
Introduction
On Wednesday, July 6, the US House of Representatives passed a watered-down version of HB 2646, the so-called Helping Families in Mental Health Crisis Act. The bill, which is now a House Resolution, is usually referred to as the Tim Murphy bill, after its principle author, Representative Tim Murphy, PhD, who is also a clinical psychologist.
The bill passed the house with a noteworthy tally of 422-2, with nine abstentions.
On July 6, the Wall Street Journal published a helpful summary of the issues: House Passes Mental Health Bill, authored by Louise Radnofsky. Here are some quotes, interspersed with my comments:
“The bill passed 422-2, overwhelming support that reflected a decision by sponsors to defer debates on some of its most controversial aspects. The bill would reorganize the federal agency overseeing mental health policy, direct funding to combat serious mental illness as opposed to general mental health programs, and change Medicaid reimbursements for treating patients with illnesses like schizophrenia.”
“…as opposed to general mental health programs…” is a reference to the federal Substance Abuse and Mental Health Services Administration (SAMHSA), which the eminent psychiatrist, Jeffrey Lieberman, MD, has described as “a proxy agency for the anti-psychiatry movement…” (here). But here’s what Oryx Cohen wrote about the Murphy Bill and SAMHSA on November 6, 2015:
“The Murphy Bill threatens the recovery and community integration practices that current consumers of mental health services and survivors of coercive psychiatric interventions have worked so hard for over the last 40-plus years to create for those most in need. In particular, the bill would dismantle the federal Substance Abuse and Mental Health Administration (SAMHSA), which actively funds and supports important efforts to rebuild the community and family life of people dealing with mental health issues through non-medicalized institutions such as peer-run respites (short-term crisis centers managed by people living with mental health concerns and available to “self-referred” individuals seeking to avoid hospitalization through support from peers). SAMHSA also supports suicide prevention initiatives, trauma-informed practices, Emotional CPR (an educational program aimed at teaching people how to assist others through an emotional crisis), Wellness Recovery Action Planning and much more, all of which would suffer if SAMHSA were dismantled.”
And another quote from the same article:
“If the Murphy Bill is passed, psychiatric hospitals and pharmaceutical companies will reap huge financial benefits as a result of increased hospitalization and forced treatment. One way the bill will do this is by creating a financial incentive for states that implement ‘assisted outpatient treatment’: court-ordered treatment (including medication) for people whom a judge deems as living with ‘severe mental illness’ and unlikely to willingly take prescribed psychiatric medications.”
Oryx Cohen is a member of the National Coalition for Mental Health Recovery.
. . . . .
Back to the WSJ article:
“The bill’s main author, Rep. Tim Murphy (R., Pa.) has for the past few years been blunt in his assessment of mental health care in the U.S., painting a picture of federal incompetence that diverted money to frivolous and unproven programs for general mental health. He said current practices impede treatment for serious mental illness by emphasizing patients’ civil liberties ahead of their treatment.”
“Mr. Murphy, a clinical psychologist, was tapped by House leaders to investigate mental health treatment in the U.S. in the wake of the Sandy Hook shooting in 2012. He and other advocates of changing the system have cited the obstacles family members faced in caring for people with serious mental illness, including privacy laws and provider shortages.”
This theme, that the proximate cause of the mass killings is the “mental illness” of the murderers, has become a staple response from psychiatry to the charge that psychiatric drugs, particularly SSRI’s, are the primary precipitators of these incidents. In the Sandy Hook murders, for instance, there were reports that the killer, Adam Lanza, had been receiving psychiatric “treatment” and had been taking psychiatric pills. But the authorities refused to divulge the nature of the pills for fear that it would “… cause a lot of people to stop taking their medications.”
. . . . .
Back to the WSJ article:
“Earlier iterations [of the bill] sought to change the privacy rules in the Health Insurance Portability and Accountability Act so that providers could share details of a patient’s diagnosis, prescriptions and appointments with a known caregiver. The earlier version would have also required states to pass laws compelling treatment for certain people as a condition of federal funding and restrict advocacy groups that receive federal health funding from helping patients bring legal challenges to their treatment.”
The bill’s sponsors have not given up on these matters, but as mentioned in the first WSJ quote above, have simply deferred them for later consideration.
The confidentiality issue is important, because client privacy has traditionally been one of the cornerstones of the mental health system. The proposal to legitimize divulging sensitive information to a person’s family would essentially reduce the individual’s legal status to that of a child. This is particularly critical, in that many of the individuals who would be affected by such legislation are in conflict with their families, and emphatically don’t want their confidentiality breached in this way.
Note also the proposed use of the federal purse-strings to increase the amount of forced “treatment”, and make it more difficult for “patients” to sue their psychiatrists. Why shouldn’t an advocate help clients bring legal challenges to their “treatment”, if the “treatment” has been unhelpful and damaging? Isn’t that what we’d expect an advocate to do? Whose interests are being served by restricting an advocate’s activities in this way? Certainly not the clients! Psychiatry is extraordinarily resistant to criticism of any kind.
. . . . .
Back to the WSJ article:
“Many of Mr. Murphy’s dropped measures had drawn opposition from patient advocates such as the Bazelon Center for Mental Health Law, an organization that focuses on protecting the human rights of people with mental disabilities. The center had said that it was alarmed by the attempts to reduce the privacy and civil rights of people with mental illness, as well as a shift toward compelled treatment, which the center doesn’t believe has been proven to be effective.”
The National Coalition for Mental Health Recovery has also come out against the bill.
. . . . .
Back to the WSJ:
“The prospects for mental health legislation in the Senate are uncertain, given the compressed calendar in an election year and the fact that sponsors there have their own ideas for changes, including Bill Cassidy (R., La.) and Chris Murphy (D., Conn.) In a statement, the two senators pointed to the House’s overwhelming vote as ‘proof that there is broad, bipartisan support for fixing our broken mental health system.'”
Note the phrase “broken mental health system.” This is actually an accurate description, in that the system is based on the spurious premise that all significant problems of thinking, feeling, and behaving are illnesses, and in practice, is destructive, disempowering, and stigmatizing. But this is not what psychiatry proponents mean by the phrase. Routinely in pro-psychiatry circles, the phrase is used to legitimize calls for more psychiatric “treatment”; more coercion; “early intervention” and routine integration of psychiatry’s spurious concepts and practices into schools, foster homes, nursing homes, group homes, GP’s offices, the armed services, prisons, juvenile detention centers, and, indeed, any setting where pills can be peddled.
Psychiatry Capitalizing on the Fear of Violence
The notion that the public needs to be protected from “mentally ill” people is not new, but has enjoyed a marked revival after decades of decline. Much of this revival can, in my view, be laid at the feet of the Treatment Advocacy Center (TAC).
D.J. Jaffe, a marketing executive, a founding member of TAC, and a former NAMI board member, gave an address to the Staten Island AMI in December 1994. The speech was titled “How to reduce both violence and stigma”, and was written up in the Staten Island AMI newsletter, December 1994. Here are some quotes:
“And recently adopted policies and laws won’t allow these individuals to be treated involuntarily until they become a ‘danger to self or others.'”
“We have to ‘head ’em off at the pass’. Treat individuals with NBD [neurobiological disorders] before they become a ‘danger to self or others'”
Earlier in the address Mr. Jaffe had explained that he was using the term “NBD” as essentially synonymous with “mental illness.”
The critical point in this quote is that Mr. Jaffe is proposing that the laws be changed, so that individuals who have been given certain psychiatric labels can be committed to enforced “treatment” before there is any actual danger to self or others. And he is absolutely clear that an individual’s refusal to take psychiatric drugs would be considered a valid reason to enforce “treatment”.
“For example, some individuals who become psychotic refuse treatment because they believe the medicines are poisons being administered by the CIA. A ‘need for treatment’ standard would allow someone else to be assigned the right to decide on treatment for this individual until he/she regains the ability to reason. The decision to administer medicines could be made before the individual becomes a danger to self or others, thus averting needless violence and another stigmatizing headline.”
Note the example Mr. Jaffe gives as to why a person might refuse psychiatric drugs: that the drugs are being poisoned by the CIA. But in fact most people who refuse psychiatric drugs do so for perfectly valid and rational reasons: that they cause irreparable brain damage (e.g. tardive dyskinesia) and they produce extremely unpleasant effects (e.g. akathisia). In 1974, forty-two years ago, Theodore Van Putten, MD, published Why Do Schizophrenic Patients Refuse to Take Theirs Drugs? Here’s a quote:
“The reluctance to take antipsychotic medication was significantly associated with extrapyramidal symptoms—most notably a subtle akathisia.”
