

Public support for the US National Suicide Prevention Lifeline is soaring. In 2017, the rapper Logic released a Grammy-nominated song titled with the Lifeline’s 800-number that peaked at No. 3 on Billboard. Since then, call volumes have increased more than 25% as bloggers, vloggers, health zines, and news media from BuzzFeed to USA Today have run promotional stories. COVID-19 pushes volumes higher. Recently the federal government passed legislation mandating that, by 2022, all calls to “988” will be routed to the Lifeline—and some telecommunications companies have already begun implementation.
Driving much of this is growing awareness that calling 911 for issues of emotional distress can lead to deadly police interventions. Yet under-reported and under-investigated is the fact that calls to the National Suicide Prevention Lifeline (NSPL)—which prominently advertises itself as “confidential”—are often covertly traced. Callers get subjected to police interventions and forced psychiatric hospitalizations. Police shootings occur. Many callers describe their experiences as terrifying and traumatizing, and say the betrayal has made them feel more isolated than ever. And if 988 is implemented as currently planned, insiders say, every independent crisis call center in America could soon feel pressured to join the NSPL and trace calls.
NSPL call-tracing has been practiced for years. But inquiring journalists are told it occurs only in “rare” situations of impending death, and are asked to avoid frightening people from seeking help. Complaints on social media, however, are increasingly visible. For example, below this therapist’s video promoting the Lifeline, amid many testimonials about positive conversations there erupts a never-ending stream of comments from people—including children—devastated after their calls were traced.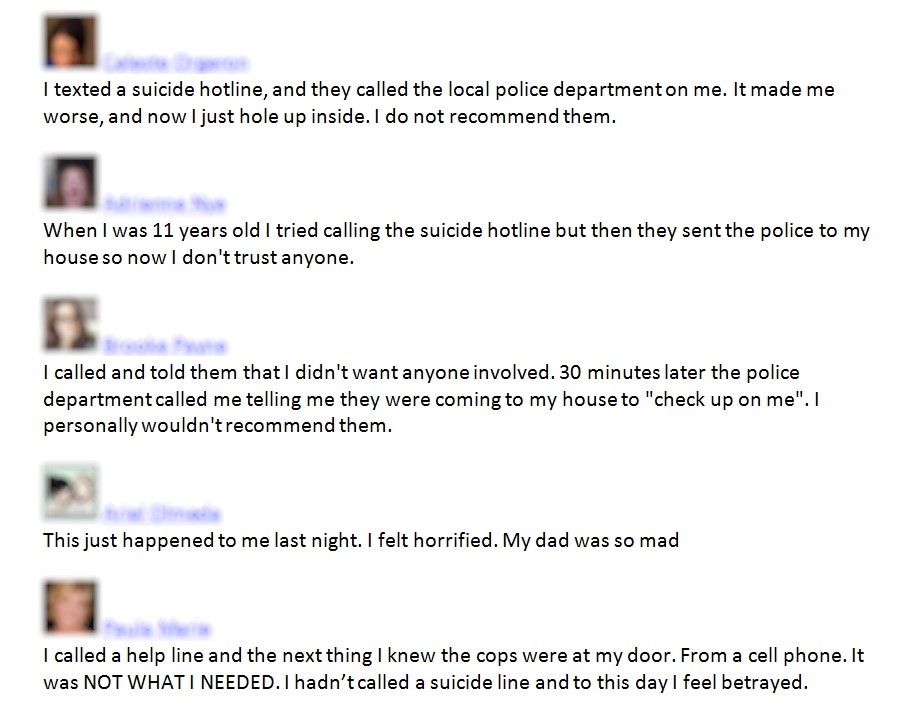
A Police Visit at Work
Most of the people who’ve been subjected to call-tracing requested anonymity for this story, usually for the same reasons they wanted anonymity when they called the National Suicide Prevention Lifeline in the first place. They were concerned about potential repercussions in their lives, families, and careers if they revealed their feelings—and their experiences after calling the Lifeline only intensified those concerns. In these cases, only the initial of their first name has been used.
One of these people was S., a mid-twenties, African-American veteran who works in commercial aircraft maintenance. Though he emphasized he’d never endanger anyone else, a lawyer has confirmed his future chances to get security clearances could be jeopardized by what happened.
When feeling stressed at work, S. sometimes called the Lifeline. “The negative emotions are less oppressive, like there’s a burden lifted that someone’s helping me share,” he says.
One day last year S. called during lunch—he says he wasn’t actively suicidal but was just “feeling pretty down.” After ten minutes, he cut the call short to get back to work. Twenty minutes later, police arrived at the hangar. They said they’d heard he was suicidal, took his access badge, and escorted him to an ambulance.
S. was stunned—he’d used his personal cell phone, and hadn’t shared his name, location, or type of work. He had no idea the Lifeline could trace calls. “It was really embarrassing and traumatizing,” says S. “All my coworkers and my lead and supervisor, they saw me get taken away.” Police are especially intimidating to him, he says, because growing up in New York he was frequently subjected to random stop-and-frisks, and as a 6-foot-3 black man, he imagines he can look dangerous.
S. was detained in what he describes as an “absolutely miserable” veteran’s hospital. He was only allowed to leave several hours later when his brother-in-law came to get him. S. was saddled with a $1,050 ambulance bill, and had to get clearance from another doctor to be allowed back to work. He wonders if these events played a role in his getting laid off three months later, ahead of people with less seniority.
“The hotline was the most reliable place for me to get help when I needed it, and now I feel I can’t trust that place anymore,” says S.
