
When I was researching Anatomy of an Epidemic and sought to track the number of people receiving a disability payment between 1987 and 2007 due to “mental illness,” I was frustrated by the lack of diagnostic clarity in the data. The Social Security Administration would list, in its annual reports on the Supplemental Security Income and Social Security Disability Insurance (SSDI) programs, the number of people receiving payment for “mental disorders,” which in turn was broken down into just two subcategories: “retardation,” and “other mental disorders.” Unfortunately, the “other mental disorders,” which was the category for those with psychiatric disorders, was not broken down into its diagnostic parts.
However, starting in 2010, the Social Security Administration began providing—at least to a certain extent—such diagnostic information. Last month, the Social Security Administration published its reports for 2013, and there are two conclusions to be drawn:
- The rise in the number of “disabled” mentally ill is continuing its march.
- It is affective disorders—and not psychotic disorders—that is driving this increase.
And that latter finding is precisely what could be expected based on the scientific literature regarding the long-term effects of antidepressants, and the risk of antidepressant-induced mania. Increased use of these drugs could be expected to lead to an increase in the number of adults disabled by mood disorders.
The SSI and SSDI Data
In Anatomy, I reported that the number of people receiving an SSI or SSDI payment because they had been “disabled” by a mental disorder rose from 1.25 million in 1987 to 3.97 million in 2007. I calculated this total by adding the SSI and SSDI numbers in the “other mental disorders” category, and then making an adjustment for the fact that one in six SSDI recipients also received an SSI payment (in 2007). This was a method that others—such as E. Fuller Torrey, in his book The Invisible Plague—had used to track the number of “disabled mentally ill” in our society.
Now here are the 2013 SSI and SSDI numbers for diagnostic groupings that, in pre-2010 reports, would have comprised the “other mental disorders” category.
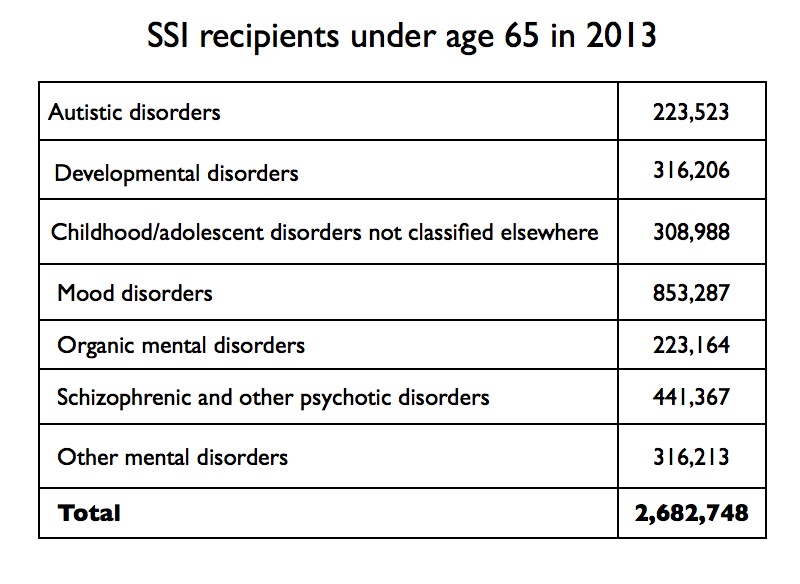
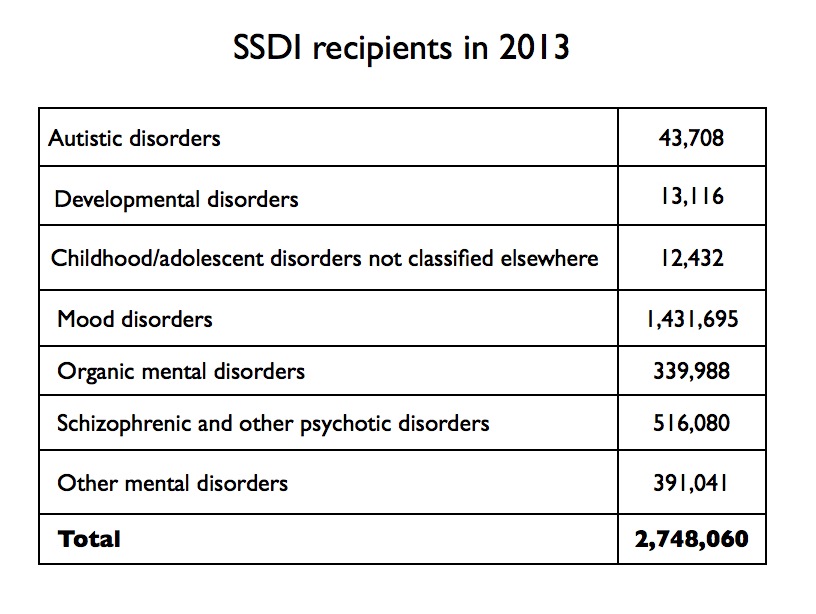
In 2013, the SSDI report stated that one in seven recipients also received an SSI payment (compared to one in six in 2007.) Thus, the number of people disabled by mental disorders in 2013, based on the method I used in Anatomy, was 5.04 million (2,682,748 +(.857 x 2,748,060.)) That is an increase of more than one million since 2007; the epidemic marches on.
However, now that the Social Security Administration has broken down the “other mental disorders” into specific categories, it is easy to see that there is one group—organic mental disorders—that should not be considered a “psychiatric disorder.” That group includes patients with dementia. Remove that organic group from the 2013 numbers (about 10% of the total), and you end up with a total of 4.5 million disabled by a psychiatric disorder. This is compared to an estimated 3.7 million disabled by a psychiatric disorder in 2007 (once the organic mental disorders are removed.)
The Rise of Disabling Mood Disorders
As I wrote in Anatomy, studies on the long-term effects of antidepressants provide reason to conclude that widespread use of these drugs will increase the number of people disabled by affective disorders. The annual SSI and SSDI reports since 2010, combined with a review of earlier data on affective disorders, provide evidence that this is indeed occurring.
In 1955, there were only 50,937 people in state and county mental hospitals with a diagnosis of major depression or manic-depressive illness. The prevalence of those affective disorders, in a severe form that “disabled” people, was quite low. Moreover, the understanding within psychiatry at that time was that the great majority of patients in these two diagnostic groups could be expected to recover, and many would stay well indefinitely. These disorders were seen as episodic in kind, and during the time between episodes, people could expect to function fairly well.
However, modern studies have found that medicated depression is much more likely to run a chronic course. Indeed, in longitudinal studies, the disability rate for those who stay on antidepressants is much higher than for the unmedicated group. For instance, during a six-year NIMH study on depression that was conducted in the 1990s, the patients who took antidepressants were seven times more likely to become “incapacitated.” In a Canadian study on disability, antidepressant use was associated with a two-fold risk of going on to long-term disability.
In addition, the use of an antidepressant increases the risk that a unipolar patient will have a manic episode and convert to bipolar. One large study by Yale investigators of patients diagnosed with anxiety or depression found that antidepressants increased this risk three-fold. Once a person has turned “bipolar,” they are seen as having a chronic illness, which is regularly associated with poor functional outcomes.
Prozac came on the market in 1988, setting off the dramatic increase in the use of antidepressants in our society. During the 1990s, several researchers noted the increase in people with an affective disorder diagnosis appearing on the SSI and SSDI disability rolls (without attributing that increase to the explosion in the use of SSRIs.) One report concluded that affective disorders, by the late 1990s, now accounted for 37% of those on SSI and SSDI due to psychiatric disorders.
Jump forward to 2013. There were 2.1 million people disabled by mood disorders in 2013 (853,287 + .(857 x 1,431,695)). That was 47% of the 4.5 million people on the 2013 rolls due to psychiatric conditions.
The annual reports since 2010, with the different disorders broken out, do produce one surprise: the number of people disabled by schizophrenia and other psychotic disorders has remained relatively stable since 2010, and lags far behind mood disorders. In 2010, there were 861,000 people on the SSI and SSDI rolls due to a psychotic disorder. This number increased to 883,000 in 2013, a rise of only 22,000. Psychotic disorders accounted for less than 20% of the disability due to psychiatric conditions in 2013.
A Global Epidemic
Since Anatomy was published, I have gathered disability data for a number of other countries. The story is much the same in country after country. Iceland, the U.K., Norway, Sweden, Denmark, German, Australia, and New Zealand have all reported marked increases in disability due to psychiatric disorders, and in all these countries, where SSRIs are popular drugs, the increase is being driven, at least in large part, by affective disorders.
Critics of Anatomy have argued that I mistook correlation for causation when arguing that increased use of psychiatric drugs is driving the marked rise in disability numbers. But this is more than a story of correlation. It is a story of research predicting that this would happen, and that is particularly true in regard to SSRIs.
Think of the evidence in this way. You have research showing that antidepressant usage is associated with a higher risk of becoming disabled by depression over the long term, and you have research showing that antidepressants can stir manic episodes that will lead to a bipolar diagnosis. Then, you study the disability numbers, and find that in the Prozac era, when usage of antidepressants has soared, the number of people disabled by mood disorders has soared too. The disability data can be seen, in that equation, as confirmatory data.
The Social Security reports issued last month, detailing the 2013 numbers, provide yet another data point in this tragic equation. This website has also published numerous personal stories from people whose lives went astray after initial exposure to an antidepressant, and of course their stories also contribute to the “evidence base” on this matter. So too the rising disability rates due to mood disorders in other countries that have adopted widespread use of antidepressants–yet another data point. But, of course, this is a collective body of evidence that tells of harm done, and of a need to rethink use of antidepressants, and that is evidence at odds with the beliefs that drive our societal use of these drugs. And so the response: correlation doesn’t equal causation. That is a response that sounds scientific, but in this instance, provides a way to turn a blind eye to what might best be described as an “inconvenient truth.”
And so the disability numbers march on.











I was initially prescribed Xanax for ‘work-related stress” (if that’s a “mental illness”, the ENTIRE WORLD is “mentally ill) after starting my first new job straight out of an intense graduate program. Up to this point I was a highly functioning and capable professional with no history of so-called “mental illness”.
Within a few months on the Xanax, I was experiencing what I now know to be tolerance, interdose withdrawal and toxicity and I became suicidal.
Enter Psychiatry, their drugs, bogus labels…5 years later, spellbinding, lots of manipulation to believe the labels by my doctor and therapist, I’m on a total of SIX Psychiatric drugs and I am physically, mentally, emotionally and psychologicaaly sicker than I had ever been in my entire life. In the latter 2 years of the 5, I took FMLA twice and then ultimately wound up having to resign from my job because I could no longer function in that capacity (or in day to day life, really).
Once I found out the drugs were my problem, I stupidly (was unaware of the need to taper and the prescribing doctor was having none of it, insisting that I “needed the drugs for life”) detoxed in a facility that was more than glad to take 40k off of me and label me an “addict” for AS PRESCRIBED use of psychiatric drugs.
Now, over 4 years into cold-turkey withdrawal and I am still unemployed and on disability for what I’m sure SSD considers a “mental condition” but really is (and has been all along) iatrogenic illness strictly and solely from the prescription polydrugging, toxicity, tolerance and protracted withdrawal.
I would’ve been a tax-paying, contributing citizen all this time had psychiatry not maimed and crippled me and stole my ability to function on all levels, other than basic activities of daily living. Now I am a burden collecting SSD. The financial repercussions on all levels are immense.
Perhaps the “success” and “treatment” in their eyes is that I started out with work-related stress….and now I can’t work! So, they solved that problem, didn’t they?!
Report comment
I’m sure some / a lot of this is true — but the author makes it too simple…..
He’s using logic that IQ of people who smoke is lower than IQ’s of non-smokers; therefore, if you stop smoking, your IQ will go up !
1) Of course, the more serious your depression — the more likely that you will be given anti-depressants. The more serious your depression, the longer you will be on anti-depressants.
2) Society’s knowledge and acceptance of depression has significantly changed.
3) The treatment of depressed individuals and definition of who is depressed has changed. In the 50’s and 60’s, after a stressful day at work (which was often interpreted as everyday) — people came home and drank 2-4 martini’s. They also had 2 martini lunches. So people were self-medicating with alcohol (and the definition of an alcoholic was significant different back then also).
4) Our lives and workplaces and the job market have changed significantly. Also, standards of acceptable work-place behavior have changed.
