
In the May 2018 issue of Current Psychiatry, there’s an editorial by Henry Nasrallah, MD. Dr. Nasrallah is a highly renowned psychiatrist, and is editor in chief of the journal. He is also chair of the St. Louis University Department of Psychiatry.
Here’s the opening paragraph of the article.
“As the end of the academic year approaches, I always think of one last message to send to the freshly minted psychiatrists who will complete their 4 years of post-MD training. This year, I thought of emphasizing the principles of psychiatric practice, which the graduates will deliver for the next 4 to 5 decades of their professional lives. Those essential principles are coded in the DNA of psychiatric practice, just as the construction of all organs in the human body is coded within the DNA of the 22,000 genes that comprise our 23 chromosomes.”
So, Dr. Nasrallah wants to set down the “principles of psychiatric practice” by way of encouragement to “freshly minted” psychiatrists. It is not unusual for the more senior members of a profession to pass on what they perceive to be important precepts to the newcomers, but the DNA metaphor strikes me as bordering on bizarre. We can’t change our DNA, and there is, I think, in Dr. Nasrallah’s metaphor a suggestion that the newcomers can’t (or perhaps must not) change the principles on which current psychiatric practice is based. In addition, the term “freshly minted” strikes me as slightly insulting, as if they were coins being stamped out of a mint: each identical to the next. But I’m sure that Dr. Nasrallah knows more about newly-qualified psychiatrists than I do, so perhaps he’s right. Perhaps the culture and direction of psychiatry schools is geared to the production of drug-prescribing automatons programmed to ignore obvious facts and realities of human life, and to see instead clusters of “symptoms” that need to be “treated” with neurotoxic drugs and high-voltage electric shocks.
In the next paragraph, Dr. Nasrallah repeats the DNA metaphor:
“So here are the principles of psychiatry that I propose govern the relationship of psychiatrists with their patients, encrypted within the DNA of our esteemed medical specialty:”
One of the meanings of “encrypted” is difficult to discern, and as the principles in question are highly flattering to psychiatry and psychiatrists, readers might find the term more apt than Dr. Nasrallah has intended.
Also note the phrase “esteemed medical specialty,” which inevitably raises the question: esteemed by whom? In reality, psychiatry, as the illustrious Jeffrey Lieberman, MD, pointed out in 2015, is the only medical specialty that has its very own anti-group. It is also noteworthy that the size and impact of this anti- group is growing exponentially, as the nature and scope of the psychiatric hoax is being increasingly exposed.
Dr. Nasrallah provides a list of twenty-seven principles. Most of them are tawdry, self-serving platitudes which most critics of psychiatry will find unworthy of credit. Here are some examples:
. . . . . . . . . . . . . . . .
“Provide total dedication to helping psychiatric patients recover from their illness and regain their wellness.”
. . . . . . . . . . . . . . . .
“Maintain total and unimpeachable confidentiality.”
. . . . . . . . . . . . . . . .
“Demonstrate unconditional acceptance and respect to every patient.”
This might be a little challenging for a profession that routinely conceptualizes its clients’ statements as symptoms, and where ultimately all interactions are conducted under the threat of involuntary commitment.
. . . . . . . . . . . . . . . .
“Adopt a nonjudgmental stance toward all patients.”
Unless, of course, the “patient” decides to stop taking the pills.
. . . . . . . . . . . . . . . .
“Provide evidence-based treatments first, and if no response, use unapproved treatments judiciously, but above all, do no harm.”
The contradiction here is glaring. All psychiatric “treatments” do harm. Electric shocks cause memory loss. Benzodiazepines and SSRI’s are addictive. There is abundant prima facie evidence that the SSRI’s are implicated in the murder-suicides, but psychiatry refuses to conduct a definitive study of the matter. And, of course, the permanent and disfiguring harm done by neuroleptics has been known for decades. In real medicine, the injunction to do no harm has genuine significance. In psychiatry, it’s an empty slogan. Whatever marginal benefits the drugs and shocks might confer in the short term are almost always eclipsed by the long-term harm, which in many cases is truly devastating.
. . . . . . . . . . . . . . . .
“Establish a strong therapeutic alliance as early as possible. It is the center of the doctor–patient relationship.”
. . . . . . . . . . . . . . . .
“Educate patients, and their families, about the illness, and discuss the benefits and risks of various treatments.”
In other words, tell them the falsehood that they have an illness, even though there is no evidence to support such a contention. And “…discuss the benefits and risks of various treatments.” And remember, these principles aren’t just exhortations to psychiatry’s newcomers; rather, they are, according to Dr. Nasrallah, the principles that underpin and drive current psychiatric practice; the principles that are coded in the DNA of psychiatric practice today! Well I have to say that in my experience, the great majority of psychiatrists routinely overstate the benefits of the drugs and shocks, and understate the risks. In fact, I have even encountered psychiatrists who cautioned against informing clients of the risks of tardive dyskinesia and akathisia with neuroleptic drugs, on the grounds that nobody would agree to take them if they received this information! And in this regard, it is noteworthy that on May 12, 2017, Columbia’s Psychiatry Department, under the leadership of the renowned and scholarly Dr. Lieberman, issued the following statement in a press release titled Benefits of Antipsychotics Outweigh Risks, Find Experts:
“An international group of experts has concluded that, for patients with schizophrenia and related psychotic disorders, antipsychotic medications do not have negative long-term effects on patients’ outcomes or the brain. In addition, the benefits of these medications are much greater than their potential side effects.” [Emphasis added]
The press release — including this blatant falsehood — was picked up by the media and printed by various news outlets, including UPI, Science Daily, and Medical News Today, all of which repeated the Columbia assertions more or less uncritically. Perhaps Columbia’s psychiatry department hasn’t got the genuine psychiatry DNA!
