

In the wake of back-to-back mass shootings in El Paso and Dayton last month, President Trump stated that millions of Americans posed a great threat to public safety, and that many in this group needed to be locked away.
“We must reform our mental health laws to better identify mentally disturbed individuals who may commit acts of violence, and make sure those people not only get treatment, but when necessary, involuntary confinement,” he said.
At a subsequent rally in New Hampshire, Trump spoke more explicitly about his plan: “We will be taking mentally deranged and dangerous people off of the streets so we won’t have to worry so much about them. A big problem.”
The idea of locking up those society calls “mentally ill” or “mad” has long been present in American society. Trump’s calls for locking up the “mentally deranged” presents us with a Back to the Future moment: the impulse to lock people up for public safety reasons is an age-old one, but it comes at a moment when digital technologies are making it easy to monitor an individual in our society. Indeed, there is now on the market a newly approved pill offering society the possibility of creating what might be called a digital asylum. Those deemed dangerous to society may be ordered to take an antipsychotic equipped with a sensor that will not only provide society with assurance that the person is taking the pill, it will provide other personal information to monitoring authorities. The haunted asylums of the past may be replaced by a Big Brother pill that has now arrived.
Back to the Future
In 1751, when Quakers and other community leaders in Philadelphia petitioned the Pennsylvania Colonial Assembly to build a “hospital” that would house the “mad,” Benjamin Franklin wrote both of how hospital care could prove curative to many and of how there was a need to sequester the many lunatics “going at large [who] are a terror to their neighbors, who are daily apprehensive of the Violences they may commit.” When Pennsylvania Hospital opened in 1756, the “lunatics” were kept in gloomy, foul-smelling cells, and regularly “chained to rings of iron [or] restrained in hand-cuffs or ankle-irons.”
That societal impulse, to lock up those deemed mad for public safety reasons, has waxed and waned ever since. In the 1790s, Quakers in York, England reconceived of the mad as “brethren” and created a Retreat that sought to provide humane care consistent with that conception. American Quakers then established similar asylums in several states, and the notion that the “mad” were a threat to public safety waned, at least within the philosophy that governed the creation of those facilities.
In the late 1800s and first decades of the 20th century, eugenic ideas began to take hold in the United States, and those deemed “mentally ill” were put in large hospitals and regularly kept there for years in order to “segregate” them from the general population. However, this public policy was not driven by a societal worry that the “mentally ill” were a threat to public safety, but rather that they needed to be locked up to prevent the “mad” from passing on their “bad genes.”
In the wake of World War II, public support for eugenic ideas lessened, as it was these ideas that had fueled Nazi Germany, and thus the “public safety” rationale for locking people in mental hospitals waned. In the early 1960s, the emptying of the state hospitals began, with the public informed that a combination of outpatient care and antipsychotic medication could help the “severely mentally ill” live decent lives in community settings. During this decade and the next, there were even a number of popular novels and films that presented the patients in mental hospitals as heroic characters living in a mad society. In One Flew Over the Cuckoo’s Nest, it was those who ran the hospital who were seen as truly mad.
The tide began to turn again in the 1980s. Homeless individuals showed up on city streets, and while that was seen by many as a policy failure, one created by Reaganomics, E. Fuller Torrey began pushing for societal policies that would force the “mentally ill” to take their antipsychotic medication, and he used a “public safety” argument to make his case. People with schizophrenia off their medication were likely to commit horribly violent crimes, he said, and as he pushed states to pass laws that authorized forced treatment in community settings, he used instances of mass killings to bolster his argument in his media appearances. Without such legislation, he told 60 Minutes in 2013, our country would just have to accept such regular outbursts of random violence. “There are the consequences, when we allow people who need to be treated to go untreated,” he said.
The NRA has put Torrey’s claims to political use. Blaming “the mentally ill” for mass murders became a way to deflect attention away from laws that allow for easy purchase of assault weapons. “The truth is that our society is populated by an unknown number of genuine monsters — people so deranged, so evil, so possessed by voices and driven by demons that no sane person can possibly ever comprehend them,” said NRA President Wayne LaPierre after Sandy Hook. “They walk among us every day.”
This “dangerousness” narrative, of course, is countered by academics, advocates, and policy-makers who are familiar with the scientific literature, which tells of how there is no meaningful link between mass shootings and people said to have a “serious mental illness.” However, people with psychiatric diagnoses are at increased risk of being victims of violence. As Vanderbilt University researchers Jonathan Metzl and Kenneth McLeish wrote in a 2015 paper: “Blaming persons with mental disorders for gun crime overlooks the threats posed to society by a much larger population—the sane.”
While that response to the dangerousness narrative gets some play in the media, it doesn’t win the hearts and minds of a majority of the public. In a 2018 Post-ABC poll following the mass shooting at Parkland, 57% of respondents believed that “mass shootings were a result of failures to identify and treat individuals with mental health problems.” Seventy-seven respondents said they thought that “more effective mental health screening and treatment could have prevented the shooting at Marjory Stoneman Douglas High.”
In a sense, we are now back to where we were in 1751. Benjamin Franklin argued that new treatments could prove curative to many lunatics, and that the public needed to be protected from the “lunatics” because of their violent ways. That is, in essence, the same argument advanced by Torrey, with antipsychotics the curative agent of the day, and as for the language employed by LaPierre, who told of “monsters” walking free in our streets, his words were much harsher than any used by Franklin and his fellow Quakers.
A widespread belief that the “mentally ill” are responsible for much of the violence in our society presents several ‘policy’ questions. Who are the “seriously mentally ill?” How can they be identified? And once they are, how can their behaviors be monitored and “treatment” insisted upon that, at least in theory, will present them from acting in such violent ways?
The mental hospital long served as the confinement of choice. Compulsory outpatient treatment legislation has served as an extension of that confinement. And our society is now glimpsing a new possibility. The introduction of the first “digital pill” into the marketplace, Abilify MyCite, portends a Black Mirror-esque asylum that would reside within the human body: a digital version of the 18th century panopticon.
The Panopticon
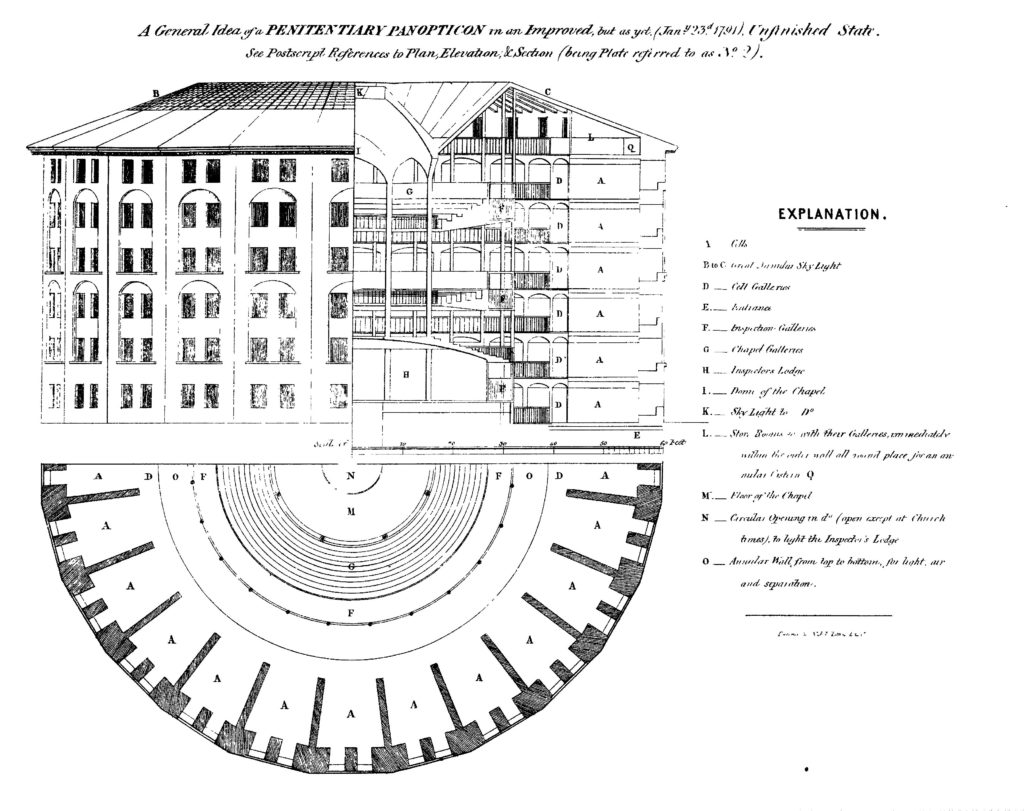
In 1791, English philosopher and social theorist Jeremy Bentham designed the panopticon, both a physical structure and a self-contained surveillance system. The panopticon’s circular design gave the guards, situated in the center, the ability to observe all inmates simultaneously. But the incarcerated persons could never ascertain if or when they were being watched:
“The Building circular — an iron cage, glazed — a glass lantern about the size of Ranelagh — The Prisoners in their Cells, occupying the Circumference — The Officers, the Centre. By Blinds, and other contrivances, the Inspectors concealed from the observation of the Prisoners: hence the sentiment of a sort of invisible omnipresence. — The whole circuit reviewable with little, or, if necessary, without any change of place.”
— Jeremy Bentham (1791). Panopticon, or The Inspection House
Bentham’s panopticon would become a central metaphor in the work of French philosopher Michel Foucault, and the emerging field of surveillance studies. Foucault’s theory of panopticism referred not just to a physical building, such as a prison, hospital, factory, or school, but to the ways that power and knowledge function across society, and how social control is exercised.
Foucault theorized that power is based on both the ability to observe others and the knowledge obtained through that observation. There is always an inherent power imbalance between the “omnipresent” and “invisible” watchers and their “permanently visible” subjects. As Foucault wrote in Discipline and Punish: The Birth of the Prison:
“Traditionally, power was what was seen, what was shown, and what was manifested . . . Disciplinary power, on the other hand, is exercised through its invisibility; at the same time it imposes on those whom it subjects a principle of compulsory visibility. In discipline, it is the subjects who have to be seen. Their visibility assures the hold of the power that is exercised over them. It is this fact of being constantly seen, of being able always to be seen, that maintains the disciplined individual in his subjection.”
In George Orwell’s dystopian novel Nineteen Eighty-Four, the physical infrastructure of the panopticon becomes the Telescreen, a device that “received and transmitted simultaneously,” functioning as a television, security camera, and microphone. The Thought Police used the Telescreens to continuously monitor persons deemed of interest to Oceania and to root out the presence of “Thoughtcrime” among them.
Orwell wrote of the Telescreens: “There was of course no way of knowing whether you were being watched at any given moment . . . you had to live . . . in the assumption that every sound you made was overheard, and, except in darkness, every movement scrutinised.”
1984 Came Early for “Mental Patients”
In her 1984 poem “To Be a Mental Patient,” psychiatric survivor and cross-disability rights activist Rae Unzicker wrote:
“To be a mental patient is to be stigmatized, ostracized, socialized, patronized, psychiatrized.
To be a mental patient is to have everyone controlling your life but you. You’re watched by your shrink, your social worker, your friends, your family. And then you’re diagnosed as paranoid.
To be a mental patient is to live with the constant threat and possibility of being locked up at any time, for almost any reason.”
Unzicker told of a life lived under surveillance, and of suspicion. Psychiatry has its “Thought Criminals” too—those persons diagnosed with “serious mental illness” who will not admit to their illness, or comply with a doctor’s orders. Such individuals are pronounced as suffering from anosognosia, or “lack of insight.” They are not willing to observe themselves as ill, and therefore, to desire care; that is, to submit to medical authority.
Gail Susan Harris, my mother, came to be viewed as one of those “dangerous, noncompliant” types. My early childhood was spent inhabiting two distinct realities. The first reality was life with my mother when she was heavily medicated on Haldol. Most days, she was able to attend to my basic needs, but she was often sleeping, at times so sedated as to be nearly impossible to wake. I learned how to fend for myself, making cheese sandwiches and eating them in front of the TV as she slept.
The second reality was when she made the decision to flush her meds, a choice she would make over and over during the course of her short life. During these times, my mother would transform into a different person. She stopped sleeping as much. Her eyes went from dull and glazed to alert, flashing, darting this way and that. She let me in on a terrible secret, in hushed, conspiratorial tones: Nazi doctors were hiding among us in plain sight, and she was meant to expose the truth and save the world.
My mother’s fear of surveillance was all-encompassing. She would stop answering the telephone and would open the door to no one. One frigid winter day in 1979, convinced that the Nazis were monitoring her thoughts via the television screen, she heaved it out of our third-story apartment window. In such instances, our family would bring the police to break down the apartment door and forcibly take her to the Milwaukee County Mental Health Complex, the local public psychiatric institution. I’d end up either on a family member’s couch, or in foster care. This cycle would repeat, over and over, until the State finally took me away from her when I was five.
Reflecting on Unzicker’s experience, and my mother’s story, I can’t help but wonder: Maybe the very people who have been diagnosed with “paranoid schizophrenia” for insisting that they were being monitored and tracked by powerful government entities were not quite as “delusional” as everyone believed. Maybe they were actually prophets of a sort, picking up on dystopian realities yet to come.
