
My historical study of the Essex asylum, just outside London, which was recently published in Psychological Medicine, finds that those who were admitted showed significant disturbances of behaviour or evidence of organic disease. Almost two-thirds of those who had psychological, as opposed to organic, disorders were discharged recovered or improved (mostly recovered). The idea that asylums acted as places to incarcerate unmarried mothers and social deviants is not borne out by this or other asylum studies. The current research does suggest, however, that modern mental health services fulfil similar functions to the old asylums—providing care for those who are unable to care for themselves, and containment for those whose behaviour is disturbing to others.

I started training as a psychiatrist at the tail end of the asylum era. These huge institutions, once a looming presence in the suburbs of cities and towns, were reduced by the 1990s to a few scattered wards, and over the next decade or two most of them disappeared altogether. Looking back, they were both better and worse than the system that replaced them. The asylums provided a ready-made community for both patients and staff. They were often situated in beautiful rural settings, with gentle activities like gardening on hand to take part in, and regular social events.
Today many patients live on their own and are isolated and lonely. Local amenities and activities may be far away, and many have little access to green space and countryside. Staff are dispersed and demoralised. Trade unions are smaller and weaker and collective activities are few and far between.
Nevertheless, my experience was that the community of the old asylums was a strange and insular one. Cut off from the rest of the world, it existed in its own bubble—a bit like a boarding school or reformatory.
While asylums existed, it seemed they were indispensable. Now they are gone, we realise they are not. So how did they arise and what purpose did they originally serve? How was it that 19th century society was persuaded to undertake one of the most expensive public building programmes ever to have taken place, and this at a time when the central state and national taxation were still relatively new? The asylum programme predates the formation of the psychiatric profession and the triumph of the medical approach to madness, so they were not intended for medical purposes, at least not as we would understand these today. What function did these places fulfil, therefore?
Scholars have answered this question in a number of ways. Some claim that the asylums were always intended to be therapeutic places where people could recuperate and shelter from the harsh demands of the outside world.1 Others claim they were covert prisons for social deviants, including unmarried mothers and political activists.234 Somewhere between these two positions, historian Andrew Scull suggests that the asylums were part of a broader system of social welfare and control, under the umbrella of the Poor Law in England, and linked with the workhouse (and its equivalent elsewhere). The workhouse was designed to force the “able-bodied” poor into work, and the asylums developed as a specialist alternative for people who were unfit for this plan.5
I looked at the medical case notes of people who were admitted to the Essex asylum, situated just outside London, at the beginning of the 20th century. I was helped by Joseph Rehling, an MSc student at UCL. We also referred to a history of the asylum compiled in the 1950s.6
We looked at the notes of 100 men and 100 women admitted consecutively in 1904. Most people admitted were working class; wealthier people would have been admitted to private asylums or made other arrangements. All the people admitted showed significantly disturbed behaviour. People were frequently described as “raving,” “incoherent,” “delusional”; some were singing, shouting or praying in unusual circumstances, and many were noted to be unable to care for themselves. People complained of hearing voices through the telephone, of having electricity in their heads; one woman thought her husband was Jack the Ripper and another that she was a steam engine. We classified the problems described in terms of modern concepts of mental disorder using broad categories (Table 1).
Table 1. Retrospective classification of presentations
| Male (N=100) | Female (N=100) | Combined (N=200) % | |
| Psychosis | 16 | 29 | 22.5% |
| Mania | 11 | 16 | 13.5% |
| Non-psychotic depression | 7 | 9 | 8% |
| Psychotic depression | 5 | 4 | 4.5% |
| Other organic disorder (epilepsy, delirium, unspecified) | 22 | 16 | 19% |
| Learning disability | 12 | 7 | 9.5% |
| Syphilis | 8 | 2 | 5% |
| Alcohol-induced disorder | 5 | 4 | 4.5% |
| Abnormal behaviour (unclassifiable) | 1 | 4 | 2.5% |
| Personal crisis (‘adjustment disorder’) | 2 | 2 | 2% |
| Dementia | 11 | 1 | 6% |
| Perinatal mania or psychosis | 5 | 2.5% | |
| Perinatal depression | 1 | 0.5% | |
| Total | 100 | 100 | 200 |
A total of 44% had an “organic” disorder, including dementia, delirium, epilepsy, learning disability, syphilis and alcohol-related conditions. Thirty-six percent had a psychotic or manic episode, and 12.5% had some form of depressive episode, with or without psychotic symptoms. The presentations of five people were unclassifiable, but they all showed disturbed behaviour including a young man who took his clothes off and attacked staff at the Workhouse infirmary from which he was transferred, and a young woman who was constantly laughing and described as “apathetic” and “unfit to manage herself.”
