
Researchers recently completed a first of its kind, large-scale international survey of attitudes about mental health and they were surprised by the results. According to their analysis published in this month’s issue of the Journal of Affective Disorders, people in developed countries, like the United States, are more likely to assume that ‘mental illnesses’ are similar to physical illnesses and biological or genetic in origin, but they are also much less likely to think that individuals can overcome these challenges and make a full recovery.
“Perhaps surprisingly, where illnesses were believed to be ‘not like physical illness,’ they were also considered more amenable to prevention and recovery,” wrote the researchers, led by Neil Seeman from the University of Toronto.
“Respondents from developed countries, despite believing that mental illness was similar to physical illness (and, as a consequence, one would think, treatable and curable) had less hope for a person being able to overcome mental illness than did respondents from developing countries.”
Seeman and his team used a new survey method to gather opinion data on stigma and conceptions of mental health from all countries in the world simultaneously. The online method allowed the researchers to survey over one million people in 229 countries and protectorates around the world for each question. The researchers asked respondents about their experiences interacting with people diagnosed with mental disorders, the likelihood of violence among those diagnosed, whether ‘mental illnesses’ were similar to physical illnesses, and whether people could ever overcome such a condition.
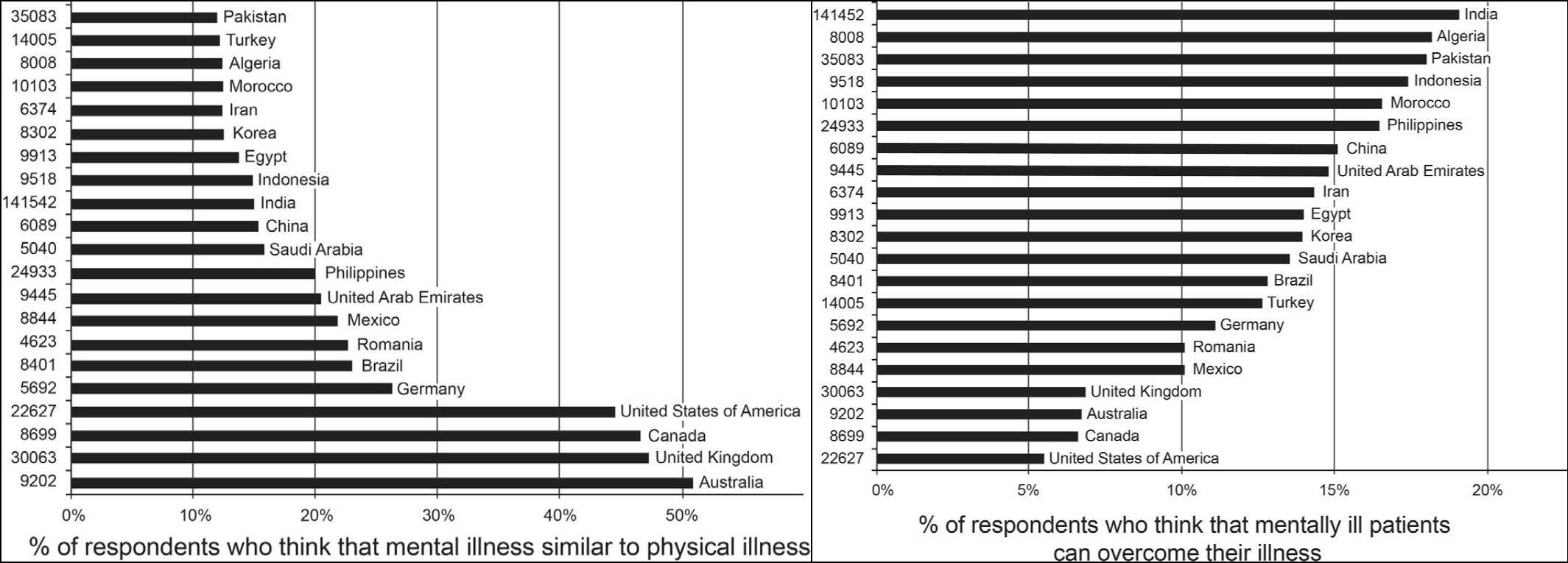
In the developed countries, like the US, UK, Canada, and Australia, 45% to 51% of those surveyed reported believing that mental illness was similar to physical illness while only 12% to 15% of respondents from developing countries agreed with this statement. However, those in developing countries were much more likely to think that patients are capable of recovery.
“A surprisingly low proportion (7%) of respondents from developed countries endorsed the statement that persons suffering from mental illness can overcome their illness.”