In 2019, it can no longer be considered paranoid to say that they’re watching us. Whenever we are on the Internet, our behavior is being monitored, analyzed, and remembered. Cameras monitor our streets, our public spaces. Credit card companies track and analyze our spending habits. All of our health care visits and drug prescriptions become part of an electronic health record. The digital panopticon is in place, and “they” are discovering new ways to watch us, all the time.
Big Brother Moves Inside You
At the 2018 meeting of an industry conference called HLTH, Otsuka Pharmaceutical CEO Kabir Nath and Proteus Digital Health CEO Andrew Thompson gave a presentation titled “The Future of Medicine.” They were there to tell about the world’s first digital pill, dubbed MyCite, which combines the antipsychotic drug Abilify with a sensor that reports whether the patient has taken a daily dose. When their turn to present came, the pair walked triumphantly onstage to the strains of Van Halen’s “Right Now.”
After waiting for the applause to die down, Nath, in an elegant, soothing baritone, told of the medical reality now at hand. “We’re excited to be here this afternoon to talk to you,” he said. “Not only about the fact that the future of medicine is digital . . . but that [the] future is here already.”
Otsuka is the manufacturer of Abilify (aripiprazole). Proteus developed the sensor technology, and when it was Thompson’s turn to speak, he provided the audience with what might be described as the official MyCite origin story, one that everyone could feel good about. He told of a collaborative partnership between the tech company and mental health service users that had led to its creation.
“We began working with mental health patients in 2009. We began with a deeply human-centered design process, where we partnered with patients who were bipolar or had schizophrenia. And then we worked with leading physicians who treat these patients, and we designed everything about our system around first, patient life flow, and then physician workflow. We learned a lot. And what we learned was that patients liked our solutions so much that they didn’t want to go back onto drug therapy after a three-month trial.”
In other words, MyCite is on the market today because psychiatric patients wanted it and industry listened. According to Thompson, these psychiatric patients set up tables at National Alliance on the Mentally Ill conferences, advocating for drug-makers and doctors to put microchips in their pills. This group’s passionate and vocal advocacy then attracted the attention of Otsuka Pharmaceutical, which reached out to Proteus Digital Health in 2012 to pursue a collaboration that would combine the “blockbuster” drug Abilify and Proteus’s sensor technology.
This drug-device combo is known as a Digital Medicine System (DMS). Each pill contains a tiny sensor no larger than a grain of sand, called an ingestible event marker (IEM), composed of trace amounts of minerals found in the human diet: copper, magnesium, and silicon. Upon contact with the gastric fluids, the sensor sends a signal to a wearable patch located on the user’s chest. The patch then conveys the “drug-adherence” data to an app on the patient’s smart phone, which in turn sends the data to a cloud-based server that can be accessed from a provider’s desktop.
The user can also designate up to four additional recipients of such data, including family, friends, or caregivers. However, the user cannot opt out of sharing their data with the medical provider. The data collected by the DMS includes not only whether a pill has been taken (within one minute with up 97% accuracy), but also activity level and physiological markers, such as heart rate and sleep.
https://youtu.be/G0LR_g0Iw48
“For the first time,” said Otsuka’s Nath, “physicians know something about what happens the 99% of the time that the patient is not under their direct control or care.”
In other words, an ever-present surveillance system. “It’s really important to understand that what we’re talking about when we talk about the world of digital is an end of statistics and probability, and the emergence of calculus and certainty,” he said.
What this means is that your doctor—and others—will now be able to know for sure whether you took your Abilify on schedule. And whether you are awake, and up and about. And all this in the first digital pill; one imagines that future Digital Medicine Systems will provide additional information about the activities of the “patient.” A MyCite app on the phone, for instance, could easily send GPS tracking information to the provider. The wearable patch, while ostensibly serving to tell of the digestion of a prescribed drug, could link every movement of that person to the Cloud.
Why Was the First Digital Pill an Antipsychotic?
When the FDA approved Abilify MyCite in November 2017, it became the world’s first FDA-approved “digital medicine.” As such, it was the first in a new “category of drugs” to be reviewed by the FDA, and this was the first new approval category added by the regulatory agency in 35 years. One industry-funded paper observed that it was “challenging to overstate” the clinical significance of this New Drug Application (NDA) approval, “given the rarity of new pharmaceutical categories.”
Even so, the question that had many scratching their heads was this: why would the first digital pill be an antipsychotic? Why not make it for a non-psychiatric illness? Even some leading psychiatrists were skeptical about this choice.
In a New York Times article titled “First Digital Pill Approved to Worries About Biomedical ‘Big Brother,’” Columbia University psychiatrist Paul Appelbaum said: “A system that will monitor their behavior and send signals out of their body and notify their doctor? You would think that, whether in psychiatry or general medicine, drugs for almost any other condition would be a better place to start than a drug for schizophrenia.”
Similarly, Virginia Commonwealth University psychiatrist James Levenson told The Washington Post: “Patients who have a lot of paranoia might be uncomfortable with the idea of a medicine that is transmitting signals. The patient may be afraid to take it.”
Or as late night talk show host Stephen Colbert joked: “Because nothing is more reassuring to a schizophrenic than a corporation inserting sensors into your body and beaming that information to people watching your every move.”
While the choice of an antipsychotic as the first digital pill may seem strange, there is an economic rationale for it. All you need to do is follow the money.
The “Non-Adherence” Market
Proteus acquired the ingestible sensor technology around a decade ago. The immediate purpose of this technology was to increase medication adherence, which was understood to be a pressing medical need and thus a potentially big market.
Studies have found that rates of non-adherence tend to be uniformly high across the gamut of chronic health conditions, ranging anywhere from 30 to 50 percent. As a result, non-adherence to drugs is routinely cited as America’s “$300 billion health care problem.”
The New York Times called it “an out-of-control epidemic in the United States that costs more and affects more people than any disease Americans currently worry about.” Meanwhile, a 2018 study published in the Annals of Pharmacotherapy, examining drug-related morbidity and mortality, estimated that the cost of non-adherence may be as high as $528.4 billion annually, or equivalent to 16% of total US health care spending.
The medical community has been seeking to solve this problem for decades. Reliance on self-reports is generally inadequate, as people tend to overestimate their adherence rates. Pharmacy records don’t reveal whether individuals have actually taken the prescriptions they filled. Blood tests can detect the amount of a drug in someone’s system, but reveal nothing about daily adherence rates.
In institutional settings, such as hospitals and nursing homes, there is “direct observation therapy” (DOT), where staff watch to make sure patients take their pills. Higher-tech attempts at adherence solutions range from mobile phone reminders and alerts, to the Medication Event Monitoring System (MEMS), which consists of bottle caps equipped with electronic devices that can detect if a bottle has been opened. However, this system still can’t tell if a medication has actually been ingested into a human body.
The digital sensor technology offered an advance in “adherence monitoring” compared to all of these other efforts. And while Proteus has been testing it for a broad range of chronic illnesses, from a market perspective, it made sense for the company to focus on “serious mental illness” as its first commercial target.
According to one systematic literature review, people diagnosed with “schizophrenia” have among the highest non-adherence rates, said to hover in the 60-70 percent plus range, due to “insufficient efficacy, intolerable side effects, or for other reasons.” People diagnosed with bipolar disorder are also known to have high non-adherence rates. So the “seriously mentally ill” are seen as a problematic patient population.
In addition, the public has been primed to think that when people with a “serious mental illness” stop taking their antipsychotics, they are likely to relapse and become violent. As a result, there was already public support for legislation and other efforts that would ensure they took their drugs, which could help Otsuka introduce a digital pill to the market.
The medication-adherent product of choice for psychiatry has long been “long-acting injectable antipsychotics” (LAIs), which remain in the body for anywhere from 30 to 90 days. LAIs are said to eliminate the need for providers to conduct detailed adherence assessments at every visit, and reduce the chance of people going off their drugs during transitions from prison or hospital to the community. Families and caregivers also tend to like LAIs: they are seen as reducing or eliminating power struggles and the need for “grilling” around medication-taking or appointment-making.
However, LAIs may be disdained by some health care providers because of the difficulty in achieving accurate dosing, and perceptions of injectables as stigmatizing and coercive. People forced to take LAIs report considerable pain at the injection site, and often object loudly to this form of forced treatment.
Add these factors together, and Proteus could see a rationale for making an antipsychotic the first digital pill it would bring to market. People diagnosed with serious mental disorders regularly stopped taking their antipsychotic medication; the public had come to believe that medication compliance helped protect public safety; and the current method used to improve medication adherence, LAIs, was understood to have its limitations.
Equally important, Otsuka contacted Proteus in 2012 for a pressing reason of its own: its best-selling drug Abilify was set to go off patent in 2014. It needed to create a new patent-protected place in the market for Abilify, and turning it into a “digital” medicine offered the possibility of doing just that.
Pharma’s Market
While speaking to the HLTH audience, Otsuka’s Nath spoke about the “patent cliff” and the threat it poses to the financial wellbeing of pharmaceutical companies.
“So people talk about drug pricing and they define drug pricing as the problem. Let me posit to you that it is not the problem. The Pharma business model, and especially the innovation model in the industry, is the problem. If it costs $5 billion to create a drug and then you have 10 years to make a return, then by definition the price of that drug is going to be high. Pharmaceuticals are a very risky business. R and D costs billions. It’s very hard to predict success. When you get a product approved, it can be very hard to get it paid for. Pricing must be high in this model, and by the way, your competitors in the bulk chemical industry are all waiting for a date certain when you lose your patent, and they can take over your business. It’s a very bad business model.”
While he did not mention Abilify by name, Nath surely had it in mind. From April 2013 to March 2014, Abilify had been the top-selling drug in the United States, with sales of $6.9 billion. Abilify accounted for nearly half of Otsuka’s revenues at that time.
In April 2015, the FDA approved the first generic aripiprazole. Abilify sales were about to fall off the cliff, and Otsuka was desperate to keep up the revenue stream from this drug. Adding a sensor to Abilify provided Otsuka with a way to fairly quickly bring a new patent-protected product to market.
As Thompson explained at the HLTH conference, the FDA has developed a “streamlined” approval process for products that are a “combination of a drug and a device.”
“To gain an approval for a digital medicine, there is a separate NDA process, a new NDA pathway through CDER. So you take an approved drug, you add the approved ingestible sensor, you test for stability, bio-equivalence and human factors. This takes about 20 to 30 months and it costs about $50 million. That may sound like a lot, but in case anyone isn’t aware of this, a regular pharmaceutical takes about 10 years and costs about $5 billion.
So you get a new NDA and new NDC code and new naming convention and you can create a new business with a much better product, with a very streamlined FDA pathway.”
Since Otsuka had already received FDA approval for Abilify in 2002, it was not required to test MyCite for therapeutic efficacy, or for drug-related side effects. And since Proteus had obtained FDA approval for its ingestible sensor in 2010, there wasn’t much additional safety testing of the digital monitoring system that was needed. All Otsuka and Proteus needed to show with their clinical trials was that patients could be instructed how to use it, that the patch wouldn’t have adverse safety effects, and that the digital sensor functioned as designed, which is to say that it sent a signal to the patch worn by the user that the drug had been consumed. Otsuka and Proteus did not even need to show that their product led to increased medication adherence.
As the FDA reviewers of MyCite trial data wrote, “The FDA’s conclusion is simply that the pill, patch, and app function as intended, and that most patients with schizophrenia, bipolar I disorder, and depressive disorder could successfully use the product.”
Otsuka priced its “digital pill” at $1650 a month, compared to $20 per month for generic oral aripiprazole. This cost, of course, will be mostly borne by the taxpayer, as the “seriously mentally ill” who are forced to take medications are usually covered by Medicaid. As Akin Gump, Otsuka America’s lobbying firm, wrote about their five-year collaboration: “As with all revolutionary medical products, success hinges on reimbursement by the Centers for Medicare and Medicaid Services.”
Doing Harm
While researchers have pointed out the flimsy nature of the clinical trials that Otsuka and Proteus conducted to obtain FDA approval for MyCite, there has been little discussion in the general media about the ethics of promoting a digital pill to improve adherence to a medication that can cause a long list of adverse effects, and belongs to a class of drugs that impair a person’s cognition, deaden emotions, and reduce the possibility of long-term recovery. They may also cause early death.
Even over the short-term, Abilify and other “atypical antipsychotics” are known to cause metabolic dysfunction, parkinsonian symptoms, and brain shrinkage. Antipsychotics over longer periods of time may cause tardive dyskinesia, which is evidence of permanent damage to the basal ganglia. Studies in elderly populations show that they markedly increase the risk of death, and in a 2018 meta-analysis, UK researchers concluded that this heightened risk of death is apparent in general mental health studies too. They concluded: “Antipsychotic drugs precipitate excessive mortality across the spectrum. Prescribing of antipsychotic drugs for dementia or for other mental health care should be avoided and alternative means sought for handling behavioral disorders of such patients.”
There is now abundant evidence that regular antipsychotic use worsens long-term functional outcomes in persons diagnosed with psychotic disorders. Indeed, clinical practice guidelines in “first-episode psychosis” programs now stress the importance of judicious medication use and working collaboratively with service users and their social networks. The Open Dialogue approach pioneered in Finland incorporated those principles, and a 2015 paper exploring its success concluded that the single most important variable in a positive prognosis for “typical schizophrenia” was “a rare or low-dose use of antipsychotics.”
