

There is no question that Andrew Rich, on the evening of May 8, 2017, was in a disturbed state. A 911 caller in Kohler, Wisconsin had said that there was a “naked man in the parking lot (of a golf course) howling like a wolf,” and, according to police reports, when officers arrived and approached Rich, his legs were covered with mud and he squared off “as if to fight.” The police subdued him with a taser and handcuffed him, and even then, as he lay face down on the ground, he shouted Bible verses and proclaimed himself to be God, Jesus, Damien and the devil.
After taking Rich to a nearby hospital, the police filed criminal charges against him for disorderly conduct and resisting an officer. In addition, the police filed a Chapter 51 emergency detention petition, which allows the police to detain and seek treatment for a person deemed mentally ill and a danger to self or others. Rich was soon taken to a county detention center.
At that moment, there were two possible legal paths ahead of Rich. He could be tried on the criminal charges or he could be committed, through a civil proceeding, to a psychiatric facility.
The county pushed for the second option, and while Rich fought against it, his mother Elizabeth, who had worked as a civil and criminal defense attorney in Sheboygan County for more than 30 years, supported it. Her son wouldn’t get a criminal conviction on his record, she reasoned, and instead would get treatment for whatever had led to his psychotic behavior.

Soon Rich, after a spate of legal proceedings, was committed to six months of treatment and sent to Winnebago Mental Health Institute. After roughly a month at Winnebago, he was discharged on an outpatient order that required him to get regular injections of Invega Sustenna, a long-acting form of the antipsychotic paliperidone.
Although Rich thought he would be free after that six months, in December 2017 a civil court judge extended the outpatient commitment order for another 12 months, and then on December 4, 2018, the order was renewed for yet another year. At each extension hearing, Rich’s psychiatrist, Daniel Knoedler, testified that Rich wouldn’t admit that he was mentally ill and needed medication, and that was why the court-mandated treatment was necessary.
After the last hearing, Rich’s despair about being under state control deepened, and he began talking about suicide. On January 11, he was found dead from an overdose of morphine and codeine.
“Looking back on it,” his mother Elizabeth said, in an interview with MIA, “I made so many mistakes in how much faith I had in the mental health system to help my son.”
AOT at 20 Years
Twenty years ago, New York State passed Kendra’s Law, which authorized compulsory outpatient treatment of the “seriously mentally ill.” While this was not the first state statute authorizing compulsory treatment outside psychiatric wards and hospitals, this was the law that kicked off the expansion of “assisted outpatient treatment” (AOT), and today, 47 states have passed such laws, with Massachusetts, Connecticut, and Maryland the only holdouts. SAMSHA and the Department of Justice provide federal funding for AOT initiatives, and AOT is now supported by Congress, the National Sheriffs’ Association, the National Alliance on Mental Illness, and the American Psychiatric Association.
Although there are still peer-led organizations—and other organizations that are sensitive to their arguments—that are opposed to AOT, any larger societal debate over its merits seems mostly over. But much as it was an anecdote of deadly violence—the story of Andrew Goldstein pushing Kendra Webdale in front of a New York subway train—that prompted New York’s passage of Kendra’s Law in 1999, the story of Rich’s death provides reason to take a fresh look at AOT, and its operation in real life.
Rich didn’t have a record of psychiatric hospitalization prior to the day he was reported naked and howling at the moon, but rather a criminal record, from 2008 to 2013, mostly for drug-possession and petty theft to fund his drug habit. If he had stayed within that criminal justice framework, facing charges of disorderly conduct and resisting an officer, he very likely wouldn’t have done any jail time, or a short stint at most. In May of 2017 there were 68 defendants charged with resisting/obstructing an officer or disorderly conduct in Sheboygan County, and those defendants were sentenced to a combined total of 132 days in jail. Most received no jail time at all. But Andrew, against his will, had been shuttled into compulsory treatment, and that sentence, in his case, had no end.
The questions raised by Rich’s story are many. Did Rich meet the stated criteria for AOT in Wisconsin? Were the civil proceedings that mandated treatment conducted in a manner that provided Rich with a fair hearing? And more broadly, now that AOT has a 20-year-record, is there evidence that it is—in the language of medicine—effective? Does it provide the “benefits” that the public has been told it does?
E. Fuller Torrey: Making the Case for AOT
In the early 1980s, the failures of deinstitutionalization—the emptying of the state mental hospitals—had become visibly evident. The “seriously mentally ill” were cycling in and out of hospitals, showing up homeless on city streets, and being carted off to jail for petty offenses. Now and then there was a report of a mentally ill person committing a violent crime. This was the societal landscape that led psychiatrist E. Fuller Torrey and others to call for compulsory outpatient treatment.
In his 1988 book Nowhere To Go: The Tragic Odyssey of The Homeless Mentally Ill, Torrey set forth his case. “Serious mental illnesses like schizophrenia are brain diseases in which parts of the brain are not functioning properly,” he wrote. “Since the organ is impaired, it makes little sense to insist that only those persons should be treated who want help and ask for it.”
Those who resist taking antipsychotics lack insight into their illness, Torrey argued. Compulsory drug treatment, rather than infringe on the civil liberties of the mentally ill, would serve to protect “their minds and their lives.”
Torrey was making this case at a time that the American Psychiatric Association was promoting its “chemical imbalance theory of mental disorders,” which, if true, provided his argument with a compelling logic. The public was being told that antipsychotics fixed a dopamine imbalance in the brain, like insulin for diabetes, and if that were so, then compulsory outpatient treatment could be seen as bringing help and comfort to the severely mentally ill who didn’t understand they needed this treatment.
This argument was repeatedly echoed by proponents of AOT in newspaper op-eds and other forums, and often such pleas came from parents, who told of their desperation to help their adult children. One such op-ed, which is still promoted on the Mental Illness Policy website today, was penned by Herschel Hardin, the father of an adult child with schizophrenia, who, according to the website, was known for his “defense of liberty” work with Amnesty International. Hardin wrote that people diagnosed with schizophrenia were “prisoners of their illness,” and that mandated outpatient treatment could set them free.
“Their personalities are subsumed by their distorted thoughts. They cannot think for themselves and cannot exercise any meaningful liberty. The remedy is treatment—most essentially, medication. In most instances, this means involuntary treatment because people in the throes of their illness have little or no insight into their own condition . . . Medication can free victims from their illness—free them from the Bastille of their psychosis—and restore their dignity, their free will and the meaningful exercise of their liberties.”
Compulsory outpatient treatment was being presented to the public as an instrument of freedom and liberation for the seriously mentally ill, and, at the same time, as legislation that would protect the public from seriously mentally ill people who went off their meds and turned homicidally violent. Torrey claimed that mentally ill people were murdering more than 1000 people a year, and the implication was that nearly all of these murders were by those who had stopped taking their meds.
In 1998, Torrey created the Treatment Advocacy Center to lobby for outpatient laws that would “establish clear consequences for noncompliance,” and the following January, Andrew Goldstein made Torrey’s case for him when he pushed 34-year-old Kendra Webdale in front of an oncoming subway.
Twenty-nine years old, Goldstein had a long record of psychiatric hospitalizations and assaults, and now the press had a story of the violent “madman” that Torrey had been warning about. Goldstein, wrote the New York Times, “should have come with a message plastered on his forehead: ‘Ticking time bomb. Suffers schizophrenia. If off medication, run for cover!’ “
In November of that year, New York State enacted Kendra’s law, which set forth a civil procedure for committing the severely mentally ill to compulsory outpatient treatment. According to the statute, only those who had a history of non-adherence to treatment and had either been hospitalized twice in the past three years, or had committed an act of serious violence toward self or others in the last four years, would be subjected to such forced treatment.
While several groups mounted legal challenges to Kendra’s Law, arguing that it violated the constitutional rights of those deemed “mentally ill,” in 2004 the New York Court of Appeals put its stamp of approval on the legislation. The state already had legal authority to commit people to a mental hospital, and Kendra’s Law simply extended that existing commitment power to a community setting. Newsday called the court’s decision a “triumph of common sense.”
At this point, the one element missing from the “case for AOT” was evidence that it was “effective,” and that it achieved the promised ends. It had been pitched as a medical intervention, but the first two randomized clinical trials of AOT had not shown that it met this efficacy standard. However, in March 2005, New York issued a “Final Report on Kendra’s Law,” and while it didn’t provide any findings from a scientific study, it still provided Torrey and other proponents of AOT with results that they could use to push for expansion of AOT laws nationwide.
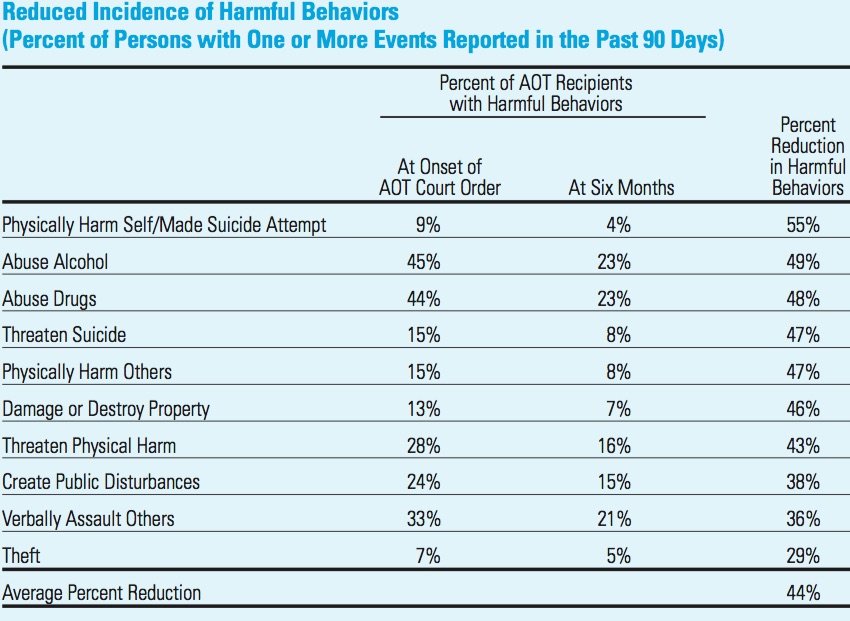
From November 1999 through the end of 2004, there had been 4,041 petitions filed for AOT orders under Kendra’s Law, with 3,766 of those petitions granted. In its report, the state detailed how often this group had experienced various problematic behaviors in their three years prior to AOT, and then calculated the “percentage” that these problematic behaviors decreased during their time on AOT (which could be six months or longer.)
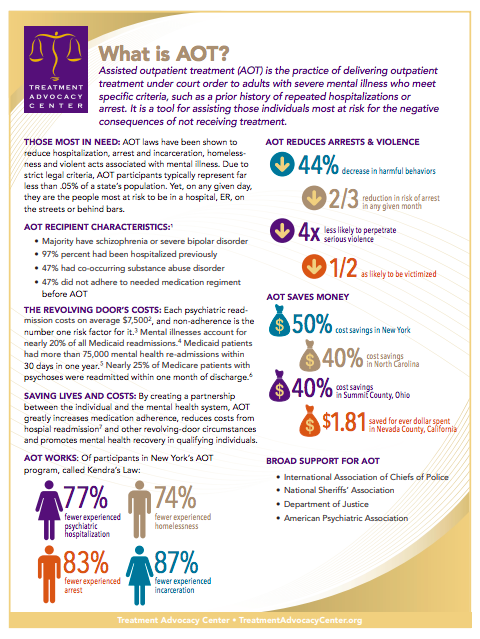
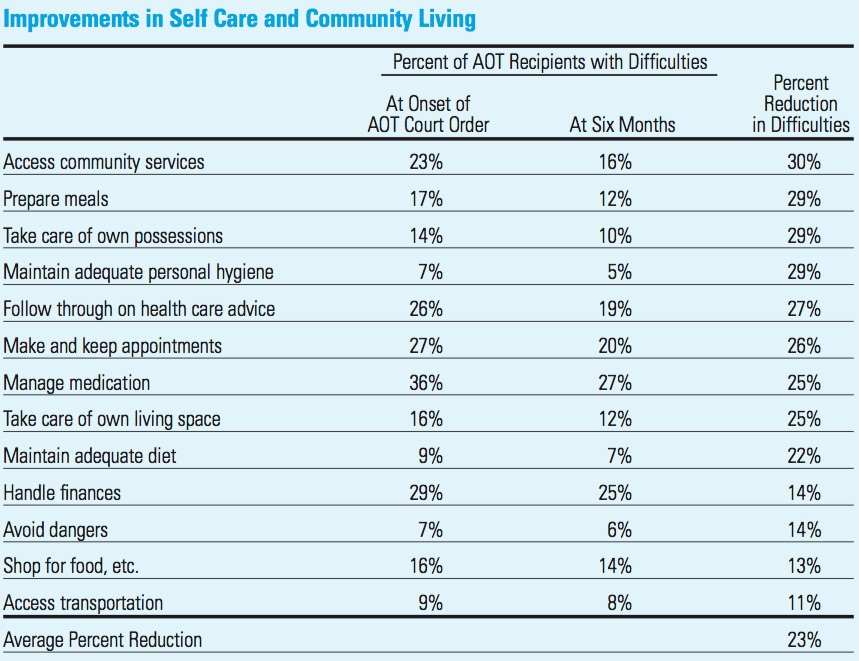
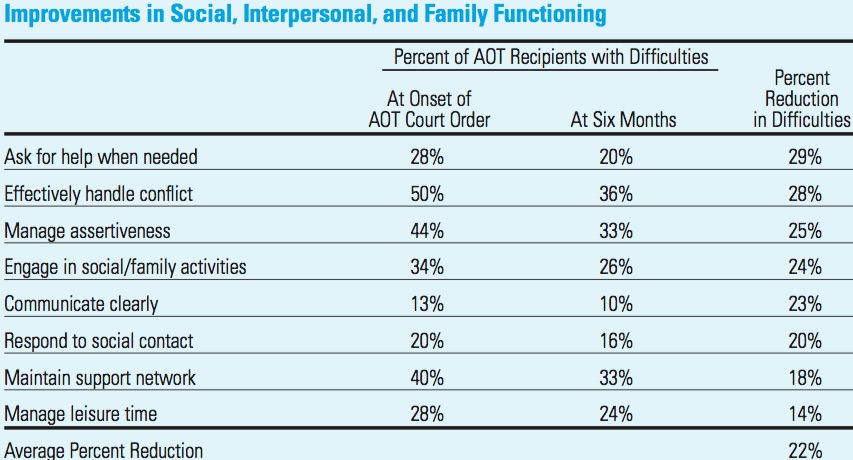
The results, at least at first glance, did tell of impressive results. Incarcerations were down 87%; arrests 83%; psychiatric hospitalizations 77%; homelessness 74%; harmful behaviors 44%; difficulties in self-care and community living 23%; and difficulties in social, interpersonal and family function 22%.
Torrey and others still cite this report today. Here is a picture of Treatment Advocacy Center’s “one page” summary of the evidence for AOT:
Once New York issued its report, Torrey and others continued to lobby other states to adopt AOT legislation. Torrey regularly played up the violence element, informing the public that it was due to the seriously mentally ill being off their antipsychotic medication. In a 2013 appearance on 60 Minutes, Torrey said that even mass shootings could be blamed on the absence of forced treatment laws.
“We have a grand experiment: what happens when you don’t treat people. But then you’re going to have to accept 10 percent of homicides being (committed) by untreated, mentally ill people. You’re going to have to accept Tucson and Aurora. You’re going to have to accept Cho at Virginia Tech. These are the consequences, when we allow people who need to be treated to go untreated. And, if you are willing to do that, then that’s fine. But I am not willing to do that.”
Again and again, it was this “dangerousness” argument that prompted states to adopt AOT laws, with state legislatures moved to act after someone with a “mental illness” committed a homicide. Many of the state laws were named after the murdered person. California passed Laura’s Law; Louisiana passed Nicola’s Law; New Jersey passed Gregory’s Law; Kentucky passed Tim’s Law; Michigan passed Kevin’s law, and so forth.