5) People with substance abuse (many who are also depressed) — are now often viewed as having illnesses, and therefore are no longer guilty of their addictions. (Plus, you can now take FMLA leaves for entering addiction treatment programs).
6) The more money we spend on depression studies, the more drug companies develop and release new anti-depressants, and the more psychiatrists produced by a society — the more consumers for these products / providers we will have.
When economies are tough, it is harder to get jobs and harder to hold on to jobs. Very few people now work 9-5, and only 5 days per week. Plus, now most households consist of 2 bread-earners — there are few “stay at home moms.” Technology changes on a daily basis, workers are required to constantly learn the new technologies, work 80-100 hrs per week (including weekends) and also care for children at the same time. Therefore (and we will not even discuss the added stress here), many people who were depressed 60 years ago — could still function and work in our society — there was enough “downtime” for person to deal with his depression and / or his decreased level of productivity than today. (Also remember, that in 50’s and 60’s, many people had the same job for 30-40 years and received full benefits. ) Plus, global trade and global competition was far less. And then, of course, we had a pre-internet and internet world. Remember, pre-internet: immigration restrictions — protected many domestic jobs. There were no overseas call centers — because you had to physically live in US and be physically on-site — in order to access the data …..now, with the internet, call centers can be located in India and throughout Asia.
The world has been re-invented in the past 20 years, and people’s views have been re-invented many times over the past 60-70 years……
I ran into someone about 5 years ago — who had been fired from his job, because his job had become more demanding and he could not keep up. He collected unemployment for the maximum period of time and then hired an attorney to try to get him disability benefits. His argument for applying for SS disability was that he always had a disability and was able to work for 25-30 years with his disability — but when his job became more demanding, his disability then prevented him from being able to work anymore — because he couldn’t keep up with the raised bar at work.
In many countries (for example in leading countries in Asia), depression carries heavy stigmas and many people don’t recognize that it is an illness. Since there is heavy shame, there are very few people who admit they have depression — but does that mean there are far fewer depressed individuals in say Japan and Korea — just because they “stay in the closet.” (Look at recent news regarding handicapped and depressed Koreans who were forced into becoming slaves on a Korean Island and gather salt. A number of these people were freed and brought back to Korean mainland — where many remain homeless and wish they were back as slaves on that salt island. Since most Koreans don’t recognize depression as an illness, government and society can’t see depressed people, and there are few government resources available to them.) Furthermore, employers who discover employees on anti-depressants and other similar med’s — can be fired — they lack laws similar to the ADA. However, in Japan and Korea — it is perfectly acceptable in the evening to get so drunk — that you simply pass-out. So, many depressed people hide in the closet and self-medicate with alcohol — which is perfectly acceptable in these countries……..
And all these soldiers returning from Iraq — I think 25% of them supposedly suffer from PTSD, etc. How long has this been a recognized illness???
On the other hand, with the newest MRI studies with people with depression, it shows that taking anti-depressants — permanently affects the pathways in your brain. This is a new finding — and the levels and the consequences of these changes are yet known.
And as medical technology improves — so does our ability to define what is and what not an illness. And of course, politics, society, and religion also tell us what is an illness and what is not. (Recall, Tom Cruise and Brooke Shields fierce debate several years ago concerning postpartum depression ???).
Anyhow, what does all the above tell us ? Changes in acceptance and acknowledgement, changes in medical instrumentation, changes in the workplace, changes in the economy, changes in public opinion, changes in what is deemed politically correct, consequences of not dealing adequately with depressed individuals (i.e., mass shootings), etc. — all have major components here. (Often, police departments faced with pressure to lower crime, change the definition of certain crimes, rezone their communities to exclude the areas of major crimes, and encourage some people not to report lower level crimes, like pick-pockets, telling them it is a waste of time to report these crimes. So, the REPORTED levels of crime decrease – but do the actual number of crimes decrease ???)
It is the same thing here.
Report comment
All of what you said COULD be an explanation, but it is no more supported by data than any other explanation. As a matter of fact, if you read the book, you’ll find that Whitaker’s explanation is much more consistent with the data than the possible hypotheses you put forward. There is a clear biochemical mechanism that explains why taking antidepressants in the short term can produce more chronic depression. And you also fail to take into account that if antidepressants really work as promised, a good percentage of those taking antidepressants would become well again and be able to work.
There are confounding factors, but considering that this phenomenon is occurring in multiple countries around the world, with big variations in government assistance programs and employment rates, it’s hard to argue that it’s all because of social variables.
You need to read the book. Your explanations are more comfortable for society at large, but that does not make them true.
—- Steve
Report comment
Thank you for your thoughtful review of the multiple potential interpretations of the data the author cited! While the author has raised a valid concern, he writes as though his preferred interpretation is the only or most likely possibility. The data he himself cites do not support that conclusion.
Report comment
I’m proof, “The data [Whitaker] himself cites do not support that conclusion,” is an untrue statement. As is the now black box warning on the antidepressant drugs:
“Suicidality and Antidepressant Drugs
“Antidepressants increased the risk compared to placebo of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults in short-term studies of major depressive disorder (MDD) and other psychiatric disorders. Anyone considering the use of [Insert established name] or any other antidepressant in a child, adolescent, or young adult must balance this risk with the clinical need. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction in risk with antidepressants compared to placebo in adults aged 65 and older. Depression and certain other psychiatric disorders are themselves associated with increases in the risk of suicide. Patients of all ages who are started on antidepressant therapy should be monitored appropriately and observed closely for clinical worsening, suicidality, or unusual changes in behavior. Families and caregivers should be advised of the need for close observation and communication with the prescriber. [Insert Drug Name] is not approved for use in pediatric patients. [The previous sentence would be replaced with the sentence, below, for the following drugs: Prozac: Prozac is approved for use in pediatric patients with MDD and obsessive compulsive disorder (OCD). Zoloft: Zoloft is not approved for use in pediatric patients except for patients with obsessive compulsive disorder (OCD). Fluvoxamine: Fluvoxamine is not approved for use in pediatric patients except for patients with obsessive compulsive disorder (OCD).] (See Warnings: Clinical Worsening and Suicide Risk, Precautions: Information for Patients, and Precautions: Pediatric Use)”
And the psychiatric industry knew antidepressants caused “mania” in 2000, as is documented in their DSM-IV-TR. And knew then that claiming this known adverse effect of the antidepressants should not be used to railroad patients into a completely iatrogenic form “bipolar” diagnosis. A quote from the DSM-IV-TR:
“Note: Manic-like episodes that are clearly caused by somatic antidepressant treatment (e.g., medication, electroconvulsive therapy, light therapy) should not count toward a diagnosis of Bipolar I Disorder.”
What a shame the DSM5 has seemingly lost this wisdom. But I’m quite certain, “The data he himself cites do not support that conclusion,” is not data he himself alone cites. It’s data that both the FDA and the previous psychiatric DSM cite as well.
Report comment
Orbit
How do you figure that? Give some examples of what you mean. It’s easy to say that the data he cites doesn’t support that conclusion but you don’t give any examples to prove your point. On this site you have to back up what you say with some observable proof. You don’t just get to sit there and say, “the date doesn’t support the conclusion”.
Report comment
You’re making good points but they still don’t explain why the rise in mental illness seems to be awfully specific to a certain subset of those “illnesses”.
In any case, even being very careful about the causation – it seems like these drugs are not really helping the problems.
Whether depression can be called an illness, especially when you can point to very specific life circumstances which make one depressed, and on the topic of disease-mongering in general – that’s a different conversation altogether.
Report comment
Btw, the only way to figure out if anti-depressants cause bipolar is to give it to “normal” people and see what happens. That is deemed unethical. But when they are given to “depressed” people and a big subset of them turns bipolar it’s seen as an “unmasking” of underlying illness or “it was not major depression, it was latent bipolar disorder presenting itself in depressive phase”. It’s an acrobatic explanation but in the insane world of psychiatry there Occam’s razor is never used properly it sells.
Report comment
Thank you for writing… Its been my experience working with those that use Xanax, that this drug is one of the most dangerous ever approved. I am seldom wrong when I suspect seizure activity, even with very small doses. The withdrawal, seems to be in a class by itself, several orders of magnitude worse than Heroin.
And of course, the drug as a causative agent of your symptoms is completely overlooked by whoever prescribed it for you. Blaming, those victimized by their process comes naturally to those that profit from prescribing this drug.
Sadly there are many hundreds of thousands of people who have been affected, just as you were, unfortunately, they have lost the ability to warn others about the disaster that awaits them, when they are prescribed this s0 called medication.
Thanks again for writing.
Report comment
Thanks, Bob, I am very grateful you are pointing this out. As I was one who was misdiagnosed, according to the DSM-IV-TR, with “bipolar” due to the adverse effects of a SNRI (the not “safe smoking cessation med,” Wellbutrin). And I’m heartbroken the DSM5 was changed to make this iatrogenic pathway to the “major mental illnesses” an acceptable standard of care. Since I know with 100% certainty that the antipsychotics and mood stabilizers do not cure the adverse effects of the antidepressants. They, in the combinations the psychiatrists are now commonly prescribing them today, just cause the symptoms of the “major mental illnesses.”
Report comment
In my particular case, a bunch of sick doctors defamed me to my family for years claiming anticholingeric intoxication poisoning was “bipolar.” Thank God for decent nurses who “think some of the doctors in our neighborhood are really disgusting.” They couldn’t explain how the doctors had made me sick, but they did hand over my family’s medical records. And, of course, no doctor will ever confess to any other doctor’s malpractice, leaving it up to the patients to research medicine on their own. Thank God also for the journalists who are pointing out this form of iatrogenesis.
Report comment
My personal research implies that psychiatry is basically one big Ponzi scheme of mental illness creation, not an industry interested in curing anything. It’s about making people sick for profit. And it is the “dirty little secret of the two original educated professions” historic and current way of defaming, discrediting, and torturing people to proactively prevent potential malpractice suits for the incompetent doctors and cover up sexual abuse of children for the religions and wealthy.
Report comment
People on SSDi for mental health receive a very small sum, just enough to barely survive in the lowest income housing, unless they have someone to live with as I now live with my mother, though before for about 7 years lived in low income where i was very unhappy and conditions were no where close to being sufficient for good mental/emotional health.. The low income lifestyle is counter to healing or good health as it contributes an environment of gloomy toxic despair, danger, low social status,no money for quality food,resources etc..that can help a person reach higher potentials. It is depressing in and of itself and while ssdi recipients receive a very meager stipend and stew and stagnate in the low income,medicated lives the drug companies make billions and psychiatrists and counselors get a career.I’m not saying that therapists and mental health people are all bad or inadequate or unneeded, I’m saying that I agree that there needs a lot of improvement in the system and I’m also saying that benefits should be much more generous and creative, or perhaps we should have a universal basic income.I know that I can’t work or be employed with my emotional,psychological,physiological and social difficulties and am glad to receive something but if I didn’t live with my mother I would likely be homeless or at best barely existing in the worst lowest income housing. S I’m think there should be something in place even though I do not embrace the disease model of depression and mental health as I believe that people are afflicted with a combination of natural human problems and issues that stem from many sources and cause depression,altered states of mind,suicidal inclinations,extreme mental states.
Report comment
“It is depressing in and of itself and while ssdi recipients receive a very meager stipend and stew and stagnate in the low income”
SSDI pays out twice and in some cases even more than twice what SSI pays out. I live on SSI — it’s 700 dollars a month. And it’s needs-based too. So it’s 700 a month only if you absolutely need 700 this month. If you get a case manager up in your business, some months it may be 500 a month because your parents bought you food, other months it may be 400 because you spent a week in the hospital, etc. My aunt lives on SSDI, she gets a little over 3,700 a month because she worked for 20 some years. And because it’s not considered “welfare”, she gets that money no matter what. She could be a millionaire and would still get that money. If my father dies before be begins drawing his social security, because I was deemed “disabled” before age 22, I could get as much as 1,400 a month. If he lives to 65, and I sure hope he does, then I and my future are doomed.
Report comment
Hi Bob-I totally agree with the long-term outcomes of antidepressants being bad. I do wonder, however, whether the rise in SSI and SSDI can be totally accounted for by the use of drugs. I think that bad economies also have something to do with the rise. I remember the 60 minutes segment on the almost the whole town be declared disabled after the local factory was closed. I would chalk the rise in disability to the availability of labels. I used to evaluate people for disability. The label of depression has a pretty low bar. It’s an easy case to make. There was also a major swell in the rates of children getting SSI for ADHD. (I think in recent years, the Social Security System might have tightened up on the criteria for ADHD.) When its hard to earn and the criteria are low, people will find a way.