Mr. Jaffe outlines four proposals to promote the above agenda and then he adds:
“In addition, from a marketing perspective, it may be necessary to capitalize on the fear of violence to get the law passed.” [Bold face added]
In other words, it may be necessary to deceptively exploit isolated incidents of violence to secure the legal authority to forcibly drug many people who had never exhibited any violence, on the sole grounds that they were refusing to take neurotoxic drugs that have devastating adverse effects, including irreversible brain damage.
Mr. Jaffe continued this theme in an address he gave five years later at the 1999 NAMI Conference. Here are some quotes:
“Laws change for a single reason, in reaction to highly publicized incidents of violence. People care about public safety. I am not saying it is right, I am saying this is the reality.”
“So, if you take nothing else away from what I’m saying, it’s gonna change in reaction to violence, and you gotta make this a public safety issue, and indeed it is a public safety issue.”
“We can talk to these people from their perspective, and then what we can say to them as family members, is, and this is also good for the individual. It’s gonna prevent them from becoming homeless, psychotic, suicidal, uh, incarcerated. We have found extraordinary…and I’m gonna show a poster in a minute…we have found extraordinary help, and again I gotta give credit to the Treatment Advocacy Center here, uh, of reaching out when there is an instance of violence.”
“We immediately call both the perpetrator and the victim. And we say to them, ‘We understand what happened here when your sister was pushed in the subway by Andrew Goldstein. It happened because he wasn’t getting treatment.”
“Uh, the family of Webdale, you may know Kendra Webdale was pushed in the subway, lost her life. Somebody with untreated schizophrenia. Edgar Rivera was pushed in the subway. He only lost his legs. But, uh…and he’s been a strong supporter. And what happens is, the media goes and interviews these people, and because we’ve been to ’em first, they are telling our story.”
In other words, manipulate the media to inject into their reports of isolated violent incidents, the notion that people who haven’t been violent, and may never be violent, need to be forcibly drugged – just in case! Elsewhere, Mr. Jaffe openly acknowledges that the majority of “mentally ill” people are not violent. But he has no hesitation in infringing their rights to self-determination if they stop taking their neurotoxic pills, just in case. In the criminal justice system this would be the equivalent of guilty unless proven innocent. In fact, it would be worse than that. It would be guilty, with no way to prove one’s innocence.
“Now what I’m gonna do is I’m just gonna show you very quickly, uh, the story of Kendra’s law in the media. As I’ve said, change happens as a result of acts of violence. And what, and so, when these acts of violence occur, the media goes out and writes stories about them, and then we start approaching the media. We have in New York…it’s called Kendra’s Law…it’s a law we’re trying to pass. It’s an outpatient treatment law…assisted outpatient treatment. What a brilliant phrase. It’s not involuntary commitment, it’s assisted outpatient treatment. That was…came out of the Treatment Advocacy Center.”
What a “brilliant phrase”! Almost as brilliant as “Helping Families in Mental Health Crisis”.
Back to the Tim Murphy Bill
In a House Energy and Commerce Committee press release (July 6, 2016), Fred Upton, committee chair, is quoted:
“We continue to hear tales of great loss where intervention was lacking or nonexistent.”
One can readily detect the manipulatively deceptive tones of D.J. Jaffe cited earlier. Representative Upton made no mention of the many tales of great loss where psychiatric intervention and drugging had been present. For instance:
Prior to about 1960, the status of people who were confined to mental “hospitals” for extended periods could accurately be described as pre-civil-rights. Gradually, as the adverse effects of institutionalization and psychiatric “care” began to be exposed, their legal status improved. The Murphy bill is, I believe, the first concerted attempt to roll back these protections.
Civil Rights
Interestingly, Congressman Murphy was asked about this matter by CNN’s Jake Tapper in an interview on January 27, 2014.
The question came at 1:25 into the interview.
Jake Tapper:
“There was a period in the country when the civil rights and civil liberties of people with emotional and mental problems, and we obviously don’t want to stigmatize these people, however much even talking about it might do that. But when those civil liberties became very, very important, and they had more rights, they were bestowed more rights. Did we go too far as a society? Did we not take into account society’s needs beyond the individual’s needs?”
This question could have produced a fruitful discussion on civil rights, but watch how Congressman Murphy neatly sidesteps the issue.
“I think we swapped the hospital bed for a jail bed, quite frankly. Somewhere between forty and fifty percent of people in our county jails, our state prisons, our federal prisons, are mentally ill. That is the ultimate removing of their rights. It is…we segregate them there, we end up not treating them there. And the same thing goes where we’ve tripled the homeless rate. This is not the way we should be doing it. We’re acting like a third world country quite frankly. It is embarrassing, it is immoral, it is unethical what we have done, and so you have as one person so eloquently said, they end up dying with their rights on, because we say you have to consent to treatment. But how do you get somebody to consent to treatment if they don’t even understand reality. They can’t sign a contract, they can’t do anything else. And what we need are other options. Not just the option of you have to be adjudicated to say you must stay in a hospital, but also an outpatient treatment option like you just described the case where the guy stabbed his mom. He could have been taking medication, he could have been doing much better. And many of these other assaults that have taken place – Aurora, Colorado or Arizona, etc., the person later on realizes gee, if I was in treatment I wouldn’t have done this because I would not have heard those voices commanding me.”
In other words, the bill doesn’t really infringe on people’s rights, rather it protects their rights! So we will forcibly inject large numbers of people with neurotoxic poisons to guard against the possibility that a few of them might otherwise end up in jail or prison.
The assertion that forty to fifty percent of the incarcerated population are mentally ill is routinely trotted out by psychiatrists and their adherents in these kinds of debates. But in fact this is an artifact of psychiatry’s spurious medicalization of virtually every significant problem, including criminal behavior. According to psychiatry’s DSM, threatening or intimidating others, using weapons, being cruel to people and animals, stealing, robbing, raping, burglarizing, shoplifting etc., constitute a mental illness called conduct disorder (DSM-5, p 469). Not surprisingly, a great number of these people end up in prison. And let us be clear, psychiatry’s contention here is not that people with other “mental illnesses” commit these crimes, but rather that the commission of these crimes, in and of itself, constitutes a “mental illness”. So of course forty or fifty percent of the incarcerated population has a “mental illness”. For psychiatrists, virtually all criminality is “mental illness.”
But even if we set that consideration aside, there is in fact no shortage of psychiatric “treatment” in prisons. Here’s a quote from the Federal Bureau of Prisons Mental Health page:
“The Bureau provides a full range of mental health treatment through staff psychologists and psychiatrists. The Bureau also provides forensic services to the courts, including a range of evaluative mental health studies outlined in Federal statutes.” [Emphasis added]
“Psychologists are available for formal counseling and treatment on an individual or group basis. In addition, staff in an inmate’s housing unit are available for informal counseling. Services available through the institution are enhanced by contract services from the community.”
And here’s a quote from California’s Department of Corrections Mental Health Program website:
“Referrals to Mental Health”
Any inmate can be referred for mental health services at any time. Inmates who are not identified at Reception or upon arrival at an institution as needing mental health services, may develop such needs later. Any staff members that have concerns about an inmate’s mental stability are encouraged to refer that inmate for evaluation by a qualified mental health clinician (psychiatrist, psychologist, or clinical social worker). [Emphasis added] Under certain circumstances, referral to mental health may be mandatory. A referral to mental health should be made whenever:
- An inmate demonstrates possible symptoms of mental illness or a worsening of symptoms.
- Upon return from court when an inmate has received bad news such as a new sentence that may extend their time.
- An inmate has been identified as a possible victim per the Prison Rape Elimination Act.
- An inmate demonstrates sexually inappropriate behavior as per the Exhibitionism policy.
- An inmate who is written up for a disciplinary infraction was demonstrating bizarre, unusual, or uncharacteristic behavior when committing the infraction.
- An inmate placed into Administrative Segregation indicates suicidal potential on the prescreening, or rates positive on the mental health screening, or gives staff any reason to be concerned about the inmate’s mental stability, such as displaying excessive anxiety.
- Upon arrival to an institution when the inmate indicates prior mental health treatment and medications, especially if not previously documented.
Referrals to mental health may be made on an Emergent, Urgent, or Routine Basis. An inmate deemed to require an Emergent (immediate) referral shall be maintained under continuous staff observation until evaluated by a licensed mental health clinician. An Urgent referral is to be seen within 24 hours. A Routine referral should be seen within five working days.
Referrals are made on the CDCR-MH5, Mental Health Referral Chrono, and forwarded to the mental health office. Emergent and Urgent referrals should also be made by phone to facilitate a timely response. The referral chronos, when received at the mental health office, are logged, entered into the data tracking system, and scheduled for follow-up with the appropriate clinician.
Inmates may also self-refer for a clinical interview to discuss their mental health needs. Inmate self-referrals shall be collected daily from each housing unit, and processed the same way as staff referrals.”
