
In a recent post, Robert Whitaker asked us to consider the psychiatrist’s dilemma:
“Patients were told they suffered from a chemical imbalance in the brain, the public understood that was true, and all the while academic psychiatrists—and APA leaders—knew that it wasn’t. This obviously presented psychiatrists with a ‘cognitive dissonance’ moment: how could they reconcile those facts with their own self-image as medical doctors who treat their patients well, and in an ethical manner?”
In this regard, I began to wonder if the facts are really so problematic for doctors. Let’s consider the situation from the perspective of an ethical and rational psychiatrist.
 First: The Way the Brain Works Is a Mystery
First: The Way the Brain Works Is a Mystery
Most knowledgeable folks, psychiatrists included, agree that we have only a very crude understanding of how the human brain produces our mental and emotional experience. So even if the serotonin theory of depression is debunked, that doesn’t necessarily invalidate drug treatment. It just makes it a mystery about how the drugs work. There are many (most?) prescription drugs for which the mechanism by which they produce their impact is unknown or merely hypothesized.
And telling stories they know are or may be untrue has become standard practice in psychiatry. After all, we are dealing with mentally impaired patients; we know better than they what is best for them. Telling them, for example, that antipsychotics are “like insulin for diabetes” is justified by the false belief that the drugs are highly effective, necessary, and safe. Thus, psychiatrists feel justified in focusing their efforts on getting patients to take their medications.
Once you have such a conviction, it is a small step to set aside the need to provide truly informed consent, especially when you have technical training and expertise unavailable to lay persons. Furthermore, there is a frequently unexplored assumption that patients suffering from “mental illness” are incapable of using reasonable judgment regarding their care. So, even if you are just telling a story and you happen to be one of the psychiatrists who knows the story is untrue, there may not be a great deal of painful dissonance. And, in my experience, it is simply a fact that many medical doctors, including psychiatrists, still don’t know that the “correcting chemical imbalances” story is untrue.
Second: They Are Not Just Prescribers; They’re Users
A personal experience suggested to me that the “better living through chemistry” philosophy may be more than an approach to the treatment of others; it may be far along in the process of becoming a belief system—a way of life among mental health clinicians.
More than 20 years ago when I was the primary source of income for my wife and two young sons, I applied for a million-dollar life insurance policy. The insurance company sent a phlebotomist to my home. After I came out of my bathroom, she also measured the temperature of the urine sample I had just provided; for them to bet a million dollars that I wouldn’t die, they wanted to be sure they were getting blood and urine samples from the actual applicant. Then, after having my blood drawn and answering detailed questions regarding my medical history, I was required to sign numerous forms allowing the insurance company to collect verifying information from just about anybody I had ever known. There was no sense trying to hide anything in my medical history as I was giving them permission to check with everyone who had ever treated me. So, like most such life insurance applicants, I told the truth.
When we were done, as she was leaving, she mentioned that I was the first of the psychiatrists or psychologists she had interviewed who was not taking an antidepressant and/or Ritalin. She said she was repeatedly surprised to find that many were using both simultaneously!
I was stunned. The first! You have to realize that her service area was Newton, Massachusetts. In Newton, there is a zoning law that requires at least one psychologist or psychiatrist on every block. (Seriously, there are a lot of us in Newton.) I asked her to sit down for just a minute while I asked questions to verify her offhand comment. She had been doing this for years. She had been somewhat surprised when she first started to learn about this unbroken pattern. And she was then genuinely surprised that day to come across a psychologist who wasn’t taking an antidepressant, a stimulant, or both.
I immediately realized that there would be no way to get information like this from a research survey. Anonymous surveys might, at best, get a 10% response rate that would be biased by the characteristics of those who were willing to report their drug usage. This data was research gold. Based on just this sample, we can be statistically certain that probably over 90% (but definitely over 80%) of those mental health clinicians applying for life insurance are taking an antidepressant, a stimulant, or both! And while life insurance applicants may not be a random sample, we know from actuarial statistics that they are not all that different from the general population. In fact, the whole purpose of interviewing and getting information releases is done to ensure that the applicant is not likely to be an outlier whose risk of death is outside of the norm.
Fuller disclosure
By the way, for full disclosure, about seven years earlier in an attempt to save my first marriage, I obtained a six-month supply of fluoxetine (Prozac) from my primary care provider. And it almost worked. I was less reactive and easier to get along with. Unfortunately, the problems in my marriage had become deeply ingrained and were not just due to my reactivity; the changes were too little too late.
In any case, one day during this time I went to the gym. As I was walking in, I noticed that my mouth was quite dry and I was very thirsty, which I recognized as a common side effect. Then I was startled as I realized that, despite my thirst, I had walked by the water fountain without noticing it. For me, Prozac wasn’t an “antidepressant.” Rather; it made me less reactive, slightly less sensitive to impinging sensations whether they were thirst, hunger (they were originally going to market Prozac as a diet drug), sexual arousal (it made having an orgasm markedly more difficult), or emotional states. Being less sensitive to one’s feelings can be experienced as either “emotionally deadening” (a commonly reported side effect of the antidepressants) or as a relief from chronically painful ruminations.
By the way, the reason these drugs weren’t marketed for weight reduction is that there is a tendency for the body to adjust to their effects; the appetite reducing effect would then go away and weight would not only revert back, but frequently there is unwanted weight gain. You could then up the dosage but the process would be repeated. Eventually, one would be on a fairly high dose and when the body again adjusted you couldn’t increase it further. Now you’d have a person whose body was accustomed to the presence of a high dose of a drug that had none of the intended effect and plenty of adverse side effects. Withdrawal, however, would often leave the drug-adjusted body without the chemical it had adjusted to, which then produced another set of problematic effects. Though this scenario was not actualized with the drugs as diet pills, this is precisely what we now often see after those same chemicals were marketed as antidepressants.
Third: We Have Evidence of Significant Improvement
As noted, for some people, being less reactive to unpleasant thoughts and feelings might very well be a relief. In a recent meta-analysis of the drug trials submitted by the pharmaceutical companies to the FDA, a small proportion of folks who took an antidepressant did appear to experience a clinically significant decrease in the standard depression score used in research studies. About 10% of those taking a placebo experienced this improvement vs 25% of those taking an antidepressant, yielding an improvement over placebo that appears to actually be due to the drug in about one in seven patients (15%).
