30 mg of fluoxetine and has a SCARED score that shows no improvement or is worsening, doctors are advised to “increase medication gradually.” In the case of a rising score, they’re advised to “increase [medication] slightly.” With a substantially improving score, they’re to “continue medication at current dosage.”
Cassels said that he believes programs like PSP-CYMH involve many well-meaning people, but those people are “naively” accepting information from others involved who have strong ties to the pharmaceutical industry, like PSP-CYMH scientific lead Dr. Stan Kutcher.

“Kutcher was a co-author of one of the most fraudulent, scandalous mental health studies in the last fifty years,” said Cassels, referring to Study 329, which was featured in Alison Bass’ book Side Effects: A Prosecutor, a Whistleblower and a Bestselling Antidepressant on Trial. It was a highly influential, large-scale study of Paxil in adolescents that went through multiple revisions with the help of a medical writing firm paid for by GlaxoSmithKline, as crucial data about adverse effects were hidden and key markers and interpretations of the outcomes were changed. The U.S. Department of Justice summarized that the final article “distorted the study results and gave the false impression that the study’s findings were primarily positive, when they were, in fact, primarily negative.” In the same $3 billion lawsuit settlement, GlaxoSmithKline also admitted bribing physicians with “expensive meals, weekend boondoggles, and lavish entertainment” and “cash payments” cloaked as consulting fees.
“The conclusions of Study 329 were completely contrary to the body of evidence about the safety of those drugs in children,” said Cassels. “In my opinion, the people who put their name to that study should be in jail.”
Scandalous lies or business as usual
Elia Abi-Jaoude also described Study 329 as “ludicrously scandalous,” but he hastened to point out that it’s not an aberration. Abi-Jaoude is a neuropsychiatrist affiliated with the University of Toronto who sometimes treats children and is part of an international team that is currently re-analyzing for re-publication the original trial data from Study 329. Abi-Jaoude said innumerable psychiatric studies have been equally manipulated by pharmaceutical industry influences, but most of them don’t become the target of government lawsuits and public exposés. “Study 329 is a good representative of practices that pervade the literature,” said Abi-Jaoude, adding that he believes this is why the Journal of American Academy of Adolescent and Child Psychiatry still hasn’t retracted Study 329, and why the study’s false conclusions and co-authors like Kutcher remain immensely influential.

Abi-Jaoude doesn’t endorse mental health screening programs. “The evidence doesn’t support screening,” he said, while adding that potential harms are obvious. “Labeling someone, especially at such a young age, with having a mental illness is no small matter. You’re contributing to their identity at a very vulnerable time in their lives. The other thing it opens up as a risk is interventions that are unwarranted and are potentially harmful, especially at a vulnerable stage of the lives of these young, developing brains.”
The PSP-CYMH materials often discuss the importance of first trying to help children through practical supports, coping strategies, cognitive behavioral therapy, exercise and healthy eating; however, the spectre of conditions requiring more intensive interventions is never far in the background, if a child or youth is “not functioning as well [as normally]” over “more than several weeks.” Notably, the PSP-CYMH doesn’t provide physicians with any substantive training in non-drug approaches, while BC’s public health care pays for physicians and most drug costs but very little for any non-drug therapists or approaches. Yet there seem to be no discussions about risks of over-diagnosis or over-medicating in the PSP-CYMH materials, even though prescribing of antipsychotics to children has increased four-fold in BC since 1996 and ADHD medicating has tripled in ten years.
“I don’t believe people promoting such programs are particularly concerned about the risk of the inappropriate diagnoses of mental illnesses, or the inappropriate use of our interventions,” commented Abi-Jaoude. “I stop medication at least as much as I start. It is routine to see people on inappropriate medications, or too many medications.” Many psychiatric drugs can have very serious, damaging side effects, especially over the long term, explained Abi-Jaoude, adding that, “Evidence for the long-term use of medications, whether in children or adults in psychiatry, is sorely, sorely lacking.”
The PSP-CYMH materials often indicate that kids could be taking psychiatric medications over the long term, yet there seems to be no discussion of that severe dearth of long-term safety and efficacy evidence. The training materials even repeatedly assert that antidepressants decrease suicidality in adolescents, though Canadian and U.S. health regulators have issued warnings to physicians about clinically observed increases in suicidality in youth taking antidepressants.
Medical education or drug promotion program?
Mickey Nardo is a retired psychiatrist, psychotherapist and internist who blogs about current psychiatric research as 1 Boring Old Man – he’s also part of the team re-analyzing Study 329. When read quotations from the PSP-CYMH materials, he became increasingly concerned about how often they strayed from any relationship to the scientific evidence base and became more like propaganda.



For example, Kutcher begins a lecture on “Pharmacologic Treatments” by instructing physicians “to be really aware of the language” that they use. “If we use the word ‘drug’ treatment, that has particular connotations for people,” says Kutcher, pointing to various negative impressions of that word. “So when you offer your patient a medication, [say that] it’s a medicine as opposed to a drug.” Kutcher emphasizes that the choice of words is important because it’s part of an “ideology” battle between people for or against psychiatric medications.
That’s just “sales language,” commented Nardo. “It’s a way to sell that these are medications and not street drugs.” He pointed out that, in fact, the vast majority of psychiatric medications are more like symptom-masking headache drugs than disease-fighting medicines.

This theme of how best to communicate about psychiatric medicines continues in a key PSP-CYMH training document co-authored by Kutcher, “The Life Span and Mental Disorders: An overview and useful tips for primary care practice.” In the section about “engaging” and “educating” patients and their families, the document describes how “there may be resistance to, or denial of, the diagnosis and rejection of recommended treatments.” In such situations, doctors are advised, “Psycho-education that identifies mental illness as a brain disorder is a useful technique by which to challenge these misperceptions, gain patient and family trust, and redefine understanding of the illness.”
This section also describes common “myths” and “misconceptions” regarding psychiatric medications that doctors should dispel. These “misconceptions” include the statements, “Medications are detrimental to general health and well-being,” and “Psychiatric medications are addictive.”
Nardo called this unqualified, misleading characterization “shameful,” pointing out that an entire class of widely used psychiatric drugs – the anti-anxiety benzodiazepines – is highly addictive, and many others are difficult to withdraw from. (Health Canada and the FDA also identify most ADHD drugs as addictive.) Meanwhile, the long-term adverse effects of many psychiatric drugs, from obesity and diabetes to growth suppression, sexual dysfunction, and liver and kidney damage are well documented.