Similar programs and procedures are in place in prisons in other states, and in other countries.
. . . . .
On to the Senate
The article in the Wall Street Journal states:
“The prospects for mental health legislation in the Senate are uncertain, given the compressed calendar in an election year and the fact that sponsors there have their own ideas for changes…”
But the various vested interests are already lobbying hard. Here’s the text of a letter sent to the Honorable Mitch McConnell, Senate Majority Leader, and the Honorable Harry Reid, Minority Leader, by the APA and other groups on July 13, 2016:
“Dear Majority Leader McConnell and Minority Leader Reid:
On behalf of the undersigned organizations, we are writing to urge you to bring S. 2680, the Mental Health Reform Act of 2016, to the Senate floor for a vote as quickly as possible. Last week, the House of Representatives voted overwhelmingly to pass H.R. 2646, the Helping Families in Mental Health Crisis Act. It is now the Senate’s turn to act.
Mental illness is widely prevalent in the United States. Over 68 million Americans have experienced mental illness in the past year which is more than 20 percent of the total population of the United States. Lifetime rates are much higher with some estimates approaching 50 percent. More striking, in 2013, over 41,000 Americans died by suicide. Many individuals with mental illness or substance use conditions are unable to access or receive the appropriate services and supports for these illnesses, and they remain constantly challenged by mental health service delivery systems that are largely fragmented and uncoordinated across the country.
The Senate Health, Education, Labor, and Pensions Committee voted unanimously to advance S. 2680 in April. Notably, this bipartisan bill strengthens federal coordination of mental health resources, increases reporting on mental health parity, advances integrated service delivery, supports the mental health workforce, and increases early access to mental health services.
We now need your leadership to pass mental health reform and bring millions of Americans and their families help and hope.
Thank you for your consideration. We stand ready to work with you to ensure this critical first step in mental health reform can be sent to the President’s desk for signature this year.
Sincerely,
American Psychiatric Association
American Academy of Child and Adolescent Psychiatry
American Association on Health and Disability
American Congress of Obstetricians and Gynecologists
American Foundation for Suicide Prevention
American Nurses Association
American Orthopsychiatric Association
American Psychological Association
Anxiety and Depression Association of America
Association for Ambulatory Behavioral Healthcare
Children and Adults with Attention-Deficit Hyperactivity Disorder (CHADD)
Clinical Social Work Guild 49
Corporation for Supportive Housing
Depression and Bipolar Support Alliance
Eating Disorders Coalition
The Jewish Federations of North America
Mental Health America
National Alliance on Mental Illness
The National Association for Rural Mental Health
The National Association of County Behavioral Health and Developmental Disability Directors
National Association of Psychiatric Health Systems
National Association of Social Workers
National Association of State Directors of Special Education
National Council for Behavioral Health
National Health Care for the Homeless Council
National League for Nursing
National Register of Health Service Psychologists
NHMH – No Health without Mental Health
Sandy Hook Promise
The Trevor Project”
Note that the first signatory is the American Psychiatric Association.
It is sad that the list includes the National Association of Social Workers, who are squandering a rare opportunity to get on the right side of this debate and sever the shackles that bind them to the psychiatric hoax.
Note also the number of self-serving clichés that the APA have managed to work into this letter:
- Wide prevalence of “mental illness”: 20% annually and 50% lifetime, but no mention of the fact that this includes every significant problem of thinking, feeling, and/or behaving, including childhood temper tantrums, habitual disobedience, habitual delinquency, shyness, adult temper tantrums, road rage, etc.
- “… over 41,000 Americans died by suicide”, but no mention of the fact that in 2010, 23.8% of suicide decedents tested positive for antidepressants post-mortem. (CDC Suicide: Facts at a Glance) Nor is there any mention of the fact that the rate of antidepressant use in the US is increasing in step with the suicide rate. The latter has been climbing steadily since 2000. Here are the figures/100,000:

[Source: CDC]
So the national suicide rate increased by 25% between 2000 and 2014. Note also that the curve is steepening. The increase from 2000 to 2005 was 4.8%, but from 2010 to 2014 it was 7.4%.
The CDC also reports that between the period 1994-2002 and 2005-2008, the rate of antidepressant use in the United States among all ages increased from 6.4% to 8.9% (a 39% increase).
Of course the fact that the increase in suicide rate coincided with the increase in antidepressant use doesn’t prove that the latter caused the former. Many factors impact suicide rates. But it certainly suggests that the matter warrants investigation. Yet psychiatry, the primary promoters of the drugs, have persistently failed to take on this responsibility. Brian at AntiDepAware has been single-handedly gathering information on this matter for years. The sheer number of incidents he has logged is persuasive and compelling.
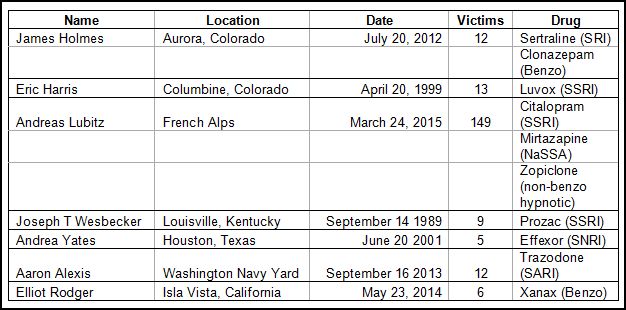
In addition, there have been numerous first-hand accounts of this phenomenon, including an article by Katinka Blackford Newman published on August 15 in the UK’s Independent. Here’s a quote:
“On 13 March 2016, French investigators released a report on the case of Andreas Lubitz, the German wings pilot who locked himself into the cockpit of a plane and crashed the plane carrying 150 people into the Alps. When I opened it I felt sick; just nine days before the accident, he was put on exactly the same antidepressant medication that I had been on when I became psychotic and nearly killed my kids. It was clearly stated in the toxicology report – citalopram, mirtazapine and zopiclone sleeping tablets.”
Ms. Newman’s article is detailed and graphic. Please take a look and pass it on.
Jeffrey Lieberman, MD, Supports the Bill
On June 16, 2015, the very eminent psychiatrist Jeffrey Lieberman, MD, presented testimony to the House Energy and Commerce Committee regarding the Tim Murphy bill. Here are some quotes from his address:
“Our failure to take mental health care as an urgent public health need and national priority, has adversely affected our country in many ways, but there are several consequences which represent the tip of the iceberg of when it comes to our neglect of mental health care that are particularly disturbing. These begin with the seemingly recurrent incidents of mass violence in which the perpetrators are persons with untreated mental illness, and the shocking rates of suicide and PTSD in our military, but also includes domestic violence perpetrators and victims, the displaced mental patients who comprise 30% to 40% of the homeless and the growing rate of mentally ill prisoners. All of these would be limited or prevented by an effective mental health care system.”
Again, note the shameless regurgitation of the D. J. Jaffe marketing argument. If you’re a Dr. Lieberman fan, as I am, do take a look at his full statement to the committee. It’s classic Dr. Lieberman stuff, including:
. . . . .
“Stigma of mental illness is pervasive in American society and is actively perpetuated by a virulent Anti-Psychiatry Movement. Psychiatry has the dubious distinction of being the only medical specialty with a movement dedicated to its eradication.”
Of course there are very good reasons why psychiatry has this “dubious distinction”. I’ve listed and discussed these in an earlier post.
. . . . . . . . . . . . . . . .
“In fact I would go so far as to consider SAMHSA a proxy agency for the anti-psychiatry movement, which is to say that the agency has resisted the scientifically driven evidenced based approach to mental health care that psychiatric medicine has embraced since its scientific revolution began in the 1970’s.”
This is the “scientific revolution” that was based on the blatantly deceptive - and now widely debunked – premise that virtually every significant problem of thinking, feeling or behaving is caused by a chemical imbalance in the brain; a chemical imbalance which is correctible by taking psychiatric drugs, often for life. So if that’s the revolution that SAMHSA is resisting, I’d say: good for SAMHSA!
. . . . .
“So many painful and dispiriting elements and incidents in our society would be ameliorated by the advent of a comprehensive effective public mental health system and have a dramatically uplifting effect on public morale and quality of life.”
A dramatically uplifting effect on public morale and quality of life! Is there just a hint of grandiosity here?
The prescribing of antidepressants and neuroleptic drugs has been increasing markedly in recent years. We have even reached a point in the US where detectable levels of antidepressants are being found in the drinking water in many areas. If these trends continue, perhaps “public morale” and “quality of life” will be off the charts. Perhaps we’ll all be dancing joyously in the streets, and rival gangs will be holding choral concerts in the spill of the streetlights. Oh Happy Day!
. . . . .