Given my experience, I believe that the mechanism of additional relief over the placebo effect for those folks with a significant decrease in depression scores may have been the reduction in their reactivity to their worries and concerns. 15% of those in the drug trials may have benefited from reactivity reduction that doubled the average decrease in depression scores produced by placebos alone. (A more detailed discussion of the meta-analysis is presented here.)
It is important to note that the majority of private practice psychiatrists and primary care providers who prescribe most of the antidepressants aren’t working in clinical psychiatric settings of the kind where the research was carried out. Like my case, many people who are prescribed antidepressants don’t present themselves at clinics seeking relief from depression. I was worried and very unhappy about my situation (my failing marriage), and often angry.
I may have been a member of a population with unease that is likely to resolve itself; throughout human history, most people recovered from painful losses and other temporary stresses without medication. This population is probably underrepresented among truly depressed patients who seek help specifically for depression in psychiatric clinics and is probably overrepresented in the practices of those physicians who prescribe most of the antidepressants. Thus, the real-world experience of many prescribers may not match the reality found in the clinical studies: The drugs don’t work for the majority of depressed people who have long standing depression, especially when their depression is a response, as it often is, to overwhelming problems.
A colleague of mine consulted with a medical service run by a university medical school in a large city in an extremely poor black neighborhood rife with social problems. She told me that when she asked the department chair about the effectiveness of drugs, “He just sort of shrugged and said, ‘The people we see have shitty lives. No drug is going to fix that.’”
In contrast, reducing reactivity in those who are just going through a temporarily stressful period may make the drugs appear to the prescribers to be more effective than they are for those who suffer from true clinical depression. And though reactivity reduction may be helpful at times, it has its down side.
Regarding the latter, back in 2004 shortly before Loren Mosher died, I did a video interview with him and Bob Whitaker. Loren told us that this decrease in reactivity to internal concerns appears to be the mechanism by which an increase in suicide and lethal violence is produced in a small percentage of young folks taking antidepressants. Adolescence is a time of turmoil. During turmoil, turning down one’s inhibiting thoughts and feelings can be dangerous. And as of today, we have no way of identifying the 15% who may get significant relief from these drugs from the 85% who don’t, some of whom will suffer the negative and sometimes tragic effects of these medications.
The Limits of the Prescriber’s Perspective
Analyses of the clinical trials of antidepressants have found that there is only a very slight difference in symptom reduction between the antidepressant and placebo groups. However, the prescribing physician never sees the similarity between drug and placebo responses. Having no comparison group in their clinical practice, the prescriber will naturally attribute all of the improvement to the drug.
Based on the recent meta-analysis, the clinician is likely to see that, on average, their drug-treated patients have some modest symptom reduction, which in the FDA trials was a 10-point decrease on the Hamilton Depression Scale. They will attribute all of that improvement to the drug, forgetting the placebo response altogether. They won’t be seeing that in those same trials the average placebo patient improved by 8-points. Two points is a negligible, clinically insignificant difference on this 52-point scale.
In short, the clinicians have no access to the perspective and understanding that comes from comparing drug response to placebo response.
Furthermore, patients without any improvement along with those who experience significant adverse reactions are more likely to stop taking medication and drop out of treatment; not needing follow-ups for refills, they are simply less likely to continue to see the prescriber. This means that those without improvement and those whose experience is negative will be less visible. So, for the prescriber, the picture is of prescribing and getting generally positive results. When patients with negative results do continue in treatment, then “that’s the disease coming back” or we are dealing with “treatment resistant depression,” a label, which, in one study of real life patients, was given to 41% of long-term patients.
Thus, most psychiatrists have treated people with antidepressants and seen improvements, with negative impacts being less visible to them. Of course, the research shows us that the good results are seen in a fairly small minority of patients and are due in large part to the very real and significant placebo effect and the natural tendency for depression to remit. But how are psychiatrists supposed to know the cause of the improvement based on their direct experience? They prescribe. On average, patients get better; sometimes dramatically so. As David Hume noted in A Treatise of Human Nature:
“A CAUSE is an object precedent and contiguous to another, and so united with it that the idea of the one determines the mind to form the idea of the other, and the impression of the one to form a more lively idea of the other.”
Indeed, the function of research is to differentiate between what seems to be causal in our limited experience composed of sequential, contiguous events, from what is really operating in a causal manner (though Hume might insist that all we ever have are mental impressions of contiguous events and we then just call the precedents “causes”).
Yet, even if psychiatrists read the actual research to get a better grasp on the meaning of their limited personal experience, they would see that the evidence seems to indicate that, in addition to the small group for whom the drugs appear to double the average placebo effect, there may be some real improvement among the very severely depressed over placebo, though a recent study casts doubt on this and suggests that the severely depressed may benefit the least. Less uncertain, they would learn that placebos clearly show some limited improvement (the average eight-point reduction in depression scores). So, the evidence shows that antidepressants are drugs that may help the very severely depressed (a little), about one in seven a significant amount, and they also provide all the (real) benefit of taking a placebo.
And in Short Term Use They Are Relatively Safe
If we were to try to hold psychiatrists responsible for the small but real increase in the risk of violence and suicide and other unpleasant side effects that antidepressants cause, we must keep in mind that many medications that medical doctors routinely prescribe can cause extreme damage (often even referred to as “death” in the warnings included in today’s endless TV ads for drugs). And the long term poor outcomes (see Rush, et al. and Piggott, et al.) for those on antidepressants are not readily apparent in practice since so many intervening, real life events seem to be responsible for the ups and downs experienced by long term patients. Additionally, as noted, a positive view of the medications is bolstered further by the fact that patients with adverse reactions are more likely to drop out of treatment making the negative effects less visible to the prescriber.
Back in 1995, a very large Consumer Reports survey showed that “patients benefitted very substantially from psychotherapy … and that psychotherapy alone did not differ in effectiveness from medication plus psychotherapy.” So, the benefit from therapy versus therapy plus medication was identical; on average, there was no additional benefit from adding medication to psychotherapy. If, as in the FDA drug trials, 15% of those in that survey sample who received antidepressants experienced a large improvement, then there must have been as much harm produced for the overall effect of drug vs no drug to have been the same. That is to say, if medication was significantly helpful in some cases, it must have been equally harmful in others in order for the presence and absence of antidepressants to have shown no statistical difference. However, since the medication plus therapy group tended to do as well as the therapy only group, all of whom on average “benefitted very substantially,” most of the medication patients in this study improved. Thus, even though, on average, the medication did not help and in some cases probably caused significant harm, the clinician’s overall experience was that their patients who took medication improved.