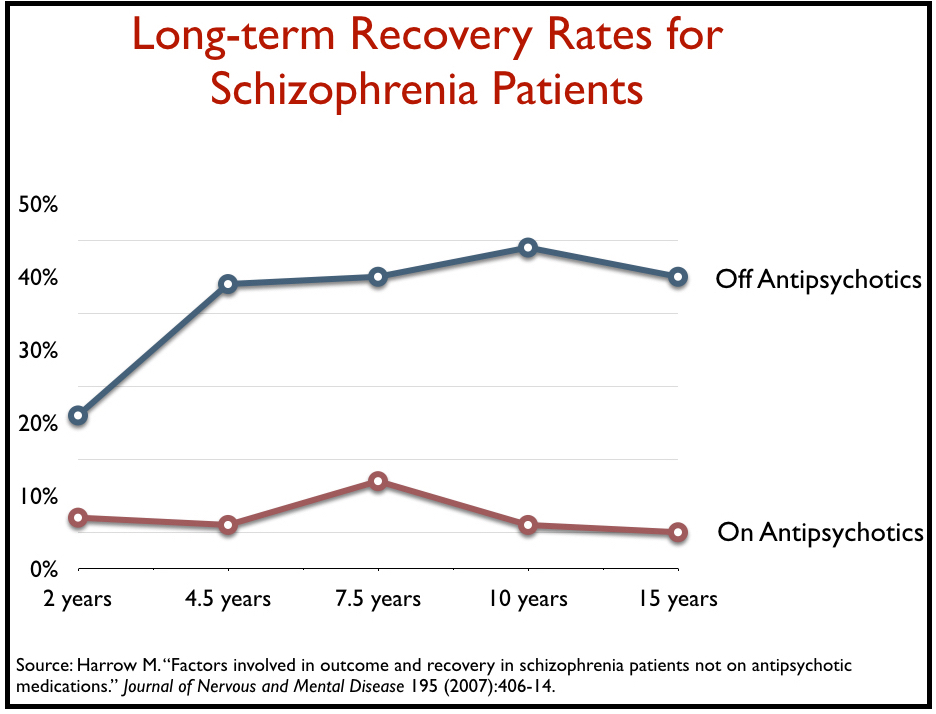
In a long-term study of schizophrenia patients in the United States, Martin Harrow found that the recovery rate was eight times higher for those off antipsychotic medication than for those who were medication compliant.
All of this is glossed over, or missing altogether, in public discussions about the “benefit” of laws and policies designed to make sure that the “seriously mentally ill” take their drugs. Also missing in this discussion is recognition of the fact that these drugs may induce akathisia, an extremely agitated state of mind and body, which is a risk factor for both suicide and interpersonal violence.
MIA’s recent report on “The Case Against Assisted Outpatient Treatment” details this risk that comes with use of antipsychotics:
“Patients suffering from akathisia described ‘violent urges to assault anyone near,’ and wanting to kill ‘the motherfuckers’ tormenting them in this way. A 1990 study determined that 50% of all fights on a psychiatric ward could be tied to akathisia. Yet another study concluded that moderate to high doses of haloperidol made half of the patients markedly more aggressive.”
And that was indeed the case for my mother.
My Mother on Antipsychotics
My mother’s psychiatric record reads like a hellscape of violence, desperation, and despair. She was detained over and over by the police for things such as “bizarre and dangerous behavior,” “throwing herself in front of passing cars,” “laying down in the street,” “street-walking,” “smashing glass,” and “allegedly assaulting a neighbor.” Yet, she had no history of violence before being put on psychiatric drugs.
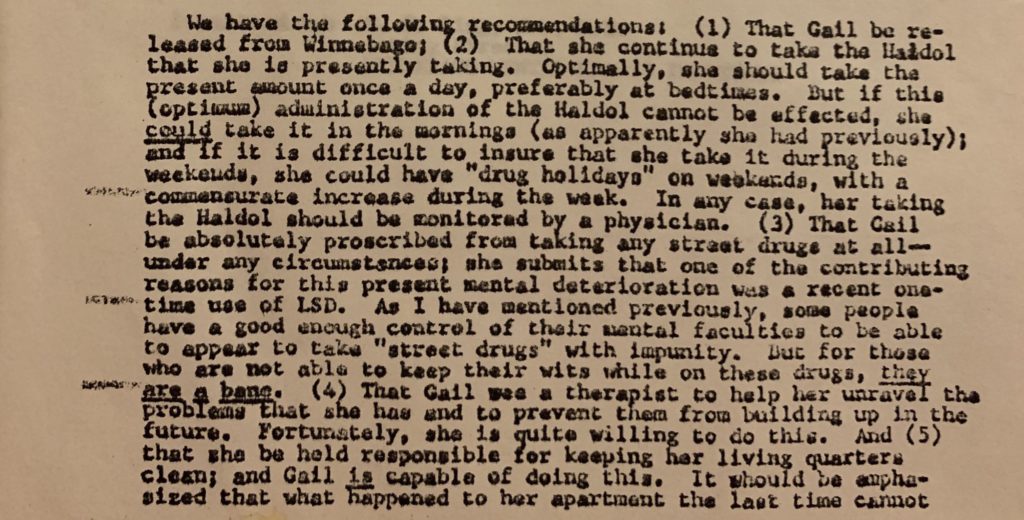
In 1986, my mother was enrolled in Wisconsin’s Medicaid-funded Community Support Program (CSP), as she met criteria with a diagnosis of “serious mental illness” and a high risk of re-hospitalization, given her past history. I have, in my possession, a gigantic accordion file with pages upon pages of yellowing case notes that attest to the weekly visits and careful observations, adherence assessments, and documentation of my mother’s lifestyle choices, behaviors, and habits. The words “compliant” or “noncompliant” are found on nearly every single page.
Eventually, the CSP began to “work” as intended. In the final two years of her life, my mother remained compliant with oral medications and was not re-hospitalized. By all “outcome metrics,” this was a win for her, as she hated being shipped off to the Milwaukee County Mental Health Complex. And it was a win for the family, who very much disliked dealing with her when she was “off her meds.” And it was a win for Wisconsin’s public mental system, which was saving thousands of dollars that would have been spent on her repeated institutionalizations.
However, this tallying up of the “benefits” didn’t account for the health consequences that came along with such medication adherence. The drugs my mother was forced to take over the years likely contributed to her developing diabetes mellitus, which became another chronic condition that she was then expected to manage. Other medical issues she faced due to the drugs included restlessness and akathisia.
Cigarette smoking eased the worst of the drugs’ agitating adverse effects, and thus helped her cope with the akathisia. But the decades of smoking eventually led to her developing COPD. No one could compel my “unmotivated” mother to comply with a diabetic diet and to exercise, or to quit smoking. I suspect that making so-called “poor lifestyle choices” was the only avenue of resistance left to her.
As documented in my mother’s chart, on the night that she died in April 1996, she waved off a friend who wanted to call her an ambulance for her COPD-related breathing difficulties, saying she “just had a cold” and she’d be fine in the morning. The friend acquiesced to her wishes. Her final act was to refuse to go to the hospital for intubation, a simple medical procedure to open her airway, a procedure that would have saved her life, at least, for that night. While I miss her every day of my life, I believe that she was exercising what little choice she had left in a life dominated by nearly three decades of medical and psychiatric surveillance and control.
In the last case note appearing in my mother’s chart following her death, the RN spends several lines documenting her “compliance” with her meds, and her “noncompliance” with a diabetic diet or recommendations for the treatment of COPD.
The final line reads: Death appears to be of natural causes at this time, followed by a list of medications she was taking when she died. She was 46.

Rolling Out the Digital Pill
Although the FDA approved Abilify MyCite in November of 2017, Otsuka could not expect to immediately begin selling it. There was no existing market for this new category of drugs, and thus Otsuka has had to create one. In August of 2018, it entered into a collaboration with Magellan Health, with the “aim of providing real-world evidence to demonstrate the value of this drug-device combination product over time.”
Magellan Health is a Fortune 500 company. It is a large manager of behavioral health services, and it will first test this new product on Medicaid patients in the South. In their announcement of the collaboration, Otsuka and Magellan presented this roll-out as one that would bring “innovative technologies” to patients that rarely have access to them, with privacy protections in place too. “Patients can opt in if they want to try it, and Magellan will not have access to patients’ individual-level data on whether and at what time they ingested their pills,” STAT News reported.
In this preliminary test phase, it will be Otsuka that collects and analyzes all the data sent by the sensor. The data-collection process is in fact being presented and “branded” as an Otsuka product. The press release described how it will be done:
“The ABILIFY MYCITE System provides an opportunity for a connected care approach to treatment, and tracks if ABILIFY MYCITE (aripiprazole tablet with sensor) has been taken. The system is comprised of: the ABILIFY MYCITE tablet (an aripiprazole tablet embedded with an Ingestible Event Marker (IEM) sensor); the MYCITE® Patch (a wearable sensor); the MYCITE® APP (a smartphone application) and the MYCITE®Dashboard (a web-based portal for healthcare providers and caregivers).”
The press release makes it seem that the sensor will simply track whether the drug “has been taken.” For an individual, that is a data point of minuscule size. However, when Otsuka trumpets this technology as an advance in medical care, it tells a very different story. Then its device suddenly becomes one that can track a large number of real-time processes, which in turn generates huge amounts of data about each individual wearing the patch. As Dr. William Carson, President & CEO of Otsuka’s Pharmaceutical Development and Commercialization division, told Startup Health TV:
“The amount of data that Otsuka collected [in the MyCite trials] was more than all of the data that we’ve ever had in all of our clinical trials. And that really stands out, as it really makes you think. In the world that we’re in now, we have a wealth of data which will help us to understand patients better and help us to make sure that they are able to manage their medications.”
In addition to the Magellan collaboration, Otsuka is funding a trial of Abilify MyCite that will focus on recruiting military veterans living in the South. The study is called DIgital MEdicine Study (DIMES) for Adults With Schizophrenia, Bipolar I Disorder, or Major Depression Currently Using Aripiprazole, and is designed to measure differences in adherence rates between those who take Abilify as usual, and those who utilize the digital version. Recruitment is currently underway via the Durham VA Medical Center in North Carolina, and is planned for the Michael E. DeBakey VA Medical Center in Houston, Texas.
There is at least one other testing program in the works. In June of this year, Otsuka announced a collaboration with Thriving Mind South Florida (contracting as the South Florida Behavioral Health Network), a nonprofit organization supported by Florida’s Department of Children and Families. That same month, Thriving Mind broke ground on a 280-bed jail diversion facility in Miami, funded by a blend of public behavioral health and criminal justice dollars. The collaboration and the eventual facility could provide Otsuka with an opportunity to demonstrate Abilify MyCite’s use in a captive population.
The Digital Asylum Beckons
The eerie possibilities that await can best be seen in the above statement by Otsuka’s William Carson: the company collected more data in the MyCite studies than it “ever had in all of their clinical trials.”
Just how will that data be used in the future? And if the collection of enormous amounts of data is already possible with this first edition of a digital pill, what can we expect from subsequent generations of digital medicines?
“The use of smart pill technologies is described as an intervention to achieve medication adherence,” wrote Eric Swirsky and Andrew Boyd in a 2018 paper published in the American Journal of Bioethics. “However, this application of the digital pharmacopeia is more accurately described as surveilled compliance.”
And hence, the creation of the digital asylum. The American public has already embraced state laws that require the “seriously mentally ill” to take their medications; use of a digital pill would help monitor their compliance.
As early as 2012, when the idea of a digital pill first began taking hold in the public mind, Patricia Deegan, PhD, whose professional work has focused on giving people voice and choice in their use of medications, raised an alarm about the potential coercive applications of digital pills:
“What should informed consent be like in the event that we are offered a ‘Police Pill’ or, phrased more benignly, an ‘Assisted Treatment Pill’? Who should control access to the personal information that is generated by such pills? What action should be taken based on the information that is collected by such pills? Should your employer be warned that you have not slept in 2 days? Should a psychiatrist or case manager come to our home if we have not swallowed prescribed medicine in a timely fashion? Should family members receive a notice if the microchip says that we have not been sleeping enough? Should our doctor or nurse adjust dosages of medication based on biometric information received from these ‘smart pills’?”
Moreover, it is easy to foresee the possibility that authorities will require people receiving government disability payments because of a psychiatric disorder to use the pill.
In a 2018 paper published in the American Journal of Bioethics, Dominic Sisti and Mélanie Terrasse noted that participation in “monitored medication adherence” programs could be dangled as an eligibility requirement for programs to access housing or other needed resources. This technology, they noted, could also be used for “big data policing”:
“It is also likely that mentally ill persons involved in the criminal justice system will be pushed to use treatment monitoring devices, and, therefore, disproportionately bear any unforeseen adverse consequences of these new technologies. This population is significantly more likely to be surveilled through methods such as neighborhood over-policing or ‘big data policing.’ Data from these devices may be repurposed for forensic aims, to evaluate individuals’ suitability and eligibility for particular rehabilitation or reentry programs, or to attempt to predict dangerousness.”
Trump, of course, spoke about how society needed to take “mentally deranged and dangerous people off the streets,” which was understood to be a call to return to rebuilding the asylums of old. But even at a cost of $1650 per month, digital Abilify may ultimately come to be seen as a more cost-effective way to control the lives of those deemed “mentally ill.” And it is because it can offer this control, that it will be seen as a superior alternative to long-acting injectables (LAIs).