In 2011, DJ Jaffe, a founding board member of the Treatment Advocacy Center, launched Mentalillnesspolicy.org, to promote the benefits of AOT to the media. Torrey was already the go-to psychiatrist for media covering this topic, and soon Jaffe became a second favorite source for newspapers and broadcast media, his website today listing his many interviews.
Their efforts have stirred newspapers and other media to report on the “success” of AOT. “The treatment required by Kendra’s Law,” the New York Times wrote, “is proven to reduce a patient’s risk of hospitalization, suicide, and violence.”
In 2016, the 21st Century Cures Act signed into law by President Obama expanded federal funding for involuntary outpatient treatment programs, which gave Torrey reason to declare victory. “After lounging on the doorstep of respectability for the past decade,” he wrote in the Psychiatric Times, “assisted outpatient treatment has finally entered the mainstream.”
The Case Against AOT
The case for AOT, when carefully parsed, is based on six assertions:
- The societal failure evident in the early 1980s—revolving door patients, homeless mentally ill, and so forth—was due, at least in part, to the failure of the seriously mentally ill to take their medications.
- Antipsychotic medications are drugs that treat a brain illness, and effectively so.
- People who don’t want to take their antipsychotic medication lack insight into their illness.
- Antipsychotics are protective against violence.
- Studies have shown that AOT reduces hospitalization, arrests, violence, and difficulties in social functioning.
- AOT laws have strict criteria that limit their application to the severely mentally ill who haven’t adhered to treatment, and either have had repeated hospitalizations, or are a danger to self or others.
The case against AOT—and this is quite apart from any civil liberty claims—is that all six of these assertions are belied by history, science, and a critical review of AOT research.
The Revolving Door Syndrome
In 1963, when President John Kennedy unveiled his plan for reforming the nation’s care of the mentally ill, he announced that the discovery of new antipsychotics had made it “possible for most of the mentally ill to be successfully and quickly treated in their own communities and returned to a useful place in society.” The state mental hospitals could be closed and replaced with a matrix of community care.
That vision never turned into a reality, and not long after Kennedy set the nation on this new path, the first study of the longer-term effects of antipsychotics provided scientific reason to doubt that it ever would.
In 1961, the NIMH launched a nine-hospital study of newly admitted schizophrenia patients. At the end of six weeks, those treated with one of three antipsychotics (known as phenothiazines) were doing better than the placebo group. This finding was understood to establish the short-term efficacy of these drugs, and helped create societal belief that it would now be possible to move care of the seriously mentally ill into the community. However, the one-year results, which NIMH investigators announced in 1967, were of an opposite sort. The patients that had been treated with “placebo” in the hospital, the researchers reported, “were less likely to be rehospitalized than those who received any of the three active phenothiazines.”
This was a result that hinted of in-hospital drug treatment that increased the likelihood that a person diagnosed with schizophrenia or some other psychotic disorder would become chronically ill, and clinical observations soon added reason to suspect that might be the case. Patients were now cycling in and out of mental hospitals, and in the 1960s, psychiatrists dubbed this new clinical course the “revolving door syndrome.”
Jonathan Cole and other prominent psychiatrists at the National Institute of Mental Health soon described what they thought was happening. Patients regularly hated how the drugs made them feel, and after discharge from the hospital often abruptly quit taking them, which led to relapses that tended to “persist and intensify.” Yet, even when patients reliably took their medications, relapse was common, and it seemed that “relapse during drug administration is greater in severity than when no drugs are given.”
These clinical perceptions led the NIMH to fund three studies in the 1970s that assessed the longer-term outcomes of schizophrenia patients treated with and without antipsychotic drugs. In each study, the longer-term outcomes were worse for those randomly assigned to the medication group. This led William Carpenter, who conducted one of the three studies, to pose a haunting question: was it possible that antipsychotic medications made patients “more biologically vulnerable to future relapse than would be the case in the natural course of their illness?”
This was a breathtaking moment for psychiatry. If this were so, these drugs were worsening the very symptom—psychosis—that they were supposed to treat.
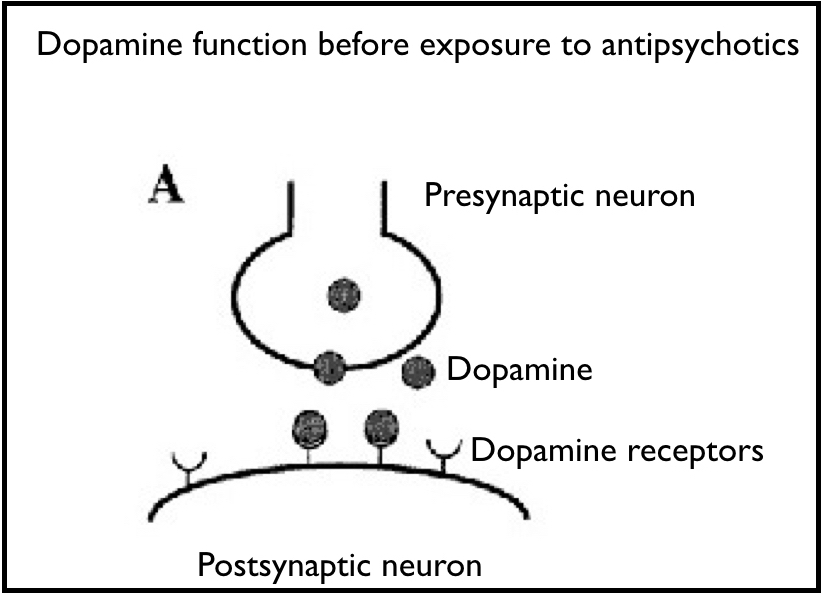
Two physicians at McGill University, Guy Chouinard and Barry Jones, then put forth a biological explanation for why this might be so. Antipsychotics block dopamine receptors in the brain, and in compensatory response, the brain increases the density of its dopamine receptors. In other words, they induce the very abnormality—a dopamine supersensitivity—hypothesized to cause psychosis in the first place.
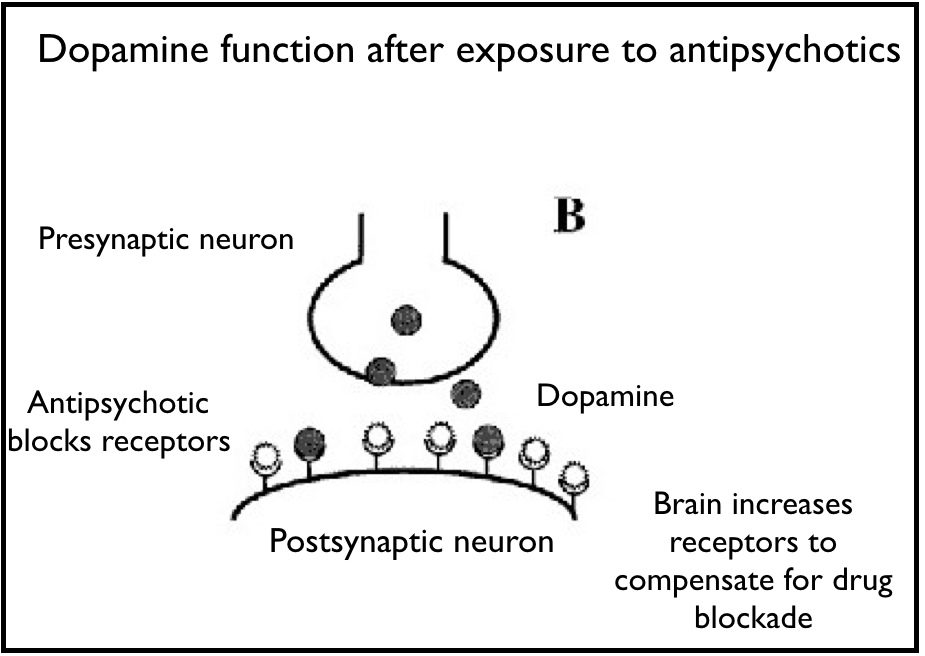
“Neuroleptics can produce a dopamine supersensitivity that leads to both dyskinetic and psychotic symptoms,” they wrote. “An implication is that the tendency toward psychotic relapse in a patient who has developed such a supersensitivity is determined by more than just the normal course of the illness.”
As a result of this drug-induced dopamine supersensitivity, patients were at particularly high risk of relapse when they withdrew from the drugs, Chouinard and Jones said. Yet, if patients stayed on the drugs indefinitely, they were at risk of developing a chronic “tardive psychosis.” When this happened, they concluded, “the illness appears worse” than ever before. “New schizophrenic or original symptoms of greater severity will appear.”
That was the state of the research literature on antipsychotics in the early 1980s, when the failures of deinstitutionalization were becoming so apparent. And while there were obvious social factors that had contributed to this failure—the United States never fully funded the matrix of community care that President Kennedy had envisioned, and homelessness spiked in the early 1980s after President Ronald Reagan cut federal funding for mental health services—the research literature revealed that deinstitutionalization had rested on a clinical hope that had never panned out.
The scientific literature was telling of drugs that increased the likelihood that patients would become chronically psychotic and functionally impaired over the long term. The fact that so many patients hated how the drugs made them feel only added to this system-wide failure, because it led many discharged patients to abruptly stop taking the drugs and fall out of any system of care, and into homelessness or jail.
Today, it is clear that this research presented our society with a defining moment. If these scientific findings were to guide societal thinking, then we would have needed to rethink the use of these drugs. However, the public heard little of this research. Instead, Torrey and others put forth an argument that the failures of deinstitutionalization arose, in large part, because of a failure of the seriously mentally ill to take their drugs. By making this argument, Torrey and others were in essence doubling down on the very drug-centered paradigm of care that had failed.
Scientific research should be predictive of the future, and given the research literature that had emerged by the early 1980s, it could be expected that this doubling-down would lead to a continuing societal failure, and that has indeed proven to be the case. While there are many metrics that attest to that failure, two in particular stand out.
The first is the nationwide disability count. In 1987, there were 1.25 million adults on government disability due to mental illness, or one in every 148 Americans. Today, there are more than 5 million adults on disability due to mental illness, or one in every 61 Americans. The disability rates have soared in the past 40 years.
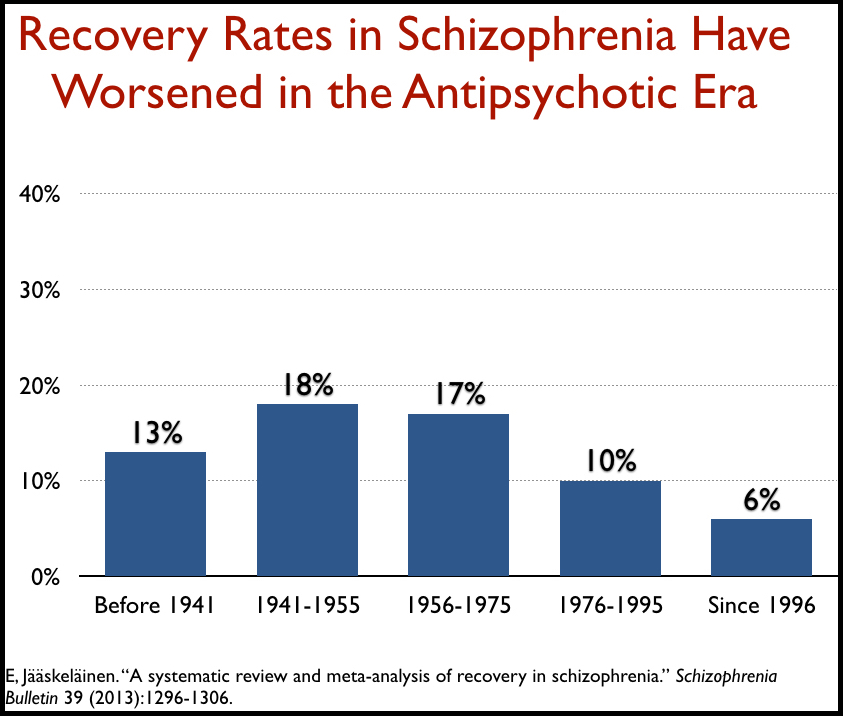
Second, recovery rates for schizophrenia patients have steadily declined in the antipsychotic era, from a high of 18% in the 15 years prior to the introduction of antipsychotics in 1955 down to 6% in studies conducted since 1997. This current recovery rate is the lowest for any period since the schizophrenia diagnosis was first constructed more than a century ago.
Antipsychotics are medications that treat a brain disease, and thus are an essential treatment for this illness.
In their arguments, Torrey and other promoters of AOT speak of schizophrenia as a brain disease, and for the longest time, the public was informed that this illness was due to too much dopamine activity in the brain. Antipsychotic medications, by blocking dopamine, helped normalize that dopamine activity, like insulin for diabetes. That was the soundbite that helped sell AOT.
However, the dopamine hypothesis of schizophrenia started falling apart in the 1980s, and in 1994, John Kane, a well-known schizophrenia researcher, concluded that “a simple dopaminergic excess model of schizophrenia is no longer credible.” While there have been researchers since then who have continued to investigate dopamine function in people so diagnosed, in 2012 Swedish researchers echoed Kane’s conclusion. “It is unlikely that a single neurotransmitter system can explain such diverse symptoms [of schizophrenia] . . . Thus, any simple, exclusive pathology of the dopamine system was and is doubtful.”
Instead, research has shown that antipsychotics, over time, alter the brain in harmful ways. As Chouinard and Jones noted, they induce a “dopamine supersensitivity” that appears to make patients more biologically prone to psychotic episodes than they would otherwise be. They also cause tardive dyskinesia in a significant percentage of patients, which is a form of permanent injury to the basal ganglia region of the brain. MRI studies have found that these drugs shrink the brain, with Nancy Andreasen, the long-time editor of the American Journal of Psychiatry, linking this shrinkage to cognitive decline and increased functional impairment in one of her reports.
This is not a record of scientific findings that tell of a class of medications that—as Torrey and other AOT proponents inform the public—are an “essential” treatment for a known brain disease.
People who don’t want to take their antipsychotic medication lack insight into their illness.
Torrey argues that 50% of people diagnosed with schizophrenia, and 40% of those diagnosed with bipolar, suffer from anosognosia, or a lack of insight into their illness, and this is why they refuse to take antipsychotics and other prescribed medications. Yet, the research described above reveals how such drugs can make patients feel worse and hinder their functional capacities, which is precisely what many people so diagnosed complain about. In addition, long-term studies reveal that tapering off antipsychotic medication, rather than being a route to clinical deterioration, can be a path to long-term recovery.