Report comment
I very highly doubt that it is simply due to more labeling. Yes, it is very easy to get labeled and drugged and damaged but getting SSI or SSDI approved is very, very hard. People need to have a very compelling and documented case and are many times denied for years and years and many give up. Go in the withdrawal forums/groups and see for yourself. Many people that deserve and need to get assistance are not getting it including myself, so the real disability rates are really much higher than the numbers reflect.
Report comment
“Yes, it is very easy to get labeled and drugged but getting SSI or SSDI approved is very, very hard.”
It’s not only very hard, it’s not sustainable living one way or another. These programs were designed to be so broke and meager that even the poorest people in the country wouldn’t be able to live better off of them. They succeeded. Nobody would choose to live off of 700 dollars a month. Of course, as Whitaker showed here, the majority of people going on disability for affective disorders are drawing SSDI and now I have come to determine that THIS is the problem. Do away with SSDI for mental illness. Make those same people have to go on SSI and WATCH THEM ALL GO BACK TO WORK!
Report comment
To put living off of 700 dollars into perspective.
Minimum wage 40 hours a week: $1,160
Wal Mart average starter salary 40 hours a week: $1,409
“Sociologists William Thompson and Joseph Hickey estimate an income range of roughly $35,000 to $75,000 for the lower middle class…”
35,000 a year / $2,916 a month
75,000 a year / $6,250 a month
Report comment
There is no way you can live of off of ssdi unless you have a PT job – and then you risk getting too many hours as well as the old – well, you’re working PT, why can’t you work FT run-around. Its shameful.
Report comment
Yes, it is shameful, and in a nation that pays for endless war all over the globe, there is no excuse for it.
Report comment
SSI amounts vary. In California the amt is closer to $1000. Individuals with disabling developmental disabilities (autism, intellectual disability, CP, epilepsy) also can receive services and supports (including housing) from the regional center system, and Medi-Cal. There is no comparable state system for those receiving SSI solely for a non-developmental mental disorder. Free MH services in CA are negligible.
Also, I’m sure you all are aware that individuals with developmental disabilities frequently have mental health disorders as well. Many regional center clients in California are found SSI eligible under a mood, psychotic or other mental health disorder, rather than under their developmental disability,as well. I don’t think those stats are tremendously reliable for demographic info on who has what.
Report comment
“SSI amounts vary. In California the amt is closer to $1000”
SSI is federal and the monthly maximum payment is $733. State services do vary, but in my experience and in my area are only available to wards of the state and people who completely and happily comply with abusive psychiatric drugging. Case in point: I once tried to use a local service called supported employment, which would take 13% of my paycheck for as long as I worked wherever they found me a job, but they refused to work with me unless I were seeing a psychiatrist and allowed them to talk to that psychiatrist. Another example: I tried to get subsidized housing after my living here in my often angry moods was too stressful on my parents, but they told me because of my psychiatric history that I only qualified for group home housing. When I talked to the people from there I found out I would be forced to take cocktails of neuroleptics and “mood stabilizers” in order to live there, and that this was a policy decided by staff that existed completely indepedent of peoples diagnosis or whether or not a “doctor” even thought they should be on them. So even if I found a Peter Breggin-esque psychiatrist who said I was fine without, they’d make me go doctor shopping to get the drugs one way or another before letting me stay there.
Report comment
To JeffreyC, there is this thing called lying. You can lie and say you take the psych drugs/meds, but in reality do not. You would do this to get the decent housing. Only if you have a criminal record could they enforce the drugging, otherwise it is your freedom to choose the method of ingestion of the psychiatric drugs.
Report comment
“You can lie and say you take the psych drugs/meds, but in reality do not. You would do this to get the decent housing.”
Being in a group home means living with a “staff” who would certainly make sure that residents were swallowing their “medication”, and besides that the effect they are looking for is sedation enough to keep them from being bothered, so even if I managed to cheek it successfully all the time I’d still have to stay in bed all day and pretend to be zonked out. In any case, I gave up on all that years ago.
Report comment
JeffreyC,
I agree with most of what you’re saying in these comments, but this particular one is hurtful. You’re absolutely right that nobody would choose to live on $700 a month in the US. That’s why it’s BS when people make a “free rider” bogeyman out of people on disability. I am on SSDI and I get $825 a month and can tell you that nobody would choose to live on that. It’s not right that you get $125 less than I do, and I’m sorry about that. It’s a lot of money to anyone who sees as little as we do, but I assure you, it’s not enough for me to be enduring the slow murder of poverty if I had any other options.
Wouldn’t it make more sense to say that anyone who is disabled is entitled to at least live above the artificially low poverty level, instead of playing along with the conservative and fauxgressive game of dividing those of us who are disabled by arbitrarily separating the so-called “deserving” from the so-called “undeserving”? I mean, it reminds me of when non-unionized private sector workers get played into thinking that public sector workers should not have benefits because THEY don’t have benefits. It’s totally missing the point, imo, which is that EVERY worker deserves benefits.
Report comment
@uprising, offending anyone was never my intention. I was aware that SSDI amounts vary but according to different rules. SSI is “needs-based” whereas SSDI is a government run “insurance program” (it’s really not, and is in fact a welfare program since the tax money being paid “into” it is really not apportioned to it) and so payments are based not on need but on work history and past income. It’s enrages me sometimes to think about how SSDI was designed to keep rich people rich and poor people poor. To protect the class system in times of disability. Like my aunt who had her hip removed due to rheumatoid arthritis. Because she worked for 20 some years and made close to six figures a year she gets close to 4,000 a month. Oh no, we cant have our government let rich people become poor, cant let country club people have to shop at wal mart.
Anyway, people can also combine SSDI with SSI if their SSDI is low enough that combing the two would not put them over the $2,000 resource limit. Which is how young people can easily surpass the 1,300 a month that is normally the typical SSDI ammount. You should try it if you haven’t already.
Report comment
JeffreyC,
Yes. Most of our social institutions have been set up to do just that and SS is no exception. I think it’s BS and that anyone who is disabled should not be sentenced to slow murder by poverty, not to mention the added discrimination and poor shaming that is rampant in our culture. I think anyone who is disabled in a nation that can manage paying for endless war all over the globe should be entitled to a life of dignity, period – individual work history or not. They should not be subject to damnation by society and left to starve in the shadows or to submit to abuse just so they can attempt to get their basic human needs met.
Also, are you sure about the numbers you gave for the possibility of supplementing SSDI with SSI? Do you have a link? Because I looked and couldn’t find anything. And I once relocated to California briefly and automatically received an additional $100 or so per month from SSI that CA paid for, but that was it, and I think CA has the highest state-paid amount for that kind of supplementation. Either way, I appreciate your suggestion. Thanks.
Report comment
I’m not 100% sure about the numbers. I’m recollecting within a range. I do know you can combine SSI and SSDI, but to do so your SSDI cant be over a certain amount a month. If I were to figure this out, I call my “case manager” at the department of human services. I don’t know what it might be called where you are.
Report comment
Bob,
Thank you for this update. I have had many conversations with colleagues about the validity of the term mental illness…what it means and whether it is valid or helpful…this information will help me explain my concern about illness labels and how our medical model, corporately owned system actually creates much of what is perceived as a medical (mental) illness…
Your work has given us a firm foundation upon which to stand as we speak truth to power. This community is where I turn for both information and support.
Thank you,
Cindy
Report comment
Hey-no problemo; our new Koch congress has SSDI slated for a 20% decrease in 2016…what coreyjwiley states above is true; I anticipate a surge in homelessness/suicide. That’ll fix our economic/social problems!
Report comment
The rest will get locked up in private prisons and, if some people’s hopes get fulfilled, brand new “humane” asylums (no doubt private and for profit). What a shiny bright future ahead.
Report comment
Jill,
Thanks for the note. I don’t think that psychiatric drugs are the only reason for the rise in disability. I think the disability numbers serve as a marker of how our drug-based paradigm of care (and liberal diagnostic boundaries) are increasing the burden of “mental illness” in our society. There are many people, as comments here attest, who may have been prescribed a benzodiazepine, an antidepressant, or some other psychiatric drug, and then years later, find themselves struggling in a way they never had before (and with multiple problems.) The disability data is a marker, I believe, for that larger unfolding tragedy.
And of course ADHD awards are part of this rise too. They show up in the development disorders category.
I should note, however, that this continuing rise in disability due to mental illness is coming even though it is becoming increasingly difficult, at least upon first application, to get an award for SSI or SSDI. In 1992, for instance, 47% of initial applications for SSI led to an award; that number has steadily decreased in and in 2012 was 27%. Award rates for SSDI applications have similarly declined.
Given that there are many who leave the SSI and SSDI rolls each year (with death one primary reason), and given that it is becoming more difficult to get on one of these two programs, it might be expected that the increase in the number of those on disability due to a psychiatric disorder would level out (or perhaps even begin to climb.)
My general point though here is that these rising numbers of people disabled by mood disorders, with other countries experiencing rising disability rates due to mood disorders in the Prozac era, is evidence of a failed paradigm of care, that needs to be dramatically rethought.
Report comment
“And of course ADHD awards are part of this rise too. They show up in the development disorders category.”
I’d not be surprised if they didn’t contribute to bipolar and psychotic disorders too – ADHD drugs are for the most part amphetamines and the most well known side effect of these substances is psychosis.
Report comment
How many more might be qualified for disability if not for meds? A more liberal criteria may have helped many who would have been left out in the cold.
Paul Markovitz says less than 80 mgs a day of Prozac doesn’t offer the therapeutic punch BPD patients need for full relief. At 80 mgs they show remarkable progress, not observed at 60 or 40 or 20, though he’d prefer 10 could do the trick.
Fortunately there are kids who avoided prison no doubt because they caught their ADHD in time! The propensity of ADHDers without treatment to commit crime is known.
Report comment
Jeez, I guess this guy doesn’t read my posts at all. It has been shown in every review since 1978 (the first was done by none other than Russell Barclay himself) that stimulants DO NOT REDUCE THE LIKELIHOOD OF CRIMINALITY in “ADHD” youth. There is NO DATA, NONE, to show that kids given ADHD are less likely to be delinquent or to be jailed as adults. It is a fantasy.
Additionally, most psychiatrists agree at this point that giving SSRIs to people with bipolar diagnoses is probably a bad idea, as it makes it more likely for manic episodes to happen. Manic episodes are clearly stated side effects in the product information for SSRIs.
Finally, the WHO studies both showed unequivocally that employment is much more likely ( 60% or more) for those diagnosed with schizophrenia in developing countries who are less reliant on drugs for treatment. Whitaker also cites studies showing the social recovery rate for schizophrenia in the USA in the 50s (pre-Thorazine) to be much higher than today. Whatever your beloved drugs are doing, they aren’t saving people from the disability roles.
Your “facts” appear to be fantasies that you really need to be true. You should really read the book before you bother to comment. You have a lot to learn.
—- Steve
Report comment
I suggest you improve your text comprehension and read through the article again…
As for BPD (which is not a diagnosis but a sophisticated insult but that aside) there are no drugs treatments that psychiatry agrees should be recommended. They have tried everything from anti-psychotics, through benzos to SSRIs (because these drugs don’t treat any specific problem but at best tranquilize people so whenever they have a new label they just throw that stuff at you and see if something sticks) and came back with nothing.
Report comment
How are double-blind, controlled drug tests conducted among children with depression using a placebo?
Report comment
Bob, how do researchers justify giving placebos to children when they present with depression which is often associated with suicidal ideation? Any ideas? Suicide. Children. Placebo. Seems to me that is an ethical issue that needs to be addressed.
Report comment
Well, since there is no evidence that antidepressants reduce suicidal ideation, except maybe in the extremely depressed, who are generally excluded from the trials, I’d say the ethical risk is pretty low. Actually, there is little to no evidence that antidepressants are even effective in children, and there is definite evidence that they INCREASE the likelihood of suicidal feelings and acts in those who didn’t have them before. The only one even approved for under 18 is Prozac, and that was based on one single study that has been roundly criticized in hindsight.
So perhaps the real ethical question is why we would give antidepressants to children at all?
—- Steve
Report comment
Comment removed.
Report comment
If you would like to draw attention to published research, please do so in a comment that is free from personal attacks and within our posting guidelines for the site: http://www.madinamerica.com/posting-guidelines/
Report comment
Bob , do you realize about half of schizophrenics recover or nearly recover completely? Just go to the literature.