One Call Endangers Her Legal Career
A young white student with close-cropped hair and a calm, measured tone, H. had recently left an abusive relationship and moved to Ohio for law school in 2018. She was feeling isolated and self-doubting, but had no health insurance and couldn’t afford therapy. “I was just depressed and kind of wishing that I might just die,” she says. “I wanted to talk to another person and maybe be reassured a little.”
The Lifeline conversation was awkward. “I didn’t feel like she was really hearing me. She was kind of using canned responses.” Much later, H. learned the call-attendant was secretly ushering her through a suicide screening questionnaire.
The call-attendant asked, “If you were going to kill yourself, when would you do it? And how would you do it?” H. hadn’t thought seriously about it before, but suggested to the call-attendant that she’d likely overdose with pills. “I just kind of gave her the first answer that popped into my head. I thought it was kind of a weird thing for them to be asking me, because isn’t the goal to try to talk me out of committing suicide, instead of helping me make a plan?”
The call-attendant started suggesting H. go immediately to a psychiatric hospital, but H. said she had a class soon. The call-attendant wanted to send police out, but H. said that was unnecessary. The call-attendant replied, “The police can determine that.” Frightened, H. hung up.
Fifteen minutes later, police and an ambulance came. H. says she was “freaked out” and worried about her new neighbors seeing “this spectacle.” The police, she says, “had already made up their mind.”
H. was strapped to a stretcher. At the hospital, she was forced to strip completely with several people watching. She was put in a small room with nothing but a bed, and left for twelve hours with no explanation what was happening.
“I was terrified,” she says. A social worker came by for about five minutes. “He diagnosed me with bipolar disorder. I don’t know where he got that from. And he was trying to make it sound like I told them I had tried to overdose prior to calling the hotline. And I was saying, ‘No, that’s not what I said at all.’ And he told me that now I was lying.”
H. had no previous experience with psychiatric hospitalization, so didn’t know that everything she was being put through is disturbingly common—as Susan Stefan’s Emergency Department Treatment of the Psychiatric Patient shows.
H. had arrived at 8:30 p.m. and was too anxious to sleep all night. At 10 a.m., she says she was “brain dead” from exhaustion when she was run through various interviews and told she’d be detained for evaluation in the psychiatric unit.
She felt “panicked,” she says, but told herself, “Just try to act calm, don’t give them anything they can use against me.” The way she was being treated, she says, put her in a “criminal defense kind of mindset.”
H. was put in a room with someone violently detoxing, prescribed two psychiatric drugs, and reprimanded for skipping breakfasts and some of the group therapies. After 72 hours, she was told a court application would be made to keep her longer. “It has very serious career implications, because when something like that goes to court, you’re introducing it into the public record,” says H.
When applying for a license to practice law, she explains, anything hospital staff noted or said about her could make the state board of bar examiners question her “mental fitness.” It’s a common bar practice that’s increasingly criticized.
“I knew that I had to avoid going to court at all costs, and my only way to do that was to sign myself in voluntarily… There was fuck-all that was voluntary about this.”
Two weeks later, H. was discharged—with a hospital bill for $50,000. “It was more than my student loans!” says H. She negotiated it down to $20,000 and a ten-year payment plan.
H. says she’s considered complaining to the National Suicide Prevention Lifeline, “But at this point, I just don’t want any further contact with any of these people.”
Some Avoid Hospitalization, Some Don’t
When asked, many callers are genuinely perplexed about why their calls were traced, and suggest that the call-attendants were over-anxious themselves, over-eager to “help,” or just misunderstanding.
Peer-support worker Valerie Clark says they got a police visit after trying to persuade a local call-attendant to help expedite a therapy referral. Clark got into an argument, called the attendant “useless,” and hung up. When police came, Clark kept a “low tone” and presented as “solid and stable and credible,” and the police departed.
J., a PhD science student and transgender man of Middle Eastern heritage, knew about call-tracing but thought he was safe because he’d bought a disposable phone and, after his call to the Lifeline, removed the battery. Police found him anyway.
His voice shakes as he describes questioning the need for drugs, and a group of men at the hospital grabbing his 5 foot 8, 105-pound frame and holding him down for an injection. “I’m just crying… Please don’t touch me. Please don’t touch my body… One is pressing upon my forehead so hard that I think my glasses are going to break…”
J. was discharged a week later. “I was so traumatized that I dropped out of university,” he says, likening the experience to being raped. J. has been working on formal written complaints, but to get past the shame and humiliation, he says, “I have to pretend it wasn’t me, that it happened to someone else.”
Unreliable Science, Aggressive Policy
Delving into the policy, science, and call-data, it’s clear that such disagreements and misunderstandings between call-attendants and callers are not only possible, they’re probably very common.
The NSPL is managed by a nonprofit, Vibrant Emotional Health, under contract to the US Substance Abuse and Mental Health Services Administration (SAMHSA). John Draper directs the NSPL, Disaster Distress Helpline, Veteran’s Crisis Line, and other interlinked national hotlines. About 170 community crisis centers are members of the NSPL, and comply with Vibrant-NSPL policies. Calls to the NSPL’s various 800 lines get routed to the geographically closest member center, and other centers provide backup. Centers also take calls through their own local numbers. Call-attendants are often a mix of staff and volunteers.
The NSPL’s website and ads declare all calls to be “confidential,” and do not prominently disclose any limits to that.
Member centers vary in whether, how forthrightly, or how often they might disclose. The practice of forcibly intervening is described in NSPL policy and in a journal article co-authored by Draper.
A caller is identified as at “Imminent Risk” when the call-attendant believes that, in the relatively near future, the caller might take their own life. Actual “suicide attempts in progress” are just one, apparently rare, subcategory of Imminent Risk. To determine if other callers are at imminent risk, call-attendants secretly run callers through a risk-assessment questionnaire to determine if a caller has the desire, intention, and means to kill themselves. “Buffers” against suicide might also be considered, such as the presence of others in the home or the caller taking actions suggested by the call-attendant.