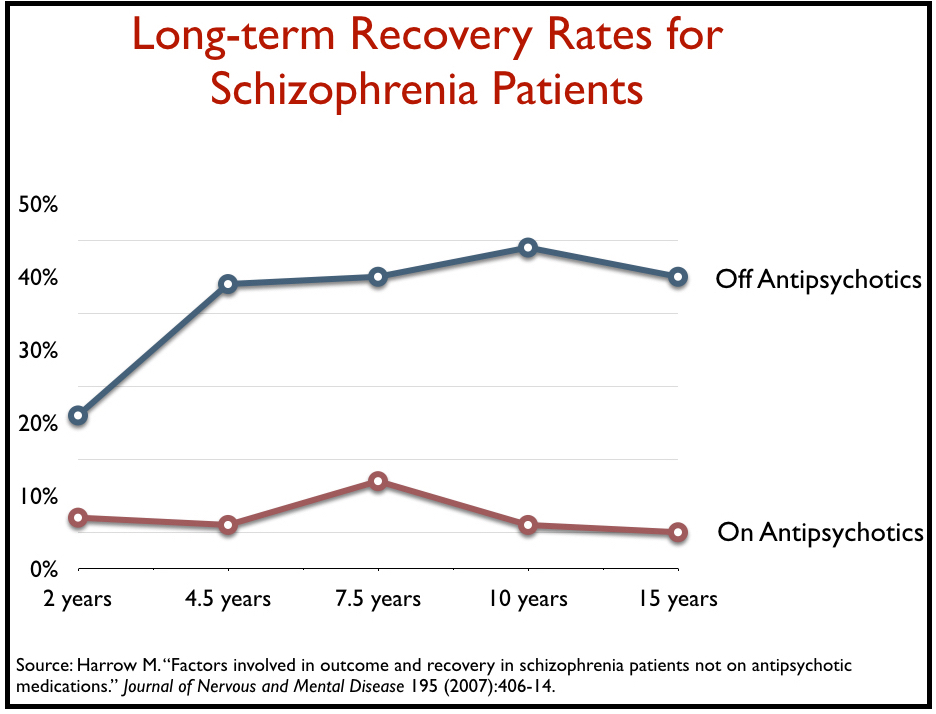
The most compelling evidence for this comes from Martin Harrow and Thomas Jobe. In the late 1970s and early 1980s, they enrolled 200 psychotic patients, who were mostly suffering from either a first or second episode of psychosis, into a longitudinal study. All were treated with drugs in the hospital and discharged, and then Harrow and Jobe periodically assessed how they were faring and whether they were taking antipsychotic medication. A difference in outcomes between the medicated patients and those who, on their own, had stopped taking the drugs, showed up at the 4.5 year followup, and by the end of 15 years, the schizophrenia patients who had quit taking antipsychotics were eight times more likely to be in recovery than those who had continued taking the drugs.
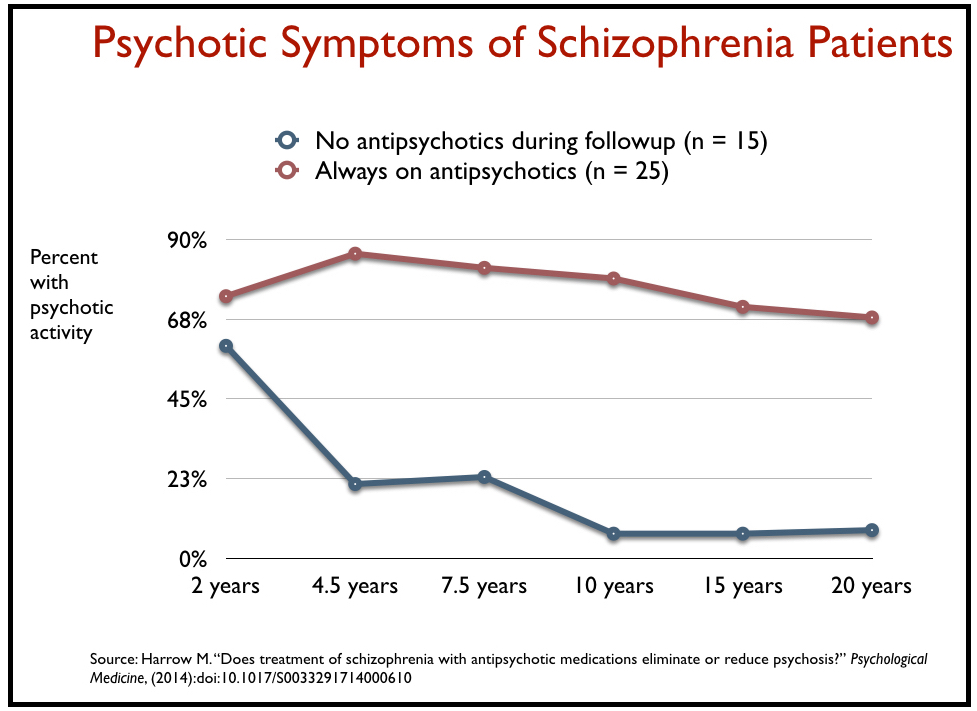
Furthermore, Harrow and Jobe found that those who got off antipsychotics early and stayed off them throughout the study were much less likely to suffer relapses than those who were consistently medication compliant. They reported that 72% of the patients who were “always on antipsychotics” were persistently psychotic; 46% who were “sometimes” on antipsychotics fell into this category, and only 7% of those who never used antipsychotics after year two did.
In a presentation at the 2008 annual meeting of the American Psychiatric Association, Harrow summed up his findings in this way: “I conclude that patients with schizophrenia not on antipsychotic medication for a long period of time have significantly better global functioning than those on antipsychotics.”
There are several other long-term studies that have found higher recovery rates for psychotic patients that have quit taking their medications. Furthermore, surveys of psychotic patients reveal that their beliefs about the drugs are in line with that research. While many patients told researchers that they found the drugs helpful over the short-term, the majority said that the drugs impaired functioning over the long-term, and thus were a “barrier” to recovery.
When this research is considered, it is easy to see that stopping antipsychotic medication, rather than be taken as a sign that a person lacks insight into an illness, might instead be seen as a sign that a person is finding that the drug treatment is worsening symptoms and his or her capacity to function, and that by stopping antipsychotic medication they are giving themselves a better chance of recovering over the long term.
Antipsychotics are protective against violence.
It is clear that when people diagnosed with a psychotic disorder go abruptly off their drugs, they are at high risk of becoming psychotic again, and that in this state, there is an increased risk that they may commit an act of violence. But that is a risk that arises within a drug-based paradigm of care, as opposed to a risk that might arise in relation to the disorder itself.
Prior to the introduction of antipsychotics in 1955, four studies of patients discharged from mental hospitals found that that they committed crimes at either the same or lower rate than the general population. However, this risk of criminal behavior changed once hospitalized patients were regularly treated with antipsychotics. Eight studies conducted from 1965 to 1979 determined that discharged patients were being arrested at rates that exceeded those of the general population.
The research literature provides reason why that might be so. The drugs may induce violent urges, and, at the same time, abrupt withdrawal from the drugs may also lead to a period of elevated risk of violence.
In the 1960s and 1970s, patients treated with haloperidol and other powerful antipsychotics regularly complained that these drugs, rather than serve as tranquilizers, could induce an excruciating inner restlessness and anxiety, the pain so severe that they “just wanted to jump out of their skins.” Starting in the 1970s, a handful of researchers began publishing case reports about this phenomenon, which they dubbed akathisia, and concluded that it led to an increased risk of suicide and violence.
In their case reports, researchers described how patients treated with these drugs, seeking to escape from this misery, had jumped from buildings, hung themselves, and stabbed themselves. In one study, 79% of mentally ill people who had tried to kill themselves were found to have been suffering from akathisia.
Such violent urges, the researchers reported, could also be directed at others. Patients suffering from akathisia described “violent urges to assault anyone near,” and wanting to kill “the motherfuckers” tormenting them in this way. A 1990 study determined that 50% of all fights on a psychiatric ward could be tied to akathisia. Yet another study concluded that moderate to high doses of haloperidol made half of the patients markedly more aggressive.
A few case reports linked akathisia to bizarre murders. One thirty-five-year-old man, asked why he had stabbed a grocer he had known for some time, said he did it to get the drug-induced pain out of his head. “The only reason I knifed the guy was Haldol messed me up. Prolixin makes me want to kill, too.” Such case reports led researchers to conclude that haloperidol could produce a “marked increase in violent behavior,” even among those without any prior history of assault. (See Mad in America, pages 186-189.)
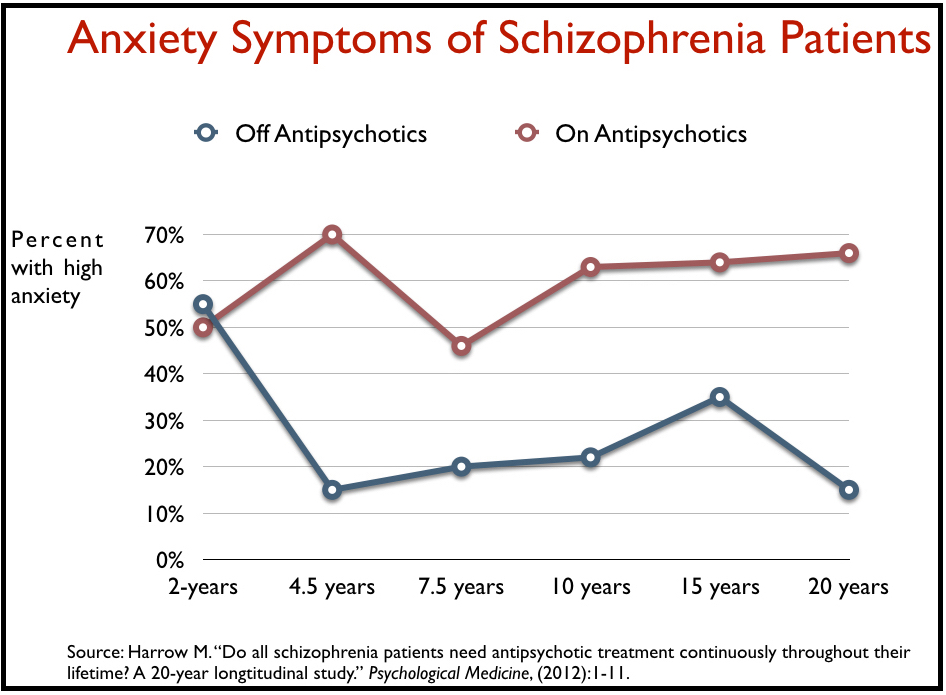
This drug-induced anxiety also showed up in Harrow’s long-term study of psychotic patients. More than 60% of those on medication reported suffering from “high anxiety” throughout the study, compared to 15% of those off antipsychotics.
While such case reports tell of violent behavior by people on antipsychotics (and in particular on high-potency drugs like haloperidol), researchers have also reported that akathisia may become more severe after quitting the drugs. Add in the fact that psychotic symptoms following drug withdrawal may often “persist and intensify,” then it is easy to see why a drug-centered paradigm of care, which exposes patients to the hazards of akathisia while they are taking the drugs, and to increased akathisia and psychosis when withdrawing from them, could lead to an increase in violence by the “severely mentally ill.”
In fact, the poster boy for AOT, Andrew Goldstein, is better seen through that lens, rather than as someone who committed a senseless murder while “off his meds.” His first “psychotic” episode occurred at age 19, when, while on vacation with his family, he bizarrely turned over a table where two women were sitting. Over the next few years, he became a revolving-door patient. He was hospitalized 13 times alone in 1997 and 1998, and during a two-year period, he assaulted people 13 times, which included assaults on clinical and hospital staff. As his hospital record on 7/30/98 noted, for the “last 6-12 months patient has been acting aggressively and impulsively by striking out unprovoked.”
Goldstein’s last hospitalization in 1998 was from November 24 to December 15. He was treated with antipsychotics and yet, at discharge, was described as still quite psychotic. The drugs had not quelled his symptoms, and it was only 18 days later, during which time he apparently stopped taking his medication, that he pushed Kendra Webdale in front of a subway train.
Goldstein’s behavior was presented to the public as a binary story. Off medication he was a murderous psychotic; on medication, or at least this was the implication, he was fine. But, in fact, his story is of a revolving-door patient who became quite assaultive and ever more psychotic while going on and off drugs. He serves as an example of a failed paradigm of care, rather than as an example of how people diagnosed with schizophrenia may become violent if they go off their medication.
There is still much controversy over the risk of violence by the seriously mentally ill. The increased risk has been found to be of a minimal sort in some studies, particularly if the “seriously mentally ill” are matched to a “normal” cohort living in the same community (and thus of a similar class). The risk is certainly exaggerated in the public mind, and this is particularly true of the societal understanding that the violence that does occur can be attributed to people being “off their meds.”
A meta-analysis of 110 studies that looked for “risk factors for violence” in psychotic patients found that medication non-adherence was of only “moderate importance.” Factors that were of greater importance included having been a victim of violence, homelessness, substance abuse, and most notably of all, non-adherence with psychological therapies.
In sum, the risk of violence by the “severely” mentally ill emerged within a drug-centered paradigm of care that helps create revolving-door patients, who may then go off their drugs upon discharge. Meanwhile, studies that predate the antipsychotic era remind us of a time when this elevated risk of violence was not found to be present in the “mentally ill.”
Studies have shown that AOT reduces hospitalization, arrests, violence, and difficulties in social functioning.
Although Kendra’s law was passed 20 years ago, and AOT laws have been enacted in 47 states, with such programs supported by federal agencies, there have been only three randomized clinical trials (RCTs) of AOT—two in the United States and one in the UK. RCTs, of course, are seen as the gold standard in medical research, and thus these three studies can be seen as providing the best evidence regarding the “efficacy” of AOT.
The first RCT was conducted as part of a pilot project on AOT at Bellevue Hospital in New York City during the 1990s. In the study, 142 patients were randomized either to court-mandated outpatient treatment and enhanced services, or to enhanced services alone, and after 11 months following discharge, “on all major outcome measures, no statistically significant differences were found,” the researchers reported. Rates of rehospitalization, arrest, and treatment adherence were all the same, as were the patients’ “quality of life” and “symptomatology.”
The second RCT, known as the Duke Mental Health Study, assessed outcomes for 331 people who had been involuntarily hospitalized and were then randomly assigned, upon discharge, to regular community care or to outpatient commitment under North Carolina law. There were no significant differences between the two groups at the end of one year, including arrest rates, which were 19% for both groups.
The Cochrane Collaboration is known for its systematic reviews of medical interventions, and in a review of AOT, Cochrane researchers calculated that, based on the two RCTs in the United States, it would require placing 238 patients on AOT orders to prevent one arrest, 85 on AOT orders to prevent one hospital readmission, and 27 on AOT orders to prevent one episode of homelessness.
The RCT in the UK, which was conducted more recently than the two in the United States, involved 333 hospital patients discharged to either a compulsory treatment order or to similar outpatient care but without the compulsory aspect. The researchers “found no support in terms of any reduction in overall hospital admission to justify the significant curtailment of patients’ personal liberty” by commitment orders.
In all three RCTs, there was no significant difference in outcomes. The Cochrane review concluded that compulsory outpatient treatment orders do not “result in better service use, social functioning, mental state, or quality of life compared with either standard voluntary or supervised care.” The only superior outcome for those on compulsory orders in these three RCTs was that the patients were “less likely to be victims of violent or non-violent crime.”
However, Torrey and other promoters of AOT do not cite those RCT results when making their case, or else they dismiss the findings as insignificant or irrelevant. Instead, they mostly depend on three sources for making their case: a “subgroup” finding from the North Carolina RCT; the 2005 report by New York State; and a study of rates of violence by people on AOT orders in New York.
After the North Carolina RCT failed to show superior outcomes for the AOT group, the investigators combed through their data looking for evidence of efficacy among subgroups in the AOT cohort. They determined that those who were on compulsory treatment orders for longer than six months, and who also had three or more clinical contacts per month, had better outcomes—lower hospital readmissions, arrest rates, violent acts, etc.—than the patients in the non-compulsory cohort.
This is the type of data mining that pharmaceutical companies, when faced with a failed trial, will do. They will seek to isolate a subgroup of patients treated with their drug who fared better than the median outcomes in the placebo group, and thus declare that the drug works for that particular type of patients. It’s a biased comparison, because you are comparing outcomes for a select set of “good responders” in one group to the average response in the comparison group, and it is known to be an example of bad science.
In this case, those who were under an AOT order for a sustained period were a group of initial “good responders” to that “treatment.” Those who had to be rehospitalized wouldn’t be included in the outcomes of the “sustained AOT” group, because they would have been deemed treatment failures in the first six months. The researchers then compared this subgroup of good AOT responders to the outcomes for all of those in the comparison cohort, including its failures during the first six months. In that way, the North Carolina investigators claimed that it was “sustained AOT” that produced a benefit, which is a finding that has been echoed by Torrey and other AOT promoters.
