
Mental Health America (MHA) has finally unveiled its new National Peer Specialist Certification over much protest. Let us all take a moment of silence, whilst we weep.
First, a Little History…
Clifford Beers was born in 1876, one of five siblings. In 1900, he was first hospitalized for emotional distress. His experiences within the system were long-term and intense. At one point, he was confined to a straightjacket for 21 consecutive nights.
In 1908, he wrote A Mind That Found Itself, detailing the abuses to which he’d been subjected. His aim was to expose the state of the mental health system and make real change. In 1909, he founded the National Committee on Mental Hygiene, geared toward taking the steps necessary to reform that system. He continued the fight until his retirement, although he ultimately died in such an institution in 1943.
Ten years after his death, the organization that he founded turned the chains and shackles used to previously restrain individuals incarcerated in psychiatric institutions into the “Mental Health Bell,” a supposed symbol of its mission of change. At some point, the organization took on the name by which we know it today: Mental Health America.
It’s hard to imagine what Beers would think of what his creation has become. Current day, the organization is led by a man, Paul Gionfriddo, who claims no personal psychiatric experience but who has nonetheless capitalized on the struggles of his son through his book, Losing Tim. Note: Gionfriddo challenges the claim that he has capitalized on Tim’s life. In fact, he commented on a previous article of mine that Tim has been a fully consenting participant in his plight. However, I’m not sure how a man who has spent so much time speaking to his son’s lack of competence and decision making ability can suddenly then claim him ‘competent’ in this one self-serving instance.
Gionfriddo is also the same man who coined the Twitter-ready slogan “B4Stage4,” essentially taking things a step or two farther than the National Alliance on Mental Illness’s (NAMI) diabetes references, and straight up comparing psychiatric diagnosis to the stages of cancer. Meanwhile, among top tier MHA donors (Diamond, Platinum, and Gold) are no less than six pharmaceutical companies: Teva, Eli Lilly, Jaansen, Lundbeck, Otsuka, and Takeda. (Astrazeneca was also included as a Diamond donor in the last annual report, but has since disappeared from the ranks.) For whoever’s really listening, these points speak for themselves.
About that MHA ‘Mental Health Bell’…
Briefly, back to the bell. When I think of MHA today, I keep forgetting about that bell and all 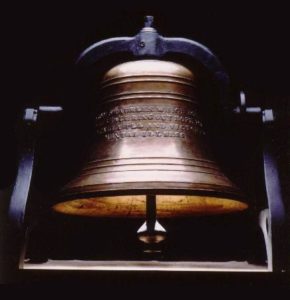 its parts. I think it’s willful on my end. I’m blocking it out because it hurts to think about it. The bell is inscribed with the following:
its parts. I think it’s willful on my end. I’m blocking it out because it hurts to think about it. The bell is inscribed with the following:
“Cast from shackles which bound them, this bell shall ring out hope for the mentally ill and victory over mental illness.”
How presumptuous, paternalistic, and condescending. Even for the 1950’s. It’s as if MHA missed (and continues to miss) the point entirely that at least some of the victory we seek is over the system and its abuses, and not some contrived, medicalized interpretation of our suffering.
This use of the shackles that once bound incarcerated humans is tone deaf and gross, not righteous. Clearly, MHA is among those who we must seek victory over. Not who we want fighting by our side.
And for MHA’s Next Trick…
So, of course, the next move that makes sense for an organization such as MHA is to bring us national ‘peer’ certification.
Because, when one carefully considers the peer role — and how “being with” and “connecting with” are at its very core — a costly online exam is precisely what comes to mind. Right? MHA’s Patrick Hendry (Vice President of Peer Advocacy, Supports & Services) attempts to defend this development by listing off the names of people who identify as ‘peers’ (an increasingly problematic term in and of itself) who were involved. (One article refers to it as a “something of a who’s who of peer support”). Yet I’ve personally heard at least one of those very individuals listed confess to feeling beholden to their employer, and thus restricted in what they say.
Hendry also acknowledges that doctors, psychologists and social workers were involved at the forefront, because collecting up people in peer roles — some of whom already feel pressured to tow the line — and mixing them in with individuals in classic power positions is sure to foster integrity. Wait. What!? How does any of this make sense?
Okay, But What the Heck is This Thing?
It’s a training. It’s a test. It’s a training? It’s a test? It’s a bird? It’s a plane? No, it’s just a test.
Okay. It’s definitely not a training. Sure, I had to dig around a long time to find an absolutely definitive statement saying that this MHA certification does not involve any sort of actual training from MHA, but that is indeed the fact of the matter. (I’d link to that super clear statement here, but I can’t seem to find it a second time.)
So, it’s just a test. A 125-item multiple choice exam, to be exact. It costs about $450 (between application fees and associated testing fees) to take the first time round, and another $200 every couple of years to renew (in addition to any costs associated with requisite continuing education credits earned). Individuals who become certified are actually receiving their credential from the Florida Certification Board, and not MHA directly. (If lots of people respond to this ‘opportunity’ and pay all those fees, it’s unclear to me who stands to gain what financially, but I’d certainly be curious to know at some point.)
Individuals must qualify for the test in a number of ways, including having logged 3,000 hours of work experience in some sort of paid or volunteer peer role and taking one of the approved trainings on MHA’s list. But to what end?
“Moving peer support into the private sector requires national, higher, and uniform standards. This certification is designed to satisfy the needs of the private sector, opening up new opportunities, career pathways, and higher wages for peers.”
Maybe, though saying so certainly doesn’t make it true. I remain confused. In the same document, they also claim:
“MHA has conducted a series of pilot programs placing peer specialists with enhanced training as providers of peer support within a national HMO, Kaiser Permanente (KP).”
So, that brings us back to that training issue again. The implication here is that the certification is synonymous with “enhanced” training, but one doesn’t typically become a “peer specialist” at all without some training. And, looking at the list of ‘approved’ trainings I find that they’re mostly all the basic trainings (some of them surely more questionable in quality than others) that various states already require for that initial ‘Certified Peer Specialist’ (CPS) step. The DBSA CPS program. The Appalachian Consulting Group’s CPS program. The core 5-day Intentional Peer Support training, accepted by some states as equivalent (or preferable) to a CPS program.
I’m kind of at a loss, but here’s the best I can sum up: MHA’s national certification is actually offered through the Florida Certification Board and not MHA. It’s just a free-floating test, but somehow transforms the test-taker into someone with “enhanced training” (even though they’ve likely only taken the same sort of training that all other CPSs have taken). It’s kind of costly (both in the short and long-term), but it will likely lead to a higher paying job (that may or may not resemble an actual peer role). Some day. Somehow. Maybe.
Okay. Cool. Got it.
But if Not You… Then Why Not MHA?
To his credit, Hendry has tried to face criticisms of MHA’s new certification process head on. Except that one of his most prominent defenses seems to basically amount to, “Well, somebody had to do it.” Here’s an excerpt of more precisely what he had to say on the matter:
“One of the leading criticisms about MHA creating a national certified peer specialist credential is that many people feel this should be done by a peer-run organization. Unfortunately, no peer-run organization has taken on this challenge yet.” – Patrick Hendry, ‘An Open Letter to the Peer Community’ July, 2016
Hey, so, here’s a thought for you: Maybe no ‘peer-run organization’ has stepped up because it is a bad idea. And, even if it is worth considering, since when is a void equivalent to an invitation?
No one’s written a sequel to Gionfriddo’s book about his son. (Oh, wait. Please tell me he hasn’t?) Maybe I should step in and get it done. And, I’ve been waiting oh so patiently for (insert questionable idea pertaining to a marginalized group I’m not a part of) to happen, but it hasn’t. I guess that means they’re just not capable, so I better take that one on too. I mean, somebody has to, right?
Nope.
Co-optation is Real (Thanks, MHA, for the Illustration)
Co-optation is a real thing, and it’s dangerous. Systems change requires that organizations trust and integrate much of what people who’ve ‘been there’ have to say. But they should never be the leaders or the loudest voice. Mixing that point up has many very real consequences that might not seem obvious at first glance. For example, providers (like MHA) who appoint themselves as ‘experts’ on peer support (under the guise of allyship, or whatever the case may be) inevitably pull resources into their court.
And resources tend to follow resources. Sure, there is the occasional foundation seeking only to fund organizations with budgets under a certain threshold, but that’s the rarity. More typically, securing the money necessary to implement a certain idea or project means that organization also gains the privilege of racking up the years of experience, the social capital (knowing the right person to even learn about the next opportunity), the reportable outcomes, the documented grant management experience and the reputation to keep attracting more funds.
Even if it means that the people from whom the providers originally got their ideas are left in the dust. Even when those providers’ priorities — no matter how intriguing those ‘peer’ ones initially seemed — begin to shift toward some other ‘next new thing’ that’s caught the organization’s eye. Even when those original voices and passion begin to slip from the memory banks (because maybe providers never really got it in the first place… because of course they never lived it themselves), and mission drift begins to occur.
We have offered up what we know to be true to improve the conditions for our own community. Not to earn some organization a new contract, or help them make their grant proposals sound more genuine.
Our expertise is our own, and it’s been hard won through our pain, suffering, and ongoing fight for our rights and voice. When an organization like MHA takes it for theirs, it may seem a benevolent gesture at first. They just want to help! But it inevitably pushes those with the firsthand experience back down — creating the illusion that that big organization actually has more expertise and reliability than those on the ground — and eventually twisting up the messages shared, too. (For more, see Searching for a Rose Garden: challenging psychiatry, fostering mad studies, edited by Jasna Russo and Angela Sweeney and including a chapter on this very topic by Darby Penney and Laura Prescott.)
Speaking of Twisted Messages…
Another criticism of MHA’s national certification is that it will lead people in peer roles down a clinicalized road. Hendry steps up to the plate again, and assures us that this is not the intent as follows:
“We have never intended to move peers towards doing clinical work in any way. Our efforts are to give peers every tool they need to perform as true peer supporters in a wide variety of settings. Peers are never expected to cross the line into a clinical role or to promote any clinical practice.” – Patrick Hendry, ‘An Open Letter to the Peer Community’ July, 2016
Hey, that’s reassuring. Thanks so much. Surely, we should trust the guy who uses enough ‘mental illness’ language to stuff a DSM. But, uh, hang on just one second. What about this?:
“More detailed knowledge of clinical interventions will be needed so that peer specialists know when and how to support individuals in treatment. For example, Hendry explained, research has shown that when an individual is receiving DBT for a personality disorder, peers must have enough knowledge about the phases of DBT to avoid “getting in the way.” This can occur when the individual’s therapist “withdraws,” leaving the individual “alone” to face challenging situations as a means of developing essential distress tolerance and emotional regulation skills. Peers who recognize the phases of DBT treatment can adapt their interactions with the individual in ways to support the therapeutic goal.” – Same guy, same month/year, different document (‘A single National Standard for Peer Specialist Certification‘, also July, 2016)
So, given that Hendry said these two things in the exact same month of the exact same year, either he’s the kind of flip flopper that should consider running for political office… or he has an extraordinarily different idea of what constitutes ‘clinical’ work than the average bear. I mean, it’s not even just the fact that the above statement wreaks of peer turned mini clinician. There’s also the inherent assessment involved, and the fact that it allies the peer supporter with the clinical team over the person receiving services. Meanwhile, it renders the most important values of peer-to-peer support (self-determination, voice, and choice) entirely disposable in favor of clinical theory.
To boil it all down, in that last passage Hendry basically suggests that the peer supporter needs to learn their place, recognize when a clinician has withdrawn support for ‘treatment’ reasons, and straight up ignore someone asking for contact. This is a pretty clear flag that MHA sees the clinician as ultimately controlling the relationship, and leaves the person in the ‘supported’ role even more powerless than ever. It runs contrary to literally everything that peer-to-peer support is supposed to be about.
Oh, Did We Forget to Mention?
Much less talked about is the fact that anyone who becomes certified through this process must sign on to the Florida Certification Board’s Code of Ethics. (See page 7 of the ‘National Certified Peer Specialist Process and Forms‘ for details on this particular requirement.) The Code is long and covers many points. Here are a few of the highlights:
“An applicant or certified professional shall not use, possess, or sell any unprescribed or illegal substance”
Well, I know I personally love signing on to documents that attempt to regulate what I do on my personal time at home. How about you? (Oh, and by applying, you also agree to a “random criminal history check to ensure compliance.” See also page 7 of the same document named above.)