“Increase medicine based on a rating scale… We just don’t have that kind of precision in mental health,” said Nardo. “It’s crazy.”
When read the instructions to use SCARED scores for adjusting antidepressant medication levels, Nardo was nonplussed. “Even in hard-core internal medicine, we don’t do this kind of thing. Increase medicine based on a rating scale… We just don’t have that kind of precision in mental health,” said Nardo. “It’s crazy. I wish I could say something erudite about that, but it just seems nuts to me.”
Throughout the PSP-CYMH materials, there are frequent assertions about the biomedical basis of mental illnesses. Various materials suggest that there’s “strong” evidence of “genetic” causes of mental illnesses, describe mental illnesses as “like any other physical disease,” compare psychiatric drugs to insulin for diabetics, and suggest psychotropics balance brain chemicals that “are not working well.”
Nardo’s reaction to these quotes? “This is the far right. This is the American Tea Party version of biological psychiatry.” He said such statements “push a particular view of mental illness” which is “a denial of the mind, of psychology, of bad parenting, of abuse, of social disorder, of all of the other things that we know are huge factors in the life of children. It just denies all of that and simplifies it down to, ‘They’ve got bad chemistry.’” Nardo said there’s no scientific evidence to support these PSP-CYMH statements, and said he personally knows many biological psychiatrists who “rave” in outrage when they hear such far-fetched assertions. Indeed, a recent official statement from the American Psychiatric Association acknowledged that there are no biological markers of any kind for any mental disorders.
How did the creators of the PSP-CYMH respond to these criticisms?
Accountability to the public?
Both Dr. Kutcher and BC Children’s Hospital’s Dr. Jana Davidson would not agree to be interviewed by Mad In America, and also wouldn’t answer any specific questions by telephone or in writing about the scientific evidence informing the PSP-CYMH materials. And despite their communications offices apparently making efforts, neither Doctors of BC nor BC Children’s Hospital could provide any psychiatrist to be interviewed about the scientific evidence. The BC government also did not provide anyone. Even the communications staff at TeenMentalHealth.org – an organization led by Kutcher whose website declares, “We are thrilled to provide expertise and advice in many areas of adolescent mental health and do our best to accommodate all media requests” – said to try again in several weeks, and then in six months.
“The science is shaky and they know it,” commented Cassels. “If their positions were supportable they would be able to cite the scientific evidence quickly and easily.”
Nardo similarly speculated that the PSP-CYMH psychiatrists know their training program is based more in opinions than solid evidence, but they’d be reluctant to admit that publicly. “It’s something they think, it’s not something they know,” said Nardo. “I think a lot of things, too, but I’m not sitting here trying to sell you what I think.”
Eventually Dr. Tyler Black of BC Children’s Hospital (BCCH) responded in writing to a small number of concerns raised by critics about both the PSP-CYMH program and its informational handouts about specific drugs developed by BCCH psychiatrists.
Black wrote, “[T]he goal was to create documents that are readable at a grade 6-8 reading level. Terms such as autonomic dysfunction and catatonic stupor are not appropriate for use in a patient education document.”
The handouts about antipsychotics warn families about the “fever,” “sweating” and “irregular heartbeat” characterized by the onset of antipsychotic-induced neuroleptic malignant syndrome, and advise contacting a physician immediately. The handouts do not warn of the more serious potential consequences that health regulators warn about, such as autonomic dysfunction, catatonic stupor, and the fact that the syndrome is fatal in 10-20% of cases. Asked about this, Black wrote, “[T]he goal was to create documents that are readable at a grade 6-8 reading level. Terms such as autonomic dysfunction and catatonic stupor are not appropriate for use in a patient education document.” Black did not comment on the omission of “potentially fatal.”
“In grade 6 to 8, I understood the word death,” commented Nardo. “He’s selectively reporting… He’s not giving you X% get neuroleptic malignant syndrome, X% die. It’s like the mumbling at the end of the commercials on our stupid direct-to-consumer ads: You might die, your head might fall off, you may never walk again, but meanwhile in the background the music plays.”
No discussions of the problems of over-diagnosis were readily apparent in the PSP-CYMH materials. And tardive dyskinesia (TD), which is characterized by repetitious, uncontrollable motor movements, is described in the BCCH handouts as a “rare” side effect of antipsychotics, even though statistically somewhere between dozens and several hundred children per year in BC are likely developing the often permanent motor dysfunction. Asked if BCCH was concerned that the PSP-CYMH could ultimately lead to further increases in the number of children and youth developing TD, Black did not dispute these numbers, but replied that, “We are not concerned that primary screening, or supporting primary care providers with psychiatric education will increase the amount of TD in children.”

“Why isn’t he worried?” Nardo said, shocked. “There’s nothing casual about giving an antipsychotic to a child. It’s something you worry about.”
As to why the PSP-CYMH materials were not very forthcoming about the dearth of evidence for the long-term safety and efficacy of psychiatric medications in kids, Black cited a few studies of 1-2 years in length and wrote, “The lack of trials is a cause of concern for all of us in child and adolescent psychiatry, but it is important to recognize that the absence of evidence is not evidence of absence.”
In line with this sort of thinking, Kutcher and other members of the PSP-CYMH design team evaluated their own program in the November 2013 Journal of the Canadian Academy of Child and Adolescent Psychiatry. They determined that the PSP-CYMH increased family doctors’ abilities to more readily identify mental disorders in children and youth and treat them. Whether this actually had any positive impacts on children’s lives wasn’t evaluated. “The initial results encourage broader roll-out” of the program, they concluded. They declared no conflicts of interest.


So how can a prominent program of this kind, that could ultimately affect so many children’s lives in such profound and potentially damaging ways, be so utterly immune to accountability – either scientifically or politically? Is its propaganda really so persuasive? Or are there other reasons that governments are so eager to fund initiatives like the PSP-CYMH?
