
Most of us know that there are serious issues with the National Alliance On Mental Illness (NAMI) at the national level. And if you don’t know or have any lingering doubts, please oh please, check out at least one of these articles:
- Back to Basics: What’s Wrong with NAMI
- Do NAMI and MHA Suffer from Anosognosia?
- Dear NAMI: My Apologies. I’ve Been Unfair.
In quick summary: NAMI is pro-force, heavily funded by pharmaceutical companies, and one of the lead perpetuators of the whole “we know it’s all a brain disease” myth. In spite of the fact that NAMI leadership has at least feigned moves to reduce pharmaceutical funding due to public backlash, one can still look at their 2017 annual report and spot more than two fistfuls of pharmaceutical companies on their list of corporate donors. There’s also the disturbing addition of genetics-based companies like 23andMe that encourage the average citizen to turn over DNA samples for casual testing. Think on that for just a minute. Seriously.
I’ll wait.
Yet, each and every time I write about NAMI, at least one person approaches me and says, “But not all NAMIs!” People constantly want to let me know that the local NAMI chapters across the country vary tremendously. And, in fairness, that much is true. While many NAMI chapters have busied themselves with such admirable tasks as giving an award to now disgraced Tim Murphy back when he was trying to push through the atrocious Murphy Bill (shout out to NAMI New York!), some of them are undoubtedly more progressive than others. Certain chapters have helped coordinate talks on alternative approaches like the Hearing Voices Network, or invited speakers who challenge the dominant paradigm. I’ve even heard of a few that intentionally avoid pharmaceutical dollars. For example, in 2012, NAMI Vermont pledged to not accept any pharmaceutical money to fund their activities. And, in 2016, they made their annual walk a local event to avoid association with Alkermes, a pharmaceutical company that became an elite sponsor of the national iteration.
So, here’s the thing: I’ll never say that all people associated with NAMI are bad. There are plenty of good people in there. (Most of them, really.) For those seeking support, they often land with NAMI for lack of any other option, and it’s awful hard to blame desperate people for chumming up with the psychiatric equivalent of the devil’s right hand when they’re faced with a choice between the sense of community they might find within versus complete isolation on the outside. For people ending up in employee roles, sometimes it’s about their wanting to make change “from the inside,” or because they’ve been just as lied to as anyone else about the fact that there’s more ways to look at things (or some combination of both). But, none of that changes this small fact: Yes, all NAMIs. Every. Last. One.
Yes, even the local chapters of NAMI are a problem. Saying “Not all NAMIs” isn’t all that far off from any other “Not all” statement. “Not all men.” “Not all white people.”* Because even the best of them are somehow benefiting from the systemic oppression perpetuated by the dominant group to which they are tied. Sure, not all parts that are associated with the whole believe the same things or act in the same ways. And some of them are even willing to go to bat and stand up to their national head over issues like Involuntary Outpatient Commitment (euphemistically known as Assisted Outpatient Treatment), as NAMI Massachusetts (among others) has consistently done. However, they all benefit from the privilege of association with power, and participate somehow in sustaining the imbalance.
For example, being associated with NAMI means…
-
You (NAMI folk) are most likely to be the one to get the call when a local school or other group is looking for speakers.
Because, well… familiarity. And familiarity often means not entertaining even a second thought to look any further. For example, the Western Mass Recovery Learning Community where I work has had a strong presence in Western Massachusetts since 2007, and is home to multiple internationally recognized speakers. Yet in spite of our extensive outreach efforts and local and national media presence, we can’t compete with the NAMI machine. Colleges and high schools will still frequently seek out speakers from the NAMI office nearly two hours away without ever realizing we’re right in their back yard.
I’m aware that might just sound like “sour grapes” to some, but the implications are pretty substantial. If nothing else, behaving as if NAMI is the only act in town creates a self-reinforcing loop that keeps individuals (and perspectives) not associated with NAMI on the outside looking in, and perpetuates the idea that there just isn’t anything or anyone else to know.
When one requests a NAMI speaker, there’s a possibility that they’ll end up with family members or other employees without first-hand experience of their own, either in addition to or to the exclusion of people who’ve lived through it all themselves. However, much more commonly, it’s the ‘In Our Own Voice’ crew who now responds to the bulk of these requests in many areas. This program was developed under the NAMI thumb by and for people who’ve been diagnosed.
Well, sort of…
In Our Own Voice was originally called ‘Living with Schizophrenia and Other Mental Illnesses’. It was first funded in 1996 by a grant through Eli Lilly, which not-so-coincidentally pushed Zyprexa through FDA approval that same year. (Let’s never forget how pharmaceutical industry experts have publicly written about how “advocacy groups” like NAMI are their best marketing tools, as detailed in my ‘Dear NAMI‘ article.) But Eli Lilly funding did not stop there! It continued funding the program at least until 2002 when “Living with Schizophrenia” changed its name to “In Our Own Voice” according to a NAMI press release as follows:
The National Alliance for the Mentally Ill (NAMI) has named one of its premiere education programs-in which consumers with mental illnesses speak directly to community audiences about their experiences with brain disorders, treatment and recovery-in honor of In Our Own Voice, a documentary produced independently by Idaho Public Television (IDPTV) with funding from the Idaho Department of Health & Welfare. The IDPTV documentary includes interviews with NAMI Idaho members and received NAMI’s national media award for outstanding public education in 2001. For more information, click here.
Now, I’m told that NAMI further updated the program in 2017 to move it away from a strictly medicalized view of things. The changes were hard won and are supposed to be significant and move away from the old categories of “dark days,” “acceptance” and “treatment” (etc.) to much broader ones (“what happened,” “what helps,” “what’s next”) that can more readily hold many different perspectives. However, if one looks at the national NAMI website, it’s hard to see sign of that revamp in its generic statement. (Could it be that this is all just a way to appease those calling for a shift while not risking too much of their own skin?) Meanwhile, many local chapters continue to describe In Our Own Voice in the same old medicalized way as they always did. (See, for example, Cook County, Illinois’s detailed description.)
We are actually lucky in Massachusetts that at least some NAMI employees take a more expansive view of the root of their and other people’s experiences, and have for quite some time. However, whether or not all NAMIs across the country will truly follow suit remains to be seen. (Apparently, the deadline for the big shift is in February.) And, regardless, I’m still left wondering whether this undeniably positive shift may do little more at the systemic level than make NAMI national look better, while further securing their relative monopoly on the outreach game.
-
You (NAMI folk) may find yourself with an automatic seat on various legislative committees and commissions.
For example, check out the 21 members of a recently formed Massachusetts commission on “community behavioral health promotion and prevention.” Note that in addition to NAMI being among the 10 organizations (along with the state’s provider lobbying organization, Association for Behavioral Healthcare, and so on) granted a seat, there doesn’t appear to be a single spot that requires anyone to have any kind of psychiatric history (not that one would be enough, anyway).
Legal Authority: Chapter 208, Section 1 of the Acts of 2018
Section 219. (a) There shall be a commission on community behavioral health promotion and prevention located within, but not subject to the control of, the executive office of health and human services. The commission shall work to promote positive mental, emotional and behavioral health and early intervention for persons with a mental illness, and to prevent substance use disorders among residents of the commonwealth.
(b)(1) The commission shall consist of 21 members, as follows: the secretary of health and human services or a designee, who shall serve as the chair; the commissioner of mental health or a designee; the commissioner of public health or a designee; the chief justice of the trial court or a designee; the director of the center for health information and analysis or a designee; the house chair of the joint committee on mental health, substance use and recovery; the senate chair of the joint committee on mental health, substance use and recovery; 1 person appointed by the speaker of the house; 1 person appointed by the senate president; 1 person appointed by the house minority leader; 1 person appointed by the senate minority leader; and 1 representative from each of the following 10 organizations: the Association for Behavioral Healthcare, Inc.; the Massachusetts Association of Community Health Workers, Inc.; the Massachusetts Association for Mental Health, Inc.; the Massachusetts Organization for Addiction Recovery, Inc.; the Massachusetts Public Health Association; the Massachusetts Society for the Prevention of Cruelty to Children; the National Alliance on Mental Illness of Massachusetts, Inc.; the Social-Emotional Learning Alliance for Massachusetts, Inc.; the Freedman Center at William James College; and the Massachusetts chapter of the National Association of Social Workers, Inc.
Whether or not it’s the case here, this sort of thing tends to be the result of many years of high-priced, pharmaceutically funded lobbying efforts to convince everyone that the NAMI voice belongs at every table. Unfortunately, it also often encourages those legislative bodies to believe they’ve somehow ‘checked the box’ for including people with first-hand experience on the matters they’ve set out to discuss, thanks to NAMI’s ongoing efforts to convince everyone that family members are “peers,” too. (Granted, many NAMIs do maintain a percentage of their staff who actually have psychiatric histories themselves, but these legislative seats set no such prerequisite by design.)
P.S. Dear Legislators: Those boxes are still decidedly unchecked. Please bear in mind that most people who’ve been through the mental health system have had their lives interrupted in substantial ways. They don’t understand the complicated legislative process any better than any other average human, and have often been granted even less access to education on the matter than most. They’ve also frequently received the message that their voice doesn’t count (or even that it’s likely to be ignored if they speak up), and they have absolutely no access to lobbyists. If you truly wish to check that box, it’s on you to dig (way) deeper and invite people in.
-
When news happens, you (NAMI folk) are likely to be contacted for your opinion on whatever is going on.
And, if you aren’t contacted, you’re frequently cited as a primary local resource, even if any actual support offered is minimal and there are other groups providing much more substantial resources. In fact, it is my experience that many local NAMI chapter offices are woefully unprepared to support someone who is actually in distress.
In fairness, I should add that many chapters are clear that direct support is not their main gig (if it is their gig at all). Yet, it seems to me that these supposed national experts on psychiatric diagnoses ought to be able to do better than the average bystander when faced with a crisis, and I’m just not convinced — from all I’ve seen — that they’d be able to do that at all. But, hey, maybe with your help we can test that out? Perhaps some of you are willing to perform an experiment: Show up to that local chapter office. Say you’re thinking about suicide, or hearing scary voices. Act really angry or sob uncontrollably. See what happens to you. Frankly, I’d be stunned if a significant number of ‘secret shoppers’ didn’t find themselves surrounded by blank stares, and people reaching for their phones to dial 911. (Note: I’m saying this in jest. Please don’t actually do this. I have no back-up plan for the bad things that may befall you up to and including being shipped off to a hospital. I do not… I repeat… I do NOT… have the personal capacity to bail you out.)
In the end, all this representation basically amounts to free advertising for this already unstoppable self-promotion beast, as well as further access to shaping public opinion which is key to keeping things as they are.
-
You (NAMI folk) may find yourself with new contracts for which you didn’t even have to apply.
For example, recently, a Massachusetts-based funder supplied NAMI Massachusetts with a sizeable chunk of change to research impact and experience of local emergency psychiatric crisis services on the individuals and families who’ve used them. NAMI did not need to apply or engage in any sort of competitive bidding process for this contract. They then used the funds to create a terrible survey devoid of any input from people who’ve been through those services and that basically required people to identify as ‘mentally ill’ in order to even respond. I complained loudly to NAMI and the funder and refused to help circulate it (undoubtedly earning some ire). As a result, the funder did ask NAMI to make some changes to their wording… but they still got to proceed.
Meanwhile, Massachusetts is a state that hosts at least one prominent and well respected research organization that has demonstrated its ability to collect meaningful data with the intentional involvement of people who’ve been ‘in’ the ‘service recipient’ seat in the mental health system (e.g., Human Services Research International), as well as five Recovery Learning Communities where the voice of people who’ve been ‘in’ the system is (at least supposed to be) centered at every level of all they do. Nationally, there’s also Live & Learn led by Laysha Ostrow (who has absolutely worked with multiple folks in the Northeast) that is all about survivor-led research. It’s a wonder in this landscape why said funder would ever think NAMI was the right place to land this sizeable contract, and without any sort of competitive bid process.
In Other Words, All NAMIs…
In other words, NAMI’s existing voice and ‘brand awareness’ serves to only increase their access to financial resources, voice, and power. And it’s not as if we all have equal access to achieve the same results. There is no way for us to quite “pull ourselves up by our bootstraps” here. NAMI’s ability to get to the point where their name recognition was so significant that it all just kind of keeps feeding itself required them to have substantial financial backing from their early beginnings, and included a combination of pharmaceutical dollars and lobbyists supplied directly by Big Pharma. In other words, their willingness to play party to unethical practices is what allowed them to reach this point. And, it’s a point that those who are determined to act with integrity simply aren’t able to attain.
Imagine if it was somehow okay for us all to just “do what we need to do” to build our name and then (and only then) disavow our association with the backers who got us there? But that’s just not how it can or should work. And what this means for those who have done this — those local NAMI chapters who claim to no longer be benefiting from pharma dollars — is that they still basically are… They might be able to minimize their benefit by not taking dollars now, but it’s kind of too late to entirely wash off that stink. It’s how they got where they are, and there’s no denying that fact. In fact, there is another level of ‘gross’ here, because those chapters get to scream “Not all NAMIs” the loudest in some ways, while still ultimately benefiting from the power and privilege that was expressly gained because of the many years of being in pharma’s cushy bed. There’s just no winning here. Even if I’m to believe that some of these changes are for the best (and they certainly are, at least at the individual level), there’s still so many reasons to be mad, and not accept it as “enough.”
And that’s the good ones. The best of the best. The closest to “Not All NAMIs” that there could ever be. Meanwhile, most NAMI chapters actively perpetuate the worst messages. Here are a few examples:
-
- Stigma Warriors: It’s hard to decide which is worse… The massive push that was CEOs Against Stigma and that got championed across Massachusetts with such fervor for a few years that some organizations literally reported feeling pressured to sign on, or the cloying “Stigma Warriors” campaign in Maine that appears to do little more than lead one to a donation button. Either way, it’s clear that NAMIs across the country are far too comfortable getting all self-congratulatory for pouring money into confusing discrimination with marketing schemes (aka all those anti-stigma campaigns that say, “Hey, stop making them feel bad so they’ll accept their diagnosis and go get some of that treatment our funders are trying so hard to sell”).
