
“We have now sunk to a depth where the restatement of the obvious is the first duty of intelligent people.” (George Orwell: Review of Bertrand Russell, in The Adelphi, January 1939)
If we learn one thing from the Royal Commissions into child sexual abuse and the banking and insurance industries (see note 1), it will be this: left to themselves, secure institutions will never conduct the sort of self-critical analysis that the larger society expects — and deserves.
In late February this year, a conference on Mental Health in Crisis was held in Sydney and then at five cities in New Zealand. Major speakers included Prof. Peter Gotszche, of the Nordic Cochrane Centre; Bob Whitaker, from Boston; Dr Melissa Raven, from Adelaide; Prof. Roger Mulder, from Dunedin University, NZ; and Maria Bradshaw, from Auckland. I spoke about studies on ECT and several other speakers contributed their harrowing personal experiences of psychiatry.
Subsequently, an article in a New Zealand paper was critical of antidepressants, which provoked the Royal Australian and New Zealand College of Psychiatrists (RANZCP) to issue a press release (March 9th 2018; taken down soon after) which was openly hostile to the idea that people could criticise antidepressants. As part of that press release, it was claimed that psychiatrists “only ever (prescribe drugs) in partnership with the patient and after due consideration of the risks and benefits.”
My experience is that this claim is absolute rubbish and I lodged a complaint with the RANZCP to this effect.1 On April 27th, I received a letter from the president of RANZCP, Dr Kym Jenkins, assuring me I had it all wrong, the RANZCP meant no harm, but she firmly reiterated the claim that provoked my complaint:
“I wish to highlight the College statement goes on to say, ‘the prescription of…medications is something that a psychiatrist only ever does in partnership with the patient and after due consideration of the risks and benefits.'”
As a result, I thought I should check the veracity of her claim. After a quick survey of my practice, I submitted a paper to the lesser of the two RANZCP journals, Australasian Psychiatry, on May 6th. The following is a slightly amended version:
PROVIDING INFORMATION ON PSYCHIATRIC DRUGS: A PILOT STUDY
Following adverse reports in a New Zealand newspaper regarding the efficacy and safety of psychiatric drugs, on March 9th 2018, the Royal Australian and New Zealand College of Psychiatrists (RANZCP) issued a press release in rebuttal: “Claims by New Zealand newspaper The Press that antidepressant and antipsychotic medications don’t work are highly irresponsible and potentially very stigmatising for people experiencing mental illness…”
It continued: “Psychiatrists are highly trained medical professionals with expertise in managing both physical and mental health…. The prescription of antidepressant or antipsychotic medications is something that a psychiatrist only ever does in partnership with the patient and after due consideration of the risks and benefits.”
It has long been my experience that patients report they were given little or no information relating to the major side effects of psychotropic drugs, in particular, the risks of obesity, sexual dysfunction, akathisia, aggressive and suicidal impulses, neuroleptic malignant syndrome, and dependency. In view of the sweeping claim quoted above, a preliminary file survey of my current patients was undertaken.
Mine is a private, bulk-billing (government-funded) practice in working-class areas of suburban Brisbane. Compared with standard private practices, patients are typically younger, more likely to be male, immigrant, unemployed or on disability pensions, and with histories of major family disturbance, poor schooling, poor work records, social disruption, crime, and drug and alcohol abuse. That is, they are typical of out-patients in any public service in most countries.
Of 176 current files, nearly half the patients had a history of prior psychiatric contact. Their files were checked to see if they had been given information on the nature of the disorder and side effects of the drugs. Where the information was not recorded, patients were asked the following questions, either at their next attendance or by phone or email:
- What were you told about how this drug works on your diagnosis?
- Were you told about its side effects?
RESULTS
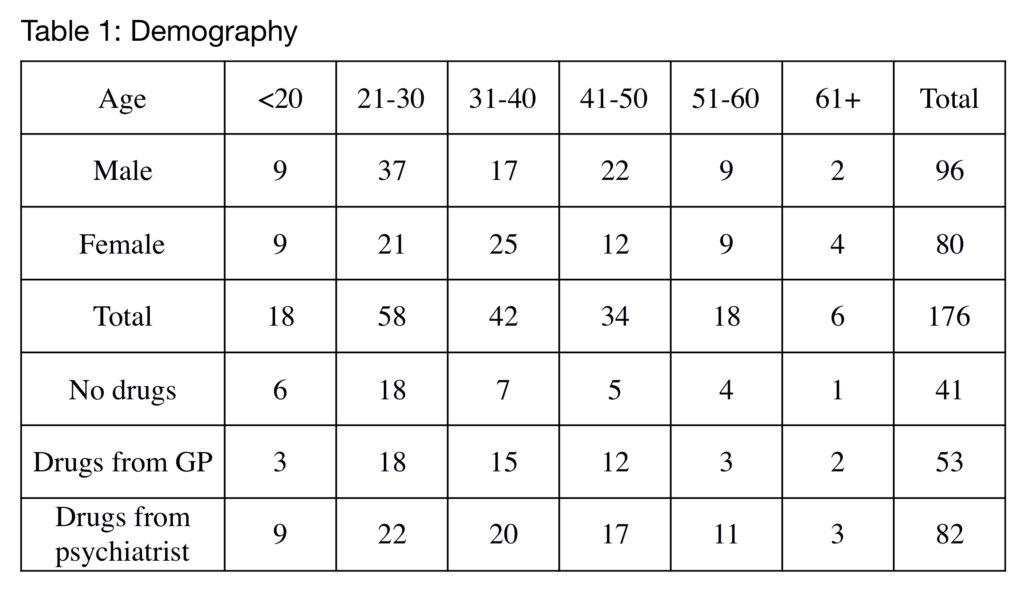
The results are shown in the accompanying tables. Because this is a pilot study with small numbers, results have not been converted to percentages. At the time of referral, 135 of a total of 176 current patients were taking psychotropic drugs (Table 1). In 82 cases, the drugs were prescribed by a psychiatrist while the remaining 53 were prescribed by general practitioners (GPs). There was a clear tendency (not shown in the table) for male patients to have seen psychiatrists while female patients were more likely to have been prescribed drugs by their GPs.
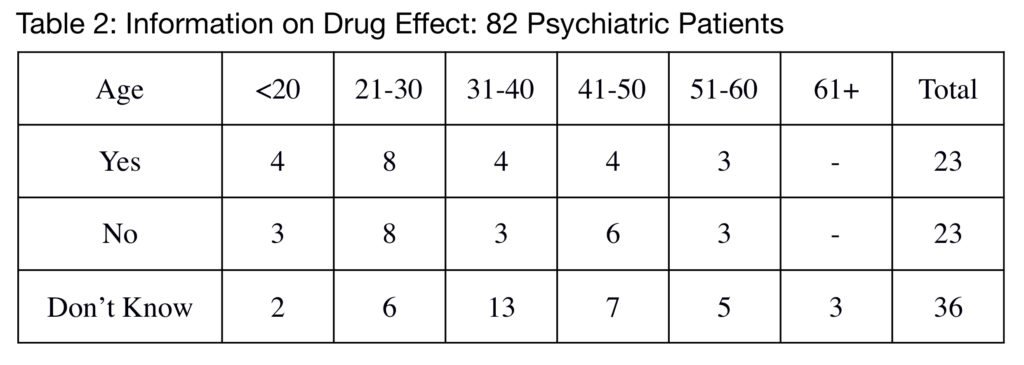
Question 2 could have been refined as there were two parts to it: Were you given a formal diagnosis? and How does this drug work in your condition? Of the 82 psychiatric patients, only 23 stated that they recalled having been given information on the mode of action of the drugs (Table 2). Most people who recalled a diagnosis stated they were told only a name (schizophrenia, bipolar disorder, ADHD etc). There were either told or they assumed it amounted to a “chemical imbalance of the brain.” This, however, misses the point that 59 out of 82 patients (72%) didn’t understand why they were taking their medication. There appeared to be no difference between private psychiatric practices and public services.