“Active rescue”—the euphemism for call-tracing and interventions by police and ambulance or mobile mental health crisis teams—is to be executed as a “last resort.” Yet interventions can also be triggered simply if a caller’s general mental-emotional state seemingly might lead to “harm to self or others,” and when third parties say someone they know might be at risk. Draper’s paper justifies intervening without caller knowledge or consent with a seeming doublethink premise: a) suicidal callers are not in a rational state of mind, yet b) suicidal callers rationally grant “implicit” consent to interventions simply by calling the hotline. The paper acknowledges “small but significant disagreement in the crisis center community” about this logic.
Certainly, US law gives broad latitude for breaches of confidentiality and forcible interventions that are intended to help others in danger. But how many people who call a suicide line to talk about suicidal feelings do not have any desire or intention to kill themselves nor access to any of the most common means such as pills, poisons, ropes, guns, jumps, and suffocation? So, with an average 10-minute call duration, is deciding who gets a police visit basically a crapshoot?
Yes—according to all the research, including the NSPL’s.
A 2017 meta-analysis found that expert ability to predict suicide barely beats random chance, and “has not improved across 50 years of research.” A 2018 review found that suicide risk-assessment methods all produce an “unacceptably high false positive rate.” A 2016 study of NSPL centers acknowledges that “an empirical foundation for warning signs of imminent suicide risk is lacking,” and the whole concept of Imminent Risk “is fraught with problems such as lack of clarity and imprecision.” SAMHSA-NSPL documents show a history of “inconsistent” assessments; one study of just four NSPL centers found that the number of times police were sent out ranged from 0.5% to 8.5% of calls.
So how many people is this actually happening to? And is there any way to protect against it happening?
A Well-Meaning Invasion of Privacy
Christopher Parsons, senior research associate at University of Toronto privacy-and-surveillance monitoring group Citizen Lab, had not heard of suicide-line call-tracing, but his explanation of how it’s likely done is confirmed by various sources, including a paper from the National Emergency Number Association, which NSPL representatives helped draft, and a Canadian telecommunications report.
With Caller ID and a landline, location can be found using widely available databases. With blocked Caller ID, mobile devices, and online chat, call-attendants contact 911 and get routed to a “Public Safety Answering Point” (PSAP) for “Enhanced-911” (E911)—usually police. Call-attendants give the exact call time, or the IP number. PSAP staff then obtain number, billing, and/or location information from telecommunications databases. They can also “triangulate” locations using cell towers, but most commonly today they covertly ping the GPS chip in mobile devices.
Can GPS-pinging be blocked? “This isn’t an operating system feature,” says Parsons. “This is baked right into the guts of the phone itself. It’s going to bypass the controls that you may have set in place.”
The GPS-pinging can work even if the mobile is turned off or main battery has recently died. This manufacturing standard was nobly intended—when we call 911, emergency responders can now quickly find us. However, Parsons says Canadian police have been evasive about other uses. The Electronic Frontier Foundation is fighting cases where US police tracked suspects without warrants.
Parsons says it’s concerning that there are few legal rules and no public transparency surrounding E911 usage. “Step one: I think that when novel policing technologies are being developed, or being deployed, or in use, there needs to be with it an explanation of the law and how that operates, as well as a mandatory reporting framework. That’s the institutional, bare minimum.”
Electronic Frontier Foundation’s Andrés Arrieta was also surprised, and similarly wants more transparency. “They should simplify and explain to people at the beginning what ‘confidential’ means,” says Arrieta. “And how many times a day do they query for the location data?… What was the reason? Was it reasonable? What was the result?”
SAMHSA and Vibrant/NSPL are anything but transparent.
Both refused to provide detailed statistics. I initiated a freedom of information request, and SAMHSA alternately ignored my requests for months, claimed they had nothing, or delivered trickles of general information.
SAMHSA finally handed over a survey:
The NSPL received 2.2 million calls in fiscal year 2017-18. Many call centers didn’t complete the survey or answer certain questions, but out of 1,020,142 calls, 21,055 callers were labeled as “Imminent Risk” and subjected to “Active Rescue.” Extrapolating that 1-in- 50 rate to all NSPL calls, that’s 44,000 callers who got visited by police that year. A percentage reportedly involved caller “collaboration”—but that includes callers who buckle to pressure.
This 2% rate is what the NSPL admits publicly. However, the number and rate of interventions appear to be much higher.
Mobile mental health crisis teams were sent to visit another 108,386 callers—teams that are often accompanied by police and may also forcibly hospitalize people.
The survey did not ask NSPL centers how often they dispatched police in response to calls coming in through their local numbers—that’s 8 million more calls and, assuming the same 2% average, 160,000 more police interventions annually.
Of course, there are likely many repeat callers and, notably, only about 20% of calls are suicide-related. So, the number of callers to NSPL centers who get police visits each year is in the hundreds of thousands, and the rate of forcible interventions on callers who specifically talk about suicidal feelings could plausibly be anywhere from 2 to 20 times higher than Vibrant/NSPL implies publicly.
What’s really going on? I stopped digging for more data when SAMHSA and the NSPL’s Draper promised me interviews—which they then didn’t give. Vibrant/NSPL media representative Frances Gonzalez also refused to answer any questions about Imminent Risk practices.
Meanwhile, in a promotional video, Draper actually criticizes how the mental health system forcibly intervenes on suicidal people, and repeatedly lauds how, conversely, the NSPL is all about “empowering” callers to make their own decisions about “what kind of care they want, how they want it, and when they want it.”