Interestingly, the 100 women we included were admitted over a shorter period than the men, suggesting that women were more likely to be admitted. Women had a higher rate of psychosis or mania, and men showed a greater frequency of organic disorders.
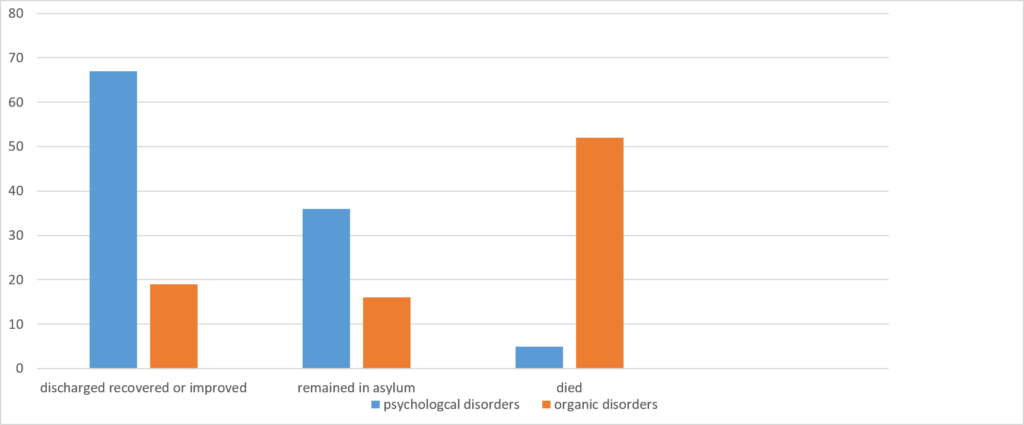
There is no doubt that people were discharged from the asylum if this was possible. Overall, 45.5% of the sample were discharged “recovered,” “improved,” or, in rare cases, “not improved” in the judgement of the medical author of the case notes. Just under 30% died in the asylum, usually shortly after admission. There was a marked (and statistically significant) difference in the outcomes of those classified as having an organic condition versus those with a non-organic or psychological problem (see Figure 1).
Among those with a psychological disorder (psychosis, mania, depression, perinatal conditions, behavioural crisis and “abnormal behaviour”), 62% were discharged either recovered or improved (52% recovered and 10% improved). A third remained in the asylum or were transferred elsewhere. For those with a diagnosis of psychosis, the rate of discharge either recovered or improved was 33%, with 62% remaining in the asylum. Among those with mania, 85% were discharged recovered or improved and 11% showed a chronic course and stayed in the asylum. Among those with an organic disorder, almost 60% died in the asylum, but 22% were discharged recovered or improved.
Figure 1: Outcome of organic and psychological disorders (%’s)
Unfortunately, we could not look at people’s ultimate outcome, because people might have been readmitted to several other asylums in the vicinity. These figures only relate to the outcome of the current admission. Those who were eventually discharged remained in the asylum for an average of 6.4 months and women stayed longer than men (eight months vs four months).
Interestingly, some female patients admitted with psychotic disorders showed evidence of recovery after protracted periods of disturbance. Agnes, for example, a 52-year-old married woman, was admitted with psychotic depression and continued in an agitated state for almost two years but then improved and was discharged recovered. Chrissy, a 27-year-old barmaid, was admitted with delusions and rambling and incoherent speech. Two years after admission she was still described as symptomatic, but after three years she was discharged recovered. Thirty-year-old Harriet was admitted with “melancholia” and delusions and was later described as hearing voices and looking “perplexed.” Over subsequent years she became “excited and violent” and required seclusion, yet she was discharged “recovered” five years after admission.