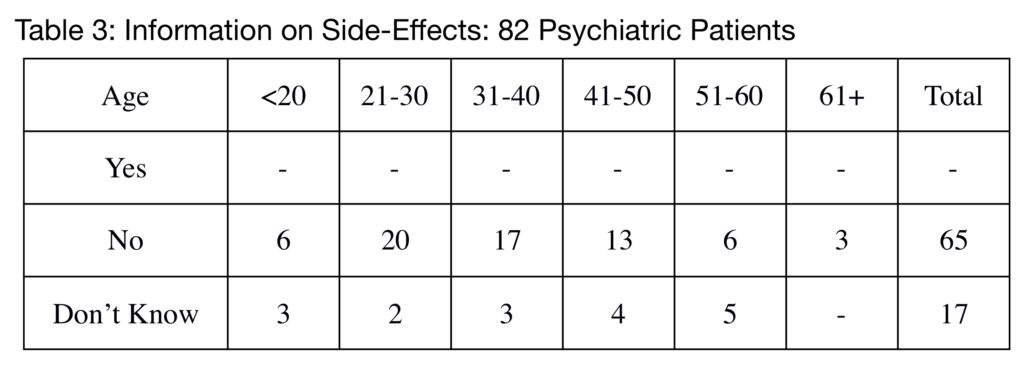
The most telling result is for information on side effects (Table 3). No patients with previous psychiatric contact had been given any more than the most superficial information relating to side effects (e.g. “It might make you a bit drowsy” of olanzapine).
To reiterate, these questions were asked:
- What were you told about how this drug works on your diagnosis?
- Were you told about its side effects?
Typical responses were as follows (expletives deleted):
Mrs JH, a 54yo mother first admitted to hospital at age fifteen, had had something like twenty admissions over the years, with at least twenty-five different drugs as well as fifty ECT. At the time, she had just been discharged and was taking four drugs:
Q1: “They never said anything. In those days, they didn’t even talk to you. Still don’t.”
Q2: “Of course not.”
Mr DT, a 29yo fireman injured in a fall, became intensely agitated after he was prescribed fluoxetine so was referred to a psychiatrist:
Q1: “They just said I’m bipolar and that’s that. Maybe somebody said something about brain chemicals or I read it somewhere, I don’t know. I think it was the antidepressant messing with my brain. I’ll never take them again.”
Q2: “I wasn’t told anything. They put me on lorazepam (7.5mg per day) but nobody told me how addictive it is. It’s a nightmare, that stuff, they shouldn’t be allowed to prescribe it.”
Ms TM, a 26yo social worker, was treated with large doses of antipsychotic and antidepressant drugs after a brief psychotic episode following major stressors. After taking olanzapine 40mg per day and mirtazapine 45mg per day for fifteen months, her weight went from 58kg to 105kg:
Q1: “They kept telling me I’ve got a chemical imbalance of the brain and I’d have to take drugs for life. That was so depressing, I can’t tell you.”
Q2: “No, they never said a thing. I kept telling the doctor I was gaining weight but she just said I should watch my diet. I assumed it was my fault, that made me feel even more guilty.”
Mr KV, a 29yo military veteran discharged after sustaining a major back injury, was prescribed a range of antidepressants as well as quetiapine as a hypnotic:
Q1: “They didn’t say a thing. Nobody said anything.”
Q2: “You’ve got to be joking. Nobody said a thing about side effects, especially about losing your sex life. I’d like to give (quetiapine) to that psychiatrist and see what he thinks of it.”
Ms BM, a 23yo student, developed a psychotic state after she started using marijuana and other drugs, including methamphetamine. She was prescribed perhaps a dozen different psychotropic drugs in rapid succession but her mental state did not settle. She gained a great deal of weight and was constantly confused and erratic. In response to the questions, her mother said:
Q1: “They said she’s schizophrenic but she was the brightest and happiest girl before this. I don’t believe it, there’s no mental disorder in our families, how can it be genetic? They said the drugs would fix her condition but she’s not getting better. Now they’re calling it treatment-resistant schizophrenia.”
Q2: “We were never told a thing. The hospital tell us over and over again the drugs are safe and non-addictive but it’s not true. And the weight she’s gained, she was such a pretty girl, now look at her.”
Mr BW, a 42yo post-graduate, had had about twelve admissions to private hospitals over twenty years. He had had every available drug, often in huge doses:
Q1: “I’ve been given every diagnosis, schizophrenia, bipolar, autism, social anxiety, depression, the lot. What causes it? Oh, something chemical, that’s what they say.”
Q2: “Of course not. I’ve been on everything but there’s no point complaining, they’d just say it’s my disease and I need more drugs. Quetiapine was the worst, it drove me completely mad. I found out it’s called akathisia but the psychiatrists didn’t believe me, they said I’m schizoaffective so they gave me ECT.”
Mr EG, a 49yo senior manager with several admissions to hospital:
Q1: “I’m bipolar, is that what you mean? They say it’s chemical, the drugs will fix it.”
Q2: “Nothing. They don’t believe their drugs have any side effects. I told them I couldn’t think because of the lithium so they stopped it suddenly and of course, I flipped out. They said that’s my disease coming back. It wasn’t, it was drug withdrawal, I’m not stupid.”
Mr GD, a 43yo man, has had a singularly torrid psychiatric history. His father recently said: “They asked whether he’d ever had clozapine. I told them he’d had it twice but each time they had to stop it because it affected his heart. I said they couldn’t give it but they went ahead anyway. He refused so they held him down and squirted it down his throat. Then his enzymes went everywhere and the cardiologist told them to stop it.”
DISCUSSION
On these results, the claim that psychiatrists “only ever” prescribe drugs after discussion of the risks lacks empirical justification. It would be more appropriate to characterise it as “hardly ever.” The question arises: How could a responsible professional body make an assertion which appears to be so patently wrong? The philosopher, Harry Frankfurt, has written extensively on the concept of truth and falsity.2 He defined a lie as “…an act with a sharp focus. It is designed to insert a particular falsehood at a specific point in a set or system of beliefs, in order to avoid the consequences of having that point occupied by the truth. This requires a degree of craftsmanship…” The liar, he said, knows precisely what he is doing. He knows the truth and wishes to lead his audience away from it.
However, between truth and falsehood, there is another epistemological category, in which the speaker’s utterances are neither true nor false but are designed to sway the audience to a particular conclusion regardless of the facts. This Frankfurt called ‘bullshit,’ which is “…more expansive and independent, with more spacious opportunities for improvisation, color, and imaginative play. This is less a matter of craft than of art.” The ‘bullshit artist’ is recklessly disregarding of the necessity for truth; it is a tool to be wielded but not a value in itself. Certain fields of discourse, such as politics, advertising, sport, entertainment, fashion, etc., lend themselves to bullshit. It is unfortunately also true of psychiatry.3
We can now attempt to categorise the statement in the College’s press release. Was it just a matter of the College officials cobbling together a statement to calm the jittery public so they keep taking their tablets, i.e. did it meet criteria for bullshit? It seems unlikely because, as this survey shows, it was a statement that could be falsified with the greatest of ease. In general, bullshit statements are not of this form but are largely matters of taste or sentiment: “This great country of ours…” “Our wonderful sports heroes..” Others relate to the future: “We will bring jobs and growth.” “Make our country great again,” etc. Crucially, because they are neither true nor false, most bullshit statements cannot easily be refuted.
Moving to the category of frank lies, it is an essential part of the definition that the speaker is fully cognisant of the truth but carefully and deliberately changes something critical to mislead the audience. Does that apply to the college’s action in issuing this press release? This is problematical. If, for example, the public became aware of the true risks of obesity, diabetes, sexual dysfunction, suicide, etc, what would happen to psychiatry’s reputation? I believe a reasonable person could conclude that the statement was factually false but was no more than a panicky attempt to retain control of the narrative that psychotropic drugs are safe, effective and are only prescribed for noble reasons. That is, they can use the defence coined by the eminent immunologist, Peter Medawar4, in his review of Teilhard de Chardin’s book, The Phenomenon of Man:
“(The) author can be excused of dishonesty only on the grounds that, before deceiving others, he has taken great pains to deceive himself.”