The results of this survey buttress previous research conducted by Pescolido et al. in 2010, which found that neurobiological conceptions of mental illnesses, rather than lessening stigma, actually increased the likelihood of social distance and community rejection.
*
Seeman, N., Tang, S., & Brown, A. D. (2015). World survey of mental illness stigma. Journal of affective disorders, 190, 115-121. (Abstract)














If “mental illness” is not physical, it’s not “illness”. It should be, in other words, easier for anyone to recover from a “false positive” than a “false negative”. That is, it’s much easier for people to recover from diseases they don’t have, but are thought to have, than it is for people to recover from diseases that the diagnostician missed. Recovering from the treatment, well, that’s a different matter.
If it’s not “illness”, it’s a “false positive”. Why whaddya know? We’ve got people recovering from “false positives”. Far be it for me to point out that we’ve got people recovering from “diseases” that literally don’t exist.
Oh, there’s a way around this dilemma, we could be dealing with “trauma”, and “trauma”, like head trauma, is “injury”, however, “psychological trauma”, that’s a whole nuther ball game, “false positive” again. I’m not denying some “trauma” may be involved, I just know that the extent of it is often exaggerated. Should a person, who is not lame, desire a crutch? You get the picture.
Of course it is easier for people who have figured the game out to play it through to the end. Were no end in sight, the way it isn’t if you’ve got a physical illness for which no cure has been found, there would be no end to arrive at. Franz Kafka knew and, therefor, his Joe K. We don’t have terminal illness here in any event, when we’re dealing with what folks call “mental illness”, we’ve got some kind black joke.
Anyway, no doubt if the developing world keeps at it they will be able to find a way to “disable” folks with words just as effectively as they’ve managed to do in the developed world. “Disabled”, that’s another good one, isn’t it? Funny thing, there are all sorts of “disabled” people who literally don’t have “disabilities”. I’m not going to unwind that one for you folks right now. I’m not, for one thing, theorizing. A hoax then can’t be a hoax if it’s a religion.
Report comment
there are all sorts of “disabled” people who literally don’t have “disabilities”
many of those people suffer from social disability i.e. stigma, which renders them unable to overcome the barrier to entry back into the economic system available to those without social ostracism.
Report comment
“many of those people suffer from social disability i.e. stigma, which renders them unable to overcome the barrier to entry back into the economic system available to those without social ostracism.”
This is an excellent point, and one way in which the government and society-at-large are tripping all over themselves.
Report comment
Don’t you think relabeling one’s victimization by socioeconomic exploitation/oppression as a “disability” is a bit disingenuous, not to mention disempowering? Again it’s put back on the individual who is “able” to do many things if the system would permit it.
Report comment
‘Disability’ can just as easily be a political term as well as a literal one. Ovrecoming it means either healing from something, adapting to something, or getting away from a sick society. Can’t be generalized.
Report comment
Don’t forget the very real physical disability of iatrogenic damage from psych drugs and/or electroshock.
Report comment
“A surprisingly low proportion (7%) of respondents from developed countries endorsed the statement that persons suffering from mental illness can overcome their illness.”
This is because the US psychiatric professionals are point blank claiming the scientifically invalid DSM disorders are real “life long, incurable, genetic mental illnesses,” to their patients and their families, despite no proof.
And this lie is being propagandized via the mainstream US media, via drug ads that propagate belief in the now defunct psychiatric “chemical imbalance” theory, to the entire society.
Report comment
Exactly. People are told that it’s hopeless, and they feel more hopeless. Seems pretty logical to me.
—- Steve
Report comment
“But mental illness runs in families”
So does voting Democrat, Republican or Libertarian.
So does being a Mets or a Yankees fan or even liking sports at all.
So does being Christian or Jewish or Muslim , that runs in families too and no one says that is genetic.
Report comment
Similarly from J Aff Dis:
“Depression is who I am”: Mental illness identity, stigma and wellbeing.
Highlights
• Identification with a group, even a stigmatized group, is protective for wellbeing.
• These relationships have not been tested in the context of mental illness identity.
• We surveyed 250 people with depression from 23 countries.
• Identifying as depressed predicted lower wellbeing.
• Identifying as depressed predicted conforming to the norms of depressed people.
Abstract
Background
Previous research has found that in the face of discrimination, people tend to identify more strongly with stigmatized groups. Social identification can, in turn, buffer wellbeing against the negative consequences of discrimination. However, this rejection identification model has never been tested in the context of mental illness identity.
Methods
A survey was conducted with 250 people with diagnosed depression or current symptoms of at least moderate clinical severity.