So what does this tell us about the nature and functions of the asylum system? We found no evidence that people were admitted for “social deviance” such as having illegitimate children, political activity, or petty crime. The only woman who was admitted pregnant and gave birth in the asylum had persistent psychotic symptoms and remained in the asylum for at least the next six years. Local rate-payers paid for the upkeep of asylum residents, so there was an incentive to discharge people, although the process was certainly not as speedy as it is today. Many patients seemed to be given a few weeks and sometimes months respite between being deemed “improved” and being discharged.
On the other hand, asylums were clearly places where people who were unable to look after themselves or were disturbing the peace, for reasons of organic disease or psychological disturbance, were sequestered until such time as they recovered their health or their sanity. The fact that many of them did recover owed nothing, of course, to any medical intervention that would currently be considered to be therapeutic. In this sense it was not a medical enterprise by today’s standards. Nevertheless, it seems that psychiatrists, politicians, and others at the time believed they were engaged in a therapeutic endeavour. The asylum system was founded on the belief that it could restore people to sanity, and regular inspections were designed to maintain these goals and ensure the quality of care.
I wonder if things are so different today? Although the mental health system is now firmly branded as “medical,” the long hypothesised biological basis of “functional” psychiatric disorders has failed to materialise, and psychiatry still has no treatments that target the supposed biological basis of symptoms as other specialties do. While it may not live up to its own self-image as a modern and sophisticated technical enterprise, the system does, however, provide care for those who are unable to care for themselves, and containment for those whose behaviour is disturbing to others. Such people still include a mixture of those with organic disorders and psychological problems.
Modern treatments can effectively suppress some symptoms, which may reduce the time people need to spend in an institution, but it is not clear that current recovery rates are any better than they were at the beginning of the 20th century. In fact, David Healy and colleagues found that people were more likely to be in institutional care of some sort in 1996 compared with 1896, but in 1996 the care was more diverse, including residential homes and supported housing.7
Recent research on recovery shows pretty dismal findings for people who have a psychotic episode or a diagnosis of schizophrenia. In a randomised trial comparing maintenance antipsychotic treatment to a supported reduction in people with a first episode of psychosis, only 29% of people overall recovered by 7-year follow-up—and of those who were allocated to antipsychotic maintenance treatment, less than 20% recovered.8 Another 15-year follow-up conducted in the 1990s found that over 80% of people diagnosed with schizophrenia showed significant social disability.9
Maybe the function of a mental health system is, after all, to provide care or “asylum,” while trying, at the same time, to foster people’s own abilities to recover.
****
Rehling, J. & Moncrieff, J. (2020). The functions of an asylum: an analysis of male and female admissions to the Essex County Asylum in 1904. Psychological Medicine. doi: https://doi.org/10.1017/S0033291719004021. Published online 15 January, 2020. (Abstract)














“The asylum programme predates the formation of the psychiatric profession and the triumph of the medical approach to madness, so they were not intended for medical purposes, at least not as we would understand these today. ”
There is no “medical” approach to distress. However, there is a chemical approach, not to be confused by “medical”.
Perhaps the original question can only ever be answered by those who left suitcases or a sock behind.
Report comment
PRACTICAL PSYCHOLOGY
The way I DEALT with my ‘antipsychotic’ withdrawal “HIGH ANXIETY” was to FOCUS on how my BODY felt, and NOT on my THINKING.
WHEN my Anxiety SOFTENED, there was NO PROBLEM; and I KNEW what TO DO.
SITTING WITH FEELINGS is NOT EASY – BUT IT WORKS.
Report comment
Even during my taper I had fewer emotional problems.
Suffering a lot of physical pain now. But no longer suicidal. No meltdowns.
No therapist or groups. All they ever did was remind me how hopeless I was anyhow.
Report comment
It is the perfect SET-UP.
You go in for hopeless feelings and have someone mirror back that indeed you are hopeless. Perfect scam.
How much more cultlike can it get?
Report comment
“Cult like” is exactly right!
According to “Mental Health”, if you suffer from “Bipolar” – there is no cure.
I got my Practical Psychology ‘organically’:-
Dr Wayne W Dyer (author of ‘Your Erroneous Zones’) was one of the innovators I studied.
Report comment
I partially read a history book on asylums and psychiatry for a whole country (which was from about 1850 onwards). There was a gradual rise of the asylum population from about 1 per thousand (around 1850) to about 3 per thousand in the first half of the 20th century. Slightly over half (~= 60%) had some sort of psychotic illness. The highest proportion were in the larger cities (up to 0,4%). Not sure what the average stay was before being released or transferred. The goal seemed to be recovery.