- Communicating More Effectively: This fabulous NAMI chapter based in the Northeast offered a talk (on my birthday, no less!) called “Communicating More Effectively with People who have Mental Illness”. Terrible graphic design aside, the postcard for the
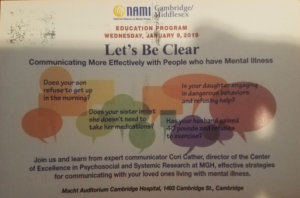 event symptomizes everything from weight gain to sleeping late. Even worse, the designer apparently lacks the insight (yes, I said “lacks insight”!) required to recognize the absurdity of printing those two “concerns” next to one about a sister who refuses to “take her medications” (perhaps because of how much weight she’ll gain or how hard it will be to get up in the morning). Ultimately, the frame of the whole event appears to be, “How to talk your diagnosed loved one into accommodating your own agenda.”
event symptomizes everything from weight gain to sleeping late. Even worse, the designer apparently lacks the insight (yes, I said “lacks insight”!) required to recognize the absurdity of printing those two “concerns” next to one about a sister who refuses to “take her medications” (perhaps because of how much weight she’ll gain or how hard it will be to get up in the morning). Ultimately, the frame of the whole event appears to be, “How to talk your diagnosed loved one into accommodating your own agenda.” - Mental Illness Teachings: Meanwhile, as one Ohio-based NAMI Chapter illustrates, many local affiliates act as little more than a pipeline back to the national site. For example, if one clicks on “About Mental Illness” on NAMI Summit County’s page, they’ll quickly find themselves led back to the national site to be informed about an array of “mental illness” topics. Take “Anosognosia,” for example. Anosognosia is an actual neurological condition that results from damage to certain brain structures typically caused by a stroke or other similar events, and basically boils down to one’s inability to recognize that something is wrong. NAMI national enthusiastically claims that it is a real and proven thing where psychiatric diagnoses are concerned. Of course, it is not, but it sure serves as a convincing reason to not listen to folks and drug them up instead.
- Grand Finale Newsletter: But sometimes people really go all out. For example, another Northeast-based NAMI Chapter let us know what they truly thought about everything from what to do when someone’s in crisis to how to talk to someone who might be suicidal to some gems about hearing voices, all in the very same Fall 2018 newsletter. And, it can be summed up pretty much as follows:
- People who hear voices are very dangerous and scary. (“Auditory hallucinations, or voices, may be giving life-threatening suggestions or commands. The person believes they are hearing, seeing, or feeling things that aren’t there. Don’t underestimate the reality and vividness of hallucinations… In extreme situations, the person may act on these sensory distortions.”)
- Do all the most stereotypical stuff people tell you to do in response to someone who might be suicidal, even though all that stuff has been proven useless or harmful. For example, be sure to ask them things like whether or not they have a plan to kill themselves, and then immediately report them to medical professionals so they’ll never answer that question honestly ever again. (“Are you thinking about suicide?” “Do you have a plan?” “Please remember a suicide threat or attempt is a medical emergency requiring professional help as soon as possible.”)
- People in crisis are extraordinarily dangerous… kind of like ticking time bombs. Be. Very. Careful. Run, if you need to, and feel free to do whatever needs doing behind their back because, well, they’re kind of like a wild animal. (“Avoid continuous eye contact.” “Move slowly.”)
But, that’s okay, because they love and accept you (just read their newsletter and you’ll see!), and a god that you may or may not believe in also loves and accepts you… So, they’re just going to proceed like you believe in that (every last one of you, no matter what you say) because who cares what you believe in or not, anyway. After all, even though they “accept” you, they still know you’re crazy, and their belief system is the dominant one and they have more power than you. So, they don’t actually need to care what you think.
Playing Twister with NAMI
I’ve watched organizations contort themselves for all these ‘Not all NAMIs’ based on a wide array of justifications. Sometimes they are even doing so in an effort to try and build enough of a rapport that NAMI might someday be influenced to change. And, in some ways, I can appreciate that strategy. Hell, I’ve implemented it myself in other scenarios. Yet, my question to such organizations and groups is: How’s that working for you?
Is the time and energy invested actually getting you the results you want? What have you had to give up or compromise on as a result? And what groups with even less power than yourselves might you be harming along your way to trying to tap into the power that NAMI currently holds? Is it all actually worth it? And, if not, wouldn’t your energetic resources be better spent elsewhere?
I just recently had an argument with a friend on this topic. He suggested that if we could just reach some of the lowest hanging fruit — the local NAMI chapters that seem most open to change — that perhaps those local NAMIs would then take on the task of influencing the national NAMI to change, too. I don’t buy it. Not for a second. All I see being accomplished is our spending our energies working on an impossible goal when we could be working on something else. Another common feature of systemic oppression is the tantalization of marginalized groups who are somehow convinced to willingly turn so much attention to unwinnable battles, rather than doing something productive. It reminds me of my high school physics class where we compared the energy created by pushing on an immovable wall, versus a heavy stone that, while hard to push, will actually roll.
However, my friend did make one point that caught my attention. Specifically, he suggested that maybe if certain local NAMI chapters could be so radicalized as to, at some point, choose to drop the NAMI name and affiliation altogether, we could perhaps make some progress. Now, there’s something I could get behind. How best to chip away at a gigantic force than to convince some parts of its actual body to fall entirely away, and morph into something unrecognizable as once being a part of the whole? There are, in fact, people in some of those NAMI chapters doing good work, and maybe this is a way for that good work to stay good, and not inadvertently strengthen something bad.
But, of course, that would require all those local chapters to give up the power and privilege they gain through that affiliation. They’d have to be willing to not only speak differently, and argue for different things, but accept that they’ll face much bigger challenges and barriers simply for excommunicating themselves from the parent with all the power.
Until then, I’m unconvinced. Some NAMI chapters may not be taking (as many) pharma dollars anymore, but they’re still benefiting from all the years that they did, and that NAMI national still does. They may now be at the start of offering more varied narratives about what “mental illness” is and how to move through it. Yet, this comes only after decades of harm caused by the “mental illness is just like diabetes” empire that’s been built, and that continues to thrive. I’m interested in the dismantling, not the building further up. The building further up scares me, even (and maybe especially) if some of the new blocks are made of good, solid wood.
Now, I should add that inevitably I’ll get some backlash for this piece. There’s a certain expectation that we all exist under a “big tent” that welcomes “many perspectives,” and that anyone who bucks that is the real problem. (See also: It’s a Circus Under This Big Tent.) Yet it seems just a little bit strange that I should be expected to “play nice” with a group whose history includes fighting for all the most damaging, force-ridden and dangerous ideas and actions (and sometimes lies) against people that my job and my life and my values demand that I defend. Stranger still that I should be the one at risk for exclusion (new diagnosis: “Doesn’t play well with others!”) should I not be willing to do so. And, strangest of all that I — with my tiny fraction of access to any speaking platform at all — should be critiqued for using it to speak my truth, and not wanting to share with people who have already claimed the other 98% or so of platform real estate on this particular topic.
In reality, I don’t need to pretend that what’s been said and done hasn’t been harmful for the sake of aimless diplomacy or avoiding conflict. I’m going to have to accept the losses that come with speaking truth, because I can’t accept the losses that come with silence. Because why on earth should those who’ve been harmed be expected to go out of their way to keep those who’ve done the harming comfortable, or to make space for them to continue to do damage? Where does the idea that that’s how it should be even come from? I’m not the one who owes a debt, here. But I won’t be holding my breath for those who do to fully pay up any time soon.














thanks, sera davidow. 🙂
I, too, pretty much argue that it is, in fact, all NAMIs. Here where I live, in my situation, my “non-compliance” did not sit well with the local NAMI people. They seem to function like an extra layer of brain washing and enforcement, in the “asylum without walls.”
One could ask–as I have asked myself– “well, what’s the harm? people who have been thru the system need support, and so do their loved ones, right?”–to which I would now reply (yes, to myself, even…crazy, huh?) “there are far better ways of spending time and money” and “if a family aims to suport a psychiatrized individual, NAMI is going to prove detrimental, in potentially catastrophic ways.”
so, once again, thank you. I actually read over one of your previous articles, on the fabulous Big Pharma funding of NAMI and friends. I vaguely recall seeing something similar in Mother Jones, but then…I kind of lost interest in Mother Jones when they featured an article by a lady whose family member was labelled with “schizophrenia” and ended up dying in her 50s, after receiving “high quality care” that included long acting haloperidol injections for a long, long time. Now, that’s a true blue “progressive” for you, isn’t it? ugh.
Report comment
Thanks, yeah_I_survived.. .For reading and sharing some of your own experience. I missed that Mother Jones article (ugh), but yeah, I wish the “liberal” ends of our media and society in general weren’t so hell bent on keeping their head in the sand where psychiatric oppression is concerned. I actually wrote an article about that at one point, too… :p
In case anyone’s curious about that one: https://www.madinamerica.com/2016/04/dear-self-proclaimed-progressives-liberals-humanitarians-youve-really-messed-one/
-Sera
Report comment
Psychiatry is the religion of the faux left. Don’t expect their help.
Not sure this is a complicated matter. NAMI is our enemy, plain & simple. It needs to be defeated, not argued with.
Report comment
Not really expecting help… Just wanting to say my piece, Oldhead. 🙂
Sera
Report comment
Thank you for you for writing this important article. As a LPC I’ve heard usually good things about NAMI from others in various MH systems. Most professionals I’ve heard talk about NAMI don’t say anything critical. They assume that speakers bureaus, education, and outreach are all worthy activities because it can decrease stigma and increase engagement in treatment. Not until reading MIA did I realize the harm done by groups like NAMI. I have assumed that they do good work, but of course that is the convenient narrative for paid helpers to believe (especially when we’ve been indoctrinated by the culture of “mental health treatment”). I was a victim to being “educated” about only one point of view, the disease model. Every place I have worked uses DSM codes to bill, and even that was never presented as a potential problem for the people we supposedly care about, our clients. There’s a lack of critical thinking in medicine and MH systems. We all go after the money and disregard the harm which is being perpetrated by the system, such as forced hospitalizations and drugging. NAMI has no issue with continuing the status quo because it works for them. This is the same with psychiatry, APA, DSM, MH centers, and Big Pharma. Nearly everyone is getting wealthy (well, NAMI employees don’t get paid much or are volunteers) off the suffering of others, but they convince themselves they are compassionate and doing good work. Cognitive dissonance is strong amongst these groups.
Report comment
A wile back I called the NAMI helpline 1-800-950-NAMI (6264) and asked if they took money from the pharmaceutical companies. I couldn’t tell if they were instructed to lie and tell me no or if the volunteers were just ignorant.
I called several times and talked different people and then got someone that sounded like a supervisor.
I got the sense that supervisor guy was upset that I caused problems by getting the volunteers to start questioning by asking why if NAMI was a patient advocacy organization why doesn’t NAMI have anything to say about rampant abuses behind psychiatric locked doors or crimes by the pharmaceutical industry such as the Risperdal and Zyprexa scandals.
Report comment
Good job.
Report comment
Wow, nice work, the_Cat! What exactly did they say when you asked about pharma money?
Report comment
I don’t remember the exact words but they deny it.
This was 2 years ago. http://www.madinamerica.com/forums/topic/someone-call-nami/
And this, https://www.madinamerica.com/forums/topic/write-a-review-for-nami-om-yelp/
Bummer my review is gone, everyone pile on some Yelp reviews of NAMI ! Link above.
Report comment
Thanks for sharing your experience here, Shaun! And for taking the time to read all this and be open to things being different than what you were first told. That openness is so important. 🙂
-Sera
Report comment
Another excellent stab at what’s wrong with NAMI (almost everything).
Anosognosia in particular is one of the more insidious accusations made against patients because it’s so patently false almost all of the time. Anyone who has witnessed a stroke can describe it. (During my fathers first major stroke, he did have to be threatened with arrest by a police officer before he complied and got in the ambulance, and in the emergency room all he wanted was the remote control with no TV in sight. It’s a very clear clinical presentation.) Instead, the way the term is used against psychiatric patients is really “we know this is best for you despite anything you say about how it effects you and whether those effects are tolerable so we’re going to force you to do it and it’s really for your own good“.
I was never involved with my local nami chapter and am lucky I suppose to have a family that doesn’t care what happens to me, and certainly wouldn’t waste their time at a support group they thought would help me. Given the alternative, I’m going to interpret having a terrible family of origin as a net positive.
Anyway, it’s always good to get a refresher on anti-NAMI talking points since they’re the biggest name in mental health consumer advocacy. (‘Consumer advocacy’ being their only real point which makes them little more than a well coordinated lobbying group.)
Report comment
As in advocating that people consume “mental health”?
I debated some NAMI people at a public event when they first were getting started in the late 70’s/early 80’s. Got a standing O, and lots of agitated abuse afterwards from the NAMIs, when i pointed out that “concrete thinking” (a “symptom” of “schizophrenia”) is exactly what psychiatry engages in when it talks of “mental illness”; hence by its own logic psychiatry is “mentally ill.”
Report comment
“As in advocating that people consume “mental health”.”
Well, yeah, essentially. From everything I’ve read, their mission does seem to be to act as a thinly veiled PR arm for the pharmaceutical industry, using concerned family and friends to coerce people into not just taking their meds but singing the praises of their “illnesses”. The people I’ve known who actually have been involved in the local NAMI chapter seem awfully committed to their diagnoses and drugs and “recovery” as it pertains to being a compliant patient.
Report comment
Actually it’s “mental illness” they want us all to swallow. 😛
Report comment
Thanks, Kindredspirit! For reading, and especially for sharing your experience as to what anosognosia truly is!
-Sera
Report comment
Some kind of dessert?
Report comment
Thanks Sera. This is so very frustrating because an agency which is supposed to “ help” many times is doing the work of the devil with out even being aware. It is like the parable of the 12 blind men trying to describe an elephant- 12 different versions of the truth without any any coherence.
I think this is part and parcel of other disabilities and medical condition groups. It helps to have folks in the know but as long as there are particular founders who are using these groups for profit and greed nothing great will come out of any of these agencies.