“An applicant or certified professional shall not perform services outside of their area of training, expertise, competence, or scope of practice.”
Pretty tricky territory, here. This is the sort of regulation that Tim Murphy and his brethren have attempted to push through on any number of occasions to regulate peer support. Imagine all the topics and tasks certain people will claim are “outside of our area of expertise”?
“An applicant or certified professional shall not recommend to a consumer any unnecessary, ineffective or unsafe device, treatment, procedure, product or services.”
Well, okay. But who gets to decide what’s “ineffective or unsafe”? I’ve seen people like Susan Inman claim that Hearing Voices groups are “dangerous.” Just stop for a moment and imagine where this could head.
“An applicant or certified professional shall place their application or credential(s) on inactive status for any mental, physical, or behavioral health related adversity that interferes with their professional functioning.”
Uh, what? I need to notify the board if I’m having a hard time? Can’t I just take some time off? Who precisely decides what’s interfering with my “professional functioning”? I employ people who see it as a benefit that they sometimes still struggle with suicidal thoughts and can talk about that openly with others as a way to demonstrate humanity and mutuality and build connection. Where do they fit in? You want to talk about dangerous… Well, this particular ‘ethic’ that everyone taking the MHA national certification will sign on to… This is it.
Closing with a Kiss
As I was writing this, a certain image came to me. (Forgive me, for it’s a bit over the top.) It  was that of a dementor from Harry Potter. You know, those creatures who would latch on to people, and sort of slowly suck out their psyche via a dementor-style kiss?
was that of a dementor from Harry Potter. You know, those creatures who would latch on to people, and sort of slowly suck out their psyche via a dementor-style kiss?
I can’t shake that image now. I feel like MHA and other organizations like it — that are led by individuals who are decidedly not people who have any understanding of what it’s like to be caught within the clutches of the psychiatric system themselves — are sucking out our psyche and our soul. Their intent may certainly be better than your average dementor, but I’m not even sure that is always true across the board.
These organizations sometimes shroud themselves in so-called ‘peers’, but often only those who don’t flinch at having their identities boiled down in such a way. That is not to say that they aren’t still good people with voices as potentially valid as the next, but all too often they’re also the ones who have a job they can’t afford to lose and so feel constrained within their organization’s ‘party lines’. Sometimes they’re the people wrapped up in so much internalized oppression they can’t see through their own medicated haze. Or, they’re the tokenized one committed to “creating change from within” who started out with such a clear vision, but have fallen so far in that they can’t quite see they’ve lost their center.
In the end, it is up to each of us to ‘just say no’ to MHA’s national certification (and to spread the word for others to do the same). It is dangerous to what we call ‘peer support’ for Mental Health America to have done this. Even if they did it well. Which, as best as I can tell, they did not.














Thank you very much for writing this (along with everything you write!). I practice peer support in the state of Maine. What MHA is doing is dangerous. I fear for the future of the paid positions in peer support because of people like that, and especially because of the current political administration.
Report comment
You are very welcome, and thank you for reading and commenting! I agree it’s absolutely dangerous. Even more dangerous is the fact that so many people seem blind to that fact. 🙁
-Sera
Report comment
Sera
Thank you so much for sharing your insights and the danger that lurks. I envision an international peer support certification process perhaps built upon the peer-developed and peer run national Canadian Certification model which as I see it is completely aligned with the values of peer support. Might I add that peer competencies have already been developed by INAPS and then expanded upon by SAMHSA and published on SAMHSA web. These competencies are aligned and consistent with the Canadian peer to peer support competencies. Would it serve the US peer support community to develop competencies that unlike the fear-based, pathology MHA competencies would be Trauma Informed, socially inclusive and respectful of the wisdom gained by those of us who have been through the mental health system, understand the impact of Menal health oppression and are skilled at supporting people through emotional distress and into a full life in the community ?
I am committed to create such a US or international certification. if anyone else is interested let me know via email, [email protected] or email INAPS. I hope that INAPS will step forward to coordinate a certification that will genuinely enhance our ability to support each other on our healing journey’s.
Report comment
Yes, Lauren,
It would be beneficial, and makes
total sense.
Count me in for help with this.
Julia R. Scott
Report comment
I emailed you, Lauren, in the case this has gone anywhere and in the case that I can be part of the conversation!!-Mayla
Report comment
Thank you Sera,
Your article is very enlightening, and I’ll do what I can to spread the word.
Julia R. Scott
Report comment
Of course, this will be for the regulations that they deem fit. And what would those be? Well since Pharma is going to be sponsoring this MHA certification, we all can read between the lines on this one.
The latest statistic is that 90% go off medications. Well a lot I suspect will return to normal and figure out that the drugs don’t work so how does the industry combat that? Hire peer counselors to make sure everyone TAKES THEIR MEDS! Imagine the addition to the bottom line profit on this little boondoggle.
Reminds me of the Nazis hiring or recruiting Jews as officers to round up the masses in the Ghettos for shipment to the camps. I can hear the sales pitch to take these jobs, “But they pay X an hour!” You just have to sell your soul!
Report comment
Yes. A lot of us develop the “disease” they call “agnosognosia” from reading all those naughty books, articles and websites like this. They never should have allowed us to learn to read and write. It ruined us as cash cows and lab rats for the MI industry!
Report comment
Anonymous, It’s unfortunately highly prevalent for people working in ‘peer’ roles to be lured in and used to try and silence others. It’s very sad. Thanks for reading and commenting.
Report comment
Ah Yes, Anonymous – and the people I know who have been tapped for “peer work” really really need the money – to go from destitute to earning a salary? What a dream! Even though, the peer paid positions I’ve seen are little more than minimum wage – but it’s work! How exciting!
There’s just that tricky “sell your soul” part. Oh well, was I really using that?
Sera – this is some awesome research you have done – except for the opinions (which I agree with) this is some fine journalism!
Report comment
Since there is a drug test, you can probably bet your bottom dollar that they can check whether the peer is med complaint, pretty easily. Step out of line and the first thing probably will be to prove that the individual is taking their meds. Seeing that the drugs are mostly lobotomizing, yes, the individual is selling their soul in my opinion.
Secondly the position screams, yes, I am a mental patient and you can see that by my job title, no need to enforce HIPA. So maybe $1.00 above minimum wage is worth the price? I don’t think so. Yes they need the money, but is it worth the price?
I am sorry but I’m going to have to agree to disagree.
Report comment
When they drug test they do not text for psychiatric drugs to see if people are med compliant. Not every peer takes the drugs, some do but many do not. I do not take any of the drugs and have been randomly drug tested many times with no problem about whether I was taking the drugs that I left the “hospital” with when discharged. I suspect that these kinds of things would be a HIPPA problem since you’re not to reveal anything about a person’s medical records. Unless I reveal it, no one in the ‘hospital” where I work, which is the same one I was held in, no one knows my diagnosis or the drugs I was supposed to take. These would be huge HIPPA violations that I could bring suit against the “hospital” for, under federal prosecution.
Report comment
It’s one thing to release records for privacy sake (I don’t know HIPPA details)
But it is possible that as an EMPLOYER, they can insist on it.
Report comment
Here’s a fine HIIPA story for you, Steven. The last time I interacted with psychiatry was about a dozen years ago, give or take, but HIIPA was in effect at the time:
I’d gotten the call that one of my parents was dying, and made the trek back to my hometown, where deathbed admissions were made and family skeletons tumbled from the closet, confirming memories I’d had of incest. They ended up slipping into a coma but woke after a few weeks. The whole experience shook me to the core, and the standard 3-day bereavement leave was nowhere near enough time off work to integrate everything that happened. Even though I had been working with an MFT for awhile, the insurance required an MD to sign off on the time off. Kaiser assigned a psychiatrist that seemed to be sufficient, but after a couple of appointments with him, he suddenly became unavailable (but they always assured he’d be back in a week or two), and no matter which psych-du-jour it was that was filling in for him would only write me a 2-week extension. Having to address my situation with a new person every 2 weeks made healing impossible, and when I got fed up and demanded to be assigned to a doctor who was actually there to do the job, his boss got exasperated with me and said “Cut the guy some slack, he’s depressed!” This was the guy just beneath the head of the department, and REALLY should have known better! I lit into him: Did DR. Depressed give you written permission to disclose that to one of HIS PATIENTS?! I rather doubt that. And you don’t even know me! You have no idea how that info will be received by me, or what I might do with it. I’d call that reckless disregard for his emotional well-being AND mine!” The next call I got was from the dep’t head, who gladly signed off on the 8 months’ leave that an independent eval suggested. I was too twisted up by it all to follow through on my intention of reporting him to the AMA, APA, medical licensing board, etc.
Report comment
I actually get paid a really good salary; far better than what I was paid for teaching high school for fifteen years and as a hospital chaplain for fifteen years. Of course, I suspect that this varies from state to state. If we had peer workers in the state where I live they probably wouldn’t be paid as well as I am since I get paid by the state since I work at a state institution.
Report comment
Nice article Sera. Regarding this paragraph:
““More detailed knowledge of clinical interventions will be needed so that peer specialists know when and how to support individuals in treatment. For example, Hendry explained, research has shown that when an individual is receiving DBT for a personality disorder, peers must have enough knowledge about the phases of DBT to avoid “getting in the way.” This can occur when the individual’s therapist “withdraws,” leaving the individual “alone” to face challenging situations as a means of developing essential distress tolerance and emotional regulation skills. Peers who recognize the phases of DBT treatment can adapt their interactions with the individual in ways to support the therapeutic goal.” – Same guy, same month/year, different document (‘A single National Standard for Peer Specialist Certification‘, also July, 2016)”
It’s hard to overstate how flawed this virtual word salad is, given that serious problems in thinking/feeling don’t break down validly into discrete “personality disorders”, that such labels are extremely stigmatizing, and that all the “efficacy” of DBT is based on is short term trials of getting people to tamp down their thoughts and feelings in a medicalized way… and there are other approaches to severe distress that may work better and in a less stigmatizing, medicalized way than DBT.
Report comment
Yeah, don’t get me started on DBT and what it means to be an ‘evidence based’ practice. Oy!
Report comment
I know I’m unsuited for this, for the same reason I’m unsuited to work in the average residential substance abuse facility- I can’t stop myself from getting my charges on supplements, whenever it seems likely to benefit them. When I first got on B3, I knew I had to help myself, with minimal or no aid from anyone else, so I studied the relevant literature and then let myself become a resident sorcerer for a group of local dopers, who knew me because I was a volunteer in a crisis center (popular in those days) and also a collector of hallucinogenic mushrooms. I did a number of things as well as treating simple dysperceptive states- supervising and assisting a heroin withdrawal (but not of someone with a giant habit) and a couple of physical withdrawals from alcohol, being able to safely speed them up by using simple documented methods for all of them.
In the 90’s, while working in the residential substance abuse program, I started up again, after watching a number of treatment failures occur, because of staff ignorance. While the program director was firing me (she wanted me to quit, but I wanted unemployment), I had to bite my lip when she and the clinical supervisor had a side discussion about two residents who had graduated, despite a poor prognosis, because they’d been taking niacinamide (courtesy of yours truly). The supervisory dignitaries would then have sacked me with cause, had they found out, denying or delaying my unemployment benefits.
I’d expect to be even more grievously punished, working as a peer specialist.
Report comment
Hi bchariss, Thanks for sharing a bit of your experience working around the ‘system’.. I wish it didn’t have to be that way! Sera
Report comment
yes, Sera, all you said
when they say: “Moving peer support into the private sector requires national, higher, and uniform standards. This certification is designed to satisfy the needs of the private sector, opening up new opportunities, career pathways, and higher wages for peers.”
This seems like it could be some kind of tactic to provide these lower-paid and potentially easily stigmatized staff for the private sector, which may mean for-profit firms too and private practices. The drive to have more credentials and more tests with constant recertification to meet “national standards” is going on in other fields too, even where people are considered professionals who already have graduate degrees. This is a money-grabbing and unnecessary and dangerous program.
Report comment
Eileen. Agreed! I wish I had some better sense of how much they stand to make off of it.
Report comment
Yes, Eileen. There’s that profit motive!
Why hire a professional or a nurse practitioner, or a nutritionist, or pharmacy consultant when we can have a lowly grunt do the handholding, the social work (helping with appointments, apartments, etc.), the tempering of emotional distress?
You could have an army of part time peers (with no benefits) for the price of one MSW.
It sounds like a great way to increase share price, which is the ultimate goal of a corporation.