They don’t answer the question as to why chronicity is so much higher today, they emphasize that is the role for, or responsibility of, psychiatry to answer.
The question remains, if about 1% today are diagnosed schizophrenic, the most serious of mental illnesses, why weren’t the asylum populations 100 years ago much larger for the psychotic illnesses?
Why are prescriptions of antipsychotics so high today, about 2,5% of the adult population?
A possible answer is the neuroleptics themselves. Recent studies (on haldol, clozapine and olanzapine) suggest they increase hypofrontality. The most debilitating aspect of “schizophrenia” is cognitive impairment.
Report comment
“Recent research on recovery shows pretty dismal findings for people who have a psychotic episode or a diagnosis of schizophrenia….”
This is likely because, unbeknownst to the psychiatrists, at least according to their DSM, which neglects to include this information. The “schizophrenia” treatments, the neuroleptics/antipsychotics, can create the negative symptoms of “schizophrenia,” via neuroleptic induced deficit syndrome. And the neuroleptics/antipsychotics can create psychosis, hallucinations, and other positive symptoms of “schizophrenia,” via anticholinergic toxidrome.
https://en.wikipedia.org/wiki/Neuroleptic-induced_deficit_syndrome
https://en.wikipedia.org/wiki/Toxidrome
And, of course, when the treatments for a “disorder,” actually create the symptoms of that “disorder” – but all the psychiatrists claim ignorance of this fact. Well, of course, you will have dismal outcomes.
As to the primary actual societal function of today’s “mental health” industries, according to the medical literature. It does seem that covering up child abuse and rape – again due to a DSM flaw, an inability to bill to help such victims – is the primary actual societal function of today’s so called “mental health professionals.”
https://www.indybay.org/newsitems/2019/01/23/18820633.php?fbclid=IwAR2-cgZPcEvbz7yFqMuUwneIuaqGleGiOzackY4N2sPeVXolwmEga5iKxdo
https://www.madinamerica.com/2016/04/heal-for-life/
https://www.psychologytoday.com/us/blog/your-child-does-not-have-bipolar-disorder/201402/dsm-5-and-child-neglect-and-abuse-1
So we should ask ourselves, does society actually benefit from having – iatrogenic illness creating, primarily child abuse and rape covering up, pedophile and child sex trafficker aiding, abetting, and empowering – “mental health” industries?
https://www.amazon.com/Pedophilia-Empire-Chapter-Introduction-Disorder-ebook/dp/B0773QHGPT
https://community.healthimpactnews.com/topic/4576/america-1-in-child-sex-trafficking-and-pedophilia-cps-and-foster-care-are-the-pipelines
I’d say no. Especially since those “mental health” industries are also murdering 8 million innocent people every year, based upon their “invalid” DSM “diagnoses,” and with their neurotoxic drugs.
https://www.nimh.nih.gov/about/directors/thomas-insel/blog/2015/mortality-and-mental-disorders.shtml
https://www.nimh.nih.gov/about/directors/thomas-insel/blog/2013/transforming-diagnosis.shtml
That’s a psychiatric holocaust of approximately 400,000,000 people over the past 50 years. I’m quite certain our modern day psychiatric holocaust of innocent, mostly child abuse and rape survivors, should be ended!
Report comment
thank you for this, Dr.Moncrieff. well-written, succinct, and well-researched. 🙂
as a “consumer” / “client” / “mental patient,” I find there are times when I yearn for a real, honest to goodness asylum. A place of respite, of protection…from a hostile, cut throat society. Is there such a place, now? Was there ever, really and truly?
The asylum system Dr.Moncrieff describes seems to stem from a genuine sort of noblesse oblige, and I would assume also from a value system of a bygone era, one marked by far more cohesion and stability than the anomic, disintegrating world that neoliberalism has brought us.
I am thankful that Dr.Moncrieff and her colleagues have taken the time to do thorough research and offer a more nuanced, thoughtful perspective on the asylum than those of their predecessors.
