
To me, “May is Mental Health Month” has always seemed like an excuse to hold an annual four-week-long commercial for Pharma and bio-psychiatry. Under the guise of raising “awareness” and reducing “stigma,” the PR reps out there make it safe for us average Joe’s to admit how bad we feel or how stressed out we are. Then they tell us what our problem is (“mental illness”) and conveniently offer us the solutions they are selling (pharmaceuticals and professional treatment). It’s like the soda industry taking over July and turning “thirst” into a public health concern. Yes, every summer, you suffer from an urgent, potentially deadly, recurrent craving for liquid — but thank god Coke and Pepsi have thoughtfully created products that will relieve your symptoms if taken daily as directed!!!
Suffice it to say, I’ve become a bit jaded. The flashy flyers, sagacious slogans and tantalizing toolkits notwithstanding, my pessimism about the possibility of anything paid or professional in the mental health industry to actually make the world I live in better instead of worse has grown exponentially with repeated exposure. For sure, during the first few rounds, there was excitement from the initial hype and the opportunity to actually participate and DO SOMETHING. But inevitably, for me, this was followed by let-down as retrospective awareness set in. Hey, WTF…? I just put a boatload of energy and effort into this. But very little that actually matters to me has actually changed…
The release of the Power Threat Meaning Framework by the British Psychological Society earlier this year1 might just have changed that for me. Thanks to the British Psychological Society (BPS), there might finally be a provider-proposed paradigm that is worth the effort of making the public aware. In contrast to the medical (“mental illness”) model, the Power Threat Meaning Framework (PTM) is a non-pathologizing, unifying model of human bio-psycho-social functioning. It applies to all human beings — not just those of us with mental health labels. It is also not just for providers. Rather, it invites everyone to look at and offer their experience. And it supports all of us to recognize, and make sense of, the diverse, culturally relevant strategies that people around the world may employ in order to survive, meet our core needs, protect ourselves or cope with overwhelming emotions.
This is a key difference between PTM and mental health as usual. Conventional mental health approaches take society as “normal” and endeavor to treat so-called “maladaptive” individuals who fail to “adjust.” PTM, on the other hand, makes clear that meaning and distress must be understood and addressed at social, community and cultural levels, not just individual ones. In a 400-page meticulously-researched tome, PTM connects the dots and persuasively links wider social factors — like poverty, discrimination, abuse and violence — with the distressed or distressing emotional and behavioral responses that are currently being pathologized as “mental illness.” It joins the United Nations in urging a global shift in focus from “chemical imbalance” to “power imbalance” in mental health awareness and practice.2 3 As PTM aptly observes, “The less access you have to conventional or approved forms of power, the more likely you are to adopt socially disturbing or disruptive strategies in the face of adversity.” Accordingly:
The crisis in mental health should be managed not as a crisis of individual conditions, but as a crisis of social obstacles which hinders individual rights. Mental health policies should address the “power imbalance” rather than “chemical imbalance.”
Why This Matters
We don’t care if you have MD’s or think you are the boss of us. We’re no longer going to follow your orders or consider ourselves bound by your thinking. We think you are wrong on the merits. We think your approach is hurting our clients. Accordingly, we are throwing out the model you developed and proposing our own.
In a word, it’s a revolutionary act. Every other mental health-related profession in nearly every country in the world has basically caved to whatever the medical model is dishing out. Despite the claim of psychologists, social workers, psychiatric nurses and clinical mental health counselors to be “professionals” in their own right — that is, to have their own specialized knowledge, to promote the greater good, to operate in the public interest, to serve needs and interests of the clients who sought their services4 — these self-professed “independent” bodies have, by and large, abdicated their responsibility to conduct their own independent analyses. To the contrary, they have all but chewed up and swallowed whole whatever the psychiatric industry was dishing out.
Their major excuse: “We can’t do anything. The insurance industry has tied our hands.” Which begs the following questions:
- What kind of profession, worthy of the name profession, let’s slimy corporations like insurance companies determine how they do business?
- What kind of profession, worthy of the name profession, claims to serve the public interest by conforming its knowledge and practice to the dictates of insurance claim examiners?
- What kind of profession, worthy of the name profession, claims to serve the best interests of its clients, when it continues to perpetuate an insurance billing model that does not reflect the actual needs and life circumstances of the lion’s share of its clients?
- What kind of profession, worthy of the name profession, continues to bill insurance companies and collect tax dollars from medicare and medicaid on the one hand, while, on the other hand, whispering to their clients behind closed doors and out of public eye: “We know the DSM is a disaster and we don’t believe that you really have x-diagnosis. But you don’t want to have to pay for this out of pocket, right? [Wink wink nod nod].”
- What kind of profession, worthy of the name profession, continues to actively and publicly represent that more and more social services funding is needed for more and more off-target, non-responsive services that slander the very clients they claim to serve — because that is what insurance companies will pay for?
I don’t know about you, but the law school I graduated from had a 5 letter word for this kind of conduct: F-R-A-U-D.
Declaration of Independence
Not true, however, with psychologists in the UK. They stopped relying on the Nuremburg defense: “Someone else is responsible for my values.” Unlike other mental health “professionals,” they did not delegate their duty to their clients or their duty to develop an informed opinion to the “higher authorities” of doctors, insurers and drug companies. Instead of taking the easy route and abdicating their responsibility, they actually did the hard work that therapists have been telling their clients to do for decades. They stood up. They took back their voice. They took back their agency. They took back their self-respect, their dignity and their personhood. They did their own research and reached their own conclusions. They developed their own hypothesis of what is going on in the minds and bodies of the people they serve.
And when all was said and done — the analysis in, the research exhaustively reviewed — they said to biopsychiatry:
No more. It is finished. We withdraw our consent. We can no longer, in good conscience, defer to your judgment about what is right for the vulnerable, trusting souls who cross our threshold in search of our honest expertise and aid.