As for the 2005 report by New York State, which Torrey’s Treatment Advocacy Center features today on its website, it did not tell of outcomes from a scientific study. The state simply compared the frequency of problematic behaviors among the 3,766 recipients of AOT in the three years prior to their being committed to AOT to the frequency of such behaviors during their time—six months or more—they were on AOT. It is a before-and-after comparison, and it was bound to show a reduction in problematic behaviors during the AOT period.
In order to be eligible for AOT, the “mentally ill” patients needed to have had a difficult time in the three prior years. It should be expected, then, that they would have fewer difficulties during the much shorter time they were on AOT, when they were also receiving a “package of enhanced services,” which included better access to housing and vocational services.
For instance, the 2005 study tells of a “77% reduction in hospitalization.” Ninety-seven percent of the AOT patients had been hospitalized prior to being put on AOT, and that is because hospitalization was basically a requirement for an AOT order. These patients were then treated with enhanced services in the community for six months or more, and the only possibility was that their collective hospitalization rate would go down. In this case, 22% of the AOT patients were rehospitalized. Is that good or bad? What would the rehospitalization rate have been for this same group of patients if they had been given enhanced services, but without the compulsory treatment? Without a comparison group, which an RCT provides, there is no way to know.
In addition, the state’s use of “percentage reduction” in unwanted outcomes during AOT leads to a misleading impression. For instance, 9% of the 3,766 AOT recipients sought to “physically harm self” prior to AOT and only 4% did during AOT. Even though there was an improvement in only 5% of the patients, this was calculated, in the 2005 report, as a 55% reduction in self-harming behaviors. Seven percent had engaged in “theft” before AOT; 5% did during AOT. This was recorded as a 29% reduction in theft. And so on, as the graph below shows.
This misleading presentation of outcomes is present in all of the New York State statistics cited by Torrey. The majority of the 3,766 AOT patients were not deemed to have behavioral problems during the three years prior to their AOT commitment, or to have difficulties in “self-care” and “functioning” at the time of their commitment. As a result, if there was even a small percentage of patients who moved from the “had problems” category before AOT to the “didn’t have problems” category during AOT, it showed up as a substantial “reduction” in the unwanted behaviors.
The data cited by Torrey regarding the reduction of violence by AOT orders in New York State is similarly misleading. The statistic that Torrey loves to promote is that patients who are not on AOT are four times more likely to be violent than those who are. This claim comes from a 2010 study commissioned by New York that compared outcomes for 76 individuals mandated to AOT, who received enhanced services and “priority to housing and vocational services,” to a group of 108 patients discharged from a mental hospital who only got standard community care. There was one act of serious violence in the AOT group of 76, and five such acts in the second group of 108, and while that second number is indeed more than four times higher, it obscures the fact that 96% of the non-AOT patients did not commit any violence.
Indeed, the investigators who conducted the study viewed their findings very differently than Torrey, as they noted that mandated treatment included “priority to housing” and other enhanced services, which the comparison group did not receive. As such, they wrote, “the results do not support the expansion of coercion in psychiatric treatment.”
AOT laws have strict criteria that limit their application to the severely mentally ill who have had repeated hospitalizations of arrests and a history of non-adherence to treatment.
Kendra’s Law requires that all of the following criteria must be met before a New Yorker can be placed on AOT.
- Be unlikely to survive safely in the community without supervision
- Have a history of non-adherence to treatment that has resulted in hospitalization or act of violence toward others or self
- Be unlikely to voluntarily participate in treatment
- Need AOT to prevent a relapse that would likely involve risk of harm to self or others
Yet, according to New York’s 2005 report on Kendra’s law, of the 3,766 individuals who had been placed on AOT by that time:
- Only 18% had difficulties in self-care and community living at the onset of the court order (an average across a range of tasks)
- Only 32% had “difficulties” in social and family functioning (an average across a range of tasks)
- Only 36% had difficulties with “medication management” (and 34% were taking the medications just as prescribed)
- Only 15% had threatened suicide or physically harmed others in the 90 days prior to the order
According to this 2005 report, the majority of the 3,766 people who had been placed on AOT, at the onset of their order, were living in the community and taking their medications, and only a small minority had threatened to harm self or others in the previous 90 days. Nearly all of them had been hospitalized in the past three years, and so it would seem that inpatient hospitalization was the one criteria that all met. But clearly the majority didn’t fulfill all of the criteria that was legally required before one could be put on AOT.
The Case for AOT Deconstructed
As can be seen, Torrey, Jaffe and others have sold the public on AOT with a public argument that appears to be based in science, but, in fact, ignores science at every turn. There is no presentation to the public of the research that tells of a failed paradigm of care, e.g. of drugs that may worsen psychotic symptoms, shrink the brain, impair the chance of long-term recovery, and produce an inner agitation associated with suicide and violence. There is no telling of how outcomes for schizophrenia patients are now worse than ever before, and that RCTs have found that adding compulsory treatment to decent community care produces no added benefit.
And as Andrew Rich’s story reveals, this ignorance of science—and the slapping of AOT orders on people who don’t meet the criteria—can produce a fatal despair.
Death in Wisconsin
Andrew Rich is remembered by his mother Elizabeth, and other family members, as being quite precocious as a toddler—reading by age three and naming a child’s version of Homer’s Odyssey as his favorite book by kindergarten. “He was very, very intelligent, bright and charming from the beginning,” she said.
He was the oldest of three children, his mother an attorney and his father a plumber, and as a Sheboygan Press article wrote, his childhood didn’t foretell of later problems. “He was a writer, an animal lover, a Boy Scout who hiked with this father and attended plays with his grandparents. He was an altar boy throughout his youth and enjoyed traveling. He saw most of the 50 states and countries like Australia and Fiji with his family.”
The one place he did struggle was in school. His teachers described him as a “square peg in a round hole,” his mother said. “Andrew was the kid not lining up. I was forever getting calls about that. Andrew doesn’t sit still, doesn’t stay in the line, follow instructions.”
His real troubles began in high school, when, at age fifteen, he was in a car crash and injured his knee. A doctor prescribed Oxycontin for his pain, and when his prescription ran out, he turned to petty theft to fund his newly developed drug habit. Friends remember him getting into some fights in high school, and soon he was a regular in the courtroom, appearing in Wisconsin and Illinois courts 11 times from 2008 to 2013. “He was in trouble most of his [adult] life,” his brother Jacob said. “Nothing serious or violent. Mostly drugs.”
A felony conviction for heroin possession in 2013 turned Andrew in a new direction. He stopped using drugs, and found a girl who, he told his mother, was the “love of his life.” However, the felony conviction made it difficult for him to qualify for educational loans and get a good job. He worked building roof trusses, but “felt that he was stuck in a dead end, like his life wasn’t going anywhere,” his mother said.
Then, in early 2017, he broke up with his girlfriend. He became quite despondent, took a 30-day sabbatical from work, and moved back into his mother’s home that April to write a book. It was then he started showing signs of emotional instability. “He was manic, just really up there in terms of racing thoughts and energy. He was talking on a really deep level,” his mother recalled.
That was the lead-up to his arrest, on May 8, for disorderly conduct and resisting an officer. This date had special meaning in this life.
Andrew had always been close to his father, Jeff, and when he was a child, they had often gone on hikes together, where they would swim in rivers during the day, and howl at the moon like wolves at night. But that was before Andrew became addicted to Oxycontin and his life spiraled out of control. Then, in 2010, his father died unexpectedly. The night before his funeral, Andrew was so distraught he took out a gun and threatened to kill himself. And now, seven years later, with his mind racing, he was thinking of how May 8 was his father’s birthday, and, as one friend remembered, Andrew was hearing his Dad’s voice, telling him “to come find him.”
And so, after hitching a ride to visit his Dad’s grave in Plymouth, he began walking to the Kohler golf course with his Dad’s words urging him on.
The first legal battle
Soon after Andrew’s arrest, the Sheboygan County DA dropped the criminal charges, and instead decided to petition a civil court judge to commit Andrew to a mental hospital. Andrew’s county-appointed public defender urged him to take the deal, but Andrew refused. “I’m not crazy,” he told his mom. “I don’t belong in there.”
The county now had to prove, at a probable cause hearing, that Andrew met the criteria for an extended period of involuntary commitment to a psychiatric institution. Andrew acted as his own attorney at the hearing. He argued that none of the prosecution’s witnesses had provided adequate evidence that he had a mental illness, and noted that none of the police units that had responded could provide body-cam or dash-cam footage of his parking lot behavior. Remarkably, the judge ruled in his favor.
“He was brilliant and extremely articulate,” said his mom. “No one wins mental health probable cause hearings. I’ve never seen it happen.”
At that point, it seemed that Andrew would go free. However, county authorities put him back in jail, and, on May 25, filed a new Chapter 51 emergency petition. This plea was signed by three Sheboygan county employees who had interacted with him, and although Rich had successfully defended himself at the first hearing, the three now described Rich as having been persistently delusional since his initial arrest. They described him as becoming “increasingly more delusional and paranoid” and acting in violent ways, both toward himself and others. He also was “refusing medication.”
At the second probable cause hearing, a medical expert testified that Andrew was mentally ill, and a trial was scheduled for June 14. Andrew represented himself at that trial, and while he waged a valiant battle—the trial last for ten hours—he lost and was mandated to six months of inpatient treatment at Winnebago Mental Health Institute in Oshkosh, Wisconsin.
Six months of mandated treatment
Winnebago was a facility with a troubled past. In 2007, it had been reported that nearly three dozen acts of violence or sexual aggression had occurred during a two-year period, including three patient deaths and a rape. Andrew landed there on May 25, and, based on a report by federal investigators seven months later, the institute was still beset by problems. The investigators issued Winnebago 48 citations for improper patient care, inadequate nursing staff, poor oversight of medical staff, and an unsafe physical environment. One patient who fell and hit his head didn’t get any medical treatment for 12 hours and died 17 days later. Google reviews of the facility, written by former patients, are filled with complaints about unprofessional staff, medication mismanagement, and prison-like conditions.
Andrew ran into his own spate of trouble during his thirty days there. He made a complaint about the treatment and soon a staff report told of how Andrew had been restrained because of “aggressive” and “dangerous” behavior. Andrew’s version of the event, however, was quite different. He told his mom that, as he was making a “soft-spoken complaint,” four guys “came up behind him, grabbed him, slammed him on a steel table, tied up his wrists and ankles, and left him in seclusion for hours and hours.”
Despite the case report, Andrew was transferred to a less-restrictive residential facility on June 23, and then he was soon discharged from that facility, on an outpatient treatment order that required him to get regular injections of Invega, a long-acting antipsychotic.
Andrew, his mother recalled, hated how the injections made him feel. “Everyone could see the Invega completely changed his personality. He was impotent. He had no physical sensation. He couldn’t taste food. He couldn’t experience [anything].”
Twice, Andrew missed an appointed to get his injection, and soon the police were knocking on his door. “You know, those appointments that they said I missed, I don’t feel I got any type of proper notice to come and show up,” Andrew later told the court. “I got arrested almost the day after the appointment on both cases. The cops showed up at my house, in front of my house and made me look bad in front of my neighbors and came and cuffed me and brought me [to the hospital] . . . somebody could have called me and asked me to come [to the hospital]. I would have showed up, you know.”
This was his life on the outpatient order. Andrew “was afraid to express himself,” said his friend Tanya Payne. “He thought if he said something wrong he would be sent to get more medication or to go back to Winnebago.”
But other than those two missed injections, Andrew complied with the order. He had moved into his own apartment and secured a job as a laborer. He looked forward to December 2017, when he could expect to go free.
A Second Legal Battle
In its 2018 “Grading the States” AOT report card, Torrey’s Treatment Advocacy Center gave its highest grade to Wisconsin, a 96 out of a possible 100. The Wisconsin law, much like Kendra’s law, stated that an AOT petition could be granted only if specific criteria for eligibility were met, such as being a danger to self or others, or being “unable to satisfy basic needs for nourishment, medical care, shelter or safety.”
These criteria didn’t seem to apply to Andrew at all, at least at this time. He wasn’t suicidal, he was working, and he was living on his own. However, Sheboygan County’s Department of Health and Human Services petitioned the county court to extend the outpatient order another six months, and a social worker employed by the county, Leigh Ullman, laid out the argument for why it was needed in a deposition. “Andrew Rich views himself as an unconventional individual who is being treated unfairly by society,” he wrote. “Basically, he has no insight into the fact that he has a mental illness. Finally, he has no understanding of the benefits of psychotropic medication.”
This clearly was not an argument specific to the legal criteria for an AOT order. Instead, it was a petition that echoed E. Fuller Torrey’s talking points for AOT, and how people with schizophrenia suffered from anosognosia.
At his trial, the county called upon psychiatrist Daniel Knoedler, who was under contract with Sheboygan County Health and Human Services, and who had been Andrew’s supervising psychiatrist since June 23. Although the first psychiatrists and professionals who had seen Andrew following the May 8 incident had given him various diagnoses, including bipolar and psychosis NOS (not otherwise specified), Knoedler—who was appearing remotely through videoconferencing—told the court that, after having seen or spoken to Andrew on the phone at least six times, his diagnosis was that Andrew had schizophrenia.
Knoedler acknowledged that he had never seen Andrew in a psychotic state, but he said that his diagnosis was consistent with the description of Andrew’s behavior on May 8 and the following few days. In addition, he testified that Andrew had told him in August that he was “thinking of telling someone he knew that he was a werewolf just to see what their reaction was.” This, Knoedler concluded, “is a very unusual statement to make and so I am concerned that again reflects his underlying illness.”
Having diagnosed Rich with schizophrenia, Knoedler told the court that the order needed to be extended because Andrew “said he doesn’t have a mental illness, and he doesn’t think that he needs the medication, and repeatedly indicated he would like to be off the medication.”
That was the county’s case against Andrew. It didn’t produce any evidence of erratic or dangerous behavior by Andrew, beyond his behavior on May 8 at the golf course. It didn’t provide any evidence of ongoing psychotic symptoms. As Andrew’s attorney Charles Wingrove noted, the county’s case rested on how Andrew “might” act, and what he might “think.” Those “mights” didn’t meet criteria for an AOT order.
Judge Kent Hoffman thought otherwise. He explained his reasoning:
“The court heard the testimony of Mr. Ullman, and while I know Attorney Wingrove pointed out the ‘might’ in his letter, I think [Ullman’s] testimony is very clear that he agrees with Dr. Knoedler, and while he initially thought that perhaps [Andrew] wouldn’t have a need for a commitment, despite his meeting the standards for commitment, because he was hopeful that Andrew might voluntarily cooperate and might willingly go along with treatment, he, Mr. Ullman, ultimately decided that the extension of the commitment was appropriate. And so I think there has been a sufficient basis to show if treatment were withdrawn he would meet the standards for a commitment.”
In other words, Andrew’s past actions didn’t meet the standards for commitment. He was being placed under state control for another year because of what might happen in the future, a verdict that left Andrew’s mother aghast.
“Andrew’s done nothing wrong since May, not so much as a traffic ticket. He’s just working and minding his own business. How can they keep him under this commitment when all of the evidence [of mental illness] goes back to the original incident?”
Under Wisconsin law, Andrew was entitled to a second hearing in court if he could find a medical expert to challenge the testimony. He met with three psychiatrists to plead his case, but all three refused to testify on his behalf, with one of the three, forensic psychiatrist Robert Rawski, refusing in large part because of Andrew’s “skepticism about mental illness . . . and the anti-med bias he shares with his mother.”
The three doctors, his mother said, “all sang from the same hymnal.”
Toby Watson, who formerly worked as the chief supervising psychologist for the Wisconsin Department of Corrections, said this was no surprise. “Defense attorneys only have access to a small pool of psychiatrists and psychologists who are indoctrinated into the faith that meds work. It’s sacrilegious for these doctors to speak out against the mainstream medical model.”
And now, with this extension order in place, Andrew’s psychiatric care—and chance that he would ever get out from under state control—remained in the hands of Daniel Knoedler.