. . . . . . . . . . . . . . . .
“Do not practice ‘naked psychopharmacology.’ Psychotherapy must always be provided side-by-side with medications.”
Whilst I am sure there are some psychiatrists who offer talk therapy to their clients, I believe their numbers are very small indeed. It is certainly not one of the “essential principles” of current psychiatric practice, as Dr. Nasrallah contends. And if readers are wondering why this is the case, Gardiner Harris’s New York Times article “Talk Doesn’t Pay, So Psychiatry Turns Instead to Drug Therapy” (March 2011) provides some insights. And even the most venerable Dr. Lieberman acknowledges this reality in his article “Change, Challenge and Opportunity: Psychiatry in the Age of Reform and Enlightenment” (2013). Here’s what he wrote:
“In the past few decades, the focus has shifted more toward the brain and away from the mind. And changes in reimbursement systems today have rewarded hurriedly written prescriptions and encouraged psychotherapy to be provided by nonpsychiatrist therapists. Paperwork, insurance procedures, and government regulation have stretched physicians’ tolerance and limited the opportunities for meaningful interaction with patients.” [Emphasis added]
Note how the admission of “hurriedly written prescriptions” is effectively nullified by shifting the blame to “changes in reimbursement systems,” and “Paperwork, insurance procedures, and government regulation.” Psychiatrists would love to have more meaningful interactions with their customers, but they just can’t, because — well it cuts into the bottom line! Poor lambs. Oh to be torn between greed and duty.
Douglas Mossman, MD, a psychiatrist at the University of Cincinnati, wrote Successfully navigating the 15-minute ‘med check’ (2010). Here’s a quote:
“Even psychiatrists who deplore 15-minute med checks recognize that they have become standard care in psychiatry.”
And in 2017, Mark Moran, a senior reporter at the APA, wrote a piece for Psychiatric News in which he stated:
“The 15-minute medication management visit has become one of the standards of psychiatric practice.”
In the article, Mr. Moran quotes extensively from William Torrey, MD, a psychiatrist who laments the fact that the 15-minute med check has become the norm in psychiatric practice. But in reality, psychiatrists who are dissatisfied with this state of affairs have no one to blame but themselves. They vigorously promoted the deception that all significant problems of thinking, feeling, and/or behaving are illnesses which need to be corrected by drugs and electric shocks; they established themselves as the experts in the diagnosing of these fictitious illnesses and in the prescribing of the drugs and shocks; and they streamlined the process to maximize their earnings.
Is Dr. Nasrallah seriously contending that the provision of psychotherapy side-by-side with “medications” is standard practice in psychiatry today?
. . . . . . . . . . . . . . . .
“Support the patient’s family. Their burden often is very heavy.”
In some cases, this might be reasonable enough, but there is no recognition that the burden that family members sometimes impose on the client can be equally heavy.
. . . . . . . . . . . . . . . .
“Emphasize adherence as a key patient responsibility, and address it at every visit.”
And, of course, adherence means take your pills and electric shocks as the doctor ordered.
Although in this context of providing encouragement to “freshly minted” psychiatrists, Dr. Nasrallah is stressing the need for adherence, and, by implication, the value of the “treatments,” he was less enthusiastic about the drugs in an earlier article “The Dawn of Precision Psychiatry,” (December 2017). Here are some quotes:
“So, while clinicians go on with the mundane trial-and-error approach of contemporary psychopharmacology, psychiatric neuroscientists are diligently deconstructing major psychiatric disorders into specific biotypes with unique biosignatures that will one day guide accurate and prompt clinical management.” [Emphases added]
“Precision psychiatry will ultimately enable practitioners to recognize various psychotic diseases that are more specific than the current DSM psychosis categories. Further, precision psychiatry will provide guidance as to which member within a class of so-called ‘metoo’ drugs is the optimal match for each patient. This will stand in stark contrast to the chaotic hit-or-miss approach.” [Emphases added]
So, current psychiatric practice is a chaotic, hit-or-miss approach. Nevertheless, Dr. Nasrallah stresses the need for adherence on the part of the customer to the drugs prescribed through this hit-or-miss approach.
“Precision psychiatry also will reveal the absurdity of current FDA clinical trials design for drug development.” [Emphasis added]
“Precision psychiatry will completely disrupt the current antiquated clinical paradigm, transforming psychiatry into the clinical neuroscience it is.” [Emphasis added]
So, back in December of last year, when Dr. Nasrallah was promoting his fanciful vision for the future of psychiatry, he was extremely critical of the “current antiquated clinical paradigm,” but when welcoming “freshly minted” psychiatrists into the fold and encouraging them to embrace the essential principles of current practice, no intimation was given that the current principles are hit-or-miss, antiquated, and chaotic. I wonder if Dr. Nasrallah informs his customers that current psychiatry is hit-or-miss, antiquated, and chaotic. I wonder if, when he is emphasizing adherence (at every visit, remember?), he informs his customers that the prescriptions, to which they are being enjoined so vigorously to adhere, stem from a system that is hit-or-miss, antiquated, and chaotic.
. . . . . . . . . . . . . . . .
“Uphold the medical tenet that all ‘mental’ disorders of thought, mood, affect, behavior, and cognition are generated by disruptions of brain structure and/or function, whether molecular, cellular, or connectomic, caused by various combinations of genetic and/or environmental etiologies.”