“Let me state at the outset that by mental illness I am referring to what are traditionally considered mental illnesses (e.g. schizophrenia, bipolar disorder, depression), addiction (e.g. substance use disorders) and intellectual disabilities (e.g. autism, Fragile X syndrome). The distinctions between these are arbitrary as they all are conditions affecting the same real estate in the brain and manifest by disturbances in common mental functions.”
So, the distinctions between the psychiatric labels schizophrenia, bipolar disorder, depression, addiction, autism, fragile X syndrome, etc., are arbitrary! I’m not sure what point Dr. Lieberman is making here. My Random House Webster’s College Dictionary (1992) defines “arbitrary” as:
“1. subject to individual will or judgment without restriction; contingent solely upon one’s discretion; an arbitrary decision. 2. decided by a judge or arbiter rather than by a law or statute. 3. having unlimited power; uncontrolled or unrestricted by law; despotic; an arbitrary government. 4. Capricious; unreasonable; unsupported; an arbitrary demand for payment. 5. Math undetermined; not assigned a specific value: an arbitrary constant“
So the distinction, for instance, between “schizophrenia” and “depression” is subject to individual (presumably a psychiatrist’s) will or judgment without restriction. This sounds like there’s no essential distinction between these so-called illnesses. Perhaps Dr. Lieberman is coming over to the anti-psychiatry side. I’ve always said he was our greatest ally. Or perhaps he just got a little confused in his choice of words. Maybe he’s tired. Laboring assiduously against “a virulent Anti-Psychiatry Movement” must take a dreadful toll.
A Dissenting Psychiatrist
Dinah Miller, MD, a psychiatrist/instructor at Johns Hopkins, pointed out on February 4, 2015, that the APA endorsed an earlier version of the bill before the full text had been published! Here’s a quote from Dr. Miller’s post:
“Still, I heard the news and was terribly disappointed in the APA. The decision to support this sweeping legislation was made without a vote by the Assembly, with the knowledge that some of these issues are quite polarizing. In addition to the HIPAA disqualification, the issue of outpatient civil commitment, in particular, is controversial. Although proponents are quick to point to research that show its benefits – the research has been done specifically on Kendra’s Law in New York, where $125 million was placed into that state’s mental health system to shore up services – we don’t have the research to know if what helps is providing more services or strong-armed coercion. The text of the bill will be released in the coming weeks. At the very least, couldn’t the APA have waited to see exactly what it is we endorsed?”
The Link Between Psychiatric Drugs and Murder/Suicide
There is an abundance of anecdotal information linking psychiatric drugs (especially neuroleptics and antidepressants) to violence, including murder, and suicide. There are also several formal papers, most by psychiatrists, going back to at least 1978, which confirm these reports. For instance:
Neuroleptics: Violence as a Manifestation of Akathisia, W Keckich, MD, Journal of the American Medical Association, 1978
Suicide Associated with Akathisia and Depot Fluphenazine Treatment, K Shear, MD, A Frances, MD, P Weiden, MD, Journal of Clinical Psychopharmacology, 1983
Homicide and Suicide Associated with Akathisia and Haloperidol, JL Schulte, MD, American Journal of Forensic Psychiatry, 1985
Behavioral toxicity of antipsychotic drugs, T Van Putten, MD, SR Marder, MD, Journal of Clinical Psychiatry, 1987
Fluoxetine, Akathisia, and Suicidality: Is There a Causal Connection?, W Wirshing, MD, T. Van Putten, MD, J Rosenberg, MD, et al, Archives of General Psychiatry, 1992
Akathisia, suicidality, and fluoxetine, MS Hamilton, MD, LA Opler, MD, Journal of Clinical Psychiatry, 1992
Akathisia as Violence, I Galynker, MD, D Nazarian, MD, Journal of Clinical Psychiatry, 1997
Causality and collateral estoppel: process and content of recent SSRI litigation, PD Whitehead, MD, Journal of the American Academy of Psychiatry and the Law, 2003
Antidepressant-induced akathisia-related homicides associated with diminishing mutations in metabolizing genes of the CYP450 family. Y Lucire, MD, C Crotty, MD, Pharmacogenomics and Personalized Medicine, 2011
The relevance of cytochrome P450 polymorphism in forensic medicine and akathisia-related violence and suicide, SJ Eikelenboom-Schieveld, Y Lucire, MD, JC Fogleman, PhD, Journal of Forensic Legal Medicine, 2016
Antidepressant use and violent crimes among young people: a longitudinal examination of the Finnish 1987 birth cohort., E. Hemminki, MD, M Merikukka, PhD, M Gissler, PhD, et al, Journal of Epidemiology Community Health, 2016
Brilliant Phrases
Congressman Murphy is as attuned to the power of catchy slogans as D.J. Jaffe. Here are some “brilliant phrases” that Dr. Murphy has used in an article and in speeches promoting his bill:
Mental illness is a medical emergency
Treatment before tragedy Minute 9:02
Delayed treatment is denied treatment Minute 1:22
Where there is no help, there is no hope Minute 1:26
Little has been done to get those who need help the help they need Minute 0:22
And Incidentally
Here’s some information on the sources of Tim Murphy’s campaign finances for the past four election cycles:
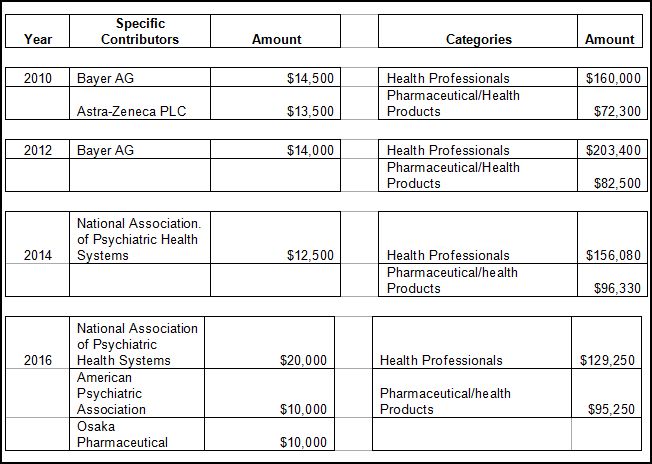
[The source of the financial information listed above is Open Secrets.org, a “nonpartisan guide to money’s influence on US elections and public policy.”]
To put these numbers in perspective, Rep. Murphy’s total campaign expenditures, again, according to Open Secrets, for the years in question were:
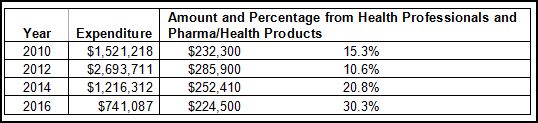
So the contributions detailed above represent a sizable portion of Rep. Murphy’s campaign expenditures.
Deceptions and Slogans
And so, my dear and patient readers, there it is: D.J. Jaffe’s tawdry marketing tactics and slogans from the 90’s, adopted today by an ambitious, pharma-psychiatry funded politician, and shamelessly embraced by organized psychiatry.
There are truly no depths of venality and deception to which psychiatry will not stoop to draw attention away from the link between psychiatric drugs and murder/suicide.
And to save their so-called profession, they are even willing to pass the blame for the murder-suicides onto their own clients, for whom they profess such care and concern.
Organized psychiatry, committed irrevocably and wholeheartedly to drug pushing and to their corrupt and corrupting relationship with pharma, simply will not countenance the fact that their primary product is fundamentally flawed and destructive. So they hire a PR company; they fund and lobby politicians; they parrot slogans; and they encourage one another to ever-increasing heights of self-congratulation. But they will not commission a definitive study to clarify and assess the scale of this problem once and for all. And the reason for this inaction is because they know that it would be bad for business. It would “cause a lot of people to stop taking their medications.” So the pharma-psychiatry cartel thrives, and the dance of death goes on.
Finally
If you live in the US, please write to your Senators and ask them not so support this legislation.














Excellent exposition of truth telling! My legislators know my views well, and I don’t see many minds opening. Purse string tighten neuro-space available for intake of knowledge–diagnostic code for that?
Report comment
Berta,
It’s called cash-induced learning disorder. Incurable!
Report comment
—-“How to reduce both violence and stigma”,
Who mentors anyone into believing a stigma is worthy of deep distrust.
Report comment
Harold,
That’s a good question! Who indeed!
Report comment
Hi Phil
We did a segment on the Murphy Bill on anosognosiac podcast a few weeks ago. I had a hard time describing how alarming it is. It may be the very worst thing to happen to our outstandingly broken system since direct to consumer advertising. It is exactly, preposterously wrong on so many levels. Using the phrase “evidence based” is especially Orwellion.
Over the past few years I’ve mostly had hope. There is more evidence (actual evidence) being published every month, and more people are willing to ask questions and challenge assumptions about “mental health treatment”. The Murphy bill is a devastating setback to hope.