Use of LAIs is an efficient and relatively low-cost method for assuring “medication adherence.” If that were the only purpose of Abilify MyCite, then it is difficult to see how it could become a commercial success. However, the fact that a prescription of Abilify MyCite requires the “patient” to wear a patch sending reams of data to the Cloud is what separates it from LAIs. The wearable patch is already able to provide huge amounts of real-time personal data, and it could easily be used to provide minute-by-minute monitoring of a person’s location. The digital pill offers systems and society the opportunity for 24-hour surveillance and control, and the possibility for corporations to profit from it.
And Then They Will Come for Everyone
For Proteus and Otsuka, Abilify MyCite is simply the first of the many digital pills they plan to bring to market. In an agreement signed in October 2018, Otsuka promised to pay Proteus $88 million in “related equity and other payments” for the “development and commercialization of digital medicines over the next five years.”
Proteus already has 31 digital medicines in its pipeline, including cancer medications and opioids, and is looking to expand into pre-exposure prophylaxis (PrEP) medications designed to prevent HIV transmission. In a 2018 address to the Royal College of Physicians in the UK, Proteus CEO laid out his vision for a futuristic world of digital health:
“Digital companies have been able to use phenotyping to create exquisitely tailored products and services. Amazon phenotypes how you shop and delivers precision commerce. The same will happen with medicines. Your care team will know how you take them, how your body responds and will deliver precision Digital Medicines.
On the device side we will move from fun toys to FDA-certified consumer friendly, medical grade wearables that deliver accurate, actionable health data.
Digital apps will be much more sophisticated and make use of sensors and analytics integrated into the consumer’s own mobile devices. These apps will store data and forward actionable insights to care teams based on AI, and provide engagement tools that support patients and their families.”
If Thompson is right—and Otsuka just bet $88 million that he is—then the digital medicine panopticon may be coming for us all.
If you have been part of an Abilify MyCite clinical trial or have otherwise used this digital medicine system, Mad in America would like to hear about your experience. Please contact the author or submit your story here.
****
MIA Reports are supported, in part, by a grant from the Open Society Foundations



Just imagine, fraudulent medical treatment has become an acceptable way to take away peoples’ citizenship rights, and here we are reading about a trendy techie method by which it can do so. Big pHarma R and D is going after their next big jackpot, and so what do the rights of plebes mean to them anyway? Gulp. Watch out for the future. If it’s still there anyway. Between pervasive surveillance and the monitoring of flagged deemed sub-humans, and massive global warming, what kind of a future do we have left?
Report comment
Nothing like seeing the world through those rose colored glasses, Frank. (; Although I will concede, humanity has definitely been going in the wrong direction for way too long, sadly. And this “progress” is not a sign of the needed U-turn.
So sorry for the harm they did to your mother, Leah, and of course, the subsequent harm they did to you and your whole family.
“1984 Came Early for ‘Mental Patients’” … “And Then They Will Come for Everyone.” It’s a shame the psychiatrists repeat the worst of human history, over and over and over again. They never learn.
Report comment
I don’t know what happened to my rose colored glasses. Must have misplaced them somewhere.
I would caution though that “progress” is often subjective, and that there were times in the distant past that were much more “progressive” than anything anybody has going today. Should this “progress” actually be “regress”, then I beg to disagree, it is time for a U-turn.
Report comment
It seems prudent to mention the newest proposed government agency – HARPA, meant to digitally surveil those deemed to be potentially dangerous for early warning signs and “intervention”.
https://www.rawstory.com/2019/08/trump-mulling-uniquely-dystopian-proposal-to-use-ai-to-identify-mental-health-issues-as-risk-factors-for-gun-violence/
Report comment
Yes, thanks much for mentioning. HARPA is something I have my eye on for sure.
Report comment
I have only just begun reading the article and noticed this mistake:
“In the wake of back-to-back mass shootings in El Paso and Texas last month,”
I’m sure you meant to write: “in El Paso, Texas and Dayton, Ohio”
Okay, reading on now…
Report comment
Ha! Thanks for the catch.
Report comment
No problem.
Great article. Scary fucking world.
Report comment
Australia provided financial aid to one of the poorest nations on the planet, East Timor, to help build up their government once they achieved independence. They bugged their offices and used this spying to gain an advantage over them in negotiations surrounding the oil and gas in their territory. Someone thought this was a bit low and let it be known. They are now being prosecuted along with their lawyer because of their treasonous conduct.
Trust my government with information obtained from spying? How low does it get basically stealing off the poorest Nation on the planet?
A Land of Corporate Gains
Report comment
I think all mass shootings are connected to mental illness. All mass murder. In fact all hate and killing arises from mental illness.
It’s just that polite society is not willing to denote hate as illness. Whereas personally I believe hate to be a very intensely ill state of mind.
I also believe that all extremist thinking is a form of mental illness. Including fascistic thinking. Or its preferred new term, alt right. The alt right movement is replete with mentally ill thinking.
I also consider neoliberalism as mentally ill.
For me, the DSM is just as problematic for what it discludes, as what it includes.
Report comment
It sounds like you are defining “mental illness” as any condition that results in people behaving in dangerous or destructive ways. Do you really see these behaviors as “illnesses” in the medical sense? Do you believe that something is physiologically wrong with someone who does these things, and that this explains fully why they do so? Or are you simply stating that these people may meet the “criteria for mental illness” as defined by the DSM, which we all know is something decided on in committees and voted on by the APA, rather than detected by any legitimate test of “health” or “illness?”
If it is the latter, then claims that all shooters are “mentally ill” is pretty meaningless, as it seems to be defined simply as behavior that a society disapproves of.
Report comment
The legal definition is basically useless. A disturbance of thought, mood …… etc. This includes such acts as sneezing which disturbs your ability to think. A moment of insanity for which you can now meet the criteria. There are of course the ‘exclusions’ such as sexual preference, political or religious beliefs or being affected by drugs but these are easily overcome by ‘verballing’. For example a belief in God becomes a paranoid delusion because you think you are being watched. This ‘verballing’ is used all the time here in Australia to remove the protections afforded by the law. So basically it comes down to being whatever the doctor you sit in front of wants it to be..
The recent removal from the Act of the exclusion of drugs was done to shift the drug addiction problem from police to Mental Health. Aren’t all the druggies in for a surprise when they find themselves under the ‘care’ of these vicious bastards who can assault them using drugs. They will be wishing for the good old days of police beatings in no time. And with the addition of a Euthanasia Act our streets should be cleaned up in no time.
There is and never will be a definition of Mental Illness that works, it a rubber ruler that is used to beat up oin sections of society the way the National Socialists did with mental defectives and Jews during the war.
Personally I think a mental illness is anyone who doesn’t think like me. Which is basically what was said by the committee that wrote the DSM.
And lets say we get this Euthanasia Bill through and we have doctors who are snuffing out 30 patients a day, Would they be considered mentally ill, or would these compassionate killings be excluded? Not done out of hate but more to make a few bucks to feed the family.
Report comment
Of course, I agree with you completely.
Report comment
Well, FWIW: we do have real-life examples for how these things are handled.
Regarding “the insanity defense,” for good or ill, it’s rarely used, and very rarely successful; unlike on TV. I wrote a little about it here:
https://www.quora.com/When-a-clearly-mentally-ill-person-i-e-Down-syndrome-commits-a-crime-do-they-go-to-jail
Regarding euthanasia and mental illness, I find it impossible to believe we will be seeing a combination of these two inside of a century. Today, voluntary euthanasia (for medical illness) is available only in Belgium, Canada, Colombia, Luxembourg, The Netherlands, Switzerland, and in six US States.
Voluntary euthanasia for mental illness is available only one place in the whole world: the Netherlands. It requires leaping through multiple hoops. And it is relatively rare. (A report last winter that a teen girl had “been euthanized” for depression by doctors was false. In fact, the girl had been denied, and she startved herself at home.)
https://www.google.com/amp/s/amp.theguardian.com/world/2019/jun/05/noa-pothoven-netherlands-girl-not-legally-euthanised-died-at-home
Report comment
Steve McCrea wrote: “It sounds like you are defining “mental illness” as any condition that results in people behaving in dangerous or destructive ways. Do you really see these behaviors as “illnesses” in the medical sense?”
When I use the term mental illness I do so in the awareness that it is a metaphor. That metaphor in general use encompasses all the unknown diseases, syndromes, damages and congenital malformations to and of the human brain.
Unlike others I don’t have an ongoing neurosis about the term mental illness. I see it as a metaphorical holding pen for all that is currently unknown or tentatively understood about the human brain going wrong in some way or other.
I think the sensible — although very frightening and unnerving and difficult — probability is that something is physiologically wrong (or to coin the technical term, cock-a-hoop) with someone that goes on a spree killing, yes. There are numerous known physiological causes that can give rise to such wanton violence. We don’t know them all. We may never know them all. And it’s not a routine matter to dissect and closely examine the brains of these murderous lunatics. It should be a routine matter, but it isn’t. On here that physiological cause is often attributed to antidepressants. That’s overstated, but nonetheless a perhaps plausible very minor addition to the very long list of already known possible physiological factors.
Everything we do think feel say decide and so on has a physiological factor.
I do not much like the majority of human beings, if I get to know them. So the trick is to not get to know them, in order that I can go on liking them, and interacting with them. Deep down, most people operate under that mischief. It takes a narcissism of tremendous achievement to get to the point of holding a gun and deciding on a slaughter of the innocents. To seek out that kind of narcissistic resolution to one’s natural and largely repressed misanthropy takes a tremendously cock-a-hooped brain and central nervous system and gastrointestinal system. To witness such an event is to witness a human machine gone awry. It’s a breakdown event. A malfunction event.
To see it any other way, to me, lacks a sense of proportion or basic humanity. People behave like this because something has gone seriously wrong with their bodies, and thus their being. They are, again to coin the technical term, tapped in the head. In that “tapped” process they will often seek out justifying grand narratives, something big and extreme and loathsome and dangerous. Yet often, too, they won’t, and be self-justified by nothing more than I-don’t-like-Mondays.
Brains go wrong. The brain is the most complex known organ. It goes wrong in so many ways and in doing so can give rise to breathtaking horrors.
A sphincter is a much less complex bodily mechanism. It also goes wrong, and it also can give rise to breathtaking horrors.
Why do people here so easily accept that the sphincter goes wrong but struggle so much with the notion of a malfunctioning brain?
Report comment
I don’t think anyone here doesn’t believe that a brain can malfunction. I don’t agree that a brain malfunction is the only thing that can be behind someone being violent or depressed or whatever. It sounds like you believe the brain creates the mind and therefore HAS to be responsible for any actions that occur. I don’t see it that way – I see the mind as being the mechanism for controlling the brain, at the minimum an “emergent property” that extends beyond the mechanism that created it. I also hold the strong possibility that we are spiritual entities that are responsible for our bodies, though it is difficult to prove or disprove this kind of premise. In any case, it is pretty clear from direct observation that the mind can and does control most aspects of the brain. Even the revered PET scans show that when someone simply THINKS something different, the PET scan changes. For instance, someone can think of a sad event and their brain shifts gears into a “sad” profile, and shifts back when they think of something that isn’t sad. This belies the idea that feelings “just happen” because our brains are bad.
Even if we accept the premise that it’s all in the physical universe, there is still the “computer model” to consider. While I don’t believe that the human brain is much like a computer really, it is fair to suggest that we have “hardware” and “software” operating, in the sense that there are physiological structures that are used while thinking and making decisions and emoting, but there are also “programs” in the sense that we make MEANING out of things and we make decisions based on values that are programmed in starting early in life.
Using this metaphor/analogy, what if the problem is not in the hardware, but in the programming? You can’t solve a programming problem by replacing memory chips or rerouting the power supply. The program is contained within the chips, and really consists only of on/off switches. It is only because the programmer assigns MEANING to the switches that the computer works at all. It seems to me that what is wrong with the “mind” most of the time is faulty programming, or perhaps more accurately programming that doesn’t create the desired result from a social perspective. Of course, then we get into the question of who gets to decide what the “desired result” is, which is a whole different question. However, it is likely that those who are violent have, in most cases, grown up with and/or developed value systems in which murdering people is not wrong or is justifiable under certain circumstances. This is something that can not ever be improved by physiological intervention.
So the catch-all of “mental illness” does not necessarily imply any kind of problem in physiology, even if you take a strict materialist point of view, any more than a computer malfunction has to be a function of the hardware. The vast majority of computer problems are programming issues, and the same analogy almost certainly holds true for “mental illnesses” as identified by the committee-driven DSM.
Report comment
Of course, there is also the problem of who the “programmer” or operator of the mind actually is…
Report comment
“It seems to me that what is wrong with the “mind” most of the time is faulty programming, or perhaps more accurately programming that doesn’t create the desired result from a social perspective. Of course, then we get into the question of who gets to decide what the “desired result” is, which is a whole different question.”
I believe the “desired result” can only be defined by the individual who is seeking results, it’s really not for anyone else to say. It’s actually no one else’s business, unless a person knows how to be supportive rather than competetive, invalidating, judgmental, etc.
If one goes by “social perspective,” then one is buying into the social programming. The “faulty programming” is how we were raised/programmed. This is what people are correcting now, one by one.
Report comment
I could not agree more with your sentiments here.