Report comment
Yeah, if you live in Brazil or Nigeria. Not so much in the USA…
Report comment
Thanks so much for your articles and all you are doing that will hopefully result in a positive change for so many people who suffer.
I wondered if you could explain why you think the number of people experiencing psychotic disorders has remained stable despite standard use of antipsychotic medication.
Report comment
Some instances of psychosis gets re-branded as … with psychotic features. Bipolar can be one of them.
Report comment
In the research I’ve done, as I was going through the mental health world and for a fraction of that time, receiving disability, being ‘on disability’ carries the most profound stigma of all, given that it reflects a socio-economic position. So I feel, by and large, it’s a political tool–an image filled with misconception and distortion, for the purpose of divide and conquer, in a social sense.
While my actual and real disability began exclusively due to toxic medications and what I consider to be gross psychiatric malpractice on many levels, my actually being dependent on disability payments for survival was prolonged greatly and unnecessarily due to, both, discrimination and political corruption within the system. I know this because it’s my work and I learned a lot about the system and its tangents in my various interactions over the years. I experienced a lot of sabotage, specifically because of stigma and discrimination, by some really clueless people in power, and it was easy to prove, over and over again.
None of the agencies with whom I worked either knew the spirit of, or followed the guidelines of, American Disabilities Act (ADA), because mostly people feel that the voice of a disgruntled patient/client carries no weight. So of course, this is fertile ground for oppression and power abuse, which is disabling in all sorts of ways, and definitely keeps people on disability. I was fortunate to break through this barrier several years ago, when I won my discrimination meditation, based on ADA law. Thank God, I found an public employment attorney OUTSIDE legal advocacy in the system. She’s been miraculous support as I’ve traversed all of this.
With all the corruption and smoke and mirrors that has become inherent in the political world of ‘disability,’ it’s certainly a formidable challenge to seek clarity. Having been through all that, I’ll just say that it’s like being on the other side of the looking glass, truly bizarro world. I do believe there are a lot of answers here. Thanks for bringing this up, Bob.
Report comment
Correction–discrimination MEDIATION, not meditation. Although that was vital to win this suit!
Report comment
“being ‘on disability’ carries the most profound stigma of all, given that it reflects a socio-economic position.”
You cant have ANYTHING on ssi without having to feel like the whole world is against you. Even if you find yourself only buying the great value brand cereal with your bridge card, you’ll still have people shaking their heads at you as if you were only supposed to buy the plain rice instead. I don’t do my own shopping, my father does, but he tells me about it all the time and I read about it now and then on the internet too. Enrages me.
Don’t even think about having a cell phone, even if you need one. Don’t even think about receiving gifts — and hide them if you do, cause you cant let your belongings put you over the resource limit or you’ll lose your SSI! This computer, a couple of cheap DIY suped-up guitars and amps, and I’m teetering at the brink of the limit all the time! (House-hold goods, defined as necessary to daily living, E.G. appliances, and “personal effects”, E.G. wedding rings but not electronics or collectables, are the only exceptions to the resource limit.)
Being on SSI doesn’t just put you in poverty. It FORCES you to live in poverty. If you had a decent life before you became disabled, well odds are then you worked and will go on SSDI and live happily ever after. But if not, then you have to sell that decent life away and move to the ghetto before you even qualify for SSI.
Report comment
There aren’t any good choices in a society of socio-economic oppression. It’s why we’re seeking radical change. It’s not easy, but it’s doable, with focused intent.
Report comment
Sa,
That is a good question, and I really don’t know the answer. What seems to be happening is that a significant percentage of people with psychotic disorders “disappear” from the disability rolls each year.
For example, there 433,835 people receiving an SSI payment in 2010 because of schizophrenia or other psychotic disorder. From 2010 to 2013, there were 157,000 new awards for schizophrenia and other psychotic disorders. Add those two together and you get 590,000 by 2013, minus of course whatever number who died, left the program for unknown reasons, disappeared, or went to work (the latter is a small number.) And you see that the total number of people on SSI disability due to schizophrenia/psychotic disorders was 441,367, meaning that about 150,000 people in this category left the SSI rolls during those four years. Where did they go?
That is a question that deserves to be investigated. It is also notable that 60% of people receiving SSI in this schizophrenia/psychotic disorders category have been on the SSI rolls for 14 years or less.
So, I don’t know. But there is a question to be investigated here.
Report comment
Bob,
What impact across diagnostic categories does premature mortality of 25 years of potential life lost (NASMHPD) have on SSI and SSDI statistics for any given year? Tragically, “attrition” is rarely more then a source of lamentation in the mental health system.
Report comment
Joe
Its a terrible thing if its true that maybe a sizeable percentage of people in the figures would have died in 4 years. But most of the ‘schizophrenics’ I knew when I was in Ireland in my 20’s have died. These friends were ‘well on medication’ most of the time, and most of them didn’t live badly (and were part of the community).
Report comment
About a third recover sufficiently to stop using antipsychotics entirely while some only need meds occasionally and can go back to work, etc. 150,000 is about one third of 450,000.
Report comment
Citation please? I have understood it is closer to 10-15%.
“Sustained recovery occurs in less than 14% within the first five years following a psychotic episode2 ” [http://www.nimh.nih.gov/about/director/bio/publications/rethinking-schizophrenia.shtml]
— Steve
Report comment
I’m quite familiar with this claim that “about a third recover.” It’s one of those factoids, i.e. a piece of propaganda, which is regurgiated over and over by the disciples of E. Fuller Torrey and his forced drugging fan club, the so-called Treatment Advocacy Center.
Report comment
Goebbles and Torrey would have agreed on many points.
And even if it’s true, which I seriously doubt, Columbia and India and Nigeria still kick our ass by a factor of 2 with very little use of antipsychotics. If my data is correct, we’re talking 4 times better recovery rates in these “primitive” cultures who have not yet seen the wisdom of drugging people who behave differently than the scared “norm.”
— Steve
Report comment
I agree, Steve! Whenever I see this kind of propaganda promoted by acolytes of the Treatment Advocacy Center, I am reminded of that famous quote, attributed to Goebbels:
“If you tell a lie big enough and keep repeating it, people will eventually come to believe it.”
I, too, am familiar with the accounts of higher recovery rates in poorer countries. What is really infuriating to me, though, is that we’ve seen recovery rates (from “psychotic disorders”) as high as 80 to 85 percent RIGHT HERE IN THE UNITED STATES, claimed by (dissident) psychiatrists like William Glasser, John Weir Perry and Loren Mosher, who focus not on treating “diseased brains,” but on restoring respect, relatedness, balance, and hope to the troubled person’s life. I talk about my informal research on this topic here:
https://www.youtube.com/watch?v=ajOCdShLPUk
Also, I would like to take this opportunity to ascertain that I do indeed know how to spell “regurgitated.”
I could use a good copy editor.
Report comment
Shhh! Start talking like that and people will get CURED, and what will they do for clients then?
I will watch that video. But if people like you and me know these things, there is no excuse for the bigwigs not to know them. Which means they really do know them and are very intentionally lying. Which kinda pisses me off!
—- Steve
Report comment
Isn’t ‘mood disorder’ or ‘psychotic disorder’ a vital issue here? That seems to be the topic of great divide–is it a real condition vs. is it culturally contrived?; is it a ‘chronic disorder’ vs. a temporary state?; is it a sign of illness vs a sign of spiritual awakening?; is it merely judgment in personality types and an indication of an extremely low-permission, uptight and anxious society?
That’s one thing that keep coming up for me here, the issue of a chronic disorder. I think that’s an illusion, totally, that so well-serves the capitalist nature of the mental health field. AND, it keeps people on disability, the total confusion around this illusion.
Report comment
Shame and shaming are big players in this equation. That will muddle things up every time, and keep things in emotional chaos. Life is complicated enough without this in the mix, but it’s there, adding insult to injury.
Certainly, that’s one change that can be made on a personal level, and there’s responsibility on both sides–to not shame others and to not take on shame from others. When it comes to poverty, disability, ‘mental illness,’ etc., that’s a significant issue, as it is quite disempowering when we buy into it. Personally, I think it’s a tool used knowingly to try to throw others off their game, and that’s almost too sinister to even write about. Still, I know it to be the case, so I’m going to call it out.
And its nothing short of evil (owning my judgment, here) when done to others, especially someone who is obviously courageous enough to make themselves vulnerable. That sets a terrible example, bar none. And, it is easily a crime against humanity, by my definition. To me, that’s critical to clean up, for clarity and unity to occur.
Report comment
I am trying to get SSD for mental disorders. I have been diagnosed as Borderline Personality Disorder, Dependent Personality Disorder, severely depressed and Deep Anxiety. There are no meds that can help Borderline Personality Disorder. And I am on Paxil and Lorazepam for depression and anxiety. I have had my SS Evaluation and am waiting to hear. Without SSD or SSDI I can not afford to live and will be stuck living with my ex-husband (who is a catalyst in all this) forever. Does anyone know what are the chances of approval may be?
Report comment
Jedimom,
Have you done any research into long term use of SSRIs (Paxil) and depression/anxiety? There is information that long-term use of SSRIs actually cause depression. Many people report them exacerbating anxiety as well. You should also investigate long-term use of Lorazepam and how benzos are central nervous system DEPRESSANTS so they actually cause depression. Not to mention how in long term use they worsen anxiety because of tolerance and interdose effects? They aren’t indicated for long-term use and are supposed to only be prescribed intermittently or for short-term use (less than 2-4 weeks). Both drugs also carry risk for physical dependence and severe withdrawal syndromes (so, they need to be tapered properly if one chooses to discontinue them)
Perhaps your drugs are part of the problem. They were for me and many others.
Here’s the Ashton manual in regards to the benzos: http://www.benzo.org.uk/manual
I’m sure you can find some information here as well on withdrawal: http://www.cepuk.org
Best of luck to you.
Report comment
I asked my physician about the Lorazepam because I knew it was only for short term use and he said to just use it when I need it – well I need it all the time in the situation I am in. I have been on Paxil so long it stopped working years ago I know but he doesn’t want to switch. I see a Psychiatrist in May (soonest I could get in) and I hope he changes things around
Report comment
Sounds like a new psychiatrist might be helpful, but only if s/he listens to you! You sound like a poster child for why drugs as a primary solution don’t work very well. If they were effective, they would help people become less disabled and more able to work, but it’s clear that you have not had that experience. You are absolutely right that Lorazepam should not be prescribed for the long-term, and yet the doc continues to prescribe it contrary to the manufacturers’ own recommendations. The Paxil stopped working but the doc doesn’t want to change it. Why not? Is he getting kickbacks from these companies? That’s just bad doctoring, plain and simple. If something doesn’t work, it needs to be discontinued, but that almost never happens in the world of “mental health.” Instead, you get a new diagnosis and new pills.
Based on your diagnoses, I’m going to hazard a guess that you have experienced significant levels of trauma earlier in your life, and perhaps right up to the present day. I get the impression that this doctor doesn’t give any credence to the impact of earlier experience on your current functioning, but is focused exclusively on manipulating your brain chemistry. Many years of experience as a counselor have convinced me that dealing with the impact of history is the most effective way to actually reduce anxiety, depression, and emotional instability. How to do this varies greatly from individual to individual, but I have never seen drugs do anything more than temporarily decrease symptoms, and without any other substantive intervention that deals with things like PURPOSE, SELF-CONCEPT, POWER, and RELATIONSHIPS, giving drugs does not usually lead to anything but ongoing dependence and disability.
I say this not to discourage you, but to encourage you to seek other pathways to healing. One very simple and generally free option is a support group for people who have been through similar experiences – not based on diagnosis, but on history, such as exposure to violence between parents, to child abuse, or to domestic abuse in adulthood. These groups connect you with people who understand your emotions and reactions, rather than treating you like there is something wrong with you. From there, you may be able to get some recommendations for therapists and even psychiatrists who actually deal with the consequences of life trauma, rather than treating you like a brain on legs that needs to be chemically manipulated, rather than understood and supported.
I hope this is helpful to you. I want to validate that your psychiatrist is missing the boat, and is clearly not listening or treating you with basic respect. S/he is treating you as a subordinate whose opinions or observations are of no interest. This is insulting and hurtful, and certainly does not lead to any kind of healing. There is a better way to go.
Take care of yourself, and feel free to respond – I will check and continue the conversation if you would like to do so.