Results
Experiencing mental illness stigma was associated with poorer wellbeing. Furthermore, people who had experienced such stigma were more likely to identify as a depressed person. Social identification as depressed magnified, rather than buffered, the relationship between stigma and reduced wellbeing. This relationship was moderated by perceived social norms of the depressed group for engaging in depressive thoughts and behaviors.
Conclusions
These findings suggest that mental illness stigma is a double-edged sword: as well as the direct harms for wellbeing, by increasing identification with other mental illness sufferers, stigma might expose sufferers to harmful social influence processes.
Report comment
The lead fails to mention another finding – a much higher percentage of people in the less developed countries perceive people with mental illness to be more violent than those who do not have mental illness.
Report comment
Who gets to call who mentally ill?
People who are overcome by their feeling of anger ARE mentally ill? Rather than criminals?
People fear the “mentally ill” will be angry? so drug them for life? to prevent them from becoming criminals?
Report comment
People don’t have mental illnesses. The way these questions are asked stems from the way the APA and psychiatrists have distorted the narrative about what life problems and emotional suffering are over the past 35 years. It all goes back to the guild interests and pharmaceutical company pressure that Whitaker and Cosgrove wrote about in their book. Most of the public answering these questions have now been duped into believing that mental illnesses are valid and separable from “normality”, and so they answer the question based on these distortions.
But people don’t have or not have mental illnesses. Emotional problems occur along a continuum of severity and anyone can experience mental problems to different degrees at different times under different stresses. The lack of validity and reliability of the psychiatric diagnostic categories is also the reason why most psychiatric research is non-replicable garbage.
Report comment
People do have mental illnesses , but the wealthy and powerful usually get to decide who is and who isn`t.
An example where the person is NOT mentally ill, but another person thinks they are is the husband and wife who are fighting. In the past if the man was wealthy enough he could put his complaining wife away in a “hospital” after accusing her of being mentally ill for not obeying (his) orders.
Today people do use the persuasion of psychiatry on their misbehaving children, who are not really “sick” in a medical way. Little do they know of the damage they are causing to their child’s soul.
An example of genuine mental illness would be the hoarder. I think you have seen examples on TV . The person has an irrational fear of throwing anything out, and their homes are firetraps and/or full of bugs and vermin.
Another example of genuine mental illness is someone who abuses drugs such as alcohol , in excess. They use so much drugs their life is unmanageable, as in they can not perform any kind of work.
Report comment
This is BS. There is no known etiology behind “alcohol abuse” being an illness, or “hoarding” being an illness. These are highly variable complex behaviors occurring along a continuum of severity, caused by many different causes in each case. They’re not illnesses like diabetes or influenza.
Come on dude. If you want to say alcoholism and hoarding are illnesses you need to provide some evidence. Until then they’re problematic behaviors.
The only mental illnesses we know of right now are Alzheimer’s, dementia, Parkinson’s, etc.
Report comment
I agree with your first two paragraphs, that so called ‘mental illness’ is not a real biological illness/disease like diabetes or influenza, but I disagree with your last paragraph.
Alzheimer’s, dementia, and Parkinson’s etc are NOT ‘mental illnesses’, they are classified as organic brain disorders. These conditions are known to affect the brain and are physical/biological in nature. So called ‘mental illnesses’ (such as depression, anxiety, etc) affect the mind, and are nonphysical/nonbiological and therefor not an illness/disease.
Although they are connected, there is a difference between the mind and brain. Psychiatry does not acknowledge that distinction, which is why they claim that ‘mental illness’ is a real biological illness/brain disease/chemical imbalance, which as I’m sure you are aware, is a complete load of hogwash.
Report comment
Regarding “alcoholism and hoarding”…”they’re problematic behaviors”.
A behavior is something you can choose to do , or not to do. In both drug addiction and hoarding the person is not in control of their actions. They apparently have no choice.
Drug addicts have a physical dependency on a chemical. The hoarder might be already on mind altering psychiatric drugs.
Report comment
Ragnarok,
I mostly agree with this. I am certainly not an expert on things like Parkinson’s or dementia. But I think you’re right I should have said that these are varieties of real brain illnesses. I think that that distress and suffering in all its forms is reflected in brain chemistry too; it would be foolish to deny this, but I don’t think it’s caused by misfiring brain chemicals or that different forms of distresses are separable as discrete entities by talking about them as discrete brain based illnesses. That is ridiculous as you said.
MarkPS2,
I have to say I don’t understand these reasonings. You said,
“A behavior is something you can choose to do , or not to do. In both drug addiction and hoarding the person is not in control of their actions. They apparently have no choice. Drug addicts have a physical dependency on a chemical. The hoarder might be already on mind altering psychiatric drugs.”
