
“We must give major consideration to building new institutions,” President Trump declared at last month’s White House mental health summit, which was previously reported on by one of this article’s authors. “When I was growing up in Queens, in New York,” the President recalled, “we had a number of mental institutions. And I’d look and I’d see these big buildings. And all of a sudden, you go and you don’t see them anymore. And you say, ‘What happened to all of those beds? What happened to all of that work? And where are those people?’ And in many cases, those people are living on the streets.”
The President was referring to deinstitutionalization, the unofficial name of the federally funded discharge of the majority of long-stay state psychiatric hospital patients into community-based settings, which began in the 1960’s. News reports, quoting mental health professionals and advocates, regularly conclude that deinstitutionalization policies have resulted in an unreasonably large percentage of the country’s most seriously mentally ill becoming homeless and incarcerated
Before the President’s speech, celebrity physician Dr. Drew Pinsky kicked off the summit, entitled “Transforming Mental Health Treatment to Combat Homelessness, Violence, and Substance Abuse,” with a similarly negative assessment of deinstitutionalization. Pinsky said that the federally-funded process failed “because there were no resources and no plan.” Ex-patients, he opined, “were pouring out of the state hospitals by the hundreds of thousands. And they were going to nursing homes, prisons, the streets, and death. Those were the four potential outcomes.”
Pinsky also criticized the passage of patient civil rights laws in the 1960’s and 70’s that, he claimed, maintain a “silent genocide” in places like Los Angeles County, where three homeless people died a day last year. He bemoaned that only individuals in “the most severe states of psychosis” can be involuntarily committed to a psychiatric hospital. Even then, he noted, all a psychotic patient has to do to get discharged is name the closest place to get food and say they have a place to live. “That’s it,” he fumed, “out, no treatment, no assessment, no ability to determine what the probabilities of future success are with your care. You can just go.”
The former Celebrity Rehab host asserted that failed deinstitutionalization policies and civil rights laws are largely the result of the misguided machinations of 1950’s and 60’s government bureaucrats.
He also blamed the supposedly disastrous policies and laws on a counterculture that had “run amok.” For example, he said, there “was a growing consensus, which was bizarre, that institutions caused mental illness.”
Pinsky additionally alleged that Americans were misled by the 1962 novel One Flew Over The Cuckoo’s Nest.
Cuckoo’s Nest, about a fictional group of harmlessly eccentric psychiatric hospital patients battling tyrannical clinicians and staff, was adapted into a Broadway play and Oscar winning movie. In all three versions of the story, the nurses, doctors and orderlies use antipsychotic medication, shock treatment and lobotomy to cruelly control and punish the patients.
Quoting White House homelessness czar Robert Marbut, Pinsky said Americans incorrectly believed the Cuckoo’s Nest film was based on a true story. “Our country watched this and thought they were watching a documentary,” he seethed. “They were watching a fictionalized account, a movie, about an imaginary institution!”
Cuckoo’s Nest author Ken Kesey, who passed away in 2001, would likely have disputed Pinsky’s movie review.
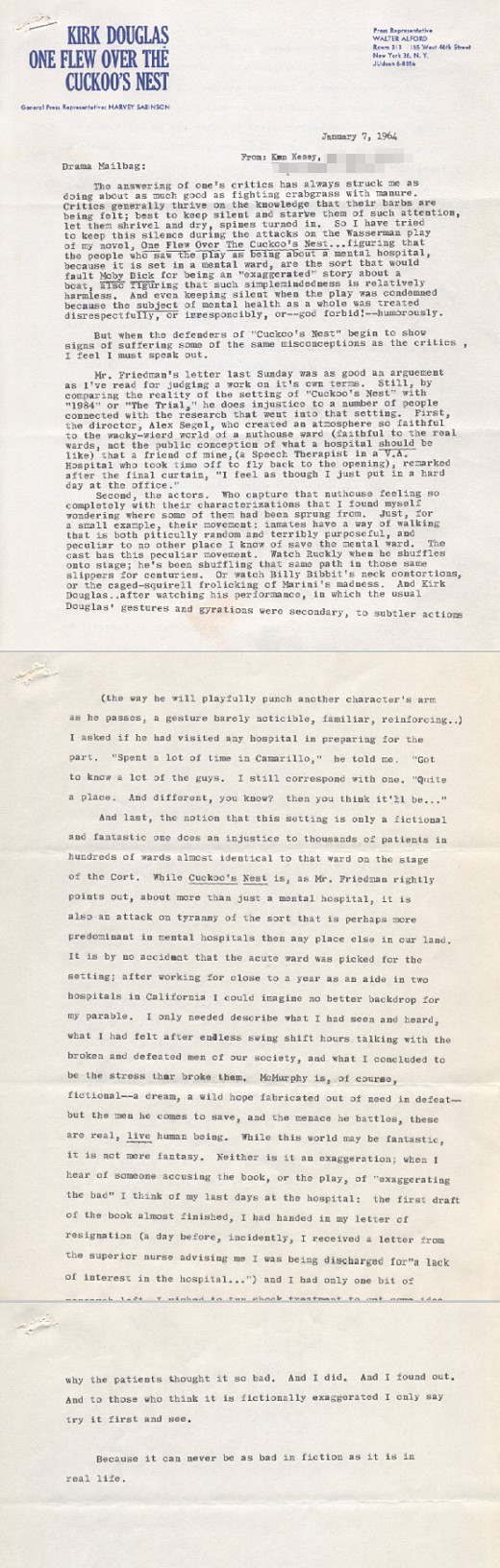
After The New York Times’ chief theater critic called the book’s 1963 Broadway adaptation a “shameless catch-all of farce and melodrama,” and two letters to the newspaper labeled the play a “fantasy” filled with “warped absurdities,” Kesey fired back, in a typewritten letter, that “the notion that this setting is only a fictional and fantastic one does an injustice to thousands of patients in hundreds of wards almost identical to that ward on the stage of the Cort (theater).” He argued that, while Cuckoo’s Nest is “about more than just a mental hospital, it is also an attack on tyranny of the sort that is perhaps more predominant in mental hospitals then(sic) any place else in our land.”