Guilty before Trial
Knoedler worked under contract to Sheboygan Health and Human Services, earning $163 per hour for his services. He was known by patients in the area for being quick with the prescription pad, a reputation backed up by prescription data published by the Centers for Medicare and Medicaid. In 2016, he wrote 38 prescriptions per patient, double the 19 prescriptions-per-patient average among the other Wisconsin psychiatrists who accepted Medicare. That year, the government paid more than $1 million for the drugs Knoedler prescribed, which put him into the top 3% of all U.S. psychiatrists who accepted Medicare, in terms of their government prescribing costs.
In March of 2018, Knoedler changed Andrew’s mandated treatment from a drug injection of Invega to Abilify, a less powerful antipsychotic. This led to an improvement in Andrew’s mood and energy, his mother said, but he still struggled with physical and mental side effects with this drug.
Beyond that, Andrew and Knoedler remained at odds in therapy sessions, as Knoedler would focus on getting him to acknowledge that he was mentally ill and needed antipsychotic medication. “His ‘diagnoses’ always seemed to involve a swipe at Andrew,” his mother said.
“He clearly did not like him. Andrew would get so frustrated at the sessions, because he said nothing that comes out of my mouth can be right. If he would relate an accomplishment at work, he was narcissistic. If he would talk about something he was writing that he thought was particularly insightful, he was exhibiting grandiose thinking. Nothing was right. If he said, ‘I can’t do anything right,’ then he is clinically depressed. He said every word that comes out turns against me.”
Andrew’s AOT order was set to expire in December 2018, and it was expected that Knoedler would wait until November to submit a recommendation to the court on whether it should be renewed. Instead, several months earlier, he informed Andrew that he had already made up his mind and that he would advise the court that the outpatient commitment order should continue.
“I was outraged that [Knoedler] would rob him of hope like that,” his mother said. “It’s not supposed to work like that. There is supposed to be a proceeding with a fact finder.”
Soon Andrew stopped talking to Knoedler during their mandated sessions. While his family tried to buoy his spirits, Andrew “was just getting more and more depressed,” his mother said. “He was living a life he didn’t want.”
His brother and friends saw the same thing. “He said he could never escape the state, the forced drugs,” Jacob said. “He felt like this was going to be a permanent thing. And he felt like he wasn’t able to keep relationships while being on the drug because it just really dulled his personality.”
Added his friend Tanya Payne: “He would call crying and upset, just to have someone to talk to. He was miserable with everything he had to go through. I think the drug dissolved his will to be here.”
The Final Trial
The “recommitment hearing” that was held on December 4, 2018 proceeded in much the same way that the trial a year before had, although this time it was even more perfunctory. The county’s attorney, Samantha Bastil, only called one witness, Daniel Knoedler, who once again testified via videoconference. Knoedler told the court that he had diagnosed Andrew as having schizophrenia, a diagnosis that established he was mentally ill. Most of the questioning then focused on Andrew’s state of mind, and his possible future actions. What “might” he do if was not recommitted, for another year, to outpatient treatment?
Knoedler told the court that Andrew mistakenly viewed his psychotic behavior at the golf course as a “one time episode,” rather than an “ongoing illness.” The AOT order should not be lifted until Andrew understood that he had a chronic illness that required antipsychotic medication, Knoedler said. “If he stops the medication, his [likelihood] of psychosis will be extremely high.”
Nobody was called by the prosecution to testify that they had ever witnessed Andrew in a psychotic state. Upon cross-examination by Andrew’s attorney, Knoedler acknowledged that he had not personally witnessed any psychotic symptoms in Andrew during the 18 months he had been treating him. Andrew, he said, “was actually doing very well . . . living in the community.”
In his turn on the witness stand, Andrew told the court he had been working at Plymouth Industries for more than a year, and now had his own health insurance. If the commitment order were lifted, he promised that he would voluntarily see a psychiatrist, meet with a therapist, and take medication. He testified:
“I would like to have a little more role in [my treatment]. By active role, I mean for example if I come to the doctor with a concern and say, ‘this medication is affecting me in this way and it’s making me unable to work or unable to sleep or unable to do this,’ I would expect that there would be some type of reaction or result or adjustment right away rather than just telling me to ignore it or have it continue.
“[The county] makes it sound like it’s all really nice and good and helpful and everything, but it’s not really the same when you are going through the other side. And you know, I mean, I am trying—I do my best to comply with all the rules and everything, but to me it seems like a never-ending process. Honestly, like, some aspects of it seem borderline unconstitutional . . . this whole situation has been rather confusing for me because I didn’t know stuff like this existed.”
The prosecutor did not cross-examine Andrew. His mother then took the stand, telling the court that initially she had been “relieved that the county was taking over and putting him on a commitment” order, but her feelings had changed.
“Andrew has been working. He lives independently. He mows the lawn. He shovels his snow. He shows up for work. He has been promoted and given raises on a regular basis. He is a supportive, loving son to me. And I think that this incredible restriction of his civil liberties is affecting him in a negative way. It affects our family in a negative way.”
The drug treatment, she added, “impairs [Andrew’s] ability to think quickly and clearly . . . He is a human being with his own mind and he is being denied the opportunity to participate meaningfully in his treatment . . . this has been going on for way too long.”
At the end of the testimony, there was little dispute over Andrew’s past actions. Andrew had behaved in a psychotic manner on May 8, 2017, and after that initial psychotic episode, which may have lasted several weeks, nobody had seen any psychotic symptoms return. During the last year, he had been working and living successfully in the community. At issue was that he didn’t agree with his psychiatrist that he was chronically ill.
“The bottom line is this is your life,” Judge Stengel said, as he prepared to announce his decision. “And we want you to have it to the fullest extent possible under your control. And it sounds like you’re doing so many positive things with your life. You’re out there working. You’re helping your mom. You seem to have a vested interest in your situation and tried to learn as much as you can.”
All of this sounded promising. But then Judge Stengel decreed that Andrew would be placed under outpatient treatment for another 12 months. “There are certain areas that the Court has to rely upon expert opinions because that’s not within my area of expertise,” he said.
This was a decision that reflected, in every way, the story told by Torrey and other promoters of AOT. The “patient’s” own self perceptions could be discounted because the “severely mentally ill” lacked insight into their illness. The testimony of his psychiatrist, who understood that psychosis was a brain disease that required antipsychotic medication, should govern his life.
Andrew, crushed upon hearing the decision, now had a haunting question for the court, and really for all who would countenance AOT:
“So long as [Knoedler’s] testimony stays the same, the commitment will never end? I really want a yes or no answer on this because it messes with my stability and my sanity and I just don’t like it. Because to me, it seems like a never-ending process. Like, it’s cool that everybody can sit here and tell me it’s not, but it doesn’t seem that way to me. Because [Knoedler] seems to have the same opinion the whole time and I never said anything about not taking my medication or anything like that. I feel like . . . these words are getting put in my mouth.”
A Life Gone
After the hearing, his mother said, “everybody was worried. We spent Christmas Day with my mother-in-law. . . [On our way home] We had a four-hour conversation about [suicide]. He was curious about death, and what it would feel like.”
His brother Jacob made him promise to call if he thought about “hurting himself.”
Much as Andrew had told the court, the decision “messed” with his stability. In early January, Andrew told his mother that his thoughts were now racing, but that he liked it. “It makes me feel alive.”
His mother worried that a crash was coming and that he should go see a therapist. “No,” Andrew replied, “they will lock me up.”
His mother now similarly felt there was nothing to do. “I didn’t tell anyone or call anyone to get him help [when his thoughts started racing], because I knew he was right. They would have locked him up, and not given him any meaningful treatment.”
When Andrew didn’t show up for work on January 11, the police were called to his apartment to perform a wellness check. They found Andrew on the floor, in a sitting position, with a syringe and drug paraphernalia next to him. He was dead from an overdose.
***********
Part Two: More on Andrew Rich, his legal battles, and MIA’s survey on forced outpatient treatment.
****
MIA Reports are supported, in part, by a grant from the Open Society Foundations



Thanx for an outstanding essay.
Report comment
Mad In America is about the complete lack of success of the existing Mental Health system, and need for use of the alternative workable solutions (that are available).
Below is a research paper from my historical Psychiatrist from Ireland (1998) on the benefits of Psychiatric depot medication (in the community).
https://ps.psychiatryonline.org/doi/10.1176/ps.49.10.1361-b
Over the years that I remained a Psychiatric Patient my Historical Psychiatrist had maintained occupational disability, to be my main problem.
But my Psychiatrist had been incapable of telling the difference between the effects of the drugs he was prescribing, and genuine mental illness.
While I consumed long acting depot injection drugs at Galway Southern Ireland I experienced suicidal hospitalization after suicidal hospitalization. When I attempted to stop these drugs (with permission) I ended up in hospital again fairly quickly. When I was offered an alternative (depot injection) I also ended up suicidal and in hospital again (1984).
I could ONLY come off these drugs very carefully and with suitable help, and when I did, my suicidal hospitalizations and disability ENDED.
I can describe the practical psychological process by which I was able to cope with the drug withdrawal, and how it worked in the long term. BUT any qualified psychologist might do the same.
Suicide and Homicide in Mental Health are often closely related, but from my own experience, I would say that “compulsory depot injections” are more likely to cause Suicide and Homicide than to prevent them.
Report comment
This is a wonderful article, and amazingly calmly presented, considering the context, but then:
It’s quite clear to me that Andrew Rich knew what was going on with him, also in regards what was labeled as “schizophrenia,” but the only way for him to get out of it was to be dishonest, he would have had to act like he believed he had a chemical imbalance, and that he had a disease, which seems given the whole affair not too difficult, since the whole system is more easily fooled into non reality based behavior than a “schizophrenic.” Which brings another thing up before I start listing everything non reality based about the system defining something else besides it’s own behavior as “schizophrenic,” a split brain, a rift from reality.
Nowhere just about, not even with his mother at first, do I see any rational, grounded or even decent attempt to relate to what Andrew thought was going on with him, in fact when he simply states that he was thinking about telling someone he was a werewolf just to see how they reacted, THAT was seen as a sign of a disease.
How can this be a disease at all? I’ve had it myself that responses I’ve had to life, which to me in latent respect seemed “psychotic,” or had a riff with reality, I’ve had it myself that I was quite unable to understand the meaning of the symbolic reality my mind created, EXACTLY to point out what might change my life, would I understand it. That’s NOT a disease. With our physical sense we see only ONE point in time, and unless we use our imagination we can’t navigate past that, and yet it’s exactly there that the mind can try to express underlying trauma, inner wounds, reflexes and belief systems we’ve taken on that were forced on us. And here, the latent ability to understand concepts that when understood or not might determine how our life proceeds, this is seen as a disease, and when the need to understand such expression doesn’t go away, it’s seen as a disease, rather than there’s decent, appropriate or responsible attention given to what resolves the situation. Oh, but then it’s not seen as a disease anymore!
And with Andrew, it was simply that he wasn’t going to have them tell him that what was going on with him was something other than it was.
Added to this, a society which allows bankers to hoard the money resources of a whole nation, and bankrupt it (while someone with too many cats or a house full of things they ever thought might have some purpose but later see no one engage with, they are called hoarders); a society that also finds the present economic trends more important than whether they are causing global warming, than whether any developing country moving away from exploitation can actually build a stable economy, than whether the voice of minorities or poor people that really suffer is really heard without saying they have a disease while trying to get them on antidepressants. And people are SO defensive about believing that survival is adapting to such a system, that even when they disagree with it, would someone express dissent they don’t understand, they become vigilant as seeing it as a psychiatric disease, strengthening that delusion when things inevitably get worse. Then empathy already is “schizophrenic.” And all of the other things, such as whether you are wearing clothes or not, not being able to say things others don’t understand which they think is harassing while it’s OK to be bombarded with commercials the whole day (online, on the TV, in your mailbox, while driving your car, while reading a periodical, would you have a telephone etc. etc.), would you be paranoid about something for a short time and have it go away it’s a symptom of a disease although if you aren’t so paranoid that you think we need funding for a military that can blow up all human life on the planet more than 20 times to kill the enemy along with us and everyone else, then you’re non reality based again and can be put in jail for not going along with it when there’s a draft; and then there are silly things such as someone out of fashion is seen as lesser although the fashion industry and clothes industry will change the fashion to get you to buy more stuff you don’t need while the stuff you already bought the first time stuff changed is already outdated and you could have spared yourself the cost then already, and we come upon such terms as “consensual reality deportment,” or “statistical based norms,” when would you truly honor statistics or what’s consensual and look at what it usually leads to in regards to what you’re supposed to adapt to, it’s more of the above, and NOT reality based; and not following it without appropriate concern is “schizophrenic, again. “Consensual reality,” in such a case refers to a “reality,” that isn’t reality based, which you have to adapt to as the current fashion, the current economic model, the current ideology or the current institution, “culture,” or mob, or gang, or cult or…..
That’s reality based?
When a schizophrenic goes along with that they are healed?
Oh and yeah, when you give people treatment for “schizophrenia,” and they also are given privileged housing, the ones left underprivileged and without “treatment” are going to get more violent… which means they needs more treatment, rather than housing etc.
And what’s going on with all of the “mental illnesses,” is that trauma is being expressed, and if trauma was understood for what it is, then the world would have to look differently at what it believes discipline is. Even for people who are criminal, even for tyrants, even for psychiatrists, because if trauma was acknowledged for what it was, rather than a means of mind control doling out rewards or punishments, being used a deterrent or encouragement (one of the rewards or encouragements being you’re one of the good guys and deserve the right to dole out trauma to others when they don’t behave); if trauma was acknowledged for what it was, then the criminal, the tyrants, the sociopaths and all of the rest would have grown up in a different society, and they wouldn’t have ditched their humanity.
Instead, what would change things is seen as a disease.
And sorry, but I don’t see it as a loss to not be fit for such a society, WHATEVER you say about me.
But yeah, now in regarding “schizophrenia,” medications, I can say that they cause dopamine sensitivity, which leads to more relapsing. But I’m talking about something occurring because it needs to be understood, not because it’s a disease. So this isn’t really relapsing either. Is it? You give somebody something that causes a disease doesn’t mean you were ever treating a disease when you administered it, and it certainly doesn’t mean you need more leeway to administer it when it causes disease; but it also doesn’t meant the the “relapsing,” is of a disease that was there to begin with. Those are two quite different things.
Does anyone see the irony?
You call something a disease, which it isn’t, and you cause more of it with a “treatment” that in REALITY is more of the trauma that might have been what needed attention to begin with, and like magic, you can talk about relapsing or not, and about diseases or not, and…..
You’re focusing on what something isn’t, and then determining when what it isn’t goes away; and in the mean time you’ve avoided the whole….
All to avoid understanding what’s going on to begin with, because it might stretch your conception of reality, might burst the bubble of your comfort zone.
And I never went asking for “medications,” wasn’t even forced on them, although people would have if they could; so I’m REALLY simply concerned with what was going on in the first place, and what has the whole time. And it’s NOT really a disease, and when you hit someone on the leg, and this causes pain because there’s bruising and damage, that’s a BRUISE, that’s also not a disease. Neither is it a malfunctioning of the body. Emotional wounds are NOT diseases. And the expression of such wounds, rather than having a riff with reality are more objective than what’s labeled as objective reality, because they deal with reflexes, with memory, with trauma, with beliefs, with emotions and in doing such deal with the intangibles that our core part of how we respond, and what we bring to us in life, regarding all of those. What it’s about. Whether a factory is making a certain product or not, when there’s a better design for it, and only the machinery has to be adjusted, this doesn’t make the fact that that product isn’t there yet non reality based, nor when the machinery has to be understood as to how it works. The product comes out of the factory. What comes our way in life is determined with how we respond to it…
And adjusting that process seems to be grossly ignored, repressed even, would there be some message in “psychosis.”
Watch a Shakespeare play, Read a Dickens Novel, Go to a Museum, Read Emily Dickinson, Listen to
Mozart or Josquin
Or write your own story, Go crazy….