—- Steve
Report comment
Thank you. I have been delving into meditation which has helped a bit. I am in a very small town so thee is little in support groups, etc. (Cancer, of course, and addictions, but little in mental health.) We have on psychiatrist in the area who works for our community center – and I am currently on the waiting list. Relaionships are screwed – my ex who has a chronic disease for over 18 years and is a catalyst for a lot of my problems, and the guy I like who has “friendzoned” me. I just feel utterly broken
Report comment
Meditation has been a life saver for me. I was fortunate to have lucked into a good therapist on my first try, and this was in the 80s before every manifestation of emotional discomfort was a reason to drug someone. (Though she did offer to connect me with a doctor who could prescribe Valium, as I recall, which I immediately and scoffingly rejected). Self-help books have also been a godsend. I particularly like Dr. Wayne Dyer’s “Your Erroneous Zones” and “Pulling Your Own Strings,” as well as “When I say ‘No” I feel guilty,” by a Dr. Emmanuel Smith (I think). Walking in the woods, riding my bike, and just sitting in the sunshine breathing in the clear air can also be highly therapeutic.
I know you feel broken, but you sound like a person with a strong spirit. Sometimes those of us with strength end up seeing things from a deeper perspective, and that can be painful. I consider myself one such person. There is a lot of ugly crap going on that can obscure how beautiful the world actually is. Sometimes just getting into the moment and appreciating the miracle of life is the best therapy of all.
Another option to consider is a hotline. There are lots of local, statewide and national hotlines for a variety of purposes. It can be super helpful if you’re feeling lonely and just need someone to talk with, or if you’re having an immediate crisis and need another perspective. Many are staffed with volunteers who have been through similar things and can empathize.
I think the hardest thing is finding people who can accept what is going on and don’t condemn or look down on your for having some difficulty dealing with what life has been like for you. The best thing of all is to have someone really listen deeply and be interested in hearing your story. Keep looking and don’t give up until you find at least one person who can do that, and then don’t feel bad about using the help they offer. You deserve and need some support that you are not getting, and I can promise you that conventional psychiatry will never be able to provide that support. There may be individuals in the system who buck the trend and really care, so look for them and latch onto them if you find one, but anyone who is trying to tell you that drugs are the answer is selling you down the river. You’ve tried that, and it clearly has not led to a better life. Time to try something else, eh?
Hope that is helpful!
— Steve
Report comment
I know you may be feeling you need it but staying for a long time on benzos is a disastrous idea. They are addictive and they are a hell to withdraw from. I doubt that a new psychiatrist will have anything good to offer (based on my experience with multiple ones) and will likely add a drug to the mix and not help you to taper off (never ever get of the drugs cold-turkey – real insanity can occur not mentioning physical suffering).
Sadly I don’t know what to advice you otehr than try to get off the drugs (slowly) first and see how you feel.
Report comment
Thanks Steve. I have always been an feeling, emotional person. I’ve had a crazy life – even battling cancer twice. I am trying to plan ahead, of course money is the biggest holdout. I do read some self-help books, but some are just mired down in minutiae. And many more say “just do this” but never tell you HOW to do it. Just be happy – okay, tell me how!
Report comment
Yes, it is always easier said than done. It’s almost insulting sometimes the tone that they assume. But I have learned to read beyond that and check for the substance of what they are saying. I do believe that thinking certain thoughts leads to feeling certain feelings, but it is a big challenge to really change one’s thinking – that’s what good therapy is supposed to help us do, I suppose. But good therapy is exceedingly hard to come by. I lucked out, but that was back in the 80s. I’d say the odds of getting a savvy, flexible, empathic therapist on the first go-round these days is probably in the 1/20 range or less. Everyone wants to diagnose you, but nobody has much to offer in terms of the “how to” question you so aptly put. I guess my only answer, in referencing my own path, is that it is a lifetime journey that continues every single day. And nobody is “just happy.” Life can be very tough, as yours has, and the world we live in isn’t exactly overflowing with empathetic concern for those who are struggling. I guess we who see more clearly have to be there for each other, ’cause no one else is going to do it!
Hang in there!
—- Steve
Report comment
I’m hanging!!!!
Report comment
“There are no meds that can help Borderline Personality Disorder.”
And bless the Lord and mother nature for that.
Report comment
I always been disturbed by how the highest functioning “disabled” people get the most money just because they used to work — and of course because THEY COULD work — but the people so screwed up THAT THEY CANT, are forced to live in extreme poverty. It’s an ass backwards system. So what if it’s harder for them than “normal” people, send the “bipolars” back to work! Then increase the SSI payments to developmentally disabled and brain damaged victims 4-fold so that they can at least live a decent life, since it’s not up to them and any choice they make whether or not to work!
Report comment
It’s not necessarily harder for the prospective employee, it’s harder for the employer. Otherwise, the burden is totally on the one wanting to work. Employers don’t want to deal with accommodating anyone, only controlling. And I don’t mean this cynically, I’ve just never known an employer who didn’t, in the end, resort to control to shut down any kind of challenge.
And if you ask someone that you are describing as ‘bipolar’ to accommodate the culture of the work force, then you’re trying to fit a square peg in a round hole, fertile ground for oppression. That’s where the system, at large, and how we operate as a culture, is backasswards, and totally counterproductive to individual, as well as social, well-being.
Not sure if this is reconcilable, other than to begin to imagine a more balanced society. That’s gonna be a stretch, although I do wonder if there are any good examples in the world from which to draw. As far as where I’ve been in my own life, along with what is most prominent in the media about the world, I haven’t seen anything yet to fit the bill. We’re scrambling.
Report comment
Talk about divide and conquer. This is exactly the kind of thinking that keeps us from achieving unity and therefore, effective, politically.
Report comment
I am devastated…………..this happened to me. 15 years on
Effexor with what they called treatment resistant depression.
After losing my job and home in the recession, I fell into a suicidal depression. I was on Effexor and Welbutrin. Finally I was put on a dose of lithium and the depression lifted………….it didn’t disappear, but went back to the mild to moderate depression I had lived with all these years. I finally had enough and weaned off the anti-depressants…….it was hell coming off effexor. A few weeks later I have a manic episode. I was told I had bipolar 2 this time.
I lost my sex drive because of the ssri and snri meds I took. The welbutrin was prescribed to help with that but it never did. I am sick after reading this. I now have to take a mood stabilizer for the rest of my life. WHO do I sue? There should be a class action lawsuit. I feel violated. I kept getting the run around about drug resistant depressions and I would have to live with depression the rest of my life. I know what happy is, I felt it “before” but never after taking anti-depressants.
I am a poster child for this article……………..
Report comment
A class action lawsuit is very much overdue. I’m sorry you have been damaged so badly by this senseless paradigm. I hope it helps to know you are not alone.
—- Steve
Report comment
“A class action lawsuit is very much overdue.”
Yeah…
Report comment
bintim,
You said, “I now have to take a mood stabilizer for the rest of my life.” You don’t actually have “bipolar II,” you likely had an antidepressant withdrawal induced “manic” episode.
I’d recommend trying to get weaned off the “mood stabilizer.” I’ll warn you this, too, could cause a drug withdrawal induced “manic” episode, however. So I’d find some good friends or family who could take care of you if this happens, and only go to a hospital if absolutely necessary.
Your best bet is to try and get out of the system.
Report comment
Just an FYI, this is what the DSM-IV-TR says about adverse reactions to antidepressants, “Note: Manic-like episodes that are clearly caused by somatic antidepressant treatment (e.g., medication, electroconvulsive therapy, light therapy) should not count toward a diagnosis of Bipolar I Disorder.”
I think the DSM5 now claims this iatrogenic pathway to a bipolar diagnosis is acceptable standard of care. But the “mood stabilizers” and “antipsychotics” don’t cure the adverse effects of the antidepressants, trust me, been there, done that. And they are all extremely toxic in the long run. My best to you.
Report comment
There’s a chance that the mania caused by withdrawal from anti-depressant is going to be temporary. The main challenge is to find a safe environment where one can experience mania and not be funneled back into the system and put back on drugs.
Report comment
Thanks Mr. Whitaker for another great article. I would just like to address one portion of it:
“This website has also published numerous personal stories from people whose lives went astray after initial exposure to an antidepressant, and of course their stories also contribute to the ‘evidence base’ on this matter.”
The glaring problem with this assessment, as I’m sure many of us are already aware, is that personal histories should not constitute an “also” to the “evidence base.” There is nothing “also” about innocent people being killed (whether directly by the drugs or by the suicidal effects of the drugs), or about innocent people being driven to madness, psychosis and violence. There is nothing “also” about brains destroyed, families ripped apart, and lives ruined. There is nothing “also” about the millions of precious children diagnosed with fictitious diseases, or the helpless homeless and despairing elderly that are coerced and drugged against their will. This IS the evidence base. It IS based on real human lives; real people, with real hopes and dreams, really destroyed by psychiatry and Big Pharma.
Enough is enough. Slay the Dragon of Psychiatry.
It should not rest upon the millions of innocent victims of psychiatry and Big Pharma to prove their case. The burden of proof is with survivors of psychiatry. It is psychiatry and Big Pharma that must be held accountable for their evil deeds and crimes against humanity. The scientific studies, percentages and statistics are necessary, but these constitute the real “also” to the hard evidence of destruction, suffering and death in the lives of real people.
Report comment
This commenter is suggesting we abandon the scientific method? An assortment of personal histories, even including tragic deaths, do not make a valid evidence base for scientific knowledge. It’s getting very difficult for me to read this website, sympathetic as I am to valid CONCERNS about big pharma.
Report comment
Regarding “Abandon the scientific method?”
You are joking right?
Do you remember the lobotomy? Doctors removed/destroyed the brain as the solution to behavioral problems?
The scientific method? There is no physical illness in mental illness and they apply physical solutions… this makes sense?
The second worst solution to the problem of mental illness is passing electricity through the brain. How in the world can this electricity help the cognitive function of the patient?
Psychiatry is based on using force instead of using reason(cooperation) with their subject/patient.
Psychiatry exists for multiple reasons, the chief one is that regular people need a doctor to legitimize their use of drugs. Without a doctor what differentiates them from the back ally junkie?
Report comment
Yes. Abandon the pseudo-scientific method that poses as a cover for coercive, abusive, and lethal psychiatry. Adopt the real scientific method which clearly proves, and has proven throughout history, that psychiatry and psychotropic drugs cause irreparable harm to innocent individuals.
We’re all in favor of real science. It’s the scientism and pseudo-science of psychiatry that must be discarded.
Report comment
What scientific method? This one:
http://www.slate.com/articles/health_and_science/science/2015/02/fda_inspections_fraud_fabrication_and_scientific_misconduct_are_hidden_from.single.html
?
The whole system is so corrupt that there can be no talk about “evidence-based medicine”.
Report comment
Also, in the world of mental illness – it is very hard to be an “educated consumer.”
Your rights are limited, and of course, because you are “mentally ill”, many doctors, hospitals, and clinics (even psychiatrists) will treat you differently than other patients and “talk down” to you. In certain settings, people will only talk to your psychiatrist — and will ignore you — because the psychiatrist is always right and always knows better than you !!!
Some psychiatrists tell you one thing — and then they tell other doctors something totally different. (I only discovered this in hind-site.) Furthermore, a number of times I tried to get copies of my OWN medical records from psychiatrists — only to discover that psychiatrists will NOT give you copies of your OWN medical records !!!)
One of the main reasons I initially consulted psychiatrists was due to a severe case of insomnia. The psychiatrists were reluctant to give me sleep aids or sedatives –instead, they attributed my insomnia to depression — and they instead put me on SSRI’s for years — all of which had their own serious side-effects and none of which actually cured my insomnia — the main reason I had consulted a psychiatrist in the first place.
Finally, after many years on SSRI’s, I was told that SSRI’s, themselves, interfere with sleep and can even cause insomnia !!! So for years, I had pleaded with psychiatrists to try other solutions other than SSRI’s for my insomnia — but they told me to stick with the SSRI’s and they would help my sleep. Imagine my shock when I saw a sleep specialist and he wanted to know why the hell I had been on SSRI’s for so long. (And, he was also the 3rd sleep specialist I saw, the other 2 I saw, saw I was on SSRI’s — and then, because I suffered from mental illness as per psychiatrists, they never really listened to anything I had to say !!!)
So, many psychiatrists who treat depressed patients and have studied for many years to become psychiatrists — actually discriminate against patients who suffer from mental illness or have other mental related problems. And the lack of transparency for a patient that is trying to be “an educated consumer” — can significantly hinder the patient’s progress !