And if the peers “toe the company line,” all the better. Having a “national company line” – for ANY corporate practice – is a disaster! (though, looks darned appealing to the corporations!)
Report comment
Thank you Sera for this extensive piece of research! You make an interesting point that MHA saw a “gap” where they believed national credentialing should be, which may have just indicated that others believed nationally credentialing was an undesirable outcome and therefore declined to take on the task (rather than an incompetence narrative). Of course this wouldn’t be the first time there were vastly different perspectives on desirable and undesirable outcomes in our work!
I am wondering what your recommendations are for those who would “just say no,” aka the resistance. Your vision/leadership is appreciated!
Report comment
Good point, Laysha! (And excellent piece, Sera!). There is no “gap” – as Laysha noted, many of us believe there should be no certification, national or otherwise. I find state certification equally as appalling, excellent in the rare instance where it’s controlled by people who’ve been through the system. I fought certification in NY when I worked for the state, but the person who followed me in that role has imposed it.
Report comment
It’s hard to argue against a *something* with what looks to the outside like negative space. I’m sure there’s a name for that kind of logical argument/fallacy in philosophy; it escapes me….
What I usually try to point out — not specifically about certification, but about places that engage in peer support more generally — is that we can all agree that accessing the mental health system is an impossible nightmare for many people (whether you believe in the services provided or not). Peer support is the ONE space where people can still go, and feel safe, and be real without an appointment or an insurance card or a driver’s license or a cell phone. For anybody who’s ever tried to get an appointment with a psychiatrist and then ended up at the ER after a million unanswered calls, that kind of access is invaluable!
Report comment
Laysha,
It is a really good question, and not one to which I have the answer. Of course, my fantasy is that articles like this one and word of mouth will prevent so any people from taking the damn thing – or organizations from being willing to pay for it – that it will fall apart for lack of funding. Unfortunately, that seems unlikely, but it won’t keep me from trying!!
Do you have any other suggestions?
-Sera
Report comment
I was thinking about where this certification is positioned and how we as a society deal with problems in the ambiguous place between public and private where the healthcare system often lurks. The certification is not being implemented by a government agency — there are no elected officials or even bureaucrats to protest or threaten with votes. It’s not exactly a private good that one can boycott or publicly shame until investors get nervous.
While voting with one’s feet is always an option as you mention, I suspect that will be ineffective because there is a large enough pool of workers who need work.
Maybe you could look into the literature on other low-wage/low skill jobs and disenfranchised workers…Sera Davidow: the Cesar Chavez of peer support!!
– Laysha
Report comment
Thanks, Sera. If/when I get my wife thru the healing process, I’ve kind of been interested in the peer specialist stuff, if I were welcome…
Report comment
Thanks, Samruck2. I hope you and your wife get to a better place soon.
Report comment
The Munchausen Syndrome by Proxy NAMI parents are the WORST , Pete Early, Rick Warren, Michael and Barbara Biasotti and I now I hear of this Paul Gionfriddo. All cut from the same Munchausen Syndrome by Proxy mold. Same behaviors poor me and buy my books… For those that might read this and don’t know MSBP is characterized by feigning, exaggerating or intentionally producing physical or emotional symptoms in another person in order to place that person in the sick role with the primary motive of gaining attention for themselves and or sympathy from others.
Here is the polar opposite of a MSBP NAMI parent, Maryanne Godboldo, The true story of how Maryanne Godboldo took on the state of Michigan and a Detroit SWAT team to protect her daughter from being given dangerous psychotropic drugs, Risperdal. https://www.youtube.com/watch?v=BmEdjwqNbBs
Report comment
Hi The_cat. Comparing some of what happens in this world with Munchausen Syndrome is interesting… There does seem to be a bit of a common element in terms of somehow getting emotional gratification via public attention associated with one’s child’s struggles… Although, I’d stop short of the idea that most of these parents don’t also really care about their kids and wouldn’t find it much more important for their kids to be in a happier, better place.
Thank you for the story! I look forward to checking it out.
Report comment
Terrific article, Sera. But, the elephant in the room is this: whatever MHA’s past might have been, it is now “led” by the alt-light sect of the NAMI and TAC crowd. These Mommy and Daddy Munchausens DO NOT want their sons and daughters to enjoy ANY real relationships. Despite these freaks’ hysterical and ludicrous claims, even *they* do not believe that “mental illness” is “just like diabetes or dementia”. If they did, then they’d have NO FEAR of letting their Mad family members ditch the quacks, connect with loving people, and, in that way, begin to focus on their own dreams and goals. Honestly, psychiatry would not be able to pathologize Mad people WITHOUT keeping us isolated, shunned, endangered, and completely demoralized. We could be more openly Mad than we’ve ever been, and STILL retain our liberties, so long as large numbers of us were not expendable. Good jobs, friends, and partners are the three fastest pathways out of that state, so it’s no surprise to see peers “credentialized” out of a paraprofessional system that provided all three. It’s fine to weep, but we must also fight. Mad people’s “treatment compliance” CANNOT be secured by impoverishing us or by estranging us from our closest allies.
Report comment
Thanks, J! I can’t pretend to know what some of the people referenced truly believe, but I do agree that we must fight.
Report comment
I really have a hard time with the idea that everybody who goes into treatment for some so-called mental health issue or another, sometimes two or three, should come out working for the system as a mental health paraprofessional, that is, if they want to be successful. I’m not sure what a “peer role” is exactly. I do figure it’s something you want to get away from if you want to be cured of the god awful mental health indoctrination system.
Coming on the tails of the mental asylum building movement of the 19th century, that reform movement, you’ve got the mental health movement of the 19th etc. centuries, this reform movement. The movement, in other words, that gave Mental Health America its name. The driving force of this evangelical cause is their virulent faith in something called “mental illness”. It isn’t a “mental health” movement in reality, for mental health is kind of like modern art, nobody knows just what the heck it is, it’s a mental health treatment movement. A treatment movement much like the asylum building movement that proceeded it. Mental patients, in other words, should neither be seen nor heard, but we’ve got a place for them.
I don’t think you get reason out of being unreasonable. I don’t even think more unreason is the answer to unreason. I mean I’ve got my limits when it comes to the utilization of anybody’s total waste of time machine. What was it Dante saw etched above the gate he entered? Oh, yeah. “Abandon all hope, ye who enter here.” False hope though, that’s another thing, isn’t it? Myself, I’ve finally figured out that there must be another way circumventing this absurdity, and if I can find that other way, believe you me, I’m taking it.
Sera, there’s always been a lot wrong with the MHA. Their crusades for more treatments, and for the money for treatments, are not my crusades. Heaven defend me from them. I’m actually for well enough being left alone. Why couldn’t the MHA be for something good like that. Instead it’s all about pounding the round peg into the square hole. De-criminalize de-medicalize crazy confusion and disorientation, and no problem. Fools have a way of coming to reason in the end anyway, if their folly doesn’t destroy them first. Legislating, as we have, against folly is rank folly in itself. Whatever it is the system is trying to force on people, one thing I know is that it isn’t wisdom. As long as that is the case then, it isn’t for me.
Report comment
I agree with you there Frank. I’ve been encouraged to go for my MSW and become a therapist because I’m “high functional.” Interesting how many of us called high functioning are on smaller doses of “meds.” Whenever I was allowed any say I would opt for fewer drugs even when I thought I was hopelessly insane. I could never become a therapist at a mainstream MI center because I want to help people, not keep them suffering and drugged up.
Some workers I have known would get frustrated at the way we got worse and made poor life choices. It’s hard to behave maturely or responsibly when drugged out of your gourd, taught that all your thoughts and feelings are crazy and wrong, and alternately shunned by mainstream society or patronized by Big Brother in the psychiatric ghetto.
Report comment
Very true, people perform up or down to expectations. People who are not treated like responsible adults are not likely to act like responsible adults. One option is to call them “sick” and to create “providers”, sort of like surrogate parents, for them. Another is to treat them like adults anyway, within limits, and see what transpires.
Report comment
Frank,
Overall, I agree with you the idea that everyone who goes into the system should come out as its employee. However, there are many people for him that has been a really important path. Many of my co-workers have seen the depths of the system, and now get much satisfaction out of fighting against it in the way that they do. Of course, most of them also work with the RLC which is much less direct than working for a traditional provider. Working in a traditional provider in a peer role is a terribly hard position to sustain and not lose sight of one’s self again.
Report comment
I see the corruption that starts with the psychiatrists in bed with drug companies extending to paraprofessionals in bed with their former wardens, metaphorically speaking, of course. Mental health treatment as the gateway into work in mental health treatment seems rather myopic in a dull way to me. I just kind of feel that adult baby sitting is something that we shouldn’t need so much of, and I’d like to see the practice diminishing. Of course, if you’re out to bribe people, or twist their arms anyway, sure, make it hard for them to get paid work anywhere else.
Report comment
But adult babysitting is what some people who’ve been in the system seem to want. The people responsible in my state for creating the training and certification program for peer specialists went out into many communities across the state and asked people who’d been in the system what kind of services they wanted from peers and the answers were things like, “I want someone to take me to my doctor appointments”, or “I want someone to take me shopping, or do my grocery shopping for me”. Things like this formed the majority and bulk of the information that was gathered. I didn’t find much of anything dealing with people wanting motivation towards moving out of the system and leaving it behind. There was nothing mentioned about facilitating discussion groups or things like Hearing Voices groups. Hell, almost no one in this state knows what Hearing Voices groups are to begin with.
Granted, peer workers in the community do a lot of things like what I mentioned above but in the doing they’re supposed to form relationships where they walk with people so that these people find their own voices and strengths so they can evolve to the point of being able to stand on their own and hopefully do these things for themselves. We are not about keeping people tied to the same place and can gently challenge people to look at things in new ways so that they find what it is that they need to fulfill their own lives. I believe that peers fail in their work if all they do is continue to do what might be seen as “babysitting” work.
But what I’ve also found is that many people who’ve been in the system learned their lessons well and continue to believe that they’re not capable of taking control of their own lives, even if this takes some time to accomplish. I guess that this is to be expected since very few people have ever told them anything different. I help facilitate a recovery group where I work and when I ask people what their definition of recovery is I hear a litany of “take your meds and work your program and stay away from people that will try to lead you astray from this.” It’s like a mantra tape that is turned on immediately when they hear questions like this. When my partner in crime, the other peer worker, and I introduce ideas like becoming recovered everyone looks at us as if we have horns sprouting out of our foreheads. If I didn’t know better I’d think that they make the sign against the evil eye behind our backs when we’re not paying attention! I run into very few people like you or Oldhead or FeelingDiscouraged in my work and it’s extremely frustrating and it saddens me. How do you separate people from the learned helplessness that they learned so well when they’re frightened of even thinking about a different life for themselves? What I’ve found is that the idea of recovery is more frightening for many people than it is intriguing or positive because it requires taking responsibility for your own life. The system has deprived people of doing this at the appropriate age and it scares the bejesus out of people when they’re in their late 30’s, 40’s, and 50’s. Who wants to become responsible for their own lives, especially in today’s world where so many things are in flux and so few things are certain? This is the challenge handed out to peers in the state “hospital” where I work. It is challenging to figure out how to help people wean themselves off of the learned helplessness and gradually replace this with personal responsibility. I think it can be done but it’s time consuming and you have to keep faithfully hammering away at it each and every day. But of course, all the other staff in the “hospital” give them the totally opposite message and theirs is the prevalent message. So people are faced with a choice of opting for our peer message or continue to drink the Kool-Aid and repeat their mantras.
One thing I’ve learned from Sera in all of this is that nothing is simple or easy. Lots of times it’s a huge mess to be waded through without drowning in all of it. One thing that I do know for myself is that I don’t want to babysit people.
Report comment
“But adult babysitting is what some people who’ve been in the system seem to want.”
Often at the behest of the parents of ‘adult babies’ it would seem, the parent of ‘adult babies’ who have, frankly, if truth were told, been abject failures at the weaning business (i.e. the business of making independent ‘adult adults’ out of their children.)
As for the implications of what your saying (some people don’t want to be ‘adult’), true enough. Institutionalization, with community treatment programs as a prime example, has, within the community at large, given dependency a whole new dimension.
People in the system are paid for perpetuating the system. This is anything but seeking rational solutions. People are “sick” in this “sick” system in the same way that the system itself is “sick”. Take homelessness. A whole service industry has evolved around “serving” the homeless. Are we any closer to providing affordable housing and jobs with decent wages. F**k no. It would throw too many people out of work to do so.