If a behavior is only something you voluntarily choose to do, then I guess an ISIS prisoner being forced to walk from a prison to their mass grave site is not a behavior. Or a North Korean being forced to toil on a farm against their will is not a behavior.
Regarding drug addiction, I think people have less choice than they would like to have, but can also with help get increasing power to control their behavior. After all if people were truly drones who took drugs with absolutely no control over their actions, then no one would ever stop taking drugs. But through things like psychotherapy and support groups people can stop or at least reduce their intake of drugs. This indicates that the behavior can be controlled and modified. So it is not an involuntary illness.
As for hoarding, that is flatly ridiculous to me to call it an illness. Where do you draw the line between the guy who needs to keep 2,676 old magazines in his bedroom and the guy who only needs to keep 65?
Key issues here are causality/etiology, reliability, and validity and we simply have no clear evidence that biological processes are causing behaviors like hoarding and taking drugs. Also these behaviors are complex and can vary in intensity at different times. So it is not easy to separate them from lesser forms of the same behavior or related behavior. That is why I think they are not illnesses like diabetes which have a more reliable presentation and a clearly known biological basis, and thus have validity.
Report comment
@bpdtransformation, B.A.
Regarding “Where do you draw the line between the guy who needs to keep 2,676 old magazines in his bedroom and the guy who only needs to keep 65?”
If the guy with 2,676 magazines has other rooms that are fully functional ( bathroom , bedroom, kitchen), yes there is no difference between the two. If the guy with 2,676 magazines lived in the country, no one would care if his house caught on fire or was filled with bugs/vermin. Its only because he is close to others who have possessions in a city that an individuals hoarding can be questioned by authority.
Regarding ” an ISIS prisoner being forced to walk from a prison to their mass grave site…. a North Korean being forced to toil on a farm against their will”
Or a person labeled mentally ill is forced to take-ingest chemicals that shorten his life by 25 years?
ISIS prisoner could chose to get shot where he stands. Korean could chose not to eat/work.
“etiology + biological processes”
Right. You say there is no mental illness as in biological illness. That is why its called mental not physical illness.
I say there is no such thing as money (physical), yet everyone else believes money exists.
Report comment
Bottom line, Mark, is that you or whoever are setting arbitrary standards of “illness” that would never be accepted in the world of physical medicine. What is and is not considered problematic is very much a socially-mediated question. “Normal functioning” is defined differently in every culture and subculture, and pretending that interference with “normal functioning” constitutes an illness is most definitely a scientific fallacy of a high degree.
As to whether people have a choice or not, we seem to have dropped the concept of unconscious motivation out of our discussion of “bad behavior” in the last 40 years. People make choices, but they’re not always aware of why they do so. The hoarder is CLEARLY deciding to prioritize keeping unnecessary things because it meets some internal need that s/he is not aware of. The fact that this need and the attendant choice is not conscious does not make it any less of a choice. In fact, really good therapy, in my experience, is very much about making people aware of WHY they feel they have to act a certain way, which enables that person to make a more conscious and intentional choice rather than feeling s/he has to go along with the script unconsciously laid down by his/her past experience. I’d say the same applies to drugs or alcohol, although long-term use does make quitting a much more challenging decision to make. No one stops drugs without deciding to stop. It is a decision to continue, even if it doesn’t feel like it’s in the addict’s control.
—- Steve
Report comment
Markps2
You stated: ” In both drug addiction and hoarding the person is not in control of their actions. They apparently have no choice.”
People with addictions DO have a choice. It is ultimately a CHOICE that allows people to stop their addiction. This is part of the reason why it should not be classified as a disease, in addition to the fact that there are no biological markers.
People may have to struggle to overcome physical (and cognitive) urges and cravings, part of which are compulsive thoughts to continue the negative behavior.
No body chooses to become an addict. It is usually a process that creeps up on a person until they finally realize that the drugs, alcohol, or other addictive behavior seems to controls them more then they can control IT.
Then they must find a way to overrule those thoughts that justify continuing the addictive behavior and develop new thoughts and behaviors that lead to different and more healthy choices.
I believe many of the same concepts also apply to overcoming hoarding behaviors and the thoughts that justify those habits.
Richard
Report comment
To Richard — Thanks for clarifying your take on addiction. It makes sense to me.
Report comment
These “examples” of “genuine mental illness” are examples only of disturbing and self-destructive thought, feeling and behavior.
“Mental illness” is a logical impossibility; it is never “genuine.”