This I find simply appalling !!!
Report comment
Dapper,
I’m pretty certain that all doctors, including psychiatrists, are required by law to hand over copies of your medical records if you request them (you will likely have to pay a fee per page). I’ve definately heard of psychiatrists refusing, and the laws may differ by state, but I do think all doctors are legally required to allow patients access to their own medical records. Best of luck.
Report comment
“are required by law to hand over copies of your medical records if you request them”
Nope. I tried for years in Michigan to get my psychiatric medical records, especially the ones from my childhood. The most I could get were dates of appointment times and hospitalizations with the names of doctors and service providers. Everything else was excluded by law because it might be “dangerous” for me to know it.
Report comment
Oh and I want to emphasis that it is a law that restricts them from giving you the records. That way the psychiatrists themselves can hide behind that law, act like they want you to have your records, but then act all friendly and be like “Sorry, we could get in trouble if we gave them to you!”
Report comment
I paid an attorney to get my psychiatric records (in USA). It was very difficult to read them but I realized the person being written about was heavily poly drugged and no longer me.
Report comment
JefferyC,
As I mentioned, I’m uncertain of the laws in all states, but did you check into what the law supposedly was? Are you certain they didn’t just lie to you? I definitely have heard of that happening to others, especially when it comes to drugging children. I’m sorry about what happened to you, and you should have a legal right to those records because they are absolutely relevant to your current medical issues.
Report comment
As far as I know, psychiatrists in most states – either will not or cannot give you copies of your own medical records — unless they are ordered to do so by a judge. So, yes, you would actually have to sue them — to get copies of your own records !!!
Furthermore, I dare you to get a psychiatrist to even tell you what his official diagnosis is of you !!! (I am referring to the specific codes used by the psychiatric community). These are the codes that will label you — and determine your course of treatment and whether you qualify for assistance.
There is no transparency here !!!
Report comment
dapper,
I’ve been handed over copies of almost all my medical records related to my psychiatric system experience. Some decent nurses, of their own accord, handed over my PCP’s medical records, likely after they’d realized I was being intentionally poisoned. My next doctor did too, after he refused to treat my family, due to the prior malpractice, although of course he didn’t confess to this.
My therapist and neurologist neglected to hand over two appointments each. And the therapist put Black Sharpie marks on her very first comment and most of the names of her friends, whose gossip was the basis for her assessment of me, unbeknownst to me at the time. But I know who I went in to her to discuss, so was able to decipher them. She did want me to sue to get the records without the illegal “doctoring up.” But everything else was handed over.
My psychiatrist’s receptionists tried to avoid handing over his records, but did so fairly quickly. I will conceded, the receptionists were right, his handwriting is difficult to decipher. But his final assessment of his treatment of me, “Foul up,” was quite easy to read.
My hospital records were handed over at a cost, but with no particular problems, actually twice. The only problem was that the second time I requested them they were sent not just to me, but to my PCP illegally (without my requesting that). Thankfully, I’d already explained to him the entire situation I’d been through and given him a medical synopsis of the “snowing” that had occurred at that hospital. And I had decent nurses following my family from doctor to doctor trying to protect us, so they just called and asked if it’d be okay if they just shredded the hospital’s records. Of course I said, yes, thank you.
Oh, yes, there was the hospital records from the hospital that shipped me to Kuchipudi’s hospital. They were handed over, again a at cost, but with no problems.
The records from the state hospital I was forcibly held, and force medicated for a nonexistent UTI, were not handed over until after the two year statute of limitations to sue were up, but were handed over after my right to sue was gone.
And the records from the hospital that gave me a forced physical, resulting in a “medically clear” diagnosis, then shipped me to the state hospital, were handed over without problem. And once I’d pointed out their illegal shipment of me to the state hospital, they did agree to forgive the $5000 physical charge.
Ironically, the only records that seemed to be missing en mass were the records from the “bad fix” on my broken ankle. Thankfully, what was handed over did include the information that I actually needed, my former PCP’s husband had been the “attending physician” at the “bad fix” on my broken ankle. This was my PCP’s motive for initially drugging me and then shipping me to psychiatric practitioners, to be defamed and poisoned.
“The dirty little secret of the two original educated professions,” shame on the medical and religious communities for using the psychiatric community to defame, discredit, and poison innocent people to cover up easily recognized iatrogenesis and pastoral sins.
Report comment
Dear someone else,
I am very sorry to hear of all your bad experiences !!!
Well, some laws regarding medical record’s may be state specific.
At least in my state, private psychiatrists and private therapists will not or cannot give you copies of your medical records.
However, I believe that all records from your primary care doctor (even if psychiatric related) — are available if you request them. Records related to hospitalizations and from clinics in hospitals — I do not know.
You may be right — I may be entitled to get my records from private psychiatrists and private therapists – but they will not give them to you. Furthermore, my current therapist told me that even if he receives a subpoena from a judge — he would refuse. (I am not really sure what that means — refusing to comply with a subpoena — normally subjects individuals to heavy fines and / or prison). I have checked records of a number of psychiatrists who I was interested in seeing — and saw that a few had been formally charged for refusing to comply with subpoena’s and refused to release patients medical records even after rec’ing subpoena’s.
It probably has to do with their fear of being sued for malpractice. (BTW: without going into details, I did get to see my full medical records of one psychiatrist and one therapist…..you’re right, their hand-writing is terrible and some of their notes / opinions — are pretty weird and far fetched…..) Furthermore, as I suspected from that psychiatrist, her notes were incomplete — and it was pretty much impossible to obtain a history of which med’s she had prescribed to me — from her records; she simply had not recorded the med’s and dosages she had given me……
But the circumstances under which I obtained them — were unique and subpoenas had been issued to these 2 doctors. So, again, in the state in which I live, you can only get these records if a subpoena has been issued (albeit, some doctors — will still stall…..I guess like Nixon, if they are afraid of being sued, they will lose some of their notes). And again, the notes were incomplete and often not really focused on our discussions……
I notice that my current psychiatrist (who has a phobia of being sued) starts scribbling frantically when i am discussing things that are off topic — but might help him if I ever sued him — although we are on good terms (so it’s his own phobia that’s kicking in). Also, I do not discuss certain topics with him I don’t want in my records — and a few times I asked him first if we could discuss several topics “off the record” and he agreed — but none-the-less continued frantically writing his notes……
Also, interesting enough my prior Psych kept coming up with additional diagnosis of me almost every week — according to him I suffered from something like 20 + depressive disorders. however, my newest Pysch has told me that he thinks there is hardly anything wrong with me……somehow, my correct diagnosis must lie approx. in the middle of these 2 doctors opinions…..But again, when I ask my current Pysch what his official diagnosis is of me — he will not tell me. He says that if he tells me — then it will make my recovery much harder……But it greatly annoys me — that as a patient — he will not tell me his official diagnosis of me. I did ask my current therapist, and he rattled off about 12 things. I questioned him about 4 of these – where he got them from — he could not explain (I think he was confusing me with another patient).
So, anyhow, again there is lack of transparency here — and as i mentioned what the doctor tells you and what he thinks and writes in his records — plus the exact codes hs uses — he will not tell me……. Of course, part of this is for my own good — as he keeps telling me to do things I cannot do, and he keeps telling me I can do them. Maybe he is right — but over the past 2 years that I have seen him, I have tried to do these things — and I have yet to be able……
I hope things are looking brighter for you, and I guess we both learned from trial and error that there are some really bad psychiatrists out there — and you must fire them if you have to. The problem I have, is that where live — it is almost impossible to find any decent psychiatrists that still take insurance, and w/o insurance their sessions can be as high as $500…….so I have been stuck with some pretty bad doctors at some points…..
Best of Luck !!!!
Report comment
dapper,
I’m sorry for what you’re going through as well. And thank you, yes, things are looking better for me. I’ve been completely drug free and divorced from the “system” (got away from all psychiatric practitioners) over six years ago now.
I hope and pray you are able to get weaned off all drugs, and get away from the “medication spellbinding,” maddening, and insanity making “system” as well.
The point of my story is that the historic function of the psychiatric industry is to proactively prevent legitimate potential malpractice suits for the incompetent mainstream doctors. Once you’ve been defamed with a “mental illness” by a psychiatrist, you’ll never find a lawyer to take a malpractice case.
I recommend you stop trying to get your medical records while you’re being medicated. And don’t discuss malpractice with doctors at all. Lie, if need be (tell the doctors the drugs are making you better, so they may be decreased), to get weaned off the psych drugs. But read up on weaning off psych drugs (I don’t know what drugs you’re currently on, but understand Breggin has a recent book on properly weaning off psych meds, and there are many discussing specific drugs on the internet).
I will warn you that it is likely you will suffer from a drug withdrawal induced super sensitivity mania or psychosis (look up the definition of these terms, if need be). Find friends or family that understand you will get sicker (and will need loving kindness and unconditional love) before you get better, and ask them to only take you to a hospital in case of an absolute emergency.
Try and convince doctors you’re doing better, so it’s okay for them to wean you off the drugs. Then, after you’re drug free, try and pick up your medical records and figure out what actually happened. My prayers are with you, dapper.
Report comment
I paid an attorney $ 300 to write a letter to my old pdoc and when I saw my records were incomplete had another letter written stating what was left out. Double check, most USA states OK you getting your psych records but the psychiatrists will fight you on this saying giving you these records “will upset you”. Remember the records are only a perception of you on drugs.
I find it interesting only pdocs won’t let you see your med records?? They don’t have full picture of you, only a slanted view. My records didn’t have how I was socially active, only negative comments and any developments were only seen as worsening mental illness never toxic drug effects. My pdoc loved to brag he verbally recorded all his daily patient contacts in his car on the way home. How exact is that?
Report comment
…and even when you get them you may discover that they are full of lies and omissions. My documents contain a whole list of sophisticated insults, mixed with lies (invented to justify the use of coercion) and somehow forget to mention such medically irrelevant details as drug names, doses and side effects. I was appalled that this passes as “medical documentation”.
Report comment
Well, I’ve piped in enough on this one, there are a lot of volatile and very personal issues attached to ‘disability,’ etc. Mostly, I see a lot of stigma and self-stigma here that I do understand is really hard to shake, but, personally, I think it’s a good goal. That’s incredibly stressful.
Where I seem to be mostly at odds with this community, in general, is that, even though I know the meds make people sick and disabled, for me, it was temporary. In the world of healing from where I come, absolutely everything is healable, nothing at all is chronic, and for me that turned out to be undeniably true. If not, I’m sure my partner, family and friends would be the first to tell me that I’m living in some delusion of wellness. Of course that’s not the case, not in the slightest.
Most unfortunately, this seems to be the hardest habit to break–the notion that people are ‘permanently damaged.’ To me, that’s yet another illusion, and only true if that’s what a person actually believes about themselves because everyone is telling them this, or treating them this way. When a person believes they can heal, they do. Those who deny that we can heal, deny their own healing.
I realize this challenges many people, but it’s my truth and I felt it was important to share, especially if we’re trying to resolve the issues of such high rates of ‘permanent disability.’ This is a complicated network of deceit and illusions, heavily mixed with social stigma and politics, and all sorts of preposterous misconceptions. I do hope this can be cleaned up. A lot of people are suffering due to these illusions, and that needn’t be the case. It’s also stagnating our society a great deal, causing it to sink into despair and violence. I think it’s a most critical issue.
Report comment
“Most unfortunately, this seems to be the hardest habit to break–the notion that people are ‘permanently damaged.’ To me, that’s yet another illusion, and only true if that’s what a person actually believes about themselves because everyone is telling them this, or treating them this way.”
Or it’s because you wake up in the morning and it takes you three hours to take a shower and get dressed because of neurological movement disorders. Then it would be impossible to drive to work. Take the bus? Yeah, that’d be quite an adventure. Thankfully I’m not THAT bad anymore, not since my teenage years. But even at its best, my movement disorder is socially unacceptable and nobody would ever hire me. NOBODY feels comfortable being around somebody with involuntary movements. So unless a person can somehow be qualified to work at home and/or by themselves, and then manage to find someone who would pay them to do said work, then it truly is a disabling condition.
Report comment
JeffreyC, it’s good to hear, at least, that your condition has improved over time. I am sorry if my posts agitate you further. I just always like to leave room for hope. None of us has a crystal ball, so the future is always uncertain.