Report comment
That’s my position as well. Social control should be named what it is. It’s not “treatment” of “mental health issues.” It’s an attempt to control “deviant” or “undesirable” behavior from the point of view of the status quo. Naturally, it’s a very slippery slope when we start reframing “He’s doing something that annoys his neighbors and should be stopped” as “He’s got a ‘mental disease’ MAKING him do something annoying and heneeds to be ‘treated.'” Again, what is “deviant” is defined socially, not medically, and it’s a pretty big scam to pretend otherwise.
Report comment
Steve’s ideas about what is going on with people that we call the “mental” part of life are the closest to what I have learned. The only reason it seems “difficult to prove” is that most people are unaware of the work being done in this area. There is a cultural bias favoring the brain model that has been very difficult to change. Perhaps the most visible “alternative” work that I am aware of concerns past lives, which is basically a for-sure phenomenon at this point. This work alone destroys the brain model. There are even real psychiatrists working in this area. Yet it remains “fringe.”
Elements of the psychiatric community are gradually pulling away from drugs and ECT as they are increasingly exposed as coercive, damaging, and unsuccessful. But as a group, they are not pulling away from the brain model. And we won’t get it right until we do. The “health” of the mind does not depend on treating the brain in any way. It is that simple. The mind is a whole new world, and these doctors and the people supporting them don’t want to go there. Programming? Yes, that’s an important element of the new model. Should the old model become totally untenable, programming is probably what the advocates for a new model will focus on. But that’s a machine viewpoint of life. It does not fit the human condition, either.
Report comment
Hence, the question of who the mysterious “programmer” of the mind actually is!
Report comment
I believe ultimately, we’re looking at DE-programming from all the false information and responses to all the illusions which have been projected at large, for the purpose of control. The result has been separation from who we REALLY are, each of us, our natural tendencies based on how something makes us feel. I think that can be a bit crazy-making.
Our emotions are essential to how we make choices, they guide us toward or away from things. We’ve been programmed to invalidate or ignore our emotions, and go toward “approval.” Well-being, balance, and self-agency come from paying attention to how we really feel from moment to moment. I believe that is our “natural programming” (our personal nature), and we’re each unique in this regard.
From our brainwashing society, there’s a lot from which to deprogram, and that is a process which takes time and requires being awake and paying attention to how one feels, rather than what anyone else thinks. Best case scenario is heart-mind synchronicity, then there is no question about the truth of the matter.
Report comment
Deprogramming sounds right to me!
Report comment
There are already laws against “disorderly conduct.”
Report comment
Great, Steve, I’m glad to hear that because when we deprogram for the lies and illusions we’ve absorbed and discover the truth of our hearts underneath all that bs, that is the ultimate healing and is what creates core change.
Going from brain-consciousness to heart-consciousness shifts perspective and, therefore, reality. It will become a heart-based reality. That is emotional and creative freedom. No more programs, just living our truth. No need for psychiatry (or any such thing) at that point because we become our own guides and healers.
A community of heart-based humans, where individuals are aligned with their personal truth, would be the most powerful. And there are such communities in the world, at this point. They are up and coming as more and more people wake up and make that core shift within themselves.
Report comment
Alex, I’m following along and just wanted to say I love your idea of de-programming and embracing heart-consciousness! This is clearly the path I am on but you put it to the language I needed to express this concept. Thank you!
Report comment
“There are already laws against ‘disorderly conduct.'”
That’s why I say heart-mind alignment is optimal. Emotional intelligence is a real thing. I call it being “heart smart.” I think it’s part of our human evolution, we learn as we grow. We can be true to ourselves AND stay safe in that scenario.
I also believe it’s what we’re most missing in our society, which is why things have degenerated so much. When I look at our leaders right now, emotional intelligence is one thing that is not standing out, quite the contrary. More like a bunch of regressed adults acting like angry children looking to express their so-called “power” in any way, shape or form–never mind integrity, fairness, and justice. Apparently, these are just too complicated to apply!
That’s not true and real power, from where I sit, but more a product of lying and fear-mongering, so it depends on people actually buying the lies and fearing illusions. We don’t have to, if we’re heart smart. And if we don’t, we empower ourselves while disempowering the elites, because we’re not only not buying it any longer, we’re also not living in fear. That’s a program which only serves the elite, at everyone else’s expense.
Report comment
Well said Alex.
Report comment
KS, thank you for saying this. It is the path I took for myself, too, and it was amazingly healing and enlightening, changed everything. And then my partner followed suit, so two of us focused this way is super-powerful. We’re manifesting very well together these days, in synch. The more the merrier!
This has been very challenging to put into words. Been working on that, and this dialogue unfolded well so that I had another opportunity to put this into context. I’m very happy to hear it is coming across with clarity and that it resonates 🙂
Report comment
“De-programming” as a name for the desired activity has been compromised by people who kidnapped and tortured people who had joined various religious movements, calling it “deprogramming.”
The data on how mental programming was actually accomplished is too incredible for most people to believe. But the closest activity we have like that on Earth is psychiatry, particularly when they use hypnosis. This is a Manchurian Candidate sort of scenario. Of course, hypnosis does not have to be used for evil purposes, but it can be.
Report comment
Deprogramming from a cult, deprogramming from bad parenting, deprogramming from false beliefs, deprogramming from self-sabotaging thoughts, deprogramming from group think, deprogramming from toxic psychotherapy, deprogramming from abuse (esp gaslighting abuse)…it’s all a choice, and it doesn’t have to be done by someone to another. We can deprogram ourselves from one set of beliefs (neural pathways/habits) if these beliefs no longer serve us, only taking us in circles making us feel stuck, and we want to shift our experience toward that which is more natural to us, where we are learning, growing, expanding in our thinking and awareness. We discover what this is as we go along, how our process takes us through this. We’re each unique in this regard, we each do it our way.
It’s really just a matter of noting what our thoughts are, how these thoughts feel to us, deciding whether we want to continue with the beliefs we’ve long held, or are we seeing from another perspective now?
That’s how change happens, and it’s more natural than not. What is not natural, what is most effort, and what keeps us out of balance and moving further away from our center, is RESISTING CHANGE. That’s going against nature, which is ever-changing. When we allow change to occur, we are deprogramming from old beliefs and allowing new thoughts, vision, and inspiration to come to light. That is simply the nature of evolution. And we need newness now, not more of the same.
Best I can do at this point. Trusting our intution and allowing ourselves mistakes in the process are vital because this is how we learn to trust ourselves, especially after we’ve been let down and betrayed repeatedly. We’re human, not machines. Life is what we make it to be. Language can be limiting, but the soul knows the truth. Get in touch with your soul, and you will, too!
Report comment
I have never seen someone successfully “deprogram” themselves. There is a technology that accomplishes it, but it requires a group effort. Any idea that we can get through this without sound organizations with strong memberships is misguided, I believe. THEY are organized. We have to do better than that.
Report comment
There are TONS of people who have successfully self-healed and deprogrammed themselves or who are well in the process of it, all over the world! And many of them ARE organized and/or are getting organized, with a strong intention and focus on creating and allowing change to happen, which is happening, little by little, as more and more people heal by leaps and bounds and own their power. That is the new reality. It starts from within to be real and true core change, no two ways about that.
Begins with healing our hearts, that is transformative. I believe the energy from our hearts (which is our spirit) has more influence on the mind than the brain does. That’s my intuitive hit, not scientific. But it fits my reality.
These folks are called Lightworkers, and they are healers, teachers, artists, and manifestors who have experienced core transformation (aka “deprogramming”), and who, in return are supporting people who are waking up to all kinds of truths beyond the family and social programs, to pay it forward. That would be the natural ripple effect of energy. No technology needed, just our intention, focus, awareness, and bodies.
I know many lightworkers who’d been entangled with the system and psych drugs, even hospitalization, etc., and who got off the drugs, stopped therapy–basically rejecting and eschwing all of that–and did it this way, by depgrogramming–exactly this–along with detoxing and realinging in a new way, new grounding and perspective, and who are now teaching and supporting others in their process of healing and awakening in order to shift their reality into something more amenable to who they really are, based on their heart’s desires. I’m one of them, and I’m almost 60. Most former mh clients-turned-lightworkers whom I know are younger, in their 20s and 30s. They are very smart and caught on sooner, God bless them! I follow many of their teachings, they all overlap, not in conflict with each other. After the mh industry, that is entirely refreshing!
This is a layered process and it is rather unpredictable and it requires focused attention. Out with the old, in with the new. That’s exactly what change is, and all we have to do is allow it at this point because it is well in motion. Even the Earth is shifting, no way human conciousness can avoid shifting now. We’re in an age of expansion.
You can easily research this on YouTube, search “lightworker” or “lightworker healing” or “planetary ascension” or even “healing from narcissistic abuse”–that’s a powerful deprogramming and probably the most relevant and eye-opening right now, and there are people who’ve accomplished this and who are helping others do the same, guiding them through this complicated and very rich healing. It’s not always easy, but its doable and seriously stress-relieving, to a new level.
Deprogramming is the most common form of healing these days, and it also causes awakening, that is its natural progression. Neuroplasticity is key, we can change our entire inner landscape this way. It’s powerful stuff! And the path toward freedom.
Report comment
I did a search and found this video posted last year called “Lightworkers and the Ascension Process” in which teacher Michael Mirdad explains from his perspective what I’m talking about here.
https://www.youtube.com/watch?v=tn5lDimiqig
This is more common than not now, this is how this is being channeled and taught these days, totally from a person’s lived experience and the truth they gleaned from their deprogramming/healing/awakening, along with multi-cultrual ancient widsom, and its becoming more and more widespread, as a result. These are integrated teachings applied to our times for the expressed purpose of creating core change in the world.
Not all will accept this information or will be able to hear this, as unfortunately, part of programming from an oppressive system/society is intended for people to resist light, so that they stay in the dark (angry, confused, split off from their nature, feeling overall powerless and dependent), which is why I say it is layered work. It’s program upon program upon program. We awaken when we’re ready. However, this IS the new paradigm. Perhaps it will speak to some people on here, but I imagine not the majority. I’d love to be wrong about that second part!
Report comment
Proof, Steve, proof. I do find your dysfunctional brain theory dubious. Elliot Valenstein, a psychology and neuroscience professor, authored a book he titled Blaming The Brain, and subtitled The TRUTH About Drugs and Mental Health. I would imagine, having read Mad In America and Anatomy of an Epidemic, you might get an idea of where I am going with this thing. *Tongue in cheek* She’s a bright girl, with a lovely personality, whereas he, her brother, he’s a dumbbell with a brain dysfunction, or is he? Perhaps he’s just a convenient scapegrace. Anyway. Thank heavens we’ve got institutions, electro-shock, Abilify, and you name it. Otherwise, he could become a real problem for us.
Report comment
I am never arguing for any kind of “broken brain” theory. I am saying that there ARE brain problems, which are handled by neurology or some other actual medical specialty. I was trying to explain within Rassel’s context of materialism why “mental illness” still does not make sense as a medical problem. I’m not a materialist by any stretch of the imagination!
Report comment
I agree with you that there are neurological conditions as distinct from psychological or psychiatric ones. Head trauma is still head trauma, and generally leads to medical attention. PTSD, well, that might be something else altogether.
Report comment
My dad has worried i have Lyme Disease. I explained how psychiatric “remedies” damage the brain and CNS. Especially long term.
I think this comforted him. He is surprised I can function off the “meds” the experts swore I needed for the rest of my life.
Report comment
Rasselas, I do not believe hatred arises from “mental illness”.
What does it mean when you say “I don’t like the majority of people”. I suppose there is a big difference in “not liking” and “hating”. To hate is to passionately dislike someone or something.
I know millions of kids are getting antipsychotics and Ritalin. Wonder what the explanation for that is. Must be their organic brain disorder or mental illness.
And old folks get drugs in their food. I wonder what their diagnosis was.
Are behaviours mental illness? Or are they behaviours that certain people don’t like.
Duh, of course your behaviours can be quantified by peeking in your brain, OR better yet, the result is of course seen AFTER the behaviour. You know, all the little things going off and dancing around in chaos and disorder. And we know that quantifying has not happened so everything beyond that is opinion.
Yes mankind kills. Yes we get angry, We hit walls. We dislike people.
And yes I am allergic to the “mental illness” word, and according to my own assessment of that “neurosis”, is because I am defiant. I am defiant of someone telling me I’m going to hell and that I have a soul.
I am defiant of someone telling me that my “symptoms” or my anger are a mental illness.
See, I am sensitive to my own feelings. When I don’t like the “majority of people”, I feel as if that is not “normal”, then I fear I must have a mental illness, because the idea of mental illness convinces a heck of a lot of people to doubt themselves.
Besides, any entity where nothing but harm comes from it’s practice, why would I not be “neurotic” about that system?
You could convince me to the validity of psychiatry if the labels could not result in loss of jobs, not having rights within court systems as a parent (if one parent decides to use your label as a way of gaining custody) if psychiatry did not invent their ridiculous behavioral and symptom labels, if people were not force drugged.
I completely understand why you try to explain oddities or crimes by mental illness.
the thing is, it includes everyone. It is a matter of degree.
Report comment
I struggle with the urge to go full misanthrope myself.
In my phone talks with Julie Greene she told me that distrust–even hatred–for most of humanity is common to psychiatric survivors.