So, we need to remember that, in their training to be medical doctors, psychiatrists had to come to terms with the fact that interventions with real power to change things for the better will, on occasion, produce tragic results. (Which of course is what led Peter Parker’s uncle to warn Spider Man about the relationship between responsibility and power.) Before they even start their training to become psychiatrists, they will have had to come to terms with the fact that unavoidably negative outcomes will occur in the practice of medicine.
Then, having no experience actually treating mental disorders, in their psychiatric residencies, they turn for instruction to the experts in their field, which is largely focused on the administration of psychotropic medications. When they then compare what they were taught about how they can intervene helpfully with drugs with their actual experience, they appear to have a significant basis for accepting what they were told. In their clinical experience, (1) antidepressants appear to be helpful, (2) there is no direct experience of the lack of a significant clinical benefit over placebo that the drugs provide to most people, (3) there is little experience of the non-existent benefit and not infrequently negative experience of those who are not responsive to the placebo effect provided by taking medication (many of whom drop out of treatment), and (4) there is even less experience of the very serious harm the drugs can occasionally cause.
The Profound Power of the Pen, Personality, and Placebo
There is no question that the act of writing a prescription for an antidepressant often provides a foundation for a hopeful bond between a psychiatrist and a patient. And both — hope and human bonds — appear to be helpful when dealing with the inevitable pain of living.
Furthermore, we know that the impact of placebos can be greatly affected by their presentation. In this regard, consider that some psychiatrists (like some people in general) are very good at appearing confident and forming a caring bond, which together provide the essence of a supportive and hopeful relationship. This combination may, in turn, be essential in helping people recover from depression (with or without any form of “treatment”). And some psychiatrists (like some people in general) are quite inept at forging this type of relationship.