It is easy to suspect that the BC government’s support for the PSP-CYMH may be linked to the pharmaceutical industry. The BC Chief Coroner, who ultimately controls all coroner’s report recommendations from deaths like Freya Milne’s, is a provincial political appointee, and Cassels and the Vancouver Sun exposed that over the past ten years, pharmaceutical companies have donated 14 times as much to BC’s current governing party as to the main rival party. Industry representatives meet with government officials regularly. The government has made a slew of pharma-friendly decisions, including stacking industry representatives on a drug policy task force, and firing or cutting funding to researchers who’ve criticized certain drugs or raised the ire of the pharmaceutical industry.
However, health policy analyst Wendy Armstrong suggested that understanding support for the PSY-CYMH purely in terms of financial influences limits our understanding of broader political movements going on. Programs like the PSP-CYMH, she said, are really one small part of a dramatic expansion of psychological screening, surveillance and risk management systems targeting children and youth going on internationally. And this is a trending approach to governance, she and other experts argued, in which not being scientifically or democratically accountable is central to how the programs operate and exert powers over citizens.











Awesome article. Though it describes what is going on in Canada, of course this is happening all over the world now. I certainly agree that the psychiatrists who are doing this belong in prison.
Although our movement does not have the numbers right now to fight this directly, I have been saying, and I say it again, that we should be concentrating on the psychiatric abuse of children. The general public has been sold on the idea that “the mentally ill” are the crazed killers wandering the streets talking to themselves. So why not just lock them up on the (clearly unconstitutional) grounds that they are “in need of treatment?” In other words, let’s just give psychiatrists a free hand to incarcerate anyone they feel like.
But when we start talking about children, I think the public sees things differently. For one thing, these may be their own children to be labeled and drugged. And most people perceive the abuse of children as a lot more serious than locking up the stereotypical demented killer wandering the streets.
The recent case of Justina Pelletier is an example of this. Tens of thousands of people were involved in pressuring the State of Massachusetts to free her. A teenage girl being abused by psychiatry…what an opportunity to educate the public about what psychiatry really is about. Unfortunately, the “consumer leaders” there mostly ignored what was going on right under their noses. They weren’t taking advantage of the opportunity to point out what was really happening, and so the public saw (and the media presented) the issue as a clash between diagnoses, and not the power grab by psychiatry that was essentially the cause of Justina’s ordeal.
Recently I have been in contact with many people now who consider themselves to be “survivors” and/or “anti-psychiatry” (I am both) and want to start effectively fighting back. We need an alternative to the various meetings and fake organizations funded by the mental illness system. Over the next few weeks I will be participating in discussions with other concerned survivors and anti-psychiatry people (who are not necessarily survivors) to get our movement back on track.
And this excellent article, I think, suggests some directions we should take.
Report comment
“But when we start talking about children, I think the public sees things differently. For one thing, these may be their own children to be labeled and drugged. And most people perceive the abuse of children as a lot more serious than locking up the stereotypical demented killer wandering the streets.”
Excellent point Ted. I think these types of screening programs for youth with see a surge in disgruntled parents as the ‘lambs are selected for slaughter’. It may provide a point where the public becomes aware of the abuses that have been occurring under their noses for years, and just might result in some questions being asked about the validity of the ‘science’. Though I think it may be a small window of opportunity.
I also think that the lack of accountability would be fairly easily demonstrated. I know we have laws here in Australia that are designed to protect the community, but they are never used. And I mean never. The measures for accountability are in place, but those charged with ensuring compliance with the law are simply neglecting their duties. It really is as simple as that.
With the levels of negligence and criminality in our system I’m surprised that there aren’t lawyers crawling all over the place. For some reason they do not wish to touch anything once the words mental health are uttered. I understand this to some extent, but even where there is ample evidence they will not pursue any cause of action. The few lawyers who do pro bono work are struggling to even assist 1% of all those who do need help.
Good luck with your discussions.
And thank you for this article and I look forward to the second part Rob
Regards
Boans
Report comment
Count me in, Ted. Email me at our clinic – [email protected] – and I’ll give you my personal email. If we don’t effectively fight back, psychiatry will succeed as they have the power and infrastructure to boggle the mind. And they will do anything to “help” people as expressed by the leader of MK ULTRA – George Hamilton White. On retiring, he told the psychiatrist, Sidney Gottlieb…..”It was fun, fun, fun. Where else could a red-blooded American boy lie, kill and cheat, steal, deceive, rape and pillage with the sanction and blessing of the all highest?”
In a documentary on Camp X (the “School of Mayhem and Murder” in Oshawa in the 40s), one of the spies – still alive at age 90, spilled the beans. He said, “Do you know why I am still alive? Have you ever heard the saying – THE GOOD DIE YOUNG?” We’ll all be dead, Ted, leaving the evil behind us and a trail of drug addicts, ruined economy, birth defects and this evil mental health movement meant to created a society of psychotropically drugged consumers.
Report comment
Thank you for writing this article. It is just heartbreaking to me that the governments are advocating the stigmatization and drugging of children, with addictive kiddie cocaine, benzos, and antidepressants known to cause suicides, mania (“bipolar”), and violence. And to put a child on an antipsychotic is blatantly evil.
The pharmaceutical industries need to be broken up due to their continued “organized crime” tactics, not given free reign to “torture” as many children as possible.
Report comment
Rob,
This is a fantastic, very thorough article that should be widely distributed and read by every parent and citizen of the globe. This literal mental death assault on humanity is now global so that the 1% psychopaths in power can continue to rob the world’s wealth and resources and enslave/destroy the rest of us while making huge profits doing so. This is obviously the case with biopsychiatry and its life destroying stigmas and toxic drugs used for typical human problems, losses, crises and stressors that are quite common for normal people with a conscience, empathy, compassion and other human traits so sorely lacking in these psychopaths/malignant narcissists (or just plain evil) in power.
The point that psychiatry serves as an agent for social control has been well known and exposed by those like Dr. Thomas Szasz and Dr. Joanna Moncrieff. Since psychiatry sold out to Big Pharma allowing them to make billions with their mutual fraud and ever expanding predation on one and all with their ongoing disease mongering in their junk science DSM, so called democracies have been turned into fascist “therapeutic states” with biopsychiatry/Big Pharma now the enforced state religion with its own Inquisitions and Witch Hunts. As with Stalinist Russia, they were smart enough to put their focus on brainwashing the children to mold their version of good, obedient citizens in the type of surveillance state you describe as the goal of our own so called democracies being bought out by Big Pharma and other corrupt oligarchies that are supposedly too big to fail or jail for their many crimes against humanity as well as too lucrative for politicians and other so called government officials to resist given the cost of getting elected and wealthy at the same time.
