
Every culture has its share of individuals who break down in bewilderment. People who hallucinate, behave beyond norms, seek to die, think in strange ways. Called many things—witches, patients, healers—we are met with as many responses, each reflecting how our culture understands help. The photograph below was taken in a Denver psychiatric hospital in 2016.1 Look closely: this is what help in the U.S. looks like today.
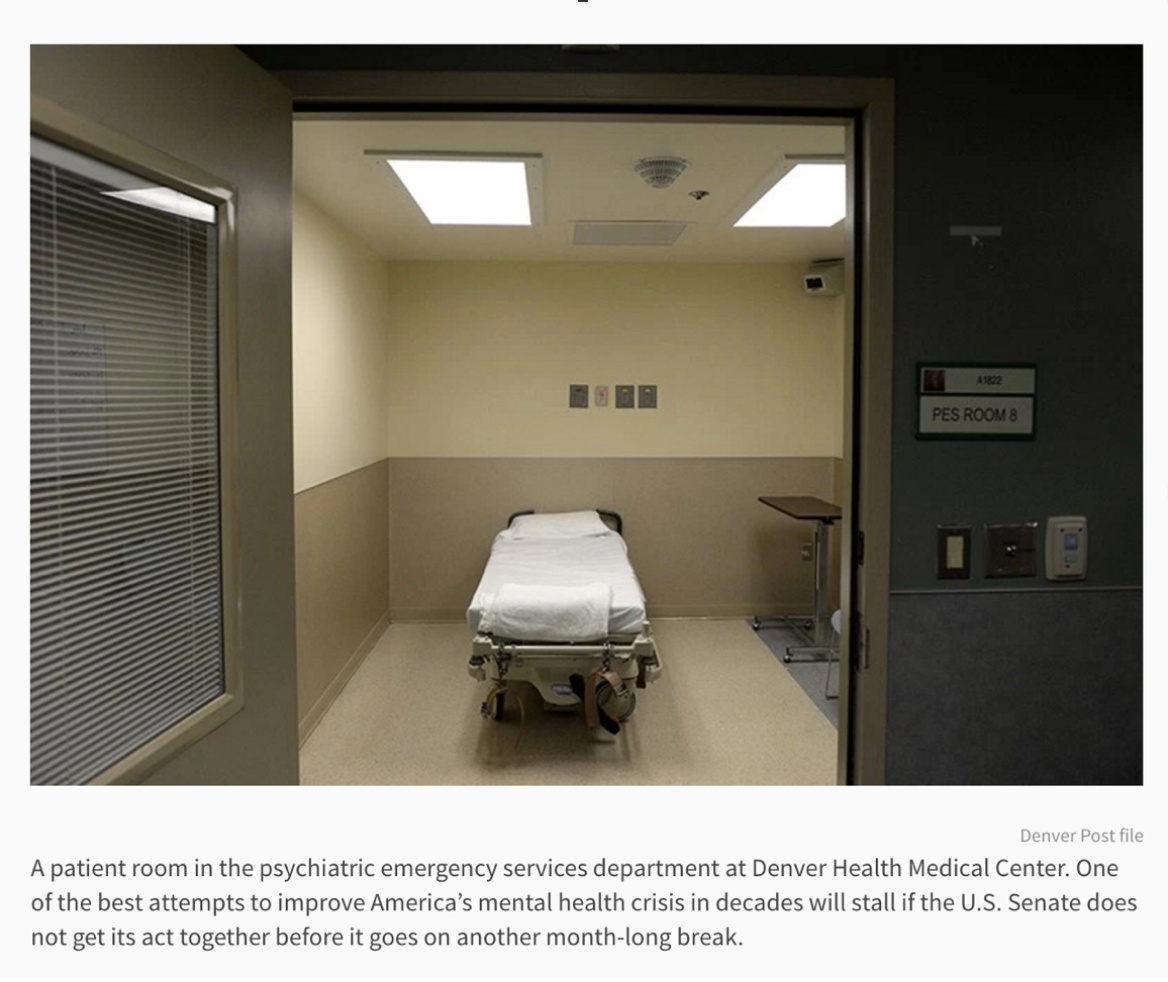
On a surface level, a clinical level, I see a rollaway bed with leather belts dangling. Belts that strap people down to be hauled without contest. I see an impenetrable camera lurking in the corner. Instead of first and last names, I see numbers and acronyms coding the roomʼs function. Fluorescent light drops evenly so nothing hides in shadow; I see brown and beige and dark grey cooling an empty box. Order reigns.