Now, that, in my book is something worth making the general public aware of. So here goes:
May 2018 is Power Threat Meaning Month: Online Series
This online series of mental health awareness events introduces the Power Threat Meaning Framework released earlier this year by the British Psychological Society. All events are online and accessible by computer or telephone. Workshops and mini-retreats feature facilitated discussions on the foundational topics and concepts of the PTM model. Sessions will revolve around several core questions adapted from the PTM materials:
- What has happened to you? (In what ways have you felt over-powered, under-powered, dis-empowered …?)
- How did this affect you? (What threats has this posed to your needs and survival?)
- What sense can you make of it? (What did these situations and experiences mean for you?)
- What did you have to do to survive? (What strategies did you use to respond to threats or create meaning from adversity?)
- What values, strengths and resources have you been able to access? (What power resources are known and available to you?)
- What is your story? (How does all this fit together?)
To Join Us:
Join by computer: https://zoom.us/j/119362879
Join by phone: +1 669 900 6833 or +1 646 558 8656
Enter Meeting ID: 119 362 879
International callers: https://zoom.us/u/jkwt3wHh
Schedule of Remaining Events
Wednesday, May 9th ~8-9:30 pm EST
Surviving Rejection and Invalidation
Friday, May 11th ~8-9:30pm EST
Surviving Childhood Adversity
Saturday, May 12th ~2-5pm EST
Mini-Retreat
Power, Threat and the Meanings of “Mothering”
Tuesday, May 15th ~8-9pm EST
Emily Sheera Cutler
Death by Oppression: Suicide as a Natural Response to Marginalization
Wednesday, May 16th ~8-9:30pm EST
Surviving Disrupted Identities and Roles
Friday, May 18th ~8-9:30pm EST
Surviving Setbacks and Defeat
Saturday, May 19th ~2-5pm EST
Mini Retreat
Power, Threat and the Meanings of “Suicide”
Sunday, May 20th ~2-5pm EST
Mini-Retreat
Power, Threat and the Meanings of “Mania”
Wednesday, May 23rd ~8-9:30pm EST
Surviving Entrapments
Thursday, May 24th ~8-9pm EST
Emily Sheera Cutler
Smashing Paternalism: Intersections Between the Consumer/Survivor/Ex-patient Movement and the Fat Acceptance Movement
Friday, May 25 ~8-9:30pm EST
Surviving Disconnection and Loss
Saturday, May 26 ~2-5pm EST
Mini-Retreat
Power, Threat and Angry Meanings
Sunday, May 27 ~2-5pm EST
Mini-Retreat
Power, Threat and Addictive Meanings
Sunday, May 27th ~Starts 10pm EST (Ends 12:12am EST on Tuesday May 29th)
MEMORIAL DAY STORY-TELLING MARATHON
26.2 Hour Vigil — Our lives go the distance
Bring your story — Bear witness to others
Drop in or sign up for time in advance
Tuesday, May 29th ~8-9:30pm EST
Surviving Social Exclusion and Shame
Wednesday, May 30 ~8-9:30pm EST
Surviving Coercive Power
For more info:
- Email Sarah at: [email protected]
- Visit our conversation on Facebook at the Wellness and Recovery Human Rights Campaign, facebook.com/groups/WellnessRecoveryRights/
Power Threat Meaning (PTM) in a Nutshell
Mental “illness” has meaning. The meaning comes from this:
1. Lack of Power
For a variety of personal, social and cultural reasons, we come to feel under-powered, over-powered, powerless or accountable to be powerful in ways that seem vitally important to us.
Here are some common examples of ways that lack of power can touch our lives:
- Body power — society values preferences, attributes and abilities that we don’t have or identify with
- Coercive power — we are subjected to violence, aggression, threats
- Legal power — systemic rules or sanctions limit our choices
- Economic power — we can’t afford needed goods, services, activities or opportunities on a par with others
- Interpersonal power — we can’t meet basic relational needs for intimacy, care and human protection
- Social/cultural power — limited access to knowledge, connections and qualifications that make life easier
- Ideological power — values, language and meaning are defined by powerful others
2. This feels threatening
Needing power and not having it is uncomfortable and often highly distressing. Some common feelings (“meanings”) that arise from lack of power include:
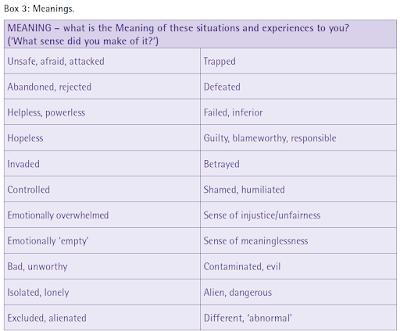
3. Survival (coping) responses get labeled “symptoms” of “mental illness”
We respond to threat in ways that seek to overcome, escape or re-balance our perceived power deficits. Our responses can affect every aspect of our lives — e.g., physical, mental, social, spiritual. Here are some examples:
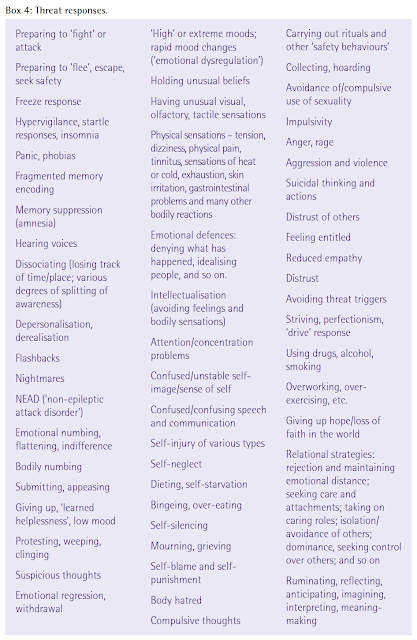
Threat responses often have appear strange to others — and sometimes even ourselves. Their meanings may be intuitive and unspoken — even to us. We may not understand or appreciate that gravity of what we are up against. This is especially true if we live in a group or culture that marginalizes our core experiences.