Your exposure of the drug company KOL’s like Kutcher and his cohorts pushing their literal Big Pharma sales pitch juxtaposed with the long term experience, ethics and common sense of Dr. Mickey Nardo exposing this screening agenda as the further medicalization and drugging of typical environmental/social child stressors was superb.
Anyway, I’ve been researching the “mental health” field for many years and I can’t think of anything to add to this fantastic, very eye opening, hard hitting article on the ongoing and growing global agenda to fraudulently stigmatize, drug and disable/destroy our youth so they will be unable to challenge these intraspecies predators in power as in “Occupy Wall Street” and other typical youth protests aimed at injustice by those in power. The term “intraspecies predators” comes from Dr. Robert Hare, world authority on psychopaths and author of Without Conscience: The Disturbing World of the Psychopaths Among Us and Snakes in Suits: When Psychopaths Go to Work. Dr. Hare consults for the FBI, police and other security people throughout the world. Perhaps he might be a good source for a future article on those without ethics or conscience in psychiatry and child psychiatry in particular.
I will look forward to reading the second part of this enlightening article.
Report comment
The road to hell is paved with good intentions.
Report comment
I found some phone numbers on the teenmentalhealth.org website.
Faten Alshazly Public Affairs Advisor 902-470-6582
Mitch Shea Communications Coordinator 902-470-8444
I think I should call these numbers and tell these people about the study below and how sick I got after falling for the serotonin scam and taking psychiatric drugs.
“In 11 placebo-controlled studies of the treatment of acute manic episode, including 1,506 patients (117 person-years) in the combined active compound group and 1,005 patients (71 person-years) in the combined placebo group, no suicides and no suicide attempts occurred. In four placebo-controlled studies of the prevention of manic/depressive episode, including 943 patients (406 person-years) in the combined active compound group and 418 patients (136 person-years) in the combined placebo group, two suicides (493/100,000 person-years of exposure) and eight suicide attempts (1,969/100,000 person-years of exposure) occurred in the combined active compound group, but no suicides and two suicide attempts (1,467/100,000 person-years of exposure) occurred in the combined placebo group.”
http://www.ncbi.nlm.nih.gov/pubmed/15800158
Seem that taking those drugs for that “just right mood” described in the article are likely to be associated with a 2.22 times greater risk of suicidal acts than placebo or no treatment !!!
Report comment
Parents are being mislead by a multi billion-dollar a year child drugging industry that a diagnoses of “mental disorder” (ADHD, Bi-Polar, Social Anxiety Disorder) are medical diseases or illnesses. This is a fraud. No child has a brain scan, blood test, X-Ray or any evidence of physical abnormality to verify they are “ill” or “diseased.”
Yet websites like teenmentalhealth.org continue to pound the public with misleading and fraudulent statements that these so called mental disorders are biochemical or neurological conditions. That is totally false. They are simply a list of behaviors that psychiatrists vote into existence and insert into their billing bible, the Diagnostic and Statistical Manual of Mental Disorders.
It’s dishonesty and it’s all over that teenmentalhealth.org website with those pictures of brains and all that trickery to deceive people into thinking they ‘need’ expensive dangerous drugs to fix something medical. I fell for that scam cause it works and then those “medications” almost killed me.
Report comment
“Kutcher was a co-author of one of the most fraudulent, scandalous mental health studies in the last fifty years,”
“The U.S. Department of Justice summarized that the final article “distorted the study results and gave the false impression that the study’s findings were primarily positive, when they were, in fact, primarily negative.” In the same $3 billion lawsuit settlement, GlaxoSmithKline also admitted bribing physicians…”
Umm… this is what happens when our government doesn’t bring criminal charges against these people for the harm that they cause with their lies and corruption. What I see when I look at that guys picture, I see a repeat offender who, like all others like him, should have been locked up in federal prison when they were busted the first time!
Report comment
I spent an entire summer submitting detailed research on “that guy” to the College of Physicians and Surgeons of Nova Scotia. I spent my own money on copying, postage, etc. In the end, I got a cursory letter from the College stating that they were not going to do anything about it and there is no recourse.
Report comment
Terrific and timely post! Children and adolescents are being targeted for psychiatric labeling and drugging more and more these days. The media frenzy over acts of violence is feeding this trend. Many of those who have perpetuated violent crimes were ALREADY in the mental health system prior to their crimes. The suggestion has been made that by expanding the mental health system we will be preventing future multiple murderers from achieving their ends. The reality is that the numbers of people labeled, drugged, harmed and even killed by psychiatry are escalating. . If anything, increasing numbers of desperate characters sifted through an ineffective mental health system are likely to up the violence rate even farther as well. Also, violence by the state has long eclipsed the violence of any solitary gunmen The NIMH has one statistic that always gets under my craw. They say that fully half of all cases of people labeled “chronically mental ill” were diagnosed by the age of 14. My thought, if they weren’t targeting children, we wouldn’t have so many lifetime mental patients burdening the taxpayers. Children are innocent, and rather than the pawns of defective genes, they are the prey of predatory agencies, hateful parents, and corrupt officials. We should be teaching them the truth. We should be working to reverse the present mass manufacture of people with “chronic severe mental illness” labels and “multiple murderers” rather than contributing to it. Turning a blind eye to the reality, of course, can only make matters worse.
Report comment
The baffling part of this for me is that these youngsters were deeply embedded in the mental health system, and in the case of the first, there is a direct and observable link between her “treatment” and her death, and yet somehow, this leads to a call for “more treatment!”
Not sure I can even come up with an analogy. Why are people who read these news articles so impervious to the obvious failings of the “treatment” these young people were receiving?