Could modern society revive the asylum system, most likely in a modified form? Perhaps. Where I live, all the ‘experts’ emphasize ‘recovery’ and ‘the recovery model.’ Truth? I don’t think the US will throw the poor and working classes crumbs at this point, much less a clean, safe, quiet place of retreat from the neoliberal nightmare. Should an asylum system take hold in these United States, it will, in all likelihood simply mirror an increasingly unjust, harsh, inhumane society. No, thank you.
I appreciate Dr.Moncrieff’s disillusioned reflection upon the rather dismal rates of recovery from Schizophrenia. Is “Schizophrenia” even…real? Honestly, at a personal level, I don’t care. Sometimes, the mind breaks. The mind can break towards what they call ‘mania,’ and then the chances of (re)joining mainstream society are favorable. When the mind breaks in the way that they call “Schizophrenia,” then one’s chances of such a (re)integration are low. Perhaps a humane, livable asylum would prove an ideal situation, both for those in the asylum and for society, as a whole.
Report comment
yeah_I_survived Unfortunately society in these times was also very harsh, inhumane and cruel… The author mentions so-called workhouses: English people who were deemed fit to work, but were unable to support themselves were routinely sent to these institutions where they had to live and work in horrible conditions.
Report comment
true. somehow, that escaped my mind while I was writing my reply. Maybe I was day dreaming, a bit?
thanks for your reply. 🙂
Report comment
I support the above sentiments.
Though hinted at, a notable absence is any data on how the patients were treated. But the hint (that they were simply allowed to rest, eat, and follow some sort of non-challenging level of activity) gives us a hint of what we should have done with our mental health system, rather than deliver it into the hands of modern psychiatry.
I live in California and am part of a group that monitors state-level legislation on the subject of mental health. There have been at least 27 pieces of legislation introduced so far this year! I don’t know how this compares to legislation on other issues, but to me it seems like a lot of attention is being paid to this. And from what I can tell so far, most politicians are assuming that our “mental health” system actually produces mental health. If it did, this would be an entirely different discussion.
Why don’t we still have something like an asylum system if it worked as well as this research indicates? I know that our research indicates that German asylums were in a terrible state by the early 1900s, and institutions such as Bedlam have for long periods had a less than honorable reputation. Was the older model of care disappearing because it worked?
When it comes to psychiatry, I would not at all doubt that to be the case.
Report comment
chains were deemed as unacceptable, and created the much preferred by patients, straightjackets?
They keep improving “mental health care” The chemical straightjackets will soon be seen as unacceptable.
“Pinel created an inoculation clinic in his service at the Salpêtrière in 1799, and the first vaccination in Paris was given there in April 1800. In 1795 Pinel had also been appointed as a professor of medical pathology, a chair that he held for twenty years.
https://en.wikipedia.org/wiki/Straitjacket”
Psychiatry would say that they have come a long way lol. Obviously they do not believe this nonsense. They are becoming increasingly frustrated and perhaps should drop the “medical model” altogether.
It is making them look beyond stupid.
Report comment
And I think that one’s chances of reintegrating mainstream society after an episode of psychosis are much higher than you believe. The problem is that so many people don’t realize that recovery is perfectly possible, that the very concept of “schizophrenia” has no scientific validity and that it is absolutely not true that people with this diagnosis have to take antipsychotics until the end of their lives. When people see themselves as incurably mentally ill, recovery is very unlikely.
Another problem is the persistent stigmatization of people diagnosed with “schizophrenia”. The label is so stigmatizing that it has a very damaging impact on a person’s self-esteem (for some years I was not even aware how damaging it was to my own self-esteem) and life. People diagnosed with “schizophrenia” are still very often discriminated against by society if they are open about their diagnosis or their stay in a mental hospital.
And when people diagnosed with “schizophrenia” don’t fully reintegrate mainstream society in the sense of having a job, getting married etc., in many cases it is not because their mind is broken, but because leading a “typical” life would be much too stressful for them and because some of them have never found socializing easy… I personally think that my experiences with being frequently rejected and excluded by my peers and co-workers have not only contributed to my psychotic episode, but also explain why I now don’t feel ready to work in jobs where I may again feel painfully rejected and excluded by other people.
Report comment
We can learn that for people who were caught or who seek help things should be worse, but should not be completely absent.
Report comment
Attention everybody
29 Feb 2020
“A desperate hunt is underway for an unknown coronavirus spreader in Surrey who gave the deadly illness to the UK’s 20th victim – the first Briton to catch it in the country – amid fears of an explosion of cases in the county.