The only silver lining is that its certain to increase the number of bad outcomes, which may eventually force the public to rethink their faith in the cult of “mental health” experts. It will also be incredibly expensive, and drive more people to disability.
The bill passed with overwhelming bipartisan support which is another breathtaking irony. (I wonder who the 2 dissenters were)
One thing that hasn’t been discussed is the position of ordinary psychiatrists, and how this measure will put pressure on them to “err on the side of caution” in both medications and diagnosis. They may now feel obliged to medicate more aggressively then they already do. Even if they feel a person isn’t a danger to themselves or others.
Once again you’ve articulated the issue precisely. I only wish your spotlight was shining on something more hopeful.
Thank you
Mike
Report comment
When I read these controversies, I think of the statement by Oliver Wendell Holmes, MD (among other things): “If we physicians threw all our medicines into the sea, it would be that much better for all of us and that much worse for the fishes.”
Report comment
These days the “medicines” ( and not only the ones that put people in suspended psychotropic animation),and facilities of the pharmaceutical cartels manufacturing them as well as other eugenic and supporting cartels would have to be disposed of as if they were toxic nuclear wastes. I forgot, they dispose of those in the oceans as well . Wendell Holmes, MD (among other things) must not have been a fish eater.
I guess the government of the 1% is becoming even more toxic to the people as well . Luckily the ocean is big . Fortunately I distill my water .
Report comment
bcharris,
Nice!
Report comment
The bill passed with overwhelming bipartisan support which is another breathtaking irony. (I wonder who the 2 dissenters were)
The 2 dissenters were Congressman Thomas Massie from Kentucky (my state) and Congressman Josh Amash, Michigan.
Report comment
Congressman Josh Amish .. not Amash
Report comment
No, Amash. He should be getting messages of congratulations.
Report comment
They apparently opposed it because they are opposed to increasing the role of the federal government in health care in general: “Republicans campaigned on reducing the federal government’s role in healthcare, so why would Republicans vote to expand the federal government’s role in healthcare?”
Source: http://www.nkytribune.com/2016/07/bill-straub-the-hits-just-keep-coming-for-massie-as-he-continues-to-add-to-his-legend/
It doesn’t sound like opposition based on individual liberty or related concerns.
Report comment
That’s beside the point.
It sounds like he’s primarily interested in consistency and has the courage to stand for his convictions. And he gives us an excellent point to be making to “conservatives” when arguing that they should vote against Murphy.
Another feather in his cap is that he has co-sponsored legislation to repeal the Patriot Act.
Report comment
Michael,
Thanks for coming in. It is a discouraging development. But I also see it as a kind of desperation on the part of psychiatry. Reeling from the barrage of anti-psychiatry broadsides, they are doubling down, so to speak, in their insistence that they are real doctors, ad that their “treatments” are good and wholesome.
Best wishes.
Report comment
The bill passed with overwhelming bipartisan support which is another breathtaking irony. (I wonder who the 2 dissenters were)
The dissenters were Reps. Massie (Kentucky) and Amash (Michigan), both Republicans.
Mike, the vote, heavily influenced by corporate and psychiatric industry pressure, was not based on any sort of careful evaluation of the “issues”; it was rushed through before anyone knew what was happening — based on a rule allowing “non-controversial” bills to be considered out of turn and without debate — and before we had a chance to register any organized resistance. They may try to sneak this through the Senate the same way.
That’s not to say that people here who consider themselves to be “activists” of any sort bear no responsibility for their inaction, or for leading people to believe that somehow it’s “all being taken care of” by those who know what they’re doing better than the rest of us. This is a surefire recipe for defeat.
Report comment
Andrew Scull began his recent piece, The Sociological Study of Mental Illness: A Historical Perspective, at MIA as follows:
“Mental illness, as the eminent historian of psychiatry Michael MacDonald once aptly remarked, “is the most solitary of afflictions to the people who experience it; but it is the most social of maladies to those who observe its effects” (MacDonald 1981: 1).”
http://www.madinamerica.com/2016/07/the-sociological-study-of-mental-illness-a-historical-perspective/
In my view, this is a set up. It’s like calling people with psych labels “voiceless” or “helpless” or “America’s most vulnerable citizens”. (They are, without constitutional protections, citizens?) Given a question, anybody it doesn’t go to could be characterized as “voiceless” on that question. You don’t hear them saying “powerless”, but that may be coming closer to the point.
Tim Murphy, Jeffrey Liberman, D. J. Jaffe et al., by supporting and promoting this legislation, are doing exactly the same thing, setting up a section of society, but not setting them up, of course, for success, quite the reverse. They are setting them up for the mental health system, and the failures and frustrations that go along with it. They are the “solitary”, “voiceless”, “helpless”, “most vulnerable”, and often “hurting”, etc. Not a pretty story!
It’s about time these guys learned, we can speak for ourselves, and allowed us a spot at the table. Then we are not so “solitary”, “voiceless”, “helpless”, “hurting”, and “vulnerable” as they would have us.
The mental health system is not broken because the mental health system should not be seen as a mechanism for violent crime prevention to begin with. Violent crime is going to happen because people commit violent crime intentionally and with malice aforethought regardless of psychiatric treatment histories. This takes us back to due process, something you don’t get where the law dictates medical practice, as in the mental health system.
Thanks for this very timely and important post. Yes, we need people to oppose what is happening, and now. I know Congress wants legislation. This is a matter professional politicians trying to claim they did something about violent crime. As politically advantageous to their career interests as it may be, they need to be told, this is bad legislation that in the end is going to do much more harm than it could conceivably do good.
Report comment
Frank,
Yes, the hypocrisy of we’re-going-to-help-these-poor-wretches is palpable. Thanks for drawing attention to this aspect of the matter.
Report comment
This Tim Murphy, from a district in the Southwest of Pennsylvania, excluding Pittsburg, and bordered on two sides by WV. They say that in WV they consume huge amounts of prescription pain killers. Some are calling them “Pillbillies”. I believe that Murphy’s district is likely much the same.
But I have a greater concern. From my view, those opposing the Murphy Bill are taking a pity seeking, or Uncle Tom approach. They are accepting the concept of mental illness, and especially the ideas of Recovery and Therapy.
So then this does absolutely nothing to oppose Murphy, as its supporters will simply point out that it really only effects the more severe cases, so we needn’t worry.
The opponents of Murphy are legitimating the main axes of abuse, therapy and recovery, instead of demanding justice. And we know that what underlies Murphy and the Psychiatric System are simply the bogus sciences of Social Darwinism and Eugenics.
So if we oppose Murphy by endorsing Psychotherapy and Recovery, we are just helping those who need scapegoats to justify extreme economic deprivation and extreme coercive conformity. It sounds like we are just asking for leniency, “Let us have our therapy and recovery, please.”
Where as what we should be doing is showing how most all of this is simply the ramifications of familial child abuse and social stigmatization, and then denouncing all psychiatry, psychotherapy, and recovery, and pledging that the more draconian parts of Murphy will be unenforceable.
Here from one of your quotes:
”
recovery and community integration practices that current consumers of mental health services and survivors of coercive psychiatric interventions have worked so hard for over the last 40-plus years to create for those most in need.
”
I say that we must completely disavow any mental health or recovery services consumer status.
Nomadic
Report comment
Nomadic — I totally agree with the thrust of your comment. I guess you’re aware that we’re developing non-“mental health” oriented points for fighting Murphy at the organizing forum, but just a reminder.
Report comment
Oldhead, thank you for responding to me. I’d not been seeing posts from you, and so you were missed. And no I did not know you were developing non-“mental health” oriented points, or about any organizing forum. Please tell me more. I would very much like to be involved in this.
Quickest and most reliable way to reach me:
http://freedomtoexpress.freeforums.org/
Here I have several replies to this Beatrice Birch and Inner Fire Healing and Recovery.
http://www.madinamerica.com/2016/08/inner-fire-healing-and-recovery-without-meds/
I my last reply I make it clear that I would never let anyone subject me to “Healing and Recovery”. And I would never let anyone I cared about be subjected to it either. Even though I know there are some with personal stories which would seem not to support this, looking at all the evidence myself, I cannot see how anyone would ever end up in Psychiatric care, Psychotherapy, or Healing and Recovery, unless they were already made the family scapegoat and abandoned.
Or even more, what the parents really want is for the child to commit suicide, as that would give them their final vindication. Like Daniel Mackler has said, “Suicide is the Ultimate Victory for the Family System.”
So I see their Healing and Recovery Programs as simply a continuing familial child abuse.
And then there are the Psychotherapists who advertise to parents, that they will fix their scapegoat and do it by exonerating the parents in the eyes of the child. That is really creepy.