—- Steve
Report comment
I am going to chime in as a parent who used to give her child medications in the class of psychotropic medications. I finally listened to my own child at 13 who was taking them mostly on until he could take no more of the side effects. I was scared about them taking my son away if I did not give him the medications. CPS can do that. I do not have custody of my son, but i have told my son we all are in it together with his health. I will never ever ask him take the drugs again. I think therapy is sufficient for him to deal with his problems. The thing is some of the therapist tout child drugging for psych problems. So he is wary of this. When I took him off the medication it was a sound decision by my son and I due to the side effects he can’t take them. His anger was two fold when taking ADHD medication, and the same with the others as well his moods were erratic at best and his mood swings intensified with the medications not without. I say this to all psychiatrist who want to help the children be wary of all the drugs out there. I am adult 44 year old who has problems with these drugs, imagine how the children will be if they take it? There bodies are more changing than mine. Do not just screen and give drugs. They need to do way more testing on the drugs before they hurt more children. It is evident it is doing harm.
Report comment
Great article!
It’s so clearly brainwashing by this pseudo-profession of the industrial mental health complex and great PR on the part of the drug industry. I agree with you birdie as another parent who said “Enough”. Not only did I quit feeding my kids these toxins in pill form, I also pulled my youngest from the disgrace of a public school system that bends over backwards to be in line with this psychiatric stupidity.
It is obvious that my kids didn’t need medications. They weren’t AD/HD, bi-polar or Autistic as I had been told they most certainly were. The medications did more harm than good. I even had a son who was thrown into periods of severe hallucinations due to Risperdal and wasn’t told that was a possible side effect. I guess it was my fault for not reading the insert that came with the prescription!
This abuse has to stop.
Report comment
I am also a survivor and anti-psychiatry. It is clear to me that if we want freedom for ourselves and our children no one is going to give it to us. Freedom must be taken.The question is how to best gain freedom for the children when, where, and how? How can a conversation be had as the oppressors listen in ? Does it matter if they hear ?Can we even stop them? What are truly the best moves ? I am certain the answers lie within the survivors and our true allies. Can we reach each other without the conventional barriers?
I know there are people who need to meet in person that are thwarted by financial barriers. Our enemies have a bottomless war chest . We are even afraid to put a fruit cream pie into the face of even one of our children’s oppressors as was put into the face of Anita Bryant, a gay basher,years ago by a brave activist. It was a historical moment. I’m sure it’s on you tube somewhere. I understand today if a psych-survivor tried it, with or without a lawyer present they might face psychiatric drug , electric ,and/or prison retaliation. What to do ? I live on the Oregon coast 95 miles from Eugene . Produce a lawyer for protection and to make a statement, a video camera man ,someone to take a film handoff if necessary. I’ll supply the cream fruit pie, gas to travel a couple hundred miles and the follow through to place the pie in the face of a proper deserving spokesman psychiatrist or some such as chosen. Maybe it will start a trend, logic doesn’t seem to work. You got a better idea???
Report comment
I forgot here’s my e-mail [email protected] How do I know if the wrong people contact me?
Report comment
I can sort of chuck a pie in their face right from here sort of by putting up links on the google index by using the right keywords.
Report comment
Copy Cat and others , your gonna love this: http://www.youtube.com./watch?v=LXACBDHd3C4
Report comment
How awful. Most people assume that out of all of Canada, the West Coast would be the most progressive place in general – at least it has that reputation. If BC is so gripped by the far right-wing of biological psychiatry, is there hope anywhere in this country? Not just for children, but for adults, too.
Rob, I would be interested to know if there is a region of Canada that has higher recovery rates and lower medication uses, with more non-drug and tapering services available. Is there anywhere that has a humane and successful system?
I live in Manitoba, and here it is very much all “You have a brain disease” propaganda. Really no alternatives. Lots of psychiatric patients who live but don’t really function well or thrive. And no accountability for the system that keeps them like that. In fact, the same message – get more people into “treatment”, “Treatment helps”, more “brain disease”-based mental health “awareness” is needed. Sadly, I’m in the same boat. Stuck on an antipsychotic for years, still depressed, fattened from the drug, subject to involuntary hospitalization if I have troubles again, no clear way out of all this. Yet the public tends to believe the system works.
I’ve even thought about moving to BC, hoping there would be more alternatives and non-drug help available, but your article has made me doubt that. Sometimes I think I’d move anywhere in the world that would have me, if I could get help that actually helped. But practically speaking, leaving Canada is not a very strong option.
It would be nice to see some reporting about places with systems that worked, other than open Dialogue. Even just places where doctors only put people on psych drugs temporarily, and believe in tapering them off. Or places with a high concentration of affordable, effective therapists. It would be nice if there was some database of “doctors’ attitude towards psychiatric drugs” in different parts of Canada and the world, so people could decide where to live based on where they were most likely to meet a doctor with a non-biological-reductionist perspective. By the time you get stuck on psych drugs for years, you need some serious help, not just getting off the drugs, but also recovering from your initial distress and all the added distress from hospitalizations and drug effects. Sadly, psychological understandings are so limited after someone is declared “mentally ill”.
-S
Report comment
Try contacting these guys:
http://www.psychintegrity.org/
I wrote to them and they gave me some information about people in my area.
Report comment
Hi S,
In reply to your question, I know of nowhere with a better “system” overall. And BC is from a legal civil rights perspective almost certainly the most regressive jurisdiction in all of North America for people who’ve been psychiatrically certified. There has been very intense and very successful lobbying in BC to expand the criteria for committal and to make it impossible to refuse forced treatment. In Ontario, Yukon and Alberta, at least, a separate, second-stage process is required to declare you “incompetent” to make decisions about treatment. The Yukon has also developed some legal options that allow people to develop Advance Directives about their care if they are ever declared incompetent. BC does not allow advance directives for mental health care, nor substitute decision makers, nor any fundamentally protected right for anyone to refuse treatment under any conditions, and a person can be committed if the person is simply “at risk of substantial mental or physical deterioration.” Also, the appeal process occurs before administrative tribunals, not even courts with judges.
On the other hand, it’s true that there are a lot of alternative types of practitioners in Victoria and Vancouver. None of them can be accessed through public health care, though. There are always a few more thoughtful psychiatrists around just about anywhere, but they don’t advertise their non-mainstream thinking for fear of reprisals and marginalization, so you have to find your way to them through talking to people and the quiet back doors or purely accidentally.
Rob Wipond
Report comment
Really well-written article, Rob, and I look forward to reading Part 2. Am I right in thinking that the proposed Kimberly’s Law died of natural causes?
Report comment
To my knowledge the effort continues. Though I don’t know of any government that has yet implemented the recommendations. That said, the recommendations were arguably already in place in many respects.