The victim, announced last night, is understood to be a man who was treated at Haslemere Health Centre before being transferred to Guy’s and St Thomas’ hospital in London.”
“Haslemere Health Centre”
https://www.dailymail.co.uk/news/article-8059159/Health-officials-desperate-trace-contacts-20th-British-coronavirus-victim-Surrey.html
2018
“Contagion! The BBC Four Pandemic – The model behind the documentary”
Abstract
“To mark the centenary of the 1918 influenza pandemic, the broadcasting network BBC have put together a 75-min documentary called ‘Contagion! The BBC Four Pandemic’. Central to the documentary is a nationwide citizen science experiment, during which volunteers in the United Kingdom could download and use a custom mobile phone app called BBC Pandemic, and contribute their movement and contact data for a day.”
https://www.sciencedirect.com/science/article/pii/S1755436518300306#bib0065
“1. Introduction
In a nationwide citizen science experiment, 360 Production, commissioned by the British Broadcasting Corporation (BBC), launched an app called BBC Pandemic that was available for download to smart-phones via App Store or Google Play. Using the app, the volunteers could participate in two studies: (1) one focusing on Haslemere, a town in Surrey, where there was a campaign to enroll a considerable number of people and volunteers’ mobile phone locations were simultaneously tracked with permission over three consecutive days, and (2) a bigger study for users across the United Kingdom that, with permission, recorded volunteers’ hourly locations to the nearest square kilometre over 24-h period chosen by the volunteer.”
“one focusing on Haslemere, a town in Surrey”
Report comment
“First potentially locally acquired case of #COVID-19 in the UK is in …. Haslemere
This is where our virtual #BBC4 Pandemic started in 2018.”
https://twitter.com/petrakle/status/1233547642803826689
Report comment
asylums are proven not to work when the patient can not complain. https://www.youtube.com/watch?v=rPBhuaxpL90
Report comment
Being hospitalized nine times or going to institution long term care is terrible.
It’s bone thugs n harmony singing, “We don’t belong here.”
There are choices and options.
Report comment
Removed for moderation.
Report comment
Dr. Moncrieff things are worse today–in a number of ways.
There are a number of problems with locking up people who have committed no crimes. Few of the people locked up were violent and failure to separate them from the harmless reminds me of the prison system William Wiberforce decried.
Not all were inhumane. But those that were seldom were held accountable.
Recovery from bizarre mental states was acknowledged to exist. Now it is not. This is used as an excuse for endless druggings–and proof of how necessary the pharma-psychiatrist is.
Nowadays we have the asylum without walls. This sounds better. But because they are able to “incarcerate” much greater numbers in the system and fewer are able to leave (numbers not percentages) there is a lot more suffering.
Psychiatry causes segregation as well as disability. While HIPAA may keep them from blabbing your label to the community, they will tell your loved ones. You need a go between. Sadly you are excluded a lot. And when included they talk over you. My mental illness team–as I call them–kept telling my parents how hopeless I was.
How I could never function normally and would be sure to be naughty and must be forced to take my “meds” regardless of how I complained. And if I didn’t recover they could be sure it was only because I was spitting them out on the sly.
I completed a four year degree in just eight years. I’m surprised I could do it at all. When I complained how I couldn’t concentrate they would tell me: A. It’s just your illness. Not the medicine! B. Sometimes the meds do that. It stinks but it’s necessary since horrible things will happen if you don’t take it religiously.
I took my drugs religiously for 24 years. Nobody believed I was taking them–except my family and a few others. Why? Because I deteriorated and wanted to kill myself.
My mental illness team kept promising me bad stuff would happen if I went off my “meds.” And occasionally mentioned good things might happen if I were really, really good. Showing insight and unquestioning compliance. A whole lot of stick with just a bit of carrot. Best way to keep us dumb beasts under control. 😛
When I told them how the “antipsychotics” caused disjointed thinking and psychotic symptoms and the “antidepressants” made me miserable and anhedonic–they told me that was proof of my illness. I was too crazy to know how they were helping me.
Which begs the question–if these drugs make crazy people sane why do these now sane people go off of them? Shouldn’t having these miraculous sanity inducers prevent noncompliance? Going nuts is no fun I can tell you. My true insanity was all drug induced. And the gaslighting my mental illness team dished out did not help.