This is unadorned bio-bio-bio psychiatry. All “disorders” of thinking, feeling, and behavior are caused by disruptions of brain structure or brain function! And don’t be misled by the word “environmental.” All that Dr. Nasrallah is conceding here is that some of the putative disruptions of brain structure/function may be due to environmental factors. This is a far, far cry from the reality that the great majority of thinking, feeling and behavior problems that psychiatry considers symptoms are in fact not the result of neurological “disruptions,” but rather are reasonable and understandable responses to current and historical losses, adverse experiences, and adverse circumstances (including, incidentally, the adverse circumstance of becoming enmeshed in the psychiatric system). It also needs to be pointed out that, apart from those problems described as due to a general medical condition or the effects of a substance, none of psychiatry’s so-called mental disorders has been consistently and causally linked to any defined disruption of brain structure or function.
And note the word “tenet,” which my New World Dictionary renders as: a principle, doctrine, or belief held as a truth, as by some group — synonym: doctrine. The critical point being that a tenet is a principle that is held to be true without evidence.
What Dr. Nasrallah is effectively conceding here is that the bio-bio-bio brain illness perspective
- Is the philosophy underpinning psychiatry (encrypted in its DNA, no less!)
- Is unproven (it’s a tenet, remember?)
- Is to be foisted on the “freshly minted” psychiatrists who will be entering the work-force this year (“Uphold the medical tenet…!”)
. . . . . . . . . . . . . . . .
“Learn and use clinical rating scales to quantify symptom severity and adverse effects at baseline and at each visit. Measuring the severity of psychosis, depression, or anxiety in psychiatry is like measuring fasting glucose, triglycerides, or blood pressure in internal medicine.”
Psychiatric rating scales are always subjective. Measurements of glucose, triglycerides, and blood pressure, by contrast, are objective. Pretending that these very different kinds of assessments are comparable is just one more facet of the psychiatric hoax. Blood glucose measures are an essential part of diagnosing and managing diabetes. So the assertion that a scale for assessing depression (say) is “like” a glucose test is essentially equivalent to the long-touted but false assertion that depression is an illness, just like diabetes, for which one must take pills, often for life. The purpose of psychiatric rating scales is to convey the impression that some kind of scientifically valid assessment is being conducted before, during, and after “treatment.” But this impression is false. In reality there is no definition of any psychiatric “disorder” that would meet scientific standards. The fundamental assumption of psychiatry, that all significant problems of thinking, feeling, and/or behaving are brain illnesses, is simply false. Depression, for instance, far from being a neurological disorder, is the normal, adaptive human response to loss or adverse circumstances. Its evolutionary purpose is to alert us to the need to make some changes in our lives or circumstances.
. . . . . . . . . . . . . . . .
“Advocate tirelessly for psychiatric patients to increase their access to care, and fight the unfair and hurtful stigma vigorously until it is completely erased. A psychiatric disorder should have no more stigma than a broken leg or peptic ulcer, and insurance parity must be identical as well.”
Note: “increase their access to care,” the inevitable corollary of which is: more business for psychiatry. Bring us your huddled masses, and we will sell them drugs to fix their brains, even though their brains aren’t broken. If they stay on the drugs and shocks long enough, however, their brains will be broken.
Also note: “fight the unfair and hurtful stigma,” when in fact psychiatry’s groundless and unproven illness tenet is the major source of stigma for those hapless individuals who get caught within its web (Angermeyer et al, 2011; Deacon, BJ, 2013; Read, J, et al, 2006).
. . . . . . . . . . . . . . . .
“Recognize that every treatment you use as the current standard of care was at one time a research project. Know that the research of today is the treatment of tomorrow. So support the creation of new medical knowledge by referring patients to FDA clinical trials or to National Institutes of Health–funded biologic investigations.”
This reminds me of something that Carl Elliott, Bioethics Professor, University of Minnesota, wrote for Mother Jones back in 2010:
“Research subjects are the most highly prized commodities in the clinical trials industry. Four out of five clinical trials are delayed because of difficulties recruiting subjects. These delays can be costly, as the patent clock on new drugs starts ticking as soon as the patent is filed.”
So, when Dr. Nasrallah encourages “freshly minted” psychiatrists to refer “patients” to clinical trials, whose interests are being served?
It is also noteworthy that the only kinds of research included in this principle are drug trials and biological investigations. There’s no mention of research into psychotherapy which Dr. Nasrallah had earlier contended “… must always be provided side-by-side with medications.”
. . . . . . . . . . . . . . . .
Dr. Nasrallah concludes his editorial with this:
“You, the readers of Current Psychiatry, include thousands of experienced psychiatrists with years of practice in the real world. I invite you to add to this list of principles by writing to me at [email protected]. Join me in providing the freshly minted psychiatrists words of wisdom about the DNA of psychiatry to guide them before they embark on their careers as psychiatric physicians.”
In other words, keep them within the pseudo-medical world of bio, bio, bio psychiatry. Make sure that they don’t fall prey to the pernicious influences of anti-psychiatry. Guide them in the path of psychiatric orthodoxy. Chain them to the hoax. Get them young and they’re yours for life.
BUT
There’s one principle of psychiatry that Dr. Nasrallah has omitted, if, that is, we are to consider his own career to be exemplary of psychiatric practice:
Cultivate mutually beneficial relationships with pharmaceutical companies.