Kesey additionally told of how, on one of his last days at the hospital, he wanted to try shock treatment, “to get some idea why the patients thought it so bad.” After he “did” and “found out,” he advised critics who think Cuckoo’s Nest “is fictionally exaggerated” to “try it first and see.”
“Because,” he warned, “it can never be as bad in fiction as it is in real life.”
A few minutes after implying that Cuckoo’s Nest exaggerated the poor conditions inside of American psychiatric wards, Pinsky briefly backtracked. He conceded that “some of those hospitals were not in great condition” and that “there was grave concerns about what psychiatrists were doing. They were maniacs. They were taking ice picks out of their coat pockets (and) their shirtsleeves and doing lobotomies — their ‘great’ intervention.”
Pinsky disclosed that he had taken care of lobotomy patients decades after they had been operated on. “It was a mess,” he recalled. “This was not a good form of treatment. Yes, some of those hospitals were not in great condition. They were underfunded, understaffed. Not good.”
Nonetheless, the host of Dr. Drew Midday Live stressed that the “laws and systems” advocated for by government bureaucrats, civil rights attorneys and radical authors are no longer necessary. “The 60’s were almost 60 years ago,” he said. “In those 60 years, we have developed some better understanding of these brain conditions, some better ability to treat them, armies of professionals that are well-equipped to help us.”
The problem with current policies, he explained, is that Americans with “serious mental illness” are now “privileged by the law” to refuse medical treatment.
Contradicting Pinsky’s “privileged by the law” statement, news reports from the past 15 months indicate that, if anything, there needs to be more legal protections for Americans held against their will in psychiatric hospitals.
This past December, the Tampa Bay Times reported “glaring weaknesses” in Florida’s involuntary mental health system, ranging from “a lack of parental consent, to students being wrongly committed, to facilities that put students in harm’s way.” In the past seven years, the paper reported, “children have been taken from public schools in Tampa Bay more than 7,500 times and temporarily placed in mental health facilities. They often leave campus handcuffed in the back of police cruisers. Some are as young as 6.”
Also in December, ProPublica reported on a lawsuit that called a Chicago psychiatric facility a “‘hospital of horrors,’ where children as young as 7 were allegedly sexually abused and others were injected with sedatives and physically attacked — all while officials covered it up.” The lawsuit was preceded by ProPublica Illinois and Chicago Tribune investigations that revealed similarly disturbing allegations.
In October, The Seattle Times reported that “(Washington State’s) largest private psychiatric hospital, with 157 beds, routinely has held patients by claiming they wouldn’t be safe if released, only to be contradicted by government evaluators who find no grounds for committing them.” A hospital clinician said that “executives would yell at hospital staffers if they released patients whose insurance had authorized a longer stay.”
In September, another Tampa Bay Times report found that North Tampa Behavioral Health hospital “illegally cuts patients off from their families. Then it uses loopholes in the (involuntary commitment) statute to hold them longer than allowed, running up their bills while they are powerless to fight back.”
In May, the Cherry Hill Courier Post reported that “A whistleblower lawsuit claims New Jerseyans with intellectual or developmental disabilities were inappropriately diagnosed with mental illnesses, given psychotropic drugs and forced to stay in state psychiatric hospitals long after they were deemed stable enough to return to the community.”
In December 2018, The Wall Street Journal reported that more “than 100 psychiatric hospitals have remained fully accredited by the nation’s major hospital watchdog despite serious safety violations that include lapses linked to the death, abuse or sexual assault of patients.”