Report comment
Frank
Thanks for responding and I agree with everything that you say.
Report comment
Getting “peer specialists” “out of the way” seems to be the point of this. If they won’t be handmaidens to the “authorities,” they have to be bumped off. And Lord help us the “peer” should have any kind of “mental health issues!” Do psychiatrists and psychologists have similar requirements to resign or go on leave when they “have issues?” Are the authors unaware that psychiatrists are at the top of the charts for professionals who commit suicide?
Unbelievable! Or I wish it were unbelievable…
— Steve
Report comment
I think I heard several years ago that psychiatrists commit more suicides than any other professionals. Could it be that many of them fail to suppress their consciences indefinitely?
Report comment
Or, living and working in an atmosphere of constant failure could be a despair-inducing situation.
Report comment
Yes. Assuming that they actually empathize with the failures of those they dehumanize. Some–perhaps many–do. I try to think as well of people as possible.
Because of how psychiatry functions, our failures are their successes. Our stigmas are their awards and professional aggrandizement.
Not all psychiatrists act like villains off the Rocky and Bullwinkle cartoons. 🙂 But the system of psychiatry is corrupt and based on human oppression.
It degrades not just the oppressed but the oppressors. While they don’t suffer as we do they also experience a deterioration of the soul. No one “gets away” with evil–unless you count becoming a remorseless, soulless sociopath a good thing….
Report comment
They don’t empathize with their patients, but seem driven by the humiliation of being a failure, since few, if any, of the patients get well while on their conventional treatments.
Report comment
Steve, I get the impression from what I read that the Florida Board may have similar requirements for many different ‘professional’ fields. However, even so, it’s absurd and *much* more dangerous for a ‘peer’ role than the others… Oy.
Report comment
I have known a ton of therapists and psychiatrists who practiced for years while fully qualifying for a “mental illness” diagnosis. Anxious, depressed, delusional, emotionally unstable – all the labels they throw at their “clients.” There is ZERO accountability until something horrible happens. It seems very clear to me that these “peers” will be held to a much higher standard, based on pre-judgment and bias against their role and them as persons. I find it offensive to assume that “peers” have “mental health issues” and assume that the “real professionals” don’t!
Report comment
Maybe this is the point. The stigma has passed onto the MD itself so that’s why MD are choosing not to enter the profession. I’ve read in articles that they are having problems recruiting for psychiatrists but have never seen any statistics. I think this is just like Amway, recruit more people into the system because maybe they are losing recruitment numbers on the MD side and just need warm bodies? Just a thought. God I hope so. Haven’t they ruined enough lives?
And just think you get to go to work every day admitting that you got pulled into this pyramid scheme of how many different drugs can I consume before I’m lobotomized?
By the way, anyone know the statistics?
Report comment
Anonymous2016,
Pieces of the info of what you asked can be found at:
“Anatomy of an epidemic”, by Robert Whitaker, at page 266 (chapter 13).
Quote: “… but during the 1970s, the percentage of medical students graduates choosing to into it ] psychiatry [ dropped from 11% to less than 4%. This lack of interest in the field, the New York times reported in a article titled “Psychiatry anxious years”, was seen as a particularly painful indictment”.
That NYT article was written by: Bryce Nelson (02 November, 1982). It can be found (2 pages) here:
http://www.nytimes.com/1982/11/02/science/psychiatry-s-anxious-years-decline-allure-career-leads-self-examination.html
………..
Now… the years have passed, and unlike the peers morons (sorry), the APA is not naive, saw it coming… and Whitaker at his book (Anatomy), explains it very well.
So (at Europe, at this days) a psychiatrist working at the very same organization, working with the same person/problem… a psychiatrist can gets payed by consultation (all of them not famous), more 20-30€, by a single appointment… than a psychologist.
And then if you look from a famous psychiatrist… then you pay 3 digits (euros), by one single appointment.
Despite that… Jeffrey A. Lieberman said, the psychiatrists “wanna-be”… are being bullyed. Oh… the poor Lieberman, wants MORE money (and silence the dirty truths) 🙂
………..
So, here is one ideia for those sheep that are not yet lobotomized enough:
Saw that NYT article, the whole 2 pages?
Is dated (1982), yes?
Never mind is not dated enough. Tey were worried? It hurted them?
There you go! Now have the solution and it is simple: HURT THEM WHERE IT HURTS. Quite simple, really 🙂
Report comment
I am just hoping it is continuing. It is 1982, at the height of the anti-psychiatry movement. I think Prozac hit the market in 1987. I know Xanax hit in 1981. There doesn’t look like any current data.
Without legitimacy and the MD to sell the drugs, psychiatry as a whole will contract and end. That’s my hope. Unfortunately it a misled wish but, a wish at least.
Report comment
Meanwhile at AA and NA anyone can play substance abuse counselor or peer support specialist with no certification at all. I do it especially when I see someone is hurting and one of the evangelical AA types was big booking them totally oblivious to the fact that preaching AA mantras was not what the person needed at the time. Person is all bugged out with anxiety and withdrawals please STFU with the honesty and step thing right now. Thats lived experience being bugged out with anxiety and withdrawals myself just dying and having someone from AA do that honesty and step thing to me in that state. Thats how I know.
I talk to them get their story and be like listen I was where your at and the shitty way you feel, it will go away, do not mistake the beginning of sobriety for a permanent condition, that is the mistake I always made and said F it before I got better. I don’t say the same thing to everyone but I often say its takes balls to get sober and beat this thing. No pain no gain, tough out the shitty part you are in now.
I took all the classes for mental health tech, the one class on the brain pushing all that serotonin crap just pissed me off and I argued about it.
I never took the test, I can’t work for the system knowing what I know expected to go along with treatment stuff I disagree with like all the keep you sick pills they dish out and also I don’t believe total absence from drinking is right for everyone including myself. I drink sometimes, the sky does not fall, I do not pick up where I left off, I do drink more then I expected to sometimes and get a whopper of a headache. Some people should never drink or use again, I can’t argue with that but for others the whole thing becomes a self for-filling prophecy when they are told if the pick up everything falls apart. Fall off the wagon ? STFU and jump back on.
I usually keep that moderation thing to myself not cool around these parts but they need to teach harm reduction.
“Individuals must qualify for the test in a number of ways, including having logged 3,000 hours of work experience…” Oh give me a break. The mental health mafia wants you to work 3,000 hours BEFORE taking the test !!
“Applicant attests to lived experience as an adult who has been in recovery for a minimum of 2 years from a substance use or mental health condition.” http://flcertificationboard.org/certifications/certified-recovery-peer-specialist-adult-family-or-veteran/
I have been in recovery alot longer then 2 years, whats the definition of recovery ? Never went 2 years without a drink but my recovery date is when I got better, kicked daily heavy drinking and got off all psych pills except maybe something to sleep sometimes.
Do I qualify if I was honest ? I should qualify, I went from hopeless disaster ‘revolving door’ patient to successful moderation, drinking maybe once every two weeks, when they said that moderation is impossible AND I that I needed to be medicated or I would never make it. Maybe they could learn from me !
I don’t know what else to say about the The Florida Certification Board, The Mental Health Mafia and all this. They have their own agenda.
Report comment
Hard to say. Bill W. took a lot of heat toward the end of his life when his plugged niacin as a remedy for alcoholic depression, after he and 20 out of 30 of his AA buddies also did (he got the 30 guys to try this in order to see if his own loss of depression was a fluke). Some of the old line AA guys thought he was just getting strange, if not demented.
Report comment
Their own agenda indeed. I appreciate your pointing out the question of what qualifies as ‘recovery’… I talk about that silliness a lot when I tell my story… It’s foolishness, and in its foolishness it gives all those who have more credibility than us in a system of this nature it puts us in a really vulnerable position.
Report comment
Why is it that the expectation is that we talk about being “in recovery”? As far as I’m concerned I am recovered. I am not “in recovery”. I have found healing, well-being, and balance in my life and I don’t plan to spend the rest of the days I have monitoring symptoms and worrying about whether what I’m feeling today means that I might be getting “ill” again. I am not going to live like that.
When I and my companion peer worker expresses this idea everyone where we work look at us as if we had horns growing out of our foreheads. Someone even corrected us one day in a discussion and said “you are in recovery”. I thanked them not to try and decide for me what I mean when I say something. When I say recovered this is exactly what I mean.
Report comment
Stephen, Exactly. My favorite line to offer people in this vein is “When did what you call life, with all its ups and downs, become what I’m supposed to call ‘recovery’ forever and ever?” 🙂
Report comment
I was recently in the local hospital emergency room because of my hernia. While speaking with the surgeon – an MD – I said I’m a *recovered**alcoholic*. He challenged me on my use of “recovered”, in stead of “in recovery”, as he thought it should be. I pointed out to him that the book “Alcoholics Anonymous”, on the title page, uses the construction, “…many thousands HAVE RECOVERED from alcoholism”.(emphasis added). So, I’m a recovered alcoholic, because I went to A.A. meetings, and worked the 12 Steps “by the book”. I’m happy and alcohol-free for decades, now. My RECOVERY from psych drugs is almost as long. (Thanks, good to see you again, Sera! Keep up the good work!)….~B./
Report comment
“Officially certified peers.” Does the absurdly contradictory nature of this term need further elaboration?
It should be understood that the so called “peer movement” or whatever they call it originated in the political operations unit (or whatever they call that) of the NIMH/APA as a tactic for destroying the only real anti-psychiatry movement I have ever had experience with (though I hear claims that there’s one out there somewhere, who knows). What they did was identify the most opportunistic and compliant people around the movement; they then flattered and bribed them with funding for their psychiatry-friendly bogus “alternatives,” and the “peer” stuff was concocted as a big part of that. And it still is, in fact it has metastasized.
I should point out too that when some of us were still dealing with the two Murphy Bills — one of which some groups associated with MIA supported as the “lesser of the two Murphys” — the “good” Murphy bill contained this exact sort of language about peer certification, which at the time some were willing to trade off in exchange for no AOT. So none of this should come as a surprise.
Report comment
oldhead, Actually, I believe BOTH of the Murphy Bills contained similar language (as I pointed to in the article I linked to above). I agree that so much of this has been a tactic to silence – not support – our voices.
Report comment
You’re quite possibly correct about both bills containing similar language on “peer” certification, as the House version was out to smash SAMHSA projects. The trade-off was maybe better described as between AOT and “early intervention” for toddlers.
Doesn’t the very term peer also connote a “greater-than-peer”?
Report comment
The range and scope of mental patients and former mental patients, in terms of performance and achievement, are as varied and broad as they are with never-been-mental patients. This being the case, calling a person a “peer” because he or she has been imprisoned in a psychiatric prison at one time or another during his or her life is an out and out insult, or perhaps, the better way to put it is to say, it ‘adds insult to injury’. In a word, any you out there reading this should know, hey, in this sense, we’re no different from you. The mud (prejudicial predicament) of some “peer groups”, you don’t want to get stuck in, not if you’ve got any sort of destination whatsoever to be reached. If they’re going to insult you with a grouping like “peer”, there is no need to add to the insult by going along with the gag and insulting yourself.
Report comment
Sera, thanks for clarifying. Gee, I worked so, so hard at FAKING that I am a Genuine Mental Patient. I yellowed up my two front teeth and made them look perfectly cracked to imply poverty. I knocked down my apartment, downsizing it so as to make sure I appear poor as can be. I wear second-hand clothing since that’s what a marginalized person would wear. I post to MIA, of course, letting the whole world know just how pissed off I am. Perfect unemployment record for decades, and all those incarcerations….Never mind whether it’s true of not. i could be lying, couldn’t I? Maybe I am. I’m playing the part oh so perfectly, so convincingly, and now you’re telling me it’s for naught because some young whippersnapper just out of college can cheat through a test to get a fake degree in this? But I got a Real Degree in it! Paid a hefty tuition, Graduated with all the honors, too……
Report comment
Julie, I hear you. I think the only challenge with *no* training if we’re going to do this whole ‘peer’ thing is that *so* many people go through some of those life experiences and come out the other end all full of internalized oppression. I have to admit that I do find *some* training helpful on top of all that personal life experience to help work through some of that, think through what it really means to ‘be’ with people, be curious, support, etc. But overall, I appreciate your post a lot. 🙂
Report comment
One of the possible problems I see with peer workers is that if they haven’t had at least some basic training they can end up doing to others what was done to them. I’ve seen former “patients” who have been given the title of “peer specialist” simply because they are a former patient. They totally lacked any training but were turned loose on the people in the units of the “hospital”. Obviously, the Administration didn’t have any idea what peer workers are nor what we’re supposed to do. It was awful and there was more drama than you’d ever want to see. These people set staff against the “patients” and the “patients” against the staff. It was one, big pile of turmoil on the units on a daily basis. I finally went to the people up front in the Administration and told them that if they didn’t want a lawsuit brought by “patients” or family members they’d better get their “peer specialists” off the units. One such “peer worker” who hadn’t seemed to have resolved his issues about his time spent in the “hospital” seemed to be playing out his own stuff on the people in the units. It was very apparent that he liked the power he had over the “patients”. Fortunately, he no longer works at the “hospital” any longer.