This variability must be considered in the context of the fact that the research shows little difference for the vast majority of folks experiencing depression between antidepressants and placebos. The advantage that the drugs may produce in many cases could be due to the fact that they simply function as psychoactive placebos, i.e., placebos that produce enough impact on patients’ experience to make it seem certain that they are taking a real medication and are not in the placebo arm of the research. The significant improvements then experienced by a small subset of patients may be in large part due to what happens when more personable therapists with strong, confident personalities prescribe a psychoactive placebo. If this is so, then the drugs are not directly more curative of depression than placebos; they just help create a stronger placebo effect.
In addition, I am claiming that some psychiatrists are very skilled at maximizing the (real and significant) placebo effect when they administer antidepressants (or other placebos). In addition to the actual relief some may experience from taking a drug that makes one less emotionally reactive, a bond with a convincing, charismatic therapist may accentuate the placebo aspect bringing total relief into the realm of significance for the 15%.
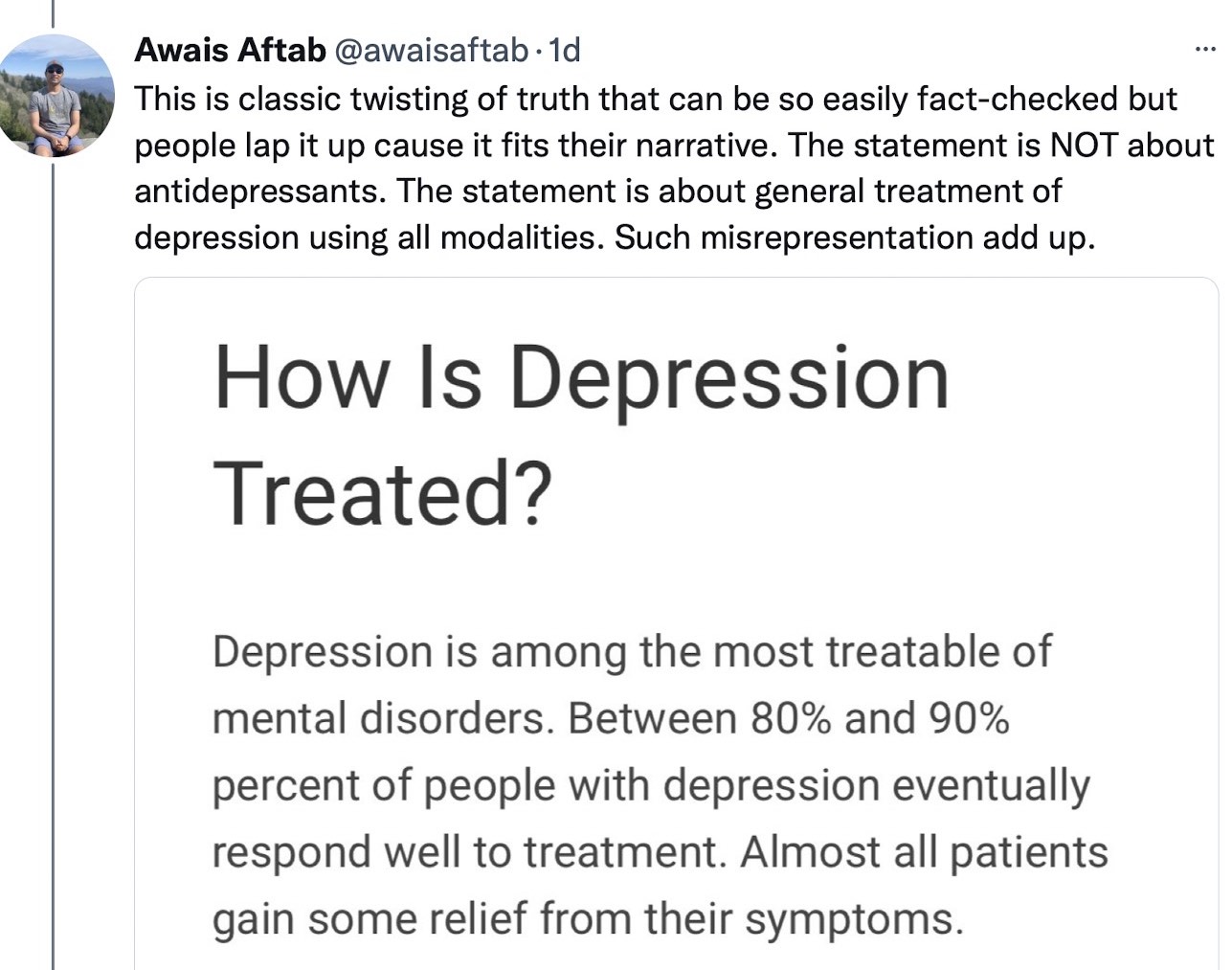
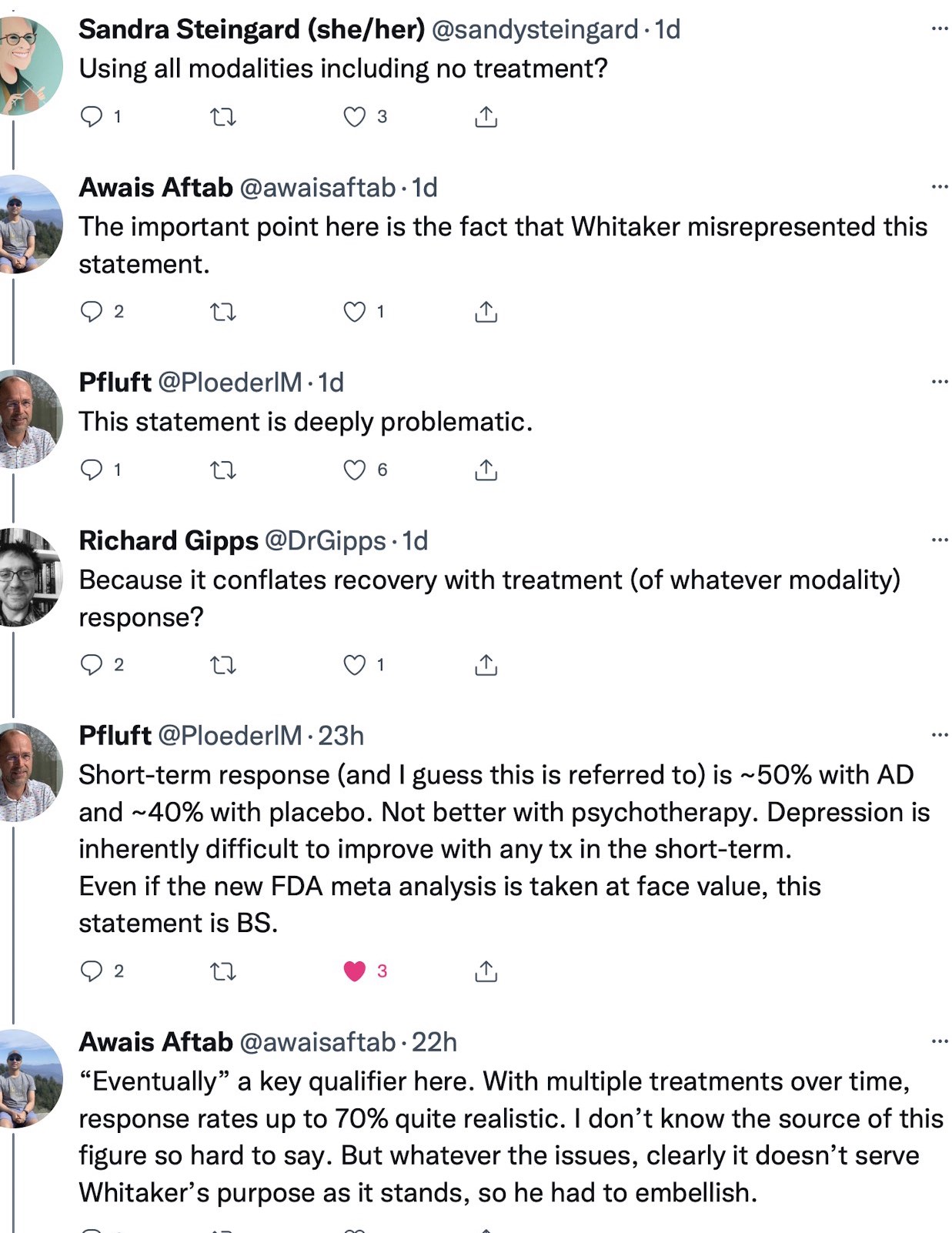
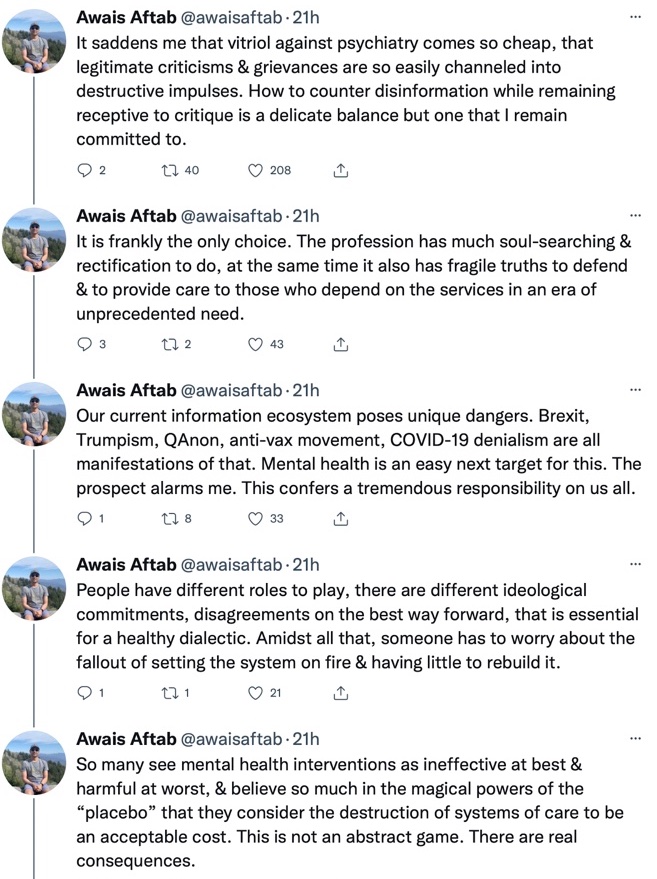
So, to recap: There appears to be a tendency for antidepressants to reduce emotional reactivity which for some people may include a significant decrease in distressing thoughts and feelings. We also know that the placebo effect is clearly beneficial for a significant number of those suffering from depression. Furthermore, it is likely that some psychiatrists are highly effective in forming a charismatic, caring bond that amplifies the placebo effect. Such psychiatrists then are likely to see higher rates of improvement in their patients than the average that is reported in the literature. These psychiatrists (and Aftab who accused Bob Whitaker of twisting the truth and misrepresentation and intentional embellishment may be one) then have a personal experience of improvements that are frequent enough to convince them that there is something of definite value in their prescribing practice.