The divide and conquer routine started early with some states funding both MH and DD and others funding each group into very unequal ways. And there was stigma but it was used against the families. It was okay to have a DD child but never the other way around.
A tangled tangled web. For decades parents of DD kids were told at birth forget you ever gave birth to this child. So there is that. And on and on in so many ways for so many things and especially HUNAN BEINGS.
I go back to trauma and maybe there needs to be a category pardon the word here shock. People go into a physical Cascade condition why not with emotions as well. This would help explain why sometimes fir whatever reason some folks see some sort of results with medication.
And a NAMI is not subtle or nuanced and maybe because there also is a bbbule most folks live in and unless they see the hand writing on the wall- they continue to be unaware and unwise.
Report comment
I’m going to suggest to some people I’m working with that we create some downloadable literature that can be printed and distributed outside NAMI events anywhere in the country. Others can do it too.
Report comment
Thanks, Catnight! That’s for sure… that NAMI isn’t subtle or nuanced! So frustrating that people continue to live in that bubble and just can’t seem to see what’s right in front of them.
-Sera
Report comment
Sera, this is a great article for which I’m grateful. But…DUH!
Report comment
Fair enough, kumininexile! I wish it were a ‘duh’ for more people, though!
-Sera
Report comment
I appreciate the perspective of unearned privilege that you lay out in this piece. I had not really thought of it that way, but it makes total sense. “There are some good ones out there” doesn’t do a thing to address systemic oppression, and in fact impedes the effort. I love the idea of convincing local NAMIs who “get it” to go rogue and disavow the NAMI moniker and all the nasty history (right up to the present!) that goes with it. I’d love to see that happen, but even people with respectable levels of integrity have a hard time walking away from privilege, however unearned it may be.
Thanks for another great article!
Report comment
Thanks, Steve, and yeah, for sure you’re right. It is hard to walk away from privilege. Even for generally good people. I wish it were otherwise.
Sera
Report comment
Much like the APA when it underwent a facelift by ousting the psycho-dynamic with the DSM-III and reactively defending itself as a “medical” profession, that is, a matter of “biology”, NAMI arose from a group of family members who lock up family members worrying about the way they were being depicted and characterized. That’s right, just in case anybody was wondering, NAMI was not started by those family members who were being locked up. It was started by those who were putting their kin into institutions.
NAMI was founded in Madison, Wisconsin by Harriet Shetler and Beverly Young. The two women cared for sons diagnosed with schizophrenia, and were tired of their sons being blamed for their mental illness. Unhappy with the lack of services available and the treatment of those living with mental illness, the women sought out others with similar concerns.
https://en.wikipedia.org/wiki/National_Alliance_on_Mental_Illness
I’m saying the above is primarily myth. The two women were NOT tired of their sons being blamed for their [sic] mental illness. The two women were tired of these boy’s mothers being blamed for what were seen as their son’s emotional disturbances. You see, in the seventies there was a lot of blaming family members who lock up family members for the state those family members that got locked up found themselves in. Letting everybody off the hook, the serious business of treating people who don’t want to be treated can go on unimpeded.
NAMI is a later development of the same mental health movement that earlier gave rise to the MHA. In all truth, it is not a mental health movement at all, it is a mental health treatment movement, and, more fundamentally, it is a medicalization movement. A medicalization movement is a movement to treat people who are not sick as if they were sick, and as such, it is something that all decent and honest people should oppose.
Report comment
Thanks, Frank. I totally agree that it is a treatment/medicalization movement which is precisely why NAMI has been such a tool for pharma… that’s precisely the point made by the pharma exec I’ve quoted in multiple nami articles (he talks about how these “advocacy” orgs are better marketing instruments than any “direct to consumer” ads ever could be).
Sera
Report comment
Frank Blankenship, I haven’t as yet seen what wikipedia has on N.A.M.I. Do you know who Mike Finkle is, however? When I was working as a peer counselor in On Our Own’s drop-in center in the mid 1980’s, Mike was the second in command there. He was, and still is, involved in a tremendous amount of statewide advocacy. Back in those days, there was a statewide advocacy coalition which consisted of the Maryland N.A.M.I., the Maryland M.H.A., On Our Own, and an umbrella organization representing all of the psychosocial programs here. For a while, Mike was the entire coalition’s lobbyist in Annapolis. Mike introduced me to Jim and Carol Howe who lived in Montgomery County, MD, and who Mike told me had founded N.A.M.I. in the late 1970’s. Of the two of them, Carol was the more accessible one. She once bought me a drink at a coalition function. This was quite some time ago, and I don’t have any idea what happened to them. But the story I got from Mike was that N.A.M.I. began in Maryland.
Report comment
Apparently Mike Finkle is the executive director of On Our Own of Maryland Inc. If I met him, which is quite possible, he didn’t make a lasting impression.
NAMI seems to have started in Madison Wisconsin. It now has affiliates all over. I just relayed what I picked up on the origin of the organization from wikipedia. I suggest that possibly Jim and Carol Howe had something to do with the founding of NAMI Maryland, the Maryland chapter of what is now a national organization.
According to NAMI Wisconsin…
NAMI was formed in 1977, when Harriet Shetler and Beverly Young, two mothers, each with a son with schizophrenia, met over lunch to discuss the similar challenges they shared raising a child with a serious mental illness. At a second lunch, the women, both active in civic and charitable activities, decided to assemble people with similar concerns.
https://www.namiwisconsin.org/mission-history/
What do we do with our problem children, I ask you? Well, some of us would lock them up and throw away the key.
Report comment
Hi Sera,
are you just venting or looking for solutions? Not blaming you if you are just venting. I know Will Hall vents here sometimes, too, on the lack of progress.
I’ve often wondered what it would take to change things. My own failed attempt on my little blog to connect with other SO’s only left me with wondering what I did wrong, wondering if my wife had simply been willing to join me, would others have listened then? Wondering if I had just found the right ‘benefactor’ would that have enlarged my voice and audience? Wondering if I could get out the ‘love-story’ between me and all my wife’s ‘alters’ (I just got engaged to the first new girl. I’m pre-engaged to another. A third has expressed interest in doing so, and all the other little ones are deeply in love with me as a daddy figure: and it’s mutual on my side), would that bypass people’s defenses and apathy and make them willing to listen?
But, alas, I have no answers; just sadness that I failed and no matter how many times I’ve begged my wife (all of them) to join me and see if that changed the dynamics, she is terrified of the stigma this culture has about d.i.d. (thank you, Switch, et al, sigh).
Sam 🙁
Report comment
Sam,
I would frame what I’m doing here largely as offering food for thought, and material to counter those who continue to argue in favor of these large entities like NAMI, MHA, etc without unpacking what’s really going on.
That’s neither as personal as venting, nor as productive as offering a solution… but I do see it as being on the road to the latter… or at least a necessary part of ever getting there.
Sera
Report comment
Sera,
I’m sorry the real point of my comment got lost in a poor attempt at a joke, of sorts. But as I re-read that first sentence, I can see why you took it the way you did.
Sorry,
Sam
Report comment
I wasn’t offended! Just clarifying 🙂
Report comment
are you just venting or looking for solutions? Not blaming you if you are just venting.
This is an insulting and inappropriate comment. It also falls into the well-known trap of “don’t criticize if you don’t have a solution,” which is a sop to the status quo.
The “solution” to NAMI is NO NAMI!
Report comment
In my research, I have found NAMI in my state to be one of the most exploitative organizations of all times. There is one big wig at the top, Sue Abderholden (she earns 6 figure salary I believe), who is the paid mouthpiece, her board of directors and then the legions of “volunteers” who work for nothing. Family members and those with lived experience are being used to push NAMI’s pro “treatment” sales pitch like a legion of lemmings pushing their way to the water. The worst part is that these people are vulnerable and taken advantage of. That and the families having the “support” to abuse the identified “ill” person with NAMI’s blessing.
I also notice that though NAMI is trying to steer itself away from their dependable pharmaceutical money, they are simply supplementing it with ties to “healthcare” facilities.
Report comment
Thanks, Squash. Healthcare facilities, and as I noted above, genetics testing places. All very disturbing. Thank you for taking the time to comment and share your experience!
Sera
Report comment
Trolling NAMI discussion groups
I complained that “my cousin” was abused inpatient, described the usual nightmare, and that now he refuses treatment because of it. What advice will they give me ?
https://www.madinamerica.com/forums/topic/trolling-nami-forums/
Report comment
I was enjoying your article Sera until you insulted me by saying “Not all white people. Because even the best of them are somehow benefiting from the systemic oppression”. Well, my white mother who came from Sicily was terrorized by a drunken abusive father. She worked for low wages in a sewing machine factory until she retired. How did she benefit from the systemic oppression? Or me, for that matter who had to struggle to make it through school and work without the benefit of knowing how to navigate through middle and upper middle class society because my working class parents didn’t have the knowledge to teach me. There is no reason, Sera, for an article on NAMI to veer off into a gratuitous attack on white people who are supposedly enjoying some unspecified privileges.
Report comment
There is of course the theoretical possibility that somewhere there is a Black woman who has lived a completely parallel life to your own in every respect, except for her race, in which case you would have an edge via “trickle down” white privilege. It could also be argued that you are suffering from class and sexual oppression rather than racism, which would be true. Nonetheless, claiming that the degree of success you have achieved is primarily the result of “white privilege” should be rightly seen as offensive. The “mother of all oppression” is capitalism, which is fed by the others. Capitalism is the “system” people never seem to specify when they speak of “systemic” oppression.
Report comment
Marie,
I can’t be sorry that I included reference to white privilege in the article, because it’s real and it’s important to keep recognizing that fact. But, I am sorry that you received it as an attack, because it surely isn’t one at all. I know it can feel awful, however, to feel as if someone isn’t seeing your own suffering. I believe that you and your family have really struggled, and faced lots of adversity.
I don’t think that that changes that you’ve received from benefit from your whiteness, but I believe that that’s been much harder to see or feel because of all the other benefits you haven’t received.
In the end, privilege really isn’t about the person who possesses it being bad, or not having earned much of what they’ve gained. Rather, it’s about the reality that our society has been built and sustained by people who’ve had their own needs and wants and beliefs most in mind… That means that society centers and prioritizes mostly white, male, cisgender, christian, heterosexual, able-bodied folks with some wealth and education. And for each of those (and other relevant) qualities that one does not possess, there are at least a few more barriers in their way to the success… and people from the dominant groups blaming them for having a tougher time because many from those dominant groups can’t even *see* the barriers the marginalized group might be tripping over… because that’s how privilege works.
Anyway, here’s a couple of samples of what’s out there about white privilege if it’s of interest:
Joy Degruy presentation on Post Traumatic Slave Syndrome: https://youtu.be/BGjSday7f_8
Joy Degruy clip on white privilege: https://youtu.be/dCv4luaBfk4
Article on white privilege: https://www.washingtonpost.com/blogs/post-partisan/wp/2016/01/16/white-privilege-explained/?utm_term=.d7571600149c
Sera
Report comment
Looks like you didn’t respond to Marie’s concerns at all other than to say, basically, “sorry if I you were offended,” repeat your own rhetoric and post a few links to support it. Why is the word “capitalism” so hard to say? Once again you talk about “systemic” oppression, but fail to define that system
Report comment
Capitalism is NOT the problem, nor is socialism the answer. The black and white fallacy going around this website gets tiring. You want socialism and to see how destructive it can be, just look south to Venezuela. And the Scandinavian states that everyone on the Left likes to point to are NOT socialist. They simply have a much bigger social, safety net than we do, but most of their industries are privately owned.
I would argue that Wall Street is much of the problem. It’s completely out of control. I read an interesting op-ed from the Left this past week that explained why OAC’s call for the 70% tax rate on the 1% is based in the history of this country, and has some good reasons for it. If I remember my history correctly, CEO’s in the 70’s made something like 60x’s the average worker, now it’s more like 400+. That’s immoral. But it’s just as immoral when I went to St. Martinique last Fall, a socialist paradise under the rule of France, and more than 40% of the populace doesn’t work because of their brand of socialism.
So, no, I don’t agree that capitalism is the problem. I believe an a-moral and unfettered capitalism is the problem. But on a similar note, I believe socialism could work under the right conditions, too, but certainly not one like we see in Venezuela or even more benignly in St. Martinique were laziness and sloth are tolerated.
Let’s talk about social nets. Let’s also discuss the value of work, even if it’s not one’s dream job. I have a college education but have worked in a factory for 25 years. I never would have chosen this, and I still hope to leave and do what is in my heart when my wife is in a better position, but this job has enabled me to raise our son and take care of my family, and for that I’m thankful.
Sam
Report comment
Hugo Chavez was elected president of Venezuela in 1998 with 56.2% of the vote, during the 14 years he was in elected office his socialist policies saw average public and private growth at around 3%, while significantly reducing poverty, inflation, unemployment, childhood malnutrition and so on. Spending on education, health, housing and social security increased to almost 25% of GDP by 2011. Compared to the state of the country under the prior failed capitalist oligarchs’ governance, Chavez’s socialism was a great success.
It galls me when I see people blindly quote the mainstream press, with their abysmally lacking critique of the socialist state in Venezuela, while ignoring the actual causes of the problems, both there and in other countries. What an amazing job the US government has done in producing a compliant population with such poor critical thinking skills that they can be so easily manipulated and propagandized into believing just about anything.
The problems in Venezuela are not caused by socialism, the issues there are caused by the same deposed capitalist establishment who sucked that country dry in the first place. They want power back, they want their high profits back and are willing to make the people suffer to get what they think should rightfully be theirs. Over the years these monied interests worked to undermine Chavez, and after his untimely death continue to do so under Maduro. They’ve been assisted by the capitalists in the US who themselves are threatened by the success of any socialist system. The US is a major contributor to the problem in Venezuela (and in fact the entire world) through both covert and overt actions. The belligerent and illegitimate American government can’t allow a socialist society to exist and thrive, if their own people saw non-capitalist society consistently exceed the propagandized expectations of their mass media, they might finally see through the lies and revolt, ousting the capitalists and ushering in a similarly structured people-centric society.
