
Editor’s Note: Over the next several months, Mad in America is publishing a serialized version of Peter Gøtzsche’s book, Mental Health Survival Kit and Withdrawal from Psychiatric Drugs. In this blog, he discusses the risk of suicide and other causes of death from psychiatric drugs, focusing on neuroleptics. Each Monday, a new section of the book is published, and all chapters are archived here.
Suicides, other deaths, and other serious harms
It is a well-guarded secret how many people are killed by psychiatric drugs. This has been obscured in many ways.
The easiest way is to wipe the deaths under the carpet, “so that we don’t raise concerns,” as a Merck scientist was told when he was overruled by his boss.51 The scientist had judged that a woman on Merck’s arthritis drug Vioxx (rofecoxib) had died from a heart attack, but the cause of death was changed to unknown, also in Merck’s report to the FDA. Other sudden cardiac deaths on Vioxx disappeared before the trial results were published.
When the many deaths could no longer be hidden, Merck withdrew Vioxx, in 2004. I have estimated that Vioxx killed around 200,000 people, most of whom had not even needed the drug.51
Fraud with lethal consequences is common in drug trials,4,51 and our major medical journals, in this case the New England Journal of Medicine, often willingly contribute to it by publishing flawed trials and by not taking action when action is clearly needed in order to save patients’ lives.51
Psychiatry is no exception. Only about half the suicides and other deaths that occur in psychiatric drug trials are published.81
Another big problem is cold turkey withdrawal in the placebo group. Since virtually all trials suffer from this design defect, they will underestimate how deadly psychiatric drugs are.
Neuroleptics
Neuroleptics are very toxic and likely the deadliest of all psychiatric drugs.4 When I wanted to find out how deadly they are, I decided to focus on elderly, demented patients. I assumed that few of them would be in treatment before they were randomised and that there would be enough patients to draw a conclusion because many of them die, whether they are on drugs or not.
I found a meta-analysis of placebo-controlled trials in dementia with a total of about 5,000 patients.82 After only ten weeks, 3.5% had died while they were on one of the newer neuroleptics, olanzapine (Zyprexa), risperidone (Risperdal), quetiapine (Seroquel) or aripiprazole (Abilify), while 2.3% had died on placebo. Thus, for every 100 people treated for 10 weeks, one patient was killed with a neuroleptic. This is an extremely high death rate for a drug.
Since half of the deaths are missing, on average, in published research,81 I looked up the corresponding FDA data based on the same drugs and trials. As expected, some deaths had been omitted from the publications, and the death rates were now 4.5% versus 2.6%, which means that neuroleptics kill two patients in a hundred in just 10 weeks.83
I also found a Finnish study of 70,718 community-dwellers newly diagnosed with Alzheimer’s disease, which reported that neuroleptics killed four to five people per year compared to patients who were not treated.84 If the patients received more than one neuroleptic drug, the risk of death was increased by 57%. As this was not a randomised trial, the results are not fully reliable, but taken together, these data show a death rate so big that I cannot recall having seen another drug the patients don’t need that is so deadly.
Can we extrapolate these results to young people with schizophrenia? Yes. In evidence-based healthcare, we base our decisions on the best available evidence. This means the most reliable evidence, which are the data just above. Thus, absent other reliable evidence, we will need to assume that neuroleptics are also highly lethal for young people. We should therefore not use neuroleptics for anyone, also because an effect on psychosis has never been demonstrated in reliable trials.
We don’t need to go any further, but it might be interesting. According to the FDA, most of the deaths in the demented patients appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia).83 Young people on neuroleptics also often die from cardiovascular causes and suddenly.
And I would expect some of them to die from pneumonia. Neuroleptics and forced admission to a closed ward make people inactive. When they lie still in their bed, the risk of pneumonia increases. Depression pills, sedatives/hypnotics, and antiepileptics also increase the risk of pneumonia. Furthermore, a closed psychiatric ward is not a department of internal medicine, and if a patient develops pneumonia while lying zombie-like in a bed, it might not be noticed.
The psychiatrists are fully aware—and have often written about it—that the lifespan for patients with schizophrenia is 15 years shorter than for other people, but they don’t blame their drugs or themselves, but the patients.84
It is true that these people have unhealthy lifestyles and may abuse other substances, in particular tobacco. But it is also true that some of this is a consequence of the drugs they receive. Some patients say they smoke because it counteracts some of the harms of neuroleptics, which is correct because tobacco increases dopamine while the drugs decrease dopamine.
It is also indisputable that neuroleptics kill some patients with schizophrenia because they can cause huge weight gains, hypertension, and diabetes, but how common is it?
When I tried to find out why young people with schizophrenia die, I faced a roadblock, carefully guarded by the psychiatric guild. It is one of the best kept secrets about psychiatry that the psychiatrists kill many of their patients with neuroleptics.
I described my experiences with the roadblock guards in 2017 on the Mad in America website, “Psychiatry Ignores an Elephant in the Room,”85 but subsequent events were even worse.
Large cohort studies of people with a first-episode psychosis provide a unique opportunity for finding out why people die. However, as there is too little information in these studies, or no information at all, about the causes of death, you need to ask.
The TIPS study: 12% of the patients died in just 10 years
In 2012, Wenche ten Velden Hegelstad and 16 colleagues published 10-year follow-up data for 281 patients with a first-episode psychosis (the TIPS study).86 Although their average age at entry into the study was only 29 years, 31 patients (12%) died in less than 10 years. However, the authors’ detailed article was about recovery and symptom scores.
They took no interest in all these deaths, which appeared in a flowchart of patients lost to follow-up and were not commented upon anywhere in their paper.