I don’t believe that we have to get a college degree in order to be people who are willing to walk with people through their issues, but I damned sure do believe in some basic training, especially about self awareness and self understanding.
Report comment
The Downfall of Peer Support: MHA & National Certification, by Sera Davidow.
Is just the old: “Divide & Conquer”… applyed to… the mad idiots?
In the old days, was: “Divide et impera” (Latin).
Every good leader/ organizer/ militar had used that…. and worked… every time.
……………..
1) Who had the idea to “use/ exploit”: patients, ex-patients, trusted prisioners, ex-prisioners, trusted slaves, ex-slaves, mercenaries, local guides?
2) Who selects/ rejects them?
3) Who gives them the training, and limits their competences?
4) Who certificates them, or cancels theirs licenses (including automatic expirations/ add the need to do cyclical training… or else…)?
5) Who decides what are the criteria to qualify for a: “PEE-R”?
6) Can those “criterias” change with the seasons/ allow the the master subjectivity/ evil finger?
7) Has any of those “certified trained ex-slaves” achieved anything… other than 30 pieces of silver (Judas’s payment for betraying Jesus). Well… what do you call telling your master… that your “not-certified-peer” is not taking his/ her psychiatric medications?
30 pieces of silver was dirty cheap (at those days, for a rich person).
8) Will the masters of the slaves (the white coats that dictate/ force the peer rules), accept anything similar TO those PEER RULES/ Code of Ethics…. at their own jobs/ personal lives?
HELL… NOOO !!! NEVER.
9) Is there any future at “certified-official-legal-community-peer-support”?
Where are these experienced peers? What have they done? What are their names?
Did they done nothing of useful? Anyting that lasted? Nothing?
Of course… that was the idea. A few “sheep with guts”… to lead even more dumber blind sheep to the injections/ pills. Meat for canon?
From the text of Sera Davidow:
“Teva, Eli Lilly, Jaansen, Lundbeck, Otsuka, and Takeda”.
That is funny… i sent a poster (artwork), to MIA (that MIA never published), that putted that at the eye level. Not good enough? Yet is what is needed… to wake the sheeps?
Maybe they like more… Andy Warhol?
……………..
To Sera,
quote: “Sure, I had to dig around a long time to find an absolutely definitive statement saying that this MHA certification does not involve any sort of actual training from MHA, but that is indeed the fact of the matter.”
I am very sure of this: when peer training is done… health professionals DONT WANT peers to have ANY access… to any higher grade training. AKA… any training that would allow “peers” to make ANY competition with them (their own jobs).
This is intuitive enough?
Is the reality… after the blah, blah (sweet talk for dummies).
Anybody that has doubts… just try.
……………..
” Follow-the-money… ”
Teva
Eli Lilly
Jaansen
Lundbeck
OtsukaTakeda…
…that pays the: APA/ NAMIS,
that promotes the DSM,
that gives the guns… to all those fake doctors & remaining parasites.
Report comment
Why do you call them “certified, fully trained ex-slaves”? Who says they’re free? Basically they’re “good slaves” who are duly “grateful” to their masters and overseers. As a reward they are put in charge of watching over the bad slaves. When the naughty ones try to one away, they rat them out. In exchange they get all the table scraps they want, first pick at the cast-off rags of their owners and a warm place to sleep by the fire.
Report comment
Regarding your comment on “sheep with guts” I think a more applicable term would be “Judas goats.” A Judas goat is a real term used for a goat placed among sheep to lead them into a slaughter house. Because they trust the goat as one of their own they follow him peacefully into the place of slaughter. Otherwise they might panic, run around, and cost the would-be butcher lots of time and trouble. The reward for the Judas goat is he will be kept alive to lead more sheep to the slaughter.
Report comment
FeelinDiscouraged,
I dont pretend to be an expert about slavery. Slavery is a very old practice… and still exists to our days. There are reports of cases… every year.
So, allow me to try to explain: it depends about the country, the time and the local law. At some cases (in special circunstances), a male or female slave could be set free. In very rare cases, i suppose… and if slavery was the law of the land… it could require a special demand to the king/Emperor.
Anyway there are cases where slaves were set free and had the legal proof with them. So if they a person that was aa slave and set free (ex-slave)… if that person stayed at that place it would be illegal to make him/her a slave again. Safe in that regard, so to say.
But i heard that the ex-slave would not find easy to:
a) find a job;
b) buy land;
c) get any respect.
That because the free folks (the masters), would not trust the ex-slaves.
And is logic… they made the abuse of slaves… a way of life. Do you think the slaves have short memory? Years, decades of abuses?
Ah, tiny detail… the freed slaves, sometimes went into the business of “recruiting slaves”. In other words… used their experience “experts by practice… so they say”… to make new slaves, and make profits with it. Maybe very sad… but true. Dirty work.
Can a person go any lower?
Yeah, i have read (here at MIA), some folks dont like this kind of comparation… with slaves, or similar comparations… even comparations that are useful… at gaining more understanding of history, the commom problems, the common solutions, the generic needs if any measure of sucess is the goal.
Pity; Vanity, Show-off: “i am a SZ and proud of it, i tell my name is Homer Simpson; Cherry-picking: “my comment is better than yours”… yada-yada.
As i see it… is short sigth. Dumb. People that dont understand: 1+1=2 are dumb.
What does Homer Simpson? He divides. Of 10 (ten) he makes fractions of unit. Splits hairs.
And at the end of the day… Homer Simpson sees televison until he sleeps. At the sofa. tired and having done noting. All day long.
………..
Anyway… some people (at some countries), menaged to get away from psychiatric medications.
And some feel “safe”… that will remain like that… since they migth have family support, money, a job, or a good relation with the local psychiatrists.
But that is the exception.
At the end of the day, the SZ that care about the others (users in the system, and the thousands that will get in teh system), the ones that are willing to figth to improve things, and break this system… are few and between.
Report comment
A passionate man stirreth up strifes: he that is patient appeaseth those that are stirred up. -Proverbs 15:18
Maybe an outlet to offer competition to mental health america on a better national certification.
Better is the poor man that privodith for himself, than he that is glorious and wanteth bread. -Proverbs 12:9
I would work as a peer anytime before I’d sit behind a computer screen explaining to everyone the way it ought to be. Well intentioned peers go to work day in and day out and make change happen in the system all while facing stigma within system head on.
~ Pat H.
Report comment
Which in the end perpetuates the existence of that system.
You do know what they say about the road to hell?
Report comment
My parents always told me to be original and not to compare myself to others. So…I’m not interested in what they say. I’m interested in the good book and my dad.
Report comment
“Work” as a “peer”? How ironic.
All these careerists in the mental health system are an indication of the vastness of the extent of corruption there is to that system. It is no longer about “healing”/”curing”/”recovering” people from “sickness”, now it is about perpetuating itself into the distant future. Some people would fancy the mental health system ‘eternal’. Imagine, having had a “sick” designation is now the requirement for a job in what purports to be about “health care”. Certainly, somebody is fooling somebody else.
I’m very glad there are other pursuits one might engage in besides and beyond “mental health treatment” (torture, abduction, imprisonment, brainwashing). Some people enter the system at a very young age, and never leave it. I don’t think anybody should be condemned to the mental health system for life. The less time a person has to spend in that system the better. In the final analysis, I’m for dropping the loony bin into the trash bin of history where it belongs. Ditto the outpatient loony bin extended from the traditional institution into the community at large.
Report comment
Pat,
I’m not sure I’m totally following what you mean? I love to write and stir things up, but as you know, I also work in a world where many of us are out there doing the work in person, too.
I really don’t think there’s agreement on this national certification business, including that it needed to exist at all. Thus, I don’t know that the answer is to simply offer MHA some competition.
-Sera
Report comment
As far as I’m concerned Steve Harrington with the INAPS International association of peer specialists was on right path with national peer certification. I was bummed when INAPS national certification didn’t go forward. It was so much better.
Steve has the right personality and attitude to bring people together and make change happen.Steve also formed meaningful relationships with therapists, nurses, and dr.s. His way is realistic and ideally what I try to do as well.
Report comment
Sera is talking about important stuff. It’s axiomatic that people who care about maintaining the power to define and control others will either try to immediately destroy threats to their power (via castigation, mocking, ignoring, etc) or to invite potential threats into their ranks, give them minimal pay and a tiny sphere as a way of ultimately gaining complete power over them as a dependent employee. To the extent that those in power are putting efforts into co-opting peer support, it’s also axiomatic that those in power believe that that the idea of peer support is too powerful to simply mock, ignore, and destroy, and so they are forced to utilize a co-opting strategy instead. It’s great that we have Sera at MIA who is staying on top of this — Bruce
Report comment
I just read your latest book Bruce. I can’t remember the title immediately–something about moralizing the populists. Great book though! I need to review it on Amazon.
Report comment
Thanks Bruce! And thanks so much for your recent article on suicide, as well.
-Sera
Report comment
To the extent that those in power are putting efforts into co-opting peer support…
“Peer support” can not be co-opted, as the peer industry itself is already a co-optation of the struggle against psychiatric oppression.
Report comment
I find it very interesting that in the state where I live they are planning a certification program for “certified peer specialists”. The requirements as far as continuing education and professional development are concerned are totally outrageous in that they require so much time involved in attending things that you won’t have any time to do any work! A good friend of mine looked at the proposed requirements. This person is a licensed social worker and a registered nurse as well as a peer. This person said that the requirements are higher than that required of anyone in going into social work or nursing. They even require people to attend ethics classes and workshops, something that will be fairly difficult to do since we are a rural state with little access to formal education in the form of college classes etc. Don’t get me wrong, we must be ethical in our dealings with people but I don’t think that our jobs require us to attend two ethics classes every other year. And I don’t think that ethics change that much from year to year to require this kind of thing.
I don’t think that they will find people to be certified because of these herculean level requirements. Are they setting us up to fail before we even begin?
Report comment
Stephen,
If I had more time on my hands, I’d be fascinated to do some research that involves not only comparing licensure requirements between these various professions and the peer role, but *also* the logistics involved in meeting those requirements as they differ for each, *AND* how they’re applied… For example, I imagine a requirement that one put their licensure on ‘hold’ as a dentist is *likely* to bear many fewer actual risks and lower likelihood of abuse than for a peer role. Oy. What a mess.
-Sera
Report comment
I forgot to mention that each peer worker will be required to, get this, have one hour of supervision per week with a psychiatrist! I thought that any supervision given to peer workers was to be done by and with a supervisor with lived experience. I suspect that clinicians had a hand in creating this requirement in an attempt to control peers.
You’ve pegged it correctly in that this is just turning into one, big mess. And as usual, the people who will really be adversely affected are those still locked in the system.
Report comment
Food for thought. All these “peer specialists” are supposed to be “meds compliant” right?
In their drugged up, perpetually sleepy conditions most “consumers” will not be capable of passing these requirements.
I foresee a severe peer shortage in the future. Not that that peers have a real function to begin with. They want to have a token “nut job” with the real professionals to prove MI voices matter. Then they can exhibit the “peer” to other consumers on special occasions.
“See X was a good consumer who took her meds exactly as prescribed. X has good insight, believes whatever we tell her and is duly grateful to us. If you are good like X, you can have a job working for us part-time at 10$ an hour. Provided you willingly self identify and appear in public wearing ‘Kick me, I’m bipolar!’ t-shirts at our stigma reduction events.” 😀
Report comment
I am not meds compliant. I threw the bag of drugs they discharged me with in the trash when I got away from the “hospital”. There are not many peers in my area so I have no way of knowing if you’re correct or not from where I’m at. I know two peer workers with one being very compliant and one who takes nothing at all, like me. I’ve wondered about this myself from time to time. But of course we’re not supposed to talk about the issue of who takes their drugs compliantly and who doesn’t, or at least this was the instruction that I received from my training. It’s made a personal choice issue.