What I notice most, however, is not the presence of severe state technology—a scene akin to capital punishment—but the absence of the most essential ingredient for anyoneʼs sanity: love. It is impossible to love in this room.
By love, I do not mean an everything goes love that lacks discernment, nor do I mean a mutated tough love that absolves punishment. I mean a deliberate effort to be vulnerable with another person in an attempt to deeply bond. Of course, love is not all we need, but the culturally-ordained, legalized intention of this room—to help people in high distress—is unachievable without it. Love is necessary for helping minds. Remove a chimpanzee from her tribe and lock her in a cage, a week later sheʼs self-injuring (a trait never seen in the wild).2 We can forcibly tranquilize her until sheʼs too sedated to do anything but obey, or we can bring her back to the tribe.
But entering a psychiatric hospital I am no longer part of an ecology. I am stripped of clothes and context, my stories reduced to sputters from a broken sprinkler. Lit and watched in perpetual spotlight, I am objectified, examined. The gulf between myself and the mental health workers trained to hold a distance—to oppose love, flames the searing disconnection that caused my crazy. And for my bewilderment, I am not only exclusively liable, but punished, in this room where violence is state-sanctioned—a violence the United Nations calls torture.3 The most likely time anyone completes suicide is within two weeks of departing a psychiatric hospital.4
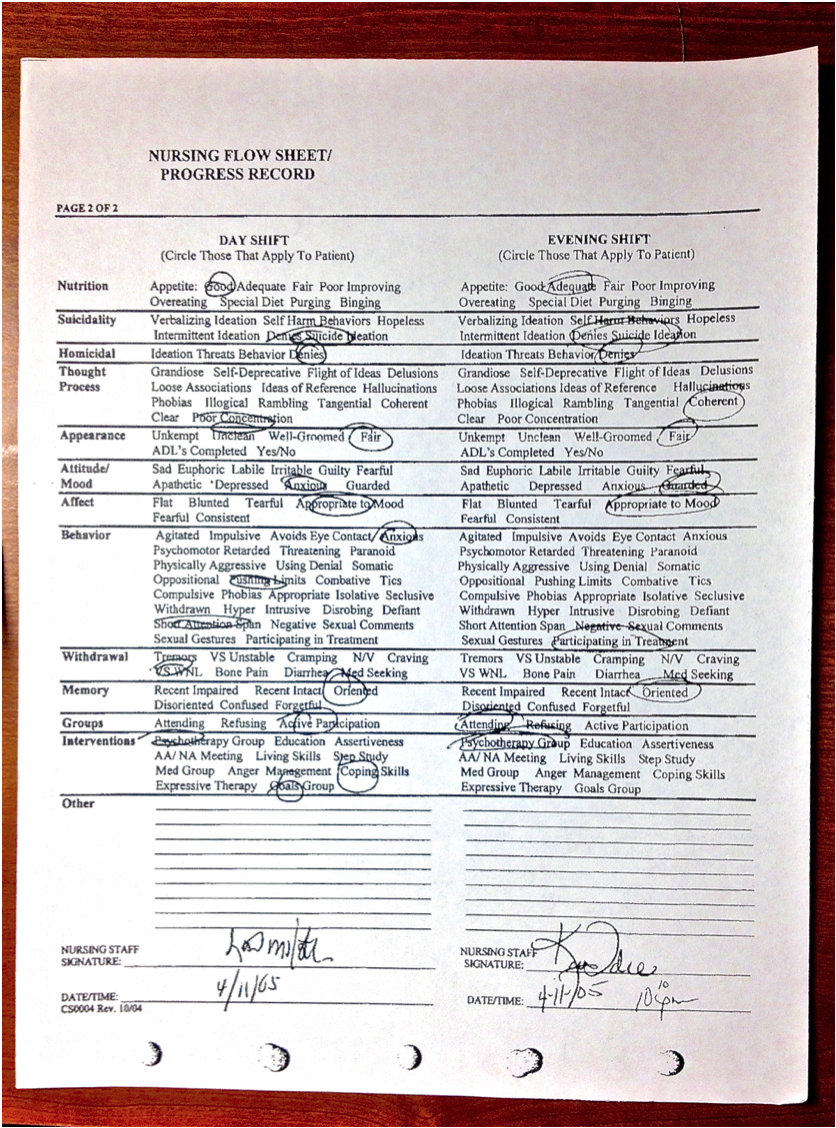
Look closely at this psychiatric nurseʼs note about me: this is the language of help. Blaming, scouring even, no mention here of the evaluator, just a collection of acrimonious terms illustrating my malfunction. Guarded, Labile, Psychomotor Retarded, Guilty, Ideas of Reference—words to affirm expertise of mind and behavior. Evaluative rather than relational, this language of help creates a distance necessary for arguing my reality as sickening. No one wakes up and says to their friend, I am feeling oppositional, grandiose, and intrusive today, with a self-deprecative and tangential thought process. We could talk together about fear, hope, pain, joy, confusion, excitement: concepts that include me in the tribe, even connect. But the first step to abusing someone is otherizing them. Thank God I was pushing limits that day.