In the text, they mentioned only 28 deaths (11%), so it was not even clear how many died. In March 2017, I wrote to Hegelstad and inquired about the causes of death. Most patients were still on neuroleptics 10 years after they started, which I considered very frightening because around half of them would have developed tardive dyskinesia (a terrible movement disorder, which is often irreversible but masked by ongoing treatment) and because many, if not all, would have developed permanent brain damage at this point.
I sent a reminder ten days later and was told I would get an answer shortly. Two months later, I wrote again and mentioned that it was important for the world to know what all these young patients had died from. I also asked if we needed to file a Freedom of Information request to get this information.
Hegelstad replied that they were preparing a manuscript detailing the information I asked for. The paper came out the next month, in World Psychiatry, but the number of deaths was now different from their first paper, and the information I had requested wasn’t anywhere.87
Two months later, Robert Whitaker and I wrote to the editor of World Psychiatry, professor Mario Maj, asking for his help in getting a unique insight into why so many patients had died so young. We hoped he would ensure that the knowledge the investigators had in their files became public by publishing our short letter to the editor and by asking them to respond. “That would be a great service to psychiatry, the patients, and everyone else with an interest in this vitally important issue.”
We explained in our letter that the authors had reported that 16 patients died by suicide, seven by accidental overdoses or other accidents, and eight from physical illnesses, including three from cardiovascular illness:
“In order to attempt to separate iatrogenic causes of death from deaths caused by the disorder, we need to know: When did the suicides occur? Suicides often occur early, after the patients have left hospital,88 and are sometimes iatrogenic. A Danish register study of 2,429 suicides showed that, compared to people who had not received any psychiatric treatment in the preceding year, the adjusted rate ratio for suicide was 44 for people who had been admitted to a psychiatric hospital.89 Such patients would of course be expected to be at greatest risk of suicide because they were more ill than the others (confounding by indication), but the findings were robust and most of the potential biases in the study were actually conservative, i.e. favoured the null hypothesis of there being no relationship. An accompanying editorial noted that there is little doubt that suicide is related to both stigma and trauma and that it is entirely plausible that the stigma and trauma inherent in psychiatric treatment—particularly if involuntary—might cause suicide.90
What does accidental overdoses and other accidents mean? Did the doctors overdose or did the patients overdose themselves by mistake, and which types of accidents were involved? Psychotropic drugs can lead to falls, which can be fatal, and suicides are sometimes miscoded as accidents.91
It is surprising that 8 young people died from physical illness. What were these illnesses exactly and what were the cardiovascular illnesses? If some of these people suddenly dropped dead, it could be because antipsychotics can cause QT prolongation.”
Eight days later, we were told by Maj that, “Unfortunately, although it is an interesting piece, it does not compete successfully for one of the slots we have available in the journal for letters.”
So, there was no space in the journal for our letter of 346 words, no longer than a journal abstract, and no interest in helping young people survive by finding out what kills them at such a young age. This was psychiatry at its worst, protecting itself while literally killing the patients.
Five days later, I appealed Maj’s decision:
“Allow me to add that people I have talked to in several countries about deaths in young people with schizophrenia—psychiatrists, forensic experts and patients—have all agreed that we desperately need the kind of information we asked you to ensure we get from the very valuable cohort of patients Melle et al. reported on in your journal.
There is widespread and well-substantiated suspicion that the reason we have not seen a detailed account of causes of death in cohorts like the one in the TIPS study by Melle et al. published in your journal is that the psychiatrists prioritise protecting their guild interests rather than protecting the patients. By declining to publish our letter and get the data out that Melle et al. have in their files, you contribute to that suspicion. We previously asked one of the investigators, Wenche ten Velden Hegelstad, to provide us with these data but were told on 10 May this year that they would be published … They have not been published, as what Melle et al. have published in your journal is not an adequate account of why these young people died.
Therefore, we call on you to ensure these data get out in the open, for the benefit of the patients. We believe it is your professional and ethical duty—both as a journal editor and as a doctor—to make this happen. This is not a matter about the slots you have available in the journal for letters. It is a matter of prioritization.”
We did not hear from Maj again. In contrast to the authors of the TIPS study, Danish psychiatry professor Merete Nordentoft was forthcoming when I asked her about the causes of death for 33 patients after 10 years of follow-up in the OPUS study, also of patients with a first-episode psychosis.92
I specifically mentioned that suicides, accidents and sudden unexplained deaths could be drug related. Nordentoft sent a list of the deaths and explained that the reason cardiac deaths were not on the list was probably because the patients had died so young. In the death certificates, she had seen some patients who had simply dropped dead, one of them while sitting in a chair.
This is how it should be. Openness is needed if we want to reduce the many deaths that occur in young mental health patients, but very few psychiatrists are similarly open as Nordentoft. I asked Hegelstad about the conflicting numbers of deaths and also asked to get details on the causes of death. I didn’t hear from Hegelstad again.
TIPS was supported by grants from 15 funders, including the Norwegian Research Council, the US National Institute of Mental Health, three drug companies (Janssen-Cilag, Eli Lilly, and Lundbeck), and other funders in Norway, Denmark, and the USA. I asked all the funders for detailed information on the deaths, emphasizing that funders have an ethical obligation to ensure that information of great importance for public health, which has been collected in a funded study, gets published.
The silence was daunting. In December 2017, the Norwegian Research Council published its policy about making research data accessible for other researchers, which left no doubt that this should happen, without delay, and not later than when the researchers published their research.
Janssen-Cilag replied: “We find the data on mortality published by Melle et al. 2017 in World Psychiatry fully satisfactory.” Both they and Eli Lilly encouraged us to contact the authors, which was absurd, as I had written to the companies that the authors had refused to share their data with us. Lundbeck did not reply.
Five months after I had written to the Norwegian Research Council, I received a letter from Ingrid Melle who had been asked by the council to respond to me. I was told I had misread Figure 1 in the original paper86 where I had counted 49 deaths. I hadn’t. Their figure is seriously misleading because flowcharts otherwise always show numbers of patients who were lost or died during a study.