CONCLUSION
It appears that, at least, the RANZCP has left itself open to the charge of self-deception. That is, while the authors of the press release probably believed what they were saying, they were recklessly deficient in ensuring its truth. Either way, it is a matter of the utmost gravity that this question should ever arise, especially as it is not the first time.5 We owe it to the general public, to our paymasters and to our patients to ensure that everything we say about drugs and treatment is true, not just a self-serving, highly selective reading of the evidence. Regardless of how embarrassing it may be, a thorough and open examination of these two matters is long overdue, i.e. the question of whether psychiatric drugs are all they are touted to be, and how it could be that a major professional body could be misled. If we do nothing, then the profession of psychiatry itself will be in grave danger. Overwhelmingly, this is a message psychiatrists don’t want to hear.
*****
On May 12th, I received the following letter of rejection from the editor of the journal Australasian Psychiatry:
11-May-2018
Dear Dr McLaren,
We thank you for your submission to the journal and regret that we cannot publish your paper on this occasion. Although this is a worthy topic of investigation, there is no methods section within your paper and it is assumed that you have reviewed the files of a single clinic. The results are influenced by subjectivity and recall bias.
Yours sincerely,
Dr Vlasios Brakoulias
Editor, Australasian Psychiatry
In an interview on their long-term study on antidepressants by Hengartner et al, the lead author said:
“…due to institutional corruption within academic psychiatry, it is quite difficult to successfully pass the review process with such papers. Most psychiatric experts reviewing for the leading scientific journals refuse peremptorily any report calling into question the merits of psychiatric drugs.”
I have previously published a critique of the psychiatric publishing industry that essentially concludes it is seriously corrupt.6 I submit that what we are seeing in this small case is a typical example of the almost-unconscious self-deceit that now characterises mainstream psychiatry. In the first place, the claim of the president of RANZCP, Dr Kym Jenkins, that psychiatrists “only ever” prescribe drugs after due discussion of pros and cons is not just empirically false, but laughably so. I will accept that, in rushing to complete the press release, it may have been the case that its author(s) took liberties with the claim, but when she restated her claim in her response to my complaint, she had my survey to hand. In the face of such evidence, it is impossible to claim that psychiatrists always do their duty by the patient and tell them about the side effects: here were dozens of cases, taken at random over the past six months, in one small practice, which categorically contradict her statement. I submit that any reasonably educated and fair-minded person could conclude that the president of the RANZCP, Dr Kym Jenkins, was at the very least recklessly deficient in her view of psychiatrists prescribing potent psychoactive substances.
Turning to the rejection advice issued over the name of a well-known academic, I agree my survey wasn’t perfect, that’s why it was subtitled “A Pilot Study,” but I will state flatly that I hope he didn’t expect me to believe his reasons because I don’t:
“One has to belong to the intelligentsia to believe things like that: no ordinary man could be such a fool” (George Orwell, Notes on Nationalism, 1945).
I find his excuses totally disingenuous and meretricious. I am absolutely certain that if any of his academic friends or their acolytes had submitted a paper which lacked a methods section (actually, that’s not true: it was clearly described in the paper), then they would have received a friendly email pointing out their error and inviting them to correct it. However, it’s the bit about “subjectivity and recall bias” that grabs attention.
When I trained, admittedly a very long time ago, psychiatry was actually about subjectivity. That’s what mental life is, so I think it is entirely fair for patients to respond “subjectively” to how they are managed. I have another patient whose weight went (objectively) from 50kg to 103kg (106% gain), entirely by the well-known, objective effects of mirtazapine and quetiapine. Subjectively, she was severely pissed off and I believe she had a right to be. Objectively, it cost her a lot of money for new clothes; subjectively, it filled her with horror and her fragile self-esteem finally shuddered and expired. Objectively, when the drugs were stopped, she lost most of the weight but subjectively, she loathed the stretch marks it had given her. So when Dr Vlasios Brakoulias, senior lecturer in psychiatry at the Nepean Clinical School of Sydney University, says a perfectly objective paper, i.e. counting responses from patients, is too “subjective” for his journal, I dismiss his objection as just another example of what Hengartner called “institutional corruption within academic psychiatry.” It actually meets the definition of bullshit, given above, but the matter is far too serious for that label.
Turning to the question of “recall bias,” I will concede that, yes, human memory is a bit of a problem (especially at my age) but I do not doubt that the patients said what they believed to be true. If they said they were told nothing, then that is what they believed. If, as a matter of historical fact, they were told something else, that is, for the purposes of psychiatrists managing the mentally-disordered, just a signal that they need to lift their game. All that counts is that the patients have no recollection of being given adequate information on the side effects of their drugs. In any event, I submit that in this type of study, any recall bias will be self-correcting, meaning patients are just as likely to believe that something they read or heard somewhere must have come from the psychiatrist as they are to have forgotten what was said to them. The case of Mr TD confirms this.
Also not included in the quotes was a 46yo woman who developed very obvious and distressing tardive dyskinesia of the face and arms as a result of eight years of quetiapine (which she shouldn’t have been prescribed, but that’s another story). Was she warned about this terrible side effect? When I rechecked with her this week, she again said she wasn’t. From years of experience, I don’t have enough confidence in the quality of the case notes of the Queensland Mental Health Services to go back eight years and see if it was recorded that yes, she was given full product information on this drug. You can believe this: she wasn’t. So much for “recall bias.” It is one of those slippery labels that can be used to justify “inherent bias,” aka self-serving prejudice.
So where does this leave us? Are we going to trust what patients tell us or do we dismiss it as biased and subjective, self-serving whimpering? For myself, if I have to choose between trusting the honesty of my patients, or trusting the honesty of mainstream psychiatry, it’s a no-brainer. And my recent correspondence with two of the most senior officials of the Royal Australian and New Zealand College of Psychiatrists confirms to me that I have made the right choice.
Note 1: A Royal Commission is the highest level of enquiry in Australia, similar in powers and scope to the Mueller commission in the US. Each Commission is established by an Act of Parliament and has very extensive powers of investigation and subpoena, as well as punitive powers. The current Liberal government fought for years to block the Royal Commission into the banking and insurance industries; now that it is in session, we see why.













Niall, thank you for this great post! I attended the Mental Health in Crisis workshop in Sydney and it was fantastic. And given the institutional corruption you noted, the response was predictable. One response showed up here in this New Zealand newspaper story: https://www.stuff.co.nz/the-press/news/101845845/claims-antidepressants-dont-work-dangerous-doctors-say. In it, famous UK psychiatrist David Nutt had some interesting and provocative things to say. And so I took the liberty of trying to engage him in a discussion about his remarks. I’m copying and pasting our email exchange below in case anyone is interested. Like you Niall, I don’t like bullshit, especially the kind that does great harm to society. Keep up the great work. -Cheers, Brett
**********
(Email to Dr. David Nutt from Brett Deacon)
Dear Dr. Nutt:
I read with interest this article from the Press (Christchurch, New Zealand): https://www.stuff.co.nz/the-press/news/101845845/claims-antidepressants-dont-work-dangerous-doctors-say. The article quotes your views on antidepressants and depression, and includes the following passage:
“There was “overwhelming evidence” supporting the view that mental health problems were caused by chemical imbalances in the brain…”It’s like the climate change debate. Some people do not want it to be true but there is a biological element. It’s not a myth. We know the chemistry of depression.”
I am a fellow scientist and practitioner with an interest in this topic. I am very interested in hearing from you what overwhelming scientific evidence shows depression and/or other mental health problems to be caused by a chemical imbalance in the brain. I’d appreciate any citations to specific studies you can provide that substantiate such a claim. Thanks very much for your time and consideration.
Warm Regards,
Brett
**********
(Reply from Dr. David Nutt)
Maybe start with this book?
https://www.amazon.co.uk/Understanding-depression-translational-Carmine-Pariante/dp/0199533075
**********
Dr. Nutt, thank you for your prompt response. I have not read that book, but I am a student of the literature in this area and have read numerous summaries of the research pertinent to chemical imbalance theories of depression and schizophrenia. My understanding from these reviews is that there does not exist clear evidence that a chemical imbalance is an established cause of any mental disorder. But I may be mistaken and was wondering if you were aware of specific studies that I am not that have established this finding. Is that the case?