I have worked in places with helping rooms. I have been locked up next to them (though privileged to have never been in one). I am not Pollyannaish to the difficulty of loving strangers who flip out or present danger, so in our culture’s vacuum of support, I can understand how this morally indefensible room intended for the least controllable of us makes logical sense. In the last hundred years, so did cramming ice picks in our eye sockets—which won its auteur a Nobel Prize,5 so did sterilizing us,6 so did institutionalizing us forever, so did electrocuting our brains against our will. All of these treatments were widespread, legal, celebrated, and considered modern scientific advances furiously defended by people with the highest education.7 They were committed in the spirit of our own good, and as such were unassailable by individuals who felt themselves harmed. Only when Life Magazine showed giant photos of these horrors to the American public did our culture begin to question whether it was helpful.8
Today, many U.S. citizens do not see that same monstrosity in this room. For decades, pharmaceutical companies and their colluding psychiatrists have crammed megaphones with unsubstantiated messages that mental illness is a brain disease— and nothing else. As such, help now means manipulating the brain, the organ of ultimate prestige; a legitimizer for psychiatry, and the most profitable.9 And theyʼve won. Witness Abilify, a drug originally developed for psychosis, last year outselling every other medicine of any class in the United States.10 Thatʼs a lot of power, and itʼs increasing.11 Never mind that trauma you likely experienced before breaking down;12 a brain isn’t manipulated on a couch but in a hospital, where doctors work, and who still, as always, know best. So the Denver Post editorial board is not outraged to see this room—in fact, their op-ed (from which the first photo is taken) is titled Congress is Painfully Close to Passing Mental Health Reform—nor is the American public. Because a brain doesnʼt need love, it needs control.
And controllers. To be clear: helping rooms are the problem, not necessarily their employees. I have sat at tables where hospital workers and psychiatric survivors alike acknowledge them as traumatizing, sometimes for both sides. Many psychiatric hospital workers find their work miserable and exhausting,13 in part because they must act in unnatural, professional (code for distant), and sometimes violent ways towards people. But insofar as staff hold all the power in these rooms, we need them to revolt.
Arguments for using state-sanctioned, legalized violence in this room often get tangled in details: What other option did we have for this person at this moment? Which illustrates the questionʼs redundancy. When you operate under a one-size-fits-all medical model funded with almost every dollar by the National Institute of Mental Health,14 there are no alternative routes in the mainstream to illustrate a better way (though they do exist outside the mainstream). We said the same thing about lobotomy: What other option? Answers cost something. Money follows public outrage.
So while I do not believe critics of this room and creators of new ways can outrun the psychiatric and pharmaceutical mammoth controlling the narrative, cash flow, and legislation for our cultureʼs understanding of help, I do believe we are building a critical culture of resistance. One ready to steer new ships should the public tide turn. And from that culture, my Hail Mary is another Life magazine exposé. A meme, a movie, a hashtag, an image that evokes the barbarism of this room to citizens who never know the bruise of leather straps with no reason to investigate psychiatric corruption. Something so potent and outrageous that the American public does not care anymore about What other option did we have for this person at this moment? They just see the horror and press Eject. No More. Like lobotomy, they say, To hell with your Nobel Prize, this cannot stand—and instead vote for love.