This would be true even if antidepressants were nothing more than psychoactive placebos, even if they lose their reactivity reducing effect over time as the body adjusts to their presence, even if their overall impact is not infrequently negative, and even if, on rarer occasions, they are extremely harmful. The personal experience of some influential psychiatrists such as Aftab and Peter Kramer, may thus be skewed. After all, within psychiatry they are “influencers.” It may not be farfetched to suggest that such highly persuasive individuals have personal charisma that may generate higher rates of apparently curative placebo responses. And based on my life insurance “research,” there is a greater than 80% chance that Aftab and Kramer are users!
It’s a Religion
[F]orgive them, for they do not know what they are doing (Luke 23:34)
In this light, it is illuminating that rather than counterattacking him for dishonest discourse, Whitaker sees Aftab’s attempt to minimize his cognitive dissonance as just normal human behavior. While I agree, I would add that Aftab’s actual experience may provide a distorted picture that is markedly better than what the research indicates. This may help him hold on to a false picture of medication’s effectiveness. Somewhat less charitably, I think it might be more accurate to see Aftab as a beneficiary of his own delusions that, as Whitaker explains, are maintained to avoid painful cognitive dissonance but simultaneously also enhance self-esteem, and generate an excellent reputation along with a substantial income. In this regard, Aftab is functioning like some of the leaders in the type of movements he claimed to be defending us from (and to which he likened Bob Whitaker), i.e., Trumpism, QAnon, and Covid-19 denialism.
Because of this, one might be inclined to call “Pharmachiatry” a cult, not a religion. But when a religious belief system has gone mainstream, we stop calling the phenomenon a cult and we use the term religion. And modern psychiatry is certainly mainstream. Thus, we need to recognize what we are dealing with: It’s a religion. Yet, one might still object to using that term since there is no God in the Pharmachiatry dogma. That’s true. Yet, Buddhism is clearly a religion despite its lack of a deity. And every mainstream definition of religion includes something like “a cause, principle, or system of beliefs held to with ardor and faith” (Merriam-Webster).
If I am correct in claiming that faith in psychopharmacology functions psychologically like a religion, then direct attacks on its beliefs, even if those beliefs fly in the face of the evidence, are only likely to make its adherents double down. “Your supposed facts be damned! We know the truth! Whitaker is a dangerous heretic.”
Unfortunately, Bob Whitaker’s suggested solution — legal action — is likely to founder. Based on many years of testifying as an expert witness in court, it has become quite clear to me that the judges who control legal proceedings also tend to be true believers of the dominant religion.
Still, I have faith in the persistent stubbornness of reality. As Philip K. Dick (who had his own long struggles with psychotic paranoia) quipped, “Reality is that which, when you stop believing in it, doesn’t go away.” Thus, as discouraging as being a minority member of an iconoclast belief system can be, I believe that in the end the truth will prevail. And I believe it will prevail not only because it won’t go away, but also because there are folks like those at Mad in America who won’t let it be ignored.
Now, if only there were a psychoactive placebo that I could use to bolster that belief.











{kind=link}
{kind=link}
{kind=link}
So someone who is feeling depressed or anxious is considered mentally impaired? And telling untrue stories is standard practice in psychiatry? What hubris. I had to keep reading to see if you were actually serious. I found your defense of psychiatric drugs smug and self-serving.
“And telling stories they know are or may be untrue has become standard practice in psychiatry. After all, we are dealing with mentally impaired patients; we know better than they what is best for them.”
Report comment
“I found your defense of psychiatric drugs smug and self-serving.”
You’d have loved our ex Minister for Mental Health then Ann.
When asked about a report where nearly 50% of women who had been in mental hospitals claimed they had been sexually assaulted, she stated that “You can’t listen to them, they’re mental patients” (in the Hansards).
Quite a different response to allegations made in the Parliamentary environment though.
Report comment
Ann
I had to read the first part twice in order to be clear that Dan Kriegman was actually using those paragraphs as a way to expose the very crude, irrational, and self serving thought process of most psychiatrists.
Overall, this was a well written expose’ of the fraud and dysfunctional nature of the institution of psychiatry.
Richard
Report comment
Richard, thank you for pointing these out!
Report comment
I got that impression aw well.
Report comment
Where do people get this idea that mood altering chemicals are good for you? How far back does it go, and what did it start with.
To me it seems no different from the vast numbers of people who think ethanol and nicotine are good ways to make it through the day. And then as their numbers seem to be dropping, there are many more now who depend on marijuana, or even on crystal meth.
And as CA Governor Gavin Newsom has signed his Care Courts Psychiatric Police State Law, his people talk about using drugs to “stabilize” people. And most of those behind this really seem to believe that member of their own family would have benefited from this:
Sickening:
12 min video
https://www.kcra.com/article/gavin-newsom-to-sign-care-court-program-bill/41203085#
So how far back does it go, and with what did it start?
Joshua
Report comment
“Before they even start their training to become psychiatrists, they will have had to come to terms with the fact that unavoidably negative outcomes will occur in the practice of medicine.”
What I had one Prof. describe to me as not ‘having the stomach for it’? Or did he mean the more deliberate type of ‘accidents’ which tend to happen to people wandering around with proof of offending by public officers which the police conveniently refuse to take, and deny access to the protection of the law whilst ‘alternative arrangements’ are made by ‘doctor’? Conceal your crimes by making the victim an “Outpatient” then ‘negatively outcome’ them in the E.D.
Yes, my ‘paranoid delusions’ which were patently apparent once the documentation relating to my ‘referral’ had been “edited” and the fact that I had been ‘spiked’ with date rape drugs removed, and the problem of me not actually being an “Outpatient” when police were called for ‘assistance’ with the person who had a knife planted on them to cause an ‘acute stress reaction’ had magically disappeared.