But enough on Venezuela, let’s talk about the value of work. A worker in a capitalist society such as the US produces wealth that does not benefit herself as much as it does her employer and her government. The employer arguably takes the majority of worker generated value and redistributes it to pay the supervisory management structure, the board of directors, shareholders and others who do little to nothing themselves to deserve this excessive reverse socialism. To add to the injury, the government skims off an additional percentage to redistribute to the war machine while throwing the odd penny towards social programs. While our labor is being stolen and we are being exploited to benefit the idle rich, it remains very difficult, if not impossible, for most to leave work. In fact unless you’re one of the wealthy your participation in this system is mandatory. If you leave work you will lose your income, healthcare, potentially also your shelter and then any possessions you may have. You may lose your children, ending up on skid row in a shelter or living on the streets. I would go as far as to state that work in a capitalist society is essentially equivalent to paid slavery because it is impossible to leave and continue to survive.
Meanwhile in a more people-centric socialist system, yes, the government will take a portion of the wealth generated and redistribute it to those who have no work and to pay for social programs like health and education, but the advantage there is obvious – if you find yourself with no work or have to leave work, then you are on the receiving end of that redistribution, you continue to benefit from provided healthcare and education and also have a minimum stipend to live off. A fully socialist society cuts out the minority who are the profit takers, those sitting in their mansions idly enjoying the lion’s share of the labor stolen from the majority.
Socialism more fairly distributes the efforts of society as a whole to benefit everyone equally, so that those who can’t work can still live. Meanwhile Capitalism promotes selfishness and hording by the few to benefit themselves, promotes international wars and theft and generates environmental destruction as it attempts to continue the ponzi scheme of ever increasing growth in a world of finite resources.
Report comment
Sam Ruck
you said:
“I don’t agree that capitalism is the problem. I believe an a-moral and unfettered capitalism is the problem.”
With the above statement you are saying that there is somehow such a thing as “moral capitalism” and “fettered capitalism.” These kind of statements are ALL oxymorons AND utter nonsense.
Capitalism is inherently exploitative and immoral, and can never be fundamentally fettered.
Capitalism NEVER allows anyone BUT the capitalist class to run the system AND make ALL THE essential decisions.
By its very nature, capitalism leads to periodic economic crises, poverty for the underclasses, racial and sexual divisions with related forms of oppression, environmental destruction, and multiple forms of war, including planet threatening world war.
We (humanity) better figure pout how to make socialism work, because it is the only thing at this stage of human history that can save the planet.
And Sera, good exposure of NAMI and many questions surrounding how to deal with it.
While I do not think every blog needs to target capitalism as the ultimate enemy, far too often people (like Will Hall and others) make grand pronouncements about the “system” and the “monied elites” without ever really defining the actual class and type of system we are dealing with.
Given the urgency of the domestic and world situation situation, overall we really DO need more and more discussion (by drawing real world links) about what is the ultimate root of modern day oppression in the world.
Richard
Report comment
I have to be honest, Oldhead, that sometimes I really do wish you’d give it a rest. You seem like you have so much time to spend in these comment sections actively derailing things, and it can be exhausting to even try to keep up.
Her main point was that she felt I’d insulted white people, and discounted her experience. I did my best to illustrate how that is a misunderstanding of what I said which isn’t an insult toward white people at all.
*You* are the one bent on dismissing that in the name of naming capitalism. Of course capitalism has a role in all this, including the fact that it is capitalism that drives big pharma to use groups like NAMI as they do. And that’s not the whole picture, and none of this – not even the white privilege part – was central to the actual point of this article… although overal features of systemic oppression certainly are.
Sera
Report comment
I have no doubt that you wish I’d hold back, as logic does have a way of “derailing” manipulative arguments.
Of course capitalism has a role in all this, including the fact that it is capitalism that drives big pharma to use groups like NAMI as they do.
Although you don’t realize it this statement exposes the bankruptcy of your narrative. You obviously consider capitalism just another “ism,” like ageism, “paternalism,” “looksism” ad nauseumism. This is at best a petty bourgeois point of view.
Capitalism is not an “attitude,” it is the death-dealing, soul-crushing apparatus that grinds our aspirations into dust, no matter how that specifically manifests in the lives of particular oppressed individuals and groups. It is the “Mother of All Oppression,” if you will. It does not simply “play a role” in psychiatric oppression, it defines our existence. And you clearly don’t get that, and in practice you have often succeeded in divided people against one another in the name of “fighting privilege,” rather than applying your supposed understanding of how forms of oppression “intersect” to promote unity in the struggle against capitalism. Richard Lewis has repeatedly pointed that out to you as well but it falls on deaf ears.
Report comment
You can also leave NAMI.
I left NAMI myself. It was not much of a privilege to be one of their subhuman drug mascots. We were only allowed to say a few words at public functions–in praise of the drugs. (I always wondered why they didn’t make us better.)
About us without us. Seems all the NAMI chapters in my state are based upon the bio–control-force model.
Report comment
Apparently as many people are addicted to NAMI as they are to Fecesbook (it just came out that way but I like it). 🙂
Report comment
Lol.
Report comment
The idea that by being white you have more privilege than non-whites is a really simplistic concept. Your other categories of privilege are also suspect. Christian? I’ve known many happy and extremely successful Jews. Male? Some of the most successful people I’ve known are women. Heterosexual? There are plenty of very successful gay people, especially in the arts. Black? I’ve known very successful black men and women, and what about our last president. I could go on. The fact is that no matter what characteristics you have there will be positive and negative impacts from the social structure that you live in. Do some groups benefit more than others? Yes. Is society unfair? Yes, but in many ways that your concept of white privilege doesn’t even touch on. And whether you intend it or not, you are insulting white people.
Report comment
Systemic oppression and privilege do not preclude the success of members of those groups, but it does speak to the default design of society. For example, our holidays and workweek and how many people are afforded time off are structured around a Christian perspective. When kids are forced to stand and say the Pledge in school or people are asked to swear to tell the truth in courts, a Christian perspective on god works its way in. Presidential candidates suspected of not being Christian have had to go out of their way to prove that they are. These are just small examples, and don’t predict the outcome or impact for each individual which will vary significantly… but it seems strange to me to suggest that folks who follow a Christian practice aren’t privileged in this society in ways that make their way of life at least a bit easier.
It doesn’t seem as if we will come to agreement on this. I believe that the insistence on seeing this as insult rather than a reality of the fabric of our society is a part of what keeps these things in place, and that seems really sad to me. But I don’t really know what else to say about it, and I don’t think it’s worthwhile to get into an extensive argument about it here.
Sera
Report comment
Removed for moderation.
Report comment
Nope, it’s really not all that simple. The richest majority black county in the country, prince george’s Maryland had one of the highest subprime mortgage rates in the country. Not because this community didn’t qualify for prime mortgage rates, but because they were easy to exploit.
Driving while black effects rich black people just as much as poor. In fact, due to racism in policing, a black man driving a luxury vehicle can be seen as suspicious behavior.
Systemic racism (and misogeny) makes its way into medical care because most research on illness and medical treatments is done on white men, and a POC seeing a white doctor is unlikely to receive care optimized for illness (and presentation) that is prevalent in the black community.
Black offenders are more likely to be given harsher sentences even from black judges.
Black children’s behavior is more likely to be seen as malicious or predatory or a sign of serious psychiatric illness than white children.
Black communities are more likely to be effected by industrial pollution due to zoning laws and city planning (going back decades) with very overt racist intentions.
Tying educational funding to real estate values has meant black communities get FAR fewer dollars per student than majority white suburban communities with higher property values.
And that’s not even to mention the fact that this country was literally built with slave labor and our capitalist monetary system thrives on wage slavery (and outright slavery in prisons effecting a disproportionately black population.)
It’s actually astounding how deeply ingrained the systemic forces are that keep POC in a place of struggle while shaming them for not achieving the myth of the white American Dream. Touting the success of a tiny percentage of a group (women, gays, Jews, and POC) to prove that white people have no systemic privilege is a huge slap in the face to all those who have died or suffered in many ways from these systemic injustices that happen every day right now here in the 21st “colorblind” century. This is the world we live in and this kind of racism is actually far more insidious than calling someone a racial slur or wearing a MAGA hat, which will get an individual pilloried on the 5:00 news but does nothing to address the effects of an oppressive system.
Report comment
You pretty much stated it all!
Report comment
Marie — We need to sort out these issues.
It’s easy to understand your emotional reaction to the nuance that you have everything you have worked so hard for just because of “white privilege,” which would indeed be an insulting and invalidating sentiment.
On the other hand, your defensive need to deny the objective fact of white privilege is really as unnecessary as denying male privilege. However while both are determining factors in the lives of many, there exists a basic state of exploitation which constitutes the essence of capitalism, regardless whether one is a member of an “officially” oppressed population; we are ALL oppressed as wage slaves at best (even those who are jobless).
There are endless variants of a murky slew of oppression and sub-oppression. They affect each group and each individual in unique ways. For example, in objective reality it is possible for individual men and individual white people to be more oppressed on an economic level than individual women or Blacks, etc. who may their superiors in the workplace. However, on a “systemic,” institutional level the patriarchy is still in power, as is white racism. Rather than competing for a larger share of crumbs, people from both sexes and all races should learn to understand the common threads in their shared oppression and unite to take power from the 1%.
Report comment
Oldhead, this is an excellent follow up that nicely captures how we’re all effected by oppressive systemic forces despite sometimes having unearned privileges like being white, affluent, or straight, etc. It isn’t about individuals but about population level effects.
Report comment
Marie, I don’t understand why you think that Sera’s analogy (“not all white people” “not all NAMIs) insults you as a white person. You don’t seem to understand the concept of white privilege. To over-simplify, it’s not saying that white people don’t face hardship, it’s saying the hardships white people may encounter are NOT because of the color of their skin. Why is that hard t understand and why do you feel insulted?
Report comment
Respectfully, I think this has been adequately addressed by several of us, and this feels like piling on.
Report comment
Marie
Every White child born in this country has a nice, big backpack of power and privilege on their backs. They don’t notice it because it’s just an accepted fact. And most of them don’t like that backpack to be pointed out to them and the fact that they did absolutely nothing to deserve that backpack. It was granted to them simply because they are White. Every other group in this country that’s not White must struggle to get that backpack.
I was given that backpack simply because of assumptions that White people made about me, thinking that I was White like them. I am not. I am a Native American or First Nations which is what many of us prefer to call ourselves today. But I don’t look like the typical stereotype that many White people have of First Nations peoples so they just assumed I was one of them. My grandfather wanted us to “pass” because we were living in New Mexico where the indigenous peoples were low people on the totem pole (excuse the pun but I couldn’t help it) with Hispanic people on top of them and with White people at the very top, where all the good stuff was to be found. It benefited us to pass both economically and socially. Not all of us have our hair braided and with feathers stuck in it. So, I was given my power and privilege backpack, which I didn’t earn. It was gifted to me because of faulty assumptions.
This power and privilege thing seems to be a very difficult concept for White people to understand and accept. It’s not their fault that it’s given to them like it is, but they need to realize that it’s there on their backs and that it’s gotten them many, many things that are denied to people who aren’t White.
Report comment
Comment removed for moderation
Report comment
And non-white people are tired of experiencing it.
You seem to be mostly opposed to learned helplessness, so I don’t see why you need to confuse the issues. Plus white people listen to brain-dead music as well.
Report comment
Aside from NPR, 95% of music on the radio is brain dead now. 😛
Maybe more.
Report comment
You mean National Pentagon Radio?
Report comment
I listen to the station for its music. 🙂
Report comment
All I have to do is replace the M in NAMI to a Z. “Not all NAZIs”
Lately in politics people are throwing around the word NAZI over nothing but psych hospitals are the most NAZI thing we have in America. Locking people up no trail by jury and with no crime committed. The forced drugging medical experiments behind locked doors. Psychiatry and forced sterilizations.
There is more but that’s enough that I don’t get in trouble for saying NAZI over nothing.
Even the Best Local NAZI Chapter is Still a Problem
Report comment
A lot of people join these groups out of desperation since they’ve been deceived and thoroughly believe they need psychiatry to survive or keep their loved ones from going totally insane.
I hate NAMI as a tool of psychiatry. But when I look at the people making up its membership I feel more sorrow and grief than anger. These individuals are precious, wonderful human beings but the lies they have been taught are what I hate. Without the lies of pharma psychiatry NAMI would not exist. Hardwired into their ideology.
Report comment
Which is why we repeatedly remind people that anti-psychiatry is directed at a system, not at individuals (except those whose blatant criminality exceeds the norm).
Report comment
Yep.
Report comment
Great article. Clears up a lot of big questions. Thanks, Sera!
Report comment
Thanks, Eric!
Report comment
Hi Sera- just wanted to make a comment about what you said regarding walking into places like NAMI and making statements regarding suicide, or about hearing voices. Places like this, or your doctor, or mental heath professional, etc take things like this seriously and follow protocol because if they don’t, they might get hit was a malpractice suit.
I agree that in the moment, when a person is feeling this way, that’s probably the last thing they want is to be committed. From personal experience, I can say that recently, when I was distraught over the death of a friend, it was a couple of friends who didn’t have “mental health” experience who ended up being the most helpful. Having worked in the field for many years, I have friends who I used to work with, who started in on me with the leading questions and the “mental heath assessment” type talk. It’s just so ingrained in people from this profession, and sometimes now even in people who don’t work in the field, because everyone and their brother seems to be loaded with an arsenal of psychobabble, and seems to be a self appointed mental health expert, and there’s this fear that if you don’t get a person professional “help”, you will be held responsible if something happens to them. And if you are a doctor or mental health professional, or an organization that people turn to, and you don’t handle protocol, you *will* be held responsible. And possibility even if you aren’t a professional, and someone turned to you for help, and friends or family think you said or did the wrong thing.
I agree about the disease model being false, but the reality is, people do experience mental distress, or don’t feel well, and that’s how they end up “seeking help” to begin with. I really like Craig Wagner’s article the other week, and his visual photo of the “web of causation” of mental distress, and the info on his onward mental heath website. I think it gave some great info on what can happen to a person biochemically, socially, behaviorally, etc that leads them to not feel well- physically or emotionally- in the first place, and what to do about it. I’ve spread that info around here and there since I saw that, it’s the most comprehensive website that I’ve ever seen.