**********
(Email to Dr. David Nutt from Brett Deacon)
Dear Dr. Nutt:
It has recently come to my attention that Dr. Patrick McGorry, psychiatrist and former Australian of the year, has a different view of the chemical imbalance theory from the one you expressed. In an interview (http://www.abc.net.au/radionational/programs/lifematters/depression,-anxiety-and-the-pros-and-cons-of-antidepressants/9391218), he stated that the chemical imbalance theory was attributable to the “drug companies, the DSM, the FDA … American psychiatrists … 40 years ago … now no one believes that any more. If you talk to any modern researcher in neuroscience or psychiatry no one would say that is the explanation. But when you go to a GP or even some psychiatrists they will still trot out that very simplistic explanation to people.”
You claimed there exists “overwhelming evidence” that mental health problems are caused by a chemical imbalance in the brain, and that failure to acknowledge this is akin to denying the reality of climate change. Yet the esteemed Dr. McGorry expressed in no uncertain terms his opinion that the chemical imbalance theory is a scientific myth that is not taken seriously by researchers in this area. Dr. McGorry’s opinion is consistent with my understanding of the available scientific evidence, as summarised in the following articles:
http://journals.plos.org/plosmedicine/article/file?id=10.1371/journal.pmed.0020392&type=printable
https://davidhealy.org/wp-content/uploads/2015/07/2015-Serotonin-and-Depression-bmj.h1771.pdf
http://diginole.lib.fsu.edu/islandora/object/fsu:252733/datastream/PDF/view
In the United States where I am from, top psychiatrists have distanced themselves from the chemical imbalance theory, claiming that it was never taken seriously by thoughtful psychiatrists and scientists or promoted to clients. Here are some examples:
http://www.illawarraanxietyclinic.com.au/uploads/7/6/0/4/7604142/lacasse___leo_tbt.pdf
https://www.npr.org/sections/health-shots/2012/01/23/145525853/when-it-comes-to-depression-serotonin-isnt-the-whole-story
I am also aware that the media frequently and uncritically promotes the chemical imbalance theory (https://link.springer.com/article/10.1007/s12115-007-9047-3). This appears to have been the case in Cecile Meier’s The Press article in which you were quoted as claiming overwhelming evidence supports a chemical imbalance cause of mental disorders, a claim whose veracity was not questioned (https://www.stuff.co.nz/the-press/news/101845845/claims-antidepressants-dont-work-dangerous-doctors-say).
I have made an effort to promote thoughtful, scientific, and public discourse about topics like the chemical imbalance story of mental disorders (for example, see http://www.uw-anxietylab.com/uploads/7/6/0/4/7604142/biomedical_model_commentary.pdf and http://www.abct.org/docs/PastIssue/38n7.pdf). I believe this is important because misinformation abounds, and patients require access to accurate information in order to make informed decisions about their healthcare. I am concerned that your comments about the chemical imbalance theory in The Press article hinder this important dialogue through your promotion of a scientifically unfounded theory as established fact. But, as I noted in my previous email, you may know of scientific studies of which I and other experts in this area are unaware that do in fact establish that a chemical imbalance is a specific, sensitive, and replicable cause of one or more DSM-defined mental disorders, particularly depression which was the subject of your recent comments. In that case, I would be grateful if you could alert me to such studies. If not, I would appreciate hearing whatever justification you can provide for your claim, in contravention to the consensus of scientific experts on this topic, that the chemical imbalance theory is supported by overwhelming evidence.
I’ve copied Cecile Meier on this message (Hi Cecile!) as she may be interested in your reply. Thank you for your time and consideration.
**********
(I never heard back from Dr. Nutt)
Report comment
Wow, either Nutt is very busy and thought the book he helped put together is enough or he is an arrogant t****er (English word that should not be translated in polite company.)
He is an interesting chap who got himself into hot water with the government over the classification of illegal drugs. He said a lot of them are a lot less dangerous than the government would like so they sacked him from his job assessing such things for the government. His views on depression however make me wonder who he is in the pay of.
Report comment
He didn’t respond to me, either, and I was studiously polite.
Report comment
Because he considers you a peon perhaps.
Dr. Goezhe in his book Psychiatry and Organized Denial does not appear to think highly of Nutt.
Dr. Nutt the psychiatrist. You cannot make this stuff up! 🙂
Report comment
I think it’s because they hit him where he lives and he knows that he can’t answer without further prevaricating, which the gentlemen writing him will quickly suss out.
Report comment
Niall as usual perfectly nailed
I have dealt with /listened to many australian psychiatrists all completely committed to chemical theory and genetic traits. All besotted with drugs. raising side effects gets you labelled as difficult and antipsychiatry..and more drugs for your family member! entire profession here a disgrace no regulation ..lots of involuntary orders no contemporary or compassionate practice avoid them at all costs. i would be very proud if they refused to publish me it means you speak the truth!
Report comment
And the one star review of Dr. David Nutt’s book recommendation reads:
“Should be entitled misunderstanding depression.”
Report comment
David Nutt, is that the one who wants to put all of us on benzodiazepines? He actually believes all alcohol in the world can be replaced with a drink he invented, which is nothing more than a benzo cocktail. The real “nutty professor”, that’s what I call him.
Report comment
Yes it seems so, he bangs on about the harm alcohol has done which is very correct. What he doesn’t inform the public of is that benzo’s and alcohol do the same thing in the brain, only benzo withdrawal is much much worse, and it happens very much more quickly. The problem we have isn’t so much people like Nutt answering our emails, it’s how to inform the public of the truth effectively and stop them.
The Labour Party UK Govt soon realised the issue with Nutt and sacked him as advisor. But what they failed to do, is realise and act on the wider, much more serious issue of benzodiazepine harm to the public.
People get hooked on benzos from GP’s and in hospital… if you drink alcohol to the point the doctors think you will be an alcohol withdrawal issue, you get a benzo at least in the UK NHS hospitals.
Report comment
but they sacked him for his work on recreational drugs. He kept classifying drugs and not very harmful and the government wanted them all to be very very bad. He was quite honest about recreational drugs, it’s the psychiatric ones he gets his knickers in a twist about. But then he was in the pay of GlaxoSmithKlien.
If only he had stuck to saying what the real risks of recreational drugs were and telling it as it is all would have been well.
Report comment
I wish he’d invent some flubber instead. Lol.
Report comment
David Nutt is also completely delusional. He is convinced that the whole world will want to drink his benzo cocktail and quit all alcohol. That’s right: ALL alcoholic beverages on the planet. It will happen within a decade or so, he says. How dumb and crazy can one be to believe such a thing? Not to worry, he says. He’ll take out the addictive part from his concoction. Good luck with that, dr. Nutt! Why can’t they just make non addictive benzos then? Totally nutts if you ask me.
Report comment
After he discovers the specific gene that causes schizophrenia and maybe the bipolar gene too. Lol.
Report comment
Dear Niall and Brett, thanks for your work in correcting misinformation from my College. In August last year I took the trouble to post a direct message to the president of the College Dr Kym Jenkins on a college forum thread which she had commenced, about “college strategic plan” which included the following “values”: “Our Values • Integrity • Respect • Compassion • Collaboration • Quality • Innovation • Sustainability”.
In regard to “integrity” – my post follows: Robert Purssey – 31/08/2017 7:06:09 PM
RE:The RANZCP Strategic Plan
Dear Kym
Re: “Integrity”
on “Your Health In Mind” (RANZCP college website for the general public) – i note – “How do medications treat mental illness – Medications work by rebalancing the chemicals in the brain” – a statement very clearly implying a pre-existing chemical imbalance. Dr Ronald Pies (along with many others) has recently proclaimed “I am not one who easily loses his temper, but I confess to experiencing markedly increased limbic activity whenever I hear someone proclaim, “Psychiatrists think all mental disorders are due to a chemical imbalance!” In the past 30 years, I don’t believe I have ever heard a knowledgeable, well-trained psychiatrist make such a preposterous claim, except perhaps to mock it. On the other hand, the “chemical imbalance” trope has been tossed around a great deal by opponents of psychiatry, who mendaciously attribute the phrase to psychiatrists themselves.2 And, yes—the “chemical imbalance” image has been vigorously promoted by some pharmaceutical companies, often to the detriment of our patients’ understanding.3 In truth, the “chemical imbalance” notion was always a kind of urban legend- – never a theory seriously propounded by well-informed psychiatrists.”