*****














This sorry room reminds me of an action Humphry Osmond did when he became superintendent of Weyburn Hospital, an overcrowded dump in Saskatchewan. He reconditioned the institution’s seclusion rooms into places patients with sensory/emotional overloads might actually want to visit, where it was sometimes harder to get them out than to get them into. Of course, he’d taken a variety of hallucinogenic drugs himself, and encouraged his staff members to take LSD themselves, to briefly experience what the patients were experiencing constantly. Had he done that today, he’d have wound up in a little sterile room like the one in the photograph.
Report comment
Psychiatric outpatient contact increased the suicide rate 8.2 times. If the person had visited a psychiatric emergency room they were 27.9 times more likely to kill themselves, and if they’d actually been admitted to a psychiatric hospital they were 44.3 times more likely to commit suicide. https://www.madinamerica.com/2014/09/suicides-rise-increasing-psychiatric-involvement/
A quick Google search of the phrase Suicide After Psychiatric Hospitalization brings up all kinds of pages showing the effects of “help” on so many people. I haven’t read all of them but they sure like to blame everything but the fact that the help is traumatizing and abusive and not helpful and pushing people over the edge that would not have gone there in the first place.
My problem that lead me to the helping rooms at the ER wasn’t being suicidal but anxiety made worse by all the “helpful” pills, it was more like fear of death that was overwhelming me, sometimes I got the $2 worth of Ativan that made it go away and went home other times the I got the psychiatric kidnapping after they called the anxiety “mania”.
In the end before I got off all those pills and got better I learned to stop at the liqueur store and gulp down enough drinks before going in so I appeared calm enough to not trigger any excessive “help”.
Never ever go to a place that has whats called CPEP
Report comment
” What ot did we have for this person at this moment? ”
One option is letting the person overwhelmed with distress have a cigarette if that is what they are complaining about. Anyone who has ever lived it or worked in these places knows the effects of enforcing the smoke free rules has on people. The get more and more agitated till staff pounces.
“But we can give you a nicotine patch…” Bla Bla Bla … Did you fail pharmacology class or are you just plan stupid ? Everyone knows you need that direct hit of nicotine you can only get from smoking for relief and that slow little trickle from those patches is completely useless.
Of all the genius that has ever come out of psychiatry forcing people in the middle of a crisis to quit smoking at the same time takes the cake.
Report comment
Stephen,
Great article and great choice of pictures.
The first picture with the bed (if it can be called that) was powerful for me, bringing back memories. I immediately thought that if Franz Kafka were writing today, he would locate some scenes from stories like the Metamorphosis or the Trial in a modern psychiatric hospital. The setting would fit in perfectly to his narrative of alienation, discouragement, senselessness, and the presence of callous, capricious authorities.
The second chart, mainly in what it omits, lays bare the failure that is the American mental health system. It’s stunning that so many potentially positive or mixed (good and bad) words are missing from the categories “affect” and “thought process”. Words like “curious”, “hopeful”, “determined”, “reflective”, “warm”, “engaging”, “planning”, have no place here. And for thought process, the only “positive” category is “clear” – as if a healthy person should be like an automaton or drone who feels very little strongly, and just functions mechanically in a socially-approved way.
Great pictures to describe a profession that has lost its soul.
Report comment
I wonder if this profession ever had a soul to lose in the first place.
Perhaps when the Quakers carried out their moral treatment of people where they fed them well, dressed them properly, and took people out for walks in nature, perhaps then the profession had a soul. But this didn’t last very long.
Report comment
The Quakers didn’t let doctors into their moral treatment homes. They suspected lack of soul in the doctors of the day, who were into treating all sorts of ailments with mercury salts.
Report comment
How wise the Quakers truly were! I suspect that their suspicion was totally correct. It certainly seems to be correct today.
Thank you for sharing this bit of information.
Report comment
I mentioned Moral Therapy in a forum for survivors of spiritual abuse. A nurse practitioner sneered at this, implying it was impossible to help brain diseased people with compassion.
She considered herself a humanitarian because she opposed “anti-psychiatry” churches. When I told her cruelty I had observed in pro-psychiatry churches she was truly baffled! She claimed they must not be educated enough about the scientific validity of psychiatry.
I would have to say the opposite, Nurse Patsy.