Also in December 2018, a Mad In America survey (conducted by one of this article’s co-authors) reported that 37% percent of 486 former psychiatric hospital patients “said they were physically abused (in the hospital) in some way.” Over half of the former patients described their hospitalizations as “traumatic.” A similar survey, conducted by an unaffiliated organization, of 63 former Washington and Oregon State patients revealed almost the exact same results.
Many other recent investigative reports, lawsuits, news stories, and blog posts have documented similar stories of the mistreatment, abuse and wrongful commitment of psychiatric patients.
Kesey’s criticism of shock treatment, today referred to as electroconvulsive therapy (ECT), also remains relevant. ECT is in use at over 500 American hospitals; has been linked to ”permanent brain dysfunction”; is the subject of a class action lawsuit; has been irresponsibly marketed and ineffectively regulated; and can still be administered over patients’ objections.
Likewise, laws passed since the publication of Cuckoo’s Nest to limit the unnecessary and punitive use of medication and restraint have had a limited impact. “In many states,” according to lawyer Susan Stefan in 2015, “patients have the legal right to refuse treatment, and there are relatively strict legal limitations on the use of restraint but neither of these are understood to limit either shows of force or threats to rescind privileges.”
For example, a 2015 City Limits investigation found that it was “standard procedure” for doctors in the psychiatric emergency room of New York City’s Bellevue Hospital to “order forced injections of psychiatric medication to sedate and overrule patients who refuse to have blood drawn during the hospital’s admission process.” One patient interviewed for the story said that, at Bellevue, “you just look at someone wrong and they shoot you up with (the antipsychotic) Haldol.”
Like his analyses of One Flew Over The Cuckoo’s Nest and civil rights laws, Pinsky’s assertion that deinstitutionalization resulted overwhelmingly in ex-patients “going to nursing homes, prisons, the streets, and death” requires additional context.

In his 1994 book The Mad Among Us: A History of the Care of America’s Mentally Ill, historian Gerald Grob concluded the “persistence of problems (related to deinstitutionalization) should not be permitted to conceal the more important fact that a large proportion of severely and persistently mentally ill persons have made a more or less successful transition to the expansion of federal disability and entitlement programs.” The misconception of the impact of deinstitutionalization, Grob noted, may be because “the media and the public are prone to focus on a subgroup of young adults or others who have a dual diagnosis of mental illness and substance abuse and who tend to be homeless.”
In a 1993 literature review titled The Homeless Mentally Ill: Myths and Realities, three researchers from London’s Maudsley psychiatric hospital similarly concluded that there are “significant methodological problems” with research suggesting deinstitutionalization policies caused a homeless crisis in the U.S. The authors added that American “homeless people whose only problem is the lack of affordable housing are being institutionalized on the basis of this erroneous assumption (that they are mentally ill).”
Recent research indicates deinstitutionalization policies and patient civil rights laws have minimal impact on the health and quality of life of the majority of homeless Americans. According to the National Alliance on Mental Illness (NAMI), 80% of homeless Americans do not have a serious mental illness. In Los Angeles County, where Pinsky said the weakness of involuntary commitment laws has caused a “silent genocide,” the Los Angeles Homeless Services Authority reported that 71% of people experiencing homelessness “do not report having a serious mental illness and/or substance use disorder.” Furthermore, the leading cause of death among homeless people in Los Angeles County (and across the country) is heart disease, an ailment that psychiatric hospital clinicians are not experts in treating (and which causes the death of people in the general population at the same rate). Likewise, antipsychotic medications — the class of drugs most likely to be given to involuntary psychiatric patients — “may increase the risk of heart disease in as little as a few months.”
Pinsky’s claim that deinstitutionalization policies and patient civil rights laws resulted in mental illness becoming “a feeder to the state’s jail and prison system” is also not supported by the available evidence. In “The Asylum Fallacy” chapter of her 2016 book Insane: America’s Criminal Treatment of Mental Illness, reporter Alysa Roth observed that “it’s far from clear that the same people who had been in the state hospitals later became the core of the jail and prison population with mental illness.” She cited research showing that “the residents of state psychiatric hospitals were largely elderly, female, and white. By contrast, people in jails and prisons are mostly young, male, and not white. Hospital patients overwhelmingly had a diagnosis of schizophrenia; people with mental illness in jails and prison show a range of diseases that is much closer to the range found in the general public.”
Pinsky’s pronouncement that certain civil rights protections for patients are unnecessary because “we have developed some better understanding of these brain conditions” is likewise belied by the facts.
In an exhaustive 2011 literature review of involuntary commitment criteria, Loyola University-Chicago Constitutional Law Professor Alexander Tsesis noted that “no techniques comparable to x-rays, CAT scans, or blood tests exist, so that (mental illness) diagnoses are entirely (based) on nonverifiable and controversial criteria.”