Please note also “Linking Molecules to Mood – New Insight Into the Biology of Depression. Krishnan and Nestler, AJP Oct 2010” – “Since monoamine enhancers improve depressive symptoms, it was suggested historically that depression is caused by deficits in monoaminergic transmission (“monoamine hypothesis”), which continues to be a prominent preoccupation of the field. However, after more than a decade of PET studies (positioned aptly to quantitatively measure receptor and transporter numbers and occupancy) (31), monoamine depletion studies (which transiently and experimentally reduce brain monoamine levels) (32) as well as genetic association analyses examining polymorphisms in monoaminergic genes (27, 33, 34), there is little evidence to implicate true deficits in serotonergic, noradrenergic, or dopaminergic neurotransmission in the pathophysiology of depression.” – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3031089/
And furthermore, re IATROGENESIS of this “urban legend” – https://static1.squarespace.com/static/51cb73eee4b07cb3e8507d7e/t/56b8f015e707eba737d9d09e/1454960662195/beh+therapist.pdf
Please explain how this “information” on College websites comports with “Integrity”.
Kind regards,
Dr Robert Purssey
MBBS FRANZCP
ps notably such misinformation (among other on the site) clearly breaches our National Health and Medical Research Council guidelines for medical practitioners on Informed Consent https://www.nhmrc.gov.au/guidelines-publications/e57
pps note also Dr Patrick McGorry’s recent quote above in relation to this matter – and the relevant weblink https://www.yourhealthinmind.org/treatments-medication/medication
Report comment
If Dr. Pies becomes so angry and offended by the idea that members of his profession are uninformed enough to believe in the “chemical imbalance metaphor” why doesn’t he simply make a public announcement to enlighten the masses when “mental illness” makes the news? Say, after a major school shooting. He could find a ready audience as a well-respected psychiatrist elected president of the APA.
Report comment
Institutional protection rachet
They said ‘you have a chemical imbalance’ They lied. They ‘diagnoised’ mental illness, which finding to be a myth, they never shared (do as we say not as we do) but finding out anyway they said ‘we had to put something down’ – did they mean me? – did it have to be so profoundly stigmatising excusing such poison?
Then they told the truth ‘we’ re concerned about your quality of life’ which subsequently lay in ruins! After ‘predicting more and more breakdowns each subsequently worse than the other’ my family and friends abandoned me. No one can predict such a future but some by these and other means can make it happen
Try again, fail again, fail better.
Report comment
Psychiatry isn’t just hurting the consumers–destroying their bodies and souls bit by bit–but it’s hurting their families and society as a whole with its inflated (often deceitful) claims about the safety and effectiveness of the products they sell.
Oddly enough I met two mothers with mad adult children. Not NAMI mommies, but well meaning women who loved their offspring and were wringing their hands in despair.
One had a son. “If only jr. would take his meds.” But the behaviors she described were not being out of it. Rather her son was an ungrateful brat. He refused to help out around the house and verbally abused her and his siblings. But she was convinced this was just his “sickness” and continued to beg him to take his pills.
(Neuroleptics can “help” people by making abusive loud mouths too tired and numb to be as mean. Still doesn’t make them think more clearly or fix character flaws. Duct tape could probably work just as well. Duct tape jr. to a chair so he can’t smash things or put holes in walls. Duct tape his mouth so he can’t verbally abuse family members. Ta da! Duct tape is a safe and effective modality of treatment.)
Telling the “mentally ill” person they are no longer responsible for their actions is bad for their characters in the long run. Besides ostracizing them from the community–both by labels and morbid obesity/uncontrollable tics/apathy/coldness from the drugs–the idea that “you can’t help yourself, you aren’t responsible for your actions, it all depends on those around you, you’re sick, if you keep “taking your meds” they have no right to complain. These can turn anyone into a jerk if they believe them. Plus emotional numbness and poor cognitive skills made me lazier and more selfish.
Communities don’t know what to do with these people. If their behaviors or suffering worsens there can be only one answer. They aren’t taking their “meds.” Exasperating for all. Devastating for the banished member.
As far as how the hyper-inflated claims of psychiatric treatments have harmed society and put the public at risk, Dr. Peter Breggin says all that I could say–only better. Read his article about the false security psychiatry provides enabling school shooters to run amok.
Report comment
Thanks Rachel you’ve inspired me to find a long lost word! When growing up we we’re warned about or threatened with psychiatry but since the invasion of the community care teams and the monumental bad pharmaceutical marketing campaigns we’ve all been made fools of. No the word might be people or person but we’re called ‘patients’ the appropriate term for legitimate health services, or user, client, survivor an apt description of those who’ve survived this fraud, rarely done on your own, thus the tendency to ostracised unbelievers, no the term I’ve failed until now to realise is ‘dupe’! The mental health movement has made dupes of nearly all of us by now, sadly!
Ohh and a handy notion when confronted is to realise that many of us might have a tendency to misdirected or angst, it’s safer that way. Just so long as you have the decency to check our own contribution, many learned folk fail to do so and automatically assume it’s nothing to do with them often misdirecting their own fears onto the mythical mentalillness. Often people’s angst is done no end of good by staying clear of those who get their goat up, that would be my default approach, and wish that the same was true of others! But I get the message you express yourself loud and clear. Less of that talk of duct tape you’ll be giving people ideas
Report comment
Doubt it’s any worse than neuroleptics. Lol.
The old chains in the attic!
I really wish the psychiatrists would differentiate between the dangerously violent and the harmless. Most fall into the latter category. “Med compliance” is not the significant factor but behavior. But they have “services” to sell the public…and us.
Report comment
Better to wish that psychiatrists would not be entrusted with such decisions, no?
Report comment
Yes. But till we kill the dragon, pulling out its teeth and removing its fire breathing ability would help a lot.
Report comment
Actually you’re making me feel sorry for the dragon, but fortunately he’s only a metaphor. But what you describe sounds a lot like goals which have been proposed, i.e. to decertify psychiatry as a branch of medicine, and most importantly, to end forced “treatment.”
Report comment
At least duct tape is a more honest approach.
Report comment
Not very scientific though. Like using a wooden ball bat instead of electroshock. Tsk tsk. Not all professional.
Report comment
And who can make massive profits off of duct tape?
Report comment
Rachel777 this is a really excellent post. I know we’re not supposed to back pat – but you’ve really hit the nail on the head – that bad behaviour is drugged too.
And then the medical model tells the person-behaving-badly that it’s not their fault, their brain is broken, so no effort is made to improve bad behaviour.
Ostracizing, community reactions (Sven is beating puppies again, we need to teach him that is not done), taking care of each other – these help with bad behaviour. If your community mirrors back to you that you are not cooperating, not flowing – then if you care, if you love your community, you might make an effort to please.
But we are so lacking in community, tribe, and this kind of mirroring, and instead, biological psychiatry gives the opposite message: “Sven is beating puppies, so his brain is imbalanced and we must drug him.”
The effect is that the drugs calm Sven, and he has no energy or inclination to beat puppies anymore – so – the perception in the community at large is that the drugs work. But Sven has no opportunity to become a better Human.
Report comment
Thank You Dr Niall and Others,
What exists in “Mental Health” is One Group of people controlling Another Group of people with Potentially Lethal Drugs, with NO Real Accountability Whatsoever.
This Sub Human Approach can easily be compared to how people were treated and killed (with contempt) in parts of Europe in the 1930s and 1940s.
https://www.irishtimes.com/news/crime-and-law/new-inquest-verdict-for-prescription-drug-related-deaths-ruled-out-1.3487104?mode=amp
I finished up with the “Mental Health Services” in Ireland in the mid 1980s.