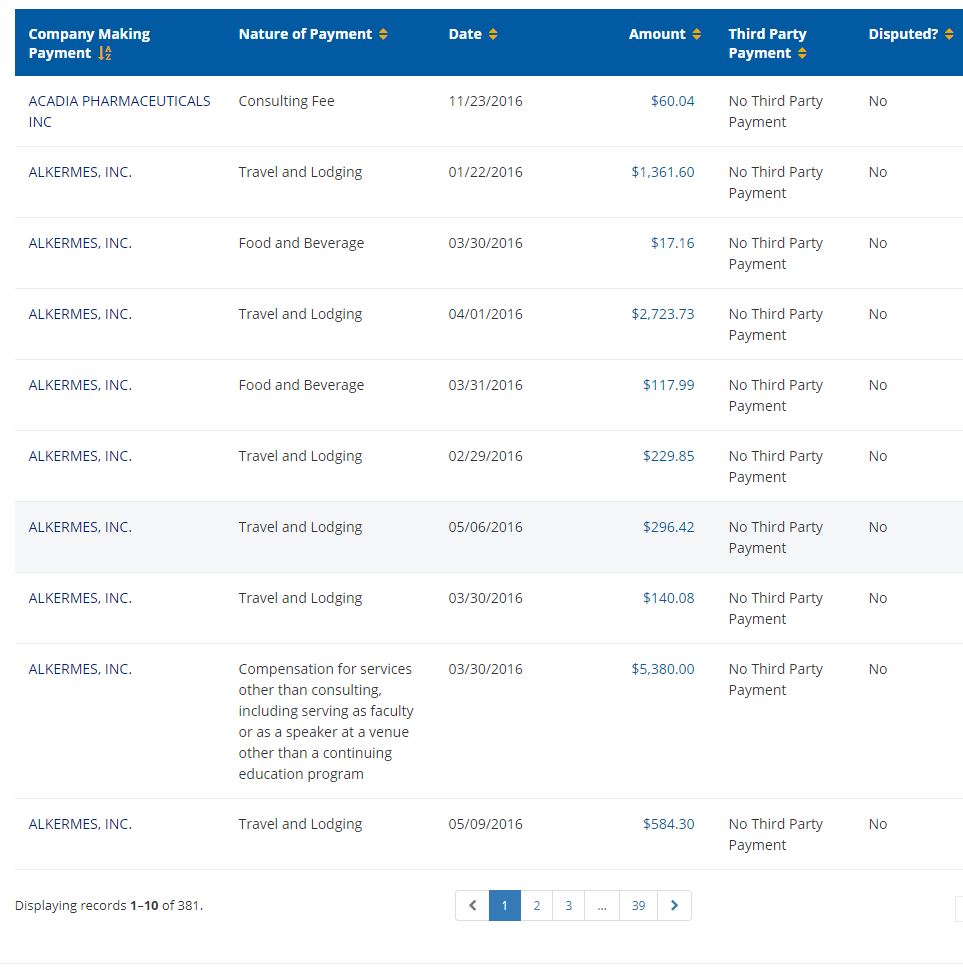
According to the site OpenPaymentsData, Dr. Nasrallah’s payments from pharmaceutical companies for the years 2013-2016 (most recent years for which data is available) were:
2016: $332,412.77;
2015: $304,252.38;
2014: $218,527.61;
2013: $114,368.32
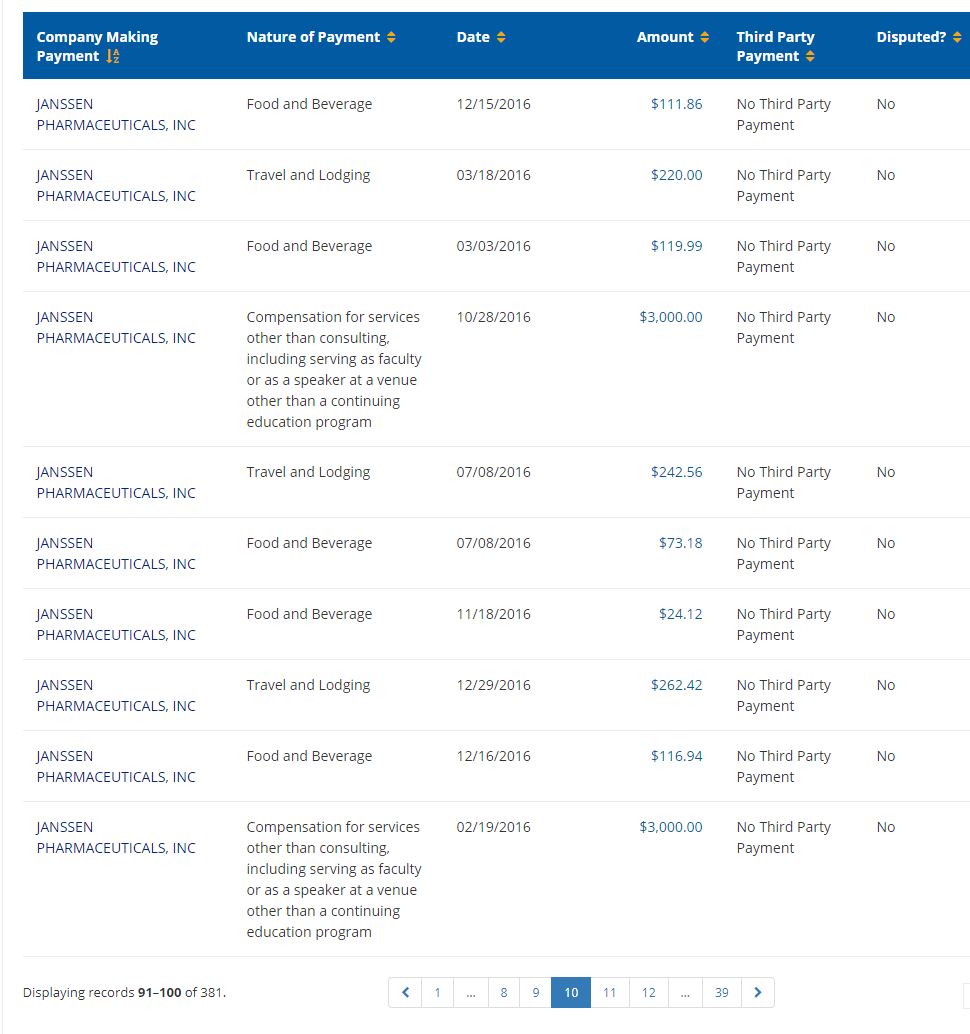
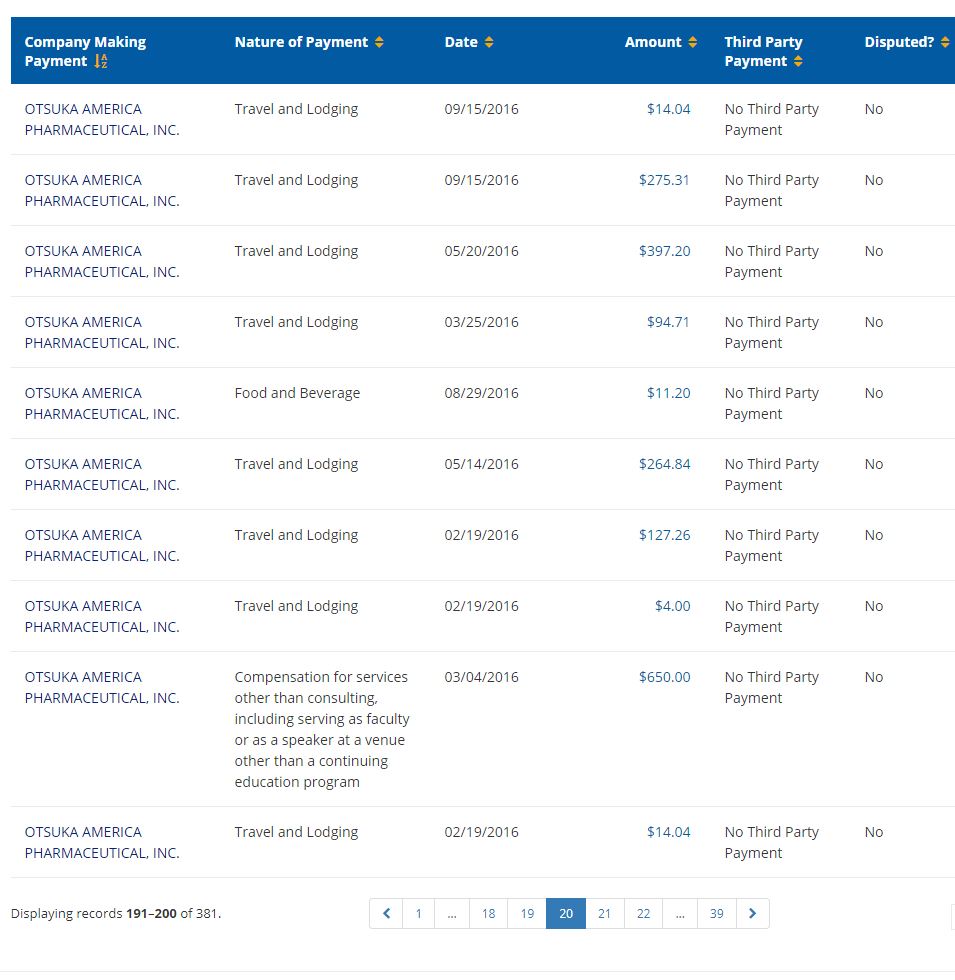
The CMS site above also breaks down the information by individual payments. Dr. Nasrallah’s receipts for 2016 ran to 39 pages!
Here is page 1:
Here is page 10:
Here is page 20:
And here is page 39:
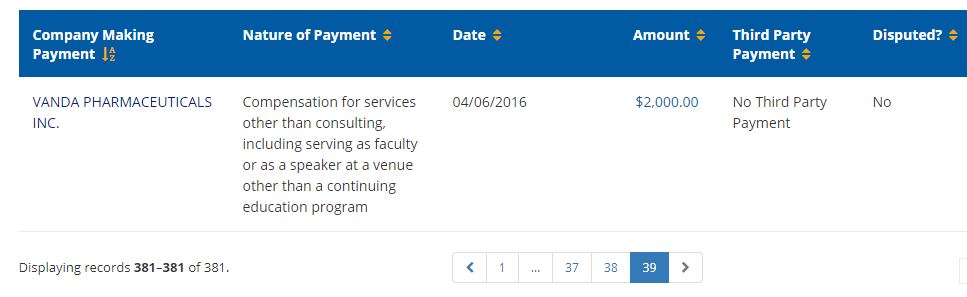
For a 2016 grand total of $332,412.77. Not bad for a practitioner of psychiatry’s chaotic, antiquated, hit-or-miss approach!
COMMENT
At the present time, psychiatry is under intense scrutiny and criticism. On all sides its “mental illnesses” and “brain-correcting” drugs are being exposed as dangerous, disempowering, and stigmatizing hoaxes. And psychiatry’s only response is denial, PR, cheerleading, and attempted marginalization of its critics.
In this article, Dr. Nasrallah is squarely in the cheerleading camp. The picture he paints of psychiatry is unrecognizably rosy. There is no acknowledgement of the fake illnesses, the dismal Kappa scores, the link between antidepressants and the murder-suicides, the adverse effects of high-voltage electric shocks to the brain, etc., etc.
According to Dr. Nasrallah, psychiatry is in fine shape. And, I suppose, from his perspective, perhaps it is.













The reality is that none of us can sleep before visiting the psychiatrist for fear of what this misinformed pseudo-medic will “do” next.
Psychiatry is not ok. In the UK it’s time the authorities looked at the misinformation campaign around the SMC and the RCPsych and ask whether people should be held accountable for falsehoods.