Nothing like telling police that a mental patient with a knife needs to be restrained to get them on edge huh? And it is a really good way of getting people to open their mouths so you can put words into it. Nobody really concerned about the means to an end…… that is a chemcial kosh and years of forced treatments based on the sickness caused by the drugs, which cause the symptoms required to justify the forced treatment.
https://www.youtube.com/watch?v=oZ9UQKBUrsg
And further, that such “negative outcomes” can be arranged, and the State will enable ‘after the fact due process’ via document “editing” of legal narrative to occur to conceal any motive for harm, and ensure that no one is ever held accountable for anything…… even ‘intended, unintended negative outcomes’ (you can’t prove the motive, and have no way of making us talk, so police will not pursue the matter as it is not in the public interest….. or more correctly not in the interest of the people using the ‘outcoming’ service).
“A good end can not sanctify evil means [ie lying, even the noble type of lying such as ‘verballing’ See Plato], nor must we ever do evil, that good may come of it” W Penn. My addition in brackets
Your quote from Luke interesting if you consider the Islamic perspective on what he is talking about, and add a “tehe” to the end (Those silly Romans). And to quote another of the SciFi writers Robert Heinlein;
“When any government, or any church for that matter, undertakes to say to it’s subjects, This you may not read; This you must not see; This you are forbidden to know, the end result is tyranny and oppression no matter how holy the motives.”
It is good to see the authors ‘taking it up’ to some of the more blatant ‘zealots’ in the ‘industry’.
Report comment
Mind boggling, the degree to which psychiatrists rationalize and excuse fraudulent practices. “We have to lie about the drugs so patients will believe they’ll feel better”? I’m beginning to think I was never the crazy one. After three and a half decades of being told that and having my life destroyed, the people who did this to me are looking more and more unbalanced and out of touch with reality.
Report comment
If that is their plan, why don’t they just give people niacin pills, and say the flush is proof that it’s working? Why make billions for pharmaceutical companies with super expensive placebo pills? Sorry, that argument does not hold any water!
Report comment
This captures quite a bit of my thinking on it all, and is well written. As has been the case before, I wish some version of it were posted in the NYT, not just a MIA or similar.
I hold the same pessimism about Whitaker’s proposal for legal action, off-hand as it may have actually been. But I also think it’s necessary for any change.
I had a discussion with a psychiatrist recently w.r.t. a person he wanted to commit and drug. The circumstances – the person had been held for a long period of time following a complicated incident, and had never displayed a hint of psychiatric distress, but you wouldn’t make clear sense of that from the medical records – aren’t too important, except that this person was cogent and, although traumatized, very much not ill. The bottom line was the institution had applied a diagnosis and had a process that compelled commitment and all the rest, and the evaluator would say, as he put it, “whatever” to achieve that end. This guy looks at me upon the slightest hint of a perception of questioning or resistance, and snarls (literally snarls) “You have court cases!?”, going on to say without waiting for a response, essentially, that unless he would be held liable for the consequences of commitment and treatment and the content of his evaluation etc., he would always do as he is doing here, partly out of fear of liability if he doesn’t given “common practice” and partly (probably moreso) because it was just par for the course. This man had never not recommended commitment in this setting in his career and made little secret of it, and that wasn’t changing. The report to the judge, which was rubber-stamped without question, was as superficial as it was riddled with blatant misinformation and derogatory. No hearing; judge wouldn’t allow it and kept delaying without providing a reason. Eventually, the poor guy gave up, although with some clever maneuvering he ending up avoiding more drugs and did great when he got out, all things considered, although the time lost and legal and medical stain, and the trauma of it all, clearly is a heavy burden.
The bottom line is that a legal hammer is probably the only thing that could set psychiatry back toward the straight and narrow. I don’t think some pedantry – and it is, or would be portrayed as, a kind of pedantry – about chemical imbalances and etiological confusion is sufficient. I know Whitaker doesn’t put forth such a reductionist argument, but it could be a lot better and it’s something I’ve noticed before here, and I’m not alone in that. The infamous Rondald Pies published another rant on his blog (ahem – excuse me, the Psychiatric Times) asserting that “they” can’t be taken seriously (following Moncrief’s study) because obviously psychiatrists (but certainly not Moncrief and her colleagues, or anyone else inconvenient) never said it was just solely only exclusively about this one “chemical”, (and that even if they did it doesn’t matter) and Psychiatrists, as opposed to psychiatrists and the rest of “them”, have an unassailable and dignified sophisticated understanding that he can never seem to actually show… But that b.s. will likely work wonders in court. Courts won’t want to insert their judgement on “medical matters”, and so will defer to what authoritative figures tell them and to what is institutionally convenient and has been done previously. It is very much a concrete part of legal doctrine that, essentially, questioning institutional entitlement, upending things in any way, is something to be avoided. If at present the APA has come to a narrative position that supports court actions previously (commitment and “treatment” following incidents etc.), however vague or inaccurate or disingenuous or whatever, courts have previously just said “what they said works for us, no begone so we don’t have to consider anything” and will likely continue to do so.
I think what needs to be done is that we need to stop beating around the bush so as to not too greatly injure people like Pies, out of fear (and also, it has to be said, shoo away some nonsense that pops up from time to time among the community, like religious interpretations of distress etc.) What needs to be made abundantly clear is that people like Pies and Aftab and Torrey are dishonest, ignorant, self-serving quacks, the drug industry is grubby (that should be less difficult), that real people are suffering terribly because of them, and that real science and real psychiatry do not fit in with “Psychiatry” and psychiatric practice and that deflections and attempts to obfuscate are yet another facet of institutional misconduct, and to demand change. In court, instead of beating one’s head against the wall, assert risk of irreparable harm, not arguments about etiology, and fraud: liability. Maybe then I won’t have to suffer conversations like the one I had with the asshole above.
Report comment
This was a very well written indictment of psychiatry’s position on prescribing antidepressants. It does reveal some of the very limited information and faulty research which some psychiatrists use to still defend their prescribing of these highly dangerous drugs.
Dan Kriegman said: “There appears to be a tendency for antidepressants to reduce emotional reactivity which for some people may include a significant decrease in distressing thoughts and feelings.”