I have redrawn the figure here:
Overview of Patient Participation in a Long-term Follow-up Study of Early Detection in Psychosis
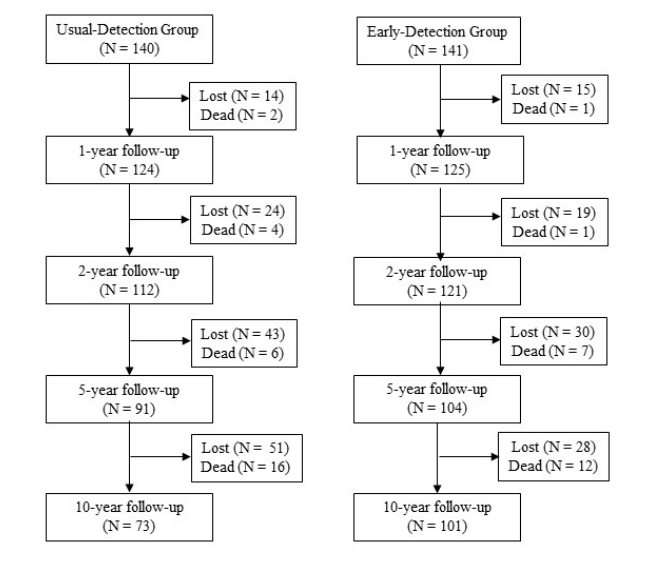
The reason that there were 31 deaths, and not 28, in Melle’s paper was because they had added one to three years of observation time, which didn’t exactly make it more transparent what the researchers had been doing.
Melle sent me a table, which was not particularly informative: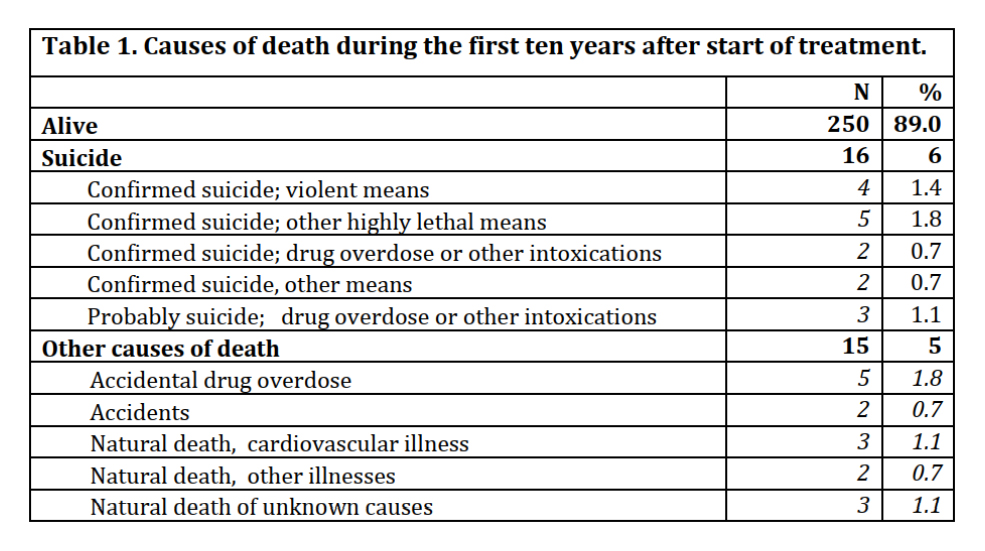
Melle explained that accidental drug overdose means taking too much of an illegal substance, or substance, or too strong a substance by accident, and that is does not refer to prescription drugs. If information about overdoses was ambiguous, it was defined as probable suicide.
This was really interesting. Why did 16 young people (6%) commit suicide in just 10 years? And why was this vitally important information not explored by the researchers? We cannot conclude it was their schizophrenia that led to suicide.
It is more likely the drugs enforced upon them, other forced treatments, involuntary admissions to psychiatric wards, humiliation, stigmatization and loss of hope, e.g. when patients are told that their disease is genetic, or can be seen in a brain scan, or is lifelong, or requires lifelong treatment with neuroleptics.
I am not making this up.4 It all happens, and some patients get it all. It is no wonder they might kill themselves when there is no hope.
The accidental drug overdoses are also of interest. The term is a bit tragicomic because patients with schizophrenia are usually overdosed by their doctors with prescription drugs and if they take an illegal drug as well, it is rarely possible to say that it was the illegal drug that killed them and not the prescription drugs. It could be the combination, and it might not have happened if the patient had not been forced to take neuroleptics and other dangerous drugs, e.g. depression pills and antiepileptics, both of which double the risk of suicide (see Chapter 1).
Finally, there were eight deaths from “natural causes.” It is not natural for a young person to die. I would have liked to know in detail what happened. It might be “natural” for psychiatrists that young people die in psychiatry but that’s because the psychiatrists ignore their own role in this.
I wrote again to the Norwegian Research Council, pointing out that Melle had told me that the data on causes of death contained the full information available to the doctors writing out the death certificates. I requested to see this information, in an anonymised format. I also noted that neuroleptics had been used liberally in the study and that some or all the deaths could have potentially been caused by the drugs the patients were on, which often involve polypharmacy.
I found it curious, considering the very high death rate of 12% (see Table 1 just above), that the authors had not discussed whether the deaths could have been caused by the drugs and had not reported which drugs the patients were on.
Finally, I noted that Melle had asked me: “Since you are writing with a Nordic Cochrane Centre letterhead, I’m curious if Cochrane has any plans for doing anything in this area?” I noted that I did not understand the relevance of this question. Why would I not use the letterhead for my own centre?