So yes, I want to be involved in developing of non-‘mental health’ points for discouraging the passage of Murphy, and for resisting it if it does pass, and also for finally letting the public know the truth.
My first hand involvement does not go back this far. But based on what I have read about R. D. Laing and his clinic in London, he was not trying to do what the Recovery and Therapy people of today are. He was not trying to fix people, to make them “passible acceptable to most people most of the time.” He may have called it therapy or recovery, but it did not mean the same thing. So while Laing was certainly no revolutionary, he was willing to just let people be. There was no goal in his caring for them. They would find their own way, and he was certain that it could not be approached in any other manner.
Now the situation is completely different. There is a very thinly veiled Salvation agenda under all of these Therapy and Recovery programs. The idea is to exonerate and vindicate the parents.
See, a therapist will try to make you believe that the pain is all in the memories of the abuse. But this is a severe mind manipulation. The pain is in not having social legitimacy in the present because our world is based on lies and denial. Those who should be speaking up, are in Therapy and Recovery, believing that that actually redresses wrong and solves problems.
It doesn’t. They way to redress wrongs and give ourselves social legitimacy, and also to protect today’s children, is to organize and take legal and political action.
Thanks,
Nomadic
Report comment
It’s a little late as the current version is about to go online, as they will be needed immediately after the “holiday” by people who should be calling their senators. We’ll be polishing them up & expanding them as time allows however. It’s on the Organizing Forum, you know how to get there.
What’s important now is for people to stop making excuses and make the two calls. It’s not a radical action, but it can make a difference here and is thus strategically appropriate. The longer we can keep the dems and repubs arguing the longer it will take to bring it to a vote. The goal is to DELAY, and with each day we do we gain momentum.
Report comment
I don’t get it. How is blaming the “mentally ill” for all violence supposed to stop stigma?
Jaffe is one ignorant turd. Unless of course he wants to perpetuate stigma. That’s an obvious guess.
Report comment
FeelinDiscouraged,
Yes. Psychiatry’s insistence that all significant problems of thinking, feeling, and/or behaving are the result of malfunctioning brains is the ultimate stigmatization.
Report comment
If leprosy was on the increase, would these guys be recommending amputations to those vulnerable to catching the disease? Quick, cut their hands off before they catch it lol
Mental illness, the only disease you can catch from backbiters.
Good work Dr Hickey.
Report comment
boans,
Good points! Thanks.
Report comment
I agree with you completely Boans.
Nomadic
Report comment
Awesome article and you bring up some great points. By the way, thanks for the laugh about antidepressants being found in most tap water. The thought of people dancing in the street and your final line of “Oh Happy day!” made me laugh so hard, I almost cried.
When I think of Lieberman, I think of Melange reborn. Who would think of trying to induce psychosis on schizophrenic patients? I could only think of it in the context of a horror movie. As far as Murphy, well it does not surprise me about the increasing money coming from Pharma. With Sandy Hook and the parents suing for the medical information to be revealed that was redacted, they are protecting their revenue stream. Pharma needs this hidden. As far as patients not taking their medication, they are not stupid. The stuff just doesn’t work.
My question is why isn’t the data speaking for itself? That the medication can cause violence, brain damage and premature death. I just don’t understand it.
Report comment
MONEY.
Report comment
Amen.
Report comment
THE ‘UNTERMENSCHE’.
I notice “…particularly SSRIs..” included in reference to “acting out”. These drugs are consumed by more than 10% of the American adult population and they are prescribed for anything at all (not necessarily serious). So this points to the drugs causing normal people people to “act out”.
The “schizophrenics” are, 20 times more likely to commit suicide on neuroleptics than OFF Neuroleptics. I attempted suicide twice ON the drug Fluphenazine depot BUT NEVER OFF Fluphenazine depot.
Report comment
Fiachra,
Ignoring or explaining away this kind of information is perhaps the most important skill in psychiatry. It is extremely rare for psychiatrists to develop any real critical perspective on their chosen profession.
Report comment
deeeo42,
I agree.
Report comment
Anonymous2016,
Follow the money! It’s really what it’s all about.
Report comment
I agree but at what point does public safety become an issue. I mean who wants to drive a 70s Ford Pinto that blows up when you rear end the car?
There came a time when the cigarette companies had their comeuppance. This is similar. At what point do they find that the medication is causing the disability?
Report comment
Sorry should read when you get rear ended.
Report comment
Phil, well done for another great article challenging the mainstream reductionism and illogic. Just wanted to let you know I am still following and supporting you.
Report comment
BPDTransformation,
Thank you. I very much appreciate your support.
Report comment
I truly believe that what’s left of the Helping Families in Mental Health Crisis Act WILL be defeated. While there IS an accurate and widespread public perception of psychiatry as abusive, mercenary, inept, and NOT SCIENTIFIC in the slightest, the proponents and sponsors of the HFMHCA have two other insurmountable obstacles as well – 1) the MASSIVE rejection of this bill from Mad people and various other groups and 2) the PR liabilities they’ve shouldered from their foolish choice to recruit the “families of the ‘mentally ill'” as this bill’s foot-soldiers. Rep. Tim Murphy has MAJORLY underestimated how vigorously Mad people would fight his bill and how long we would invest ourselves and our resources into defeating it. In the comments sections of every newspaper article I’ve read that had promoted the HFMHCA, there were ALWAYS at least two or three Mad people who staunchly rejected this bill AND psychiatry. Nor did they pussy-foot around their “threats” to defend their 4th, 13th, and 2nd Amendment rights. Ditto (minus the “threats”) for TV and radio shows where viewers/listeners could call in to discuss the HFMHCA. Now, Mad resistance to this bill would certainly have been enough to sink the HFMHCA singlehandedly, but our family members’ self-interested and sensationalized support for this bill was a critical component of the success we’ve had in watering-down, delaying, and – I hope – crushing the HFMHCA. Mad people’s family members had agitated for this bill’s passage with the ONLY interpersonal skills they’re capable of using – fear-mongering, lies, doomsaying, and guilt. And unlike other grassroots public health campaigns, where entire families would “stand up and be counted”, the family members of Mad people have almost always campaigned for the HFMHCA *without* US – the family members whose “rights” they were, supposedly, trying to secure. In numerous instances, Mad people’s family members just flat-out refuse to share their media spots with Mad people. But on the RARE occasions when they DO, they’ll fight bitterly with them, while SIMULTANEOUSLY insisting that their campaigning for the HFMHCA is the best way – if not the only way – for “family members” to get their Mad “loved ones” the “care” they “need”. Years of these (the HFMHCA has been kicked around Congress for nearly four years) system-gaming shenanigans have provided the public a fresh and much-needed reminder of how pathologically selfish, manipulative, and unloving the families of Mad people can often be. The HFMHCA’s NAMI-mommy army was finally humbled for good in March, when #ManInTree went viral. Though it’s still too early to celebrate the HFMHCA’s annihilation, I do feel cautiously hopeful that we’ll witness that outcome within the next several weeks, and AMAZINGLY proud of myself and everyone else who has so worked to hard to stop this bill from becoming law. Thank you, Dr. Hickey, for keeping the pressure on Mad people to see the defeat of this bill through to the very end.
Report comment
It passed 422 – TWO. Why will the Senate be any different? Aren’t they just as vulnerable to psychiatric bullshit and big pharma money as reps?
Report comment
deeeo42,
I believe they are, and I greatly fear that you might be correct. That’s why we need to write to the senators and tell them our views. There’s one thing that politicians take more seriously than campaign donations: votes.
Report comment
What Phil said. Remember if you know what you’re talking about you only need to make a good case to two senators.
For the record, the dissenting votes were from libertarian Republicans.
Report comment
Also remember that the political motivation for the Murphy bills is the need of politicians to claim to their constituents they are “doing something about violence.” We need to upend and expose the arguments they use to try to accomplish this at our expense. Regardless of the rhetoric, it would be foolish for anyone to believe that “improving mental health care” is any politician’s goal (fortunately for us). So no one should waste their time making arguments from this perspective, they’re totally beside the point.
Report comment
J,
Thanks for this very encouraging and hope-filled comment. One of the primary tenets of psychiatry is: Thou shalt never blame family members. Thanks for bringing this issue into the open.
Report comment
this is excellent, thanks, Philip
the common quote about 50% prisoners having Dx of MI also includes those judged to have drug use disorders, inflating the fake science even more
Report comment
Eileen,
Absolutely! And intermittent explosive disorder, pedophilic disorder, antisocial personality disorder, etc.
Report comment
Know what finally ended the Salem witch trials? They went around accusing EVERYONE of witchcraft including the governor’s wife. Whoops!
Finally it was declared that there was no Biblical evidence for spectral persecutions. Just because a bunch of nasty, demented girls point and scream at you it can’t be used as evidence that you are in league with Satan.