Callers in Danger, or Call-Attendants in Fear?
Some people who’ve taken the NSPL training or worked as call-attendants have publicly expressed concerns.
Megan Wildhood is a Seattle writer who identifies as autistic and has criticized NSPL training. In line with NSPL documents I obtained, Wildhood says the training was two half-days, with two hours devoted to making risk assessments using a question-and-answer “decision tree.”
“They tried to balance empathy with this standardized way of approaching callers who are experiencing some form of suicidal ideation,” says Wildhood. “It’s unnatural. It’s like chutes and ladders. How can you tune into another person? These questions are geared towards saving time.”
Wildhood asked about people who’d had terrible experiences after their calls were traced. The trainer replied, “We help more people than we hurt.”
Katie Tastrom is a sex worker and disabled writer and activist who worked at an NSPL crisis center for several months and wrote about how police interventions are more dangerous for people who are poor, minorities, disabled, or otherwise marginalized—people also more likely to rely on free support hotlines.
To Tastrom’s recollection, she never forced an intervention on anyone, but it was a daily occurrence in the center and she felt pressure to do it as part of her job. The numbers of interventions sometimes went up, and then there’d be discussions and trainings to bring the numbers down. “There’s definitely people who would call the police pretty quickly,” says Tastrom. “Some people just got really panicked; they felt like it would be their fault if the person killed themselves.”
Other fears and biases also came into play. “People with a specific mental health disability, people with quote unquote psychosis, things like that, definitely would be at risk of having the police called on them way more,” says Tastrom. “They’re seen as not being able to make decisions for themselves.”
Is There Something Wrong with Honesty?
Even if there might sometimes be understandable reasons to breach confidentiality, why not at least honestly disclose to callers that it could happen? In speaking with hotline operators, it becomes clear that, alongside their strongly-held beliefs about how to truly help people, their hotline’s popularity with callers and funders is at stake. And amid 988 implementation, the differences of opinion are approaching a political crisis point.
Crisis Services Canada is a similar network to the NSPL, and similarly wouldn’t discuss its call-tracing practices. However, Stacy Ashton, director of the Crisis Centre of British Columbia, says they send out police in response to about 2% of calls.

Ashton dislikes how “boilerplate” disclosures can “maintain that impression that suicide cannot be talked about.” Disclosure can also make some people unwilling to talk, she says, and harmfully isolate them further.
Of course, disclosure could also make some callers seek out other hotlines that don’t trace calls—possibly partially explaining the evasive secrecy of the NSPL and Crisis Services Canada and their member centers, who hinge their funding appeals on their popularity.
For her part, Ashton says that letting people potentially kill themselves or sending police and forcibly hospitalizing them are “two really undesirable alternatives” and “not a decision that any one of us wants to be locked into.” She describes the conundrum as “the definition of a system problem. When humans are doing the best they can with the tools they have, but the tools they have are not adequate.”
Ashton says high-profile US police shootings have had “ripple effects” in Canada. “The core assumptions of how we handle mental health crisis in our society is up for grabs. It’s an amazing opportunity to actually talk openly about it.”
She hopes to host consultations with diverse stakeholders to explore alternatives. One roadblock, Ashton says, are the crisis center accreditation standards of the American Association of Suicidology (AAS). “They don’t support a completely anonymous crisis line.”
Bart Andrews sits on executive committees of the AAS and the NSPL, and is Chief Clinical Officer at a Missouri NSPL crisis center. He supports call-tracing, and says people need to understand how much call-attendants struggle with feelings of “moral liability.”
“You’ve got to ask yourself, which problem do you want to deal with? The person being dead, or them being angry that the police come out to make sure they’re safe?” says Andrews. And families sometimes sue. “You’re not answering to the person you didn’t call the police on. If they end up dead, you’re answering to their loved ones.”
Nevertheless, Andrews acknowledges mounting research showing that psychiatric hospitalization seems to be extremely suicidogenic. “When suicide researchers talk about elevated risk, they’re talking about three times, four times, and sometimes ten times,” says Andrews. “When we talk about inpatient treatment, it’s exponentially larger.”
After being psychiatrically hospitalized and treated, people become dozens or even hundreds of times more likely to kill themselves—even if they were never suicidal before. But Andrews believes more studies are needed to understand what this evidence truly means. “The lack of data is troubling. We hospitalize people at risk of suicide, even though we don’t have any evidence that hospitalizing them is particularly helpful.”
His center’s call-attendants usually disclose the possibility of active interventions; Andrews believes this openness creates “an aggregate good.”
Psychiatrist Elia Abi-Jaoude elucidates this perspective well. Abi-Jaoude lectures and writes critically on misrepresentation and deception in psychiatry, and also works with suicidal adolescents at a Toronto hospital. He feels honesty and disclosure help build therapeutic alliance.
“I disclose limits to confidentiality upfront routinely,” he says. Some youth might become more careful in how they speak, says Abi-Jaoude, but it mitigates against the betrayal they could feel if he does at some point feel compelled to detain them. “I think it gives them some agency, and engages them in a more collaborative way. The goal is to maintain honesty and trust, now and into the future.”
For the same reasons, Abi-Jaoude believes the impacts of call-tracing should be studied and openly discussed. “We should find ways to acknowledge, validate, and support these people who say they feel betrayed and traumatized. They should be interviewed and their experiences learned from. What happened? How come there was this miscalculation? How can we learn from this?”
Considering such perspectives, I ask Andrews: Why doesn’t AAS change its policy?
“Should all crisis centers that are accredited by AAS have a disclosure that, in fact, the police could be called?” Andrews repeats back. After a pause, he says, “It’s a fair question… That’s something that AAS as an agency needs to discuss and get input on.”