People are speaking up and out about all sorts of things, change is really on the horizon. I think when we can feel at least a twinge of hope, something will shift in our favor. Improvements happen gradually, most often, but we have to be willing to see them.
But if we put a lid on hope, then I think that’s pretty damning, in general, and things will go south.
Nothing in easy here. Kind of a hamster wheel after a point, I guess…
Report comment
Alex and JefferyC,
I maintained a very positive attitude during the major drug induced poisonings I was subjected to, which I know allowed me to escape the “system.” I must confess, I share some of the long run adverse reactions of the drugs with JefferyC, although not likely as bad. I do still wake up after a night of constant brain zaps exhausted some days. And doctors are now aware these are adverse reactions to the psych meds, but they have no solutions.
And I did get illegally fired (according to the state, long story) from a job after my boss at the time saw me have an uncontrolled head movement once. The tardive dyskinesia is a problem with the atypical antipsychotics. Thankfully, it’s not often a problem for me, but the nighttime brain zaps still are. Right now I’m working out of my home. I agree a positive attitude is extremely important, but the psych drugs are toxic and damaging to people for much longer periods of time than the psychiatric industry or government admit.
Report comment
No, the doctors don’t have solutions, but that doesn’t mean solutions don’t exist. I know I sound like a broken record about this, but again, this is all energy that can be manipulated, but that takes focus and work. There are also herbs that regenerate our organs from toxic damage.
If I’m the only one here that knows how that works, then I guess I’ll need to start working on my book. This can all be explained and illustrated in about 20 or so pages, by my off-the-cuff estimation. It’s not as complicated as one would think.
Report comment
Alex,
If you have a suggestion for getting rid of morning (lucid dreaming) brain zaps I’d be grateful. I regularly check the web for possible solutions, and have yet to find any that work. Actually, I haven’t even found others who have these for such an extended period. (It’s now been 14 years, and I’ve been completely drug free for six now.)
Plus, the brain zaps do relate to the religious story of my dreams. And a friend from my church did give me a comparative religion synopsis that pointed out that one religion believes that God speaks through people via electronic like emanations, so I suppose it’s possible they relate to my “spiritual journey” rather than the drugs. I just don’t know. But they’re annoying, and do make getting up and getting going slower some mornings. I’d be grateful for any suggestions though.
Report comment
I’m familiar with brain zaps, which is pure energy. Extremely uncomfortable, I do know this.
These are, indeed, connected with what is happening with you in your journey. Although I’d look at your life journey in general, integrally, not just your spiritual journey, what you feel is a physical embodiment of energy, so it’s real on all levels. This is a multi-dimensional energy phenomenon.
The most important thing to address first is the stress this causes you, and of course, stress is part of the manifestation, in general, so the anecdote energies we’re looking for are: soothing, ease, calm, relaxation. Breathing is how we administer these through our bodies.
When these zaps hit, or any anxiety, taking slow long deep breaths while consciously focusing on these four energies–imagine them as colors and notice how those colors make you feel. Really allow your body to take them in by visualizing and feeling the energy/vibration/feeling of soothing, ease, calm, relaxation. Keep breathing in these energies and allow them to flood through your body, mind, heart, and entire energy field around you.
Pay attention to how your body shifts in vibration when you imagine these filling your body, and especially imagine them soothing and calming your brain, allowing it to release stress.
A daily habit of this exercise in meditation will allow you to release excess energy daily. Energy builds up inside of us from day to day unless we know to consciously release it, by bringing calm and ease into our bodies.
Especially when our lives have been perpetually stressful, or our minds are constantly wound up, we have to make a conscious habit of releasing energy, or we will become physically ill, or somehow, lose our balance. Eventually, as we practice this consciously, releasing excess energy becomes part of our natural process and it’s so much easier to stay centered and grounded, even in stressful situations.
In essence, at the core, that’s what you’re experiencing, excess energy. There are other things going on, as there always are multiple factors in any manifestation, but when we keep it general like that, it’s easier to release and shift, rather than struggling with specific meanings, right off the bat. Easier to get meaning once you’ve released excess energy.
If you want to look further into what all of this means to your life path, which of course it does, events like this are always significant that way, feel free to contact me for an energy reading, on the house! Happy to check it out, if you wish. It can all be done by email, if that’s what you prefer. I can also do a phone reading, whichever.
[email protected]
Hope this helps!
Report comment
I will confess, however, sometimes these lucid dreams do give me insight into my work, which is a good thing. For example, yesterday morning I was dreaming about a piece of artwork I started 14 years ago, and have yet to complete. I have called this piece “The Puzzle” for the past 14 years (long, but interesting, story).
“The pieces gone, left the puzzle undone,” is from Beautiful Lyrics Christina Aguilera – Genius, a song from that time. I did get the “puzzle” pieces back, after the school they were on loan to closed it’s doors forever. It was initially started for a school named Summit Academy, so was a work depicting mountain summits.
After I’d gotten the pieces back I did some more painting on them, I painted a man and woman singing love songs across the mountains tops. The piece is still unfinished (it’s very large and I don’t have a studio space to work on my large works right now). But yesterday morning I realized what “The Puzzle” was actually a painting of, “Go, Tell It On The Mountain, Over the hills and everywhere;
Go, Tell It On The Mountain ….”
I do have a religious story going on in my dreams. I’m not quite certain why, but I do. Except I did pray to paint for God back in art school, when I realized most of the work in the art history books was of a religious nature. I figured that’d be the best way to get into those books some day.
Perhaps I’m supposed to have the lucid dreaming so my subconscious can continue to awaken my conscious self to the actual meaning of my artwork? I don’t know, but no one else does either, including doctors.
Beautiful was one of the love songs that helped give me hope after I’d been psychiatrically defamed and had evil “voices” pumped into my head with massive major drug interactions. Here’s more of those lyrics:
“Every day is so wonderful
Then suddenly it’s hard to breathe
Now and then I get insecure
From all the pain, I’m so ashamed
[Chorus]
I am beautiful no matter what they say
Words can’t bring me down
I am beautiful in every single way
Yes, words can’t bring me down, oh no
So don’t you bring me down today.”
What if there is a kind and loving God who inspires hope, even via the pop music? No one actually knows for certain.
Report comment
Thanks for the insights and offer, Alex. The brain zaps do feel like they are a way of getting rid of excess energy, so to speak. But since they primarily occur in relation to lucid dreaming, they seem harder to consciously control. I do also seem to get them during prayers in church, not sure why that is. And sometimes when in crowds, like when watching plays or at the movies. They seem to me to relate to the “collective unconscious” theories. Thank you again, Alex.
Report comment
Oh, then you’re definitely getting ‘zapped’ by the collective energy. Those times you mention are when we are most open. That’s pure empathy, you’re an empath, which means you are especially sensitive to energy. I believe this is the case for a lot of us on here, and for a lot of people who wind up diagnosed and medicated. The psychiatric/psychological/academic culture tend to see this as a shortcoming, from what I’ve gathered. It’s what gets people erroneously diagnosed, and where environmental issues are overlooked. I’m certain, however, that it is a gift, because in essence, you are tapping into the truth of the collective, which is fantastic information. But the collective energy is filled with diverse energies, some negative and some positive, so one thing an empath can learn to do well is to discern between these, on an intuitive level. When you trust your intuition, you are on your spiritual path.
For empaths, it is especially important to practice boundaries and grounding. This is a practice and discipline of focused meditation. It’s what I learned in my healing, which was of supreme value, and one of the basic things I teach and help others practice. It can be a bit of a rocky road getting into these habits of grounding in our bodies, because it does light up some heavy energy. But that’s important, because it is where healing occurs.
If we are patient with this and simply allow it to flow out of us, as if it were a river of energy, as we breathed and relaxed best we can in the moment, then we would eventually clear our spaces of old heavy energy from trauma, etc., and come into present time with our light.
When we are grounded and with firm, clear boundaries, we can better distinguish between ourselves and the collective. We are all part of the collective on a soul level, but at the same time, we are individual people, so we work to balance these two realities. They’re perfectly copacetic.
Report comment
One thing I have been pretty sure of — is that my mood / depression seems to get worse — if I feel that there is some inflammation in my head. This probably sounds strange, I have told a number of doctors about this. I did get several MRI’s to check for tumors, etc. – but nothing was ever found….
I have found that diet plays an important role in mood — so my diet is filled with foods and supplements that are known to be anti inflammatory (for example fish oil and olive oil). And I often do feel better after taking both fish oil (but you have to take like 10 capsules for this) and olive oil…….
About 3 days ago, I read about a new study that claims there is a link between inflammation and mood / depression — so I think I was right all along. (Also, now they are talking about gut bacteria — and that the may be a link between poor gut bacteria and depression…..)
Years, ago in the early 1970’s when my grandmother was in her early 70″s she told her primary doctor that she started taking an aspirin a day — because it made her feel better. he yelled at her every time she told him this……..then some 20 years, later I’m guessing in the early 1990’s, all these studies starting coming out — claiming that an aspirin a day for some people was good. My grandmother, who was then in her early 90’s, really took pleasure in rubbing this in her doctor’s face…….my grandmother lived to almost 100.
So, you always need to try different things. And there have been several studies suggesting that high dose of fish oil is good for mood / depression. And there is definitely some truth to the matter that since fish oil cannot be patented — there are not that many studies on it — since big drug companies have little interest in things which cannot be patented. Often if I have bad mood, coffee helps (which is known to be a mild anti-depressant) — however, I seem to suspect, that for at least me, coffee acts as infammatory source — albeit, this may also be the result of the acidity in the coffee. Sometimes when I feel inflammation in my head and my mood worsens, i take aspirin — and my mood gets better…..
Years ago, I had complicated surgery on one of my ears — and that ear was pretty much always infected for many years after…..of curious nature, pretty much after my ear surgery — was when my depression / mood got much worse…….I went to dozens of ear, throat, sinuis specialists — and they all told me there was no correlation…….and again, I got numerous follow-up images of my ear and head afterwards — but no doctor ever saw anything…….
But again, 3 days ago — they released this new study suggesting link between inflammation and depression/ mood, and my use of anti-inflammatory supplements and foods — always supported my opinion of this……
Maybe when I am 90 years old and have died, the autopsy will reveal a growth or source of inflammation in my head that I always seem to feel,,,,,,????
who knows ?
Anyhow, I hope that some of my experiences / thoughts may be helpful to others……
Good luck !!!
Report comment
Dapper, yes there is a definitely a correlation between gut inflammation and mood.
What I learned in Chinese Medicine is that when our gut is not generating enough flora (lots of reasons for this, mostly stress-related), it ‘heats’ up. Warming/cooling are terms used in CM to discern between the density and lightness of energy. Warming foods are dense, and can cause the inflammation if we our dietary intake isn’t balanced, overall.
And I agree with you that it is so individual, everyone’s body reacts differently to different things, depending on so many different factors and individual preferences. We each do our trial and errors, finding what works for us best. No study will beat you to the punch of your own intuition and inner guidance.
So, when our guts get inflamed/heated up, that ‘heat’ travels to the heart, constricting it and causing anxiety, and also to the brain, which would be that feeling of inflammation you have, if nothing physical has been found. The heat would produce that sensation, and perhaps, a feeling of ‘fogginess.’ All of this would definitely translate to depression and agitation in the mind and body.
Our energy is supposed to run like clear water, but when it gets heated up and filled with density, it can feel more like sludge. That can be cleared up in a lot of ways, and dietary is one of them.
I’ve also heard fish oil helps a lot of people. For me, Kefir, probiotics, and a generally high alkaline diet (raw greens, green smoothies, etc.–these are ‘cooling’ foods) for a few days or even sometimes for a week, (if I can take it without sending my body into depravation), is what reduces gut inflammation when it occurs, while nourishing healthy flora and cooling the gut, which then relieves the pressure in, both, heart and brain.
I don’t mean to continue veering this thread like this, but when I see something about healing that I feel I can respond to with some clarity, it’s my compulsion–perhaps my nature, even–to take advantage of it. Hope it’s of value to at least some people.
Report comment
Alex,
You stated, “Oh, then you’re definitely getting ‘zapped’ by the collective energy. Those times you mention are when we are most open. That’s pure empathy, you’re an empath, which means you are especially sensitive to energy. I believe this is the case for a lot of us on here, and for a lot of people who wind up diagnosed and medicated. The psychiatric/psychological/academic culture tend to see this as a shortcoming, from what I’ve gathered. It’s what gets people erroneously diagnosed [True], and where environmental issues are overlooked [True.]. I’m certain, however, that it is a gift, because in essence, you are tapping into the truth of the collective, which is fantastic information [True]. But the collective energy is filled with diverse energies, some negative and some positive, so one thing an empath can learn to do well is to discern between these, on an intuitive level. When you trust your intuition, you are on your spiritual path.”