IDK, it just seems to me that when there is an initial problem (a person is feeling depressed or anxious, has substance abuse, is having trouble coping with life events, etc), they end up “getting help”, not really knowing what could happen to them in the mental health system, and not knowing what their alternatives are? So they turn to NAMI (or their doctor, or a psychiatrist, etc)- having no clue what is really going on behind the scenes, or how they are funded, or any of that? They just want to feel better? I think helping people to find alternative is key, but it gets tricky, because does your average person out there really know that these places are potential problems in the first place?
Report comment
If NAMI were abolished it wouldn’t be there to trick people in the first place, which is why it needs to be exposed before it claims more victims.
Report comment
I don’t disagree with you, but this is going to happen, how? And what’s going to be there in it’s place? Some other message boards that I’m a part of, and just out there in general, it seems like until someone, or a loved one, personally experiences a problem (or maybe once you work in the system and start to see he flaws) it seems to me that people are okay with, and believe in, the mental health system and also it’s drugs?
Report comment
Lenora,
You said: “Places like this, or your doctor, or mental heath professional, etc take things like this seriously and follow protocol because if they don’t, they might get hit was a malpractice suit.”
Yes to a certain extent, however:
1) That’s really misguided, and not at all supported by research evidence that says that both assessment of need and the most common interventions used are wildly ineffective.
2) Even the fear of lawsuit is misguided, as successful lawsuits blaming providers for suicide deaths is actually incredibly rare, and especially in situations where there wasn’t egregious neglect (such as there wouldn’t be should want simply *talk* to someone rather than immediately shipping them off for “help”).
3) I don’t even think that’s *truly* the motivation for a lot of people… Having *just* been subjected to a “wellness” check by a provider this past Friday myself, I strongly believe that some of these things are motivated by power and control, and excused under the cover of liability.
I don’t disagree with most of the rest of what you said, but I’m not – and never have – blamed people for falling into NAMI’s clutches. I blame the broader systems (including NAMI) that make that so damn hard to avoid. So, ultimately, I agree with oldhead… if NAMI were gone, we wouldn’t have keep worrying about all this… but that’s certainly not to say that people don’t really struggle or need support. Just not the NAMI trap brand of it.
-Sera
Report comment
Hey we must have posted around the same time, when I was responding to Oldhead. Yeah I don’t know, from talking to people who are struggling, or who have a loved one who is, it seems like people just want relief. When things like the the flaws of the mental health system get brought up, when you are taking to a desperate person, that’s not really where the person is at, and the last thing they are going to want to do is take on a flawed mental heath system, when they perhaps don’t see it as flawed in the first place. You see this on message boards, for example, when you have people who have loved ones who are struggling with substance abuse, and someone pipes up about the flaws of the Rehab industry, and the response is basically, oh shut up. They are desperate and just want help :/.
Yes I see the power and control thing. What I took away from working in Human & Social Services is avoid these organizations for myself, personally. I also avoid conventional doctors, unless there’s an acute emergency, or there’s a test I need that my Naturopathic physician can’t do, after having more than a few negative experiences, where things really could have gone south for me health wise if I had listened to them, and not my instincts. I pay out of pocket for my alternative health care, but I’d rather do that than get tangled up our health care system. I wouldn’t go anywhere near NAMI either. I hear you, about trying to change things, for people might take that route. That’s why I mentioned how much I like that Onward Mental Health website, I think people need alternatives. A lot to think about, for sure.
Report comment
I don’t disagree with you that people don’t want to deal with the politics and just want help. *HOWEVER*, part of the point here is that often they think they’re getting help and they end up getting hurt. Or, if they get legit help at the individual level, it may still contribute to hurt at the systemic level by sustaining the illusion of need for NAMI. None of that ultimately changes anything I’m saying here…
Anyway, I think we’re ultimately basically saying the same thing underneath it all…
-Sera
Report comment
“Onward Mental Health”? How could that possibly be a good thing?
Report comment
I think there’s some great info here:
https://www.onwardmentalhealth.com/integrativementalhealth
Report comment
Lenora I agree unhappy people need better social support systems.
Sadly, while NAMI and other “mental health” organizations provide some social support they take away others. Once people find out you’re supposed to be “SMI” they quit talking to you, shun your company, and tell you only a “therapist” or fellow “bipolar” can understand someone like you.
My dorm mom in college found out about my label and told the other girls to quit talking to me. She said only professionals were equipped to do so.
Report comment
That’s terrible :(. That’s the kind of thing I see happening too.
Report comment
Hi Sera and everybody
By way of agreeing with your uncompromising stance on NAMI, how could it be ethically sound or politically wise to do anything less than expose NAMI, and certainly not cozy up to them, when the VERY NAME of the organization includes the words “mentally ill.” Words have far more power than is generally recognized, and when the opponents of a powerful enemy (that’s us) accept the very words being used against people we want to support with genuine understanding and services based on understanding rather than fraudulent, so-called “diagnosis”, —when that happens we might as well say, “we have met the enemy, and it’s us.”
lee
(by way of introduction to all the good folks reading this, it is also Lee Coleman, MD, Psychiatry, but don’t hold it against me! Come visit me at YouTube Psychiatry and Society)
Report comment
Hey Dr. Coleman. Are you one of those rogue psychiatrists like Dr. K., Breggin, and a couple other writers here?
The ones called “mentally ill” aren’t the people running NAMI, btw. It’s the “mama grizzlies.” Not all NAMI mothers!
But SOME are horrible women/men who enjoy the attention they get as the parent of a sick, crazy child in their thirties or forties–forced to live in their folks’ basement or an institution thanks to being too drugged up to work.
Then everyone can say, “What a brave woman you are Pamela! I hope Bobby appreciates how lucky a bipolar like him is to have a mother like you who cares about him–sick as he is.” Bobby looks embarrassed despite his “meds” and Pamela basks in the public approval–eating it up.
Are there any animal mothers known for eating their young? I have heard of cats doing this.
Report comment
Hi Rachel, and thanks for connecting. Yes, I’ve been around since the early ’70s, quite active publicly until the middle 80’s, then preoccupied with a new development– child protective services, “mental health” and law enforcement responding to a real problem– sexual abuse of children- with a system that locks up innocent persons regularly while creating a new form of child abuse. (check out my discussion of McMartin pre-school case).
Love to have you and your friends check me out at youtube Psychiatry and Society, as well as website http://www.coleman.nyghtfalcon.com (Lee Coleman Collection)
Just today “The Reign of Error”: Psychiatry, Authority, & Law was posted on the website. The book is old, 1984, but sadly nowhere out of date, given the growing army of liars like Jeffrey Lieberman, Thomas Insel, Daniel Amen, etc.
again, thanks for connecting, and keep on keeping’ on….
lee
Report comment
Give us some lowdown on Amen if you will.
Report comment
Yes, Daniel Amen, MD, psychiatrist, said to be “the most popular psychiatrist in America,” most popular TED talk, can you imagine such a thing?
Well, if you know the fabrications that Jeffrey Lieberman, MD, psychiatrist, past president of APA, is capable of (I’m writing about him right now for MIA), imagine a situation where Lieberman is debunking Amen in Lieberman’s book “Shrinks.” “…Amen’s currently fame rests entirely on spurious practices unproven by scientific research and rejected by mainstream medicine….” Amen boasts of his “83,000 Spect scans” by which he tells parents that he has found the abnormality in the brain producing the son or daughter’s unacceptable behavior. He thrills his audiences by pointing that “Psychiatry is the only branch of medicine that is not looking ‘directly at the brain.’ ” And here is the worst part— Amen and PBS Television are snuggled up nice and warm, with the $ flowing to him and his following, in turn, bringing money to PBS. A truly ugly example of just what we are up against.
So, it’s easy to find out what Amen is all about, just google him, watch the TED talk, but not so easy to stop it, given the $ and therefore political clout behind it.
I intend to focus on Lieberman, Amen, and Thomas Insel as examples of the corruption that IS today’s psychiatry, so whatever following I can develop through critical movements, through my youtube, and any other ways you can think of, are intended to build a political movement based on EDUCATION OF THE MASSES, ordinary folks like you and me.
lee
Report comment
OK thanks. Looking forward to the Lieberman piece.
However stick to your writing, you should not be looking for “followers,” that’s not your role. The AP movement needs to be led by survivors; truly allied professionals should support our demands, which is their proper function.
Report comment
Yo, Oldhead, I don’t mean “followers” in that sense, that I lead and they follow. I don’t feel the need to try to convince you of that and I’m sure you wouldn’t want me to try. I have demonstrated it in my work, and I’m confident you will agree if you just keep check that out.
I was talking about those people who have, happily,not been victimized by the “mental health system,” but who understand that something is wrong, want to know more, and maybe even want to help. As someone trained in the profession that is doing so much harm, I have an easier time gaining credibility with the very people you want to educate as much as I do. That DOES NOT mean that I know more about the most important elements in our struggle, which are ethical and legal questions, not scientific questions.
So, I don’t see any group, not even the “survivors,” as being the leaders, but I see all of them collaborating, using their respective skills and experiences to get the message out there.
To finish for now, here are the three people who for me shine the brightest in my pantheon, on this topic– Laura Delano, a “survivor,” Bob Whitaker, a journalist, and Peter Gotzsche, a MD but not a psychiatrist.
Good chatting with you
lee
Report comment
None of these people are anti-psychiatry, although they do some good work and I respect them all. The AP movement is what I was referring to, which like any revolutionary struggle needs to be led by those who are the primary victims of the system being opposed. We have nothing to lose but our restraints and chemical stratjackets. As the old Madness Network News people would say, borrowing from Marx, “The liberation of ‘mental patients’ is the duty of the ‘patients’ themselves.” Of course today we would say survivors or psychiatric inmates.
Anyway, yes, just chatting.
By the way — Amen calls his show “On the Psychiatrist’s Couch.” How many psychiatrists have couches these days, would you estimate?
Report comment
Hi Lee,
my wife has d.i.d. but we were fortunate that she never got sucked up into the system and so her, my and our experience is so radically different than most in her position. We’ve walked the healing journey together the last 11 years, using attachment concepts as the foundation of her healing, but using other things as well like neural plasticity.
If you are familiar with the show, United States of Tara, our experience is just the opposite of that. ALL the girls (alters) are securely attached to me (got engaged to the first one in December!). Sure there was some chaos in the beginning, but there was a lot of trauma to heal at that point. Now we are dealing mostly with the dissociation, and it’s a lot more difficult to undo, but we are getting there. I have a little blog over on wordpress under this name/Loving My DID Girl(s), but it never gained much traction, and so I’ve kind of let it go dormant for now. Philosophically I agree with much that is on this website, though it’s hard simply because our experience is so different than most here.
Take care,
Sam
Report comment
Oldhead
You said:
“However stick to your writing, you should not be looking for “followers,” that’s not your role. The AP movement needs to be led by survivors; truly allied professionals should support our demands, which is their proper function.”
This statement comes across as arrogant and nonsensical. Since when is it your role to tell people to “stay in their place” (apparently somewhere in the back of the bus) when it comes to building a movement against psychiatric abuse?
Anyone AND everyone who is legitimately anti-psychiatry should be encourages to be a FULL PARTICIPANT in the struggle to abolish psychiatry and all the forms of oppression that come with that institution and its Medical Model.
There should NEVER EVER be second class citizens in the struggle to end ANY AND ALL oppression in the world. To advocate for some type of “class” or “identity” division is completely contrary to the notion of taking a particular human rights struggle to its ultimate and final conclusion. Which in essence means moving far beyond a profit based capitalist system to a classless society.
Your approach that is defined solely by identity, very often has historically led to reformist limitations to struggles where individual activists (and leaders) often morph into careerists and/or are co-opted by the system as a way to short circuit the overall struggle. In a small way the so-called “peer ” movement is a perfect example of such limitations and co-optation.
OF COURSE, any movement against psychiatric oppression should,BY ALL MEANS, promote AND bring forward survivor leadership. This is both politically necessary and basic commonsense when looking at the best ways to build various forms of human rights struggles.
But we need have an overall strategic approach that UNTIES ALL WHO CAN BE UNITED. Calling for separate groups based on “identity” or certain job classifications both within or outside the system, is no way to unite and consolidate people. Especially when such a position is put forward with an arrogant and misguided “know your place” attitude.
We are better than this.
Richard
Report comment
I’m not going to argue this again with you. Self-determination is not identity politics. Survivors will organize as they see fit. We will not have our agenda determined or “approved” by others. True allies respect this. You said last time around you were going to rethink this whole matter and clarify your views in an article, but it seems not to have been forthcoming, nor have you said anything new here.
PS If you made similar statements demanding inclusion in the inner circles and strategic discussions of Blacks or women organizing against patriarchy or white supremacy they would immediately be rejected as sexist or racist.
Report comment
We survivors have been told to “stay in our place” a good deal. By very arrogant people who think they have the right to treat us like children, trained animals, or inanimate objects. To be spoken ABOUT and over. Never directly to.
Sick of having our voices overpowered and others speak on our behalf!
About us without us.
Report comment
Stepping in to second *everything* oldhead said here:
“Self-determination is not identity politics. Survivors will organize as they see fit. We will not have our agenda determined or “approved” by others. True allies respect this. ..
PS If you made similar statements demanding inclusion in the inner circles and strategic discussions of Blacks or women organizing against patriarchy or white supremacy they would immediately be rejected as sexist or racist.”
Could not have said it better myself, especially not these days…
Report comment
“Nothing about us without us.”
It’s kind of ironic, but in our experience, it’s been my voice that is overridden at EVERY point by my wife’s healing needs, sigh. Her needs ALWAYS trump my needs and I have the choice to acquiesce or move on, but she’s my one and only…so I stay and fight for a better ending than either of us have had so far. Even our son has become a ‘big brother’ to all the 7 littler girls who joined the family, but at least they do defer to the mother figure when he wants/needs one: I rarely get to have a ‘wife’ anymore…
Sam
Report comment
Sorry Richard but I’m going to pile on here because one thing none of you experts seems to grok is that you aren’t the experts. Patients are the experts on psychiatric harm and always will be. Those with lived experience of being oppressed, losing our civil rights, having our experiences explained to us as biochemical imbalances and genetic inferiorities, being drugged so heavily you no longer know what reality is, professionals are not qualified to speak for us. You are and will always be an ally. But you will not usurp leadership from those of us whose lives have been upended by psychiatry. You will never understand or be able to speak to the patient perspective. I really hope you and other potential allies will somehow be able to come to accept this. We lead. You support. Or else you willl continue to have these struggles with those of us building the new AP movement, which will be survivor led because we are the oppressed individuals and we have as much right to self-determination and demanding to represent ourselves as any other oppressed group has done.