But Draper’s paper hints at backroom politicking heading in the opposite direction: “While two [New York] Samaritans centers in the network had historically resisted active rescue on philosophical grounds, they too agreed to adopt the Lifeline [Imminent Risk] Policy,” the paper states, explaining that Samaritans finally understood “compelling research.”
Samaritans characterize what happened differently. And they warn that the Vibrant/NSPL mission could ultimately reshape how all crisis lines across America operate.
A National Threat to Confidentiality
The New York Samaritans advertise that their hotline is “completely confidential” and, “unlike some other hotline services,” they never conduct “any form of call-tracing.”
Director Alan Ross says he understands the motives of call-tracing, but some people want absolute anonymity no matter what. “You need diverse forms of access to reach the majority of people. And the greatest gap is confidentiality. People are hesitant to seek help, because they’re scared. They don’t want people to know their business, or they’re ashamed.”
Ross points to a person questioning their sexuality or gender, an illegal immigrant, a politician, a parent in a custody battle, and many others who might be seeking help in sensitive circumstances. “I can come up with one hundred reasons why you wouldn’t want to take a chance of someone being able to identify you.”
But many Samaritans crisis lines have moved away from protecting people’s privacy and autonomy. “In New York City, we’re the dinosaur,” says Ross. “We’re the last bastion of what were the original practices and principles.”
Ross was a formal adviser to the NSPL’s development 20 years ago. He says it was a diverse collection of community-based centers collaborating to create round-the-clock support—call-tracing wasn’t required. Several years in, though, the Mental Health Association of New York, now Vibrant Emotional Health, won the SAMHSA bid to assume control of the NSPL.
At the same time, there was an expanding psychiatric-industry movement to recast suicidal feelings as symptoms of mental illnesses requiring treatment. SAMHSA, the American Association of Suicidology, and Vibrant/NSPL began to push call-tracing and hospitalization.
While the NSPL today includes 170 centers, Ross estimates there are 600 other hotlines serving communities around America, many of which don’t trace calls. Yet when the federal hotline legislation is implemented, all 988 calls—and the associated state tax funding built into the legislation—are slated to go solely to NSPL centers.
“But there are advocates in the public health community who believe that all hotlines should be included,” says Ross. “This is one of the things that sticks in the craw of those of us who run independent community hotlines. The NSPL gets all the marketing, all the promotion, all the funding. And now that they’ve created this three-digit number, it appears that things will only get worse; the NSPL could have a perfect monopoly.”
“It’s frustrating,” Ross adds. “The people who are running the national hotline have not, and you can quote me on this, have not gone, ‘How can we engage and support the hundreds of hotlines that are operating in communities around the country?’ Their focus is solidifying their network, their funding, and public policy around it.”
Indeed, during federal 988 hearings, forcible interventions on callers were promoted as “life-saving,” while Vibrant/NSPL, SAMHSA, and AAS apparently never told legislators about the scientific unreliability of risk assessments, large numbers of callers whose lives have been upended after their calls were traced, or how hospitalizations and treatments may be making people more suicidal rather than less so.
So why have any Samaritans gone along?
Ron White, Chief Program Officer for Boston Samaritans, says his center originally joined the NSPL to be part of national research, best practices development, and funding access. Their center didn’t trace calls. But around 2012, says White, “The NSPL finally, kind of, if you will, drew a line in the sand that said, ‘if you want to be a member of this network, you need to adopt our intervention policies.’”
Boston Samaritans now disclose the policy on their website. They disclose directly to some callers, too, particularly if they ask about call-tracing—which regularly happens, says White.
Does he believe 988 implementation could put more pressure on other independent crisis lines around the country to join the NSPL and, if they don’t currently, start tracing calls? “The more people are aware of 988, the less likely they are to call non-Lifeline centers,” says White. “And if 988 comes with funding, I think these small nonprofit centers are going to take a hard look at that.”
Building Relationships Instead of Tracing Calls
After researching Rational Suicide, Irrational Laws, lawyer Susan Stefan calls it “unforgivable” that some suicide lines don’t disclose that they trace calls. “It’s so traumatizing to be trustingly talking to somebody and all of a sudden have the cops show up.”

Many hotline operators express fears about legal liability, but Stefan says courts usually don’t consider the situation as similar to close doctor-patient relationships. She says her research suggested that to date it’s been “extraordinarily rare” for hotline volunteers or staff to be successfully sued for a caller’s suicide.
Stefan describes call-tracing as a “short-sighted” policy, especially since many people she interviewed said they’d never again feel safe calling. “Rather than ‘stop people from killing themselves,’ I think we need to rephrase the goal, and have it be ‘reduce people’s suffering and help them achieve a life they want to live.’”
Stefan points to an Air Force anti-suicide program that was ground-breakingly successful. The emphasis was less on intervening at the crisis point, and more on helping people with practical daily challenges and marital, financial, or other problems that might lead to suicidal feelings.
Stefan also praises Western Mass Recovery Learning Community’s “Alternatives to Suicide” trainings that help people become better at talking with each other, and its peer-run hotline that never traces calls.
Generally, peer-run hotlines appear to be less likely to have a policy of tracing calls—but RLC director Sera Davidow says even that is unfortunately not guaranteed. “In my experience, all that they accomplish [by tracing calls and forcibly hospitalizing people] is to continue to send this message that whatever you’re struggling with, the things that have happened to you, are so dark and so terrible that nobody can handle hearing about them.” By contrast, “The whole ‘Alternatives to Suicide’ approach is rooted in this idea that if we make the taboo topics okay to talk about, then people often don’t end up getting stuck in them.”