Report comment
True. In some less developed places in Central and South America people who suffer from psychological and emotional distress are kept captive in very small huts. This is something that those who talk about how much better outcomes are in less developed countries do not want to talk about. The people are virtual prisoners and often treated like animals.
Report comment
One possibility is that those in less developed countries are less likely to label “different” people as mentally ill. In order to be labeled as mentally ill in those countries one must show more violent behaviors then over here in the good old USA. That’s my hypothesis anyhow.
Report comment
I note that the first graph states that it is % of respondents who think that mental illness is similar to physical illness. The head of our ambulance service was on tv two nights ago regarding the suicides by ambos, and he stated that “mental illness is EXACTLY THE SAME as physical illness. I was gobsmacked.
Report comment
Whatever anyone feels “mental illness” is or is not, believing that there is no healing from this must make a lot of people deathly afraid of discovering their own mental confusion and darkness. We all have this aspect to ourselves, it is not a select population, it is universal.
Pessimism means lack of hope, which, to my mind, is a precursor to the darkness of life. Good luck with that…
Report comment
I appreciate you making this point, that all people experience mental confusion and darkness at one time or another. Few people want to admit this.
Report comment
Integration means owning our shadow. Once we do, we drive it, rather than the other way around.
Report comment
In fact, Stephen, this got me to thinking. When we do NOT own our darkness or shadow, and instead deny our flaws, then it repeats over and over until we finally get the hint–that it’s ok to be human and it’s ok to be whatever it is we are, that we all grow and evolve from where we came. Life is a perpetual learning curve.
That repetition, I imagine, is what eventually leads to either mental or physical illness, because no matter how we try to avoid it, it just gets bigger and bigger. That is, until we surrender to it, own it, and decide that we can love oursevles unconditionally, mistakes, foibles, flaws and all. Perhaps that is what few people are willing to do.
Report comment
This is not a surprise. But it points so why the DSM, ICD, and psychiatric diagnosing / the disease model should be utterly abolished and wiped from the face of the earth. People’s life problems are not reducible to illnesses.
Report comment
If mental illnesses are a result of biological abnormalities, it should be possible to detect these mental illnesses just like any other disease (such as detecting a condition like diabetes). But despite decades of research, scientists have not been able to find any structural or other brain differences between psychiatric patients and healthy individuals.
Due to this, diagnosis and labelling of mental illness is based entirely on doctor’s subjective evaluations (check lists) – there are no blood tests, tissue tests, X-rays or any of that – no objective tests at all. Diagnosis made this way also fails to meet the Virchowian standard of disease.
Having a label itself can be devastating to a patient, leading to more depression and thinking that they are somehow different from others, etc. Since the mind can change the brain (neuroplasticity) – as a result of a label, thinking that one is mentally ill and different from others, and ‘doomed for life,’ etc., can itself lead to more worries and depression over time, which would also change the brain (adversely) gradually.
I think instead of giving labels to mental illnesses, treatment should focus on the symptoms of the patient (such as stress, worry, a habit, hearing voices, etc.) and direct attention on treating those specific symptoms. This will also reduce stigma.
Report comment
Interesting research and discussion. Good intentioned people from politicians, policymakers and mental health professionals and others made “mental illness” more of a “physical illness” in order to reduce stigma as well as get insurance coverage. Mental health is a continuum. People do get better with good treatment and supportive environment. I have been privileged to be a part of many clients’ recovery, individuals whom really recovered especially when I did inpatient state hospital work sometimes just because someone believed in them and held hope. Certainly attitudes make a difference. If one (consumer, professional, family member, society) thinks that if you have been diagnosed within the medical model of diagnosis of DSM 5 your fate is that you will “never” be okay, “never” hold a job and be a functioning member of society, “never” get off state benefits, etc. then certainly that may become a self-fulfilling prophesy.
It takes tremendous amount of persistence and tenacity to get oneself out of the system and find healing. Though I have been part of the problem as a professional working in a broken system and disheartened many times witnessing bad care and bad treatment though I do fight back as much as I can and advocate for my clients, I have also witnessed the courage of many individuals break out of the patient role and live fulfilling lives of their choosing. I have seen good work by dedicated professionals and still hold onto that as well. It is not “us” vs. “them” as we are all humans looking for a life free from suffering. The problem arises with funding sources, how to pay for good care and environments. I have been through closing of many good places due to lack of adequate funding. Healing is often not a short process, takes time and hard work on the part of the client. You get out what you put in and healing occurs through different modalities depending on the individual, their background, resources, etc. Creating bigger support system for individuals to succeed in the communities is the key plus resources for housing and employment opportunities as need financial resources as well.