Report comment
“If ye were of the world, the world would love his own: but because ye are not of the world, but I have chosen you out of the world, therefore the world hateth you.”
Psychiatry hates all who don’t worship from their DSM “bible.” And hates all who don’t want to conform to their control of this world. While they’ve allowed this to become the sad reality, “We now live in a nation where doctors destroy health, lawyers destroy justice, universities destroy knowledge, governments destroy freedom, the press destroys information, religion destroys morals, and our banks destroy the economy.” – Chris Hedges
Anyone who doesn’t stand 100% in support of such a satanic world, largely manifested by the psychiatrists being unjustly given “omnipotent moral busy body” status by our government, is “schizophrenic” today, according to our psychiatrists.
By the way, the “schizophrenia” treatments, the antipsychotics/neuroleptics, can create both the negative and positive symptoms of “schizophrenia.” The negative symptoms can be created via neuroleptic induced deficit syndrome. And the positive symptoms, like psychosis or hallucinations, can be created via antipsychotic induced anticholinergic toxidrome.
https://en.wikipedia.org/wiki/Neuroleptic-induced_deficit_syndrome
https://en.wikipedia.org/wiki/Toxidrome
But our psychiatrists deny this reality, as evidenced by these medically known antipsychotic/neuroleptic induced adverse effects of their drugs, NOT being included in their “BS” DSM “bible.”
https://www.wired.com/2010/12/ff_dsmv/
Thank you, Robert Whitaker, for telling a story of the unjust harm the psychiatrists are participating in, while they utilize the legal system to harm people, rather than bring about justice. Because this type of unjust psychiatric harm is being perpetrated on a massive societal scale. We need a return to the rule of law in America. And a scientific fraud based psychiatric system that utilizes the law to harm, rather than bring about justice for all, will not fit into a return to an actual rule of law system.
Report comment
Well said!
Report comment
I would say that it’s clear that the “treatment” Andrew Rich was receiving caused his death – which has got to be the worst “medical” outcome.
As in Andrew Rich’s case: It would be possible to diagnose ANYONE as “mentally ill” on the basis that they don’t accept that they are “mentally ill”. This basis is similar to the basis used in medieval times to “convict” a person of witchcraft.
Report comment
And the McCarthy era.
Psychiatrist: Do you have schizophrenia?
Accused: Yes.
Psychiatrist: You admit it. I sentence you to 12 mg Haldol a day for life.
Psychiatrist: Do you have schizophrenia?
Accused: No.
Psychiatrist: Schizophrenics lack insight so you must be a schizophrenic with agosognosia. I sentence you to 15 mg Haldol a day for life. Strictly voluntary, but if non compliant we have far less pleasant ways of dealing with your kind.
Heads the shrink wins. Tails you lose.
Report comment
Thank you for this article. Andrew’s story is heartbreaking.
I came from Massachusetts where they had this sneaky way of forcing drugs by using guardianship. They also had representative payees. If all else failed, they certainly had the money there to lock anyone up and force that way.
If anyone wants to avoid AOT or other form of force, my guess would be to go to an impoverished area where the local gov’t does not have the resources to enforce any form of forced psychiatry upon its people. That is just a guess.
Report comment
Lots of places like that in my state. I don’t mean to brag but NAMI gave us a D- in our mental illness system. It’s hard to get better than that in America. 🙂
Report comment
That’s exactly what’s happening in real life. A person has psychosis as a result of taking drugs (often because of marijuana, because nobody knows that marijuana when smoking through a vaporizer causes psychosis), or without vaporizer (in case it is a teenager). After the treatment of acute psychosis, the person begins to behave as if all people are fools, because the treatment of psychosis is when with the help of pills you are simply forced to lie on the bed with excessive drooling. And this excessive drooling is like a part of therapy. And this despite the fact that psychosis, to explain briefly, erases all the old stereotypes and allows to look at the world through the eyes of a newborn, but without losing the intellect. Any nonsense becomes obvious. As a result of acute psychosis, a person is put on a consultative account in a psychiatric clinic and later transferred to dynamic accounting with an appropriate chronic diagnosis. The reasons for this may be many, for example, it is enough to offer the doctor to treat his patients not with antipsychotics but with medicinal herbs. Or just by laziness and in protest at the appointed time not to come to the hospital. Or do not shave a beard. The reason is always there, and in fairness it must be said that the behavior of a psychotic survivor is really strange. So finally we got another patient with schizophrenia, which by the way exist (with all the genes and brain abnormalities, and of course easily can be tested at the biological level). Then of course, a person commits a suicide attempt. In case of Andrew Rich, successful attempt. The system forces a person to commit suicide, and despite valuable experience and possible benefits for man as a species (lateral thinking) a lot of people do that.
Report comment
Good to see the timeline but hard to read about the death of someone caught in a tangle of modern life.
It ‘s all there though not highlighted.
Altar boy- I would wonder about abuse
Poorly fitting school environment
Opioid script possible addiction and potential nondiagnosed concussion.
Trauma/ the death of a parent
– the MH professionals should have addressed all of these issues straight on so maybe incompetentency in the MH system pervasive malpractice orgininating in education at the college and graduate level though there have been books and research on cultures but small and never integrated
into the general mind set of society.
SANSHA dual dx but never into the opioid diseaster and never into the idea of addiction as possible way of coping with trauma.
Other issues gender identity and sexuality and bullying in school and was the school Catholic? Or like the public schools of England and other countries where from Tom Brown’s School Dsys and prior to and beyond the abuse could be both from peers and or adults. Luck of the draw for all of us.
If you watch the series on Cheyrobol somehow easier to watch for me than the searing expose of pain shown in the Central
Park 5 series and documentary – the Workers st the plant – 7 to 1 and they had been programmed always to obey the leader even if the leader were clearly wrong. So much for the lessons of the Nuremberg Trials unless this is an op for interweaving how Trauma seeds do much in all our human systems.
Report comment
Thank you so much for very carefully and factually rebutting the lies that Torrey, Jaffe, and their followers have used for 20 years to spread this assault on the liberty of people with psychiatric labels. But please stop referring to this practice by its 1984 Doublespeak name “Assisted Outpatient Treatment” without quotation marks. Force-drugging people with dangerous, ineffective drugs is is no way “assistance.” When we unsuccessfully fought to stop its implementation in NY 20 years ago, we called it Involuntary Outpatient Commitment, and that’s an accurate description.
Report comment
Wisconsin. I ran for my life.
Tabitha was a few classes away from her Master’s degree when they decided to ruin her life over things that should not even be a Crime.
My Daughter Tabitha had no Transportation; she died at 27.
My other Daughter just plead NGI to 2 Felonies.
Before she plead NGI she was offered 1 year Probation by our Favorite D.A. Larry Nelson who promptly dropped dead in his office of a Lung Embolism. Some people don’t know when to drop the charges.
My Daughter was back in school not on medication and her Chapter 51 was dropped. He has known my child since she was 8. I guess he felt compelled to make sure her life was over at 27 also.
There is a crisis intervention mandate in Wisconsin now so that the police can get you “help”.
Iowa County Wisconsin just charges you criminally and releases you so they can re-arrest you, then you have a felony bail jumping also. Pretty cool how they turn 1 felony into 2 by just releasing and re-arresting you. I know they did it to me.
It really does not matter if you are out of your mind or not.
Chapter 51 and Chapter 971.17 commitments are a Nightmare.
I was lucky enough to have a Judge who liked to hang up on my entire “Conditional Release“ team during revocation hearings that occurred way too often. They tried to revoke me for Witchcraft in 2009.
Here is the transcript: https://drive.google.com/file/d/0Bxko2RDNGScFUVU3WWhPOGFKeDg/view?usp=drivesdk
I had 4 people on my team and luckily I had a private Psychiatrist and Therapist by Court order.
The Community MH center called me untreatable and refused to see me.
They really do hunt you down like an Animal.
My stepmother called Social Services on me several times.
I was hauled off to the Mental Hospital when the Police, Sheriff and Social Services all showed up at my door to take my Children away.
I was immediately Drugged against my will and put on a civil commitment which also prevented me from getting custody of my Children back.
If you “react to injustice” it is a Mental Illness just like the good old USSR.
My Children were severely abused in Foster care
When I complained I was criminalized.
I went from being a Happy Mother of 2 Beautiful Intelligent Creative little girls to a feeling so horrendous that I cannot begin to describe the pain.
I was court ordered to take several brain, mind, body and soul disabling “medications”.
I had every right to be ballistic! My Children were living with pedophiles.
It never ends and the sheer amount of cash they wasted making my life a living hell is a real crime.
I can’t begin to count how much they have wasted on torturing my Children.
I have been to Winnebago Mental Health Institute several times.
I reported a rape of a patient after hearing another patient brag about it.
I saved a Girls (age 18) life at the Racine County Jail.
The Guards were laughing about her lying in her own feces and urine. I honestly thought she would die any moment so I told the Judge when I went for my initial hearing and they HAD TO do something.
My Lawyer told me I saved her life. My charges were dropped in that County.
Ahhhh Wisconsin, the stuff of my night terrors.
No wonder my Daughter had TRAUMA INDUCED PSYCHOSIS when she returned for the first time since her Sisters Funeral.
She has 2 Associates Degrees and spent a Month in Israel last summer but 1 trip to Wisconsin and she’s an insane criminal.
She is no Angel and neither am I but I can honestly say that if I am ever dragged back to Wisconsin I will definitely end my own life. I know how it feels to lose a child to Wisconsin’s ED GEIN style treatment of SO CALLED disorders. Wisconsin…….. I could write a book on that State.
Like the time my friend Chris from Winnebago had a BRAIN TUMOR labeled Schizophrenia and he almost went to trial for several felonies until the Prosecutor ordered an MRI. Chris was doomed either way. They operated on his Tumor and dumped him on the floor of the County Jail to “recover”.
What if that Dr. found the Tumor 2 years earlier?
What if I wasn’t given Haldol for a Traumatic Brain Injury in 1990?
Report comment
You know, I forgot I knew someone, just from around, that also had had a brain injury when he was younger. He told me how he had water on the brain because of a traumatic brain injury. He had himself tried to tell a judge at one point, but that was just dismissed as crazy.
WELL!
It gets crazier, fortunately.
I had befriended this kid because I had seen him just walking around quite a bit, and was at first struck with his ability to see beauty around him, and I actually was concerned, NOT because he saw beauty, but because….
you know
“society”
He was supposed to be all wired up and not notice anything but whether he’s fitting into the mold, the pattern, the round the clock machinery… everything, and he wasn’t, he was completely in his own world seeing gentle innocent beauty.
As I got to know him… and he had been put in the mental health system by his mother a nurse, who I think was in the habit of “partying,” and such as well.
But I remember that at one point, I sat with this kid at the soup kitchen, and noticed that he wasn’t there, sort of. I’ve really quite faithfully studied spiritual healing, if that has anything to do with it. But what happened is that I saw what I now can describe as the free energy that comes from time as it resonates with itself. If life is to have any meaning at all, then the understanding of that will allow whatever gives it meaning to repeat itself till it’s understood, till it’s experienced, till the beauty of life has been felt and is there, where it came from beyond linear time. And that means infinite energy, and no resource being depleted. Or you might just call it a miracle, and I knew that perhaps he didn’t have that traumatic brain injury anymore. That part of supposedly linear time had been dissolved. I even mentioned that I thought that injury was gone, and he said: “I know….” in a very meek tone, like usually only a child can have: given that he wasn’t making too much of it, and that it would go with other poetry, with other realities of life’s play that IS truly play and that again usually only a child has the riches to experience…
I had then actually tried to get him secure housing, and had found that, but then he had found something cheaper trading with someone else, and managed to mess that up, I think because he ended up doing drugs. Which he had gotten used to, and had been raised in. He was homeless for awhile, but then I think went back into the mental health system because he would get housing taken care of, that way. Or he just fell back into it.
That’s a whole other thing isn’t it AGAIN!
Don’t challenge their ideas and they’ll give you housing, if you go along and say that you’re ill.
Up above it’s talked about as well….
There CERTAINLY are a lot of homeless people that simply don’t have a home, and are too honest to be interested in bankrupting the US government going on the 500 to 1000 dollars of drugs they are supposed to be on, in order to then be seen as disabled, to then get shelter as well. And when that caught on, how many other people go for it, and before you know it half of the US population is zombie.
Or are they already!?
Wow what a plan Mr. Torrey. Put homeless people all on psychiatric medications and they’re all functional.
It’s of course not reality based to simply give them homes, and have an economy (perhaps not so much run by the drug companies and their mob friends) that they (the “homeless” people) could be part of…..
That’s of course
um
SCHIZOPHRENIC!
Now everybody howl…..
Report comment
All of us can learn to hold space for someone in an altered state of conciousness until their needs are known and can be addressed. Most professionals and family members are in the grips of fear. Their instinct is to round up the individual who is at the center of concern like a wild horse and contain it and sit on it until it is broken.
If professionals and family members could suspend their fear long enough to cultivate curiosity-they might stop being blinded by their fear and observe subtleties and clues beneath the surface of a persons appearance and outward behavior.
Somewhere–n someone’s odd behavior—even in the throes of a crisis–lies a Rosetta Stone for resolving the situation. So many visits to the ER, resulting in harmful involuntary commitment could be avoided if individuals and families had access to other, better options.
Mutuality and mutual trust are critical for communication. Involuntary commitment destroys both.
My daughter at times cannot comprhend or speak in English-her birth language. This became more pronounced after a period of catatonia followed by ten years of institutionalization. Her inability to communicate is trauma based and complicated by years of forced drugging. Drug induced dissociation, depersonalization, as well as drug induced cognitive deficits that can mimic aphasia, dementia, etc. are episodic and dynamic–not a static. While inconvenient-it is rarely dangerous and certainly non-violent.
Symbolism and non verbal communication can fill the gap when spoken language doesn’t work. Ironically- so-called professionals by training are not aware of other forms of communication other than spoken language. It is tragic that psychiatrists, in their science based training, (or pseudo science based) are starved of the very symbols that would help them them communicate with people who navigate the margins of human experience–the humanities, comparative religion, philosophy, visual arts, anthropology–this is the ocean of human experience in which our children are drifting without grounding or guidance.
Involuntary commitment teaches our children nothing except base obedience in the same way that animals are domesticated. We can condition people to conform to rules of daily conduct through involuntary commitment-but we cant teach them to communicate what their desires are–how they view the world-and how to find their innermost purpose with the base language of force
Report comment
Madmom, your comments are beautifully written and more insightful than anything I have read about communicating with people who are not neurotypical. I’d love to communicate with you about your experiences with your daughter. You can reach me through http://andrewsvoice.org/
Report comment
What is not neurotypical? True science would already point out that a true cause of chemical imbalance is psychiatric drugging. That it’s caused by a disease remains alleged, and not proven conclusively, while psychiatric drugging has conclusively proven to cause chemical imbalance.
Report comment
That is very well said. Unless someone has an identifiable neurological disease that one can accurately test for, whatever people do is “neurotypical.” Genetic diversity is the key to species survival. We need all different kinds of people, and the sooner we learn to value what gifts everyone brings to the table, the healthier we’ll be as a society. But I’m not holding my breath on that one…
Report comment
My point was that they now use the term “neurodivergent,” (or “not neurotypical”) as catch phrases for disorders that have not conclusively proven to be biological, that do better when NOT treated as biological disorders, and that when they are treated as biological disorders are treated with agents that CAUSE biological disorder, while the belief that the disease itself is biological in order is really only alleged.
to start making references to neuro-typical, atypical, not typical, divergent isn’t scientific.
And to make references to neurodivergence, as if it’s promoting diversity, while it’s suppressing societal diversity, emotional diversity, cultural diversity, experiential diversity, along with trauma, and diversity of insight; that’s really quite profoundly misleading, and if not an all out con job, shows clear signs of lack of interest in diversity itself and an inability to look beyond accepted ideology.