Report comment
ConcernedCarer,
Psychiatry is definitely not OK. It is something fundamentally flawed and rotten. But they get away with what they do because the general public can’t believe that a “legitimate” medical specialty could possibly be this destructive.
Report comment
Wonderful. Shrinkology hasn’t been around for 200 years, and already it is encoded into the DNA of shrinks.
I have to pause long and hard over the eugenic (or nugenic) aspects of Dr. Nasrallah’s defense of the bio-shrinkology orthodoxy.
The corollary to his genetically endowed shrinks are his genetically deficient patients, and the only thing to be done is drug, drug, drug.
That, or if you can see past the drug haze, to figure out that you have been, what shall we say, “punked” by shrinkology.
This brilliant future knowledge has been leading these dummies around blindly for more than a century, but what of it? As in this piece by Dr. Nasrallah, the idea is still very useful when it comes to crafting shrinkology propaganda.
The moral is…more shrinks, more patients, more drugs, less sense. People could either wise up, or, as ‘ignorance is bliss’, settle into a extended hybernative state with which to avoid facing the increasing global warming crisis.
You say the world is getting hotter. It must be entirely due to a conspiracy of mental patients I’m sure. The answer, of course, must be to pump more and more money into shrinkology.
That way they will learn, won’t they?
Report comment
Frank,
Nice! The genetically perfect psychiatrists “treating” the genetically flawed “patients”. What next?
Report comment
Another excellent post.
“antipsychotic medications do not have negative long-term effects on patients’ outcomes or the brain. In addition, the benefits of these medications are much greater than their potential side effects.” [Emphasis added]”
The Dr should be made to take Olanzapine, it will soon cure the delusions.
Report comment
So apparently, for him, tardive dyskinesia is not a negative long-term outcome, and the death as a side effect is not greater than the “positive effects” of antipsychotics. He sounds VERY rational…
Report comment
Tardive dyskinesia and death are minor side effects when you consider that his yacht won’t pay its own bills…Oh. You’re referring to the patients and not the psychiatrist himself.
Report comment
Rachel777,
Nice!
Report comment
You don’t understand how annoying these people can be, which must be considered before complaining about minutiae such as “tardive dyskinesia.”
Report comment
Oldhead,
Yes. They are annoying. They won’t take their pills as ordered by THE DOCTOR. The fact that they know intuitively that the pills are destroying them is irrelevant. What a farce!
Report comment
It’s especially annoying when they fail to show respect and gratitude for being locked up, drugged and maybe shocked. Pretty insane behavior.
Report comment
Steve,
Dr. Lieberman has also, on another occasion, described us anti-psychiatry activists as “rabid ideologues” (https://www.medscape.com/viewarticle/879623). Rationality is not his strong suit.
Report comment
Oh that we were! Actually I’d like to see more fervently rabid anti-psychiatry activists, with an ideology (or principles/demands) that can unite the disparate elements among us. Anyone, please help. 🙂
Report comment
Dr. Lieberman’s army of anti-psychiatry idealogues is about as real as Emmanuel Goldstein and the Brotherhood in 1984. (Or the chemical imbalance.) He dreamed them up to scare people. At Bipolar Burble, the blogger is terrified of hordes of anti-psychiatry armies out to destroy her. She scheduled a 2 Minute Hate in some of her posts. “I love Big Doctor!” All perfectly rational of course. Mindlessly accepting whatever someone says and being afraid to think are signs of good insight and lead to meds compliance. 😀
B.B. is scared to read a word of anything Bob W. or others write. She might catch a bad case of the thought disease called anosognosia. “Mentally ill” folks don’t have paradigm shifts or Aha moments. Just a lot of scary symptoms.
Cult members also behave this way.
Report comment
That’s a really good point. They should be required to take ALL of the wildly popular, hugely profitable drugs they prescribe. Particularly those approved with two 6-8 week clinical trials or the ‘breakthrough therapy’ tagged innovations that sprint through the approval process in as little as 4 months.
Report comment
astrong,
It would be interesting if someone could conduct a study to see how many psychiatrists or their children/spouses take these pills.
Report comment
Maybe if the doctor took olanzapine himself, it would add the weight to his arguments that it would add to his physique. What do you think, streetphotobeing?
Report comment
OMG – add weight to his argument! You cracked me up!
Report comment
Well he will look like Mr Blobby:
https://www.youtube.com/watch?v=4KzoiRX0gOg
Report comment
Mr. Blobby looks like a character from a dream I had when I decided to go off my psych drugs. (Hadn’t tapered too much. But my agonized decision inspired this dream.)
I was at a long table with friends and family. Then somehow I escaped something holding me back.
I divided into two. One–the Real Me–looked at the other. I was thinner, had a healthy complexion, and could think and feel like a real person.
I looked back at the other. She was a bloated doll with grotesque, knobby features. Green, the color of poison or vomit. Occasionally foul-smelling toxic gasses leaked out of her. She WAS an inflatable doll.
The friends and family ignored me. They continued to treat the Doll like the real human being. Occasionally they seemed to hear my voice when I called to them. They would just scowl and turn back to the Doll.
They didn’t like her. But they hated me. So they chose the Doll despite her poisonous nature. 🙁
Report comment
bcharris,
Nice!
Report comment
Thanks for another great post about the fraud of psychiatry, Philip.
This is blatantly untrue, “antipsychotic medications do not have negative long-term effects on patients’ outcomes or the brain.”
http://www.mindfreedom.org/kb/psychiatric-drugs/antipsychotics/neuroleptic-brain-damage
And the antipsychotics create “psychosis,” one of the positive symptoms of “schizophrenia,” via anticholinergic toxidrome; as well as creating the negative symptoms of “schizophrenia,” via neuroleptic induced deficit syndrome, in the short term, too.
https://en.wikipedia.org/wiki/Toxidrome
https://en.wikipedia.org/wiki/Neuroleptic-induced_deficit_syndrome
In other words, the “schizophrenia” treatments create both the positive and negative symptoms of “schizophrenia.”