These concepts are critically important to get if we want to make sense of “mental illness.” In effect, it is these very threat responses — essentially our attempts to cope with overwhelming personal, social and existential odds — that are currently being diagnosed and treated as “symptoms of mental illness” by conventional healthcare.
Just as important, however, the PTM framework recognizes that power operates positively (not just negatively!). Thus, the power of personal agency and social action can be developed to create meaningful individual and societal outcomes. In other words, we can rebalance power in ourselves — for example, how we treat ourselves in the face of vulnerabilities. And, instead of blaming ourselves, we can work to rebalance power in disabling relationships, systems and social dynamics in the world we live in. This, potentially, heals all of us.














Hi Sarah, hope you’re well. Good to see you writing.
I grow a little more antsy every time I see this “Power Threat Meaning” theme being tossed about. I haven’t quite been able to put my finger on it up till now, but I think I’m starting to conceptualize and articulate my queasiness a little better. Part of it has to do with the idea that people need some kind of “program” to understand and accept (often in abstract, clinical sounding terminology) their persistent inclination to react in human ways to living under a constant state of oppression. I think if people were more keenly (and confidently) aware that their very humanity is indeed under attack every day they would not need to “search for an answer” to their misery as, after all, this system’s shit is in our faces. Understanding and supporting one another in light of our common oppression should be largely a no-brainer, not something requiring months of research, postulation and debate.
Maybe that will resonate with someone. It was triggered by seeing the mantra “Power Threat Meaning” popping up again, not a direct response to Sarah’s article, which I’ll get to later.
Report comment
Thank you for putting it so keenly into words, oldhead.
“…the idea that people need some kind of “program” to understand and accept (often in abstract, clinical sounding terminology) their persistent inclination to react in human ways to living under a constant state of oppression. I think if people were more keenly (and confidently) aware that their very humanity is indeed under attack every day they would not need to “search for an answer” to their misery…”,
Report comment
What you said resonates with me Oldhead. Our very humanity is under attack every day. I only wish that getting that and supporting each other around this actually were a ‘no-brainer.’ It may be for some people somewhere, but I haven’t found them very easy to find. Given that, I consciousness-raise. Even more, try to create spaces to talk about it, because it’s distressing to me and I need to find others (like you) who feel distressed about it too and are willing to own that.
Report comment
Two resonations, cool. 🙂 See my next couple comments.
P.S. That’s what I do too, primarily, is at least try to consciousness-raise. That’s the phase we’re in now. We’re struggling towards the development of the sort of consensus that will allow for the achievement of the critical mass needed to actually do something effective.
Report comment
Thanks Sarah great article, excellent response.
Report comment
Oldhead – The fact that you think understanding and supporting each other is a “no-brainer” and “does not require” months and years of research and inquiry (and continuous re-evaluation of how we’re doing it, and in what socioeconomic context! and what our limits, burnout points, and own needs are! and seeking competency to address cultural gaps!) is probably what’s stopping you from doing it better.
Great article Sarah.
Report comment
Are you a “mental health professional”? Because you seem to miss the point.
Report comment
Your comment to Oldhead seemed patronizing, Danny. Like him, I wonder if you’re a psycho-therapist or social worker.
Report comment
That said, I’m not as opposed to this idea as others at MIA.
Report comment
No, no sort of professional, but there but for the grace of god go I. An anarchist who understands, rather, that supporting each other competently through our struggles and organizing across difference actually requires detailed and ongoing correspondence and study. And I walk on away from circles where people (dis)content themselves with saying the same three sentences over and over.
Report comment
I think I get what you’re saying. Just because “professionalizing” helping others creates a lot of problems, it doesn’t mean it is simple or easy to know how to be a helpful person to someone in a difficult situation. It behooves us to study what is and isn’t helpful, but more importantly, it is most important to put our own houses in order so that we can really be there for those who need us. And that is NOT a no-brainer!
Report comment
supporting each other competently through our struggles and organizing across difference actually requires detailed and ongoing correspondence and study
“Competent support” is a conflicted notion in my book. When support becomes primarily a skill, “supportive” interactions start to become alienated.
Report comment
In contrast to the medical (“mental illness”) model, the Power Threat Meaning Framework (PTM) is a non-pathologizing, unifying model of human bio-psycho-social functioning.
Why do we need a “model”? Why should we care about “bio-psycho-social functioning,” isn’t that the concern of social engineers? Why do we constantly have to be watching ourselves, our feelings, our wants, and categorizing and analyzing them? The very act of doing so sends (and internalizes) a message that there’s something wrong with us. Whether people identify as “peers,” “service recipients” or “mentally ill” they set themselves apart as “special cases” that need some sort of official adjustment. Question is, who are these “officials” and why is it in our interest to adjust to their specifications? Why do people distrust themselves so much to begin with that they would even want to accommodate “society’s” demand for us to eat shit and like it?
Report comment
Interesting. I definitely felt torn about the PTM concept. On the one hand, it is awesome that the professionals involved are prepared to publicly challenge the DSM/ICD madness in a direct and public manner, and provide an alternative explanation for how/why people act in these ways. On the other hand, when I was reading the list of coping measures, I could see how easily they could become their own “labels” or “illnesses” and it still kind of felt like there is something WRONG with the people doing these things, even if they now have a reasonable and less blameful explanation for them.
It is certainly a vast improvement over “your brain is broken.” Vast improvement. And the recognition of societal power as a force creating these effects is something I have not ever seen in the world of psychology/therapy, other than some individual writers. So I see some hope here, but also a real possibility of the new framework being co-opted into just another way of creating or reinforcing superior/inferior divisions.
Report comment
If it keeps mental health professionals busy philosophizing with one another at least it keeps them out of trouble and less prone to taking their theories out on us. But I don’t think it’s that useful for people seeking some sort of emotional relief. I also hold open the possibility that this highly academic and clinical sounding document is nonetheless helping some “mh pros” make connections in the sort of language they’re familiar with, being products of their culture.