Report comment
Kafkaesque describes modern institutional psychiatry to a tee. I’ve seen it used in this context in many instances, and I couldn’t think of a descriptive term that was any more apt. Try, for instance, to plead for your own “sanity” with a psychiatrist, and he or she is likely to see “insanity” in it. People don’t wind up in “mental hospitals” because of their “sanity” runs the argument. People get out through their “insanity” though, otherwise, they are “in denial” and “lack insight”. Psychiatrists don’t diagnose “wellness”. So long as you see them, you can count on them affirming your “sickness”. You can also count on their panacea, a prescription drug. ‘Moving on’ is usually an individual decision. Psychiatry doesn’t often encourage it, especially for what are seen as the most “sever” conditions. As far as the doctor is concerned, it (“non-mental illness”) doesn’t pay the bills.
Report comment
The way you prove your sanity to a psychiatrist is to deliberately talk so wildly and irrationally that he describes you as malingering and has his aides show you the door.
Report comment
Love it – but sadly some are so stupid that even crying out the you’re seeing big white rabbits and a little girl in a blue dress running around the walls will get you seclusion and an injection.
Report comment
Some might say you have BPD causing your manipulative malingering. 🙂
Report comment
I started a thread in the forum titled “Photos from behind locked doors , help find more. https://www.madinamerica.com/forums/topic/photos-from-behind-locked-doors-help-find-more-please/ on March 4, 2014
Like they say a picture is 1000 words, if anyone has or can find any to add post them for using in articles and online writings.
Report comment
Most facilities don’t allow cell phones. The staff likes to isolate you from the outside world and they don’t want pictures taken, either. If people could see the inside of mental health facilities, and experience the same things patients experience, they’d be outraged. I hope more pictures are posted.
Report comment
I remember when my psychiatrist went to a diagnostic tool of circling smiley faces to enter how I was feeling that visit. There was no space whatsoever for why I was feeling that way. It’s was ludicrous then and it’s ludicrous now. Psychiatry doesn’t go with what is causing you to feel this way they just grab psychiatric terms for a diagnosis.
I have a sibling who is a psychologist and she keeps telling me I need to go to a new psychiatrist so he can deem me “psychologically well”. I have a false psychiatric diagnosis in my medical chart which has hindered me getting proper treatment in the ER and from primary care doctors in the past. Does it matter I’ve been off psychiatric drugs for over 10 years and haven’t seen a psychiatrist in that long either? My sibling and I both know the diagnosis is absurd but it’s still in my chart. So when I read your comment I had to start laughing because what psychiatrist would do that? “Oh yes, here is your certificate of mental competency for you to carry around in case you need it”.
Report comment
I know someone who had to go to a psychiatrist for a year to get her ridiculous;aous diagnosis removed but it worked. My problem is a) affording it, b) overcoming my stress at being in the same room as one, and c) fear of being unable to restrain myself in the face of their stupidity and venalit,y and getting a fresh diagnosis to go on with.
Report comment
I can definitely help you out on this one, “deeeo42”! Here’s 2 GREAT ones!
First, the long form:
“Iatrogenic Neuroleptic Psychotropic Pharmaceutical Cerebral Cognitive Impairment Malfunction”, or “INPPCCIM”…. Me, I prefer the short form:
IATROGENIC NEUROLEPSIS…. Iatrogenic Neurolepsis….
In plain English, it means too many Dr.’s have given ya too many drugs, that they shouldn’t have done!….
(I actually got the nurse to write “Iatrogenic Neurolepsis” in my medical record. The trick is to say it with authority, and conviction!) ~B./
Report comment
I have a drug induced psychiatric diagnosis that has seeped into too many of my medical records that primary care doctors could see. In 2002 I went to see a new primary care doctor who saw the diagnosis and I can’t even put into words how she treated me. I was a brand new patient coming because I’ve been in the hospital with pancreatitis. I do not want any reference to psychiatry and psychiatric drugs to come up when I have to see a medical specialist. My sibling only wanted me to not to be judged on incorrect information when I was in need of medical help. If only it was so simple to change psychiatric diagnoses in our medical charts.
Report comment
It’s strange that a diagnosis is trusted so readily by psychs. Misdiagnosis is a common thing, so I’m not sure why “professionals” are so willing to accept it.
Report comment
I refuse to go to any hospital where I have been admitted as a psychiatric patient, even in an emergency. One time I collapsed with an unknown condition and was taken to hospital by my sister who was amazed at how rude and dismissive the staff were. I realised that I had been there before, as a psych patient. I avoid doctors as much as I can now.
Report comment
I don’t understand how psychiatric diagnoses carry the weight they do to other physicians. I’ve learned so much from sites like this and wish it had been available to me many years ago.