I heard no more. But Melle’s inappropriate comment about my centre’s letterhead, which I used in all official correspondence, seems to have been part of a concerted effort with the aim of removing me from my job as Cochrane director.36
Harassment from psychiatrists and Cochrane
In my letter to the 15 funders, the final paragraph was:
“You may consider this a Freedom of Information request, which means that if your organisation does not have detailed information on the deaths in the TIPS study, we expect your organisation to obtain this information from Hegelstad and to send it to us. Anything short of this would be unethical in our view, and we are convinced that patients with psychotic disorders agree with us (I am Protector for the Hearing Voices Network in Denmark).”
This would seem straightforward, but the US Stanley Medical Research Institute did not write to me. Instead, psychiatrist Edwin Fuller Torrey, associate director of research at the institute, complained about me in two letters to the CEO of the Cochrane Collaboration, journalist Mark Wilson, where he, among other things, wrote:36
“The Cochrane Collaboration’s credibility rests upon the assumption of objectivity … Such objectivity appears to be very much in doubt for Dr. Peter C. Gøtzsche who identifies himself as the Director of the Nordic Cochrane Centre and as the Protector of the Hearing Voices Network in Denmark. This organization promotes the belief that auditory hallucinations are merely one end of a normal behavioural spectrum, thus casting doubt on whether schizophrenia actually exists as a disease, and that hearing voices are caused by trauma in childhood, for which there is no solid evidence. Given such clear lack of objectivity, I personally would not find any Cochrane publication on mental illness to be credible.”
Torrey also wrote that the Hearing Voices Network encourages people who take neuroleptics for their schizophrenia to stop taking their medication, and that, “It is very difficult to imagine how anyone with these views could possibly be objective regarding a Cochrane study of antipsychotics, thus impugning your credibility which is your most important asset.”
This was bizarre. How can my objectivity be “very much in doubt” when I merely ask for the number of deaths and their causes? Furthermore, contrary to Torrey’s assertions, there is solid evidence that psychosis is related to childhood traumas, with a clear dose-response relationship.29,30
Torrey also drew the logically false conclusion that because I am protector of the Hearing Voices Network, no Cochrane publication on mental illness is credible. There is no relation between these two things. Here is an excerpt of a comment the Network sent to me:
“We take issue with Torrey’s attempts to discredit the Hearing Voices Movement to add leverage in his attempt to discredit Professor Peter Gøtzsche. In 2016, we invited Gøtzsche to be protector because of his pioneering work regarding psychiatric research. We are honoured to have him as our protector.
We believe that Torrey’s comments to Mr. Wilson regarding Gøtzsche being our protector to be bordering on the ridiculous when he attempts to discredit the whole Cochrane Collaboration.
We would ask that Torrey stops using the network as a platform to insult a respected professor along with the Cochrane Collaboration. We would also suggest that he considers apologizing for his disrespectful remarks about voice hearers.”
The motto of the Cochrane Collaboration is “Trusted evidence,” which Wilson had demanded we should all use, also in our letterheads, as if we were a drug company and not an independent scientific organisation registered as a charity. He also required we used short names for our centres, which created great confusion among journalists who often wrote the “Cochrane Nordic Centre” even though my centre’s name was the “Nordic Cochrane Centre”:
Cochrane’s motto is highly misleading when it comes to its reviews of psychiatric drugs. As I have explained above, very few of them can be trusted.
My criticism of the drug industry’s organised crime,4,51 psychiatric drug trials, and the overuse of psychiatric drugs was never popular at Cochrane headquarters after Wilson took office in 2012 and changed an idealistic grassroots movement into a business with a focus on brand and sales.36
Wilson and his deputy’s harassments of me were particularly damaging after I published the article about 10 myths in psychiatry that are harmful for the patients in 2014,38 and when I explained in the BMJ in 2015 why long-term treatment with psychiatric drugs causes more harm than good.36,94
Wilson also bullied me on this occasion. Instead of dismissing Torrey’s complaint, which was the only right thing to do, Wilson wrote to me that I had broken Cochrane’s Spokesperson Policy by using my centre’s letterhead and my title and that this would reasonably lead any reader to assume that the request was from the Nordic Cochrane Centre and that the views expressed were those of the centre.
Wilson wanted to apologise to Torrey for “any confusion in this regard.” Quite interesting, that one bully wanted to apologise to the other bully when the person between the bullies had done nothing wrong.
The setup was ridiculous, and even Cochrane’s own hired lawyer didn’t find I had broken the policy, neither in this case, nor in another similar case that was also about psychiatry,36 but such trifles don’t matter for bullies. There was no problem, but Wilson invented one. It was clear that the request came from the centre; that I as Director was authorised to speak on behalf of my centre; and my views were even shared by my staff. Furthermore, my letter was not a public announcement, but a letter to a funder. No one could become “confused.”
US lawyer Ryan Horath described the farce this way:36
“Cochrane leaders became obsessed about Gøtzsche using Nordic Cochrane letterhead to send this request. And a very large number of people seem to agree with the board’s obsession … JESUS CHRIST, WHAT IS WRONG WITH YOU PEOPLE? A researcher is making inquiries about the suppression of information regarding children who died in a clinical trial and everyone is worried about what letterhead it is written on? … Even worse, it is clear the outrage over use of Cochrane letterhead is feigned outrage, as this was a private letter. Was Fuller Torrey confused about whether the letter represented Cochrane’s views? Apparently not … Instead, Torrey argued that Gøtzsche was not ‘objective’ and this damaged Cochrane’s reputation—something totally different … So, Cochrane leadership’s use of this complaint in its case was misleading. The complaint is about one thing, and they used it as evidence of another (false allegation). That is how kangaroo courts operate.”
What is the bottom line of neuroleptics?