Report comment
Thanks Steve – appreciate the ambivalence and your thoughtful points on both sides.
Report comment
Oldhead, all I can say is that for me, having a model has been tremendously helpful. Because there was none that fit for me at the time, I came up with my own model for how my mind and body function. Coincidentally, the model I came up with on my own for me has a lot in common with what I think the PTM framework is trying to get across. It helps me make sense of why I do what I do, why others do what they do, and how I can respond in ways that make my life and relationships better instead of worse. That’s the utility of a model (and my model) for me. Also, it strikes me that even Buddhists and anarchists have models, which strike me as being a lot like maps. And, yes, I can throw out the model once I get to the destination I want to arrive at. But for as long as I’m still floundering in the wilderness, there’s nothing like knowing that I have a decent map of the territory to give me hope that it will possible, somehow, eventually, to find my way.
Report comment
If it helps you make connections I would never try to talk you out of them, especially if it helps you make sense of things.
I guess you could say that everyone has a conceptual “framework” for understanding life and the world, but once again this one comes from those with a vested interest in being “service providers” (this is not a put-down, just being objective). “Human services” professionals in general live in a milieu of alienated thinking which compels them to make generalized pronouncements about large groups of people. I personally would never be able to subject myself to any “program” even remotely connected to any permutation of psychiatry or the mh system, other than, conceivably, some sort of counseling outside the sphere of “health,” should I have an issue where such feedback would prove helpful.
I think if there were a serious revolutionary struggle going on in the world at large there would be a more sophisticated collective understanding of how the reduction of people to their worth in relation to the accumulation of profit makes us all crazy, each in our own way, and far less of a tendency to hold ourselves in contempt for experiencing our pain, or to internalize our outrage. When people make the connection that we feel this shit because we are being oppressed by concrete, identifiable forces we can then learn the value of defeating those forces — something the “framework” glosses over — and changing the objective situation for us all. THAT is the only thing that will ever get us finally venturing out of our individual little prison cells and collectively experiencing humanity — and life — as worthwhile and joyous.
Report comment
Oldhead, your comment made me curious about what have you found useful/helpful
Report comment
In terms of what?
Report comment
Perhaps I should have asked how do you suggest people make sense of their lives and their struggles seeing that this framework would not work for you
Report comment
What I’m saying is that there is no formula as we are each unique. We learn from our experience, or sometimes not. As for “the framework” working or not working for me personally, there’s nothing I need to resolve at the moment to which it would be relevant. I’m sort of past needing to justify my feelings and thoughts to myself, not that any of us should consider ourselves beyond self-reflection.
Report comment
Thanks Oldhead – shit happens so we feel shit- Souldn’t be so hard really should it – But what do we make of this shit and what do we do about it, if anything?
Report comment
Well, next you’re getting into analysis and then strategy…
Report comment
And next you’d say organise!
Which is where things become problematic and people start to jockey for position as activities are professionalised people may start to sabotage those activities – it may be that it’s the 90% of professionals that give the 10% a bad name. How do you get from a position where the vast majority have no problem realising the origins of distress in life itself to a profession which now increasingly has colonised our responses and insisted the answer lies totally within? And it’s not just psychiatry, psychology and therapy that does this but seems to be universal amongst elites and their neo-liberal acolytes.
Report comment
What psychiatrists think and believe should be of no consequence, just stay away from them. It’s not a matter of “good” & “bad” individuals; the entire profession is based on absurdly false premises.
Report comment
I think it was Steve Biko who said the the greatest weapon in the arms of the oppressor was the minds of the oppressed. Psychiatry/psychology operate increasingly in the interests of elites to do just this- to colonise people’s minds and suggest various propaganda to explain away the consequences of poverty, abuse, trauma, victimisation, discrimination etc. I like you would imagine it a no-brainer to oppose such re-traumatisation but folk seem to be rendered increasingly helpless to oppose such violence! But they ‘respect’ the expertise usually delivered with the veneer of kindness never questioning the true allegiance of their ‘helpers’. Maybe it is help itself that might be the problem?
Report comment
Oh and I can avoid pschiatrists/pschologists for the most part – I only wish I could say the same about them – they seem quite keen to help for some reason and are quite willing to reach out into the community to do just that nowadays. And some of them as students of the consequence of repressive forces are worth attending to. I don’t generally critic them as individuals but attacking their ideas seems to get them even more angsty.!
Report comment
People are pretty capable of mutual support once they understand what they are supporting each other with. Since the powers-that-be need to mystify the human consequences of what they do, however, we are not encouraged to see the consequences of our blatant exploitation for what it is, but as “symptoms” of processes that only experts can grasp.
Report comment
Thanks for this, Sarah. You’ve done an excellent summary of the messages of the PTM Framework. The only thing I would add is that it was developed and funded by the Division of Clinical Psychology, which is a sub-division of the British Psychological Society (the latter represents all brands of psychologists in the UK); and, importantly, it is not official DCP or BPS policy. Rather, it is one of a range of publications issued each year, most of which are discussion documents of some kind or another.
One of the advantages of having this organisational support is that the Framework can be offered as a free intellectual resource to anyone, rather than being sold as a book or paywalled in a journal. This is in keeping with our aims of breaking down professional/service user barriers and counteracting ‘epistemic injustice’ – that is, being deprived of the knowledge to make sense of your own experiences due to unequal power relations (think of almost everyone who ends up in services and is wrongly told that their diagnoses are facts.)