It comes from being cast out of society so only a few fellow outcasts will still speak to you. Of being blamed for every violent crime committed. Of trembling every time you hear of a mass shooting since you know people will blame duly appointed scapegoats for society, known as the “mentally ill” for the actions of those you have no control over.
if it were seen as punishing a group for the crimes of a single individual, people would be forced to acknowledge the injustice. But call life long imprisonment/mutilation/druggings “treatment” and dismiss those forced to suffer. They can take pride in their benevolence and only need to fear dislocated shoulders from patting their own backs.
But we who survive the System are not fooled. We see through this faux compassion for what it is. Cold indifference to the suffering of their fellow human beings. Projecting the murder and madness in their own hearts onto the designated Other. 🙁
Every morning I feel what has been inflicted on my body. I make a conscious choice for forgiveness and love. Not easy and the damage remains. But my psyche is noticeably better.
I only know what goes on in the hearts of the scapegoating “sane” because I too am guilty of this behavior. i truly am one of them–acknowledged or not.
Report comment
Rachel, good comment.
I think it is a completely natural reaction to dislike that which has harmed and then end up having a general intolerance for those masses of people who help to keep the harm going by the sheer belief that the harm has benefits for their society, despite all the available proof and studies that it actually promotes not being well and promotes being dependent.
The thing I found absolutely shocking was that if people go to them for help (which is actually a sign of insight) leads to being treated as an oddity, as one who is not normal.
It IS what turned me completely off psychiatry.
It took me years to logically see that someone’s opinion of me does not mean anything, yet I still carry the hurt from it.
Report comment
I was the model mental patient for 22 years.
What did I get for it? Alienation. Segregation. Dire poverty. Banned from gainful employment. Massive weight gain (more than 100% body mass.) Autoimmune disease. Heart problems.
That’s how the mentalists reward you for the insight they praise. And they assume you’re stupid and warn your family that you won’t take your “meds” since “they never do.”
Of course my “insight” and reputation as a “good consumer” helped me escape once I figured out I’d been had. The real advantage to compliance.
Report comment
Most mass shooters either kill themselves or get killed at the end of their insanely narcissitic horror operas. When they don’t, we find a mentally ill person. Or, more often, someone we would perhaps deem to be personality disordered.
It is not considered fair game to denote someone as mentally ill or personality disordered because of their political ideologies. That to me is a categorical failing.
The problem then for people like Trump, is that they would fall foul of my liberalising of the DSM. In fact, there are very few politicians that wouldn’t. And then almost everyone would fall foul of my liberalising at some point in their lives. At many points in their lives.
On the one hand we say that there is no such thing as mental illness. People have problems and they need help getting over them.
And then on the other hand we turn a blind eye to religious and political extremists. We insist that holding certain political and religious views are protected, and effectively healthy and okay.
The world is a gulag populated by the mostly insane.
Perhaps there is some truth in the fact that the aliens have a vested interest in keeping humans on this prison planet. We’d cause mayhem elsewhere.
Report comment
We were ejected for good reason. Not worried though, we only get as much as a 100 years and then that is the end of MI. Hopefully we don’t reincarnate.
Report comment
Almost every human being reincarnates as a pig, a sheep, a cow or a chicken. This has long been known by people that have written similar sentences in other languages.
Thankfully most are reborn into intense modern meat farming factories and they aren’t so very long in the torment, despite the despicable end.
Happy Christmas.
Report comment
Actually I’m not coming back. No desire, because my biggest fear is that I will come back to become a psychiatrist.
Report comment
You’d have to have racked up some serious bad Karma to come back as a psychiatrist!
Report comment
Thank You Leah, for the work you’ve put into this document. The sunny video promotion with the gay colours is very very smooth.
I personally identify with Akathisia.
Report comment
Why did patients want MyCite? If they forget pills they want to take there are pill boxes.
So MyCite can monitor heart rate and sleep patterns?
In my imagination I see someone watching a monitor. “Dr. Q, Ms. X hasn’t slept at all in three weeks.”
Dr. Q, “Later. Got an office visit with Bambi. That new pharma rep.”
Monitor “Ms. X’s heart beats are off the charts. Her breathing patterns are erratic.”
Dr. Q, “Let her ride it out. I’ve got a Caribbean cruise to plan.”
Monitor “Ms. X didn’t take her Abilify at all the last twenty-four hours.”
Dr. Q, “Get the police out there immediately!”
Monitor, “Turns out she’s dead.”
Dr. Q. “At least she DIED WITH HER RIGHTS OFF.”
Report comment
That is chilling, yes, thank you. I have wondered whether something like MyCite could have saved my mother’s life by alerting authorities as she was dying, but see here’s the thing, even as much as I want her around, what if she didn’t want to be saved? What if she didn’t want to keep being intubated and returned to that way of life? She was exercising her right to bodily autonomy that night.
Report comment
Leah, they don’t care if we die. As long as we die compliant.
My friend didn’t want to die. But her shrink made her take a drug that killed her. 🙁
Two years off the “meds” I realize my heart is beating normally again. I believe doctors knew this was so but feared ramifications if they told me my “meds” were slowly killing me.
Report comment
Leah, I’m sorry you lost your mom.
Guess what, none of us wants to die, but I think even more of us really don’t want to suffer.
And in the ICU, within medicine, just like within psychiatry, we lose autonomy.
Humans like to keep some dignity, some inner peace. Medicine greatly interferes with process, physical and of the experiences of being.
Your mom went with autonomy, no one to control HOW she went. hugs
Report comment
Below is my own Experience of Long Acting Injections + Akathisia + Genuine Recovery + Medical Uselessness
https://www.madintheuk.com/2018/08/a-disorder-for-everyone/#comment-49
Report comment
Thank you for sending this. I look forward to reading.
Report comment
What an amazing and collection of information! Thanks for all your hard work to put this together! This makes me furious as I watch the reality of pharmaceuticals that are trying to sell compliance! Watch the Bleeding edge if you still trust the FDA. The last 6 minutes of questions after the Proteus talk you have above, were a great summary of their idiocy! A great deal of their presentation made me feel nausea and mounting sweat, and the part that really made me want to puk was when they said,”it is very expensive, but 90% of the expense we anticipate will be paid for by Medicare and Medicaid!” This whole mess is just GRRRRRR on so many levels of idiocy!
Thanks for your work to share these powerful truths in such a wonderfully articulate collection!
Report comment
I’ve been lurking here at MIA for a long time. Can you help me understand a couple things? I apologize for the length, but this piece finally compelled me to speak.
(I see this is awaiting moderation. I have commented respectfully and honestly, and if it is rejected I will be disappointed and no closer to understanding.)
First, two things you don’t need to convince me of:
✔ That some people would rather create scapegoats than deal with child abuse, domestic violence, poverty and gun laws — hence the false narrative that all violent people are “crazy” (and that all “crazy” people are violent), and
✔ That errors, negligence and abuses happen in the arena of psych care, meds and diagnoses.
That said…
1/ A bit of history: What people call “mental illness” or “psychosis” today has been around a very long time.
I’m not talking about “creativity” or a refusal to “fit the mold.” I’m talking about hearing terrifying voices, incapacitation due to depression, and unrelenting agitation.
Historically, most societies and cultures have not seen such people as seers or sages.
In ancient Greece, Rome, Babylonia, China and Egypt, these were signs of demonic posession. Exorcism “techniques” included starvation, floggings, and, when these failed, execution.
In 25 BC, Cornelius Celsus shacked and beat them. In the Middle Ages, many of them were imprisoned or burned as “witches.”
But punishments weren’t always imposed by force. Autobiograpical accounts reveal the lengths sufferers have gone through to hide their symptoms and finally to seek relief. Crude surgeries, forced vomiting and bloodletting were among the “cures” through the 15th, 16th and 17th centuries.
Journalist “Nellie Bly” discovered a literal snake pit when she feigned mental illness to get into the Lunatic Asylum on Blackwell’s Island. The people there were mostly societal “outcasts,” and she said, rightly, that most had been perfectly fine until after they’d been sent there. But the era is still full of accounts of people who suffered from delusions and “hysteria” without ever having seen the inside of an asylum.
I study history — not just history of psych, but history in general. And it seems to me that dehabilitating depression and psychosis existed LONG before SSRIs and Big Pharma.
It also seems that such symptoms WERE seen as “a thing” — a particular, extreme condition for some people, not just universal emotional experiences to be treated with rest and herbal tea.
Yet I often see narratives that suggest false (at best incomplete) historical narratives. What am I missing?
◈ ━━━━━━━ ⸙ ━━━━━━━ ◈
2/ Can you tell me what SHOULD have been done in each of these 3 cases?
A] I had connections within a community of Ethopian immigrants. One woman, “Abena,”
had suffered from symptoms of “psychosis” for years. Her extended family had taken turns supporting her financially and caring for her. But she’d become confused and combative, and they were at the end of their patience.
I know Abena had not received any “psych” treatment. Her family was traditional: they didn’t trust western medicine at all. They attributed her symptoms to entirely to spiritual issues, and had been treating it with prayer.
By the time they specifically asked me for advice (they didn’t speak English well and could not navigate “the system”) Abena thought her beautiful daughter was a demon, and was talking about burning the house down.
I confess that I helped her sisters get a 72-hour hold for her (which wasn’t easy). A full medical workup revealed that Abena’s delusions and hallucinations were the result of toxicity from undiagnosed liver disease.
The bad news was her liver was so damaged, she died a couple years later from liver failure. The good news (according to what Abena and her family told me, and what I saw myself), antipsychotic meds were able to decrease her delusions to the point where “the demons” went away, and she, her sisters and daughter were able to enjoy a wonderful visit to Addis Ababa before she died.
Her family thanked me at her funeral for my help. I’ve made lots of mistakes in my life, but was getting psych care for Abena really one of them?
⊱⋅ ──────────── ⋅⊰
B] Another friend (American) had a 22-year-old daughter, “Serene,” with no known psych history. Over a period of weeks, Serene went from being a bright, sociable and athletic Ivy League student to psychotic.
Serene was hearing voices, thought her mom was poisoning her, and believed she was a concubine in the harem of a powerful king. My friend found her wandering one night in the street, naked, looking for him.
Within days, Serene was in the ICU, with massive, multiple organ failure. It turned out she had lupus (the psychosis is a symptom, albeit a rare one).
Against the odds, Serene survived, but suffered major brain damage. My friend had to quit work to become her full-time caretaker. And Serene still believed she belonged to a king, was being poisoned, and tried to climb out the window to escape … when she wasn’t on meds.
When she is, though, she reads, hangs out with friends, listens to music, and helps her mom cook. This is the way Serene has been for most of the last 2 years, except for a couple periods when she wanted to stop meds.
I guess you could say her mom is “controlling her.” Maybe she thinks this is better for Serene than her being naked on the streets where she could be raped or shot.
(Actually, without financial assistance from “The System,” her mom being named legal guardian and caretaker, they’d BOTH be living on the streets. I’m unsure what people with certain symptoms, who cannot support themselves financially, should do for rent and food if they eschew medical diagnosis.)
》 So, those were two cases of “mental illness” that certainly seem to be medical conditions…”brain disorders.”
⊱⋅ ──────────── ⋅⊰
3] Just yesterday, a friend of mine decided her walls and light fixtures contained tiny people, who were spying on her and talking about her.
She got up on a ladder and used a drill to tear her ceiling and wall apart. I found out because neighbors contacted another friend, adding that she has tried to enter their home multiple times and threatened them.
This happened after several years of my friend self-medicating anxiety with marijuana (which is illegal here). To MY knowledge, she has not been on antidepressants, since I have known her. She has no insurance or doctor.
As we learned more (alarming) details, it became clear that she is “a danger to herself or others.” We are working with her parents to (hopefully) get her professional help. But things don’t seem to be going well at all. They don’t have a good relationship, and her issues may well be “their fault.” She thinks we are all part of a spy ring. None of us has the resources to care for her (and she doesn’t trust us anyway).
So, reading this made me realize I really had to respond today.
What should we do? Just let her be?
Even if she electrocutes herself?
Even if she gets shot by the neighbors?
Even if she winds up living in a sleeping bag because she can’t support herself?
Because she should have “freedom?” “Automomy?”
Help me understand.
Report comment
Posting as moderator:
Hi, Kitty,
I just want you to know that now ALL comments are held for moderation, so yours was not singled out as such, it just joined the moderation queue like every other comment.
— Steve
Report comment
Oh, yes — I assumed that all comments are moderated. I was just concerned it wouldn’t pass that step, but it did.
And BTW I agree with your comment above (“… If it is the latter, then claims that all shooters are “mentally ill” is pretty meaningless, as it seems to be defined simply as behavior that a society disapproves of.”)
Report comment
“A bit of history: What people call “mental illness” or “psychosis” today has been around a very long time.”
Not exactly. The coupling of the words “mental” with “health” goes back to the year 1803. The coupling of the words “mental” with “illness” goes back to the year 1819, and “psychosis” goes back to the year to the year 1847. Approximately, of course.
If we’re going to speak of such matters in ancient times, I think we’re going to have to look at their concepts, and their language. Things have changed a great deal, and we shouldn’t be thoughtlessly imposing the present on ancient times or ancient societies.
Report comment
Thank you, Frank.
What you say about the language of mental illness is 100% correct.
I am sorry if I wasn’t clear when I wrote:
》What people call “mental illness” or “psychosis” today has been around a very long time.”《
By qualifying it with “what people call,” and putting quotes around words, I hoped it was evident that I understand this.
My next paragraph said:
》I’m talking about hearing terrifying voices, incapacitation due to depression, and unrelenting agitation.《
Symptoms. Distressing things happening in the mind of the person.