Report comment
I don’t think that they will find people to be certified because of these herculean level requirements.
Sure they will, professional ass-kissers are a dime a dozen.
Are they setting us up to fail before we even begin?
Only if people agree to participate rather than raise hell. Once you apply for their certification you’ve already failed in any real sense, as you’ve agreed to be a shill for the system and work by their rules.
Report comment
I’d like to know, too – how do you get 3000 hours of service – before certification?
Every peer program I know (granted that’s very few) requires in-house training modules, tests and certification – and that bar is pretty high, as well.
It’s probably cheaper and easier to get a university degree and hang out a shingle.
Massage therapy requires 80 hours of pracs. A chiropractor does 180 hours? (these are just quick googles), a naturopath requires 450 hours of supervised clinical time. An acupuncturist does 1-2 years of training and 30 hours of practical clinical experience (varies from place to place. I can become a basic auto mechanic in 6 months. Why, oh why would I do 3000 hours of Hello to get this stinking certification?
3000 is 75 weeks at 40 hours a week. Most peer specialists I know start out part time – so – at least 3 years of pracs before the test? Volunteer is okay? What qualifies? Hours spent on a helpline? Is what I do for 16 hours a week on the internet considered peer support? (probably not, since I help people come off their meds safely using harm reduction).
And the fear, the danger, is that once this program is accepted by one, by two, by a few places – it may be required in all of them. Or at least all of them with corporate masters. (the slave language is apt)
Report comment
What you’re seeing was completely predictable. The conservative end of the movement wanted nothing more than a job and pay WITHIN the system. Now that they’ve got it, it is no longer about supporting those who have experienced the mental health indoctrination system, it is about being a specialist in a specialist field, and that specialist field involves perpetuating the mental health indoctrination system. I don’t see a lot of good coming out of developing a cadre of mental health indoctrination specialists out of former victims of the indoctrination system. They’ve got their careers, and the pessimistic view of mental ill health that supports their activities. The fact that you’ve got “peers” doing as much, and sometimes more, than conventional mental health professionals is something the system always tries to avoid, I mean, given this sort of role reversal, what you have is pure farce. Sure, people can change “uniforms” and “roles”. We always knew that. Adopting other roles, outside of the “norm”, given a certain conventionality developing, that can be a problem. When this medical specialty, is not even really medicine, and the medicines people are being fed are actually toxic poisons, waking people up is the last thing in the world such a system would tolerate.
Report comment
Good point!
Report comment
The conservative end of the movement wanted nothing more than a job and pay WITHIN the system
Why would you characterize such people as part of “the movement” in any way? — these are the sort of people who destroyed the movement. This is treachery, not a simple difference in philosophy.
Report comment
I’m not really sure how to put this exactly, OldHead. I would align myself with the radicals, but, surely that doesn’t describe everybody in this business. People say “peer movement”, people say “consumer” movement, people say “recovery” movement, people say you name it movement. I wouldn’t call myself a part of any of those movements.
Again, there were always these divisions, and I would be one to align myself with the radicals. Did we have a mental patients’ liberation movement? The terminology seems to have changed. I’m very wary of saying “our” movement any more because, yes, that movement has been destroyed, but I think it had a little help from people you wouldn’t expect to be doing that sort of thing, that is to say, I think some people just got exhausted with what was going on at one time, and decided to take the easier route, and that route, from one perspective, could be considered betrayal.
There are differences of opinion, too, and there are people who actually want to play the “mental patient” role. There are others who want to play “health care provider” for people in the “mental patient” role, even some who were once in the “mental patient” role themselves. There are people, in fact, praising the authorities for violating their rights, abusively manhandling them, and imprisoning them. There is this “herd mentality” on which I am going to remain silent.
“Alternatives” to “forced treatment” were always part of the problem, and the movement was to some extent intent upon creating these “alternatives”. The problem with “alternatives” is you don’t have “alternatives” without that thing that you need an “alternative” for. Once ‘in the business’, it’s easy to forget where you came from. We never needed “alternatives” to “forced treatment”, we needed an end to “forced treatment”. “Forced treatment” itself is the imposition of unwanted treatment.
Report comment
The problem with the term “alternative” is that it implies that psychiatry is filling a need, but not doing it well enough, hence the need for different approaches. But psychiatry only claims to fill a need; it’s actual purpose is social control. Like racism, concentration camps, etc., we don’t need “alternatives,” we just need to end it. If on the other hand we’re talking about helping people with problems, that’s a whole different question, unrelated to psychiatry.
Report comment
Okay.
I repeat:
“Forced treatment” itself is the imposition of unwanted treatment.
“Helping people with problems”? I’ve not found the system (or anyone connected with it) very “helpful” at all. I think we’re back to Nomadic bashing self-reliance here while I’m all for self-reliance. They’ve got a “helper” industry now that’s anything but “helpful”. Find yourself homeless, down and out, watch out! Here come the vultures, but these vultures have human features. The vultures, mind you, are anything but broke and homeless, no, broke and homeless pays their salaries from now to never. All sorts of people today are being screwed by “help”.
Report comment
Not sure what we’re supposedly disagreeing about.
All I’m saying is that any “movement” based on giving people emotional support, etc. is separate from one dedicated to ending psychiatry.
What I was alluding to is the frequent insistence that if you attack psychiatry you are obliged to provide an “alternative,” and pointing out that, like Szasz said once about mental institutions, the “alternative” is NO mental institutions, just as the “alternative” to concentration camps is NO concentration camps, period.
Report comment
I didn’t think we were disagreeing about anything.
I’m not dividing up “movements”, but if there were one dedicated to ending psychiatry, I don’t think it would be averse to lending people emotional support.
I have no argument with the Szasz statement, but when people talk “alternatives” they usually mean options over and beyond institutionalization with the force that goes along with it. No institution is certainly the preferred option as far as I’m concerned. I don’t think anybody is obliged to provide an “alternative” because that is like this business of “supports” in the community. People say you need “community supports” before you can shut down institutions as an excuse to build the community mental health gulag. No you don’t. You just need to empty the building, and close it down. The community mental health act is a law we could live better without.
Report comment
This:
“More detailed knowledge of clinical interventions will be needed so that peer specialists know when and how to support individuals in treatment. For example, Hendry explained, research has shown that when an individual is receiving DBT for a personality disorder, peers must have enough knowledge about the phases of DBT to avoid “getting in the way.” This can occur when the individual’s therapist “withdraws,” leaving the individual “alone” to face challenging situations as a means of developing essential distress tolerance and emotional regulation skills. Peers who recognize the phases of DBT treatment can adapt their interactions with the individual in ways to support the therapeutic goal.” –
Is disgusting.
Thank you, Sera, for once again speaking truth to power and keeping the flame alight.
Report comment
Thanks, Steve! (And Agreed!!!)
Report comment
Great article Sera. Hope it helps. FWIW, 2 kinds of peer support::
#1. People with lived experience support each other to achieve self-determined lives of their choosing.
#2. Providers purchase lived experience to support compliance, endorse products and increase market share.
#2. (Urban slang) Thugs who don’t give a shit use folks who don’t know shit to sell bad shit without paying shit.
Report comment
Maybe #1 should be called something other than “peer support,” maybe just “being human” — let them try to officially certify THAT.
Report comment
Yes, exactly! That’s what it meant originally, that’s the whole point.
Report comment
In a nutshell… “they” (those who promote/ pay/ make the rules/ control/ select/ train/ aprove/ supervise… in the end… can do what they like.
When a user of mental services applies to be a “pee-r”… there is a “Code of Ethics” to sign. And it may vary… but they require to know you very well, you must tell all the bad things you done at your life.
Those who have been at the university, even at medical training, know that i going too far. No freshmen/ freshgirl (that i know), has to go under that kind of degradation.
Not to study for psychiatry;
Not to have a public job (even a high grade politician).
Is the kind of thing used with…. drug addicts, or convicted criminals, ex-whores applying to clean houses?
………….
Well, see for your self:
“Certified Peer Specialists will maintain HIGH STANDARDS of personal conduct in a manner that fosters recovery”.
Well, Stephen Gilbert has already pointed that: we have to be more holy than the POPE (any psychiatrist, any nurse, any social worker, it seems). Certlainly… the Peers will have to be more “SAINT” than ANY familiar that IS part of the NAMI.
……………
See… they gave you grabbed by the B… you know what 🙂
Yet, you may think, i myself have noooothing to hide.
Well… or you are dumb & have not lived…. or you are a wannabe Jesus Christ, yes?
Is the Code of Ethics “fine stuff à la Joseph McCarthy”?
You can look for McCarthyism here:
https://en.wikipedia.org/wiki/McCarthyism
……………
Checklist: signed copy of Code of Ethics Form, with the lived experience and recovery journey to include the date when your recovery began.
Began, sir!
You will NEVER be fully 100% certified recovered… aka: “normal”. But… you can fall into “sins” again. And again. After all you have a genetic/ chemical/ dopamine/ serotonine/ broken brain/ imbalance/ a major-serious-grave DISEASEEEEE.
Is your new “yellow star” at your chest? Dont worry… now you are a “ultra-THX-certified-support-peer-allyed-in-recovery”.
So, some Code of “Ethics” examples:
1) “Certified Peer Specialists will actively pursue recovery in their own lives as well as ROLE MODEL recovery for others.”
……………
2A) “Certified Peer Specialists will keep current with emerging knowledge relevant to recovery, and openly share this knowledge with their colleagues and those they serve.”
2B) “Certified Peer Specialists will keep current with emerging knowledge relevant to recovery, and openly share this knowledge with their colleagues and those they serve.”
About 2A & 2B) is worthy to note: that health professionals DO NOT WANT… peers to have acess to higher grade training (the same stuff that: psychiatrists/ psychologists/ occupational therapists have).
Example: they do not want peers to have acess to tools to deal with: cognitive behavior therapy, crisis interventions or emergency psychologic support.
Wouldnt those 3 tols would be useful to both peers and users?
Nah. Dont create competition…
Is not much diferent to forbid the translation of the Bible from the Latin. That gave teh priests… more power to control the sheep.
……………
So, remember the quote from this same MIA article:
“More detailed knowledge of clinical interventions will be needed so that peer specialists know when and how to support individuals in treatment. For example, Hendry explained, research has shown that when an individual is receiving DBT for a personality disorder, peers must have enough knowledge about the phases of DBT to avoid “getting in the way.” This can occur when the individual’s therapist “withdraws,” leaving the individual “alone” to face challenging situations as a means of developing essential distress tolerance and emotional regulation skills. Peers who recognize the phases of DBT treatment can adapt their interactions with the individual in ways to support the therapeutic goal.”
Patrick Hendry. July 2016.
……………
Now you get it?
If you get similar education (they assume peers will (with time), understand/ dominate those tools. And peers will see the “health profissionals have no cloths”. We can do the same stuff they do. Or better. So lets deny peers acess to those tools. Better yet… lets deny them acess to that education/ tools… and when fits our agenda say those “nice things”, about THOSE HARD WORKING LOW-PAID peers. WIN-WIN!
And there is more evil than that. “They” dont allow you acess to training skills, they dont sahre what they know, but they want (DEMAND) to know “what you know”.
VERY Ethic??
Or a LOSE-LOSE-LOSE situation?
……………
3) “Certified Peer Specialists will respect the privacy and confidentiality of those they serve”.
Seems basic, yes? Huge lie. HUGE.
……………
4) “Certified Peer Specialists will never intimidate, threaten, harass, use undue influence, physical force or verbal abuse, or make un warranted promises of benefits to the individuals they serve”.
Wait?! Psychiatrits, doctors and nurses… dont do that? Ask Julie.
……………
5) Certified Peer Specialists will never engage in sexual/intimate activities with the consumers they serve.
God, i have sinned 🙂 Me and 999 hundreds thousands millions humans (give or take).
……………
6) “Certified Peer Specialists will not exchange gifts of significant value with those they serve”.
Only the money my SZ fellows never payed me back, would allow me to buy me a Samsung SSD.
I would do it again 🙂
……………
7) “Certified Peer Specialists will not abuse substances under any circumstances”.
What do you know? At Australia the wine industry began with doctors planting grapes to make wine. And for the Homer Simpsons: to make wine… we must taste it, and be good at it.
There are (at the UK), 1 studies of alcohol made with male doctors.
You may bet, they never drunk wine?