Unfortunately I have missed some of the sessions but I will try and join some of the others. We have been in touch by email – in due course I’d love to have some kind of feedback about how it all went, and ideas people may have had for developing/adapting the Framework further. In the meantime, because the main documents are pretty lengthy and complex, here are some easier ways in (in addition to your workshops): Interviews with authors and attenders at the launch: https://vimeo.com/264387393 Videos of the main talks at the launch: https://vimeo.com/267401691 Link to FAQs, a 2 page summary, and a suggested ‘Guided Discussion’ for reflecting on the ideas in relation to your own life or someone you are working with: https://www.bps.org.uk/news-and-policy/introducing-power-threat-meaning-framework Interview with me elsewhere on the MIA site: https://www.madinamerica.com/2018/03/dr-lucy-johnstone-power-threat-meaning-framework/ You can order your own copy of the shorter Overview document by emailing [email protected]. We welcome thoughts and feedback.
Report comment
Oldhead I really appreciate a lot of your comments here, particularity how you emphasize a need for emotional support first perhaps in a collective sense? And maybe insisting underneath it all that we all KNOW how to do this? That this is innate?
I also think professional distrust is well grounded, primarily because of the system of power it reproduces and reinforces. Yet we carry our knowledge as societies, as groups, people specialize. It does not mean that specialization has to lead to being disconnected/dissociated from the whole nor from community, compassion, complexity and lived experience, it can mean custodianship – carrying this part of our cultural knowledge for the rest, like others carry knowledge and skill useful to the whole.
I think it is complex. But I have to say I have experienced ‘disability’, at times acute as a result of the social dynamic and impact of what I survived. The mental health framework as it now stands has been both a boon and a burden for me. Pathology means a lot of doors will be closed to me, shame, outsider status, being relegated to the bottom of the socio-economic heap, but due to access advocacy and feminist healers and scholars and mad pride, I have been able to make some kind of life too. If I were born a few years earlier would never have been the case.
A lot still needs to be challenged in the way we are reproducing and producing knowledge and skills because the origin story in many Western cultures for our modern professions is of course toxic. But we need to decolonize this knowledge and we do need to use the available tools and invent new ones in order to protect people right now. None of us are outside of this.
Report comment
The first thing you have to do, is ascertain the difference betwen a physical cause and none physical cause. If a person suffers terrible migraine/anxiety because they have low Mg how is talking about other stuff going to help ? This actually happened to me many years ago,. I was put infront of a clinical psychologist who spent an hour telling me my pain was real and not imagined. Well yes, no kidding. Went on suffering for years until I had a IV of Mg and studied the role of Mg in the brain and sorted my problem out. The important point there is that the clinical psychologist was useless to my suffering.
The vile labeling, yeah that has got to be got rid of.
Talking to people who are coming off the vile neuotoxins and other drugs, yeah that has to be happen.
Compensation to people who have suffered (including the harmful labeling) /died appallingly at the hands of psychiatry, yeah that has to happen. I do not see any organisation pushing for that – shame on you all – other than the greedy lawyers. If you loose you’re even more fucked, the lawyer is not.
I agree with others who see psychologists pretty much as handmaidens to psychiatry. We need to totally get rid of psychiarty, and stop the deluded ‘doctors’ from drug/label destroying peoples lives for money .
Report comment
“I agree with others who see psychologists pretty much as handmaidens to psychiatry.”
Hah! I can’t see Lucy Johnstone as a handmaiden to anyone – least of all Psychiatry.
Report comment
I think Streetphotobeing is a fellow American.
This side of the pond psychologists are a bunch of spineless sell outs to Pharma-psychiatry. The whole thing is revolting.
They even use churches to spread psychiatric propaganda. “Jesus can’t save all of us. The ‘severely mentally ill’ need Prozac instead!”
Glad things are a little better in the UK, Auntie Psychiatry.
Report comment
Auntie Psychiatry is right in that PTMF is closely allied to ‘Down with Diagnosis’. But Steve McCrea is also right that an alternative is being smuggled in.
Going through the main document finding words such as ‘trauma’ helps identify what that is. ‘Trauma-informed’ is key even though ordinary ‘PTSD’, as a DSM no-no, is rejected. However, great stress is placed (p.201) upon ‘a new category of Complex Post-Traumatic Stress Disorder (Complex Trauma for short)’.
‘Our argument is that the great majority of the experiences that are described as ‘symptoms’ of ‘functional psychiatric disorders’ (and many other problems, including some examples of criminal behaviour) can be understood in this way, but with no assumption of ‘mental disorder’’
So, ‘Complex Trauma’ is NOT a diagnosis. Anyone who disagrees will be blocked on Twitter, as two UK psychiatrists have been by Lucy Johnstone. I don’t think other UK psychologists, never mind service users or psychiatrists, will be completely convinced.
Reality check here for US (and maybe UK) readers: PTMF is not official BPS policy, but it appears to have come across as such. From the last 2 months I estimate that 0.3% of tweets by the BPS have referred to it: from the BPS Clinical Psychology Division, 1.5%.
Report comment
Well she makes sense to me here, unlike the twerps I got:
https://www.youtube.com/watch?v=CGjSrzEAFZo
Report comment
Yes, this 5 minute video is very good, about a fictional person with a history of childhood sexual abuse and self-harm/relationship problems.
As others have said here, mental health funding has gone down in the UK, and I believe that the increasing loudness of ‘abolish diagnosis’ talk may have partly caused that.
Psychiatrists and (increasingly) psychologists are the ‘gatekeepers’ & if politicians hear such talk from them…well any reduction in taxes on the majority is welcome.
Report comment
Thank you…and I can assure you the same is true of my co-authors as well! – who are both survivors and professionals (and some with dual identities.)
Report comment
I would challenge the logic which holds nutritional deficiencies to be the “cause” of anxiety; usually it reflects some sort of fear. However poor nutrition or health can make it more difficult to process our inner conflicts and disturbing feelings/thoughts.
Report comment
Saw two psychologists both were useless, neither of them understood anything about the really important biology stuff in the brain re anxiety and how ( the precise way ) it is affected by stress and alcohol/benzos. One tried to do CBT and I ended up doing it to him for not challenging the drug use of the psychiatrists he worked with, so was discharged. I had akathisia during the last one and was very pissed off and in an extreme situation needing a solution, he prefered to talk about the technical details of the becquerel daguerreotype process. What a berk.