Report comment
I have to acknowledge that divide between antipsychiatry and psychiatric surviving. A lot of people, so-called experts in lived experience, are making deals with so-called experts by credentialed training, and even working for, and in, the system. We have, among credentialed experts, only so many allies of any persuasion. My view is that we should be working together against psychiatry and the “mental health” system, essentially a “mental illness” system. I could take a leap, and call it the “mental distress” system. Either way, I would be willing to work with people like Bonnie Burstow, Phil Hickey, Lee Coleman, and Richard Lewis on the goals we have in common, the abolition of institutional psychiatry, and the liberation of people oppressed by psychiatric oppression. Should we not be working together on these goals we have in common, they do not get any closer to us than they are thereby. Anyway, for what it’s worth, and a very little at that, that’s my two cents of sage advice.
Report comment
Oldhead
I do NOT deny the role of “identity” being a significant organizing aspect in the history of various movements. Many movements organically began this way and it played a very positive role in the development of certain human rights struggles.
HOWEVER, Oldhead, you are NOT some newbie just coming into consciousness as a survivor. You are a longtime veteran anti-capitalist radical who claims to be very much guided by a CLASS analysis of society and the world.
To make a PRINCIPLE out of organizing around “identity” at this stage in your evolution as an a radical activist, is a huge step backward. And not just for you, but for the political organizing efforts you are making to advance a particular human rights struggle.
And the very criticism you made of Sera above (“This is at best a petty bourgeois point of view.”) regarding her tendency of compartmentalizing various struggles and not drawing the links to the capitalist system, could be made of you when it comes to this question of “survivor only” anti-psychiatry groups. Do you not see how this can lead to the petty bourgeois careerism and narrow forms of reformism that derailed past political movements?
At one time not too long ago you were advocating for anti-psychiatry organizing for ALL who would agree to a set of anti-psychiatry principles. Somehow you changed your position without ANY summation as to why this is necessary.
And you have also NOT addressed any of my above comments about the negative aspects to setting up the basis for “classes” or second class tiers within modern day human rights struggles. You should be way beyond this type of self limiting aspects to political organizing.
Richard
Report comment
And I would add this point, what about the crucial role of FAMILY MEMBERS of people who have been harmed or killed by psychiatry and the Medical Model?
Shouldn’t family members of psychiatric survivors be allowed to play a central role in the anti-psychiatry movement?
Why would we, OR should, we ever place limitations on who we can unite against our common enemy?
And I will repeat part of my above comment:
“OF COURSE, any movement against psychiatric oppression should,BY ALL MEANS, promote AND bring forward survivor leadership. This is both politically necessary and basic commonsense when looking at the best ways to build various forms of human rights struggles.”
Richard
“
Report comment
I feel the same way about some people who are neither psychiatric survivors, nor mh professionals, nor academics, nor family members, but who are members of the general public. A lot of people realize when something screwy is going on, and I’m not going to deny them the opportunity to change some of the things that are wrong with this world.
Report comment
Frank, none of us have ever suggested we wouldn’t work with professionals within the system toward a shared AP goal. The greater AP movement of course needs allies. The problem between Richard and Oldhead that isn’t being stated in so many words and that has Richard so upset is that he is being excluded from participating in inner circle survivor only organizing. He doesn’t understand that many survivors are so traumatized from the blatant abuses committed by professionals that a lot of us simply cannot exist with them in a place of honesty and trust that’s necessary to organize and plan an effective AP strategy. Yes, survivors need a safe space free of professionals and we won’t compromise on that.
If anyone needs reminding, some professionals that consider themselves allies have openly expressed here at MIA that they feel the need to have survivor free, professional only spaces. Everything about us without us then? Fuck that.
The civil rights movement needed white allies. The feminist movement needed male allies. Allyship is a good and necessary thing. But the inner circle consists of survivors only. End of story.
Report comment
I don’t see much organizing going on. Did you have a psychiatric survivor group with an AP orientation, and you wanted to reject professionals, that is your prerogative. The question then becomes, do you have an AP group, or a survivor group, or both? I can’t answer that one. I have a little problem with OldHead’s contention that psychiatric survivors must of necessity play the leading role in any AP movement that arises. I tend to think that leadership here is mostly a matter of personal initiative. I don’t think the core membership of an authentic antipsychiatry movement would consist of nothing but psychiatric survivors, and I can’t see allied professionals being drug around by the nose so-to-speak. Anyway, if you have formed some kind of “inner circle”, good for you. I hope you can manage to get to the next level of action from there if possible. Certainly NOT the end of story.
Report comment
But the inner circle consists of survivors only. End of story.
I’ve been thinking about this comment ever since Kindredspirit made it. I know this is the attitude of some on this website, but to see it so bluntly is still painful.
I’m glad that’s not my wife’s attitude. It’s not mine either. On my blog I likened how her d.i.d. affects our relationship to a prison. She and I are BOTH in that prison room. But she is chained inside the room. For me, the door is open, and I’m free to leave if I want. So many people do leave in this culture. My one brother left his ‘broken’ wife. But there are others who choose every day to stay in that prison room right there with our loved ones, and vow never to leave until we BOTH can leave.
She and I have been thru hell together. Even our son had to learn to help care for his mother when the others started to join our family. There were panic attacks, night terrors, hypervigilance, flashbacks, ‘alters’ running off for fun and running and hiding in fear, paralyzing fear, triggers galore. My son and I were with her 24/7 for the first couple of years because things were so bad. I had the day ‘shift’ while he was in college at the local branch, and then when I was at work at nights, he took the night shift. But my wife and I did try to shield him from the worst of it, and never asked him to do more than he freely did. We couldn’t have done it without him.
On top of that things wrecked havoc in our marriage. Many times I wasn’t even allowed to hold my wife’s hand because the new girls were so traumatized and scared of everyone and everything. Real intimacy, emotional, physical and otherwise, were largely gone. But little by little we got thru it. I learned how to help each of them. The newcomers learned they were safe in our house and with me and our son, and slowly each was ‘adopted’ into the family. The lies associated with the trauma began to be undone and slowly we began to dismantle the worst of the dissociation.
I’m not unusual. I don’t think I’m a martyr or saint: just someone honoring the woman I love and the vows I made and looking for a win/win solution for both of us.
Your comments are extremely invalidating to those of us who are in this WITH our loved ones. We don’t get paid. And we certainly don’t get validated in this culture of the me-first attitude where many tell me I ought to just leave or take care of myself first as if that’s really an option.
I’m truly sorry for your personal experience. The little you’ve described elsewhere on this website sounds truly horrible, but not all SO’s are selfish and manipulative. Not all families are of the NAMI kind looking for an excuse to get rid of the ‘problem’ member. And thus the ‘survivors’ are NOT the sum total of those suffering, and until this movement enlarges the circle and recognizes there are others who have just as much of a stake in a solution as the ‘survivors’, I wonder if this movement will ever really gain traction.
Sam
Report comment
Sam, assuming you have been telling us the truth–likely you have–if your wife is ashamed of her experiences perhaps she wants them hushed. Maybe you should respect her wishes and not go public unless/until she feels differently.
It is odd she is never here. I’m sure it’s trauma you had nothing to do with. But you yourself say she doesn’t like talking about her extreme states or psychiatric experiences.
My mom has agreed to keep quiet about my “diagnosis.” Bless her!
Report comment
I do hope that the anti-psychiatry message is more widely heard and understood. Unfortunately, MIA and other such groups in America are on the fringe. The vast majority of people still believe “mental illness” is a valid construct and thus that diagnosing and “treatment” are logical conclusions. I don’t see this changing anytime soon, especially with powerful interests involved to maintain the status quo, like Big Pharma and the APA. It sure seems that for radical reform/abolishment to take place we need more than 2,500 views of articles like this one. Millions of people need to be exposed to the downsides of traditional “treatment”. Honestly, I’ve tried to educate my clients about such problems like diagnosis not being scientific and pills being potentially dangerous, and most of them say, “Well, I still want to see the doctor”. If the people coming to my clinic don’t seem to mind the status quo, it’s very doubtful there will be any significant revolt anytime soon. We can debate these issues online all we want, but it doesn’t change the system. We do need a large camp of people to come together for any substantial change to occur given the pervasiveness of diagnosis and “treatment” with pills. While it isn’t hopeless, I give us a better chance to land on Mars by 2025 than I see psychiatry removed from the system. I guess anything is possible since we did (maybe?) land on the moon.
Report comment
Sam Ruck,
I have an enormous amount of respect for your choice to take the role you have taken for your wife and for the girls who share her consciousness. I’d like to point something out to you (well, 2 things, actually, but one is a little more pertinent in this discussion, so that first): you’ve stated many times, in explaining about the love and respect you have for her/them, that you never pushed anything on them, that you always let them be in charge of the agenda. That is what a good ally does, so good on you, and good for her/them! So that’s the first thing. The 2nd thing is the one way in which you violate this respect for them: you have written before that the girls have asked to be referred to as simply that “the girls” and yet you continue to use the language of pathology when you refer to them as ‘alters,’ a behavior that you know on a gut level is wrong because on more than one occasion you write in a (gag) after referring to them in this way. You do not have to use the language of pathology; there are other options. Example: “My wife shares her consciousness with several little girls” gets the situation across just as well as “My wife has d.i.d.” but does not reduce these little girls (whom I truly believe you do love) to merely ‘symptoms’ of a ‘disorder.’ I’ve tried to point this out to you before, how this use of pathology language flies in the face of the love and respect and healing intention you claim to treat them with. There is cognitive dissonance here. How can you so dearly love these little girls yet still speak of them in those awful, demeaning terms? It baffles me; it angers me. I wish you would give this issue deep consideration and change this one sticking point. You’d be more credible as an ally, at least in my eyes.
Report comment
KS I was trying to be charitable to Sam. I don’t know him offline. DID is a psych label, so of course I reject it.
The abuse probably happened before he met her. Sam says as much. Is he further abusing her? (Deliberately.)
I can’t say. It is odd she never comes here and he never quotes her or makes her seem like a real individual.
Innocent till proven guilty. Though of course I disagree with the DID label.
Report comment
Frank
I very much see the value and necessity of bringing forward and developing survivor leadership, and I don’t mean this in some kind of token way. BUT this does NOT mean there should be any second class status for anyone else participating in the anti-psychiatry movement.
BTW, over many years at MIA there have been some extremely articulate and passionately dedicated family members of those deeply harmed by psychiatry, who would be excellent candidates to be active members in anti-psychiatry organizing. What possible reason could there be to deny them membership in an anti-psychiatry organization?
And as far the issues of ‘honesty and trust” that Kindrespirit raised:
In any political organization there is always going to be differences, and even conflicts over political agendas, egos, power and control issues etc. This is to be expected in any such political organization.There is NO guarantee there would ANY less conflict (around honesty and trust) in an all survivor organization.
And as Frank brought up, how could anyone deny Dr. Philip Hickey or Bonnie Burstow membership in an anti-psychiatry organization? Their writings and overall activism has struck powerful blows against the oppressive institution of psychiatry. They have advanced our struggle FAR MORE than anyone currently commenting in this MIA dialogue.
Richard
Report comment
Just my two cents here. I don’t hear anyone wanting to deny membership or participation to people like me or others who don’t fit the “survivor” description. And I’m not sure the most important issue is honesty or trust, either, though I don’t want to invalidate Kindred’s raising of this as a vital issue. It seems to me that the issue is one of social power. It is pretty easy for those in the one-up situation to believe they are being “fair and equitable” when they are actually exerting their unearned authority based on social biases. So making sure that the direction and priorities of an antipsychiatry movement are not only informed by, but directed by survivors seems a very important point to me. It’s not that others can’t help and be passionate and come up with new ideas. To me it’s that the ultimate test of any idea is whether those who have been through the ringer think it makes sense and would work. Survivors have to ultimately direct the effort, even if a lot of hard work is done by people from all walks of life who interact with the system in some way.
That’s MHO, for what it’s worth.
Report comment
Richard, maybe the real thing you fail to understand is that this isn’t “our” movement. You have the option to walk away any time with your letters beside your name and your professional status. Patients that walk away become ex patients that spend the rest of their lives knowing the threat of incarceration in a hospital or being subject to a community treatment order is always a possibility. Especially now in the era of electronic medical records, patients are branded for life with these spurious labels. So no, it isn’t really “your” movement at all because it isn’t your neck on the line for getting uppity and demanding rights.
White people didn’t have the nerve to call the black struggle for civil rights “our movement”. For shame! Your continued attempts to appropriate something that you can at best be an ally to is somewhat bizarre and shocking.
Report comment
I’m as nostalgic as anyone for the movement we had before 1985, but we don’t have that movement anymore. I think we have to deal with the reality of things the way they are. The psychiatric survivor movement is one thing, the antipsychiatry movement another. Sure, there are places where those circles intersect, but there are places where they don’t touch at all as well. I’m not looking for an exclusive club. I think we can get more done if we all work together than if we work against one another.
Report comment
I think Richard places far too much importance on my opinions. Nothing I have said here could reasonably be construed as trying to preclude anyone from engaging in any form of anti-psychiatry organizing they see fit. In fact I encourage it, go for it!
For me this has turned into an argument about principles, sparked by Richard’s jumping on a comment I made in response to Lee’s comment about seeking “followers,” and not about any specific organization, past or future. I do however believe that this is a good time historically for bold new projects to be undertaken on a number of fronts, and in a number of forms, and that these should all be informed by the perspectives and demands of organized AP survivors.