Davidow asks which route ultimately leads society to more loss: “Is it the path where everyone is so terrified to talk about suicide because of consequences, like having the cops called on you even by confidential hotlines? Or is it the path where we know that we’re going to lose people, and we create as much space as we possibly can to be with people in darkness and talk openly about this and support people?”
Indeed, the trend towards promoting the suicide line may simply be reinforcing our hyper-individualistic culture while downplaying our shared, worsening social-environmental circumstances that increase collective suicidality. Many suggest so, and Wildhood with particular pointedness. Wildhood says that, due to her autism, she’s had to teach herself how to build “connection,” and she now believes everyone could benefit from some re-learning.
“We are all so disconnected from the people actually in our lives that we feel safer talking to a stranger,” says Wildhood. “If you don’t want people to be alone, you show up.”
****
More documents obtained from SAMHSA through freedom of information processes are available for downloading on Rob Wipond’s website.
For updates to this story, see:
Roll-out of 988 Threatens Anonymity of Crisis Hotlines
Government Forum Reveals 988 Call Tracing Remains a Threat
Psychiatric Detentions Rise 120% in First Year of 988
****
MIA Reports are supported, in part, by a grant from the Open Society Foundations.



Thanks Rob.
Excellent helpful article, which I hope a lot of young people read.
It is called false advertising and it’s like dangling a carrot in front of a horse.
It’s really like a trap.
People should be read their rights ON the phone before they open up.
Because virtually your chat about suicide will be seen and treated like a crime, even
though it never was nor is now, a crime. And if you get scared when cops come, you could get
shot and if you did not get shot with a bullet, you will get shot with a drug. Or you will most likely
get a suicidal drug prescribed.
Hopefully articles like this will teach young people to try and form networks. The young should run from
professionals. Start demanding your rights. If you need to talk to someone, talk to someone that won’t arrest you for thinking, talk to someone that won’t drug you.
Talk to anyone that has your best interest at heart. The professionals only have a pretend liability.
Report comment
This couldn’t be more clearly about money. Yet another consequence of everyone needing to find “work”… Nobody cares if someone they don’t know might kill themselves.
Really, are there actually people out there who think that professionals care about all these people that they don’t even know? This is human trafficking (and forced drugging) for money.
Report comment
Society will spend tens of thousands of dollars jailing and drugging someone to try to prevent them from committing suicide yet when it comes to spending even less providing someone with food, healthcare and shelter it is called evil communism destroying the nation. Someone getting $800 a month for disability gets insulted as a drain on society but anyone saying spending $1,000 a month on addicting deadly psych drugs with zero benefits is bad is called a crazy cultist. Society is painted in cognitive dissonance.
Report comment
“We hospitalize people at risk of suicide, even though we don’t have any evidence that hospitalizing them is particularly helpful.”
So how about you don’t do that? It’s not that hard not to do.
Maybe you should teach your operators about the reality of it. Out of a 100 persons they want to call the cops on 1 will commit suicide anyway, 1 will be saved, 1 will be driven into suicide by the very measure that’s supposed to help them, 96 would have not commited suicide anyway, but you will traumatize at least half of them, and if you’re in the US 1 will get killed by cops or nurses.
If any of your operators still want to call the cops after that, fire them. They are clearly sadistic pos.
Report comment
Because they have got to do something. They can’t live with their guilt unless they do something. Doesn’t matter if what they do hurts people and makes life worse. They did something and therefore can wash away any sense of responsibility or empathy. They can pretend they helped someone and are good people and therefore don’t need to change.
Report comment
“They did something and therefore can wash away any sense of responsibility or empathy. They can pretend they helped someone and are good people and therefore don’t need to change.”
This.
Report comment
This is honestly what annoys me, though. THEY force people to sacrifice THeMSELVESS in order to assist them with THEIR feelings.
It isn’t the only instance of mental health workers brazenly admitting to the fact that their mental health is routinely prioritized over that of the patient coming to them for…mental health disturbances.
Report comment
Yes the alleged “help” appears to be self-serving. And the harm always gets buried.
And then there is this that at least saw the light of day:
https://www.cbc.ca/news/canada/calgary/albeta-fix-mental-health-act-1.5217203
Report comment
Hurray for Marina Glacomin, hope she keeps it up. And a HUGE hurrah for Judge Eidsvik.
And a thumbs down for the “media relations dept” Don Stewart. We all know where his income comes from. He is NOT there for the client.
And the “checklist” is a smokescreen.
Nevertheless, there will be more cases and there will be more judges who are not afraid to bring justice about.
The fucks of psychiatry were holding someone in jail for not having committed a crime. And the fucks were drugging a non criminal, to support their own habit. We really have to take the drugs away from these clowns that pretend to be doctors.
I really hope Eidsvik takes it further and checks out Robert Whitakers book. It will help her a lot in the long haul, to recognize that we are NOT dealing with “medications”
Report comment
From my experience volunteering with Crisis Text Line for two years, it was the administrators who required the workers to escalate texts to include a supervisor if there were suicidal thoughts. I rarely did this, as I did not agree with the policy. It’s not about the folks working the lines so much as the folks running the program living in fear of litigation (IMHO). Businesses are so fearful of litigation, they feel it’s worthwhile to sacrifice other human beings to protect themselves. I no longer am willing to participate in the crisis hotline industry.
Report comment
Morning,
That’s why activism for rights of people with mental illness should focus on judges and lawmakers. They need to be able to make informed dicisions instead of being entranced by psychiatries propaganda.
Report comment
This is why I am an advocate of changing the litigation. People should be as free to sue over abuses of their civil rights as they are if your employee told my actively suicidal sister to go hang herself.