I have hopes that now the pharmaceutical industry has made a similar gaffe in declaring 20% of the population “sick” and in need of brain drugs. If enough people take them they will realize that those of us who’re non-compliant aren’t really crazy at all.
Report comment
FeelinDiscouraged,
Yes. I think that pharma-psychiatry became intoxicated on their own success and rhetoric. They began to think of themselves as the Masters of the Universe, or something like that. And they pushed things too far, e.g., giving neuroleptic drugs to toddlers for temper tantrums.
Report comment
Hi Philip,
Nice to see you – on the ball as usual.
From 1974:-
“..The reluctance to take antipsychotic medication was significantly associated with extrapyramidal symptoms—most notably a subtle akathisia….”
Sometimes subtle and sometimes not so subtle.
I have attempted suicide twice on Fluphenazine depot injection with acute Akathesia; and
suffered from extrapyramidal side effects for the period of time I was on a disability payment.
I eventually approached my Psychiatrist with my extrapyramidal disability, and after a few dramatic months it was recommended I try a different depot brand that ‘would’ have less extrapyramidal side effects.
Not too long after being given the new depot medication (at twice the introductory dose and released into the community), I had to break into the “Psychiatric Unit” (in Western Ireland) with Full Flown Akathesia, presenting as desperate and at least a risk to myself. Less than 2 days later I discharged myself.
According to the notes which I have since received, my Psychiatrist had diagnosed me as suffering from a ‘pre psychotic episode’.
In my notes the records leading up to the introduction of the new medication had disappeared
(and my original extrapyramidal complaint to my psychiatrist was also not to to be found).
The original depot medication was produced by an American company and my Psychiatrist and his University had produced many Promotional Research Papers on this drug, BUT with no mention of – Acute Akathesia and it’s Effects.
My Former Psychiatrist had been doctoring Medical Records and Medical Research – and putting lives at risk. But the bogus Research paid well.
After the hospitalization in 1984 I moved to reduced oral medication, and the extrapyramidal side effects disappeared. I then became independent and made Longterm Recovery.
My Research Psychiatrist had also denied Disclosure of ‘The Option of Full Recovery’ as a result of coming off strong medications: – through Careful Drug Taper and Practical Psychotherapy.
Many years later my Former Psychiatrists University is conducting Complicated and Very Expensive, Neuroscientific and Genetic Research with a view towards discovering a cure for – “What I Was Supposed to be Suffering From – And Recovered From”, more than 30 years ago.
Report comment
Fiachra,
Yes. Psychiatry routinely attributes adverse drug effects to the “illness” or the “episode”. And the hoax goes on.
I had wanted to write more on the akathisia, but the post became very lengthy. I plan to go back to those early papers some time soon, and discuss what they showed. Some of those individual psychiatrists were actually fairly straightforward on the link: drug-akathisia-murder/suicide.
Best wishes.
Report comment
The story of a friend who used to party too hard, with too much drugs, no sleeping for days, barely eating, for months. He acted crazy, lost a lot of weight, and was expelled from college. One day, he began to behave “paranoid” and “psychotic” and started attacking people. He was arrested, sedated, diagnosed with “bipolar disorder”, and commited to a hospital.
Family was told by the Doctor: “It’s probably genetic”.
A brother said: “He never showed any symptom growing up. Everything began after he started with his parties”.
The Doctor said: “The drugs he took only brought to the surface the underlying genetic disorder”
Another brother said: “You just made that up!”
The Doctor said: “You are not quallified and don’t understand. Just follow my instructions. You all should also start using medication as a prevention.”
Psychiatry is bullshit on stilts.
Thank you, Mr. Hickey.
Report comment
camile,
I reckon there’s a whole population of “schizophrenics” that are in reality cannibas smokers that were overdoing it.
Report comment
Camile,
This would be unbelievable, except that it’s become routine. Would you mind if I quote your comment in a short post?
Report comment
What’s Causing the “Out of Character” killings in the Normal Population?
http://www.telegraph.co.uk/news/2016/08/29/family-of-five-found-dead-in-their-countryside-home-in-apparent/
http://www.dailymail.co.uk/news/article-3727704/Parents-three-young-children-dead-apparent-murder-suicide.html
Report comment
GOD BLESS *YOU*, Dr. Hickey! Succinct, huh?….
As a survivor of the pseudoscience LIES of the DRUG RACKET known as “biopsychiatry”, I find it very TRAUMA RE-TRIGGERING, to fully and carefully read this EXCELLENT article. But I get it, oh, yeah, I get it. THANK-YOU, Dr. Hickey! Can I be one of your protégés?….
Report comment
Bradford,
Thanks for your support. Feel free to be a protégé.
Report comment
Danse macabre:
https://www.youtube.com/watch?v=71fZhMXlGT4
Report comment
Phil — How ironic that my currently sole focus on fighting Murphy led me to miss this article till now, as I’ve been spending my MIA time at the organizing forum exclusively. You address some of what we’re working on, as well as other things we should be working on.
A number of us have been developing Murphy talking points for people who don’t want to approach this as a “mental health reform” issue but one of domestic repression. Those who wish to participate are still welcome but we’re on the verge of completing 6-7 arguments against the House version with documentary backup for those who can be convinced to make two phone calls to their senators, and wish to present their positions effectively and convincingly.
It’s important to discuss the Senate Murphy bill and the differences between the two, and how to argue against them both. This is the next step and needs to be taken up asap.
These discussions are taking place at the organizing forum for those who wish to seriously work on this stuff. Phil, we’ll be sending you & others info on this soon, till then y’all know how to find us.
Report comment
Incidentally, though the “Senate Murphy” apparently doesn’t include AOT, it is even more totalitarian than the House Murphy in that it openly calls for the elimination of the differentiation between physical health and “mental health.” It also calls for “early intervention” for children as young as three. I believe Chris Murphy or his co-sponsor have stated that 20% of Americans have “serious mental illnesses.” Are we being prepared for a society in which 1 in 5 people are forcibly drugged?
If people don’t call their senators the argument over Murphy will be between different factions of the pharmaceutical/psychiatric establishment.
One last FYI — the July 6 vote was deliberately announced on a Friday as people were leaving for the 4th of July holiday, leaving several of us here trying to alert people all weekend to no avail. Nor were any of the professional “Mental Health Recovery” advocates available till the following Tuesday, the day before the vote. So keep that in mind when bemoaning the lopsided vote, because they’ll likely try to sneak this through again while no one’s looking. Also it makes no sense trying to “predict” what will happen with Murphy, as what each person does has an impact on what will or will not “happen.”
Report comment
Oldhead,
Thanks for the update. I look forward to seeing your document.
Report comment
Should we contact you via the internal MIA system or is there a better way?
Report comment
oldhead,
The internal MIA system works, or you can use the contact information on a tab at the top of my website.
Report comment
URGENT BREAKING NEWS — ACTION NEEDED:
According to a Jaffee facebook group they’re trying to amend the Senate Murphy bill (SB 2680) to include Assisted Outpatient Treatment (AOT), which had not been part of the bill before.
It is imperative to call your Senators and demand that the AOT provision be removed prior to the bill coming to a vote. Emphasize that AOT is a euphemism for massive forced drugging with dangerous and violence-inducing drugs, and represents a human rights violation, and that its inclusion totally changes the nature of the legislation..
We will try to have more extensive anti-AOT talking points available by Tuesday.
Report comment
Oldhead.
These drugs:-
http://www.madinamerica.com/wp-content/uploads/2016/08/Suicide-Associated-with-Akathisia-and-Depot-Fluphenzaine-Treatment-KShear-1983.pdf
are violence and suicide inducing and Near Fatal Experiences are being intentionally omitted from patients histories – by the doctors that are paid to produce the Research Papers on these drugs.
I would say in their natural state the “schizophrenics” are less prone towards violence than the average person; and looking at the background that’s where the evidence points.
Report comment
A quote from a Jaffe facebook group:
“”Having said that, the antipsych community seems to be a heavy concentration of personality disordered people whom do not acknowledge the mutual responsibility in relation to meds. They do make clear, the lack of quality of life they live as they go untreated.””
More motivation to contact your Senators regarding everything Oldhead has mentioned.
Report comment
Message from the Jaffe group. Please contact your senators to thwart their efforts.
“”TODAYS THE DAY! The Senate is back in session today. We are close to getting mental illness reform put on their (short) calendar! Please call your Senator TODAY at 202-224-3121 (or the direct number at the link http://www.senate.gov/senators/contact/) and ask him or her to pass Mental Illness Reform Act (S. 2680) and include the provisions that are missing from it that are included in the bipartisan bill that passed the House 422-2 (Helping Families in Mental Health Crisis Act, HR 2646). Those provisions create more hospital beds, establish Assisted Outpatient Treatment, and reform SAMHSA so it focuses on evidence based practices that really help the seriously mentally ill. Those must be part of mental health reform or the seriously ill will be left out. Thank you. WE CAN DO THIS!!!””