I also believe that the natural moral leadership of the anti-psychiatry movement — even when it not is not “officially” organized — is the unsolicited bequest, and duty, bestowed by psychiatry upon conscious anti-psychiatry survivors, just as it is with the proletariat in a standard class analysis. And just as women and people of color have resisted attempts to make them subservient to white and male-defined versions of liberation or socialism, so must survivors resist attempts to stuff us into some cookie-cutter paradigm defined by those who have not personally experienced psychiatric oppression — no matter how empathic they believe they may be. Or how enlightened their general political perspectives may be.
If we were truly drawing parallels to the Civil Rights movement or the struggle against slavery, the principle of self-determination as it applies historically would be obvious; whites were often excluded from anti-slavery operations in the John Brown era, and from the membership of the Black Panther Party, which I have never heard Richard accuse of promoting “identity politics.” And although Richard has yet to delineate the differences, I can describe one: “Identity Politics” would comprise accepting one or two random members of an oppressed population as the spokespeople for the entire group based simply on their being members of such, which would be a form of individualism. Self-determination, also exercised exclusively by members of the oppressed population, reflects a collectively determined viewpoint which represents the effective consensus of that population’s political perspectives, aspirations and analyses.
By “inner circle” I highly doubt Kindred Spirit was advocating a literal cabal of survivors directing the “movement” (which remains almost as metaphorical as “mental illness”), but rather this principle of self-determination. She seems to be mainly responding ironically to Richard’s somewhat pouting sense of being “sent to the back of the bus” or not being let into the tree house with the survivors.
Ultimately it will of course take more than a “circle” of people to defeat psychiatry, however it’s also important to not be focused on numbers, but on the ability of each of those “numbers” to be an independent unit, fully capable of articulating and advocating anti-psychiatry education and activism on their own. So wherever you are folks, dream big. 🙂
Anyway I don’t plan to be continuing this discussion much, if any, longer, as it is not really fare for a mass website dedicated to promoting psychiatry.
Report comment
Kindredspirit
While I would NEVER compare my experiences to that of a survivor, neither can you deny that some professionals and others working within the “mental health” system have been harmed by psychiatry and their Medical Model.
I have fought against biological psychiatry (with 22 years in community MH clinic) for over 25 years, quite often putting my job and career on the line.
I have witnessed psychiatry and their Disease/Drug Based Medical Model suck the life out people (people that I loved and cared for) with all their labeling and drugging.
I have witnessed people being humiliated and emotionally crippled over many years by this system with their multiple cocktails of drugs and disabling forms of so-called “treatment.
And I have had a number my long term clients die as result of body and brain destroying cocktails of drugs, including several who were driven on to combine their psych drugs with illegal drugs in the street. And I have a VERY close friend who has been deeply harmed by psychiatry with drugging and ECT (including as we speak) for over 25 years.
To bear witness to all these forms of human destruction takes a toll on some of the more conscious people working in the field who know exactly what kind of damage is being done on a daily basis by this system.
To me the sum total of these experiences (combined with my reading of hundreds of personal stories written by psychiatric survivors) has been traumatizing on some level. Again I would NEVER compare my experiences to that of an actual survivor, so please do not in any way say I am making such a comparison.
But neither you nor I have possession of a “sincereometer” or some other device to measure one’s hatred of psychiatry and all the harm they do, and/or, have a way to measure the amount of passion and determination one possesses to rid the world of all forms of psychiatric oppression.
Some professionals (a very tiny minority at this point) such as Bonnie Burstow and Philip Hickey have easily proven their mettle in the struggle to rid the world of psychiatry and their Medical model.
The small number of MH workers and other professionals who are anti-psychiatry at this time are HARDLY a threat to somehow “take over” any anti-psychiatry movement that would overwhelmingly have a membership comprised of mainly survivors.
And the two professionals I mentioned above and myself are all in our 70’s. We won’t even be around much longer. We are really helping to do preparation for future struggles of the younger generation of activists that will be stepping forward in the future.
And yes, I am proud to say, and I will continue to say, that I am very much a part of the movement to end all forms of psychiatric abuse, along with ending the entire profit based capitalist system.
Richard
Report comment
I’m sorry you can’t see past your own experience Kindredspirit, and clearing NOTHING is going to convince you otherwise. I have no need for my wife’s diagnosis: I’d much prefer a healthy wife, not spending 95% of our private time with ‘littles’ who are starved for the love and attention and affection they never got from their parents the first time around.
Rachel, my wife refuses to come on these sites because when we first started this journey, she did the whole survivor sites stuff, but they kicked one of the little girls off even though she broke none of the rules and ever since they have all refused to go back. Plus you add to the mix the toxic notions about d.i.d. currently going on in this culture like the movie Switch and its sequel Mr. Glass that just opened in the theaters, and a host of other books that now love to portray people with d.i.d. as some sociopathic, super killer and even cannibal. And there still is the past excesses of the so called experts(!) of the satanic crap that is still in the minds of some like Kindredspirit as if those abuses somehow discredit the entire issue.
So instead she/they spends her/their time on other sites. We homeschooled our son, and so the two millennials (my fiancée and girlfriend) have an online personality that fits that profile and they spend it trying to help younger wives and single women trapped in pseudo-Christian, patriarchal situations. And from time to time when they can clearly see the signs of d.i.d. in people, they’ll privately reveal their own to them and help shepherd the women, if possible, to more healthy situations.
Lavendersage, yes, you know that I HATE the language that is in the common vernacular. We’ve had this conversation in the past. If you went on my blog, you’d almost never find it, but here, I realize my story is only partially known, and so we are ALL handicapped by the decision of whether to use the common language that everyone knows even if we disagree with it or go into a long explanation of what I mean. If someone new came on this website and simply heard me talking about my wife, and then in another place I was talking about my fiancée, and then in another my girlfriend, what would they think? That I’m in some kind of open marriage? So we are all constrained to some degree by the common vernacular. And you have to notice my struggle as I’ll often say both, or put alters in quotes, but sometimes my time and space is limited and so I do the best I can. The writers on MIA often express the same struggle. I’m sorry you don’t like it: I really don’t either.
Sam
Report comment
“…you add to the mix the toxic notions about d.i.d. currently going on in this culture like the movie Switch and its sequel Mr. Glass….”
?????
What I actually said was: “DID is a psych label. So of course I reject it.”
Report comment
Sorry, Rachel, I did NOT mean you as in you personally. I guess I should have used ‘one’ third, person, general, rather than you, 2nd, person, ‘specific.’
As for d.i.d. being a psych label and rejecting it. Well once again are we ALL going to start from scratch every time we discuss everything? Or are we going to use the common vernacular and go from there?
I do understand that for those who have had those diagnoses weaponized against them, then they/you see them VERY differently, than my wife and I who see those diagnoses as an ‘aha’ moment. For us it simply told us what we were dealing with, and then we learned, together, how to deal with it from there.
Sam
Report comment
I would pay a little more attention to the language you use, OldHead, if I were you.
I also believe that the natural moral leadership of the anti-psychiatry movement — even when it not is not “officially” organized — is the unsolicited bequest, and duty, bestowed by psychiatry upon conscious anti-psychiatry survivors, just as it is with the proletariat in a standard class analysis.
I’m a survivor of psychiatric treatment. I’m not a survivor of anti-psychiatry. (Sounds, to use Jeffrey Lieberman’s term, pro-psychiatry, doesn’t it?) I don’t have a problem with anti-psychiatry, with or without the hyphen. It’s kind of like referring to anti-rape survivors. I don’t think promoting sexual assault would be a good idea either.
I am not, in any way, shape, or form, an anti-psychiatry survivor. I am a psychiatric treatment survivor. I’m perfectly okay, in fact, with anti-psychiatry. Get rid of the system. It stinks.
Report comment
Like it or not, the SO’s, family members and friends have a real stake in this fight, AND we are the first line of defense against more people becoming psychiatric survivors. My wife couldn’t have done it on her own without me and our son when all hell broke loose with her ‘extreme states.’
But if some want to treat us like second-class citizens based on their own experiences of bad SO’s and family members, that’s rather short sighted. We ought to be reaching out to those who are open to a new way of thinking, and helping them and teaching them, but also recognizing so many of them are dealing with their own demons, too. We should draw the circle large enough by understanding we are ALL in this together against a system that is truly larger than psychiatry or even amoral capitalism, but the culture at large that tries to sweep trauma and abuse under the rug at any cost: psychiatry is just a tool to help them do so.
My heart is sad every time an SO or family member comes on this site and decries the trauma their loved one has suffered at the hands of the system: we have a number of authors who have done so recently. But to myself I think, “This didn’t have to happen.” And every time I read a story in the news of a cop killing someone in mental distress, I think the same thing. But until the SO’s and family members are viewed as potential allies and given a real voice for their perspective while recognizing their own distresses and issues, this movement will continue to struggle, I believe.
I think an Open Dialogue kind of model is the way to go the little I know of it because it seems to bring all 3 stakeholders into the equation: sufferers, SO/family members/friends and ‘experts’; not this ‘survivors’ first and foremost mentality.
Sam
Report comment
Sam, I do see past my own experiences. I was deeply embedded within DID specific trauma circles both in person through my psychiatrist that specialized in DID, the hospitals and day programs I attended, some of which were trauma specific, and online in DID communities as far back as late 2002, right up until 2012. I have known dozens of people with the diagnosis and seen nearly all of them drop it when it no longer suited their needs. You are not an expert in DID because of your wife’s issues.
As for the validity of the diagnosis, it was borne out of a hoax into a book of diagnoses whose validity is so disproven that the United States federal government researchers will no longer use it. There’s a perfectly valid concept of traumatic stress and dissociation that doesn’t claim the farce that the individual has a fundamentally broken psyche and has more than one person residing inside them.
The diagnosis is just as invalid and the concept just as nonsensical as the concept of bipolar or schizophrenia or adhd being discreet diagnoses rather than descriptions of experiences that interrupt one’s ability to function inside the expectations of a capitalist society.
Observationally (which is what your perspective is as well), I’ve simply seen too many people shockingly easily abandon “being multiple” when it no longer served their needs to continue to buy into the hoax. And I certainly don’t think it does anyone any good to encourage them to believe they are anything but a whole person, rather than the method you propose with dramatic descriptions of building complex relationships with “alters” that you have admitted in so many words are more like manifestations of different personality states. In fact that’s exactly what it is but it’s far healthier for the person experiencing such to learn to accept that those personality states are okay to feel and express than it is to name them and build a complex fairy tale about all the different people in the system. That’s why this is harmful and I’m sorry you can’t seem to get that.
Report comment
Kindredspirit,
some of what you have said I agree with. As well, I am aware of the various controversies around this issue. And yes, I personally operate on the premise of this being about trauma and dissociation and you can see that all over this site when I discuss particulars of how I help my wife. I agree that the various ‘girls’ are simply different aspects of my wife’s unified personality, but if I were to call her experience of things a ‘fairy tale’ all of you survivors would burn me at the stake for invalidating her experience. Instead I walk with her, where each of the girls are at, and yet I’m upfront with them that they are all part of my unified wife, but I don’t make that the basis of my interactions with them.
The problem seems to be that you want me to be the exact opposite of what most survivors on this site cry for: someone willing to walk in my wife’s reality rather than dictate to her that she follow my reality And yet, if I did that, then you would simply pillory me for being like everyone else.
Lastly, I DO get what you are saying: you’re not saying anything I haven’t heard before. I simply disagree.
Respectfully,
Sam
(edit: I guess I’ll add that even though I walk in my wife’s reality which is based on her past trauma during childhood, I model a new one without fear and trauma for all the girls, and as they live with me and our son, they are ALL moving toward this one. But I give them the time to do this of their own volition and not because I mandate it as the price to have a relationship with me.)
Report comment
Sam, I never called your wife’s experiences a fairytale and I would never invalidate her in that way. The fairytale I am speaking of is the one where you encourage her to believe that her personality states are entirely different people with names and likes and dislikes of their own and the ability to have different relationships with you. This is a construction of a new world the two (three? Uh, four?) of you all agree to participate in and does not actually encourage your wife, the person who dissociates difficult feelings away, to incorporate them into the whole. That’s the crux of my objection to your approach.
I’m not at all saying your wife doesn’t have a history of trauma that’s caused her significant harm. And I’m not trying to minimize what she experiences. But I do believe strongly and without reservation that the approach to unification of the victimized self should not include community participation of alters as distinct individuals. I believe that it’s more loving to encourage wholeness by addressing the name of the body and encouraging that person to express difficult feelings and encouraging them to stay present with you during stressful moments and teach them that way how to trust that being present is more fulfilling than dissociating. Instead, when you pick up the pieces and handle her littles with kid gloves and allow them to continue to endlessly escape into the safety of dissociation, you actually discourage unity of the self. If in the end what we want to do is heal from trauma, I can’t see a way to do that that involves your methods because those encourage a state of dissociation and the formation of elaborate relationships with each alter.
I’m not trying to be offensive to you or to anyone who has been labeled with DID, but rather to say that while your message of attachment is lovely and probably the most helpful aspect of your approach, your methods of applying that attachment strike me as completely backward in helping someone become whole, and more importantly, present in the moment again.
Report comment
Kindredspirit,
I honestly hear you. I really do understand your concerns: you aren’t the first person to voice these same exact issues. And I accept that you are honestly sharing this with me out of concern for me and my wife.
I just don’t know how to convey to you that your concerns and misgivings really are based on a strawman. I don’t know where these tropes began since I’ve heard them elsewhere, but our experience is completely different than you and others are imagining it.
First, if this is your opinion of dissociation, it is NOT our experience of it. For us/her, dissociation is like discovering a long-lost castle in the woods. it’s always been there, but the path is overgrown because no one has used it in decades. But neural plasticity teaches us that once we start to use that path, it will become worn and more and more accessible.
When the trauma happened in the past, the mind sequesters that pain and anguish from the rest of the mind so that it doesn’t engulf the entire person and a complete breakdown of ALL functioning occurs. The only reason ‘alters’ occur is because of that sequestering. So they kind of take on a life of their own.
Now I could demand, as you say, that I will only talk to ‘my wife’. But that’s not how each of them sees it. In her mind, she is a real, live entity with her own thoughts and feelings. Each girl has repeatedly voiced this to me when she first began to join us outside.
And so I accepted this starting place. My validation made her feel safe and accepted. And as we walked together, I helped each girl release the lies she had accepted from the trauma. And as I won each one’s trust, they each wanted to be ‘adopted’ into our family: the colloquial term we use for becoming securely attached to me.