To behave as if one is showing compassion against stigma by mislabeling something in order to promote “treatments” that cause what they say they are treating, this is not scientific at all.
And to then have caused an epidemic and say there needs to be more treatment, and have such legal processes as Kendra’s law which force treat someone for an alleged disease, while causing the phenomenon that’s alleged, which then isn’t alleged anymore but caused by treatment but denied…….
https://en.wikipedia.org/wiki/Neurodiversity
And that kind of pretentiousness is promoted as kindness.
Suppressing what’s labeled as symptoms for a period of time to have them re-emerge more than they occur when not suppressed, this is NOT healing.
Suppressing dissent, when would it be looked at intelligently it becomes clear there’s something very valid going on, this doesn’t magically erase what the initial issue was either. No matter how uncomfortable people might get. And no matter how much they’d have to let go of thinking they are showing kindness in suppression, whether it’s chemical, emotional, political, psychological or what have you.
Report comment
Dear Andrew’s mom. I would be happy to reach out to you through your website. Thank you for the link.
Report comment
I am happy to support this website for quality articles like this one. Thanks!!!!
Report comment
We need to have preparations in place, cards people can carry which refuse any and all mental health treatment, phone numbers to be called and websites to be visited.
Strong warnings will be given, as activists and attorney’s go into immediate action.
Report comment
Thanks for this compelling report Robert and Michael. I hope it finds its way into mainstream news. These “AOT” orders are slapped on people the same way psychiatry slaps labels on people – without knowing, caring or understanding what is really behind someone’s circumstances or distress. And these orders are being unjustly slapped on people that don’t even meet the criteria! All so typical of psychiatry and another example of the sheer stupidity of the “one size fits all” and ‘cookie-cutter’ approach of psychiatry.
Report comment
Are you also against
Pro-Life BS and “Suicide Prevention”
Forced Living Extremism
Report comment
So we are dealing with neither human beings nor citizens here but with “the seriously mentally ill”. Good to know. This is where I have to insist that human rights are always preferable to “mental patient rights”. They are, as you might well imagine, also preferable to ‘slave rights’.
Report comment
I’m sorry but I have to strongly disagree with the first sentence of this article. There was no question that Andrew was in a disturbed state!?
Sorry, but to me, all he was doing was being naked, howling at the moon, and when police approached he decided not act intimidated. It later says he was charged with resisting arrest, but all the evidence given that is really reliable is that he was tasered, which easily only means that the police felt he was a danger, and didn’t even try communicating to him with any empathy, interpreting any behavior of his as a danger.
To start an article with such a statement, already excuses the whole out of balance pretension of the society Andrew was in, and shows it isn’t so much about being human anymore, but not giving the wrong impression to go with an image of being “not disturbed.”
If someone wants to be naked, and clearly non violent, and howl at the moon, what’s really the problem; and then after being violently assaulted with a taser, respond the way Andrew did, I don’t know where this isn’t quite understandable. I think there’s no question that he was being disturbed. Later on, when he says to a psychiatrist that he’d like to tell someone he’s a werewolf just to see how they would act, that’s seen as a sign of a disease.
And I find the whole hoard of behaviors NOT seen as a sign of being disturbed that are EVER DAY overlooked without question by just about EVERYONE in society, in comparison to someone howling at the moon, quite profound.
To begin with that when someone is naked howling at the moon that others IMMEDIATELY respond with the kind of alarm they do, I find that such people are quite disturbed. Most loud music coming from someone’s car, or the kind of riled up banter between people trying to act “cool,” I might also find more “disturbing,” and the decibel level and the intrusion into the sounds of nature that otherwise would be allowed to resonate probably IS more disturbing to the environment.
I think it’s proof of a disturbed society, with the whole array of behaviors allowed people when they don’t get naked and howl at the moon. The whole decimation of nature, the ruin of lives for no other reason allowed by people coming up with strategies to make it in the economic system that would do more good for the planet IF they got naked and howled at the moon! And the “legal: system enforces that, and someone howling at the moon is seen as such a danger that they get tasered.
It would really be amazing if society would simply get over itself, the very thought that its member are decent because they don’t behave in the “disturbed” way Andrew did.
Someone naked howling at the moon gets tasered, then force drugged till he can’t stand it anymore and takes his life. In contrast someone ruining the planet through exploitation of its resources, but maintaining a hoard of $$$$$$$$$$$ in the bank, and maintaining the right to do that, and promoting that as having made it in life, they are given free reign. Or if you’re a bit more into having a different more moral image, like Bette Midler, you can blame all the violence largely illicited by the drugs falsely advertised and quite often forced on people being caused by de-institutionilization rather than the clear result, because then you get into the bandwagon of the other political party, both of them sustaining each other as member of the business party, the better of the two offering perhaps 5 to 10 percent of the change needed while any political party offering more than 50 percent of the change needed is blown away by the coalition.
Is there something wrong with me finding this disturbing?
Report comment
In Wisconsin:
Confrontation or even raising your voice is a punishable crime. (Disturbing the Peace)
Being wasted on psych meds in Public is a crime (Disorderly Conduct)
ANY MOVEMENT or vocalization of needs or pain is a crime. (Resisting Arrest)
Tazing, beating, starving, someone or letting them die in a cell PERFECTLY O.K.
Taking your Children and giving them to pedophiles because you smoke (Illegally) weed for PTSD-PERFECTLY O.K.
The commitment and revocation hearings are Kangaroo Court.
To leave the State Hospitals (Winnebago and Mendota) you need the approval of an “Independent Evaluator” A forensic Psychiatrist who looks at your chart and talks to you for 10 minutes.
Luckily for me the Judge over-ruled the Sanctimonious (insert your own expletive) every time.
Theses evaluators want you to stay forever.
Where the “Criminal Justice” and “Mental Health” systems intersect there is NO HUMANITY or REASON.
The Judges are totally ignorant to the reality of Psychiatric Neurotoxins and the B.S. Labels.
They consider Psychiatry as a valid “practice”.
I strongly believe if the truth were known about the DSM and “Medications” our fight would be strictly HUMAN, CIVIL and CONSTITUTIONAL rights.
The Legislation in Wisconsin needs to change (Chapter 51 and Chapter 971.17)
I’m not sure what to do about all of the non-caring sadistic people who need a Job torturing vulnerable people? Soylent Green? Protein Bars?
MANY benefit from all the suffering we do.
Report comment
Neither justice nor mercy from the Mental Illness System that promises both.
Report comment
“all he was doing was being naked, howling at the moon” If someone wants to be naked, and clearly non violent, and howl at the moon, what’s really the problem?
The location.
I bet people who scream and get naked want to do it around people to get a reaction from them, otherwise they should have gone away from civilization first.
Those with the gold make the rules. Money ( a collective fiction/insanity) is not going to disappear any time soon. Humans still have plenty of food and water. https://en.wikipedia.org/wiki/Plagues_of_Egypt got to come back to teach man some humility.
Report comment
I’m sure he was suffering. But there are laws against public nudity for a reason.
If some women or children had run across a naked man screaming at the moon in twilight they would also have suffered.
Not sure what to do in cases like that. He probably would fare better being tried for the crime of indecent exposure by a real court for human beings.
Report comment
Let me count the ways, of suffering
He’s suffering
They are suffering because he’s naked
And you’re suffering if there isn’t a court that makes people suffer for being naked.
Suddenly all of Africa or anywhere else walking around like they were born are all suffering, and need to be civilized for indecency
I think if he was left alone there would have been less suffering, because then he wouldn’t be disturbed, and there wouldn’t need to be an excuse for it (because others are supposedly suffering), and no one has to qualify their suffering when others aren’t
This is just amazing what people don’t come up with acting like it’s their responsibility to do something about something (the way we were born without clothes, and then to cry out in order to breath)
get over yourself
Report comment
Humans are animals. Only cultural forces – driven by religious and patriarchal oppression – teach us that our naked bodies are shameful and should be covered for reasons other than warmth. Men can expose their breasts regardless of how much breast tissue they are endowed with but women are barred by law from doing so in most places in America, and are even still being thrown out of public places for breastfeeding. There is no basis for this other than cultural mandates that bodies be commoditized for the sale of products and the control of the population. This commoditization of our bodies actually feeds the shame and secrecy that child sexual abuse thrives on.
Any trauma that might occur to a child from seeing a naked man howling at the moon is going to be augmented by the response of the adults around. If the adults respond nonchalantly, calmly removing the kid from the scene and then allowing a safe dialogue about what the child witnessed, the kid does not learn to fear such aberrant behavior. But if the adult responds with shock, incredulity and horror, the child learns that such behavior is to be feared and controlled. In any case, absent other harmful behaviors in the environment, there’s nothing especially traumatizing to children about seeing nonsexualized naked bodies. As with everything else, these responses are cultural and socialized into us.
Report comment
We must organize and look for places that we can fight back.
Very good points FrankB.
Report comment
I have a friend who works as a speech pathologist. Largely with those suffering from TBI.
She told me 90% of those who suffer extensive brain damage become far nastier and harder to live with. (I believe individual choice plays a role too but we’re discussing generalities.) When people are drunk or high on heroine or meth they don’t turn from evil killers to sweet, gentle little lambs.
Yet shrinks like Torrey claim that the way to prevent crime is to force everyone his profession has written off as hopeless and subhuman to partake of “treatments” consisting of—traumatic brain injury and mind altering drugs. Despicable. And–even those who choose to take those drugs he lies about suffer from the public defamation. Muzzled or not, no one wants to hang with Hannibal Lector
Lying all the time, zero empathy for those harmed, a profound hubris setting himself over those he has branded subhuman–these are all personality traits Torrey has displayed. Why have we made men like him the moral guardians of our society?
Report comment
BRAINS!!!! I have Jars to Fill…..donations anyone?
“Killing is my Business and Business is GOOD!”
Report comment
Back off Torrey.
I’ll sick my cat on you. Bwahahaha! 😀
Report comment
And there is actually no evidence that any psychiatric drug will stop a person from being violent.
Report comment
Bingo.
Just think. Destruction of higher reasoning functions does not lead to a reformed moral character.
Report comment
How odd! Who would have guessed?
Report comment
And how much evidence is there that psychiatric drugs do the opposite than stopping a person from being violent?
Report comment
Pshaw!
The “good doctor” Torrey says! Who are you mere mortal human to question this self appointed deity?
Not like psychiatrists would ever knowingly deceive patients or the public after all. 😛 Psychiatry is the only medical specialty that publicly maligns the character of its patients on national television.
Torrey’s sole goal in appearing on TV is the CREATION of stigma against those his profession has damaged. Ending it is the last thing his ilk would want.
Far worse than Farid Fata. He lied to patients, crippled and killed them. But at least he didn’t gas light them and go on TV accusing them of murders never committed and urge the public to segregate and imprison them.
Seems Torrey knows his BS can no longer be hidden. Too obvious his poisons are not magic cure-alls. So he is now running around urging to have all the “SMI” locked up forever. Seriously.
Wish we had surveys on how many folks labeled “SMI” started out normal and rational till psychiatry got its claws on them.
Report comment
Heh, um, must you?
In order to expose really quite simple truths, that psychiatric medications cause chemical imbalance rather than treat them, that those chemical imbalances cause the spike in mental illness that’s current, along with a spike in violence, and then also loss of life expectancy, severe side effect, severe addiction to the “medications;” in order to expose this it’s really quite simple to share statistics and scientific evidence.
But Torrey actually believes, and has been brainwashed to, that it’s the lack of medications, and that when things get worse, rather than it’s the medications causing the spike, that it’s the propaganda of the drug companies putting profits before health that’s the truth.
I wouldn’t be surprised if Torrey is on ADHD medications. I don’t know, he to me really does have difficulty concentrating on what’s really put forth, and resorts to programmed data, and ADHD medications would assist that. But I don’t know why he can’t see simple truths, I’m just putting forth a theory, and he looks to me like he has some stimulant going on.
To say that he’s making himself out to be a deity, to say that all psychiatrists willingly deceive the public, to say that Torrey’s single goal is to create stigma against those whose life he’s damaged, or that he’s knowingly gas lighting them, when he probably simply doesn’t have the syntax, the intelligence, the ability to look past the drug company propoganda; in many ways that’s a gift to the drug companies who than point out: “heh, look, all they can do is mud slinging.” And I don’t think it’s going to inspire Torrey to look closer at what he’s professing.
The poor man is highly brain washed, he actually believes he’s helping and that he can change the world, and actually believes a whole hoard of doctrines, that I can’t say isn’t normal for most people in society to have a collection of. MANY people believe that mental illness is a chemical imbalance, or genetic, and you aren’t going to convince them otherwise by throwing out remarks about psychiatrists or their instruments trying to make themselves out to be deity’s. As little as going back in history and trying to convince those believing if one doesn’t sacrifice an animal or a virgin or who knows what to the God’s the God’s won’t favor you. Those beliefs were incredibly ingrained, and you don’t change them by using hostile derogatory comparisons.
Robert Whitaker in his books also clearly points out how diagnosis such as ADHD, such as depression or such as anxiety (and I think all of us get depressed at times, get anxious or have difficulty concentrating on whatever); that those are normal phenomenon (concerning ADHD, the family often don’t really see a difference when a person is medicated, anti-anxiety medications are highly addictive as are anti-depressants, all of those having side effects that can cause psychosis, and other “symptoms” of a mental illness); but when you medicate those people, they are WAY more likely to later on have another diagnosis, and in comes the whole trend towards bipolar the last years, which many of them fell prey to, and which Allen Francis had to admit was highly exaggerated, at least at time he had to; that’s all clear evidence that normal people end up being diagnosed with a SMI, just because the MHS got a hold of them as commodities for their marketing schemes.
That evidence is there, but if in this site there’s the amount of chummy mud slinging, posts that those trying to cover up anyone finding out the truth can use to point out that we’re here all extremists, then Robert Whitaker’s patient highly articulate work ceases to be the help it could.
Report comment
K
Report comment
Heh, I don’t mean to sound like I’m chastising you, I know how immeasurably frustrating it is. And you have Parkinson’s symptoms from the “medications,” and tried to get a job, but collapsed, started crying, and had to quit.
I’d really suggest just watching Gene Egidio’s Videos
https://www.youtube.com/watch?v=g9edB02jWP0
https://www.youtube.com/watch?v=GSX-gUmxQ3M
He withstood a year of shock therapy as a 5 year old boy, and then had to be retaught how to be human, had to be toilet trained again. He was left so frail that he wasn’t supposed to do normal childhood things like play baseball. He could have died twice later on in life, but when his life supposedly fell apart, the stuff started happening again that psychiatry and the Catholic church had tried to suppress. And people just started healing in ways the medical profession wouldn’t say is possible, mostly. I’ve been watching the hands on healing parts of those videos every day, because to me it gives purpose to just being alive, also given I’m supposed to be disabled, dysfunctional. Well, then something that’s not supposed to be legit but changes people beyond what is supposed to be legit does, that starts giving me whole new insight.
Awhile ago, I had started watching a lot, and started seeing the same energy from a tree he saw when his life supposedly fell apart and healing then could start to happen to replace such “functionality.” And I started seeing auras (something else Gene was found crazy to have seen) to realize that like the double split experiments where it’s stated that something behaves like a particle because it’s observed, and otherwise it behaves like a wave pattern; that because I want to see the healing energy that’s there, it emerges (because I want to see it). And now, after a period of integration psychiatry would again say is crazy, I have shed some serious physical problems; one of them I wasn’t even thinking of getting rid of. I watch those videos every day now, even thought there’s still a weird part of my mind that acts like my life is supposed to be about something else, or that that’s just too weird. And yet every day they relax me, and make me feel at home here, and that’s when the physical problems dissolved as well. And I’m really learning to let go of old gripes, that although entirely logical and justified, were only keeping me bogged down. Part of me is trying to hold onto the old gripes, but when I watch Gene’s videos I feel differently, and see I can let go of them and things will change in a different more efficient way.