There are laws on the books. The only successful cases of litigation that I have seen regarding suicide are where the practitioner was an obvious retard about it. Like, someone comes to the Er begging for admission because of command hallucinations ordering him to kill himself and not being admitted level stupid.
Report comment
It’s frightening what these people have been through. Why does asking for emotional support need to be attached to the police? These things should be separated. Life is hard and we all need someone to talk to without the risk of being overpowered or losing a job. Really great work of getting people’s voices out and highlighting the systemic issues.
Report comment
“Why does asking for emotional support need to be attached to the police?”
Hold on tight, we have a pseudo-socialist government now. First things first; passing the legislation that Biden as VP wrote on his way out that trump then discarded; the one that would add people on disability for mental illness to a federal registry to be denied firearm sales.
States are re-opening or opening “mental hospitals”, the atrocity is coming.
AOT is growing and law enforcement is all in; Biden said he wants a “psychiatrist in every cop car!”
It was bound to happen. The idea that lead to deinstitutionalization was that these were ordinary people with problems that deserved equal rights. Now they are genetically flawed and inferior brain disorders mucking up society.
Be ready for hell.
Report comment
We are heading for some serious totalitarianism, that’s for sure.
I agree also that we are heading for a pseudo-socialist government, but I think we mean that in different ways. Because I believe we NEED a socialist government, but a REAL one — not the so-called “democratic socialism” pushed by academic self-defined “radicals” (who are actually “woke” liberals, not true socialists). Republicans play into this by absurdly referring to the likes of such capitalist predators as the Clintons as “socialists.” What I see in the near future is a growing totalitarianism that is presented as “socialism” but is far from anything Marx, Lenin, Mao or Fidel ever had in mind. This in turn will need to be overthrown, in a true revolution, not a “virtual” one.
Report comment
No, I think we mean it in a similar way, at least. Biden and co. are schills for big business, with global interests.
Report comment
OK, cool. Wasn’t sure if you were using “socialism” as a positive (as I do) or negative (as some do).
Report comment
Mental illness does not mean violence towards others or one’s self – it is interesting to see how people are conditioned to this over-simplification and “shoot their own interests in the foot” because someone has convinced them of a danger that just isn’t borne out of the facts.
The Biden legislation is bad legislation. It completely ignores risk factors and provides a police state solution motivated by profit and control. It completely ignores environmental factors (an accusation we usually apply to a particular field of medicine). Ignores links between violence and poverty, militarism and disregards routine police shootings.
I don’t like guns, most of the people I know don’t have them, some do, some enjoy target practice. The debate has little to do with guns themselves and everything to do with power.
Biden signed off on the transformation of the United States into a police state. Guns are one issue, mental health is another. The same iron fist approach has only become more convenient.
But let’s be more honest about politics? No one with a so-called mental health problem (who doesn’t have a symptom these days) should have a thoughtless favorable view of any ruling authority – we see the destruction on a daily basis.
nb – When you post on Mad In America – you have no confidentiality or expectation of privacy. Moreover you have little understanding of how your comments are used or who sees them.
I’ll end here.
Report comment
Why would he need a list for the “SMI”? Last I heard Biden wanted to abolish the second amendment and remove all guns. Rendering such a list superfluous.
Report comment
Not sure where you heard that, but it sounds pretty outlandish. No one is advocating to abolish the second amendment that I’ve heard of, and even if they did, there is NO way 2/3 of the States would support it. Biden can’t change amendments even if he wanted to. I don’t think it’s something to worry about.
Report comment
“Why does asking for emotional support”
The person is not asking for emotional support , the person is threatening to hurt or kill someone. If the police are aware of someone threatening to hurt or kill someone their job is to intervene.
The dark comedy is when the police arrive to help, very often the kill the person they are supposed to protect/serve/save.
Don’t threaten to hurt or kill anyone and you wont get into trouble.
Report comment
Like a Gilbert and Sullivan opera where a young man is scheduled for execution as the penalty for threatening suicide.
Report comment
Thank you for this important and informative article. I have never called a suicide hotline, but I have a friend who has. She said, “It was a joke.”
Personally, I find Confession to be a better alternative to confessing things to mental health professionals now that I know better. There are sometimes priests who abuse their power and use your vulnerability to emotionally abuse you, but there are good ones too.
More importantly, priests are bound by the seal of confession. They aren’t allowed to tell anyone anything you say, or even tell anyone that you went to confession. If they do, they will be excommunicated. Priests are very well provided for, but an older priest would probably have an impossible time establishing a new career. This helps with the power imbalance of spilling your guts to a stranger. If only it were so easy to get mental health professionals fired. I’ll bet they would shape up if they knew that ruining people would cost them everything.
Report comment
In the religion of psychiatry they write down the persons confession, so it can never be forgotten. Will the confession be forgiven? If you worship and consume the holy molecules of science, (medication compliant) you will be forgiven.
Report comment
If a priest thinks your confession warrants kidnapping you, locking you up for days/weeks/months and plying you with psychological torture including the pharmaceutical variety he will go to prison. A shrink will be handsomely rewarded.
Report comment
No kidding!! Great point!
Report comment
In reading about the change that will occur within the Federal Communications Commission with the language of “light touch”, and being that the telephone is conveyed to be the image of choice by which one troubled with the idea of suicide, then at what point, does the heavy touch, the wrong routing of the neural networks having agency to invade the space on is living in? There seems to be room by which a legal intervention might intercede in the behalf of those who share these stories where “suicide hotlines” operate.
Report comment
Superb work, Rob. What an obscene world we live in, where “helping” people is an industry, or rather a conglomeration of industries, and people in distress have to reach out to paid “helpers” because they have no one in their lives they can talk to – and then are likely to get incarcerated and forcibly drugged, likely for the rest of their lives, with neurotoxins which, even when they don’t directly lead to chemically-induced “suicidal ideation,” are likely to cause early death, even aside from wrecking people’s lives.