I wish my profession could go out of business and everyone would be healthy and free from need for professional intervention. Every citizen has a responsible to each other in this society. We are all called to be advocates for social justice and equality, we can all do our part by taking responsibility for our words and actions.
Report comment
You sound like the kind of therapist that was common when I started in the field. Unfortunately, your kind are becoming rarer and rarer over time. I hate to say this, but the main reason the DSM 5 diagnosis appears to indicate a fate of never recovering is not because the clients somehow infer that, but because THAT IS WHAT THEY ARE TOLD by mental health professionals. They are told they have a chemical imbalance in their brains, that it is incurable, but that if they take their medication faithfully, often for life, they may be able to function. Many with bipolar disorder of schizophrenia diagnoses are told that they should give up on their ambitions and accept that they have a disability and will be in treatment the rest of their lives. It is a most disheartening message, but it is delivered by our professionally-trained mental health workers, including psychiatrists.
And it is a self-fulfilling prophecy, especially for those for whom the medications don’t work or have adverse effects of major significance, which is actually quite a high percentage, especially when looking at those diagnosed with “bipolar” or “schizophrenia.” These people are dying years earlier than their non-drugged counterparts, mostly because of the very drugs they’re taking to supposedly improve their lives.
A fairly recent survey asked people with mental health diagnoses who gave them anti-recovery messages after hearing about their “disorder.” The #1 culprit, at something like 75% of the cases, was mental health professionals.
Folks like you may be helping, but you are a small fish in a very big ocean of distorted training and messaging. I’m glad you’re there to help counteract it, but the truth is, a large hunk of the negative stigma around being diagnosed “mentally ill” comes from the diagnosis and the people who assign it.
—- Steve
Report comment
“hunk of the negative stigma around being diagnosed “mentally ill” comes from the diagnosis and the people who assign it. —- Steve”
I agree.
This stigma is part of the system. If the “patient” feels there is nothing wrong with himself, why does he need any help?
The helper can not help the “sick” without the sick believing they are sick and need help from someone learned.
There needs to be some kind of evidence the person is ill. A brain chemical imbalance induced by psychiatric drugs is perfect.
“The antipsychotics block 70-90 percent of the dopamine receptors in the brain. In (response) return, the brain sprouts about 50 percent extra dopamine receptors. It tries to (compensate) become extra sensitive. So in essence you’ve created an imbalance in the dopamine system in the brain. You (now) have too many dopamine receptors. And what happens? People that go abruptly off of the (antipsychotic) drug, do tend to have severe relapses.” ― Robert Whitaker
Report comment
This is spot on my conclusion, too, Steve, at the end of it all. I found the stigma and mythology which is attached to ‘mental illness’ begins and ends with the mental health field.
What society at large picks originates there, these toxic and distorted messages about ‘mental illness.’ The main one being, “You are a chronically ill person who will be dependent and limited for life,” which of course inherently marginalizes a person from the get-go–not just from society, but from themselves, as well. That is a perfect split, a literally crazy-making double-binding, gaslighting message.
And as you say, I do think it is self-fulfilling, until we wake up. That awakening is vital in order to effectively address those ingrained internalized negative messages. That’s what really screws people up, those constantly running programs of perceived dependence, limiations, and marginalization. That creates all sort of distorted and self-stigmatizing beliefs, to where if no one is around to put us down, we just do it ourselves, and then we imagine everyone else is doing us, too, that’s a common projection that comes from social stigma trauma.
That’s what stigma does. I think the stigma is the root of this ‘chronic mental illness’ routine, and all of society’s fears around this. This originates in the mental health field. It’s like a cancer spreading.
Ascend those false beliefs, see the truth of the matter–that we can heal, move on, and create our life and dreams the way we wish once we ground and focus, and this is universal, I firmly believe–and that becomes a new internalized program, sans stigma, based on personal truth and self-compassion, which will support healing. That was my experience, in any event. It worked.
Report comment
And, for anyone in a process of healing, I’d highly recommend getting away from people who send you messages that you cannot heal. That helps no one, and in fact, embeds the stigma, mythology, and chronically crappy feeling. In fact, I believe this strengthens the mental health system, by default.
The idea is to create a community of yay-sayers, not nay-sayers. That will make ALL the difference in healing and personal growth, to where it is actually possible. Naysayers sabotage healing.
Report comment
” a literally crazy-making double-binding, gaslighting message. And as you say, I do think it is self-fulfilling, until we wake up. That awakening is vital,” I absolutely agree, Alex.
“It’s like a cancer spreading.” Again I agree, the psychiatric industry is functioning as a cancer on all of humanity.