A study conducted by four University of Liverpool researchers in 2019 correspondingly found that the accepted criteria for diagnosing mental illness, in the UK and the U.S., is “scientifically meaningless.” Researcher Peter Kinderman remarked that mental illness diagnoses “frequently and uncritically reported as ‘real illnesses’ are in fact made on the basis of internally inconsistent, confused and contradictory patterns of largely arbitrary criteria.”
A recent Johns Hopkins University study of 54 patients diagnosed with schizophrenia revealed the unreliability of psychiatric diagnostic criteria. After the patients received a second medical opinion of their initial assessment, 51% received a different diagnosis. The second opinion doctors determined that the patients actually had significantly less serious anxiety or mood disorders.
People of color and minorities are particularly vulnerable to getting misdiagnosed. Dr. Stephen Stralwski, a professor of psychiatry at the University of Texas at Austin, recently told the Adirondack Daily Enterprise that “African-Americans with severe depression are four to nine times more likely to be diagnosed with schizophrenia than white patients who present the same cluster of symptoms.”
The overdiagnosis of schizophrenia in African Americans may be why they “are overrepresented among persons subject to involuntary commitment and among persons admitted for inpatient psychiatric hospitalization,” as a 2009 analysis by two University of California-Berkeley professors found. In March, English researchers who conducted a meta-analysis of 2 million involuntary commitment cases across the globe similarly concluded that “black, Asian, minority ethnic and migrant groups are at a greater risk of psychiatric detention than are majority groups.”
Even Dr. Allen Frances, who helped tailor a large portion of the current psychiatric diagnostic criteria when he served as the Chairman of the DSM-IV Task Force, considers the diagnostic system horribly broken. In his 2013 book Saving Normal, Frances admitted that, despite their best efforts, the DSM-IV authors “failed to predict or prevent three new false epidemics of mental disorder in children — autism, attention deficit, and childhood bipolar disorder,” as well the “false epidemic” of adult bipolar disorder and “the overdiagnosis of several other disorders that have been puffed up by the drug companies.” He likewise confided to writer Gary Greenberg in 2010 that “there is no definition of a mental disorder. It’s bullshit. I mean, you just can’t define it.”
Doctors’ ability to determine if a patient meets the dangerousness criteria for involuntary commitment is also fundamentally flawed. In his review of civil commitment literature, Alexander Tsesis found that there is no “professionally accepted definition or definitive actuarial tools to make such a temporal prediction” about dangerousness. Moreover, Tsesis observed, “studies conducted at least since the 1970s have found that psychiatrists are no better at predicting future dangerousness than laymen.”
It may not be Pinsky’s fault that he overstated the ability of psychiatrists to accurately diagnose mental illness and assess dangerousness. To prepare his White House summit presentation, he told the audience that he relied “heavily” on Dr. E. Fuller Torrey’s 2013 book American Psychosis: How the Federal Government Destroyed the Mental Illness Treatment System. Torrey co-founded Treatment Advocacy Center (TAC), a nonprofit lobbying group that has “passed, improved or updated” 69 involuntary mental health treatment laws in 34 U.S. states since 1999. TAC regularly publishes research showing that, without psychiatric treatment, people diagnosed with serious mental illnesses like schizophrenia, bipolar disorder and major depression disproportionately become violent, homeless, drug addicted and/or gravely disabled.
Torrey and TAC also have a history of cherry-picking data — as the authors of this story have previously documented.
In 2014, Salon reported that Torrey relies on “that most modern of rhetorical tricks: the relentless and contextless deployment of bogus statistics” to advocate for “incarcerating the mentally ill without due process and forcing medicative treatment.” Torrey’s assertion that 10% of U.S. homicides are committed by untreated individuals with serious mental illness, the Salon reporters noted, “is based on sensational news reports and bad math, which he then repeats to a credulous media, like an ouroboros of fear-mongering and sloppy scholarship” (a media watchdog and patient advocate also called Torrey out on his homicide claim). Likewise, in 1997, without providing any citations, Torrey accused the “psychiatric survivors” advocacy community of causing the suicides and accidental deaths of “at least half-a-million persons who were severely psychiatrically ill.” Unsurprisingly, psychiatric survivors took offense.
Torrey is also the country’s most outspoken proponent of identifying and treating psychiatric anosognosia, a condition traditionally associated with neurological ailments like stroke, traumatic brain injury and dementia. On a video on TAC’s website, Torrey defines anosognosia as a “real neurological condition caused by the damage to the brain, most likely to the frontal and parietal lobes.” As a result of this brain damage, Torrey then says, people with anosognosia “can’t recognize that they are sick.” He concludes that “it’s very clear that about half the people with schizophrenia and roughly 40% of the people with bipolar disorder have some degree of anosognosia.” In 2010, Torrey lobbied successfully to insert anosognosia into the latest version of the Diagnostic and Statistical Manual of Mental Disorders (DSM), commonly referred to as the Bible of psychiatry.