Report comment
At what point, then Irit, can the individual or the community say that murder is occurring, directly or indirectly? For if our lives are being shortened, or even terminated, where are the ethics that show problems with the rule of the law being ignored or the scales are being tilted by the money? the promise of monies through PACS? Bullying poised as Leadership? What sort of Justice can we expect in terms of 1), 2) 3)…..
Tks,
Bill
Report comment
Well said Irit. It is the “conglomeration” that is the obscenity.
How it really matters not who one calls, it all winds up in the same place.
And how that place is no help at all, yet it began by calling a “help line”.
Friends and family regularly encourage these calls, because it seems
that emotionally we have become unable to be there for our fellow men.
Report comment
I reach out to someone by phone every day.
Report comment
I thought I’d throw this into the mix here as well (note that they quote NAMI as “experts” and provide a suicide hotline #):
SAN JOAQUIN COUNTY, Calif. —
A student has died after a self-inflicted gunshot wound during a Zoom distance learning class Wednesday, officials said. The San Joaquin County Sheriff’s Office announced the student was an 11-year-old.
https://www.kcra.com/article/san-joaquin-county-student-shot-during-zoom-distance-learning/34851597
Report comment
Once again neglecting the important question of why a sweet, even tempered young man would kill himself in the context of his school experience. (Not to mention where he got the shotgun.)
Report comment
Thank you Rob for this timely and very important report. Of great concern is how there always seems to be such an aversion to honesty in the mental health services, especially in psychiatry. With the ever expanding goal of psychiatry to label all distress or suicidal feelings as a “mental disorder” requiring psychiatric “diagnoses” and toxic drugs, it poses grave concern for people to easily end up in the clutches of psychiatry simply because they phoned a “help” line and were deceived about confidentiality or call tracing. Honesty is the best policy as the added trauma for someone having their trust breached in this manner will not bode well for anyone who hoped to get “help”.
Report comment
Thank you, Rob, for this well researched and very informative article. I think the message to walk away with is don’t call suicide hotlines. Although we can also say, it’s never wise to speak to any “mental health” worker ever, too.
I know my psychologist was absolutely obsessed with suicide, despite the fact I merely went in to her, to figure out why I was getting ‘brain zaps.’ Good thing the patients figured out that ‘brain zaps’ are a common symptom of antidepressant discontinuation syndrome, prior to the “mental health professionals” figuring this out (sarcasm).
https://www.researchgate.net/publication/247806326_'Brain_shivers'_From_chat_room_to_clinic
“Wildhood says the training was two half-days,” and two half days of training qualifies one as a “mental health professional” today?
Report comment
Am I the only one here who has to take a break from MadInAmerica every now and then because the stuff here is too painful to read? People express so much pain here in so many different forms that you need to take a breather to realise and truly feel that there’s more to life than Psychiatry.
Report comment
No you’re not the only one. But I knew that when I stepped in. Now I just need a hand out. 🙂
Report comment
you need to take a breather to realise and truly feel that there’s more to life than Psychiatry.
Yes — there’s Anti-Psychiatry! 🙂 Hopefully before long I’ll be able to direct you to such a site.
Report comment
I hear you registeredforthissite and agree it is painful to read how psychiatry has dehumanized, harmed or killed so many but on the other hand the Mad in America site has been SO informative, validating and empowering it has been a life saver for me. I make a point to donate to causes that are about exposing injustices, inhumanities and speaking truth to power to protect vulnerable people and MIA is at the top of my list. My brother didn’t survive being drugged by psychiatry (for being sad his marriage ended and kids moved away with his ex) and I was snared by the corrupt practices of psychiatry because I developed chemo-induced insomnia during cancer Tx so when I found MIA it was validating to learn I was not alone trying to cope with the harm psychiatry does to so many unsuspecting people. There is strength in numbers so I am very grateful to anyone who shares their painful story even though it is heart breaking and difficult to read. However we each must do whatever is best for ourselves and our healing journey whenever processing difficult information. Take care and best wishes.
Report comment
Would a class action be appropriate? If people calling the American Heart Association were reported to the police there would be hell to pay. Ditto for cancer. This is a huge violation of privacy and it’s dihonest, it’s a deceptive practice and our lives our in the balance. I texted, after veriftying it was confidential, police came banging on my door for more than 20 minutes. Humiliated, angry and suicidal. That’s what they did. I think we should all launch a huge lawsuit.
Report comment
This post raises crucial questions about the balance between confidentiality and safety in crisis situations. It’s disheartening to think that the very lifelines intended to help could inadvertently compromise our privacy. I hope more discussions around this topic lead to policies that prioritize both mental health support and the confidentiality of those seeking help. Thank you for shedding light on such an important issue!
Report comment
So it’s another trap from a psychotic, fascist regime of moral crusaders who actively don’t want you to live, but won’t let you die.
And they wonder why spree shooters exist.
They only want warm bodies to exploit.
This just nails both the figurative and literal coffins. I’m dying within the fucking hour.
Report comment
This post raises an important issue about the trust and transparency of suicide hotlines. It’s alarming to think that calls may not be as confidential as advertised. People in crisis need to be assured that their privacy is protected so they can seek help without fear. Thank you for shedding light on this critical topic!
Report comment
This is a really important topic that often goes overlooked. It’s concerning to hear that some hotlines may not be as confidential as they claim. People reach out for help during some of their darkest moments, and the last thing they need is a breach of privacy. Transparency and trust are crucial in mental health support. Thank you for shedding light on this issue!
Report comment