We need to learn to coexist, not take away hope, and stigmatize others – that’s childish behavior. Gas lighting people is “mental abuse,” not medical care. And taking away hope is evil.
Not to mention, today’s psychiatric “gold standard” treatment recommendation for “bipolar” (the “mood stabilzers, antipsychotics, antidepressants, antidepressant-antipsychotic, and anti-anxiety medications”) is a recipe for how to create psychosis via the central symptoms of anticholinergic intoxication syndrome, aka anticholinergic toxidrome.
“Agents with anticholinergic properties (e.g., sedating antihistamines; antispasmodics; neuroleptics; phenothiazines; skeletal muscle relaxants; tricyclic antidepressants; disopyramide) may have additive effects when used in combination. Excessive parasympatholytic effects may result in … the anticholinergic intoxication syndrome … Central symptoms may include memory loss, disorientation, incoherence, hallucinations, psychosis, delirium, hyperactivity, twitching or jerking movements, stereotypy, and seizures.”
And this information about anticholinergic toxidrome, from Wiki:
“The symptoms of an anticholinergic toxidrome include … delirium, … hallucinations, … memory loss, … myoclonus, psychosis, seizures, … Substances that may cause this toxidrome include the four “anti”s of antihistamines, antipsychotics, antidepressants, and antiparkinsonian drugs[3] as well as atropine, benztropine, datura, and scopolamine.”
It’d be nice if the psychiatric industry would grow up and get out of the business of making people psychotic with their drugs. How sick can an industry get?
Report comment
I’m actually referring specifically to the stigma generated by psychiatrty as being the cancer. I see psychiatry as the creator of the stigma, as a way of separating themselves from their patients/clients; and I see the metnal system as the conduit to society via media, starting with ‘research published in journals, etc. Of course, the DSM is the stigma bible.
And yes, Someone Else, I know you are very aware of the gaslighting and double binding tactics, good for you! To me, this is subtle awareness, and what gets so messy, of course, calling it out as the abuse that it is, it is all smoke and mirors to produce confusion and conflict. I think it’s really the most common and insisdiou form of abuse happening in general, because it remains a bit invisible to some, it creates a lot of ambiguity, that’s the point, so no clarity is achieved. Keeps things status quo.
I believe blatant stigma is used as a tool to gaslight and double bind: “if you do or say such and such, it only PROVES your the crazy one, not me.”
Total rubbish, and indeed, it is cruel mental abuse, it can be tortous for people, espeically if they are vulnerable and trusting. and it’s particlularly troublesome in the field of so called ‘mental health.’ This is what creates the illusion of ‘mental illness’ where it mostly likely does not really exist.
Report comment
Sorry about all the typos in this comment, Forgot to proof.
Insidious, not insisdiou
Torturous, not tortous
etc.
Report comment
Thanks for comments, Steve. I cannot agree more that it has been mental health professionals that have incurred a lot of harm and we need to collectively own it and change it. As LICSW I can diagnosis and legally do Section 12s. Not something I like doing but have had to if working within established mental health system. I have seen some good changes to the system though with reduction in restraints and introduction of peer specialists and increased person-centered approach. Part of the difficulty had been in retraining staff’s mentality but also changing clients’ mentality. Empowering clients now meant asking more of them, not treating them like children, but giving them opportunities and encouragement to grow which meant discussions about working, doing more for oneself, not expecting others to do for you but to be taught how to do it on one’s own. I will be honest, not everyone is buying that “recovery cool aid” as one of my colleagues at a large human service agency in Boston stated aptly said about clients leaving state institutions. Everyone is at different stages in the process. Change is slow. Growing up and maturation process for all.
Report comment
Exactly.
You would think that when peer workers talk about how everyone has the chance to heal and move on with their lives that the so-called “patients” would jump at something like that. This is not the case at all. Many people give it little if any consideration at all. There is a certain comfort in knowing what to do and what not to do, especially if you’ve been in the system for a while. Taking the journey to try and find healing is not a sure thing, you don’t always know what to do and when to do it, especially if you’ve been in the system since you were a teenager. The system has done very well at the job of helping people to learn helplessness. So, when we begin requiring more responsibility from people in the system there must be some understanding on our part that they probably may not always know what it feels like to be responsible.
Even if psychiatry’s drugging of people came to a stop tomorrow, and even if we had all the things in place to make sure that everyone could move forward out of the system, there’s going to be a whole lot of people who may decide that they want to remain exactly where they are. Even if everything changes, there will still be lots and lots of people who will probably need significant help for the rest of their lives. I sometimes have the feeling that many in the movement don’t stop to think about this. Those of us who work every day with people stuck in the system I think probably give it lots of thought.