Wrong, sir.
Look again:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2541157/pdf/bmj00460-0027.pdf
“Mortality in relation to consumption of alcohol: 13 years, observations on male British doctors”. By: Richard Doll.
And dont try that at home, kids! Is just for: high Ethics hardcore doctors. At page 3 of the PDF, at the button left… shows that not less than 154 UK doctors admitted having drinked more than 43 (forty three) units of alcohol at 1 single week (ages: 29-42 years old).
And at the UK, they dont drink that much. Other countries drink more.
……………
Lets replay (is not a typo):
“Certified Peer Specialists will not abuse SUBSTANCES under any circumstances”.
Have you seen “Doctor House” (the tv series)? He “avbvbuseedd” pharma pills?1? 🙂
Only every day of the week.
……………
More could be said? Yes, but is already a lonf post. You got the idea (or you belong to the APA).
The psychiatry likes using the peers (goats). This seem not logical… until you see the big picture.
Frank helped in that, saying a part of the “movement” wanted that peer path (the money). Compromisses were made, for Pharma money? Very Ethic 🙂
Under Influence?
Report comment
Never abuse substances? Then how are we to remain meds-compliant? What a bunch of hypocrites and liars!
Report comment
AntiP:
Example: they do not want peers to have acess to tools to deal with: cognitive behavior therapy, crisis interventions or emergency psychologic support.
Wouldnt those 3 tols would be useful to both peers and users?
No these would not be useful if presented in the context of “mental health.” It is not a special skill to give one another emotional support. It’s part of being human, at least in a less alienated society.
Report comment
oldhead,
That peer “thing”… is complicated. Unlike the DSM-5, that the APA makes… the DSM-5 (USA version), is very similar of the DSM-5 used at Germany (translated by well know psychiatrists from Germany).
Now… peers laws/ rules/ code of ethics/ pre-requirements to get selected/ the payments/ the working hours/ the limits of what a peer can do (and is forbiden to do), all that (and more)… varies. Can even vary at the same country, you know that.
To add to the confusion…
What is in the papers is not what is done (in practice). By both sides. So there can be a extreme variation.
My congratulations to those peers that despite to all the pressures done against them… still work: FIRST AND ALWAYS for the users (users with SZ and alikes). Surely… the peers cannot tell their bosses (Pharma/ APA/ psychiatrists/ supervisor(s)/…/ that they (the peers themselves), dont religiouly take their daily Risperidona, yes?
…………
Well, that is not my area (the mental tools/ mental skills), or to: name/ translate the name those specific tools/ mind skills/ mind techiques used, i would look like an idiot. I gave those 3 examples to “put the ball in the park”. Those who work in that are will know that was/ is true.
As of what would be useful in practice for peers to do… that is not allowed at ANY peer organizations (now or soon), i think.
at Sera article… did you saw the reply (or lack of it), of the “peers organizations” to the events Sera wrote? Seems promising? Or a total failure?
So, can “peers organizations” improve?
Keep dreaming (not you oldhead)…
…………
Quote from oldhead: “It is not a special skill to give one another emotional support. It’s part of being human, at least in a less alienated society.”
re: Well, my English is so bad that i may miss your fine points 🙂
We need find what we have in common, unite at that points, and work/ help/ support those that are willing to make good & lasting changes.
If that is a skill? A superpower? Ntural… or to be learnead… ai dont know.
Some people can do that, and are even good at it.
Some people suck out the energy/ time/ goodwill of the others near. Is that a skill?
At one point… i confrontated a health profissional saying something of the likes: “you do this (i explained in detail), and you must un-learn to do that, as it drestroys comunication.
Note: i did not knew (i still dont), it was something “natural” or a “learned skill (by life and/or university degree). Anyway, the result was the same 🙂
Report comment
Dear Sera: This is a most interesting article on a really important topic. Thank you! One thing that struck me is your description of Mental Health of America which was originally founded by someone with lived experience and is now run by the father of someone with lived experience. Does this pattern also apply to the membership of the Board of Directors and staff? What about NAMI? Regardless, I think its high time we organize to create a accreditation process for so-called mental health advocacy organizations. One obvious criteria for certification would be more than 50% of the Board is made up by people with lived experience, and by that I mean people who have been on the sharp end of the needle. Another criteria would be funding sources. No organization receiving funds from big Pharma or other medical technology company could be a patient ‘advocacy’ organization. Consumer safety organizations would never allow such conflicts of interest. Why do we allow this astro turfing to take place in the field of mental health? Organic farmers banded together in Oregon during the seventies to form T.I.L.T.H., an national certification process for organic farmers? This took foresight. To this day, despite strong industry lobbying, marketing of organic food is strictly regulated by experts with integrity who embrace the stewardship of the earth, water, and soil as well as the safety of consumers as their highest mission. Why can’t we do the same and shame NAMI members into accepting that their advocacy organization is little more than a front for big Pharma and advocates for AOT such as Jaffe?
Report comment
I see Jaffe as the boot-licking hunchback assistant Igor to Lieberman’s evil mad scientist. Lieberman better keep Igor Jaffe away from his pickled brain collection. You know how hunchback assistants are bad about breaking “master’s” jars with brains in them. Lol. 😀
Report comment
Quote from FeelinDiscouraged: “All these “peer specialists” are supposed to be “meds compliant” right?”
re: There are peers at many countries, and even within the same country (as the USA),… each state/ province can have variations at basics:
peers pre-requirements, the code of ethics, daly requirements: “do-this”; “dont-do-that”… or else 🙂
Many peers life are a open book, the code of ethics if applyed to the health professional would put most out of the business. And a peer not complying to the the code of ethics is reason to get fired (and that is in the signed papers of many peers).
So, if the supersivors/ bosses of the peer want (if a peer becomes problematic… if he helps the regular users too much, the peer can get fired quick and legally). They (those who have control of the peers, know tto much about them). They demand that information from the start, and all the way after.
Those who had read “Anatomy of a epidemic”, by Robert Whitaker, know that a page (cant remenber the number), he mentions a peer, that someone acused of beeing NOT-compliant with psychiatric medications. Quick result: the peer was fired (put out of peer job).
You migth recall Julie posting to apply for jobs/ interviews… as a experienced user. You know the results.
Psychiatric drug compliant… is among the first questions a user is asked (even at written anonymous queries). Why? Likely because: if the answer is NO (not compliant, not taking the psychiatric drugs… THEY WILL REJECT ALL YOU SAY/ WRITE after.
………….
That said… ex-users are not necessarily more dumb than the psychiatrists 🙂
Now… there are known posters at this MIA site that say:
we should: be vocal, be open about our secrets, be honest to reveal all our weak spots…
And then what? That information wont be used against the users/ peers?
Nah, never was done in the whole world history (IRONY) 🙂
………….
Now, lets forget for a moment the sheep and dumb sheep… lets look at the wolves for one moment, shall we?
You know Joseph Bierderman? He is quoted at least at 10 pages at “Anatomy of a epidemic”, by Robert Whitaker. And if you look how Joseph Bierderman behaved at legal courts (there are court transcriptions at the net), you will see the same techniques used by those acused of to be hardcore Mafia hitman.
That is telling? Should be, for those other other than the useful idiots.
Now… look at Joseph Bierderman wikipedia page:
https://en.wikipedia.org/wiki/Joseph_Biederman
Can you even see his birth date? No.
Does he seem a very important person? No.
Now go to re-read “Anatomy of a epidemic” again… and take your own conclusions. Joseph Bierderman is no sheep.
As for Joseph Bierderman and…. lawsuits… courts… lies… and pretending to know nothing… and having no power… =) Look at the internet.
Well what do you call to that? That he was born yesterday? Nah.
Report comment
Frank,
I read your post. Quote: “People say you need “community supports” before you can shut down institutions as an excuse to build the community mental health gulag. No you don’t. You just need to empty the building, and close it down.”
re: Well, is possible similar things/ laws/ ideas… done at different countries have very different results.
For example the very same book published at one country can be a best seller and distributed at the otehr country can have average sells.
May point… at some countries… there were a serie of laws that wanted to close the asylums, and/or parts of the general hospitals, or some big psychiatric hospitals/ wards. Maybe at the USA also?
I heard… have yet to verify… that years after that was done… the reality (not the propaganda), was the measured effect (dont know any numbers yet), was worse mental and physical health (or even more deaths, then expected).
I am not arguing this is good, that was bad, the ideal is that one. No.
My question: and you know that not all persons that passed by the system kept their mental capacities as well as you… is this:
do you have a link or something pointing that way that i can look?
I say this because many familiies already rejected them, dont want them near. Some become homeless… with all that carries… even dying at a colder nigth.
Not attacking you, just trying to learn.
Report comment
I don’t need to be pursued by the system into the community. There was a time when the system let you alone after discharge. No longer. Now there are assertive community treatment teams, group homes, assisted living facilities, etc. Assertive community treatment teams make sure “consumers” don’t forget to take their psych-drugs. Group homes have loads of regulations; group homes and assisted living facilities have “medication” queues. I’d say it’s up in the air as to whether “care”, or the lack thereof, is what’s killing people.
Italy, for instance, made a commitment to closing the asylums. In that country you have Basaglia Law or Law 180. Now I’ve read British accounts questioning the extent to which Law 180 has benefited people, but these reports seem to be biased in that they have more to do with their own agendas for back home. The write up about Law 180 on Wikipedia is quite positive. I’d say the problem is actually that more countries are not willing to attempt something so bold rather than otherwise. Things are worse, for instance, in the USA today than they used to be, at least in my opinion. I’d say this is because our country is so feign to try anything outside of the customary, or anything that might threaten drug company profits for that matter.
https://en.wikipedia.org/wiki/Basaglia_Law
Report comment
Tanks Frank, i will take a look of that law effects.
Report comment
The most interesting thing was the comment that the “private sector” required this kind of national certification and guidelines. I foresee a future when private physicians, hospitals and clinics can bill individuals or insurance companies for services provided by a peer specialist. I’m not against peer specialists being paid, but think about it – there will be a “supervising” psychiatrist or psychologist who will be able to bill for their entire usual hourly fee for services provided by a peer specialist. Peer specialists have little formal education, no student loans and are generally paid very little. What an incredible money maker for the doctors and hospitals!! (When I see a nurse practitioner, the fees are the same as for the doctor, FYI)
Report comment
OMG Julie. Nail on the head.
So the “overseeing” doctor / specialist whatever gets to BILL for peer services?
OMG that’s like a corporate wet dream!
Report comment
Frank, Sera, Gilbert, anyone ?
A small question… if you have the time?
What do you think (after reading the posts of this article)…. that nobody seems to be surprised with the lack of “response” of Peer organizations?
Quote: “Unfortunately, no peer-run organization has taken on this challenge yet.” – Patrick Hendry. ‘An Open Letter to the Peer Community’ July, 2016.”
So…. no feedback, of the reasons of the… “silence”?
………………..
There was one post, of Lauren Spiro, that wanted a “peer make the rules, peer has all the control”. Yes, but that SINGLE post seems to see the moment… as seeing a… “business oportunity”. A “variation”, so to say?. As Lauren Spiro was silent about the problems/ issues associated with this “peer business”.
First to see the problems… THEN to see the solutions, yes?
………………..
Other than that, the USA are known as a country where a lots of statistics are made, yes?
Where (links) are the best examples of statistics complied by peers themselves?
So i can see what the users of the peer services…. seems to want?
Thanks.
Report comment
Not all “peers”/ex-patients work in “peer”/ex-patient run programs (respite centers, drop-in centers, and the like). Community mental health boards are hiring “peer”/ex-patients, too, and sometimes getting “peer” jobs into the system can be a struggle in itself. Getting jobs after certification, given the nature of the system in some places, can be problematic in itself. Prejudice exists. “Peer-run” operations and the mainstream system find themselves having, to one degree or another, to work together. For the ex-patient, sometimes, its all about the much more basic issue of having a steady job and salary. I see a bit of corruption in all this, with the “peer”-run programs more and more coming to resemble the conventional system. Sera herself works for the Western Massachusetts Recovery Learning Center, in Northampton, Massachusetts, and if there’s one place where the corruption is less than elsewhere, I’d say it’s there in Northampton.
Report comment
Thanks Frank 🙂
Western Massachusetts Recovery Learning Center, in Northampton, Massachusetts, yes?
I went into the dicionary… They have a site:
http://www.westernmassrlc.org
And at a page there, quote:
“AOT stands for ‘Assisted Outpatient Treatment… forced outpatient treatment.