But in 2003 while working as a Building Subcontractor in the House of Commons, my GP Surgery at London W2 5LT, decided to Register me, for Money, as an Ongoing Severely Mentally Ill Person (without telling me).
My Commented Experience:
https://www.madinamerica.com/2018/05/antidepressant-withdrawal-can-trap-people/#comment-131809
Report comment
These drugs commonly cause Akathisia which is acknowledged to cause Suicide (and disability) – Yet Reporting of the Suicidal connection identified in 1983 is Practically Nonexistent.
https://www.madinamerica.com/wp-content/uploads/2016/11/Suicide-Associated-with-Akathisia-and-Depot-Fluphenzaine-Treatment-KShear-1983.pdf
This is why I would suggest that collectively within “Mental Health”, it can be “Acceptable Medical Policy” to KILL.
Report comment
Niall
Thanks for this, I have read your excellent paper on “Psychiatry As Bullshit” and its the best insight I have read on what is actually happening when you are being duped by your Doctor. I can’t believe I am saying that by the way, isn’t it inconceivable and motiveless for a Doctor to deceive you?
The Chemical Imbalance is alive and well – I have heard from 2 NHS psychiatrists in the last few months saying that “the cause is organic, a biochemical imbalance is treatable with medications” and “its a chemical imbalance that the drugs normalise”. If it were as simple as that then the effect size of the drugs would be significant enough to be really different from placebo, and its not. No, this is designed to make you adhere to your medication but it also rams home the bunkum notion that you are incurable – thanks very much. And then they rather paradoxically say that you could actually come off the drugs in 1 or 2 years, so the “imbalance” must just go away? Clever meds!
For side effects, they are either downplayed or omitted. They are likely to look at you blankly if you say “sexual dysfunction” and say, “well we never hear of anything”. They also believe that the mental dulling effects will get you ”back into life“ when it would seem that the opposite is more likely to be true. They greatly underplay practical measures to get “back into life” so it sounds phoney to me.
Report comment
ConcernedCarer,
In “Mental Health” the doctor would seem not to be looking after the patients interest.
If you look at:-
https://simple.m.wikipedia.org/wiki/Schizophrenia
It says under “Hope”
” …In a family treatment called “Open dialog” in Finland, eight out of every ten people with schizophrenia “get well.” In developingcountries, where doctors use less drugs, 2 out of 3 patients get well from schizophrenia. In western countries, where medications are used as treatment, 1 of 3 get well, but many suffer from drug side effects such as diabetes, obesity, and brain damage.[7]..”
Under “Official Guidelines”
“…Getting support from people who have become well from schizophrenia is also strongly recommended. In family oriented treatment program in Finland, Open Dialog, 8 out of 10 people with schizophrenia get well with no medication or very limited drug use, often only with anxiety medication….”
The evidence from (above) would suggest that a person is better off with NO “Medical Treatment”!
Report comment
Thanks Fiachra and I agree that Open Dialogue and psychosocial routes are the best way forward.
Tying all that back to integrity in psychiatry, the selling line you get is that the drugs are rather like super-effective psychosocial interventions. They would say that the drugs “give you a holiday from your voice(s)” , “help you see the world in a different way”, “think a bit more clearly”, “get you better” and therefore “get back into life”.
Your feelings of hopelessness are significant, but your reasoning is distorted because of an underlying process (which only I understand) that we need to give “a good whack to shift”.
You are left imagining what on earth this underlying process is that can’t be seen, tested or identified, but which we know can be treated with a mega-antihistamine that makes you dopey and fat.
Report comment
Institutional corruption in psychiatry helps to explain why Niall’s paper was rejected from Australasian Psychiatry; why David Nutt was trotted out to publicly defend the chemical imbalance theory following bad press for “antidepressants” in a New Zealand newspaper in the wake of the Mental Health in Crisis tour; and why the RANZCP promotes the mythical chemical imbalance theory in its public “education” materials. Psychiatry as an institution cannot be counted on for integrity (honesty) despite this being one of its core “values.” In reality, it has only one core value: self-defence. That’s why Psychiatry says psychiatrists always provide informed consent despite strong evidence to the contrary. That is what psychiatrists do because, well, that is what they must be doing if they have integrity. To acknowledge otherwise means psychiatrists do not practice ethically, and that can’t be true. Psychiatry says the chemical imbalance theory is accurate, despite a mountain of scientific evidence to the contrary, because it must be true. To acknowledge otherwise means psychiatry has been lying to society for decades, and that can’t be true. Antidepressants work because they must work. To acknowledge otherwise means 1 in 10 people have been convinced to take a drug that does more harm than good, and that can’t be true if Psychiatry has integrity. And so the bullshit continues, brought to you by an institution incapable of honestly examining itself, happy to peddle obvious untruths, and unwilling to acknowledge its shortcomings and act to correct them.
Report comment
These screeds from these assorted shrinks and their associations only further reinforce my belief that med school grads take up psychiatry because they’re incapable of practicing general medicine, but need to deceive their patients into believing that they are real medicos nonetheless.
Report comment
Psychiatry uses the credibility of medicine to misbehave. But I notice medicine backs up Psychiatry. Governments also seem to back Psychiatry up – so what are they getting out of it?
Report comment
Psychiatry serves a useful function to all institutional structures, they provide one means of silencing and getting rid of the awkward squad, anybody who fails to fit in with their expected role, asks to many questions or threatens the status quo. Simply firing someone isn’t always possible and the institution of the family for instance may balk at the cruelty of just showing the door to a troublesome member if they appear to be in no state to care for themselves or simply want to keep a handy scapegoat close at hand.
Report comment
I think “governments” have been in the pockets of the drugs industry – because the overall drug damage has now become too widespead.
Report comment
Agreed, but why did they hand over their power so readily even the so called left have collapsed in the face of a corporate charm offensive?
You’ll recall Corby said opponent to lead Labour was a former senior pharma employee, when did that ever make sense?
Report comment
This is actually a very important question: how come this institution holds power, supremely immune to criticism, able to convince everybody from governments to GPs to commentators and parents that drugs are not just the way to go, but the only way to go. It is a critically important question for the sociology of science. I’m trying to work on it but other things, like drivel from the RANZCP, keep getting in the way.
Report comment
The Mental Health Industry is already very powerful and influential, and I would imagine Public Representatives might judge it necessary for their own interests to support it.
Report comment
The GPs are now being deskilled so they’re keeping their heads down (to a certain extent).
Getting GPs to prescribe antidepressants has also aligned them to “Psychiatry”, and tied them in to a denial of disastrous outcomes.
Report comment
It is a Doctor who is finally called in to decide if the King himself is after all mad!
Report comment
That’s sort of like asking why the prison system has the power to lock people up.
Report comment
A lot of unhappy people. And a perceived means of stopping bizarre/violent criminals.
Ever watched a police procedural drama? No one commits a crime because he’s mad at his cheating ex or wants the inheritance now.
No. It’s always some fancy-pants polysyllabic term from the DSM5 to magically explain what the SMI perp thinks and outwit the madman/woman before they torture the next innocent victim to death. 😛
Report comment
Because the ruling powers in society need them, and because their “diagnoses” shift the blame off of those with the most power and place it onto those with the least. Because it absolves our society from having to do anything about the adverse conditions we create, because those who can’t “adjust” are found to be failing, rather than the conditions they are expected to tolerate.
Report comment
“… medicine backs up Psychiatry. Governments also seem to back Psychiatry up – so what are they getting out of it?”
Mainstream medicine backs up psychiatry because the psychiatrists cover up malpractice, and proactively prevent malpractice suits, for the incompetent mainstream doctors. Governments back up psychiatry because psychiatrists function as social control, outside the rule of law, and the court system. Plus, making people sick with the psychiatric drugs is a multibillion dollar industry today, and our government officials love money making industries.