As that began to happen, the trauma being healed, the lies being resolved, and the secure attachment to me giving her a safe base, we began the process of tearing down the last of the dissociation between each girl. Little by little each girl began to wear a footpath from her own, little, forgotten castle to the main pathways that all of them could access…and once we got to that phase, slowly, they each began to interconnect with the others.
At first it was extremely important to each that she was a distinct individual, but slowly as they continue to make more and more and more connections with each other, they are less concerned with being individualistic and are acting as a group. And from what I have read, more and more experts realize that we ALL act like ‘groups’ and not monolithic personalities.
But they still want me to recognize their individuality even as they shed more and more and more of their need to act on their own. Maybe some day none of them will care about herself as an individual, but what I did was give each the time and space she needed to heal and feel safe to integrate with the others. I didn’t demand any of them act like my wife even though I personally feel they are all my wife.
And at this point I just got engaged to one girl in December: she wants to be my wife. I’m pre-engaged to another. And a third has mentioned it. So one by one, each is CHOOSING to become my wife, but it’s always her choice. I make clear that I will never withhold my love or affection if she doesn’t do what I wish.
I’m just not sure how you object to me allowing my wife the space and time she needs to heal in the manner that feels the safest to each of them: that seems to be what most of the survivors here want: validated and loved unconditionally, even while I shepherd each girl gently toward the goal of healing and integration within the larger group.
Sam
Report comment
Hey Kindredspirit
I poured my heart out in my above comment about your questioning of my use of certain pronouns when discussing the movement against psychiatric abuse.
Is that the end of the dialogue on such a deeply personal and politically relevant question?
Richard
Report comment
Richard, I’m sure that was my fault because I distracted her talking about something we are both passionate about.
Sam
Report comment
From all the above it’s quite possible that KS’s fingers need a rest.
Richard, now it sounds like your feelings are hurt, which no one wants, nonetheless that they are seems pretty inexplicable and weird, and must be based on some fairly unrealistic assumptions and/or expectations on your part. To suddenly derail a discussion supposedly based on logic and objective analysis and start acting like you’ve been “expelled from the club” begs a lot of questions, the first of which being “what club?,” another being how did this become about personalities rather than ideas and principles?
It is quite disingenuous to make this an issue of specific personalities, and to essentially guilt trip survivors about “hurting people’s feelings,” especially with the implication that we are hastening aging anti-psychiatry professionals towards their deaths by selfishly asserting our right to define our own agenda. You’re the main one consistently opposing this.
Lots of anti-psychiatry survivors are pushing 70 or more as well, and not all of us are in great physical condition either. You have a history of defending professionals, such as Brett Deacon, who have tried to dismiss survivors’ legitimate concerns as “personal attacks,” rather than pointing out the manipulativeness of such emotionally-based “arguments”; you seem to be following the same pattern here.
No one is preventing you from initiating a project, or organizing anti-psychiatry activities among the professional and political circles with which you have more rapport, more access, and more common experience than do most survivors, so it seems that this would be where your AP consciousness would be most valuable and needed, and that you could work in coalitions with survivor-based AP groups and others, but that’s your choice. It seems that right now you’re avoiding whatever form of AP organizing you would be best at by preoccupying yourself organizing survivors, and especially by insisting that you should have a “vote” on what we say and do.
The basic principles of self-determination I’m defending here are not particularly hard to grasp or especially radical. Steve M. isn’t a survivor either, and he doesn’t sound threatened or at all fazed by the concept.
So, if you want to trade slogans, “Let a hundred flowers bloom!” Also, “Fight dogmatism!” 🙂
Report comment
Oldhead
Apparently you are now attempting to speak for others in this dialogue and/or trying to direct and control the discussion.
And then you proceed to totally misrepresent the content of my above comment. It is also interesting how you never respond to the main questions raised in my comment about the appropriate use of “pronouns” as a very real political question in this struggle. Instead you have chosen to diffuse and deflect. This is a very sad development in your role here.
I have never made this “personal” or attempted to “guilt trip” anyone in this discussion. For you to make these mischaracterizations and distortions of my comments is totally unprincipled and an unfortunate development in your participation here.
My above comment to Kindredspirit is very “political” in its essence. My sharing of my experience (and feelings) in the struggle against psychiatry and all forms of psychiatric abuse is to highlight the fact that people who work in the “mental health” field can be very much harmed by this system in multiple ways, AND they can have a clear stake in being a part of a movement to end this oppression. So yes, the movement against psychiatric abuse can be “our” movement.
This was NOT pointed out as a way to compare degrees of oppression or somehow equate the experiences of these two groups of people. Nor does this somehow represent a “professional” trying to organize “survivors” or direct their struggle. These are all your words AND misrepresentations.
This is pointed out to indicate that there can be a basis of unity for survivors to unite with a current minority of professionals and other workers in the field who clearly understand psychiatric oppression and are passionate and committed to fighting against this.
These are clearly very strategic AND political questions about how to advance this particular human rights struggle. This is a fundamental question of trying to “Unite All Who Can Be United.”
Oldhead, you said: “You have a history of defending professionals…”
No one at MIA has been any harder on professionals than myself. Any review of my blogs and comments will bear this out. What I have refused to do is ATTACK potential friends who are misguided on a particular issue, and therefore drive them away from potential involvement in this movement.
Oldhead, some of the latest positions you are taking on these questions AND especially some of your methods of struggle are clearly troubling.
It is too bad that certain other people who are clearer on these questions have chosen not to participate. Perhaps they are disheartened by the very nature of how this entire process has proceeded. It will certainly dictate how I choose to engage in the future.
Richard
Report comment
Lots of anti-psychiatry survivors are,,,.
Stop using the term “anti-psychiatry survivors”! I survived psychiatry. Anti-psychiatry was never such a threat to my physical existence as psychiatry was. If you’re going to specify a type of survivor, make it a psychiatric, or psychiatric oppression, survivor.
I don’t see this great division you seem to see, OldHead, between psychiatric survivors and dissident “mental health” professionals. Between “mental health” professionals, and psychiatric survivors in general, sure, but that is something different. Either we ally with each other, or we form exclusives clubs, and we don’t get so far as we would if we had allies.
Practicality means something from where I’m standing. If people just want to be difficult, no problem, the oppressors love that sort of thing. They’ve even got a couple of words for it, they call it “mentally deranged”. “Fight it out among yourselves, why don’t you, and we will just observe”, they must be saying among themselves.
Report comment
Okay, Richard, I guess I should have asked Oldhead to be more specific that I’m unable to use my hands for much right now. I’m struggling to type this but you need to hear it straight from the horses’ mouth apparently.
I do not doubt that you have seen terrible things over the course of your career treating mental patients. But let’s be clear that your participation was always voluntary. That’s the difference between you and your patients. We aren’t equals. It isn’t a matter of how much you care or a measure of your integrity. In the eyes of those judging us, your AP position might be seen as misguided, whereas I am seen as sick. And my rejection of the system seen as evidence of my illness. And I just find it utterly preposterous that you continue to dig in acting like you’re being left out of something.
This whole conversation is going on as if you think there’s some major movement going on and all the good professionals are being left out.
Congratulations on surviving this world long enough to make it to your 70s. I have heart damage from long term Lyme disease being treated as psychiatric illness. I’m not even 40, Richard, and I struggle to breathe and to walk long enough to properly care for my service dog. I’ve had an electric scooter in my amazon cart for a month, and I keep putting off the purchase because of how much it’s hurting my husband to witness me in such a weakened state. I’m not convinced I’ll live another year. So don’t you dare lecture me about all the poor old dying professionals who just want to be part of the club. You’re actually in a far more powerful position than I am and you waste time whining here in the peanut gallery of MIA about this perceived slight of being left out of something instead of using your status and position and what time you have left to organize your people.
I’m not going to respond any further to this. I like you Richard and I think your input as an ally could be invaluable but this discussion has verged on scandalous. I’d love to trade places with any of the old dying professionals.
You truly want to help? Organize your people, create an alternate professional society of clinicians pushing back against the biomedical/chemical imbalance/brain disease model. The Lyme disease community has given mental health professionals a pretty good road map for how to fight back against the system from within when the dominant paradigm is more harmful than helpful. Check out the work of the ILADS if you’d like to see how this can be done and how professionals can use their power and position to elevate patient’s voices. Mentor younger professionals for doing such work. But please, stop lowering yourself to imploring survivors to include you in their organizing. It’s a comical caricature of the position you truly occupy and the good you can do and you don’t need to ride the coattails of the efforts of sick and dying survivors to effect change if you truly want to.
Report comment
Rape survivors, holocaust survivors, torture survivors, spaghetti survivors, etc.? Please, clarify matters by specifying type of survivor, say, with a psychiatric before the word survivor. I’m a psychiatric survivor myself, and I don’t mind working with anybody who takes a position against human rights violations and psychiatric oppression.
Report comment
Kindredspirit
Thanks for your heartfelt response. It was a mistake for me to have focused some of my major political points in this thread in response to your comments, no matter how provocative they might have been for me at the time.
I can see that you indeed have a lot on your plate at this point in your life, and I truly hope you can make some headway in these struggles.
Kindredspirit, I have always liked your overall comments and participation (as well) at MIA and have learned a lot from your perspective. I hope that can continue.
Again, while I have feelings just like everyone here, I don’t ever mainly approach these questions in a personal way, nor do I feel attacked by you. And again, my use of my experience (fighting psychiatric oppression) and my related hatred of the institution was used as a way to make certain basic points about the basis of unity that can be possible in a growing movement.
Kindredspirit, if you do not trust any professionals or other non-survivors enough to work with them in the early stages of a developing movement against psychiatric abuse, I will certainly respect that position. And I only wish the best for you in any endeavor you may engage in; be it personal OR Political.
My main contention here in this dialogue at MIA (and it is where I should have solely directed myself) has been with the shape shifting positions put forward by Oldhead. He is the veteran political activist that claims to be operating from a Marxian class analysis.
It can be a divisive process, and basically impossible to have principled dialogue with anyone who distorts one’s positions and and makes up “straw man” arguments to ridicule someone’s positions and misdirect a discussion. As I stated above, this unfortunate development will clearly influence exactly how I choose to engage on these vital questions in the future.
Richard
Report comment
Thanks, Lee! I agree that the language of their name itself is hugely problematic, and powerful. I will check out your YouTube. 🙂
-Sera
Report comment
All is copacetic
Report comment
Think I’ll skip the video, thanks. But your points are right on.
Report comment
Lee Coleman, I’d like to know what your involvement was with the McMartin Preschool trial. All I can find is an analysis on ipt-forensics.com. Were you personally involved with this case?
Report comment
Hi
Yes, I was one of the experts hired by one of the defense attorneys: 7 defendants, each with their own court-appointed expert. So, I was able to study all the documents, taped interviews, medical records, everything, in preparation for testimony in the trial. Then the charges were dropped on 5 of the 7 defendants, so I didn’t testify in the criminal trial. But one of those on whom the charges were dropped sued to get her job back as a public school teacher, and sued to get her back pay. I testified in that trial on the same issues of the criminal case, that the methods used in interviewing the children were so egregiously leading and suggestive that it was absolutely essential that the judge consider whether the children’s statements were based on memory, or on learned ideas taken from the interviewers behavior. I have written all this up, and IPT published it, so you can get more details in my article. I am in the process of getting articles on this topic on the web; two are up so far on http://www.coleman.nyghtfalcon.com (Lee Coleman Collection), go to home page, then documents, then books and essays, then two articles on sexual abuse allegations.
thanks for the inquiry
lee
Report comment
To your knowledge, has any attempt ever been made to establish what the long-term outcomes were for any of the children involved in the satanic abuse hysteria cases?
Report comment
Lee, I tried to email you directly but the email address listed on your website bounced. Is there another way to contact you directly?
Report comment
[email protected] If you’re looking for info on kids caught up in a SRA case, I would look up journalist Debbie Nathan, El Paso Texas or Mike Snedeker, attorney somewhere in Oregon.
Report comment
Lee, during my senior year in boarding school in 1971, a very popular book was making the rounds of the students in that small school. Everyone, including yours truly, read it. I think the title of that book was…Black Rage? It’s been so many years since then, I’m not quite sure anymore. However, do I remember correctly that you were its author? Though I do not now remember much of what it said, I definitely remember reading it. Those were heady days, weren’t they?
How ironic that I’m encountering you personally, albeit on the internet. And on a first name basis with you, no less! I’m glad to see that you’ve survived and prospered through the years.
Report comment
Yes the name and yes it is the parents who started it and in my area many families were of the Jewush faith and though I knew professionals whose parents lived through the Holocaust theconnection between inter generational trauma and the as Dr. Carl Whittaker would say before he became a family therapy parish “ the identified patient” was never seen and there even now is now aha moment or eureka in this organizational matrix.
Codependency but ah that comes from trauma as well. And I think as Sarah did with her recent writing parents need the same creative stress response format.
Fear this I saw in MH professionals many who had relatives with issues in the system but a type of trying to save things in the family ala E. Fuller Torrey MD and his sister. And really what happened to her? In the origin story and in my reading no would not want a sibling like that No.
But there is the fear what if my kids get it? And for many people the crazy aunt or uncle or grandparent is erased. As the DD parents were TOLD to do by the docs when their child was born” not right.”
And then in medical family circles ah the shrink kids – always at least one in big do do. So the fear can become a reality and then there is the .org that comes to their rescue.
I still don’t understand the divide between ARC and BAMI though sometimes issues crossover. And is ARC still called ARC. I have lost touch. But the label was caught and mostly won.
And in the agencies inclusion was fought for but also times just to hang with the homies too. I never ever got that feeling from NAMI ever.
FYI Best Boy is an old but worthy documentary on a Down Syndrome young man leaving his parents. There is NOTHING like this type of effort in NAMI.
Also Rachel there is guilt the gift that always keeps giving. Mother’s ferl that and some husbands use it for all its worth. So the Moms in NAMI How many have heard-You Gave Birth to him or her?
Way way too many and a group like NAMI uses it for all that it is worth.
I am with Sera on all of this.
Report comment