It should be called the Mental Illness System. They don’t want you to recover. If you’re sane going in it won’t last long.
My parents–unlike many–stuck with me through my unlovable craziness. Despite the mental illness team’s efforts to cut me off from family and friends. I have had a couple good “normal” friends who stuck with me too. Thank God for their unconditional love. 🙂
They believed when I said I took my “meds” and were as upset as I was when I got worse “despite” Psych Magic. The whole thing was very frustrating for all of us.
I’m sorry for the suffering I caused them now. I never wanted to be a drug addict.
Very angry at being lied to and about! Struggling to forgive those who damaged me and really altered my life. (Some might say ruined but I refuse to think that way.)
Report comment
The reporting for asylums was not accurate as it is not accurate today.
We only have a family or psychiatry notes to tell us about the actions of a patient.
If a psychiatrist thought you had “inappropriate responses”, then reading that, we should automatically believe it to be true?
I do think shrinks have become nuttier over time, no longer able to distinguish between what behaviour troubles him or the patient.
Cops are another issue and I still can’t see a distinction except for the fact that cops generally use their fists, fat and guns and shrinks use their “expertise”. Both are an authority.
Report comment
Great point! When working with foster youth, I often found the kids accused of “assault” by staff in institutions when a very short investigation proved that the child was fighting back against the staff assaulting THEM! But that part never got recorded in the logs, did it? “History is written by the victors.” Certainly, the residents of any kind of institution are not the “victors” and their version of history is never recorded by the institution’s staff.
Report comment
Well said.
Report comment
That was what struck me about this article. The corrupt practice of verballing used to justify courses of action was alluded to by Dr Moncrieff in her paper Psychiatric Diagnosis as Political Device. This almost seems a step back from that article, when in fact what is needed is an analysis of the use of psychiatric diagnosis as a Criminal Device.
Take for example this quote
“Over subsequent years she became “excited and violent” and required seclusion, yet she was discharged “recovered” five years after admission.”
Was that what they stamped on the coffin? “Recovered”? I know from personal experience that my State government is authorizing the distribution of fraudulent documents in order to do ‘cover ups’, FACT. With that sort of environment nothing is real and you can’t trust anyone or anything in this system.
When they start calling convenience killings “unintended negative outcomes” to soften the language of what is really occurring, what use is such an analysis that is presented above? It might be worthwhile in understanding how they were ‘verballing’ then as opposed to now but ……
“We found no evidence that people were admitted for “social deviance” such as having illegitimate children, political activity, or petty crime.”
I’m sure if you looked at records where I live you wouldn’t find people being locked up and force drugged for any of the “exclusions” in the MH Act either. That just demonstrates an ability to conceal the fact that people are being locked up for being ‘social deviants’, not that it isn’t being done.
A belief in God is enough to detain and force drug someone in my State, you just need to make it sound like an illness first. “Patient believes they are being watched”, “believes the dead can be brought back to life”,.
I’ve a really good example of a ‘verbal’ here, something that is being given the full support of our government, despite a well known Commissioner stating that it will have dire consequences for the administration of justice (and I would add, the health and well being of people labelled falsely ‘mental patients’).
Negligence, fraud and slander has no place in medicine. And as this article shows, they have a hundred plus years of hiding the facts. Why are we surprised.
Report comment
Yes, a historical study based only on documentation from one point of view is unlikely to lead us to a full picture of what actually went on.
And though I am prepared to believe that this institution may have provided something resembling humane care, I am not prepared to believe that about asylums in general, and particularly about any institutions operated by psychiatrists.
That there was no financial incentive at this particular institution to do much more than provide rest and release as soon as possible, that is no longer the current financial model in most institutions. After all, that asylum is gone now, is it not?
Report comment
What can be learned from medical records of a past long gone?
The interpretation of a doctors mind at those times is my best guess.
There are no patients to ask.
I can hardly believe that they were trying to be kind! Society had many potently misaligned, cruel beliefs in those times. Many of those beliefs still hold true today guised under different ‘games’ we play. Not much has changed.
Report comment
I find the people who write this kind of thing, that is, rationalizing, if limply, the asylum system, very disturbing. I think such people ought to be confined to an asylum until such a time as they recover from such delusional beliefs, or die, whichever comes first.