Report comment
Excellent coverage. Rob, what do those who promote screening say about outcomes for those “screened” positive for mental illnesses? In 2004, I requested information from TeenScreen on outcomes for those “identified” as having a mental illness and who subsequently received treatment. In return TeenScreen send me considerable literature but absolutely nothing on outcomes.
Sadly, the following would not surprise those of us who spent any time in the adolescent mental health system: “Adolescent Psychiatric Hospitalization and Mortality, Distress Levels, and Educational Attainment: Follow-up After 11 and 20 Years,” http://alturl.com/br93x (Short URL)
Report comment
Why can’t they just let kids be kids ?
My adult job is actually easier than going to school ever was, getting up real early in the morning and then having homework assignments to stress over and tests tests and more tests. Test on Friday, and those state tests that if you screw it up no college and life is ruined…
If I smoke some meth to work harder as an adult I am an addict, but if I take Vyvance as a kid it’s medical treatment ? WTF !
If I get pissed off at work and toss my desk I will need to find a new job, If a kid gets pissed at school and tosses a desk they goto the school psychologist and before long has a ‘mood disorder’ and get put on drugs !
This is just wrong already.
Report comment
thanks for the article. If you haven’t seen it, Matt Nock’s study on suicide in adolescents is also relevant. Nock and colleagues followed a very large sample over time. Of those kids developing suicidal ideation, the bulk developed their suicidal ideation after entering the mental health system.
Report comment
This so-called mental health initiative has a fraudulent history. In 2010, psychiatrists filed a SLAPP suit (strategic lawsuit against public participation) against individuals who were outspoken about the drugging of children with psychotropic drugs. It was a $5 million suit for libel and conspiracy. These child and adolescent psychiatrists fabricated a conspiracy and called the truth libel. They did this on the day that they were in the Ontario Legislature in front of the Select Committee on Mental Health. While the Select Committee was writing up their report “Navigating the Journey to Wellness” for the Liberal Government, they waged a campaign of legal terror on us. As soon as the report came out, they dropped the suit and paid half our lawyer fees. I filed a complaint with the College of Physicians and Surgeons which they dismissed as vexatious. The Health Review Board rejected it. I wrote to the Minister of Child and Youth Services. I was told I was not allowed to talk to the Minister. I went to the Attorney General who refused to let me talk about it. I wrote to my Member of Parliament and Provincial Parliament – one never replied (the MP, Jack Layton). The head of the Toronto District School Board was also a director of the Centre for Addiction and Mental Health. The Toronto District School Board is a private corporation funded by government (so said my Member of Provincial Parliament, Peter Tabuns) and they operate independently. My own trustee works for a centre that promotes the drugging of children with psychotropic drugs. This is an insidious, vicious and cruel campaign against all enthusiastic and unique children. If parents don’t care to find out about it, we are doomed. Parents: please download the “Parent’s Exemption Form, Prior to Mental Health Psychological Screening or Counselling” from the Internet, sign it, get the principal to sign it, send a copy to the Toronto District School Board and file it in your “Valuable Documents”. Otherwise, you may have the most dangerous and powerful people – psychiatrists, the medical profession, Children’s Aid – individuals more powerful than the police and the highest courts – building a file on you and your child with devastating consequences.
Report comment
What I want to know at this point is: What was actually happening with Freya Milne? Why was she so worried? Why was she having suicidal thoughts? There is very little in all this press about her actual life. I did discover, from the Internet, that she was in the “Challenge” (gifted) program at school and had just been expelled because she didn’t feel she could complete a social studies essay in the required way. She was asking for an academic accommodation that the school was unwilling to give. Apparently, her identity rested on being in this program. I also read that the problems started when she was 10. So we have a kid with an entrenched difficulty, not someone who was overlooked and fell through the cracks, but beyond that there are no REASONS out there.
Report comment
As I indicated in the article, yes, Freya was in a program for gifted students and had a long and complex history involving school staff and mental health professionals. Some more details of that history, and of the specifics leading up to her death, are available in the coroner’s report. In addition, I know a lot more of the details through conversations with her mother. For the purposes of my article, though — which is primarily about the PSP-CYMH, not about Freya’s story — I decided that many of those details were not as important as simply noting that Freya had certainly been understood by all involved to have been struggling for years, and that inappropriate mental health interventions (and to some degree unaccommodating school staff responses as is discussed in part two) seemed to play a role in Freya’s death. What were the real “reasons” for Freya’s struggles? I don’t know if anyone can answer that definitively, or even if we should be trying to whittle that down to simplistic answers.
Report comment
I would suggest that anyone seriously interested in their future and the future of their children, born and unborn, order the book, “Psychiatry in Primary Care: A Concise Canadian Pocket Guide” by David S. Goldbloom (psychiatrist and head of the Mental Health Commission) and Jon Davine, psychiatrist. It is published by CAMH (Centre for Addiction and Mental Health, Toronto). The number is 1-800-661-1111, email: [email protected]. This book was written for your family doctor. It advocates life long medication and ECT if that doesn’t work. I started highlighting the references to ECT. It also teaches doctors how to make a diagnosis in less than 5 minutes.
We have a young woman who comes to our clinic from CAMH. She refuses to take the depo injections of antipsychotics (2 weeks in one shot) so they will not let her out. She is brought to us in shackles with 2 guards to get her functional medical care.
One of our elderly men was involuntarily committed several times one summer. They finally gave him a depo injection of Risperidal and sent him back to his family. He went home and poisoned himself to death within 48 hours. The College of Physicians and Surgeons did nothing.
I found out that people can be drugged into mental illness and trafficked to mental hospitals when they did that to my own elderly mother in August, 2000. She had no history of psychiatric care. She was deliberately given hallucinogens and tested under the influence. It is a long story, 4 complaints to the College and 2 Health Review Boards and the doctors did nothing wrong. Just a warning: if you are so audacious as to complain, they will always send you the bad news by courier just before Christmas, a family holiday, Canada Day or your birthday. That is an operation on your morale.
One word of knowledge: you cannot complain to the Ontario Ombudsman about the College of Physicians or any doctor but you can file a complaint against the Ontario Health Review Board since they are under government. It varies in different provinces, though. In Nova Scotia, there is no appeal as I found out when I filed a complaint against one of the co-authors of Paxil Study 329. You cannot sue a drug company in Canada either.