Countless unreliable studies have been concocted to fabricate a fairytale about neuroleptics helping people survive their psychosis. I have dissected some of them in my previous book.4 They have serious flaws and the patients that are being compared—those on neuroleptics and those not—are not comparable to begin with. Particularly a Finnish doctor, Jari Tiihonen, has published one misleading study after the other.4
Don’t pay any attention to these reports. Whitaker once wrote to me that it required extraordinary mental gymnastics by the psychiatrists to conclude that these drugs, which cause obesity, metabolic dysfunction, diabetes, tardive dyskinesia, lethal cardiac arrhythmias, and so on, protect against death.
Furthermore, as noted above, the psychiatrists often take away the patients’ hope of one day living a normal life. Why bother about having a healthy lifestyle, if life will never be worth living? It is not only neuroleptics, often in combination with many other psychiatric drugs, that kills the patients, it is the whole package psychiatry delivers to them.
If acutely disturbed patients need something to calm them down, benzodiazepines are far less dangerous and even seem to work better.95 When I have asked patients if they would prefer a benzodiazepine or a neuroleptic next time they developed a psychosis and felt they needed a drug, all of them have said they preferred a benzodiazepine. Why don’t they get it then?
- Do everything you can to avoid getting treated with a neuroleptic.
- Do everything you can to avoid anyone dear you to get treated with a neuroleptic.
- If a doctor insists, give the doctor a copy of my book and say you will sue, if the doctor ignores you.
- Ensure you can document that you warned the doctor, e.g. by recording the conversation, bringing a journalist to the meeting, or demanding a written note from the doctor on the spot, not later. If doctors get in trouble, they often deny what happened, and they might even change the written records.45
To read the footnotes for this chapter and others, click here.














Being on vitamins for 45 years, I find myself reading the psychiatric excuses for this sort of thing amusing, in a dark sort of way. If these Big Time Shrinks found out about me, they’d beg me to stop poisoning myself and get into proper treatment with safe proper drugs. This article helps me realize that Big Time Psychiatry is led by delusional medicos (and who’d want to be doped up by delusional individuals with poisonous neurochemicals?).
Report comment
Great, and very accurate, information regarding the neuroleptics. Thank you, Dr. Gøtzsche. And you are absolutely correct that the psychologists and psychiatrists lie to their clients and their families, claiming their “invalid” DSM disorders are “lifelong, incurable, genetic” illnesses. Which, of course, destroys marriages and takes away hope. Unless one knows, for a fact, that they have zero history of “mental illness” in their family.
And, as one who was made “psychotic” with the neuroleptics, I will mention that the neuroleptics/antipsychotics can make people “psychotic,” via anticholinergic toxidrome.
https://en.wikipedia.org/wiki/Toxidrome
And, as to the relationship of “hearing voices” and childhood trauma. As the mother of a child abuse survivor, I learned the hard way that psychologists and psychiatrists often function as the child abuse covering up arms of the paternalistic religions, at least my childhood religion. The leaders, of which, are being pointed out, as the systemic child abuse covering up criminals, that they actually are, by the ethical within.
https://books.google.com/books?id=xI01AlxH1uAC&printsec=frontcover&source=gbs_ge_summary_r&cad=0#v=onepage&q&f=false
But an ethical pastor of a different religion did confess the crimes, to which my family had been subjected, to be “the dirty little secret of the two original educated professions,” implying it’s likely most religions. And I have met with Catholic child abuse survivors’, and their parents, to whom I had to recommend Whitaker’s book, “Anatomy.”
But since I was able to get my child away from the child molester quite quickly, my child was able to heal, and go from remedial reading, after the abuse, to graduating from university with highest honors (Phi Beta Kappa), even also winning a psychology award. His psychology professors couldn’t have gushed more about how brilliant and well adjusted my son was at his graduation.
“If doctors get in trouble, they often deny what happened, and they might even change the written records.” Yes, I was handed over medical records with big black Sharpie marks all over them, covering up the name of a child abusing pastor, as well as his pedophile best friend’s, and his wife’s, names. And I was not handed over a few of my and my family’s medical records at all.
And I will say, those ELCA psychologists I worked with will stop at nothing, to cover up their, or other psychologist’s, their pastor’s, bishop’s, and the psychiatrists’, systemic child abuse covering up and profiteering crimes.
Thank you so much, for reporting on the truth, despite the attacks, Dr. Gøtzsche. In my personal opinion, you’re doing God’s work, while being defamed for being an ethical scientist. Thank you so much for all you are doing.
Report comment
4. Do you honestly believe a doctor might deny what happened, or change the written records?
https://drive.google.com/file/d/1vYO9r1FkdJSv8Bi8Q3c3u9WXNZXkmxvO/view?usp=drivesdk
https://drive.google.com/file/d/1bTUsvmamFk3-CA0wKPDlJMakxLGUJFBq/view?usp=drivesdk
Or that a Coroner might?
https://www.irishexaminer.com/opinion/commentanalysis/arid-40071311.html
https://www.irishexaminer.com/news/munster/arid-40234565.html
https://www.irishpost.com/news/cork-man-kills-his-two-brothers-with-axe-before-drowning-himself-in-suspected-double-murder-suicide-204822
https://www.irishtimes.com/news/ireland/irish-news/cork-murder-suicide-father-may-have-persuaded-younger-son-to-take-part-1.4413853
https://en.m.wikipedia.org/wiki/Akathisia#:~:text
AKATHISIA = 1. Out of Character and.. 2. Extreme Behaviour 3. ..following the (a). Stopping (b). Starting (c). or Changing (dose of) a Psychiatric Drug (i.e. Neuroleptic/’Antidepressant’).
Report comment
I notice people tend to shy away from the more frightening practices in “MH”, like treatment induced death and disability, but these need to be faced up to, so that situations can be improved.