In 2012, psychiatrist Sandra Steingard analyzed a summary of neurological studies on Torrey’s TAC website supposedly proving the existence of psychiatric anosognosia. In her analysis, titled Anosognosia: How Conjecture Becomes Medical “Fact,” Steingard observed that the differences in the brain scans of people with and without anosognosia “are subtle and do not clearly distinguish a person with ‘lack of awareness’ of psychotic symptoms from anyone else.” She concluded that the promotion of anosognosia as a real condition “confers a certain sophistication of understanding and knowledge that is not supported by the data.” An Indiana University Professor of Psychology similarly referred to the insertion of anosognosia into the DSM as an example of “some puzzling areas in which opinions are presented as fact.” He added that the debate surrounding the existence of anosognosia “should not be limited with premature claims of consensus.”
Despite a glaring lack of proof that anosognosia affects people with schizophrenia and bipolar disorder, Pinsky made the condition a central theme of his White House summit speech. He uttered the word “anosognosia” nine times, spoke exclusively about the condition for nearly three minutes and suggested it was the primary reason psychiatric patients’ civil rights need to be rolled back. “We protect that symptom from allowing us to get at the patient to prevent them from dying,” he said. “Drug addicts get anosognosia, (people with) manic psychosis (get) anosognosia, schizophrenics (get) anosognosia. It’s the same biology as in dementia, encephalopathy, and other brain conditions and yet we privilege it in the law, and people are dying.”
While there is a dearth of evidence substantiating Torrey and Pinsky’s psychiatric anosognosia theory, there are two robust studies linking involuntary commitment to an increased risk of suicide.
A 2019 study of 900 psychiatric American inpatients found that individuals who perceived coercion during their admission were “more likely to make a suicide attempt after being discharged,” even after controlling for suicidal ideation or self-harm at the time of admission.
A 2014 Danish study of 2,429 individuals in the year before they committed suicide came to an equally disturbing conclusion: The risk of dying by suicide increased exponentially for individuals who received psychiatric treatment in the preceding year, even after controlling for other risk factors. A 28-fold increase in completed suicide was associated with psychiatric emergency room admission and a 44-fold increase was associated with psychiatric hospital admission. The researchers editorialized that it is “entirely plausible that the stigma and trauma inherent in (particularly involuntary) psychiatric treatment might, in already vulnerable individuals, contribute to some suicides. We believe it is likely that a proportion of people who suicide during or after an admission to hospital do so because of factors inherent in that hospitalization.”
On the other hand, according to psychiatrists Dinah Miller and Anette Hanson, there “are no studies that prove that involuntary treatment prevents suicide.”
There may be a better way to treat Americans experiencing “severe states of psychosis,” as Pinsky called it, than involuntary treatment. In his 2012 book Anatomy of an Epidemic, Robert Whitaker told of the remarkable mental health care story happening in Finland’s western Lapland region.
For a long time, the region, which has a population of about 70,000, had one of the highest rates of schizophrenia in Europe. Then, beginning in 1969, the Finnish psychiatrist Yrjö Alanen introduced a new form of mental health treatment for psychotic patients, in which individuals were treated on a “case-specific” basis. “Some first-episode patients would need to be hospitalized, and others would not,” Whitaker observed. Interventions centered around “group family therapy — of a particularly collaborative type.” The region’s clinicians did not dictate the location and form of therapy; in fact, the patient’s home, rather than the hospital, was “the preferred place” for the first meeting with doctors. During those “open dialogue” therapy sessions, “everybody’s thoughts can become known.”
The result of this new type of treatment was that psychiatric hospitalization became much less necessary in western Lapland. Over a seventeen-year period, “not a single first-episode psychotic patient has ended up chronically hospitalized,” Whitaker reported. “Spending on psychiatric services in the region dropped 33 percent from the 1980s to the 1990s, and today the district’s per-capita services is the lowest among all health districts in Finland.” At the end of a two-year study in the early 2000’s, “84 percent of area patients had returned to work or school, and only 20 percent were taking antipsychotics.”
Today, Whitaker noted, “the long-term outcomes of psychotic patients in western Lapland are the best in the Western world, and this region now sees very few new cases of schizophrenia.”
The development of western Lapland’s groundbreaking mental health treatment program was due, in large part, to Yrjö Alanen’s belief that “the hallucinations and paranoid utterances of schizophrenics, when carefully parsed, told meaningful stories.”* Alanen thus instructed the region’s hospital psychiatrists, nurses and staff to “listen to the patients” and their stories.
Besides President Trump and Dr. Drew Pinsky, seventeen administration officials, politicians, mental health advocates and public officials spoke at the December 19 White House mental health summit.