The religions also back psychiatry because the psychologists and psychiatrists have been covering up the “zipper troubles,” seemingly particularly the child abuse, of the “two original educated professions” for decades or longer, and this is actually documented in their own medical literature.
https://www.madinamerica.com/2016/04/heal-for-life/
This psychiatric child abuse covering up system is by design. No “mental health professional” may EVER help ANY child abuse victim EVER, without first misdiagnosing them with one of the billable DSM disorders. Because child abuse is classified in the DSM as a “V Code,” and the “V Codes” are NOT insurance billable disorders.
https://www.psychologytoday.com/us/blog/your-child-does-not-have-bipolar-disorder/201402/dsm-5-and-child-neglect-and-abuse-1
“We have now sunk to a depth where the restatement of the obvious is the first duty of intelligent people,” I agree. Since it’s already medically known to all, but seemingly those who believe in the DSM disorders, that the “schizophrenia treatments” create both the negative and positive symptoms of “schizophrenia,” via NIDS and anticholinergic toxidrome. And when the treatment is known to cause the symptoms of the disease, it’s highly likely the primary etiology of that theorized disease is iatrogenic, not genetic.
https://en.wikipedia.org/wiki/Neuroleptic-induced_deficit_syndrome
https://en.wikipedia.org/wiki/Toxidrome
So please forgive me for restating this over and over again, I know it annoys some here. But I’m quite certain the majority of today’s psychiatric industry have still yet to get my message. So as an intelligent person, I keep restating it. Especially since “schizophrenia” is the “sacred symbol of psychiatry.” And that is the medical proof their “sacred symbol” is primarily an iatrogenic, rather than genetic, illness.
Thank you, Niall, for speaking out about the complete and total lack of integrity of psychiatry. I’d love to say this is just a problem with today’s psychiatric industry, but it’s not. These are historically systemic problems within all factions of the so called “mental health” industries.
https://en.wikipedia.org/wiki/The_Freudian_Coverup
That’s why the psychological, psychiatric, mainstream medical, and religious industries’ crimes against my children and I were confessed, by an ethical pastor to be, “the dirty little secret of the two original educated professions.”
I’m glad there are some decent and rightfully disgusted within today’s psychiatric field. Thank you for expressing your concerns regarding this lack of integrity and ethics within our “mental health professions.”
Report comment
I will point out that those who disagree with the religious leaders and their hospitals profiteering off of covering up the rape of children en mass. Via the psychological and psychiatric industries’ DSM child abuse covering up BS, are also writing books about the crimes committed by these religious leaders, including the crimes committed against my children and I.
https://www.amazon.com/Jesus-Culture-Wars-Reclaiming-Prayer/dp/1598868330
I’d be one of the many “widows” mentioned in the Preface of this book. My childhood religion’s massive in scope child abuse covering up crimes are remotely mentioned in the chapter on evil in this book.
I have no delusions God is ignorant of these paternalistic crimes. But do know the men and women of the ELCA, who want to continue to have their hospitals profiteer off of the psychological and psychiatric industry’s, primarily child abuse covering up crimes, do want to maintain the satanic pedophilia covering up and profiteering status quo.
One can’t see the big picture, however, unless one develops both the analytic and creative sides of one’s brain. And that cannot be said to be true for those in either the “mental health professions,” nor the religions. Perhaps this is why you’re still “trying to work on it,” Niall? As one with both a business degree and an art degree, I hope my insight helps you see the bigger picture.
Report comment
How are things going as a professional artist, SE? What mediums do you specialize in?
Report comment
Blood makes them pass out. Heh heh.
For some this is actually true.
Report comment
I don’t Know.
Report comment
I actually found this gem from the author’s biographical blurb to be the highlight of the piece:
He occupies himself delving into the philosophical basis of psychiatry, only to find there isn’t one. This has not helped his popularity with his colleagues…,
Report comment
And not much if any medical basis either beyond the allure of medical authority.
No the basis of psychiatry is always political, they are in the business of social control after all, something frequently demanded!
Best to look at your shrink as a politician not as a doctor. And sometimes rare as it is they even use their power benign, but moreover they can usually call on their ace in the hole – The placebo effect – take credit for that and any confounding effects, time limited healing, the person’s own efforts good luck, others efforts and your laughing
Report comment
The SSRI expansion was an example of the Industry taking over the Health Systems. The drugs are now out of patent and lots of Health Systems are now trying to cut the drugs use.
Report comment
“Recall bias”? Boy, that’s rich! People suffer substantial and enduring “side effects” (i.e. debilitating iatrogenic illness) from psychiatric narcotics. For f*ck’s sake, there’s NOTHING to “recall”. Thanks to the #FAKESCIENCE, you are imprisoned in an ugly, uncomfortable, dangerous body 24/7!
Report comment
Until psychiatry takes a position on death it is evading its responsibility as defined by itself. Are its customers expected to live according to a linear materialistic belief that life and consciousness end when the body disintegrates, or with a perspective that consciousness transcends corporal existence? Wouldn’t this make a difference in how one chooses to live? So why is this not seen as a key issue rather than allowing shrinks to approach or not approach matters of religion and spirituality as within the realm of personal choice?
Report comment
Consciousness transcending corporeal existence? You are operating on questions WAY beyond the comprehension of the psychiatric field! They are still having trouble with the idea that someone actually decides what they’re going to do rather than being determined to do everything they do by chemical reactions!
Report comment
Isn’t that sort of like saying that a car driving from SF to LA is caused by the engine, transmission and steering system??
Report comment
In his novel That Hideous Strength C.S.Lewis invented some highly eccentric villains that would have done credit to the Batman movies.
Dr. Frost is one of the most memorable. He is cold and detached as he experiments on people. At a turning point of the book, he indoctrinates the naive young protagonist who is disillusioned with N.I.C.E.–the sneaky corporation Frost serves–and wants to leave.
Dr. Frost tells him that love, hope, affection, goodness, evil, despair do not exist. They are merely chemical reactions in our brains randomly occurring to make us do one thing or another.
During this speech Dr. Frost has no facial expressions and talks in an emotionless almost monotone voice. He acts like a rigid automaton throughout the book. I can’t remember what his specialty was but I think he was a psychiatrist.
Report comment
In the middle ages, there were two types of fool, the artificial fool and the natural fool. The artificial fool was a person who made his or her living through entertainment, often pretending to be a natural fool for the amusement of an audience. The natural fool, on the other hand, was not the sort that had an easy time making ends meet. He or she required a keeper, or, in today’s parlance, what they call a “care giver”. In more recent times, and due to the popularity of the budding service industry, it seems there has been a sharp increase in the percentage of natural fools inhabiting this planet.
Report comment
It might a nice living if it was possible to take the money neat.
(Anyway – there can’t be that many genuine natural fools).
Report comment
The point I was trying to make.
Again, what do you mean by ‘natural fool’? If an entertainer, an actor, a performer, is an ‘artificial fool’, and if a person who can’t seem to manage a personal income is a ‘natural fool’, we are being somewhat liberal (read: figurative) in our use of the word ‘natural’. Contemporaneously it is perhaps better to acknowledge that many of these ‘natural fools’ have been manufactured, that is to say, that they are in one sense or another artificial, too, however, here we are restricting ourselves to the medieval distinction, acknowledging that in some instances a fool can actually be a fool.
The middle ages predated our current craze in medicalization, and the current craze in medicalization has mass produced fools of a natural variety, albeit artificial in substance. Where folly is artifice, what do you have? Cheech and Chong, Robin Williams, Jim Carey, Vince Vaughn, Owen Wilson, Tracy Morgan, etc. Actresses, too, Amy Poehler, Cameron Diaz, Lisa Kudrow, and the list goes on and on. The difference is that in those days you had a small population of what people called fools, and in these days we’ve exchanged the notion of folly for the notion of people with ‘mental disabilities”. Whatever that means?
Report comment
Some people aren’t smart enough to care for themselves. “Mental illness” is another matter.
“Severely Mentally Ill” people would be artificial fools, though mostly involuntary. Lowering people’s brain functions, infantilizing them, and degrading them in the eyes of society are a great way to prevent adult independence.