Report comment
There is no doubt that antipsychotics are extraordinarily toxic, are over prescribed, and don’t “cure” psychosis. In addition, I have no doubt that few psychiatrists explain the dangers of antipsychotics to their patients, which is nothing less than malpractice. Nonetheless, some people suffer so much from a psychotic condition that antipsychotics may be the only help currently available. Such a prominent psychiatric critic as Joanna Moncrieff, for example, has written, “I still think antipsychotics can be useful, and that the benefits of treatment can outweigh the disadvantages, even in the longterm for some people.”
Other toxic drugs are prescribed at times because nothing else is available, for example, chemotherapy for cancer. That antipsychotics may have limited usefulness under some circumstances does not mean that they are not misused most of the time.
Report comment
But there isn’t evidence neuroleptics have even short term benefits for psychosis. Studies claim so do so by claiming withdrawal means the drugs are good, or that sedating and disabling someone is a “benefit”. Those who want to claim disabling and drugging some one into a coma like state is a good thing, need to be up front that their idea of a benefit is social control and silencing people.
Report comment
Oh yes, there are benefits. They help to cause psychosis or more psychosis and thus the psychiatrists need to up their dosage to the patient or add other anti-psychotics or other drugs to create for the patient, an even more deadlier drug cocktail. Oh, I forgot to mention who received the benefits—the psychiatrists and big pharma, etc. And the benefits for the patient….Stammer, stutter, well they’ve got to be there somewhere like the check that never ever was in the mail. Thank you.
Report comment
These “drugs” are very even abused. The “usefulness” of those remedies always consists of one thing. – – In suppressing the will of man. They help themselves. Yet to someone. But only not to the one whom they undertake to “treat”.
Report comment
So thankful there are warriors for the truth like yourself Dr. Gotzsche striving to protect patients. Thank you for your continued research in the face personal attacks for seeking truth and facts.
“Finally, there were eight deaths from “natural causes.” It is not natural for a young person to die. I would have liked to know in detail what happened.”
My brother died suddenly and without explanation while in psychiatric ‘care’. He had temporary sadness over his divorce and children moving with their mother. He was sent to a psychiatrist and put on psych drugs. He was a musician, engineer and physically fit but instead of improving he went downhill on the drugs. He became disoriented and experienced cognitive dysfunction and when he could no longer work he was given ECT. He died suddenly one night while trying to get out of bed. No cause of death was determined, it was simply ruled inconclusive. As you state, it is not “natural” for a healthy person at 40 years old to suddenly die – with no explanation. We were shocked his death didn’t warrant any investigation and strongly believe his early death was due to psychiatry.
Report comment
Rosalee, I wonder if you started grieving him even more, with a new awareness of just what transpired
and how there is nothing that can be done, no one to convict.
Psychiatry is an insidious disease. They really are like a pathogen.
Once it enters the body, it feeds itself.
He went for support, and entered the wrong door. It’s always about the wrong place, wrong time and wrong people.
Report comment
When I first heard one of my friends committed suicide it was hard. Later I discovered the research on how every major psych drug more than doubles suicides, and how they cause akathisia which my friend had. I cried daily for two weeks, racked with guilt that I hadn’t discovered the research earlier and saved him.
I proceeded to go around mental health forums posting the research as a form of catharsis. Many people were helped including myself but for the most part the responses were insults, lies and logical fallacies followed by censorship. Turns out being pro-science to most people is defined as ignoring the evidence and covering up with illogical assumptions. Many people also view it as stigmatizing if you do not tell people they are mentally defective. It is a brave new world, drugs, conditioning, biological classes and all.
Report comment
A lot of people are “pro-scientist” rather than “pro-science.” They thing science is something that other smart people in lab coats do, and they then report their findings honestly and all we need to do is follow their recommendations. The idea that scientists could be dishonest or corrupt or just plain incompetent and narrow-minded is too much for them to process. It’s more like a religion than a logical conclusion. Real science is scary to those people, because it requires them to personally sift and evaluate the evidence, instead of deferring to “the authorities.” So they get very upset at people who question their “pro-scientist” dogma!
Report comment
I believe good people do bad science under the “publish or perish” conditions in which most academic researchers exist. Other good people do bad science under “do this or lose my job” economic conditions of corporate research. I don’t believe that most researchers who contribute to bad science are personally bad people. Just consider the way this country treats whistleblowers.
In my experience, people love to speculate about the choices they would make in various situations but you don’t actually know until you’re the one choosing between speaking up and protecting your livelihood. When you’re having to decide if some situation is really all that bad.
This is a cultural issue where we are all regularly choosing between protecting ourselves and protecting others. I once violated a company policy against telling a security client calling into our inbound call center to escalate to calling 911. I lost my job and I’m not sorry. I don’t know what happened to my caller but I’m convinced her life was in danger. But my managers took me into private meeting when I arrived for my next shift to explain how I had violated the company policy. I was told I could continue on probation or I could resign. I chose to resign. I was a low level employee and a job was a job to me. But for those at higher levels, with more years experience, they have a lot more to lose and may have made a different choice. They may have gone against their instinct and followed policy to begin with despite what they could hear on the line. The point is, we often don’t know the factors that drive individuals to make the choices they do. Good people often make “bad” choices for personal protection. And we need to understand the reasoning before we vilify them.
Report comment
@Steve — The operant contradiction is the worship of science as a value in & of itself vs. seeing it as a means to an end. Science can be used to achieve beneficial ends and incontrovertibly evil ones (ever hear of napalm?), so giving something credibility because it’s “scientific” is like automatically trusting someone because they’re “spiritual.”