I would disagree with the word, “significant.” The actual research show a “minor” reduction in so-called “symptoms.” AND I would definitely add the word “short-term” to describe the so-called “decrease in distressing thoughts and feelings.”
All of this research is based on a relatively short-term period of analysis of those people receiving these mind altering drugs. And all of this research IGNORES the significant number of people (victims) who end up going down the “rabbit hole” of a seemingly endless number of new prescriptions of other drugs, including dangerous drug cocktails.
Higher doses of a new and different SSRI (with different sets of bad side effects), and then benzos (dealing with akathisia and the higher amounts of anxiety as their depression fails to remit), and then mood stabilizers (to deal with the SSRI caused mania etc.), and then anti-psychotics (to deal with the drug induced insomnia and related psychosis etc.), and the list goes on, with perhaps multiple hospitalizations and failed suicide attempts.
AND what about all the SUCCESSFUL suicide attempts – who in the field of psychiatry and Big Pharma are actually interested to know and report those oppressive statistics?
Psychiatry and Big Pharma keep using the “blame the victim” phrase, “TREATMENT RESISTANT DEPRESSION” to describe patients who either don’t get better, or who will most likely get worse over time from their drugging.
Let’s start turning this phrase back on these criminals, and called it more accurately, “TREATMENT CAUSED DEPRESSION.”
My only criticism of this blog is that it does not go far enough. When we consider the millions of people harmed by psychiatry and ALL their mind altering and dangerous drugs, the only moral conclusion we can arrive at is to abolish psychiatry, and hold some of their leaders (along with the Big Pharma CEOS) criminally responsible.
AND lastly, psychiatry is now too big and important to the survival of the profit based capitalist system, to be allowed to fail, or have its power diminished. Mere perseverance of exposure and rational thinking or writing (THOUGH IMPORTANT AND NECESSARY) will NOT be enough to stop all forms of psychiatric abuse. Revolutionary systemic change is essential to finally end this type of institutional oppression.
Richard
Report comment
It may also cause a decrease in distressing thoughts like, “If I killed myself, my mother would be so upset, maybe I’d better try something else” or “If I shoot these people, I’d go to jail and I’m really scared of that!” So instead we get a suicide or a homicide.
“Decreasing distressing thoughts” is not always a great thing. And even if it were, I can go down to the bar and suck down a couple of ales and a few shots of Jack Daniels and decrease my “distressing thoughts” without medical pre-approval, and with similar results.
Report comment
Steve, your point here is highly convincing. Thank you!
Report comment
If psychiatrists as well as psychologists would admit that they know little about the human brain and the human condition than they could no longer claim to be “mental health experts” and testify in court for big $$$ as well as charge $375 per 40 minute session!
Psychiatry and its enablers like psychologists are LONG CONFIDENCE GAMES and they feed on the desperation and misery of the most vulnerable and the most helpless for profit!
Report comment
*Is psychiatry’s dilemma about resisting its own professional death and the loss of: face, career, status, legitimacy, power, respect, gravitas, raison d’être and prestige?
Psychiatry’s dilemma might be similar to the lawyer’s/legal profession’s dilemma?
e.g. https://www.unswlawjournal.unsw.edu.au/article/the-death-of-the-legal-profession-and-the-future-of-law/ ).
*Or does Mad in America provide a forum for DSM-5 psychiatry to continue to revive itself?
https://link.springer.com/book/10.1007/978-3-030-55140-7
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)01066-2/fulltext
Report comment
Back in the day Life Insurance policies also asked pointed questions like if you are taking benzodiazepines and non-benzodiazepines in particular along with anti-depressants and other psychiatric drugs. Benzos and non-benzos like Zolpedim cut a persons life span by at least 10 years- so that is calculated in issuing a policy. Drugs like Klonipin and Zolpedim cause dependence, cause the person to become unstable in mood and sleep leading to a life of constant shifting of drug treatments. This can further reduce the life expectancy by 20 years. It is a one way ticket.
Regarding the comment on the concentration of psychologists and psychiatrists in rich neighborhoods like Newton Mass. that is due to the fact that these so called “mental health experts” do not serve the poor or the insured but take cash, credit cards or checks. They are like vets who concentrate in cities and towns where people have lots of discretionary income.
Report comment
Good to know! Thanks! I wonder what is the practice of life insurance policies now. Do they do the same, or similar or different?
Report comment
Hi Gilbert
“Benzos and non-benzos like Zolpedim cut a persons life span by at least 10 years- so that is calculated in issuing a policy.”
So these are similar to the ‘real estate cancer maps’ held by the insurance companies? Obviously access would not be made easy, but such ‘evidence’ of the shortening of life would cause some significant problems for those claiming they are ‘first doing no harm [caveat; to their own bank balances]’
Report comment
Dan Kriegman says, “…clinicians have no access to the perspective and understanding that comes from comparing drug response to placebo response”, and “…we know that the impact of placebos can be greatly affected by their presentation.”
This explains why psychiatric drug research is useless.
Richard D. Lewis says, “….all of this research IGNORES the significant number of people (victims) who end up going down the “rabbit hole” of a seemingly endless number of new prescriptions of other drugs, including dangerous drug cocktails.”
This explains how psychiatric drug research has no connection to the real world.
Report comment
“… modern psychiatry is certainly mainstream.” And I agree, “It’s a religion.”
And, at this point – given the million plus children that the DSM “bible” thumpers have turned into “bipolar” stigmatized, with the ADHD drugs and antidepressants.
https://www.amazon.com/Anatomy-Epidemic-Bullets-Psychiatric-Astonishing-ebook/dp/B0036S4EGE
It’s most definitely a child abusing / “torturing” “religion.”
http://www.narpa.org/reference/un-forced-psychiatric-treatment-is-torture
Not to mention it’s also a systemic child abuse covering up “religion,” by DSM design.
https://www.psychologytoday.com/us/blog/your-child-does-not-have-bipolar-disorder/201402/dsm-5-and-child-neglect-and-abuse-1
https://www.indybay.org/newsitems/2019/01/23/18820633.php?fbclid=IwAR2-cgZPcEvbz7yFqMuUwneIuaqGleGiOzackY4N2sPeVXolwmEga5iKxdo
https://www.madinamerica.com/2016/04/heal-for-life/
But I will say, any psychiatrist who claims to not have been taught in med school … that both the antidepressants and antipsychotics can create “psychosis” and “hallucinations,” via anticholinergic toxidrome … is a liar.
https://en.wikipedia.org/wiki/Toxidrome
But since “telling stories they know are or may be untrue has become standard practice in psychiatry.” Well, I guess we should all now just start assuming the DSM “bible” thumpers will lie to us.