I was quite certain I was on a spiritual journey, and didn’t have a “mental health” problem when I went to a “Christian” psychologist initially. I’d had a dream I’d been “moved by the Holy Spirit,” which I consider to be the voice of common sense, although it’d been an unusually powerful dream. The “Christian” psychologist, according to her medical records, misdiagnosed me based upon lies and gossip from the people who’d allegedly abused my children.
I didn’t realize my spiritual journey, at the time, was to point out the “dirty little secret of the two original educated professions,” which now seems to be the case. Apparently, the psychiatric industry has historically, and is still today, in the business of covering up the sins of the clergy for the religions and easily recognized iatrogenesis for the mainstream medical community.
What’s fortunate for me is I had forty hours of unbiased psychologic career testing, not long before I was drugged, and no family history of mental illness, so never really believed the psychiatric defamation of me. I’m supposed to be a “judge” or “architect,” according to Myers Briggs testing.
And I agree, Alex, that my gut instincts are from the wisdom of the “collective unconscious.” I hope and pray that the mainstream religions and medical community will some day learn that it is, and was never wise, or morally acceptable, especially to God, for them to cover up their sins and malpractice via psychiatric stigmatization, tranquilization, and poisoning.
Report comment
Alex,
Hi !
Thanks for your recent info regarding chinese herbal medicine, gut bacteria, and inflammation. it sounds like you have done a lot of research !!!
Can you direct me to some good resources (books, websites) — where I can learn more ???
I would greatly appreciate it !!!
thanks !!!
P.S. I did meet with a very interesting specialist in CM a few years back; part of what made him so interesting is that he also has a formal MD as well……he did agree to make make up an herbal mixture for me — but he refused to tell me what it would contain (i.e, it was his secret mixture) – I told him that I would not take a mixture — without knowing what was in it (I have certain allergies and there is potential for interactions between med’s and supplements). He refused, so I never took his herbal mixtures…….. interesting, again lack of transparency even with CM specialist….
Report comment
The other problem with supplements — according to latest study — is that 90% of supplements are fraud – they do not contain even traces of what is suppose to be in them — and they can contain some things you may be allergic to — because there is basically no regulation in US regarding supplements and vitamins …….
Report comment
Hi Dapper, it’s my training, I’m an integral health practitioner and teacher. Plus I applied it to my own healing. So I researched it by, both, education and application, and it all worked for me.
Here’s a great website about gut health and the impact on our health from our inner ecology. Tons of info, plus products, seminars, and she’s got a great book out called The Body Ecology Diet, with great info about how our bodies process different categories of foods, in general.
http://bodyecology.com/
I partner with an herbalist in my own practice, but she’s been having website issues, so it’s down for now, but if you email me, I’ll be happy to share her contact info with you. When I was using her herbs as I healed from meds toxicity, she also made me a personal mixture and when I asked her for the ingredients (there were a bunch), she not only told me, but she educated me about them. Sound like she might be a good match for you.
I don’t want to post to this thread any longer because it’s so off topic, now, but I’ve appreciated the inquiries. Plus, this’ll be my last post for a couple of days, as I’ve got some work to do which will be keeping me busy. I’m posting my website with my contact information below. Anyone that wants to get in touch with me about healing or references, I’m happy to provide any information or services at no cost, if you mention MIA. That’s my volunteer healing work now, that was my resolution for the new year. Been a bit busier than usual, so it might take a day or two to respond, but I will.
http://www.embodycalm.com/Contact.html
Bob, my apologies for the digressions.
Best wishes,
Alex.
Report comment
The inflammation link is really common sense – think about times when you’re down with a flu. Inflammation involves immune cell signalling to brain in order to wind down activity and keep you nicely cuddled in bed in order to recover. The problem is when there is chronic low-level inflammation going on from which one does not recover. It leads to chronic tiredness, cognitive problems and depressed mood. There are many things that can cause it, obesity being one (fat cells release a lot of inflammatory cytokines). Apart form anti-inflammatory drugs such as aspirin (my favourite) sport is a great way to deal with some of the ill effects though it’s not always possible – that obviously depends on how strong the reaction is (if you can’t get out of bed you’ll not go jogging).
Report comment
What I find most amusing, is that apparently in the early 70’s with the release of “one flew over cucko’s nest” — there was supposedly a big shake-up in psychiatric treatment, and doctors were all supposed to be talking more with their patients and getting them more involved in their treatments.
At least in my opinion, regardless what psychiatrists think, little has changed. maybe it is the fear of lawsuits — if they don’t do anything for you — but yes, I think doctors continually pressure patients to take drugs that either are not working or are harming you….when you talk to them about it, usually they tell you need to take HIGHER dosages of the drug to get the full benefits and at the HIGHER dosages the negative side effects will disappear….so after they give you the higher dosages, you feel even worse — and then doctor tries to convince that you need to stay on the higher dosage for much LONGER period of time then he originally told you — to get the full benefits of these drugs and for side-effects to go away. So you stay on higher dosages for longer period of time — and you are sicker than you have ever been — and the negative side effects are so severe — you have lost all ability to function. Finally, doctor agrees that drug is not working (after 6-8 mos of your life have been a living hell) — and then you are in for one more surprise — now that you have been on this drug for 6-8 mos at this high level — it is almost impossible for you to get off these medications !!!! You are now addicted to these anti-depressants which have ruined the past 6-8 mos of your life, and you now waste an additional 2-3 mos in agony — until you have managed to wean yourself off of these med’s completely……..
While I do realize that psychiatrists are experienced and are not intentionally making anything up, going forward, I have learned to trust my instincts — and now, if a drug is not working and I have severe side effects that don’t go away after several weeks — I insist on stopping these drugs — despite my doctors advice……..
And I have been in situations where med’s which are making you much sicker — are literally being shoved down your throat — w/o ur permission……
So, have things really improved that much !!!
Report comment
In many ways this is quite helpful, pointing out how drugs correlate with an increase in mental illness. And how this correlates with what’s called disability. In ways quite valid points. Ground breaking, even.
But let’s take a different viewpoint. It also points out that when a person is on disability they are considered a non-working entity, regardless of their contribution. They’re considered unhealed. Women ALSO used to not be allowed to work for a living, did this make them all permanently disabled or was there some kind of general stereotyping involved discriminating against part of the human condition?
I mean, I understand what’s being pointed out, and how drugs are involved, but what about the “few” people who “continue” to be schizophrenic because they are on disability, even though they aren’t or have never been on medications, are these then the ones severe enough to try the “medications” on, because we still have to keep them in reserve?
I mean to judge whether someone is in the workforce as denoting whether they are healed or not, this is another “diagnosis,” fit for the DSM, in many ways, and goes with it’s politicized agenda, which really doesn’t address what’s actually going on with the humans they are judging. If you’re not adding to a capitalistic society, which keeps the drug companies running as well, then you’re disabled is the criterion used here to point out what’s wrong with the drug companies.
It’s even quite debatable, given what’s being done to the planet by people all earning a living doing it which side of the “crazy,” “not crazy” spectrum might be considered crazy or disabled. And I’m not saying this to call “those” people crazy either, it just points out the lack of attention to emotional problems, that perhaps the severest ones end up being given the money to run things lest the dysfunction of the whole system come to light.
Report comment
JeffreyC
In the state where I work I wouldn’t let my cat or dog live in any of the group homes since they’re not fit for people to live in. Staff are bullying and abusive at worst and condescending at best and the places are filthy. It’s also rumored that what little money people do have is stolen from them by the staff, who then blame it on the other residents. When the residents state that their money was stolen the staff point to the fact that they can’t be believed since, after all, they’re “mentally Ill”!
As you point out, all of these places require you to be on a drug cocktail. Even the best one of these group homes requires you to be on the drug cocktail. It’s no way for people to live. What happened to human and civil rights as well as ethics and compassion. Society doesn’t care as long as the “mentally ill” are kept out of sight so they can’t bother anyone.
Report comment
Something happened here to my post. This goes to JeffreyC for his last post below.
Report comment
I found and read it anyway and couldn’t agree more. It’s a travesty. These programs are supposed to be helping people, but are the biggest source of misery and despair in the lives of most the people they are being PAID to help. But a “mentally ill” person living on government welfare money is the lowest of the low in our social class in this country. It’s a double whammy of prejudice and hate and the more I waste my time reading forums and stuff online the more convinced I am that the system in place is supposed to be that way. Many people in this sick country would not tolerate these welfare services if they didn’t know that they were making the people who receive them miserable. They don’t want emotionally damage people to heal or get better, not unless they do it for themselves. If a journalist ever raided a group home and found residents sleeping in nice beds, playing musical instruments, gardening, etc, it would be a national outrage.
Report comment
hello everybody ,i ve read an article about the great benefits for the cure of schizofrenia and other mental hillness by fasting for long periods(25-30 days).it was practised in russia in the sixties by dr nikolayev in moscow.does anybody knows if the results are true.a doctor named alan cott made more or less the same discoveries
Report comment
Hi Robert,
I found the same in Germany.
http://www.depression-heute.de/blog/64-versagen-in-der-behandlung-depressiver-patienten.html
Antidepressive Medicine seems to be more dangerous than Neuroleptics.
The number of people who had a depression and were disabled doubled from 2000 to 2009.
In 2000 there were 12.232 depressive Patients disabled
In 2009 there were 23.532 depressive Patients disabled
(in Germany depressive disorders are called F30-F39 Affektive Störungen)
Original Data sheet is here:
https://www.gbe-bund.de/oowa921-install/servlet/oowa/aw92/WS0100/_XWD_PROC?_XWD_106/2/XWD_CUBE.DRILL/_XWD_134/D.946/14321
And worst of all: Never before so many persons were treated with antidepressants and never before there were so many depressive patients!
Best wishes to you
Peter
Report comment
“Antidepressive Medicine seems to be more dangerous than Neuroleptics.”
You’ll find that everyone experienced on this subject agrees that neuroleptics are the worst. Irreversible brain damage with every dose and permenant neurological dysfunction. They really are a chemical lobotomy. Over time, they even shrink the frontal lobes and cause a 20% reduction in brain volume in as many years.
AD’s on the other hand are more hit and miss. Some people are noticably harmed by them, some not. The tolerability of the two are also at opposites; most people can and do keep taking AD’s, but even in clinical trials they deal with high (zyprexa trials at 60%) dropout rates.
Lastly, AD’s have been around the norm population for about two decades now and it has been mostly uneventful. But follow this link to see what happens when a neuroleptic hits the norm market: http://www.askapatient.com/viewrating.asp?drug=17854&name=REGLAN
Report comment
“You’ll find that everyone experienced on this subject agrees that neuroleptics are the worst.”
I tend to agree. I was on super low doses for a short time and I still have (2.5yrs after) days when I suffer neurological side effects.
Btw, Zyprexa is not an AD it’s an antipsychotic or a “mood stabilizer” depending on whom you ask. In my view, together with Seroquel and benzos it forms an axis of evil – worst drugs ever, at least in my experience.
Report comment
SSI is supposed to be for low-income people. Yet they still want you to be disabled in order to receive it. What about people who are getting divorced and walking away with nothing? How about people whose spouses have died and left them with nothing?
Report comment
And the approval process is rife with fraud..
http://www.vocativ.com/culture/health-culture/fraud-behind-common-prescription-drugs/
Report comment
“The rise in the number of “disabled” mentally ill is continuing its march.
It is affective disorders—and not psychotic disorders—that is driving this increase.”
Surprise, surprise… Let me guess – it’s “bipolar”. I can see that the drugs are working wonders (for pharma’s bottomline).
Report comment
I am confused. What percentage of the population is SMI?
Here Whitaker writes
“the number of people receiving an SSI or SSDI payment because they had been “disabled” by a mental disorder rose from 1.25 million in 1987 to 3.97 million in 2007.” USA population 301 million
And on the official website it is written
“In 2014, there were an estimated 9.8 million adults aged 18 or older in the United States with serious-mental-illness. This number represented 4.2% of all U.S. adults.” https://www.nimh.nih.gov/health/statistics/prevalence/serious-mental-illness-smi-among-us-adults.shtml
USA population 319 million.
Report comment