Report comment
Does anyone care that Jaffee et al. are actively working and making phone calls AS WE SPEAK to spread lies and hate about us?
Let’s HOPE y’all are as actively opposing this bill as they say you are, by making the appropriate calls saying the EXACT OPPOSITE of what they’re telling their people to say in the post above. Also thanks to the Jaffee group for this: “Please call your Senator TODAY at 202-224-3121 (or the direct number at the link http://www.senate.gov/senators/contact/ )”
Let me recap: the House Murphy bill (HR 4626) is the BAD bill which has passed the house; the senate Murphy is the ALMOST AS BAD bill, except it doesn’t include AOT. Jaffee et al. are trying to get the Senate bill (SB 2680) amended to also include AOT, making the bills almost identical.
What we need to do is tell our Senators NOT to allow the Amendment to include AOT, and to withhold voting on the Senate bill (SB 2680) without time for further discussion, and more input from opponents. Tell them the issue is too important to rush through because of the congressional schedule, that to do it right a full and open debate is needed.
There’s nothing scary about calling your senator. It’s unlikely he/she will talk to you personally but if you try hard you can often engage the administrative assistant or whomever and make an impression which will be conveyed. They’re probably not used to hearing from the likes of us so go easy on them!
Report comment
ANTI-AOT/ANTI-H.R. 4626 (MURPHY) TALKING POINTS
1. “Assisted Outpatient Treatment” as described in HR 4626 is in essence a program of massive forced drugging which, though presented as being in the best interest of the “mentally ill,” is strongly supported by the pharmaceutical industry, which takes in billions of dollars for drugs with no proven scientific or medical justification; which cause untold physical damage and intractable dependency issues in many of those to whom they are prescribed; and which have been linked to many incidents of suicidal and homicidal violence. Pharmaceutical profits can be expected to rise substantially should HR 4626 become law, a fact which should be recognized when evaluating corporate support for the bill.
2. Proponents of AOT claim that recent mass shootings and acts of “senseless” violence have been carried out by people with “untreated mental illness.” This is frivolous speculation at best. And contrary to Representative Murphy’s promotional materials, several of the perpetrators of mass killings he listed as responsible for their horrific crimes as a result of being “untreated” were indeed in the “care” of doctors, and had at some point been prescribed psychiatric drugs as part of that “treatment.”
3. There is convincing evidence that many common psychiatric drugs, far from preventing violence, actually induce violent thoughts and acts in many people. The increasing frequency of these acts seems to correlate with the increasing use of such drugs, which are portrayed as “medicines” despite the lack of objective medical or scientific evidence that they correct a demonstrable pathology. For example, mass killers Eric Harris (Columbine) and James Holmes (Aurora) had been prescribed Zoloft (or a version of such). Many other high profile mass murderers have been prescribed drugs with mechanisms of action the manufacturers can’t explain, and with a list of known “side” effects including hallucinations, anger, suicidal thoughts, violence and suicide — reactions which led to their receiving black-box warnings.
4. Studies have demonstrated for decades that those labeled “mentally ill” have a lower incidence of violent behavior than the public at large. Even many of those on the “front lines” who support some psychiatric measures intended to prevent violent behavior agree that involuntary “treatment” (usually consisting of drugging) is counterproductive. So-called “assisted outpatient treatment” programs constitute costly, irrational and ultimately futile attempts to make our country safer.
5. After the Japanese military shocked the American public with the attack on Pearl Harbor, President Franklin D. Roosevelt signed an order requiring the banishment of Americans of Japanese descent to substandard “housing” camps on barren inland terrain. For up to three years, innocent people had little privacy, comfort, or autonomy, because of fears that among them were spies and conspirators. The “Murphy” bill if enacted would represent a similar program of scapegoating innocent people to pander to public hysteria and make people feel “safe” from a non-existent threat.
6. The use of physical force to transport, incarcerate, strip-search, restrain and inject powerful and unpredictable drugs into nonviolent children and adults who have committed no crime far exceeds what can be legally done to violent felons. Such treatment is routine in psychiatric wards, and constitutes a violation of the most basic human and Constitutional rights. The U.N. has emphatically weighed in as opposed in principle to involuntary psychiatric intervention as a violation of human rights and dignity.
===========================================================
http://www.madinamerica.com/forums/topic/fighting-murphy-on-to-the-senate/
Report comment
“In addition, from a marketing perspective, it may be necessary to capitalize on the fear of violence to get the law passed.” — D.J. Jaffee
Isn’t this like capitalizing on 9-11 to invade Iraq?
This quote should be posted far and wide.
Report comment
It looks like we’re being sold down the river big time by our so-called “allies.”
The National Coalition for Mental Health Recovery has been telling people to SUPPORT the Senate version of the Murphy Bill (SB 2860). This is crazy. And it may illustrate better than anything the clear line that separates so-called “consumers” from the anti-psychiatry movement. These people claim they are “advocating” for us. Here’s their ” logic”:
S. 2680, the Senate version of mental health reform, does not have the toxic language in it that is in the House bill. We must urge our senators to support S. 2680 without amendments or changes.</I.
Calling for the elimination of the “barriers” between real health and “mental” health is not toxic? Advocating “early intervention” for children as young as 3 is not evil?
I am calling on people reject the NCMHR position, and to tell your senators to vote AGAINST SB 2680, and, no matter how they decide to vote, to reject any attempt to add Assisted Outpatient Treatment to the bill. I ask for you to affirm your support for this position here as well.
Remember, NCMHR did a great job of helping us lose Murphy I by a 422-2 vote margin; now they’re setting us up to lose big time again. This is a "lesser of the two evils” approach and by following it we will reap the inevitable results of such.
Phil, any chance you can do a followup article on this?
Report comment
Perhaps we could remind the good senators that “The American Psychiatric Association {said] in no uncertain terms that psychiatrists had absolutely no ability to predict dangerousness .
The Royal College of Psychiatrists in the UK has also denied responsibility in predicting dangerousness.
In 1983, Alex Pokorny conducted a large study of the prediction of suicide of 4,800 individuals who were being admitted for psychiatric services in a United States hospital. He was unable to find any combination of clinical or other factors that could be used in practice, concluding that there were no methods to predict particular suicides “before the fact”…
It is also difficult to predict who will be at risk of harming others because of the low rate of violence among those with severe mental health problems, compared with other groups. MacArthur Violence Risk Assessment research suggested that a diagnosis of severe mental illness, in particular a diagnosis of schizophrenia, was associated with a lower rate of violence…
So on what grounds does the Murphy Bill base its claim that Compulsory Treatment in the community is required to keep the public and the `mentally ill’, safe?
Does the Bill plan to extend compulsory supervision of ALL past patients under what sounds awfully like PAROLE for extended periods or permanently because there MIGHT be an incident? Even a convicted felon has a finite term of supervision and in Australia, e.g. while there is a desire to keep pedophiles locked up/down forever because they MIGHT re-offend, there is a significant Human Rights legal challenge to this and it won’t happen. But our Mental Health system (Australia) which already has a Murphy type Bill in place, can keep ex-patients forever tied to medication and `treatment’, and if people decide to challenge this they are imprisoned, often via the police breaking down the door, or snatching them off the streets, in a mental hospital and the drugs resumed and compliance restored. Consequently a large sub group of our population live in constant fear, is that what they want?
Report comment
Consequently a large sub group of our population live in constant fear, is that what they want?
Yes, I do think that’s what they want.
We have two “Murphy” bills competing for “most oppressive” status. Due to its inclusion of AOT, the House version wins hands down. However in terms of insidiousness the Senate version could be more of a long term threat.
Any way you look at it, the idea that either version should be supported because the other is worse is simply atrocious, and I consider it scandalous that some of those who purport to speak for survivors are encouraging such support.
The American Psychiatric Association {said] in no uncertain terms that psychiatrists had absolutely no ability to predict dangerousness .
Do you have a link or something to document this with? If so it would be good to include this the next time our anti-AOT “talking points” are updated.
Report comment
In another legal case. Tarasoff vs. Regents of the University of California, the CA Supreme Court held that if a therapist’s client made specific and believable threats to kill a particular person, the therapist had a duty to warn the potential victim. During the litigation, the American Psychiatric Association filed an amicus brief, saying in no uncertain terms that psychiatrists had absolutely no ability to predict dangerousness and should never be held liable for anything like the Tarasoff situation.”) A nice little legal disclaimer.
Ted Chabasinski put this up in 2013 – I don’t know if it was in an MIA article, it may have been and would be in the archives
Report comment