Report comment
Someone Else,
Yes. And a lot more besides.
Report comment
Streetphotobeing,
Yes. Unless he’s a hopeless case!
Report comment
Dr. N has some pretty new lipstick. Coral didn’t go with the pig’s complexion; maybe candy pink will.
As far as the first principle goes, shrinks and everyone else at your mental illness center are 100% opposed to recovery since it’s bad for business.
By recovery I mean a productive, independent, satisfying life. Psychiatric “cures” guarantee none of the above!
Report comment
Rachel777,
I’m long retired. But I well remember the time when psychiatrists argued vehemently against “schizophrenics” finding any kind of productive, independent life, on the grounds that they couldn’t cope with the stress. A self-fulfilling prophecy; especially when the hapless individuals were loaded with neuroleptics.
Report comment
I have given up on those myself. Went off my drugs, but am in constant–almost crippling pain. Nonstop muscle cramps from head to toe, horrible itching and dryness, extreme sensitivity to certain noises, and exhaustion from the cramps.
Clear headed for the most part. I think I extended my life by a few years. (No longer in danger of diabetes. My heart is better. I’m losing weight which I couldn’t before.) Not that good a life though. Still can’t work and am lonely as nobody’s business. 🙁
Report comment
Best.
Nice work Philip. I myself have tried to write on this topic a few times but was not able to do so. You too alright good article.
This topic can get sidetracked. That’s fine oh b yes but dwelling can be horrific. b
b I say to me Pat get in tune to straight and arrow.
There awesome. The best. There’s not much more to say.
Report comment
PatH_America,
Thanks for the encouragement.
Report comment
“At the present time, psychiatry is under intense scrutiny and criticism. On all sides its ‘mental illnesses’ and ‘brain-correcting’ drugs are being exposed as dangerous, disempowering, and stigmatizing hoaxes. And psychiatry’s only response is denial, PR, cheerleading, and attempted marginalization of its critics.”
No one says it quite as clearly and succinctly as Dr. Hickey. Excellent article.
Report comment
Slaying_the-Dragon_of_Psychiatry,
Thanks.
Report comment
Oh, I don’t know. I still kinda’ think it’s an insult to perfectly good dragons, to compare them to the pseudoscience of psychiatry.
Maybe it should be the “Geico Gecko of Psychiatry”?
Crippled Lizard? Whatever….
LOL 😉
Report comment
Psychiatry is a theology in medical disguise. And psyche roots are pagan, Greek, imaginal, not scientific, but imaginal, poetic, which means – polytheistic. This is a death camp for psychic reality ruled by church/theology, medicine and science and they have one master – pseudo rational apollonian ego and economy = DSM power.
Yes, psychiatric language is only an empty dehumanising nominalism, for biurocratic machine to work for authoritarian sect, they all prey on the buried by theology/pseudo rationalism invisible body of human psyche, SEEN TODAY AS EVIL OR PSEUDO BRAIN DAMAGE.. You could use diagnosis only with proper understanding of human psyche, as a psychological map, not as a theological pseudo scientific condemnation in medical disguise. But without phenomenology and proper great meaning given to HUMAN psyche, we have only authoritarian BS with scientific pretensions in pseudo humanistics system RULLED BY MONEY.
Manufacture of madness, and Re- Visioning psychology are the ONLY BOOKS WHICH DESCRIBE the reality behind word STATE, mental illness, psyche. Without this knowledge and phenomenology in place of DSM, ther will be no human reality, only authoritarian fictions for money. Psychiatry created AUTHORITARIAN reality,not human reality.. . And psyche does not exists because there’s no language describing it, THE HAVE BURIED pro psychological language and the phenomenology of the psyche. The victims of psychiatry are victims of primitive psychopatic language and psychiatry knows that the language is everything. Medicine, theology and science destroyed psyche, and that’s why church has got Vatican, and psyche a death camp.
Psyche/ psychological man don’t need DSM judgements or cure but the pro psychological BLACK PANTHER’S PARTY AND FREEDOM FROM AUTHORITARIAN FAKE REALITY CREATED ONLY FOR BIUROCRATIC MACHINERY and church. AND NOT FOR PSYCHOLOGICAL MAN.
Church talks a lot about antichrist and numbers and nothing about PSYCHIATRIC DEHUMANISATION. It is not strange? Maybe the antichrist system will be a punishment for church/world/science silence?
Report comment
Danzig666,
Thanks for coming in. Certainly the dogmatism and the spurious nature of the “diagnoses” are dehumanizing, destructive, and disempowering.
Report comment
The Greek philosophers knew more about the human psyche than those quacks who deny souls exist. I would rather talk to a philosopher than a shrink myself.
Report comment
Check out ALLCAPA.com. I joined the group CAPA. Christians Against Psychiatric Abuse. The guy running that site believes pharmapsychiatry is destroying western civilization. I do too.
It’s not that hard to find evidence against the chemical imbalance myth. Just look at stuff the APA puts out.
Most people have no vested interest in doing research. That’s the only reason I can think of for why everyone still believes it.
Report comment
Are Dr. Nasrallah’s ears burning? 20 minutes ago I read his forward to a book penned by a long term patient of his. But then again, from the statements displayed in this article, we know Nasrallah is incredibly busy.
I have Tardive Dyskinesia. Dr. Nasrallah’s name comes up quite a bit in these circles.