None of the summit participants were described as former psychiatric hospital patients.
This fact was pointed out by disabled healthcare advocate Kendally Brown, who tweeted afterwards that the summit “privileged the voices of family members, caretakers, doctors….everyone BUT the disability community.”
When those ideas involve the input of ACTUAL DISABLED PEOPLE sitting at the table. But you just participated in a White House charade that privileged the voices of family members, caretakers, doctors….everyone BUT the disability community. https://t.co/Tgh8Z9zkA7
— Kendall Youens (@kendallybrown) December 27, 2019
Compounding the lack of participation of former and current patients, a major theme of the summit was that Americans diagnosed with “serious mental illness,” because of a lack of insight supposedly caused by psychiatric anosognosia, should not be able to make their own treatment decisions.
In other words, anyone watching or reading about the White House mental health summit was implicitly and explicitly instructed not to listen to the patients.
The consequences of ignoring the insights of psychiatric hospital patients was documented by psychiatrists Dinah Miller and Annette Hanson in their 2016 book Committed: The Battle Over Involuntary Psychiatric Care. The first chapter of Committed is about the involuntary hospitalization of a woman named Eleanor, who recalled her interactions with unempathetic hospital staff:
I would rather die than go in again. I am not depressed, and my psychiatrist considers me normal, but I can’t live through that again. The staff was abusive, demeaning, and dismissive. I felt in fear for my life. Any lack of cooperation was met with physical and chemical punishment.
While seeking out stories of other former psychiatric patients, the authors found that “there were many people who wanted to discuss how they’d been injured by involuntary psychiatric hospitalization.” Conversely, they noted, it was “much harder to find someone who believed that he or she had been helped by (involuntary hospitalization). An online request for positive stories was answered by only four patients, two of whom were in Australia and South Africa.”
Miller and Hanson added that there “are organizations composed of people who assert they have been injured by psychiatric treatments, of civil rights activists who strive to protect the rights of those with mental illness, and of parents who long to get much-needed help for their children—even if it means forcing that care.”
“Yet,” the psychiatrists observed, “there is no organization of patients who say they were helped by involuntary care and strive to make it available for others.”
* * *
*Alanen’s belief that “hallucinations and paranoid utterances” tell “meaningful stories” is supported by the 2019 Johns Hopkins study that found that “when someone reports ‘hearing voices’ it may be a general statement of distress rather than the literal experience of hearing a voice.”














#kirkdouglas
Report comment
After deinstitutionalization came Mental Health Care Centers. Have people just forgotten the mentally ill? I would say mostly yes!
There is no one watching what happens to the mentally ill. There is no attempt to survey or follow up with clients over the long haul to see if they are better or worse. How would anyone know?
Be certain that it is “family” that is hindered with this burden and it’s not possible for the most part. It’s complicated.
I think that professionals are awfully imaginative about their conclusions. Too many times so!
Report comment
Good Article,
“…Researcher Peter Kinderman remarked that mental illness diagnoses “frequently and uncritically reported as ‘real illnesses’ are in fact made on the basis of internally inconsistent, confused and contradictory patterns of largely arbitrary criteria.”..”
The only requirement for membership to Alcoholics Anonymous is a desire to stop drinking!
Report comment
“….And you say, ‘What happened to all of those beds? What happened to all of that work? And where are those people?’ And in many cases, those people are living on the streets.”…”
“..What happened to all of that work? ..” sounds a bit like locking people up in institutions could provide a living for other people!
And, a person doesn’t have to be “mentally ill” to be “homeless”.
Report comment
Yep. All those people on the streets now in 2020 were released back in the 1960’s.
Real math folks.
Report comment
They must all be pretty freakin’ old!
Report comment
Lol was thinkin that too.
And of course, we have to look around to see what can provide jobs for people, even if it means subduing others.
It is easy to convert a peaceable man to commit murder if he is presented with arguments appealing to something he is passionate about, or if he does not have the ability to think things through.
Besides, many shrinks are busy talking about the leaders as MI, because a shrink can basically see MI in everyone, except in himself.
The very best place to hide as a personality is among peers, or simply keeping one’s mouth shut.
Report comment
In Western Europe what ‘disadvantaged’ people might expect (and receive), is help with decent housing but not incarceration in secure buildings.
Report comment
Solution to Homelessness in Finland
https://www.rte.ie/news/world/2020/0124/1110675-homeless-finland/
Without Punishment!
Report comment
why?
Report comment
The deaths are due to psychiatric treatment.
Many deaths.
No use arguing with monsters.
Report comment
Make the monster an absolute monarch. He promises to save the kingdom if they feed him fresh meat every day. Cure the overpopulation problem.
Report comment
monsters# y?
Report comment
Why not just learn from the experience of England?!