I actually spent a couple of hours writing, and rewriting, my comment last night. (And I’m a writer!) I struggled so mightily with the right words to use, to be clear and not cause offense.
I don’t care about the language. We can call those symptoms “BZJHT” (just random letters on my Android keyboard.)
People have experienced BZJHT in all cultures throughout time.
Is that more clear?
I have seen people here say things like “I don’t know what to call it.”
It makes this extraordinarily hard to discuss.
Report comment
Random letters on a keyboard don’t even make an intelligible acronym. I don’t think ADHD a particularly intelligible acronym either, but that is that. Granted, many people in the system have communication issues, and now they have, as they have always had, alienation issues.
My concern is rather, and I can see the reasons you are there, and that they are important ones, at least for you, the impending deprivation of liberty and the scrapping of due process that goes along with it.
“As we learned more (alarming) details, it became clear that she is “a danger to herself or others.” “
“Danger to self or others” is the legal term that allows locking innocent people up for being in what one might call distressing and complicated situations. In other words, it is bad and constitutionally unsound law. I personally have a lot of issues with holding people for their own presumed good, and protection. There is, after all, a risk to all endeavors. Together with having the right to do something constructive with one’s life, I think one should have the right to do something destructive with that life. I don’t think the state should be making those decisions for a person when no crime has been committed. You don’t “treat” people against their will, the matter at the heart of this ruse, without violating their constitutional, their citizenship, and their human rights. The rule of law that this law allows circumvention of, I think preferable to the rule of thumb that you end up with.
Report comment
But the desire of the community to preserve itself is at the crux of this involuntary commitment/treatment issue. From the community’s point of view, an individual does not have a “right” to act destructively if that action violates the rights of others (current list of rights is per the Universal Declaration of Human Rights, 1948). To maintain a good balance between the needs and desires of the individual and those of the community requires a higher degree of sanity in society, and particularly among its leaders. And by definition, this has to be a self-determined change for each individual.
Meanwhile, we push for saner practices based mostly on human rights concepts in a world that remains largely insane. This doesn’t mean we shouldn’t keep pushing for reform. But it does mean that this push should be paralleled by a push to find and deliver workable mental treatments on this planet. They do exist.
Report comment
“Mental health treatment” = brainwashing, indoctrination, terror, abduction, imprisonment, assault, torture…
There is a great deal of paternalism involved in this desire to detain the deemed dangerous while much of the deeming requires a leap to judgment or prejudgment on the part of the deemer. Donald J. Trump claims we need to start locking up dangerous people. At the same time, there are mental health professionals who claim that Donald J. Trump is one of the dangerous ones, and that he himself needs to be locked up, or, at least, “treated”. I’m not sure those mental health professionals quite realize that, were they able to do so, this “treatment” would make them a danger to Donald J. Trump, and, of course, certain other human populations.
I don’t think the desire of the community to preserve itself is behind involuntary commitment. I think the real basis for involuntary mistreatment lies in the desire to lay blame on a scapegoat for problems that the community has created for itself, scapegoating made easy by the designating label “mentally ill”. The community is a community that, quite literally, is the community of a species that is not threatened with extinction in the slightest. On the other hand, it is because of this community that certain other species are on the brink of extinction think of it what you will.
Report comment
Hi Kitty,
Just wondering if “Abena” and her family were Muslim? And if so how did they get around the prohibition on the use of intoxicants (Khamr)?
I guess my first thoughts were that Abena was suffering from toxicity related to liver disease, deal with the toxicity and the delusions/hallucinations stop? My second thought was that you described her as being “combative” and well, if you tranquillize someone who is combative they tend to be a little more compliant , but its not really the treating of any disease, its a three card monte. The use of these drugs in nursing homes being an example of how traquillizing folk can be used to make them manageable.
Report comment
Boans,
Thank you for your excellent questions:
》Just wondering if “Abena” and her family were Muslim?《
No. Actually, this Habesha community was Tewahedo (Ethiopian Orthodox Christian). My then-husband was a priest, and we had a local mission for immigrants and refugees from Ethiopia and Eritrea.
Orthodox per se are not against any western medicine. Nor do I suggest they are “primitive.” My best friend was one of the immigrants; she came here, got a master’s in biology, and helps runs the cancer research center at a local hospital.
But this PARTICULAR family, Abena’s, was not educated or “Westernized,” for lack of a better word.
As for intoxicants … you are correct that they are prohibited. But I know Muslim alcoholics, and Catholics who have abortions. Folks don’t always follow religious rules especially when they come to the US.
》I guess my first thoughts were that Abena was suffering from toxicity related to liver disease, deal with the toxicity and the delusions/hallucinations stop?《
Because her situation was extreme and acute (it also involved a couple of arrests, and posession of some dangerous stuff), they had to deal with what they perceived as medical and psych all at the same time.
And her liver was permanently damaged, it never returned to normal function. My understanding at the time (and there was always a language barrier, especially with complex things) was that she was essentially already terminal by that time.
And yet (and I hesitate to share this here, but it is honest), the time between her her hospitalization and the final stages of her illness — about 2 years — it was miraculous.
She was on anti-psych meds during this period (I know that word is disputed here) and she was a person I had never met before, the person her family told me she had been previously.
She had never come to church, because she rarely left the house. She didn’t bathe regularly, and smoked constantly. She rarely ate. She kept to herself, mumbling. She literally never spoke to her child.
That was the Abena I’d known for a couple of years before they said to me, “You must get involved.”
After… my God. I had no idea how gorgeous she was. She wore makeup, jewelry, gorgeous habesha kemis. She smiled. She was witty. She went to concerts and hosted dinners at the home. She became a mom again to her daughter. And, they were able to visit home.
I am not saying she was “manic.” She acted like a normal high-functioning person during that time. She even quit smoking.
》My second thought was that you described her as being “combative” and well, if you tranquillize someone who is combative they tend to be a little more compliant《
I don’t dispute that this is true in many cases.
In this case, I am talking about a Habesha family, fairly recent immigrants, who had cared for a woman for years WITHOUT involving the psychiatric system.
By “combative” I mean she screamed, threatened, threw things, destroyed property, and at one point had collected some illegal devices.
Like many families would be, they were overwhelmed.
》 but its not really the treating of any disease, 《
Sedation for sedation’s sake, of course not.
I am aware of what happens in nursing homes.
This was different.
This was not about making a grouchy person manageable.
I am sure you don’t believe me, but it is true.
And I am not sure if this community believes in Alzheimers, but it is real, and some patients do get violent as a part of that disease.
I don’t think we have any good answers for that.
Report comment
Just regarding the prohibition on these drugs.
You speak of Muslim alcoholics and Catholics who have abortions. This is of course true, and I have met the same. However, this is a choice that these people make willingly and I assume they have been informed by their community of the dangers associated with such behaviour.
I had a discussion with one psychiatrist here some time back regarding me being a lot more fun when i’m drunk, but I do not wish to be restrained and have alcohol poured down my throat at a party because others would like me to be partying. And should I turn and become violent as a result of being forced, would they then blame something internal to me (ie my illness) or the disinhibition from the alcohol?
So the issue of choice is involved. A slippery slope indeed.
Here in Australia I have come to find out that mental health services have been given the power to drug citizens without their knowledge with date rape drugs. A refusal to speak to a mental health professional could get you a death sentence. I believe if I were in the US this would constitute torture but here in Australia doctors have been given carte blanche on the human rights abuses, not only with those with a status of “patient”but anybody they like who can be made into a “patient” post hoc. Police will not take action against a doctor. In fact they don’t even have copies of the Criminal Code they tell me. This despite our Prime Minister stating that Australians are a people who value a rule of law. Then why place doctors and lawyers above it? Though he did also note the State Corruption bodies were being used as kangaroo courts to conceal the wrongdoing of our politicians etc.
Still, given this do you think that it is right to drug someone without their informed consent in the hope that they will recognise that it is good for them? Because my issue lies in the fact that whilst being pinned down and having alcohol forced down my throat might let me have a good time at the party, but i’m also the one who has to suffer from the hangover.
I see a problem for our government using the covert drugging of citizens before interrogations, especially with people who not wish to be stupefied/intoxicated without their knowledge.
I guess my question would be when do I (or Abena) loose our right to bodily integrity? I know my government says when I don’t agree to discuss a decision I have made to leave my wife with a psychologist. They can then torture and kidnap me to make sure I am making the right decision.
I also struggle to see how you could have difficulty getting ‘assistance’ for anyone given the system we have here. My wife tells me its just a matter of telling them what they want to hear. Ie I’ve drugged him without his knowledge, he’s collapsed, and I will plant a knife and some cannabis for police when you call them and request assistance with your patient you haven’t met yet. Oh, by the way he’s a needle phobic so bring a large one to hold up and cause a little acute stress reaction, police pointing guns at him in bed might not do the trick.
Where is my right to choose in this? No liver toxicity, no bizarre conduct, police detained a man who was asleep? Whats their justification for making a referral to a Community Nurse other than he lied and said I was his “patient”?
Anywho, glad to hear you made Abenas life a little better before she passed Kitty. Because on the other side of the world there’s a man (and his enablers) literally destroying peoples lives and calling himself a nurse while he does it. And receiving support from police to do it.
Would you have intervened in the health issues of Nebuchadnezzar? Or simply left him to eat grass?
Report comment
My thoughts exactly Boans!
Abena needed an endocrinologist. Not a shrink.
Why not fix the liver?
Report comment
》Abena needed an endocrinologist. Not a shrink.《
Um … what?
Endocrinologists treat diabetes. She did not have diabetes. She had advanced liver disease.
Rachel:
I brought Abeba to the ER of our local hospital (University of Wisconsin Hospitals and Clinics) and she was in the psych ward initially because she was in crisis.
They didn’t say, “You’re crazy. Here are some chill pills.” No. As I said, they did a complete workup.
They discovered she had advanced cirrhosis of the liver from Hepatitis C that had gone untreated for decades. She was dying. The psychosis was due to hepatic encephalopathy, and yes, there was trauma in her past as well. It was multiple things.
She was in the hospital for some time, but only in the psych unit for a few days. She was in different units, under the care of a whole medical team from different disciplines, working to save her life. It was a team approach.
Psych was only one part of it. There are some psych drugs that are contraindicated for this condition, and others that are helpful. They monitored her. They did not lock her in a dungeon with rats.
》Why not fix the liver?《
Is this a real question?
Do you really think a medical team working to save someone who was dying from cirrhosis didn’t think about “fixing her liver?”
They slowed the progression of her disease. She likely would have died in a month or two, had she not been treated at that time.
But some damage cannot be reversed. A liver is not a sprained ankle.
You know…I came here and really tried to be respectful. I asked some legit questions.
I do not think it would have been better for Abena to have burned down her home, and continued to believe her daughter was a demon, than to have had a period of happiness in her last few years because psych was involved.
I am in the middle of this debate because in my life, I have been both hurt and helped by psych meds & doctors, and I have seen friends and family both hurt & helped by the same.
I realize most of you have felt invalidated and gaslighted by the psych industry. They denied your lived experiences. The same thing has happened to me, and I know how horrible that is.
But here, I feel like MY lived experiences (and those of others, as well) are likewise being denied, invalidated and gaslighted. And it actually feels more painful here, because it’s coming from others with lived experiences…who I’d hoped would have some empathy.
I just don’t have the bandwidth for this right now. So I have to step away.
Report comment
I don’t know that I feel invalidated and gaslighted by the psych industry, that only came after being kidnapped and tortured by them. And when I started complaining about them breaking the law they destroyed my family and all aspects of my social life etc. I had no idea of course that they had the level of support to do that but ….
I note that you say Abena was only in psych for a few days and was then treated in a number of untis and by a number of disciplines. Thus she has seen a number of real doctors who have perhaps ensured she got the treatment she needed. This is not what occurs at the Ariel Castro Memorial that snatched me from my bed. They don’t spend enough time with yu to take more than your age and address before injecting you with enough tranquillizers to lay out an elephant for a month.
Sad that you feel your lived experience is being denied and invalidated Kitty because I cant say I know much about it.
Report comment
Psych IS indeed good and bad. It has to have some good parts, since otherwise, we’d all have left far sooner.
Some were nice. Of course they were nice. That’s what sucked me in. Some had terrible bedside manner.
I’m currently writing a piece on why people do not leave certain types of destructive situations. I hope it resonates with people.
Report comment
Kitty never chose to share any of her own psychiatric experiences. And as far as my GAS LIGHTING Abena and Serena neither of them are here to speak for themselves.
Report comment
These are good questions Kitty.
(For my part the “antidepressants” caused my psychosis. The massive quantities of Haldol used to help caused seizures and worsened the psychosis causing terror to me and all around me. I got kicked out of school. Still forced to live on SSI thanks to years of iatrogenic damage.)
It’s good these drugs managed to shut off the right parts of the brains in both instances. This is not always the case. It’s troubling they were the only answer for people with a damaged liver and brain, since they only make those physical problems worse.
I wonder if dialysis might have helped Abena. A damaged liver causes the body to fill with toxins. She needed to have these filtered out of her somehow.
As far as the third example the use of pot and emotional trauma may be to blame. Does your friend trust you enough to tell you what’s going on in her head?
Kindred Spirit, you have Lyme Disease. What’s your take on using drugs to calm two already physically disabled people?