The power stuff is about neoliberal globalism removing all regulation and oversight thereby allowing business to over run us. The way to deal with this is not to allow ourselves to be used by either a GP or psychiatrist. It only works because people believe and have trust in them.
Report comment
Not sure how that is a response to what I said; I never suggested seeing psychologists as a solution.
Report comment
There are a lot of people who consider magnesium deficiency to be the direct underlying cause of their “anxiety” but they would certainly not consider it to be the underlying cause of all “anxiety” in all people. It makes sense to me that a deficiency in an element required for normal central nervous system functioning could cause a symptom that, for lack of a better word, people call “anxiety”. I just finished reading the full version of the power-threat-meaning framework and liked most of what I read. The part I am left grappling with, though, is how do people like streetphotobeing get the help they need when dealing with an underlying physical problem that may inappropriately get stamped with a DSM label or incorrectly considered a “power imbalance” when all he needed to feel better was to correct the underlying magnesium deficiency.
Report comment
As I keep pointing out, it’s not a “mental health industry”, it is a “mental illness industry”. The thing being sold is not “mental health”, the thing being sold is “mental health treatment”, and to receive “mental health treatment”, you need the presumption of “mental illness”, a lot of “mental illness”.
The monumental rise in numbers of so-called “mental illness” (statistics) can be tied directly to the selling (and provision) of “mental health treatment” (drugs and talk).
Posing one approach against another doesn’t really directly deal with the problem, by which I mean the mental patient role. With the PTM framework you are expecting “user/consumers” to buy whatever it is you’re selling. Liberate people from the mental patient role, and you no longer have “user/consumers” contending over what sort of fraud it is they are willing to buy (i.e. the bio-medical fraud versus the power-threat-meaning fraud).
Report comment
Has anyone ever completed a study to test the relationship between the number of people diagnosed and the number of people doing the diagnosing?
Report comment
In the UK psychiatric services have been cut but the government is stressing mental health at work and, “Parity of Esteem.” Something else is going on apart from there being psychiatrists selling stuff. There is a growing market in mindfulness teachers and aromotherapists and such like, mainly aimed at the middle class, while services are taken away from the working class. Those services are not just mental health, but also children’s centres and youth centres and women’s aid.
So I think there is something else going on. Part of it is the marketing of psyche drugs and GP’s prescribing them but also mental health being used as a distraction from the misery caused by extreme capitalism.
Report comment
There certainly are quite sinister activities ongoing. The continued increasingly successful attempts by the neo-liberal thought collective to monopolise understanding through a market understanding and monetise everything. Their aim ultimately to destroy democratic citizenship and any other type of understanding in social affairs. Even with the potentially calamitous nature of climate change humanities need to respond is being hijacked not merely by denial is but also by an insistence on market solutions, at this rate the planet may become a near totally hostile environment before they succeed!
It’s some 17 years since a group of survivors tagged our group as defenders of the ‘ consumers’ of mental health services seeming to forget their involuntary and coercive nature. I recognised a lost cause right there!
Report comment
The “consumer movement” was a deliberate strategy to confuse and neutralize the movement of anti-psychiatry survivors, and was controlled by power-hungry opportunists.
Report comment
It’s never been put so well.
It did however ( does) surprise and confuse that so many survivors (anti-psychiatry or otherwise) fail to see the problem with identifying as ‘consumers’ of ‘mental health’ or any actual health services for that matter?
We did at least manage to advocate for statutory reviews of committal but as you note these safeguards have been neutralised by the powers that be and user lead advocacy has been seen to be in collusion with those forces, sad if it weren’t so tragic.
Report comment
When people negotiate over how much abuse they’ll accept the results are predictable.
Until people realize this is not a “health” issue the confusion will continue to trip up any hope of serious resistance. And this is the intent.
Report comment
Never really thought about it that way before. But our crowd don’t even go as far as negotiating the amount of abuse people receive, they’ve seemingly been happy to be co-opted by the beauracracy with no protest, at best they might act as a valued listening ear but mostly call for more consideration of people’s maladaptive attitudes and bad choices, always impossible to ignore and the most obvious victim blaming stance. I had got involved because it seems that activism at least allows for making some common cause about injustice and history would teach that even within revolutionary change it is incremental progress that happens, nothing happens all at once and within the current clampdown the policy of the neo-liberal revolution is one of incremental regression. So for now anyway most of us at least some of the time may be negotiating how much abuse we’ll put up with as well as what benefits we demand.
But my point really concerned those who see the malevolence at work in their lives are often still heavily resistant to any concern with power. It’s easy to see when psychiatrists, psychologists, therapists, economists ignore power that that shows how they serve power but when the oppressed so to speak ignore such forces even in private, it takes some courage to stick your head above the parapet, well it’s quite odd really isn’t it?
Report comment
People are 100% entitled to their views, and I understand the suspicion about any new perspective … but I do wonder if you have read the Framework, Frank? You say: ‘With the PTM framework you are expecting “user/consumers” to buy whatever it is you’re selling. Liberate people from the mental patient role, and you no longer have “user/consumers” contending over what sort of fraud it is they are willing to buy (i.e. the bio-medical fraud versus the power-threat-meaning fraud).’ The Framework was not produced by professionals and then aimed at ‘user/consumers’ since it does not recognise such a distinction in terms of distress/extreme states/unusual experiences. The Framework was co-produced with survivors from the first meeting. It is about how we all, however we are categorised, struggle with the impact of power and with the emotional suffering arising from it. It is imperfect and incomplete but it is not as you seem to be assuming.