Wake up, world. This is a vicious operation that is nearly impossible to fight against. The whole shebang is designed to destroy those who try to fight back. The only hope we have is to educate the public. So if you want to keep your child safe, prevent your Mom or Dad from being committed, and if you want to live your life in peace, print this article and give it to your friends and family or send the link. Please do.
Report comment
Seems Texas may be looking into all the “best interests” of many, in this latest effort for the children:
http://www.zerohedge.com/print/491167
Report comment
additionally…”this from the BCFS (Baptist Child and Family Services) website page concerning the Weslaco/Palm Aire Hotel ‘facility’:
“The centralized intake facility will be the first of its kind in the nation, allowing for quick transfer of children from Border Patrol custody and expedited release to their families. The average length of stay at the facility will be 15 days. During that time, children will be provided room and board, in addition to basic education, recreational activities, medical and mental health care, case management, and religious services, if they chose to participate. The children will not attend public school.”
Interesting.
Report comment
Tesla: “The scientists of today think deeply instead of clearly. One must be sane to think clearly, but one can think deeply and be quite insane.” –
As a First Nation Ojibway man i can see that most non-native people place so much value in white coats, black robes and fancy suits – we do not, and neither did this man: i think his quote perfectly describes the field of psychiatry. ..”the street level drug dealers for big pharma”
Having fought through the pedophile parade that was the residential school system in canada, and then dealing with three different ‘doctors of mental health’, i think i am in a position to comment. I care not if i offend your sensibilities because these inane freaks are coming for our kids…again
As a First nations member i have seen first hand when these white robes and black robes work together to protect the status quo – it is we the people who suffer. Remember all those tests done on children at that hospital/church in Montreal, ALL sanctioned and performed by these insane ‘white coats’ and when they were done they would pass these kids on to the black robes so they could have their way with them, with no resistance.
How many times have these ‘doctors and scientists’ been found conducting illegal tests on human beings, after the fact. Not This Time. And so, these pedophile “wanna be’s” and ‘child rapist’ protectors in the field of psychiatry, best stay away from OUR kids.
I can smell the stink of ‘lies’ from these ‘scientists and physicians’ from here…and to the jack booted thugs (yes YOU-the misogynistic RCMP in Canada) and corrupted judiciary who protect them….”me and mine will no longer be the subject of criminal abuse.” So, its best they stay away from First Nations children lest their own children get ‘taken for testing’ – yes, that is a warning, and every First Nations in Canada and the ‘women warriors’ in them, now operate under this credo FYI.
Mad America indeed – get your f&*king pedophile freaks, and the ‘systems’ that prop them up, under control.
Report comment
http://www.cbc.ca/news/canada/nova-scotia/eskasoni-selected-for-mental-health-research-project-1.2691317
Dear Mr. Bellows, The above is a link to the next round of experiments on Canadian Indian children by the Boekh Foundation. That foundation is from Quebec, I believe. I attended a conference to research their experiments – Stan Kutcher attended it and several psychiatrists from Douglas Hospital as well as the head of the Boekh Foundation. Douglas Hospital is the modern name for Verdun where many Duplessis Orphans died during experiments by psychiatrist, Heinz Lehmann and company in the 40s, 50s and 60s.
The Boekh Foundation made it very clear that they had put a lot of money into researching psychotropic drugs and they wanted their “payback”. That is the word they used. Unfortunately, we can’t get the freaks under control nor can any Canadian as, I believe, the policies come from Tavistock in England. Please warn this First Nations reserve about the above experiment. Only we, the public, can get other public paying attention. Otherwise, we are all doomed.
Report comment
Maybe someone can warn people involved in Idle no More:
http://www.idlenomore.ca/
It’s not the only assault on the First Nations. They are trying to take their land again and the brave First Nations are fighting not only for their own survival but also for us all to protect us from disasters of global warming and environmental degradation. Please support them any way you can…
Report comment
Ted, I look forward to reading your ideas for revitalizing and focusing our movement. I think we could learn a lot from the Gay Rights Movement and follow much of their playbook. Their phenomenal success over these 40 years (using Stonewall as a find of starting point) could be ‘unpacked’ to use the current jargon, and used in an accelerated form by our movement. There are so many problems with our current situation–lack of lawyers, mis-steps like “mad pride.” No, “misfit pride.” Misfit is a term that almost anyone in the world can identify with, while “mad” is too loaded and negative. Just some thoughts.
Report comment
With the death of robin Williams we can again see signs of the same trend – use every personal tragedy of a famous person or every big horrific incident such as a mass shooting to justify the call for “more treatment, more mental health screening, more drugs, more involuntary treatment…”. Nobody cares that most of the people who are involved in these situation have already been through the system and it didn’t seem to have helped them nor that it’s never been shown that any of these interventions prevent violence, suicide or other personal and social problems. It’s disgusting, disturbing and it makes my blood boil every time I have to browse through the mass media after an event like this.
“Insanity is doing the same thing, over and over, and expecting a different result”.
Report comment
This article by Robert Bahlieda, principal for 37 years, should be read and considered by those people concerned with the future of our schools…..http://www.thestar.com/opinion/letters_to_the_editors/2014/08/11/tdsbs_reign_of_error_must_end.html
The previous superintendent of schools, Chris Spence, was not only superintendent of TDSB but also on the Board of Directors for CAMH (Centre for Addiction and Mental Health). He worked with psychiatrist Stan Kutcher to develop the current mental health programme in schools.
The superintendents and trustees should be investigated for conflict of interest concerning profits from antidepressant and antipsychotic drugs. When you do Stan Kutcher’s pre-seminar questionnaire for teachers, he is already promoting antipsychotic drugs for children. These drugs cause permanent movement disorders called “tardive kyskinesia” as well as diabetes and abnormal weight gain. The makers of antipsychotics, Lundbeck, has sponsored some of Dr. Kutcher’s books – a fact fine with the College of Physicians and Surgeons of Nova Scotia.
My own trustee in the Danforth area works for a children’s psychiatric centre which promotes the use of psychiatric drugs.