“it has become quite clear to me that the judges who control legal proceedings also tend to be true believers of the dominant [DSM] religion.” Yes, same is true for the lawyers.
“I believe that in the end the truth will prevail.” Let’s pray for the day.
You did a nice job of making Robert Whitaker be seen as the one who took the high road, and I do personally thank him for his truth telling.
And since we are fighting against those who utilize psychological warfare against their “clients.” It’s wise for us to be familiar with, and utilize those same tactics, when calling out the scientific fraud of their industries.
My son noticed, when he was seven, that Jesus’ theology – “as you wish that others would do to you, do so to them” – “has a trick to it.” And when some industries want to fight dirty (like utilizing psychological warfare against those they call their “clients,” after they’d first promised to “do no harm”).
It is morally acceptable, to point out the incorrectly assuming, gas lighting assholes, for being the scientifically “invalid” asses they chose to become.
Report comment
Removed for moderation
Report comment
I want to put in another good word for a class action lawsuit against the psychiatric drug companies and the psychiatrists who are funded by them. I am a lawyer myself, but it is very hard for me to gauge the possibility of success of such a suit. Success usually means that the defendants will have to pay out a lot of money to the plaintiffs. But whether that would happen or not, such a suit, if well-publicized, would get the general public to start asking questions about the psychiatric religion. We often hear a lot of talk about “banning psychiatry.” That would be nice, but our real and doable task is to discredit psychiatry, and a class action lawsuit might be a good step in that direction. If there is anything I can do to help this happen, please let me know.
Report comment
Thank you Dr. Kriegman, for going through mainstream psychiatry’s ethical shoddiness with a fine toothed comb. It shows how underhanded and opportunistic mainstream psychiatrists are. The trouble is, not enough people know this yet. But things are changing, and when change gets going, there’s no stopping it, and psychiatrists will finally look like the fools they are. Because I too think that “in the end the truth will prevail.”
Report comment
always curious how psychotherapy studies are presented uncritically and positively. Then again bias is always with us. Read William M Epstein’s books for a thorough dismantling of the best of the psychotherapy research – spoiler alert, none if it has any efficacy and it can also be harmful.
Report comment
[Duplicate comment]
Report comment
Dr. Kriegman’s “reduced emotional reactivity” to explain the marginal benefit of the drug over placebo is one possible explanation but my reading of the pertinent literatures suggests another. In the early stages of antidepressant drug use the drug causes brain impairment, which makes it difficult for the patient to focus on distressing thoughts and distressing life situation difficulties. At this stage the brain impairment is reversible with drug tapering. However, with long term antidepressant use the literature suggests actual structural brain damage from antidepressants (and antipsychotic drugs as well). Some psychiatric researchers have accepted the bad news on the long term use of these drugs on the brain but a few have taken the same data and re-defined both depression and schizophrenia as neurodegenerative disorders!
Report comment
Is that why anti psychotics work for nausea? I want to get off them, but they really help.
Report comment
Yes, I have carefully read the article, but without going farther down the rabbit hole of clicking & reading the links for more excruciating detail. I read carefully all the comments, many from others whose comments I have long been familiar with. And most with direct lived experience of the damage done by the pseudoscience drug racket known as psychiatry. Yes, I say again.
PSYCHIATRY IS ORGANIZED FRAUD & PSEUDOSCIENCE.
PSYCHIATRY HAS DONE, & continues to do, FAR MORE HARM THAN GOOD.
The best thing I’ve done in my life was reject psychiatry & psych drugs.
And, judging by the people I know, who are still victimized by psychiatry & neuro-toxic drugs, this article is a pathetic attempt to absolve the GUILTY.
The annual APA Conference is a veritable ORGY of PhRMA advertising.
Follow the MONEY.
Kriegman seems to be a typical leftist apologist. Nothing he says here is at all new, except for a few minor details.
Kriegman, IMHO, is equally culpable as the money-loving psychiatrists he so adroitly defends.
But hey, even serial killers deserve defense attorneys at trial….
Psychiatrists deserve conviction, and INCARCERATION. IMHO.
So here’s some MORE, of MY VICTIM IMPACT STATEMENT…..
May GOD DAMN ALL PSYCHIATRISTS.
They ALL belong in prison….
Report comment
[Duplicate Comment]
Report comment
Your suggestion that Aftab and co get good results from antidepressants because he and some other psychiatrists are good at forming “therapeutic alliances,” and the results have little to do with the drug has a certain appeal as he is charming and erudite.
His inability to answer his critics with reasoned argument is another matter entirely.
Report comment
[Duplicate comment]
Report comment
This still does not explain where the idea of using medications to treat “mental illness” actually starts.
It makes no sense, unless you are interpreting “mental illness” as indicative of some physical ailment. And “mental illness” is already a very stretched interpretation in itself.
Joshua
Report comment
[Duplicate comment]
Report comment
[Duplicate comment]
Report comment
[Duplicate comment]
Report comment
“And modern psychiatry is certainly mainstream. Thus, we need to recognize what we are dealing with: It’s a religion.”
And its most like Catholicism: sexist, tied to the body, patriarchal, corrupt, duplicitous, with a man written bible.
I have been saying the same on these comment pages for a while.
But who listens to an old woman deemed crazy?
https://www.madinamerica.com/2021/10/people-dont-recover-criminal-psychiatry/
https://www.facebook.com/gina.fournier.12/
Report comment
So we need to take the entire mental health system to pieces!
Joshua
Report comment
The nocebo effect is the lesser-known brother of the placebo effect, the Cain to the omni-present cognition’s Abel. While the placebo effect produces positive physiological outcomes through a trick of the mind, the nocebo effect produces negative physiological outcomes. Each effect is a reminder of the power of our minds connecting to our bodies all in the effort to heal and protect. More about the power of the placebo effect you will read here – net-boss.org/the-power-of-the-placebo-effect-by-randy-baker
Report comment