Report comment
Rachel777
When people Recover in the UK – the Mental Health Services try to pull them back into “Mental Illness”.
Just looking at the information in the Link (below)
https://simple.m.wikipedia.org/wiki/Schizophrenia
“.. In developing countries, where doctors use less drugs, 2 out of 3 patients get well from schizophrenia..
… in Finland, Open Dialog, 8 out of 10 people with schizophrenia get well with no medication or very limited drug use..”
These figures strongly suggest that “Medical Treatment” causes “Schizophrenia” as we know it.
Report comment
Smart or wise?
“Mental illness” is a fiction, not so folly.
In the middle ages, an artificial fool was essentially an entertainer. In my book, if anybody calls him or herself “severely mentally ill”, even in this day and age, that person’s folly isn’t artificial.
Report comment
We can choose to make ourselves dumber than we already are. Any good philosopher knows that. Szazs would agree I think.
Report comment
Dumb and Dumber, sure, that’s artificial folly.
Report comment
Artificial invalidity, or artificial disability, is another matter, not taking the issue to the level of whether of it amounts to out and out fraud or not. Social disability is a lot like social injustice, that is to say, I don’t think disability is the issue at all (in some instances).
Now whether our present head of state is an artificial imbecile, or a natural imbecile, is a matter, I think, requiring further research.
Report comment
Frank,
I was actually thinking about applying officially (with sponsorship) for the job of “Fool”.
Top rates in the UK for looking after a Severely Mentally Ill person are about £200,000 per year (and in my 30 years in this country I havn’t cost a penny, and been non the worse).
My GP Surgery (with an impression of caution) records Severe Mental Illness Symptoms that I don’t have – and havn’t had in my 30 years in the UK.
I think I could be classified as a genuine “Fool”.
Report comment
We’re counting on genuine ‘fools’, who being prepared to risk societies ire by pointing out the obvious defiencies and outright coercion, fraud and self-deceit involved and suggest better means of responding to despair, vulnerability and desperation than manipulating, coercing or exploiting the troubling situation to the max.
Report comment
The author is too generous in ascribing the false statement about “only ever” prescribing after a suitable discussion with the patient to something unconscious like self-deceit. To make a statement about the circumstances of every psychiatric drug prescription ever written, without having been present on all prescribing occasions, is to claim knowledge that one knows one does not have. It is an assumption or a hope stated as a fact, a case of “should” represented as “is” or “does.”
The person who says or writes that kind thing knows damned well how sloppy doctors are iun prescribing psychiatric drugs, but they don’t believe we should know; it would just upset us. They don’t want us upset because they don’t think there’s anything to be upset about. At the core of it is that doctors who say such things do not believe the there is anything terribly wrong with sloppy prescribing of psych drugs. They don’t believe that drugs that have been tested an approved could have terrible effects in real life. We know that the drugs have made us miserable, changed our brains, bodies and personalities, or caused us to lose touch with reality and ruin us. The person who glosses over the reality of how this all comes to be doesn’t believe the drugs cause such craziness. We are psychiatric patients. Exhibiting symptoms is our job, in the way that stepping onto little platforms is the job of circus elephants. Like so: https://pasteboard.co/HmYpaIP.png
Report comment
Of all the categories of persons that declare themselves oppressed or are recognized as such by others, there is only one category that others are allowed, or even required, to deprive of liberty and batter with their bodies, chemicals, and electrical currents, among other things, until they stop seeming to belong to that category.
It is not illegal to be gay or black in the US, although it does inspire others to cause one problems beyond the usual problems of living experienced by all people, just because they’re people.
It is effectively illegal to fit the arbitrary diagnostic criteria of a psychiatric diagnoses, at least in the sense that laws allow or require others to try to beat it out of you.
Report comment
But what happens if the Original Psychiatrist can be proven to be dishonest, and the person recovers as a result of “not taking their medication”.
https://www.madinamerica.com/2018/05/antidepressant-withdrawal-can-trap-people/#comment-131809
.
Report comment
In which case you’re a menace to society–or rather their profession–if it comes to light. No matter how successful you may be or how many people you have helped, you must be locked up, drugged and shocked. For your own good. Plus there’s a 1% chance you MIGHT commit a violent crime in the future they think. So those orphans in Africa will have to find a new benefactor while the MI System sucks you back into a bleak life drugged up in abject poverty subsisting on government handouts. 😛
Report comment
Rachel, You must be Psychic.
Both Dr Simons and Dr Gordon of my GP Surgery, Newton Medical, London W2 5LT have expressed Full Confidence in writing, in my Historical Psychiatrist P A Carney; with Full Knowledge that he was too Psychopathic to work in medicine.
Besides this, there are people Recovering from “Schizophrenia” with the help of non drug alternatives – “coming out” all the time in the UK and Ireland.
Report comment
I recovered from “bipolar” shortly after beginning my taper. Now I suffer physical problems. Chronic allergies and aches and pains for example. These come and go. In a couple years they probably won’t be bad enough to impact my life.
I’m well enough to work part time and keep my apartment clean. Never could on my XXXX cocktail! Struggling to “adult” in my mid forties. Exhilarating but discouraging too.
Report comment
it would be nice if we knew the cause of all this…..
depression and anxiety….
Report comment
My depression stemmed from loneliness and not fitting in. My anxiety stemmed from being bullied/sexually harassed and nearly homeless. (Complex story. An older woman who I thought was my friend got her husband to pressure the board to fire Dad and make our family homeless. Ugh.)
When shrinks told me these stemmed from being defective and hopelessly insane they were adding insult to injury by saying these traumas were no big deal. It was my fault for having a broken brain. Their treatment was and led to further bullying and extreme poverty resulting in homelessness.
Report comment
Rachel that is very sad… what happened to you…
those traumas were a big deal…you make a very good point…I was fortunate……i did have a good psychiatrist…
Report comment
I had one for a while. Then my parents moved and I went too. My next shrink was truly evil. I don’t make the accusation lightly.
She had a sadistic streak. Loved electroshock–especially involuntary. And I never saw her laugh except a couple times when she had reduced a patient to tears.
I don’t care for the psychiatric institution, but Dr. R was–in all justice–the only Evil one I had the pain of being under.
Report comment
I do wonder a lot about how they are able to get away with it. Ludicrous statements like “the cause is organic, a biochemical imbalance, as proven as Darwin”, in practise, don’t get challenged, even though you are smelling BS at this point.
I have concluded that, at certain times, patients and their families are uniquely gullible – and I include myself in that. You are are shocked and bewildered at somethings thats happened – maybe someone has been hospitalized, put under acute services, and you are encountering more medical people in a rather different context than you are used to.
You are trying to learn the facts quickly about the situation you are in, figuring out which drugs to be really concerned about, what dangers and side effects lie ahead, and how on earth one’s life might return to something like an even keel. Its a race against time which the psychiatrist wins. He/she is perhaps much better with words than you expect a doctor to be , and very, very keen to explain in earnest the seriousness of your situation. You might even find yourself in meetings where medical staff nod sagely about the grave risks we now face and how regrettable that we find ourselves in this situation.
You assume you will get a leaflet about the road ahead, and that before an off-label drug is prescribed that will damage your health through obesity or metabolic issues or just plain suicide, you would formally give consent, perhaps in writing. You assume that the dose will increase gently so we are all comfortable, and that you can get off it at any time. None of this happens of course – the first meek “er, OK” and its taken as you are on board. Lots of talk of about “I’ve seen loads of people get through this” and “in my clinical experience”.
By the time you are up to speed with whats going on, and pointing out that you doubled the dose you talked about at the beginning and it still has not brought about some improved view of the world, its too late. Reverse gear is forbidden – “ooh no, I wouldn’t want to come off that (failed) drug”. Instead, its about increase to “therapeutic dose” and adding another drug (but didnt’ you say you would never do that?).
And that is how it’s done. We are all used to fending off window salesmen and cold callers. But when you are in a strange office in a wierd institution, you haven’t slept and you are actually in a form of grief of a former existence that seems to have gone, you are ripe for deception. And you have just been introduced to a professional deceiver….
Report comment