Report comment
All diagnoses are misses if you consider it. That’s part of the problem.
Report comment
Your experience, Steve, like so many of those working at present within the system, if the “alternative” system, has been severely limited. You should have known “treatment” in this room that you call “the helping room”. If you had, you might not be singing a different tune, but you might not have your current employment. I see a system that favors those with the least “distressing” diagnostic labels the most, and if you want a more “distressing” label, all you have to do is resist. I’m glad, actually, that the “mental health” authorities were never able to turn me around. I did what I had to do to get out of that box, and then I’m done with them (and you). As for my lack of “distress”, or “insight”, at the current time, its our little secret.
Report comment
The photo remind me on some execution chamber.Same as there,
legal homocide,will go on.We have to admit,that Mental Health
system is deathrow,for crazy people.And this insane system will
go on forever,because I don’t see anyone capable,to challenge
their allmighty insanity!To learn this,you have to be crazy.
Report comment
Consider them an installation for the execution of the mind.
Report comment
Just adding to the 1st impressions of others — the first thing I thought of when I saw the photo was a lethal injection chamber. And I imagine at times it has been, except that we’re usually talking about a slower death in most cases. Which is a form of torture by most definitions.
Report comment
Thanks for writing this—which I will share.
Report comment
Yes, Steve, life is extremely stressful and people often do break down. We don’t have communities, people are out there on their own, and with no backup. Sometimes they just can’t take it.
But Steve, if we go along with the idea that the solution to problems is found in Therapy, Recovery, and Healing, then we are simply telling people that it is wrong to be angry and that they have to accept things the way they are, and that they can’t expect justice.
Would you Steve be willing to sign on to a message denouncing Therapy, Recovery, and Healing as the solutions to problems. People need community, but this has to be centered on political and legal activism, not just on talking people down or out of their anger, or on making them feel better.
Nomadic
Report comment
Hi Nomaidic
I know you were talking to Steve but here is my 2cents worth
I think one aspect of seeing recovery useful in whatever way you define useful does not always negates political and legal action of all types
I just heard about how compassion works better when fueled by hope rather than anger and or guilt
I think that view has value
For those of us who have been hurt sometimes multiple times by the helping system it ain’t easy but I think works better in the long run
Try everything and especially try to do what works best for you
Getting lawyers involved or legal advocates would help though at times I not sure about them in general
Just as long as they have heart and game like Jim
G
Onward!
Report comment
CatNight, but even the concept of Recovery means that the patient is not alright the way that they are.
If someone does you wrong, your innate impulse is going to be to strike back. That is how life is affirmed and perpetuated. But Psychiatry, Psychoanalysis, Psychotherapy, Recovery, and Healing are all designed to make that wrong, and instead make you see the problem as being within yourself.
So long as people go along with Recovery and the related ideas, nothing is ever going to change.
Do you agree?
Nomadic
Report comment
Here in Keene, N.H., “CMC/DHK” (Cheshire Medical Center / Dartmouth Hitchcock-Keene), had it’s 6-bed adolescent psych unit close last winter, due to the “sudden departure” of a psychiatrist. The continued operation of it’s 12-bed adult unit was also threatened. Sure enough, this summer (2016), the adult unit also closed, partly because of “lack of staff”. Funny thing IS – they’d just finished a year-long, $1.5Million renovation to their ED, specifically to install “psych rooms” just like the one pictured here! Recently, my friend was forced to wait a *WEEK* in one of these rooms there…. She was taken to the State loony bin, in handcuffs and shackles, in the back of the Sheriff’s cruiser. 3 days later, the State loony bin sent her home in a TAXI CAB…. WHO’S “crazy” here?……~B./
Report comment
I just remembered a name that is not mentioned much anymore but it would be interesting to hear his viewpoint of this type of treatment
Dr Robert Jay Liftin did a study of how doctors in the Nazi regime were able to use certain mental gymnastics to allow themselves to participate in the Holocaust
The Nazi Doctors is the title
My best guess is that this is what has happened to the main developers of recent contemporary psychiatry like Dr Robert Spitzer and others of his ilk
They are deaf and blind to the atrocities being commited in the name of mental health treatment in medical buildings,out patient centers,and prisons and nursing homes
It would be interesting to read his work and see if there are parallels
Report comment
Just thinking I used strong language
It is the afteraffects of the beginning part of my most recent treatment experience
It was bad
I am trying to acknowledge the trauma but still hold on to allowing for restorative justice and not fall into letting anger lead all the time
It doesn’t seem worth it in the long run but boy when those memories rise up yikes!