Too bad only those drugs work at calming Serene. There is a reason she hates taking them. They cause a peculiar suffering of their own invisible to spectators. And they correct nothing–biologically speaking.
Neurologists might be able to come up with solutions other than destroying what brain tissue she has left. Sadly they have abdicated cases like hers to psychiatrists.
Report comment
Thank you, Rachel. I’ve seen you a lot here.
》For my part the “antidepressants” caused my psychosis. The massive quantities of Haldol …《
Yes, I know your story, and the story of others who developed their symptoms as a result of the meds.
I don’t want to get off-track with my own story. But I am a person who suffered multiple symptoms of what I call mental illness for 15 years BEFORE I ever swallowed a pill.
I do know about Haldol. Personally. I have blogged on it. It is a horrible, horrible thing. In fact, with both Serene and Abena’s family, I discussed this and was relieved to know it was not being used in either case.
I will leave it there.
》It’s good these drugs managed to shut off the right parts of the brains in both instances. This is not always the case. 《
You are absolutely right. It isn’t always the case.
However, to me, it suggests that there is some medical basis behind these symptoms and the drugs that affect those systems. It suggests that there are, at least sometimes, physical or medical causes for symptoms like these.
》It’s troubling they were the only answer for people with a damaged liver and brain, since they only make those physical problems worse.《
In both of THESE cases, specifically, the person was in the process of dying at the time. One has died (and would have either way.) One has a likely shortened life span due to the lupus. The question, I think, was to improve quality of life if even for a limited time.
Abd yes, I am VERY aware of long-term effects stories. Very. But these “short” stories are valid to discuss as well.
》I wonder if dialysis might have helped Abena《
She did have dialysis. That doesn’t fix the liver though. There was also discussion of transplant but she was not a candidate.
》As far as the third example the use of pot and emotional trauma may be to blame.《
Yes, I am 100% sure that is true. We all are, which is why I mentioned the pot at all.
I realize a lot of folks think that while Pharma is all bad, pot is all good…the natural medicine. I think it isn’t benign.
》Does your friend trust you enough to tell you what’s going on in her head?《
Not right now, but she’d had long discussions with many friends about all this in the months prior. We all knew parts of the story.
(My mom is dying and I have been out of town. I am getting this from our friends.)
But my main question is about the acute issue.
When your friend is drilling holes into her walls and ceiling, ripping lights and wires out, and telling people they are cameras… when she is screaming accusations at neighbors….
And you (her friends) have taken turns for weeks staying with her, talking to her, listening to her, and this is happening….
WHAT DO YOU DO?
If it is WRONG to get police or psych involved, then what?
If it is WRONG to hold people against their will, and what they are doing can get them electrocuted or shot… What are the options in those hours?
That is my question.
》Too bad only those drugs work at calming Serene. There is a reason she hates taking them.《
You are reading into what I said. I didn’t say she hated taking them. She, her mom and doctors all wanted to see how she would do tapering off various meds, to see what worked and didn’t.
It was not JUST her psych meds. Lupus has a cocktail, like HIV.
Without the antiosych meds, her delusions return. And she hates THOSE.
《And they correct nothing–biologically speaking.《
Very true. But many or most drugs DON’T “correct” things. Pain pills don’t fix a broken back. Insulin does not reverse diabetes. Many drugs relieve symptoms, and almost every drug has drawbacks.
》Neurologists might be able to come up with solutions other than destroying what brain tissue she has left. Sadly they have abdicated cases like hers to psychiatrists.《
I don’t know every detail, but Serene and her mom work with an entire staff of health professionals, social workers, occupational and physical therapists.
Report comment
“Like insulin for diabetes.”
Sounds familiar.
Report comment
You seem to be ultimately asking at what point is psychiatric violence acceptable, and my answer is never. It is never acceptable to abuse another human being. Period. I don’t care about hypothetical scenarios at all. It is never acceptable to abuse another person. Alternatives to psychiatric violence? Peer support, peer-run facilities, Open Dialogue, etc. Don’t have them? Start advocating for change, so you don’t have to be complicit in violence. Raise up voices of psychiatric survivors, keep safe spaces for survivors, talk with your law-makers to provide funding for humane alternatives, etc.
Secondly, I am concerned for the people whose histories you cite. You are not them, and as such, you have no idea how psychiatric violence affected any of these people, whose histories you casually cite, pseudonym or not, as if they are not capable of finding this site. I doubt they consented to any of this, and I’d advise you to consider just whom it serves when you cite people’s personal lives like that.
Nothing about us, without us.
Report comment
Well said.
Report comment
The original “first they came for” by Martin Niemöller January 1946 does have the mentally ill named “Then they got rid of the sick, the so-called incurables.” http://marcuse.faculty.history.ucsb.edu/niem.htm
I am sorry your mother Gail Susan Harris only made it to the age of 46. With those in power assigning her death to natural causes, like https://www.madinamerica.com/2014/02/uk-mans-death-medication-side-effects-ruled-natural-causes/
The only difference between the sane and the insane is that the sane have the power to lock up the insane.
Hunter S. Thompson
The “long term recovery rates for the schizophrenic patient” can be translated to “long term recovery rates for the Communist” why would a communist work for the authority that would jail , poison or kill him/her?
Report comment
I just celebrated my 46th birthday. Sad for your mother Leah. And my own friends who died young from “standard care.” Not suicide either. Side effects.
Off my drugs for 2 years. Can finally keep my room clean, shower regularly and half way through my first written novel. My heart is beating normally, I sleep less than 12 hours a day, and I have lost over 40 pounds. I can enjoy music and the beautiful scenery where I live for the first time since 1992.
No mood swings or thoughts of suicide anymore.
I owe it all to non compliance.
But MIA is one of the few places anyone will hear stories like mine.
Report comment
Belated Happy Birthday.
And Happy Chistmas.
Report comment
Merry Christmas RR. 🙂
Report comment
Thank you for this important article.
I think that Your mother was afraid of the Nazis, because they represented apollonian ego fundamentalism. Materialism in its worse version – Nazi fantasy about wiping out the psyche and pathology. Nazis fantasies about destroying the poetic basis of mind…..Apollonian ego imperialism.
We must remember that rationalism is just a one kind of perception, it belong’s to apollonian ego materialism. Apollonian ego can’t even built a proper image of the psychological reality. Apollo (rationalism, science) is not the father of human psyche.Zeus/Hades is. Hades represent psychological reality, and we live in the Apollonian ego era…..In the age of the hegemony of rational mind. Psyche is seen as its worst enemy…
We must see the worth of the psychosis. And rational mind is not able to see it. Psychological mind can. Psychological reality has been destroyed by monism theories (by the age of reason) long time ago. To understand psyche we must go back to romanticism, to the times before Christianity. Because monotheistic man is not able to describe the real nature of the psyche.He is talking about theology an rationalism, all the time.And this is tragedy.
I highly recommend Hillman’s archetypal psychology to everyone. We must have his knowledge about the long history of wiping out the psyche form human reality. Psychological mind in the age of reason is being destroyed.
We were born in the age of destruction of everything which is not rational. Our empty egoic culture has destroyed our psychological roots. Nazis represent apollonian ego, and psyche is in their trash bin. Psychiatry is on the same level of rational hatred.
We are talking about banned identities. We are talking about killing people in the name of rational fundamentalism. We are talking, all the time.
We should fight.
——————————————————————————————————————
James Hillman on the folly of reducing mind to brain.
https://footnotes2plato.com/2010/12/14/james-hillman-on-the-folly-of-reducing-mind-to-brain/
—————————————————————————————————————–
You and Your mother are heroines.
James Hillman “Re-Visioning psychology”.
Heil Psyche!
Report comment
Thank you so much for your kind words, danzig666 and bringing in the thoughts of Hillman. You have reminded me to go back and explore Hillman in more depth. Reading Mass Murderers in White Coats helped me to see the parallels between Nazi eugenic ideas and what my mother experienced in the 1970s-1990s, at the hands of the public mental health system. I just wish I would have known about all this when she was alive, to tell her that I understood.
https://www.scribd.com/document/142597108/Mass-Murderers-in-White-Coats
Report comment
Yes. I have a dream that the future will return a stolen identity to modern slaves, and persecutors will be punished with an eternal stigma of stupidity. Without the proper image of the psyche nothing can be done. I hope Hillman will help people to understand the meaning of the psyche, the stolen meaning and the role of our suffering. I hope one day we will become humans, not biological machines used by the state.I hope so.
School children should learn about the history of psychiatric abuse.
Report comment
Over the years, I’ve noticed that a number of these shooter guys are likely hypoglycemic, as indicated by artifacts such as candy wrappers, pop and beer bottles, “Twinkie” type mini cakes, French fries and or bags they came in. Of course these aren’t “psychiatric” disorders, because they’re identified by physical testing, whereas “psychiatric” disorders are diagnosed by data messages from the Astral Plane.
Report comment
Well anything which starts off connecting the idea of ~mental health~ to these spree shootings is not going to go anywhere good.
We must oppose the idea of ~mental health~ everywhere.
Foucault & Governmentality
https://www.youtube.com/watch?v=KWTXVPHc7dU
Report comment
Leah, Thank you for all the work to present this very important and compelling piece. It is heartbreaking to hear your mom suffered such horrible effects of the psych drugs and lost her life at such a young age. That is an adorable picture of you and your mom. You both look so happy to be together and I am so sorry for your loss.
Those in power talk about the cost of non-adherence, but what about the cost or toll on someone if the drugs are having intolerable effects on both mind and body, organ damage or failure and they cause an early death. That is a very high price to pay for “adherence”. Instead of calling it non-adherence or non-compliance it should be called exercising one’s right to autonomy. It sounds calculated and highly unlikely “patients” actually wanted the digital pills, maybe accepting the digital pills was the only option they had to avoid forced injections.
Report comment
This article has spotted the basic pattern of how those who want a super-controlled society are rolling out their plans.
I don’t see any group on the scene that has been more effective than CCHR at reining in the psychiatric aspect of this strategy, which is a very key part of it. If you are going to coerce a society through the subject of mental health, then you need “experts” who are willing to cooperate in doing your dirty work. CCHR is trying to take the subject of mental health away from the criminal psychiatrists. I think it deserves our support.
But what I also see here is a lack of understanding regarding what the bigger picture is, and why people like those psychiatrists could ever rise to the status of “mental health experts” while so obviously getting no real results. And that lack of understanding leads to an incorrect estimation of effort of what it will take to turn the whole scene around.
The technologies discussed above are not the only ones under development. And though the drug model for treatment currently holds sway, I am sure other strategies are being developed, should they be needed. It is not enough to play cat-and-mouse with these monsters. We must take away their power forever. It is a huge job, and it will require considerable organization.
I just want to make sure readers have some concept of the magnitude of the problem we are up against.
Report comment
In the psychiatric field, it seems like a rather too symbiotic technology. To the point where the patient becomes the product and the research company becomes the consumer. The gathering of information is a lucrative business and choosing the vulnerable as first recipients is nothing new. GPS technology could accompany that digital technology. Maybe patients could be renumerated for accepting to be tracked. Pay the patients 1000$ per month to be used as a future statistic. However, as a doctor, I’m not, I’m not sure I would derive satisfaction in tracking my patients. And where does the technology end up? In our drinking water? I dunno. My credit card company can define my life more readily than any doctor and I don’t lose sleep over it. I can see pros and cons to it. It seems like a departure from care however.
Report comment
Trump seems to be poised to set up Homeless Internment Camps, and that will likely also be linked to a ~Mental Health~ justification. They will use this to con people into accepting case management and into disclosing personal affairs, FYOG of course.
A digital asylum is like being an out patient.
This forum must stop promoting Psychotherapy, Recovery, and Autism/Aspergers/Neurodiversity.
Report comment
Case Management is already used in Homeless Moral Reform Programs. It is a type of ritual humiliation. Kind of like Psychotherapy but without any pretext of being on the client’s side. Its a way of breaking down privacy, and a way of backing up the harmful actions of previous abusers.
Kind of like interrogating a rape survivor, and telling her that her food and shelter depend upon being open and truthful with the interrogators.
Report comment
Leah, the story of your mother sounds like the story of my life. Since I was 19 years old I’ve been dragged in and out of institutions and been on various medications with and without compliance. I have a four year old son, whom I raise alone because his mother has fallen into a cycle of harm and addiction. I would like to point out to everyone on this blog and to the bloggette, that there are multiple class action lawsuits against the companies and sub-companies responsible for producing and selling Abilify. I am a member of the current class action in Canada, your friendly neighbour to the north. I am often bothered by the sheer power of this systematic-corporatoracy that grips the people of the globe. Through exploitation of the vulnerable and a warped social view on the causation of such happenings in a vast expansionism that preys on the ignorance of our reality, the people are lost. If the people do not believe this class structure which is fuelled by capitalistic gain and is the product of our selves, how can we prevent the inevitable demise of the individual. “The virtue of the oppressed” (Bertrand Russel) has proven to be a flaw in a digitized society well before it became digital. Now, as we see the corporate cartel El Pharma sweeping the globe with patented vaccinations, remember that same group has been greatly effected in the last few years regarding the opioid lawsuits. Furthermore, if I may add, the idea of disaster capitalism. Whether SAR-coV2 was a lab leak or not, there exists opportunity to profit, and they will make those profits at the cost of many. America was effected the most. Do not allow them to stifle our dissent. Never.
Report comment