Please consider this statement by the psychiatrist, Heinz Lehmann, which is located in the book “Psychotropic Drugs in the Year 2000 – Use by Normal Humans”…..”The sense of achievement, i.e. the gut feeling ‘I have done something quite well’ is an experience which can probably be induced by pharmacological means.” This, of course, is the foundation for putting children on methylphenidates and amphetamines. Considering that Heinz Lehmann came from Nazi Germany in 1938 to experiment on the kids of Quebec, the Duplessis Orphans, to develop electroshock, insulin shock, the chemical lobotomy chlorpromazine and brain operations, we realize the SOURCE of these ideas. It is time to change as the plan is forging ahead with government and psychiatry planning to drug our children and march forward with experiments.
I always have to read books to remember what the medical profession can do, will do, will get away with and will be awarded for….google “Petition to the Vatican by the Duplessis Orphans” for a reminder. Please….don’t let it happen again.
Report comment
Very thoughtful article. Just to provide another point of view, I was denied meds as a minor for far too long and became suicidal before I was finally given access to even a basic SSRI. It’s impossible to get the full picture (at least in the US) of drugging children without looking at both overtreatment and at undertreatment. Some parents will always be too hesitant (or too much in denial) to put a severely ill child on a drug while others run to drugs too quickly hoping for a silver bullet.
Report comment
The problem with this is that SSRIs don’t prevent suicide – all the available data points in the direction of increased suicide risk on the drugs, especially for adolescence and young adults. I don’t want to disregard your experience but it may well have been a placebo effect which is very high for depression:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181672/
Report comment
SSRIs are only studied for 8 weeks. If you take them longer than 8 weeks, you become an experimental subject. SSRIs have dire long term side effects. There are 268 of them including drug-induced Parkinson’s disease, tardive dyskinesia (permanent movement disorders), diabetes, hair loss, problems with the nails, not to mention suicide and homicide tendencies. In my opinion, no child should be on any psychiatric drugs. Parents could buy and read Jeff Bland’s book, “The Disease Delusion”. Use the real new medicine…functional medicine. That is my experience and opinion.
The University of Toronto psychiatrist, David Goldbloom, recommends to family physicians in his book, “Psychiatry in Primary Care”…..lifelong medication. That has become the standard of care even though it is an experiment.
Report comment
I know this is true but can’t help by be outraged! It’s the kind of outrage that compels me to present the truth about psychiatry (it’s theoretical practices they touted as science) and the deceit for profit of the drug makers who lie to get FDA approval and the lies they tell.
I actually began to post on NAMI’s homepage on facebook information that was different than the mainstream crap they always post. I brought up their funding sources (drug companies and the medical industry in part) implying their views were biased because of it. I posted info about drug lawsuits, enforced the right of people to know about black box warning by posting them and put the flip side out there daily about all the issues. Needless to say I was banned from posting. This self-proclaimed advocacy group is a farce along with the industry it is part of. True advocacy will start only when the truth can be spoken without punishment.
But, I don’t think the industrial mental health complex can continue to hide the truth as people connect with one another and discuss things just like this. One by one I hope there will be a collection of people to take these monarchs off their pedestals and secure true help for those of us and all of mankind to be able to live like human beings and not collections of symptoms by some in power who abuse their authority to profound proportions. But, for this to happen people also need to quit demanding and expecting quick fixes and making uninformed choices about participating in this charade call mental health. It’s a hard leap to make but one that pays exceptional dividends.
More people need to be informed. Pass MIA on!
Report comment
And not just in America!
Little brother Australia is happily crawling along behind, not wanting to miss a single dollar. A frightening development I spotted in the newspaper on the 7/9/15 is a `survey’ that has found a `huge undiscovered epidemic of depression and anxiety, lying untreated in our society, leading to serious and unecessary suffering. This untreated, suffering group is children and adolescents. We have earnest comments from the Health minister about the need for more programs (drugs) for these poor kids and more avenues for them to come forward for `treatment’ (drugs). The article also says that ADHD diagnoses appear to be declining…(hopefully that message is getting out)…I don’t know about you but I sense a very smelly professional push behind this. The `altruistic’ and `concerned’ psychiatric profession aided and abetted by an amoral industry which may be responding to the wealth of criticism now about, whose concerns are more likely to be about a loss of customers are seeding anxious people who will do anything for their kids. With the broadening of the criteria (DSM V) they can and will rake in more and more perfectly normal children and `help’ them to become basket cases.
But our own society has a case to answer. WE set it up. WE want everything solved quickly, without pain. WE want to not look at the social issues behind any rise in children’s emotional difficulties. WE accept that people can walk away from responsibility to their kids, to not stay and work through tough times together. WE blame the government, `why don’t `THEY’ fix it? WE have sown the wind, now WE have to get off out backsides, accept responsibility, take charge and start to control the whirlwind!
I despair at times but I WILL stand up and try to stop these very bad, cynical people. I will write to ill-educated politicians and public servants who listen to `experts’ who strew pseudoscience about like straw over ice. I HAVE stood up at a Ban ECT rally. I HAVE stood toe to toe with an ECT advocate on his own forum, and on this one, and I believe I won (I’m not posted anymore). I HAVE sent a submission to a government enquiry about violence, abuse and neglect in mental hospitals, and if I can stir up legal proceedings on behalf of the brutalised and sorely injured victims of psychiatry, I WILL. WE ALL MUST.
Report comment
It would be great if Rob Wipond did a bit of a follow-up on this. Even just something brief.
Liz Sydney
Report comment
This is a resurgence of eugenics. Social Darwinism has never left us.
The objective is to create a huge portion of the population that are permanent basket cases.
We must organize and fight this. We can’t be frightened into submission by the prospect that they will consider as us crazy. By the fact that we can organize and take action, we will establish for ourselves a place in the world.
Nomadic
Report comment
the repugnant term MENTAL appears 115 times on this page. the term MENTALLY appears 7 times.
“According to a PSP-CYMH administrator, the effort is scheduled to expand this fall, with training of school staff to be more proactive “gatekeepers,” funnelling kids towards screening tests and treatments.”
according to raw reality, the gatekeepers are mentally shopping for child victims of sexual abuse, dysfunctional families, families of immorality and sin, emotional and mental abuse, physical abuse, neglect, toxic social environments and circumstantial disadvantages in order to feed them to the fking beast.
YOU’RE WELCOME FOR THE FEEDBACK.
Report comment