Report comment
True, but a slightly different issue from what I’m talking about. The idea of science being “value neutral” is extremely problematic, as Robert Pirsig so eloquently elucidates in “Zen and the Art of Motorcycle Maintenance.” But what I’m talking about is a form of almost religious worship of Scientists as the All Knowing, so smart and informed that us mere parishioners are too ignorant and easily misled to be able to understand their deep knowledge. Doing what the Scientists say makes us Smart and Clever free from the curses of Superstition and Blind Faith! The fact that this is another form of Blind Faith does not occur to the faithful. Science is Truth, and to question this is Sacrilege! Oops, I mean Unscientific! Psychiatry is able to use this kind of blind faith to maintain its hegemony despite the fact that their own scientific researchers (not to mention basic logic) have proven that their diagnoses are nonsense and that their “treatments” tend to make people worse rather than better, and in fact to shorten their lives. To question Psychiatry is to question Science, and who are we to question the wisdom of the Great Scientific Gurus!
Report comment
I don’t think we’re talking about different things at all, maybe slightly different inflections. Science AND psychiatry have replaced religion as something to believe in for many “rational,” “progressive” people. And psychiatry is hardly the only form of tyranny invoking “science” as its justification.
Report comment
I agree 100% on THAT point! I think I’m emphasizing more what people’s attitudes have become, and you are emphasizing more how that attitude has been used to mislead the public. There is nothing “rational” about believing some subset of humanity, with sufficient intelligence and training, can somehow determine what is “true” for the rest of us. It’s just as superstitious as believing in evil spirits. Maybe a little more so!
Report comment
Science is a means to an end. Science can serve both good and evil in equal measure. Therefore, science can in no way be a moral guideline.
Report comment
Quite so. Science is about establishing what is TRUE, not what is RIGHT.
You should read “Zen and the Art of Motorcycle Maintenance.” It speaks to this very issue! One of the best books I’ve ever read!
Report comment
A devilish substitution of concepts takes place here. The word “science” takes on a moral meaning. (Whereas it is only a means.) And from the moral comes the next “jump” – she takes on a legal meaning. And then she becomes power.
This substitution is clearly visible in the example of psychiatry. Psychiatry replaces legal concepts with psychiatric ones. Instead of guilt – disease. Instead of evidence – diagnostics. Instead of punishment – treatment.
Report comment
Steve, science isn’t even about establishing what is true. Old scientific laws and theories are being updated all the time. Science is about developing knowledge through testing and validating hypotheses. A true scientist does not try to make the data fit the conclusion. A true scientist begins with curiosity and when the conclusion does not match the hypothesis, he says “hmm, that’s interesting!”
Most current “science” is junk because the motive to conduct it is not the accumulation of knowledge but rather profit or prestige. When the advancement of your career depends on you coming up with another tome of bullshit, people comply in the essence of self-interest. Ph.Ds are called “piled higher and deeper” for a reason. There has been a lot of bullshit published in the name of science that humanity could simply compost.
Report comment
This is what makes physics so interesting. Physicists seem the most in pursuit of contradicting everything we think we know about how the universe works! They handle ambiguity really well. And you have to be barking mad to even conceive of some of the more recent experiments going on at CERN.
https://www.nytimes.com/2021/04/07/science/particle-physics-muon-fermilab-brookhaven.html
Report comment
That’s how REAL scientists act! Maybe we can get them to take a similar approach to psychiatry! I’m sure they’d be appalled.
Report comment
Many people were helped including myself but for the most part the responses were insults, lies and logical fallacies followed by censorship. Turns out being pro-science to most people is defined as ignoring the evidence and covering up with illogical assumptions. Many people also view it as stigmatizing if you do not tell people they are mentally defective. It is a brave new world
Well, this is the state of modern “discourse,” with Newspeak being a major component. “Science” is defined by what “all the cool kids” think — not based on repeatable experiments and bias-free interpretation of data, but determined by taking polls of selected people with “official” credentials of “scientist.”
Report comment
You have to distinguish the difference between science and scientism. The only real connection between science and scientism are the letters s, c, i, e, and n. Scientism is a dogma that claims the infallibility of past and present scientific conclusions, while actual science seeks to know if such conclusions are really true.
Report comment
Right you are! The very essence of science is skepticism, the willingness to invalidate any and all conclusions in the face of new data, and in fact, the drive to do all we can to try and invalidate a particular theory that SEEMS to be true, and only accepting it as truth when all other explanations are proven to fail. And even then to be prepared for new data to force modification. The concept of “scientific truth” is badly misused, as “scientific truth” by definition is always subject to change. Even Newton’s Laws of Motion, long held up as the ultimate in “proven fact,” ended up being approximations. Who knows what we’ll discover in the future, if we stop pretending that some “smart people” already know everything and that we can stop looking and just let them tell us what is true!
Report comment
Yes Sam, you are right with that analysis. For the first few years after his death I was confused as nothing made any sense as to why he spiraled down AFTER he was supposedly getting ‘help’. Then came my own encounter with a psychiatrist during cancer treatment with psych labels and many psych drugs pushed on me while I was still battered by chemo and so dizzy I had fallen and suffered a head injury. I was shocked at how dishonest and toxic the psychiatrist was, just dismissing everything and mocking the side effects and I began to question more what happened to my brother. After finding MIA I realized my concerns and fears were well founded. I do grieve his death more knowing it didn’t have to be and that he was not ‘defective’ as psychiatry likes people to believe but instead was drugged into a stupor for having a normal reaction of grieving his losses.
Report comment
And there’s this Sam, the system is so broken you can’t trust the coroner either.
https://www.eventbrite.co.uk/e/why-cant-you-hear-me-tickets-147545958935
Report comment
Peter, thank you so much for speaking to this pandemic in a conscious way.
I just noticed that there is a new Town Hall coming up with open dialogue being the discussion, and how this might unfold with perhaps the use of “less medication”.