I often wonder what my life would have been like if I’d never gotten enmeshed in ‘the system.’
Report comment
astrong,
Sorry to learn of your tardive dyskinesia. Interestingly, virtually every member of the general public with whom I’ve discussed this has expressed the belief that the tardive dyskinesia and the akathisia are “symptoms of the illness”. When I explain that they’re adverse effects of the drugs, the response is invariably one of utter disbelief. But psychiatry has done nothing to dispel this misperception.
Report comment
Dear Philip,
It’s still happening.
https://www.mirror.co.uk/news/uk-news/breaking-least-450-patients-lives-12749435
“..In fact, I have even encountered psychiatrists who cautioned against informing clients of the risks of tardive dyskinesia and akathisia with neuroleptic drugs, on the grounds that nobody would agree to take them if they received this information! ..”
https://www.madinamerica.com/2016/11/neuroleptic-drugs-akathisia-suicide-violence/
https://www.madinamerica.com/wp-content/uploads/2016/11/Suicide-Associated-with-Akathisia-and-Depot-Fluphenzaine-Treatment-KShear-1983.pdf
I notice Depot Fluphenazine Decoanate is now being discontinued.
http://www.medicinesresources.nhs.uk/en/Medicines-Awareness/Press-and-Media/Press-and-media/Discontinuation-of-Modecate-fluphenazine-decanoate-injection-all-strengths-by-end-of-2018/
http://www.hps.com.au/knowledge-centre/drugalert/discontinuation-of-modecate-ampoules/
https://www.drugshortagescanada.ca/discontinuance/42850
Report comment
DR SHIPMAN
https://www.telegraph.co.uk/news/2018/06/21/hampshire-police-hand-investigation-gosport-hospital-deaths/
THE UK GENERAL MEDICAL COUNCIL
Why didn’t the GMC fully investigate these deaths and take stricter action? Because this would be the Tip of the Iceberg of Medical Deaths in the Community.
FLUPHENAZINE DEATHS
Fluphenazine Depot Injection is accepted to cause Akathisia, which is accepted to cause Suicide. I can prove in my own case that my medical providers in Ireland suppressed my Adverse Drug Reactions to these drugs, placing me at future risk:-
https://www.madinamerica.com/2018/05/antidepressant-withdrawal-can-trap-people/#comment-131809
About 40% of Fluphenazine consumers attempt Suicide, at least 10% successfully.
Report comment
Fiachra,
Yes. Some things don’t change.
Report comment
Thank You Philip.
Report comment
So has society lost its ability to recognize false logic, or are people too intimidated to reveal their inner suspicions when they pick up on any of the disingenuous contradictions permeating such thoroughly mediocre propaganda? That’s what someone should be getting some research funds to investigate. In a “sane” world the dissemination of this sort of pablum would be roundly mocked and the author discredited.
Good to hear from you Phil.
Report comment
Oldhead,
“So has society lost its ability to recognize false logic, or are people too intimidated to reveal their inner suspicions when they pick up on any of the disingenuous contradictions permeating such thoroughly mediocre propaganda?”
That’s a great question. How can they continue to get away with this drivel? My hope (belief?) is that as more and more people join the ranks of anti-psychiatry, we’ll reach a sort of critical mass that will be hard for psychiatrists to ignore.
Of course, they’re already positioning themselves for this. Remember the great psychiatrist Ronald Pies, MD, asserting that psychiatry never really promoted the chemical imbalance theory! And currently Allen Frances is busy pushing the fairy tale that it was not psychiatry that was doing all the damage, but rather the mean ol’ GPs, and of course, pharma.
Report comment
Looks like we’re communicating in real time here.
These disclaimers signal that the most “in touch” shrinks sense a disaster, sort of like the frantic premonitions of rats that the ship is about to sink. Soon they’ll be pointing fingers and blaming each other, Pharma, Trump (no doubt), etc. etc. We need to seize upon and publicize these ruptures in the fabric of psychiatry as they occur, making the contradictions too clear for anyone to ignore.
Good timing here Phil, a lot of us needed an energizing and uplifting anti-psychiatry discussion!
Report comment
It’s all wrong, but it’s alright. I would crawl across border for that. There was nothing there but it was necessary for me to walk that way.
because I learned the way to get an respect and a moment with influential individuals. This can be significant in the mental health debate currently happening in the world.
because that’s only way that can ever get the necessary discourse that’s needed in the mental health debacle underway.
Everybody will instantaneously understand when there is a there is a chance for us to showdown and ya know advocate in an audience of prestigious individuals. Well have the time to get d are point across. because well you know. You’ll know it then.
Report comment
Everyone unquestioningly believes the chemical imbalance lie, Phil. People are dumber than a box of rocks. They swallow anything they see on commercials–literally. No one I talk to is willing to read more than a page of sustained prose. Too much work!
I blame TV. And a refusal to THINK. That’s what the “experts” are for.
I laugh at the shrinks. What are they so scared about? They grossly underestimate how stupid and gullible the doublethinking mass is. (Mass is collective. They can only function as a herd mind.) Maybe the shrinks should evaluate themselves since they sound downright “paranoid” from their rants.
Report comment
Rachel777,
Yes. But I still have hope. Perhaps a deluded hope, but hope nonetheless. The hope that psychiatry, with its fake illnesses and destructive “treatments”, will perish from the land.
Report comment
I get good ideas when it comes to this specific topic during the Zumba class. I attend several times weekly after I’ve hit the gym. It is predominantly people my age l all actually and it’s just what I need as a 40 year old man.
Psychiatric practice could go together with neuroscience. Like be improved a lot to be included with neuroscience. Reading Oliver Sax I think I would improve field a lot for people who utilize and access psychiatry.
Report comment