Report comment
Thank you for reporting on the fact that “President Trump and Dr. Drew Got it Wrong on Deinstitutionalization.” It’s a shame they’re so misinformed, or as the psychiatrists would say, “delusional,” and suffering from “psychiatric anosognosia.” Or, at least, that’s what the psychiatrists would say, if President Trump and Dr. Drew spoke out against the systemic, psychiatric harm of millions.
I know from personal experience that the Illinois’ DCFS and medical systems are completely corrupted. “Power tends to corrupt, and absolute power corrupts absolutely.” They were given too much power, long, long ago. One of my former force treating doctors was finally convicted by the FBI of massive in scale Medicaid/Medicare fraud, because he’d been medically unnecessarily harming unknown numbers of patients.
And, of course, what were the sins of those doctors? “A hospital clinician said that ‘executives would yell at hospital staffers if they released patients whose insurance had authorized a longer stay.’” I had to get rid of my “good insurance,” in order to escape psychiatry, apparently. Not that I did it intentionally, originally.
But definitely, if you have good insurance, or Medicaid, or Medicare. You’re apparently a target of the greed only inspired psychiatrists, and even many of the mainstream doctors.
“For the love of money is the root of all evil: which while some coveted after, they have erred from the faith, and pierced themselves through with many sorrows.” Many of our doctors have apparently largely lost their way, due to the insane greed of their industry. Great article pointing out the truth, thank you.
Report comment
Assuming–for the sake of argument–psychiatrists do know more about human brains now…that does NOT guarantee they will refrain from abuse. By that logic all Josef Mengele needed were more lessons in human anatomy. 😛
The idea that giving anyone absolute power with no repercussions for anyone they harm somehow benefits those at their mercy is ludicrous.
Report comment
And these guys are the alleged “Thought Leaders” of Big Time Psychiatry? Are we sure they aren’t space aliens seeking to turn the entire population into hapless zombies?
Report comment
Maybe the word “thought” doesn’t really apply here. Maybe “Delusional greedy fantasy leaders?”
Report comment
I’d rather keep my “civil rights” (and human rights) intact over any “mental condition” supposedly cancelling them out, or superseding them, Dr. Pinsky, all “anosognosia” or “illness denial” aside. Thank you anyway.
Great article. Keep up the good work.
We need to rebuild our movement, and the way we to do that is by fighting institutionalization, not by caving into it. Thank you for doing your part.
Report comment
Content moderators are being asked to sign forms stating they understand the job could cause post-traumatic stress disorder (PTSD), according to reports.
“I understand the content I will be reviewing may be disturbing. It is possible that reviewing such content may impact my mental health, and it could even lead to post-traumatic stress disorder (PTSD),” “the statement read”
https://www.bbc.co.uk/news/technology-51245616
Report comment
Don’t you mean flash forwards?
Report comment
Coronavirus is a very effective means of social control: note that it ‘coincides’ with this luna new year travel and first emerging cases seen in France (mass social unrest) and Hong Kong (mass social unrest) Probably UK (brexit/extinction rebellion unrest) by the time you read this.
Ofcourse the experts are on hand –
“Leading US health experts predicted coronavirus could kill 65million people in a year – in chilling warning ”
Wait for the pharma vaccination break through and possible enforced vacination.
Report comment
Can you say disease mongering by our medical/pharmaceutical industrial complex? Perhaps just like they did with “mad cow disease,” in 2009? Only time will tell.
Report comment
Anasognosia – to be ignorant or too stupid to recognise the god (doctor) you stand before. All efforts will be made to bring you too your knees and worship those who have your best interests at heart, and minus any human or civil rights to defend yourself you can be subjected to some ‘treatments’ that seem to do precisely this. Every once in a while they come across a Bilal ibn Rabah (a.s.), but put him out in the sun with a boulder on his chest and surely eventually he will come round to our way of thinking? Statistics show it’s a highly effective treatment.
Or he will die. An unintended negative outcome
Given what is written in the above article, I think there is a case to answer as to who it is that is suffering from being ignorant of the facts.
Report comment
I think what I fail to understand about this issue is: if the reason “mentally ill” folks are on the streets is because there was never sufficient funding for community resources, why isn’t there a push to FUND THAT? Why would the leaders just throw up their hands and say well, we didn’t fund the community resources disabled folks need so let’s just lock em up again? It’s not even remotely cost effective to warehouse people for decades upon decades. Supported housing, supported employment, teaching folks how to eat right and making sure they have access to healthy food and good healthcare is all combined FAR cheaper than building new asylums.
Could it be that our Supreme Racist Slumlord in Chief and his room of white male supporters really just wants to get the poor black and Latino folk out of sight and out of mind at whatever the cost? They can’t just throw em in prison anymore so let’s bring back the asylums.