Try it anyhow. See if you like it.
Here’s other stuff, I looked into. Stuff to not let get to you, anyhow.
I’m sure that Torrey is also lying, although he thinks that’s necessary to save the world. He’s so intent on capturing someone’s consciousness, so stimulated thinking that he can convince someone of his produced ideology, that any concern they’d have he’d find some means to fill in the blank with more of his production. And there you have the converts he’s looking for. Propped up with adds from the drug companies. I can’t believe he actually was on Charlie Rose, who then purported that they knew that mental illness was a chemical imbalance (something the drug companies selling drugs to treat that ideology can’t conclusively prove, although one can conclusively prove that psychiatric medications cause chemical imbalance). And then it even was presented as truth here: https://charlierose.com/videos/25947
Someone actually tries to put forth that you can’t treat bipolar without medications. This, despite the evidence that it’s often a RESULT of medications for ADHD, depression, anxiety or who knows what (PTDS, being gay, living in the ghetto, being a victim in a war, being poor, being intelligent enough to see that society isn’t working but not being able to process that quite, being made paranoid about natural responses to trauma, being made discriminatory and thus not understanding the language of the subconscious that would otherwise help you); or the evidence that when NOT medicated people do better.
It’s just mind boggling how silly it all is, it’s really like a new fashion everyone falls for, except it’s ideology. People think they have to have a constructed mental answer, regardless of its truth.
And then you have:
https://charlierose.com/collections/3/clip/18615
and
https://charlierose.com/collections/3/clip/14403
and the whole things:
https://charlierose.com/collections/3
I’ve seen a few times when people were involuntarily committed, and I can’t say that it didn’t happen in any of them that there wasn’t a gross misrepresentation of what was going on, and in most of them downright lying.
Here’s something I found, with an excerpt quoted.
http://psychrights.org/Articles/SzaszonTorrey.pdf
The National Alliance for the Mentally Ill (NAMI), a group with
which Torrey is closely allied, also endorses “therapeutic prevari-
cation.” The following is an excerpt from a NAMI Web site:
Sometime, during the course of your loved one’s illness, you may
need the police. By preparing now, before you need help, you can
make the day you need help go much more smoothly. . . . It is often
difficult to get 911 to respond to your calls if you need someone to
come & take your [mentally ill] relation to a hospital emergency
room (ER). They may not believe that you really need help. And if
they do send the police, the police are often reluctant to take some-424
Psychiatric Fraud and Force
one for involuntary commitment. . . . When calling 911, the best way
to get quick action is to say, “Violent EDP,” or “Suicidal EDP.” EDP
stands for Emotionally Disturbed Person. This shows the operator
that you know what you’re talking about. Describe the danger very
specifically. “He’s a danger to himself” is not as good as “This morn-
ing my son said he was going to jump off the roof.” . . . Also, give past
history of violence. This is especially important if the person is not
acting up. . . . When the police come, they need compelling evidence
that the person is a danger to self or others before they can involun-
tarily take him or her to the ER for evaluation. . . . Realize that you &
the cops are at cross purposes. You want them to take someone to the
hospital. They don’t want to do it. . . . Say, “Officer, I understand your
reluctance. Let me spell out for you the problems & the danger. . . .
While AMI/FAMI [Alliance for the Mentally Ill / Friends and Advo-
cates of the Mentally Ill] is not suggesting you do this, the fact is that
some families have learned to “turn over the furniture” before calling
the police. . . . If the police see furniture disturbed, they will usually
conclude that the person is imminently dangerous. . . . THANK YOU
FOR YOUR SUPPORT WHICH MADE IT POSSIBLE FOR US TO
PROVIDE THIS INFORMATION TO THOSE WHO COULD BEN-
EFIT FROM IT. (Jaffe, 2000, italics added)
Report comment
Thank you Njinsky. 🙂 Actually the Parkinsonism is gone. Got off the drugs in time.
My big problem now is microscopic colitis linked to a wider auto-immune disorder. There is a lot of that in our society you’ll notice. Also terrible short term memory and other things linked to the CNS. My dad is begging me to get tested for Lymes though i think it’s not that.
The reason I said such harsh stuff about Torrey is because he strongly supports “medications” to prevent crimes or just odd behaviors on the one hand. But in a book called Mind Fixers by Anne Harrington he goes on record as saying the only real help for “schizophrenics” is institutionalization. Either his memory is failing or he is talking out of both sides of his mouth.
Report comment
We must be teaching survivors to defend themselves, and by using any means necessary.
Report comment
“Destruction of higher reasoning functions does not lead to a reformed moral character.”
But that is what the drugs are for, destruction of the higher reasoning functions, and also ECT and lobotomy.
And while the middle class family only turns to drugging when earlier efforts have failed, the central organizing purpose is to psychically scar and maim children in order to get them to accept the bogus ethic known as Self-Reliance.
And when such efforts at scaring and maiming fail, they have the state licensed thought enforcer, known as the psychotherapist, with their newer editions of the pedagogy manual, and with their new moral improvement version of the diagnosis manual.
Very few people can escape this, because most all whom they encounter will be collaborators.
But once we survivors stop talking and become Women and Men of Action, then everything will change.
Report comment
And we must never go along with anything which tries to legitimate Psychiatry or Psychotherapy because these might make people less violent.
Report comment
Hi Michael and Bob,
You’re completely right about the modern day dismal “Mental Health” outcomes.
I think it would be impossible to withdraw from Neuroleptic Medication without some means of dealing with “Withdrawal Syndrome”. I heard a lady yesterday describe in a 12 Step Fellowship, how she effectively deals with High Anxiety similar to the High Anxiety of Neuroleptic drug withdrawal.
12 Step Fellowship has no monopoly on successful substance withdrawal, but I notice people in these fellowships can get genuinely better very quickly and without (much) cost – as can people that attend the Hearing Voices Network.
Report comment
We can’t be talking about ~mental health~.
We have to be talking about eradicating forced treatment and holding the perpetrators accountable.
Report comment
Fiachra, a very good book:
https://www.amazon.ca/Alcoholics-Cult-Cure-Charles-Bufe/dp/0961328932
Report comment
The American Psychiatric Association is against AA too PacificDawn. They oppose it on the grounds of how unscientific it is. 😉
Report comment
Wow! Pot/kettle?
Report comment
AA is not only unscientific, it is a cult. It is religiosity. What is also unscientific is the idea that therapy or drugs can cure anyone of ~mental illness~, or that these things are desirable for any reason whatsoever.
If the issue here is people who are believed to be violent, well that is part of life. If someone has been marginalized, the we should be teaching them how to defend themselves, and teaching them when it is appropriate to use violence, and what the risks are, and teaching them how to use violence effectively.
Like what Foucault is telling us, the government use to use execution to keep people in line. But now it no longer needs to do this. It can keep people in line simply be refusing to grant them permission to die. And this is what the mental health system does, give people no chance of restoring their honor, so they really have no reason to live. They are just waiting for permission to die.
There is no scientific way to get people to stop drinking or using, they have to want to do it. If they want to do it, then they can. But mostly, they have to see some way that they can stand up and restore their honor.
But the mental health system and the recovery movement will deny them this. And it is no different with street drugs versus prescription drugs.
Report comment
I see I’m way late here. It’s ok though, as I think I’d rather opt out of a discussion which seems to take as a premise that there is a case for AOT. It’s sort of like talking about “the case against euthanasia,” or (yes) “the case against slavery.” To seriously argue about AOT as as opposed to, say, mocking it as a legitimate debate topic, in my view gives power to Orwellian “arguments” defending AOT.
Report comment
Some people believe that AOT is necessary. Most of the would be opponents of AOC try to appease its supporters, and they do this by denigrating those who are already targeted by the mental health system. They promote psychotherapy, recovery, life coaching, community and integrative approaches.
The never go with a hard line FU.
Report comment
I agree with oldhead. And I make no apologies for coming across as an absolute zero tolerance abolitionist. It is all in territory which can never be negotiable.
Report comment
Spectacular collection of facts, and an amazing tool to educate others! Thanks for all the work your doing, and Thanks for this article to speak truth to power, and to bring validation to those of us just trying to do our best!
Report comment
E. Fuller Torrey is a
Notorious Fraud , and Pro-Life
“Suicide Prevention” Extremist
Opposed to the Growing
Right To Die , Voluntary Death with Dignity Movement for Suffering Mentally ill and other Suffering people who want a Peaceful Exit
Psychiatry and the
Mental Health “system”
Makes Impossible Unreasonable Demands upon Suffering people
We can Never Forget that
“Suicide Prevention” is
Complete BS
Pro-Life BS Propaganda and Lies
Needs to be Debunked and Refuted with the Truth about the Often hideous ugly Nature of Life and Human Existence
Report comment
Ya but he is so fun to troll!
I still get real Job offers for him!
I had a Facebook but people would get irate when they found out it was satire.
You can now find me (Torry) on X (formerly twitter) @DSM5sucks
https://x.com/DSM5sucks
Where I bust out with “killing is my business and business is good”-Megadeth
I also complain about all of you ruining my business.
Report comment
Nijinsky in the comment of
July 22, 2019 at 5:22 pm
Mentioned the hideous term
“EDP” which many people, find VERY
Offensive, dehumanizing, degrading, derogatory,
Stigmatizing, labeling of people Suffering from Unbearable Mental illness
Countless people with Mental illness Hate to be referred to “an EDP” if they are having a Mental Health Crisis, who would like to be referred to as
“an EDP”
It is a Deeply Offensive Term ,
I read that New York City Abolished that term , words matter
Anyone see this article
https://nypost.com/2019/10/21/nypd-has-new-orders-for-dealing-with-mentally-ill-lose-the-lingo/
This article Explains that the term
“EDP” is Extremely Offensive
Report comment
I thought this was “Emergency Detention Patient”.
Report comment
In October 2019 an article from
nylpi.org mentions the hideous term “EDP” being abolished and says
“We’re happy about the language change eliminating the term “EDPs”, or “emotionally disturbed persons” from police vocabulary. We’ve never liked the labelling of people as “emotionally disturbed” because it puts more distance between the police and the people they serve, just like their guns do. All people are capable of going through emotional disturbance, but it shouldn’t define us, and we like to see the person, first. That’s why this matters.”
It is a Vital Part of Human Rights,
Civil Rights, Human Decency , and the
Rights of people with Mental illness that deeply offensive hideous degrading dehumanizing stigmatizing derogatory terms such as “EDP” are Abolished once and for All everywhere in America and Worldwide, Never to be used Again .
The New Term “Mental Health Call” is an improvement ,
For a person having a Mental Health Crisis
being referred to as “an EDP” isn’t helping the person’s Mental Health and sadly makes things worse
Some people with Mental illness have even said that for them being referred to as
“an EDP” is like being called a Racial Slur
Report comment
Let’s be Frank and honest , how can anyone
Not find the term “EDP” to be Extremely Offensive, Degrading, Dehumanizing, Demonizing,
Stigmatizing, Derogatory, Labeling of
Human Beings Suffering from Mental illness
It Ostracizes people suffering from
Mental illness ,
How can anyone NOT find the
Term “EDP” to be a hideous offensive term
How could anyone possibly like the
Term “EDP”
Report comment
Honestly, I agree with you, but “EDP” is in the end no worse than many of the other labels that are considered more “politically correct.” Labeling other people as a means of “understanding” them is always offensive.
Report comment
Steve McCrea , glad we see
eye to eye , that gravely offensive terms like “EDP” need to be Abolished Everywhere in America and Worldwide
It’s just Common Sense as well
It’s Not about being “woke” or
“Politically Correct” it’s about
Human Rights, Civil Rights,
Common Decency and Respecting the
Rights of people with Mental illness
Mental Health Activists and Advocates Need to Lobby, Petition and Take Out Lawsuits in America and Worldwide to make sure such terms are Abolished once and for All Forever , get
A-List Celebrities on our side
The term “EDP” and other Terms like it
Only Perpetuates Stigma .
The term “Mental Health Call” is an Improvement, for Example Police and
EMS , other Emergency Services responding to a person in Crisis, an Individual in Crisis as an
“MH call” for short
Report comment
Did you read the rest of my comment? You seem to have ignored it.
Report comment
Yes , I read it
Report comment
I am surprised not to hear your agreement about other labels besides “emotionally disturbed.”
Report comment
Steve , could you give examples of
other labels you are referring to ?
Report comment
Sure, “Bipolar disorder,” “ADHD,” “Major Depressive Disorder,” “Borderline Personality Disorder,” pretty much anything in the DSM is simply a made-up label for a condition that psychiatrists and others don’t actually have the slightest understanding of. These “diagnoses” are arrived at through subjective behavioral checklists that bear no scientific relationship to any bodily process, but are simply behaviors that we find annoying, unpleasant, or difficult to deal with. Not saying that a person labeled “schizophrenic” has nothing wrong with them or doesn’t need our help, but calling them “schizophrenic” provides no additional useful information and makes it easier to dismiss them as having no value or rights to autonomy.
There are several “diagnoses” where two people can have ZERO “symptoms” in common and yet both qualify for the label! The whole thing is a scam in my mind, and is far worse than the dangerous medications these labels are used to justify forcing on an unsuspecting public.
Report comment
Steve , in my old neighborhood
I knew someone with
Extremely severe Type I Bipolar Disorder
With Severe Manic , Mania episodes
It was upsetting for myself and other Neighbors to occasionally witness his
Severe Manic, Mania episodes
Sadly Mental Disorders,
Mental illnesses are Very Real,
The pain and Suffering caused by these conditions are Very Real
Report comment
You miss the point, by a long ways. I don’t think I can explain it to you.
Report comment
Steve, I’m willing to listen and learn
Report comment
OK, I’ll give it a try.
First off, I am the last to deny there is real SUFFERING out there. That is not in question. The question comes down to how one views and deals with this kind of “mental” suffering.
ALL of the labels in the DSM are voted on. They are not scientifically verifiable entities, they are the results of clinicians “agreeing” on a particular set of “criteria,” which is generally a very subjective list of behaviors or thoughts or emotions that have no necessary connection to one another or any kind of “illness.” So they have no more legitimacy than “Seriously Emotionally Disturbed,” which basically means the person (usually child) says or does things that we find upsetting, confusing or inconvenient as adults. Take “ADHD” for example – one of the criteria is “acts as if driven by a motor.” Another is “Incapable of staying seated in class.” Another is “squirms when seated or fidgets with hands/feet.” Another one is “Sidetracked by external or unimportant stimuli.” Can you see that these are all simply judgments passed by an adult on a kid’s behavior? How many kids squirm or fidget? Who gets to decide what are unimportant stimuli?
But kids get this label and they are looked down upon, told they have dysfunctional brains, told they CAN’T pay attention, given controlled substances (essentially speed-like drugs) to “control their impulses,” etc. Note that there is NO attempt to ascertain WHY the child might fidgit – bored, uncomfortable chairs, dealing with trauma at home (foster kids get labeled at a MUCH higher rate), simply not a good fit with the teacher’s style? NO, it is all blamed on the kid for being inconvenient.
A similar analysis can be done for any of the labels. Scientific studies show that attributing “mental health problems” to disorders of the brain increases “stigma” (a euphemistic way of saying bias and prejudice and discrimination) and that teachers and other adults treat these kids differently once they know they “have a disorder.” Consider alone the shame of being asked in public by a teacher or parent, “Did you take your meds today?” There is a lot of shaming involved in the process, and since it has no scientific basis, I consider this kind of label just as irrelevant and damaging as saying a person is “Seriously Emotionally Disturbed.” It’s a pejorative disguised as a “diagnosis”. Look at some of the writing about “Borderline Personality Disorder” to see just how bad the discrimination can get.
Again, not saying that these behaviors and emotions don’t exist, or that people don’t need help dealing with difficulties. But the DSM labels are pseudoscientific crap voted on in committees, totally lacking in any scientific validity. Even the one-time head of the NIMH admitted this was true.
So see if that makes sense to you.
Report comment