Report comment
Thank you, Stephen, for your comments. You hit on the topic that I kept being surprised by when working in adult mental health system and quite frankly burned me out. Learned helplessness was rampant. Culture and belief system of disability not ability. Some more motivated than others. I had been working in the child and adolescent state system prior to moving to DMH adult system and our motto was get them out of the hospital and mental health system quickly, get them into society with peers that were healthy, and do not get them associated with adult system for fear they would never get out and become institutional minded. Our program offered thousands of dollars of great vocational programs free that would offer great career opportunities that myself and others I know would have jumped at due to the economy, but only a couple of the two hundred clients took advantage of it. I was shocked, but if part of a culture that expects nothing of you, that all your needs will be met, financial, housing, medical, etc., why put in the effort? For some, being a “victim”, a “mentally ill patient”, “disabled” was an identity that was comfortable. I felt often that I was working with adolescents if not younger. There were definitely developmental milestones that somehow got missed. I kept thinking how can this be a life worth living? We used motivational interviewing techniques and all sorts of ways to get clients to do more for themselves. I was impressed with the small steps that some did, getting job or volunteering after multiple years of not working, even if just a few hours a week. Institutionalization was/still is a very expensive thing, over $1200 a day. Living in the community is also an expensive thing, housing expenses, new mental health model of community case management, health care, etc. There will always be a subset that want to be taken care of and lack motivation and hope to do better for themselves. Many of their families have given up on them from burn out too and have felt guilty but had to put them in group homes. Those who have risen out of the system are unique but their standards are not what others may want or seek.
Report comment
Have had mental “health” professionals go into screaming tirades at me during groups, accusing me of not being able to accept my diagnosis.
Ironically I think I was doing an excellent job at the time, although I carried it to extremes that the professionals were simply not logical enough to understand as necessary outcomes for the beliefs they coerced me to buy into.
I took my drugs religiously, sort of like the Catholic eucharist. I thoroughly believed in my mental illness diagnosis and was duly filled with self-loathing and an uncontrollable urge to kill myself. Why not? I defy any psychiatrist to tell me why suicide is sick or irrational if you believe yourself to be broken, evil, and subhuman. That’s simply having “good insight.”
Back to the irate group leader. The things I did that seemed to cause her rage were:
1. I insisted on completing my B.A. and even talked of going to graduate school for a while.
2.I wanted to get a job–other than piecework at a sheltered workshop–and eventually get off SSI. After all, why take “meds” if they don’t improve your quality of life?
3. I got bored of hanging around in segregated groups with glassy-eyed zombies who only wanted to play bingo and watch TV.
4. I read a lot. For some reason, a lot of people in the System saw this as a threat. Claimed I wasn’t socializing enough with my “peers” and was on my “high horse” thinking I was better than everyone else. After all, who was I? Just another nut job after all!
Report comment
I do agree with you about recovery. Unfortunately, too many of the patients have been trained to believe the mantra that we are talking about. That might be a difficulty for some people regardless, but one thing we CAN change is to stop convincing them it is true! EMPOWERMENT is the key to recovery. Teaching people what they ARE capable of, sometimes against even their own deep inner belief, is what we should be doing, not teaching people that they are condemned to a lifetime of disability!
Change is slow, but it’s slower when people with vested financial and power interests don’t want the change to happen. Sadly, I think that’s what we’re up against here. There are too many people making big bucks off of the “lifetime disability” meme to allow a few inconvenient fact stand in the way. After all, if we start empowering everyone to recover, they’d have to start finding new clients!
— Steve
Report comment
I agree, the negative programming runs deep. Getting away from naysayers when possible is a good start to healing through empowerment and self-compassion. That can be a process, sometimes, not so simple. But I think it’s a good goal.
The next stage of healing would be to shift into a more positive self-belief, even if it is slight at first, at least that’s a good shift for starters. It can be challenging to shift from feelings of disempowerment to knowing our personal power, and confusing at first. Takes practice to see ourselves in a new light, but I agree, Steve, that’s how we heal.
It is relieving and clarifying to be aligned with ourselves, rather than to be at odds with who we really are. That’s what creates a lot of grief and anxiety. People deserve better than to feel condemned to a lifetime of limitation and marginalization. That belief doesn’t exactly whet one’s appetite for living.
Report comment
Bingo, vested self-interest is a real issue. Basic economic theory of supply and demand and the psychology of fear and greed. See it in business and political world, unfortunate when it occurs in healthcare and healing professions. Ethics and morality still never old topics to discuss in every discipline. Thanks for interesting topic. May we all be healthy and at peace in our own truth.
Report comment