The good news is that the ways these games are playing out among racial and class lines makes it easier to fight back. It’s makes it very clear what’s actually going on underneath the rhetoric.
https://www.nbcnews.com/news/amp/ncna1123156
2016’s The Rent Is Too Damn High Party would be a good org to consult about what’s driving homelessness.
Medicare For All would also stop people losing their life savings to pay for medical bills. (Not that Medicare isn’t driving a lot of other problems, too, the way it’s been mismanaged.)
The real problem at its base is that a capitalist society run for profit is inherently antisocial. We are trained to compete instead of cooperate from birth. We are taught to avert our eyes and walk on by when we see others suffering. After all, we worked for what we have, so why shouldn’t they have to also? We will not truly move beyond to real solutions until we realize we are all in this together and we are all better off when we are all better off.
Report comment
Thank you for your well-researched and informative article.
I don’t think Trump and company got it wrong. They don’t care about right and wrong. They care about having power over others. They deliberately cast non-conformists and the mentally distressed as dangerous, immigrants as criminals, women seeking abortion as irresponsible, and Black people as bestial in order to justify exerting more control over people’s lives, especially those who have the least to lose by rebelling against them.
Experience shows that challenging “misconceptions” does not increase our power or decrease theirs. We need to challenge their right to rule.
Report comment
I have a question for Michael and Leah.
According to NAMI (not an anti psychiatry organization) only 20% of the homeless are supposed to be “mentally ill.” That still is a significant minority.
Are any of them undergoing AOT while homeless? This is an important question to ask for sites that want to get at the truth.
I got angry at “Dr.” Drew’s assertion that the “mentally ill” all enjoy being homeless. Apparently he would have all believe these subhumans among the “normal” are not only too stupid to take the “meds” that restore their powers of reason, but enjoy exposure to the elements and threats of bodily harm.
I have sat up nights with a weeping friend who feared homelessness thanks to HUD inspections. Her executive functioning so damaged she couldn’t straighten her room properly. (As I couldn’t till recently. I finally shower regularly too. Restore normal brain function my foot!)
“Doc” Drew’s statements that all the “mentally ill” love being homeless is as insulting as it is stupid. I doubt he discussed homelessness or anything else with anyone he treated.
The man just wants to make a killing running a chain of asylums and is eager for warm bodies to cram into them. Psychiatry is the only branch of medicine easier to succeed in than day time talk shows.
Report comment
Is he is a sign of being mentally well, or capable, functioning?
Report comment
Simply preferring homelessness to what the system has to offer should not be construed as “enjoying” it.
Report comment
You got that right!
Report comment
Why did Trump choose Dr. Drew to be his policy advisor? Was Dr. Phil not available? Poor Dr. Phil, guess he’ll have to break out his copy of “Relationship Rescue” and give it another read through.
Report comment
Bwahahaha! Good one.
Dr. Phil is too behavior oriented. Jerry Springer II.
Dr. Oz would be a better proponent of the bio bio bio model. And he uses cool gimmicks.
He could fill a telephone booth with black balloons and say, “These are gloomy thoughts filling your brain.” Takes a knitting needle: “This is shock therapy.” Pops all the balloons in the booth. “See how shocks can save your life by killing those gloomy brain cells.”
Torrey would smack his head. “Brilliant! Sheer genius! How come I never thought of that?”
Report comment
lol, the black balloon booth…Better watch out Rachel or Dr. Oz will steal your idea…
Yeah I guess making a job out of asking “how’s that workin’ fer ya? ” didn’t really work out too well for Dr. Phil, at least in terms of aligning himself with pharma…Oh well he’ll be policy advisor when Oprah becomes president, and hopefully the worst that will happen then is she makes us all join her book club…
Report comment
Please everyone get it out of your heads that Pinsky, Trump, et al. are suffering from a “misunderstanding” of the issues. Psychiatry is ONLY a tool of social control and repression, and they all know it. And forget Trump, he’s being used as the front man for NEOLIBERALS, not the “right wing.” Jaffe and the rest are all “progressives.” Obama wouldn’t do a thing differently.
Trump and so-called “conservatives” who pick up on this faux-left totalitarianism see it as a way to fight gun confiscation (“control”), by using the false logic that “guns don’t kill people, mental patients kill people.” We need to make it clear to all that THIS SYSTEM kills people (and also that SSRIs cause mass shootings).
As for “Community Supports” — just give us the money, motherfuckers!
Report comment
Trump honestly believes that psychiatry prevents crimes just like Obama did. Just like 95% of the population does. Excluding shrinks.
Sometimes I wonder if uber-shrinks like Pinsky/Torrey/Murphy want mass shootings so they can use them to advance their careers. So they hand out more drugs knowing they cause violent crimes and rub their hands gleefully at every shooting that occurs. “Waste no emergency.”
Report comment
…
Report comment
wow! extremely powerful and important article. gigantic kudos and thanks for writing this.
Report comment