… Currently, 44 states in USA have AOT laws.
Massachusetts, Connecticut, Maryland, New Mexico, Nevada, Tennessee, do not”.
So… at the USA, when that glossary was written: 44 states… used the “long arm of the needle” 🙂
And 6 USA states… did not (so far). Lets see for how long.
Does not look promising. I dont undestand why some article makers at MIA seem so optimistic.
Report comment
Malcolm spoke of “house negroes.” For the most part “peers” as referred to here are “house mental patients” — given a few extra privileges and pats on the head to keep the “field mental patients” in line.
Report comment
Yep. Tasha Tracey at Bipolarburble makes a good lil’ brainwashed sheeple to keep others in line. I don’t troll, but if I did I would spend time on her site. She’s so dumb she would make an easy target!
Report comment
“Tasha Tracey at Bipolarburble” is that thing still around !?
What an A-hole that one is. Defending Eli Lilly after the Zypexa crimes.
Eli Lilly – A Drug Company Without Horns and a Tail – HealthyPlace http://www.healthyplace.com/blogs/breakingbipolar/2013/04/eli-lilly-drug-company-without-horns-tail/
More on Zyprexa and Eli Lilly http://psychrights.org/States/Alaska/CaseXX.htm
I went to that Tasha Tracey website and
“Your comment is awaiting moderation”
That figures.
Report comment
Cat,
the Natasha Tracy, mencioned…
1) Her blog, “Bipolar Burble,” has been named a top 10 health blog by Healthista, Health.com, Healthline, and many others (from Amazon).
2) Her long-running blog “Breaking Bipolar” on HealthyPlace has garnered back-to-back Web Health awards (from Amazon).
3) Her book at the amazon USA, has for 5 star: 83%. In case you dont know… many goods products dont get that % of 5 stars.
For example: “Anatomy of a epidemic”, as i write this (at the very same site), has 80% for 5 stars.
And more? She is “easy to troll”, yes?
No at this amazon review:
https://www.amazon.com/gp/customer-reviews/R28QBC9IGGGLO0/ref=cm_cr_getr_d_rvw_ttl?ie=UTF8&ASIN=1539409147
The review putted Natasha Tracy, and her blog down…
Yet… look at the 5 dog-alikes comments that folowed of that 1 star review. Harsh comments. People here at MIA are not trained to handle nothing near that.
Au contraire… we have persons at MIA that say: “tell your name, post publicly your picture, have guts!”
So, despite here at MIA many persons say should should be “saints”… The reality is ugly out there. Just saying…
I dont say to poster to have fear and back off. No.
Just to open the eyes and smell the coffee 🙂
Report comment
And yet Tasha Tracey is indeed a moron. Her arguments are inconsistent and often incoherent. She has earned the status of an a “adult baby” and no doubt finds it useful for her nasty behaviors. Often she will declare she is full of hatred but can’t help it–it’s just her “bipolar” making her do it.
Likewise she is unduly suspicious and has weird thoughts about some massive underground conspiracy of the antipsychiatry movement. Don’t know what’s in that funky cocktail she’s on but it ain’t working! 😀
No doubt there are other NAMI zombies who enjoy their status as fat adult babies. Some of them may have given the five star ratings, though it’s doubtful they read the whole book, drugged up messes that they are.
My guess is that Big Pharma-Psych Industry have surrounded their prize pet with a phalanx of professional trolls. Maybe they’re grooming her to fill Patty Duke’s shoes as Poster Child–Shill at Pharmaceutical conventions disguised as “education.” Thanks to her chemical lobotomy she’s not good for much else!
Report comment
Independent Living Specialists – It’s Time We Made the Shift,
http://peerlyhuman.blogspot.com/2017/04/independent-living-specialists-its-time.html
Report comment
(re: Funding independent, self-governing peer support)
Report comment
Well I have done my tiny bit of online activism for the day! Everybody reading this, use the link AntiP provided. Go to the negative review of Tasha Tracey’s book. At the end, click on Yes when it asks if you found the review helpful. If 20-30 of us do so, the 1 star review will go closer to the top. In spite of the nasty comments below (probably scripted.) And no names necessary! One click is all it takes.
Report comment
FeelinDiscouraged,
I did not lost my time at Tracey blog, because:
a) I have no doubt Tracey does not allow any negative comments at her blog.
I not going to argue if bipolar or SZ do exist or not (i leave that for those who like it).
The real persons (diagnosed bipolar), i had met at my life, despite seem (at their good time of the day), normal (or even very inteligent), are not reliable.
B) I explain: some bipolars (and often), say/ do things that hurt the feelings of their former friends.
Now… what do some bipolar say? That is “their disease”, they cant control themselves sometimes and they “say things”… that hurt.
Teh bipolar are (at some point)… aware they hurted other people… but they think they have wide rigths. Their friends should had… “forgived and forgeted”.
And that “forgived and forgeted”… i DO-NOT-AGREE.
SZ or/and Bipolar should not be forced to get injected with psychiatric drugs!
But… both SZ or/and Bipolar… should be fully responsable/ even legally accused for their proved bad actions (if any).
……………..
Due to a) and b) and more…
i dont have time to deeper try to understand Bipolar people.
Both SZ and Bipolar people have qualities and faults.
That is not a big problem.
The problem is there are so few… willing to make a regular commitment to help others (SZ and Bipolar, and such).
……………..
As for Tracey says/ supports one thing and does the opposite… The actions, the final result prevails. Always.
So… does the PHARMA/ APA/ NAMI supports useful (to-hire) idiots? Yes. Hire Tracey she is for… 🙂
Report comment
🙂 Some of the reasons people taught to play the role of the Bipolar or Schizophrenic Madman/Woman can’t have decent relationships very easily is:
1. They are drugged up all the time. Alcoholics and crack abusers aren’t good company. Neither are psych drug junkies.
2. The person playing the Bipolar or Schizophrenic keeps using the “illness” as an excuse to behave badly whenever it suits their purposes. Instead of Flip Wilson’s line, it’s “My mental illness made me do it!” As long as they show “insight” and stay drugged people are taught to be nice and tiptoe around their personalities. But in the long run patience wears thin.
3. Most people are (understandably) afraid to have relationships with junkies who self-identify as nut jobs. Those that do get involved often are looking for a partner to abuse. After the divorce/break-up they frequent forums and troll blogs to post rants. “My crazy ex and all bipolars are evil and mean as snakes! They should be cut apart with chainsaws and left for crows to eat!” Uh-huh. Like they’re the epitome of all that is cuddly and loveable. People that are good and nice don’t post that crap. 😉
Report comment
You hit the nail on the head Feelin.
The healing cannot begin until I, as a formerly diagnosed “bipolar,” take responsibility for my moods and managing them. Taking responsibility for my words and actions is the first step – becoming aware of when and how I have hurt others with my words and deeds. Acknowledging that I am not the only person in the world with feelings – and learning to be sensitive towards others.
It is a life’s work, really – but it is possible. And it is the largest, most important step towards “undiagnosis.”
Report comment
FeelinDiscouraged,
The reasons can be many, but the results are similar. Psychiatrits, nurses, NAMIS, and the whole circus help, yes…
a) Many of teh diagnosed/ injected… never marry, and even if living together, they avoid to have kids (family, NAMIS, social pressure, lack of $…);
…………….
b) They Feel/ think like second grade citizens, not worthy of spending time/ effort/ care with them. Is sad;
…………….
c) Yet more sad (but i have seen that), they make excuses. Not honest excuses. Like: “i do that (evil/ non-sense) thing and it does not work, i can always say:
“i can do no better, i am just a: “_____”.
Yet… they knew they crossing the line, from the start point.
Honest people dont do that… injected or not.
…………….
d) They have troubles finding/ keeping a job. Part is stigma, i know.
Yet… a hidden truth… are the priorities.
Dont know where some learned that… but if asked they say: “I have no power”. Yet fot what they like to do (i wont mention what), they always have time/ money/ and no doubts/ no concerns. What about working hard? Ah… well… excuse number 12578 is… 🙂
…………….
e) In the end, all of them agree there are differences. But most (almost all), wont help others. Even those that have the same problem. Or the new generation that will be injected.
And that… Mr. and Mrs. “Peers”… the above… remains, with or without you.
Priorities? Keep a job is first, yes?
“The money or your soul”, like they used to say back in the street robberys in the old days.
Or was: “The cellphone or your life”?
Something like that.
…………….
f) Yes, love can turn into hate. And wise persons shoud know it from the start.
Yet, DSM does not like emotions. And emotions are something that even great persons excel. Is not easy. Yet… at more developed countries people are so out of the touch with reality that see verbal/ written abuse/ or even the truth… as worse then death/ being injected.
Reminds me Homer Simpson.
Report comment
Doh! 😀
Report comment
I personally am a fan of the new route to certification.
I have gone to two interviews for CPS training, one as recently as a week ago. Both were disappointing. The first time the interviewer told me I “talk too smart” and at the second one I was told they only take people who are already working jobs as peers who need certification. I had previously searched online for peer jobs and found I couldn’t work one without the certificate. When I pointed that out they played dumb about the catch 22 they were creating.
I can not get access to a peer for my own recovery due to the shortage of them in the field. There are a lot of jobs that are unfilled due to my local chapter not training more people. The new certification would help fill the void. I don’t think going online is a negative, rather it eliminates transportation issues.
I plan to apply to this new program and hopefully it will be a way for me to get training, certification, and a job without having to deal with the double speak of my local organization.
Report comment
It will only continue to downgrade any quality and integrity of the peer role. We already know that CPS trainings are *HUGELY* problematic from states like New York. People *NEED* to gather in person and really grapple with the point of this work together. On-line simply doesn’t work.
Failed local CPS systems is not an excuse to further the failure with a terrible on-line system.
Also, you seem to misunderstand this national certification business. It’s only a test (that you have to pay a fair mount of money for). And if you don’t have any in-person training, you may not even qualify for it.
This is a money making scheme that will continue to do harm to any value peer roles actually have.
-Sera
Report comment
From the point of view of one who was a CRC (rehabilitation Counselor) and has been a CPS for the last eight years at a homeless shelter, one issue that is important is unionization. Another issue is management. Both Mangement and SEUI just do not know what to make of me (us?). One social worker/ supervisor wanted to push me out the door and then the local union rep was willing to open the door. This was more than three years ago but I have stuck around.
When I started another guy joined me as a PS but failed to complete the CPS training.
I was offered more hours but declined the offer because management were not honest with me. Soon after this a new CPS joined. A new type. She was a politically appointed PS. A real insider with good experience and good at supporting folks. After a disagreement about ethical treatment of shelter guest between me and management. I was shown the door. I learned that being driven by values and acting on these values can put your job at risk. Not being politically connected I needed the union to help me to stay at work. When I came on board I was on SSDI and not politicallt conected. Uncertainty is something I live with. Not all Peers are good or bad. Most of my days are good but I have had a few bad ones. Treating the homeless folks fairly is not a what I consider a bad day.
I am now on my 5th social worker/supervisor. I am keeping my fingers crossed. I see my work as a chance to reduce the mortality associated with homelessness. But, ignorance of some campus police, mental health workers and clinicians is hard to overcome. Sometimes I feel instead of studying rehabilitation counseling, spending time getting politically connected might have been a better way train for this particular position. My advice to a new PS is learn about self care. I went through some burn out. I take most of the trainings available. The steps I advocate for are informed by more than my own experiebce. I have gained the respect of most of the folks I work with, yet a few (including a PS) are in the range between hostility and uncertainty in my ‘ support” system. There are important ways to help others without being a CPS. Good Luck and have a peaceful heart.
Report comment
My initial response and why I am looking up this article without having read it because this has me so bothered I’m investigating other peoples observations. My initial reaction and why I’m here-in my area it seems more about people wanting a podium rather than being a peer. theres no peer about it. I can’t call my peer support. I’ve got to make an appt. the other recovery specialist routinely gossips and slanders everyone behind their back through private messaging calling it recovery and uses meetings, therapy and her place in peer support to boast about building her dreams and its like she hogs everything and it becomes about her at the top and everyone else is there to be her audience. she is destroying my household. shes got my partner so engaged in how great she is and obsessed with trying to subvert me because I go to zoom meetings and am finding recovery as a one of many, not the only one. she doesnt maybe realize he just is using her to agree with him to mentally and emotionally abuse me and knock down what my higher power is trying to build in me. shes counseling in areas she has no business and no authority in
Report comment