What bothers me about that is the use of the word “medication”. It is very obvious that the dialoguers do not want to “offend” psychiatry. People are very afraid of looking and sounding nuts or like a fruitcake, so they kiss the industry ass. The media ass.
But then it’s a business, a new one. Pretense that OD can be incorporated into the, (as Sami Timimi points out) “Rotten to the core” psychiatry.
One would think that people who have been in the system, have seen it operate, would be totally honest about it’s language.
Report comment
I can’t speak for anyone else but it may in part be a strategy in order to get people to consider the discussion and look at the evidence. The common response from people if you go and present science research showing psych drugs have no benefits is being bombarded with insults. People won’t even look at the evidence or consider entering a discussion unless you give enough lip service to their mass willful ignorance.
I’m not sure this lip service is at all effective but I understand people utilizing it. I tried various forms of changing how I presented the science in order to get people to objectively look at it. I’m now of the opinion that it has little to do with how it’s presented and more to do with people’s inability to admit they are wrong and have caused harm.
Report comment
Dr Peter, even though English isn’t your first language, you are easy to understand and compulsively readable. This book really gets the needed message across.
Report comment
Peter, I can’t thank you enough for this article and this whole series. It is hard to imagine that professionals will go to such extremes to defend/deny the lethality of what they are doing. Crusaders such as yourself are making a change in public perception, slowly but surely. I am only sorry that your efforts should be met with such opposition.
Report comment
“Science can be used to achieve beneficial ends and incontrovertibly evil ones”
https://odysee.com/@shortXXvids:e/WHOGatesCorruptionPartIII:3?src=open
Report comment
Dear Prof. Gøtzsche,
Thank you this life-saving information. I would offer the patients self-help measures for sedation, instead of benzodiazepines (which are highly addicitve and dangerous drugs):
1. Increasing doses of a mixture of sedative herbs (at least six herbs) until an effective dose is found.
2. Increased air temperature, additional clothes. Hot baths can be added too.
3. Walking outdoors for 1-2 hours daily.
4. Eat raw honey with each meal.
5. Another sedative food is animal fat, either raw or boiled in water (not fried). For example, tail fat without meat or beef fat without meat. It is safe to eat raw tail fat (and it is tasty) if it is bought in a kosher or halal store (no risk of dangerous pork parasites). The fat can be eaten with a salad or soup or alone.
6. Eat more raw nuts (preferably pulverized), another sedative food.
7. Breath-holding exercises, 3 repeats with an interval of 2-3 minutes, 2 or 3 sessions per day.
8. Complete relaxation (possibly a nap) in the middle of the day for 20 min.
9. It is important to stop all activating measures, such as sunbathing, cardio exercise, cold showers, and stimulatory foods and drinks (tea, coffee, cacao, soft drinks, chocolate, any foods containing raw meat or fish, such as sausages, cured meats, sushi, etc.)
10. The person who needs sedation or experiences hallucinations has to review his/her lifestyle comprehensively and make corrections, for example, a person eating mostly junk food and smoking cannot expect to have good mental health. Excellent ideas about healthy nutrition were published by dentist Weston A. Price almost 90 years ago, as a result of his extensive travels and examination of various uncivilized populations across the globe. His book “Nutrition and Physical Degeneration” is now freely availabe on the Internet (in the public domain). He found that such primitive populations who have no access to modern foods based on refined sugar, canned foods, white flour, etc. have no equivalent of prisons and mental hospitals because they don’t need them. Many such populations are 100% free of tooth decay even though they don’t brush their teeth.
Most of the above measures make sense, are safe, easy to try, do not require payments to a special interest group, and do not need “scientific” proof. Actually, if one or two patients with a schizophrenia label are cured by this regimen, then this is stronger evidence than a double-blind randomized controlled trial, which is inherently not designed to detect a cure.
Report comment
This is the part of the article I liked the best. :
The TIPS study: 12% of the patients died in just 10 years
In 2012, Wenche ten Velden Hegelstad and 16 colleagues published 10-year follow-up data for 281 patients with a first-episode psychosis (the TIPS study).86 Although their average age at entry into the study was only 29 years, 31 patients (12%) died in less than 10 years. However, the authors’ detailed article was about recovery and symptom scores.
” They took no interest in all these deaths, which appeared in a flowchart of patients lost to follow-up and were not commented upon anywhere in their paper. ”
That last sentence says everything about the kind of people we are dealing with here. : mass murdering psychiatrists with a reckless disregard for human life. ( Since they are fully aware of what their drugs do. ) It’s just too bad that the good doctor Peter Gotzsche has to grovel to the study authors with letter after letter to get answers about the cause of the deaths. If the Western Hemisphere had an even halfway decent legal system that actually worked for the people; legal force could make the doctors talk.
Report comment
It is the only medical “treatment” where the odds of survival are DECRASED by receiving “treatment!”
Report comment
At the end of this article, it is asked why don’t the patients who were prescribed neuroleptics offered a prescription for a benzodiazepine. However, it is well known that “benzos” as they affectionately called are probably equally as dangerous and as addictive. Withdrawal from either types of drugs can usually only be described as “hell.” I have been prescribed “benzos” without a neuroleptic (briefly) and then neuroleptics with an accompanying “benzo” prescription. The “benzo” prescription, I was told by the psychiatrist, was to offset the side effects of neuroleptics, specifically the T.D. and the restlessness and anxiety associated with the neuroleptic. I was taken off the neuroleptic and the “benzo” abruptly due to a near comatose incident that put me in the hospital. I was reintroduced to several different neuroleptics, but, I was not prescribed any “benzos” again in my recollection. In psychiatric drugs, it does not depend on which type, the only answer that should be given is “NO!” Not even briefly can they be used. These drugs are THAT dangerous! Thank you.
Report comment