Ditto Oldhead’s comment: ‘When people make the connection that we feel this shit because we are being oppressed by concrete, identifiable forces we can then learn the value of defeating those forces — something the “framework” glosses over — and changing the objective situation for us all. THAT is the only thing that will ever get us finally venturing out of our individual little prison cells and collectively experiencing humanity — and life — as worthwhile and joyous.’ I totally agree. And this is what we have tried to convey – albeit imperfectly – in the Framework. If this message really isn’t coming across at all – which I find surprising – we would welcome thoughts on how to make it even more explicit.
Report comment
I think the message comes across somewhat, but some punches are being pulled in the process, in the sense that the aforementioned “power” is left unspecified and is only referred to in a general sense. This is understandable, as to go further would require a political analysis that would likely be considered beyond the purview of the “PTM” project. Don’t know if I have any recommendations off the top of my head.
Report comment
Sunday, May 20th ~2-5pm EST
Mini-Retreat
Power, Threat and the Meanings of “Mania”
What is a “mini-retreat?”
Report comment
I could say this anywhere, but this gives me another opportunity: Even though “mania” has quotation marks around it, “it” is presented here as a “thing.” As with all such matters, the meaning of any emotional state is unique to the individual, and cannot be lumped together with outwardly appearing similarities in others or considered as a “category.”
Report comment
Yes, I follow you – maybe this is what the mini-retreat is all about.
Report comment
Sounds a little too much like Kay Redfield Jamison’s nonsense.
She’s the author of a humorous novel based on an alternate history. Touched by Fire is the name of that highly imaginative work.
Report comment
Which statement reminds you of that?
Report comment
The Meanings of “Mania.” Only Jamison would leave out the quotation marks.
Report comment
I will end my day here with what I consider to be a most pertinent quote from Karl Marx:
“The philosophers have only interpreted the world, in various ways. The point, however, is to change it.”
Report comment
I don’t mean to be so pessimistic but big corporationsl have heard Marx clearly and have been busily changing the world to suit their own interests for quite some time
Some of the $250,000,000,000 from Olanzapine has gone for just such a purpose no doubt ☹️
Report comment
As Warren Buffet has stated, “there is a class war going on, and unfortunately my class is winning” (or something close). It takes two to tango; so far only one side is seriously playing, at least in the U.S.
Report comment
It would take Warren Buffet to declare victory in a one horse race in the age of TINA. I do suspect that psychiatries fundamental argument is the same failure to construct viable alternative narratives – for now it seems the neo-liberal thought collective, like bio-psychiatry, have found viable means of countering most opposition usually with considerable recourse to intellectual dishonesty.
It still surprises me however that even the radical left seem unable to get the insidious influence of not just bio-psychiatry but also highly individualist psychologies the product of bourgeois academia, self-help gurus and motivational thought which creep about the edges of disaster responses of all kinds trying to save people from the evil of feeling injustice. It is of course always worth knowing that ‘you catch more flies with honey than vinegar’, ‘we do not see the world as it is but as we are’ and ‘its better to act your way into a feeling than feel your way into an action’ etc. But the almost conscious refutation of power dynamics and indifference to life’s genuine horrors if not pleas and praise for such resilience cloud a hidden agenda of libertarian survivalism and total deference to power and wealth accumulation. ☹️
Report comment
“…in the age of TINA.”
What is TINA?
Report comment
In addition to honey liberals seem to respond to shaming, as guilt is programmed into their puritan genes, I suspect. But psychiatry for many is the “rational” substitute for religion, and is a belief system based on faith, hence not subject to serious scrutiny.
Report comment
What is TINA?
“There is no alternative” [to capitalism].
https://en.wikipedia.org/wiki/There_is_no_alternative
Report comment
Wow, puritan liberals, that must be a hard act to sustain, do tell more as I haven’t really kept up with puritan culture since The Scarlet Letter.
Report comment
I skimmed PMT and thought it obvious. Nice to see some people have laid it out clearly though.
Report comment
Sarah,
While I like the model guideline and scientific study on what works and what doesn’t, I think we’re putting the cart before the horse. Maslow’s hierarchy of needs comes to mind every time I read a theory on how to make life more bearable. Like you, I have mostly tried to stay away from this issue because it seems unsolvable at times, kind of like taking down the tobacco industry. There are a lot of jobs at stake and the MH industry has become an industry that can be also categorized as “Too big to fail”. So while I admire that some of those in the psychology field have “drawn a line in the sand”, it still doesn’t inspire me that they will change, especially in the US where Pharma is king and the second most important industry besides banking and finance.
If we were talking about maybe boycotting filling prescriptions from medical doctors until we were given the actual drug trial data, published and unpublished, that would grab my attention. I have my doubts about this effort on the psychologists. It just seems a way to side step liability. They are the gatekeepers and have to diagnose usually first to bill the insurance company.
Report comment
billing the insurance company does not apply in the UK – not yet anyway – and this initiative is a UK one.
Report comment
Thanks so much for this post, Sarah – really enjoy your passion & insights. Like you, I’ve been very impressed w/ PTM & have followed the blow-back it has received in the UK. Trying to discern patterns & create models of human responses to overwhelming stress helps us understand ourselves and others, I think. For me, PTM effectively counters the dominant medical/disease model – & offers a meaningful pathway out.