Report comment
I must have missed the strong language (unless it’s already been moderated). Sounds like you were simply making a comparison between past and present day atrocities.
Actually you are being kind by giving him/them the benefit of the doubt (i.e. “blind.”) But such blindness is hardly vindication; it is evidence that of being critically out of touch, hence irresponsible, unprofessional and/or incompetent.
Report comment
So powerful Steven, thank you!
Oryx
Report comment
I love this article and will share it! When I saw the photo, a familiar scene to me, I was not only brought back to it, but I thought of a gas chamber because the room seemed to be so isolating that for sure, it could be airtight.
I remember such rooms in the most prestigious facilities in the world. Massachusetts General Hospital’s psych ER, for one. Boston Medical Center had the worst psych ER in the city in my opinion, MGH not far behind. I have been held in many such rooms, even though I was not violent. Certainly, while confined I had no intentions of acting on suicidal notions at all, knowing that getting caught could lead to indefinite confinement.
Ninety-nine percent of the time, whenever I had a thought or desire to do suicide, it lasted 20 minutes. Such notions had resolved in my mind by the time I was even triaged. If I phoned my doctor, the thoughts were often gone by the time the doc called back. I remember taking myself to such places simply because I couldn’t get anyone to call me back!
Showing up was embarrassing! ! What was I doing there? Sometimes I was so guilt-ridden for even showing up that I told them I was suicidal anyway, just to avoid the demeaning “lecture” they’d give telling you you were wasting their time and taking up bed space. I guess they never realized that many people show up looking for caring and a listening ear, simply because they don’t know where else to go.
I do have advice for anyone who ends up in such a place. Ask to speak with clergy or your attorney if you have one. Not all facilities have clergy on duty, but many do. While their aim is to isolate you and torture you, they must make exception for clergy and attorneys.
Looking back over three decades of psych hospitalizations I recall that only rarely did I speak with clergy while inpatient but every time I did, they were immensely helpful. Their orientation was not that I was a person who needed fixing, but a human being like any other who had questions and wanted to hash something out.
One clergy, an older one on duty at around 2am, told me we both needed to face the facts. She knew, and I knew, that I was stuck there for the time being. Maybe they’d let me out in the morning but that decision depended on THEIR inner administrative needs, such as insurance, perceived liability, and the power plays between staff over which I had no control. I decided to take advantage of the time spent alone. The clergy person convinced the staff to let me have a pencil and pad of paper. To me, at that moment, I was empowered. Writing transcended everything. In my pen was power beyond those walls, beyond imprisonment, beyond their cruelty. It still is.
Report comment
Dear Steven
thank you for this. Here in Australia 4 point restraint with straps is very common except quite often it is on a trolley in the middle of the emergency department no curtains, 27 hours tied up or more, 27 hours was described as lucky by the complaints manager as “lots of people are restrained for longer than that” – no one even pretends it is a helping room! and there certainly is no love there. Actually I’m wrong an old lady with a broken hip lying on another trolley beckoned me over “is that your son love ? they have treated him worse than an animal.. he looks like a lovely boy and I’m really sorry for what they have done.” That moment of love from a person in pain who didn’t know me probably saved me that day but those paid to “care” showed only callous indifference.
Report comment
Similar experience – admitted for an overdose – suicidal impulse overcome by me but told I would be admitted to the psych ward voluntarily or not – ok, I said. An hour later nurse came and said there were no beds as there’d been a fire, and gave me a taxi voucher. LOL!
Report comment
“Callous indifference” = contempt. My old mum used to say “you’re born but not buried” in such circumstances. An invitation to empathy.
Report comment
Psychiatrists are Real Scientists. They aren’t paid to empathize, but to treat the “mentally ill.” Empathy requires seeing the other as a human being rather than a lab rat.
Report comment
Oh my god! Those notes make me vomit. These places dehumanise you like lab rats. Pathetic. And people call this HELP?
Don’t know why this article does not have millions of views and thousands of comments.
Report comment
It certainly helps. It HELPS keep the psych system intact and the high priests of moral medicine in power.
Report comment
Psychiatrists. Cleansing.
Report comment