Report comment
Thanks, Wayne. If anyone is in doubt that the Framework does offer at least some challenge to the status quo, then follow the hashtag #PTMFramework on Twitter and you will see a whole series of brutal and very personal attacks, often from professionals using their own names…. so far we have been accused of being Marxists, ‘alt right’, (not sure how those two go together), Scientologists (of course!), of collectively bullying, silencing and ‘vilifying’ anyone who criticises the Framework, and/or of setting up ‘sock puppet’ accounts to do so, and/or of writing to people’s employees to silence them with false complaints; of deliberately obstructing the Division of Clinical Psychology consultation process (which was long and detailed); and worst, that the professionals in the project group have forced the survivor contributors to act as ‘trauma porn stars’ and trade their personal stories in order to ‘pay our mortgages.’ Bizarre analogies have been drawn with Mao, Stalin and Hitler (yes, seriously….) Senior professionals have described me and Mary Boyle, the lead authors, in grossly misogynist terms such as ‘queens and their courtiers’, ‘women of a certain age’ and ’empresses with no clothes’, while circulating sexist cartoons. Entire critical blogs have been written based on statements that do not actually appear in the documents. Allen Frances himself alluded to the Framework in the phrase ‘worse than mental masturbation.’ It is also, of course, ‘entirely without evidence’, ‘anti-psychiatry’, ‘anti-science’ and nothing more than a ‘polemic’ or ‘manifesto.’ Luckily the Framework gives us a handy way of analysing this …. we are clearly posing a threat to ideological power, which is a major theme in the Framework. Along with this we have also had some very welcome, relevant and constructive feedback – which is exactly what we want to receive, since we see the publications as very much as a first step in need of further development. I hope I have persuaded you that you need to read this appalling document for yourselves! See my comment to Sarah above which has links to the relevant documents and resources.
Report comment
Paul Salkovskis is one of the most respected clinical psychologists in the UK, and Irene Sutcliffe has a history of OCD, anxiety and depression. They spent time on their thoughtful but critical Blog piece, so why doesn’t Lucy Johnstone respond there: https://www.nationalelfservice.net/mental-health/power-threat-meaning-framework-innovative-and-important-ptmframework/ …?
Lucy Johnstone is misleading in her account of the Blog piece which contained the phrases ‘trauma porn star’ and ‘pay our mortgages’. The ‘first edition’ was arguably ambiguous and both were removed in the second edition, which did however clarify that ‘TPS’ described the experience of a survivor. Neither referred to the PTMF, but subsequent Twitter comments and attempts by Lucy Johnstone to suppress some of them suggested that some service users/survivors did make that connection: http://asylummagazine.org/2018/05/welcome-to-the-cmht-by-ria-dylan-and-pippi-elliot-designed-by-rachel-rowan-olive/
As for the ‘misogynist’ comments & cartoons by ‘Senior Professionals’, I haven’t seen those so could a link(s) be provided?
Report comment
Thanks for the link to Asylum, what a brilliant publication, great satire, you do realise it’s satire don”t you?
And!Lucy the pushback proves the PTM framework has hit a nerve somewhere keep at it the evidence is on our side.
Report comment
I don’t see pushback or intense opposition so much as suspicion as to the intent and potential ramifications of the document.
Report comment
Why do you list “anti-psychiatry” along with other things you clearly consider specious?
Report comment
Dear Sarah,
Thank you for this well prepared Article.
I’m very happy, anyway, that the British Psychological Society has stepped forward to challenge the “Medical Model”. Because, I know myself that the solutions are through the non drug approach and I can Substantiate this:-
When I withdrew from *Neuroleptics (which I had initially declined) my anxiety was such that it nearly drove me Mad. But I was able to find Psychological Approachs that worked to keep me sane and off the drugs.
In the following 30 + years I had to deal some Real Life Nightmares, and when I did I used the same Psychological Approachs (and these brought me through my Crises).
I would maintain that Psychiatric drugs are more likely to create “Severe Mental Illness” than Life Experience. I think the “figures” speak for themselves.
*Between 1980 and 1984 in Southern Ireland I was a “Chronically Disabled Psychiatric Patient” in receipt of Disability Payment, in and out of hospital; and with all the Severe Mental Illness Diagnosis.
I made Recovery in 1984 as a result of carefully coming off “medication” with the help of “Psychotherapy” ; and I came off the Disability Payments as well (Permanently).
Report comment
Whenever even the thought of social workers or therapists comes to mind I get a picture in my mind of those motherless baby monkeys in some cage in a zoo clinging to a woven wire monkey shaped construction that’s supposed to be their surrogate mother . At least the wire mom’s can’t refer the baby monkey to a psychiatrist.
Report comment
Dear Sarah,
Thank you so much for this. Finding this today has literally given me a new lease on life.
I think it’s absolutely vital to develop structures for explaining the way acute distress is centered in oppression in and for the framework of mental health. It is important for us to understand that the very institutions and professions dealing with mental health historically and to this day are patriarchal, colonial, racist, ableist. Were by and large instruments of control and oppression in themselves and this legacy and actuality lives on. For many of our modern institutions and professions this is the case. Any evidence within the institution/framework/field of mental health to the contrary is a result of resistance and intense creativity, of challenging the paradigm through concerted struggle arising from the feminist movement, from the movement for democracy, from the civil rights movement, anti-capitalist movements (which for those not in the know, are not necessarily anti-market movements just movements against gross exploitation) and most importantly ‘user’ led, deeply compassionate resistance, innovations and reforms. This resistance is important, because we cannot escape the system, we need to appropriate it, critique it and reform it to build the support we need. Many of us need that right now in order to survive, and gain any form of agency, so the Power Threat Meaning Framework is a life raft in my opinion.
I am sick of being ‘othered’ due to my distress. It is no longer enough for me to find solace in survivors groups. I want to take part in my profession of choice and be fully human like everyone else, not the defective model. I can’t wait until I am ‘fixed’. This gives me so much hope. And a way forward with my ‘peers’ who by and large have not been ‘pathologized.’
Report comment
A powerful article, Sarah, of not just by content but poetry.
But no one mentions the genocide–half a million people per year die of psychiatric drugs. That’s 5 million over a ten year period. Period. G-E-N-O-C-I-D-E
“Professionalism is the bane of society.” –George Bernard Shaw
Mostly people just want to live and let live.
What’s wrong with just listening to someone with problems–no advice, no judging, no explanations.
I suggest you all attend a national Rainbow Gathering, an anarchistic celebration of peace and love in the cathedral of nature, to see how problems are dealt with. What happened to the caring and sharing at the Woodstock Festival, where all treated one another as brothers and sisters without exception? Or was that because they all self-medicated?
Report comment