“We found no evidence that people were admitted for “social deviance” such as having illegitimate children, political activity, or petty crime.”
We found no such evidence of people being admitted for social deviance except in so far as they were “raving,” “incoherent,” “delusional”; singing, shouting or praying inappropriately, or being, given another leap to judgment (and no due process to boot) unable to care for themselves allegedly.
Social is not, to my way of thinking, a form of disability.
The successful selling of “mental illness” and it’s “treatment” in the 1990s, over the 1890s, has led to a population explosion of people deemed to be so “afflicted”. This population boom, in combo with the closing of the old places of incarceration, has led to the opening of many mini-institutions, as well as more subtle methods of social coercion, indoctrination, management and control of deviant populations. Who needs a full time staff when you’ve got ankle bracelets and neuroleptic drugs?
Okay, so maybe we’re not there yet, but given time, robotics is sure to take up the slack. Ready, aim, tazer!
I disagree, obviously. We’ve in the past seen at least two great increases in the mental patient population. The first came with the development of the huge asylums you speak of, and the second came with the advent of social welfare and psychiatric drugs. If you want sanity, you’re going to have to put things in reverse, and then fast forward to before there were any “great” asylums. Lesson learned, we still don’t need them.
Report comment
It is pretty scary. The ONLY reason shrinks aren’t arguing for the humane practice of putting us to sleep–our alleged agsognosia means they can assume we want whatever they want–is that they can’t prescribe drugs to a corpse.
The real reason shrinks are praising asylums now? They know more people with soft diagnoses will be going off their drugs or dying. Fewer will replace them. Asylum franchises can rake in way more profits than letting them live in less restrictive environments. Though the latter costs the public less.
Report comment
I agree with most of this.
The only benefit of such a study might be to highlight the relative benefits of a less “medical” approach.
The study does not adequately cover the issue of society’s treatment of “undesirables” and so makes some basic assumptions that might well be false.
The tone of the introductory paragraphs seems overly sentimental. It hints at a better approach, yet in the end fails to fully vindicate that approach. Even if that particular institution were the perfect model of care, the chances that we could reproduce that today in our world are not very high.
And I don’t think we need historical studies to tell us the answers; we just need to open our eyes and look.
Report comment
No length of imprisonment is going to make people well who weren’t sick in the first place.
Neither will any amount of federal subsidy provide the basic necessity of, plain and simple, the avenue to financial independence, purposeful labor, a job.
Nor will any amount of drugging (intoxicating pollutants) produce sobriety (sanity).
That’s the big three when it comes to what’s been done that shouldn’t have been done. The obverse of the big three shouldn’ts would be the big three shoulds. Something along the lines of liberty, industry, and health–physical health.
Report comment
Frank,
Most people that earn a good living do it through funny handshakes, there’s not much difference between a welfare check and the average wage packet.
In the UK most of the welfare administrators, are on supportive welfare themselves.
Report comment
“In a randomised trial comparing maintenance antipsychotic treatment to a supported reduction in people with a first episode of psychosis, only 29% of people overall recovered by 7-year follow-up—and of those who were allocated to antipsychotic maintenance treatment, less than 20% recovered.”
I’m not sure if the author of this piece intentionally tried to obscure the outcome of the Wunderink study in the quote above … Recovery was 40% for dose reduction, vs 17% for maintenance. Just to be clear on that. There’s also the question of properly interpreting “symptomatic recovery” in a way that doesn’t skew the results. Psychiatrists tend to be a little biased in that respect.
Report comment
Also, the subjects in the study had all been drugged (and possibly indoctrinated, depending on your definition) for at least 6 months before they were split into the two groups.
Report comment
With an odds ration of 3.5 to 1 (from a drug withdrawal study) for a better outcome if you don’t take your psychiatrists advice, can we safely conclude that seeking help from a psychiatrist is bad for your health?
Wunderink has since changed his tune (he likes pharmaceutical money after all, and doesn’t want to lose his friends in the mental health scam), writing that the sooner you begin drugging children (in the predromal phase) with neuroleptics, the better the outcome. He didn’t do a study, it was just his musings (mental masturbation), paid for by some pharma company.
Report comment
https://www.youtube.com/watch?v=RKeBjLG-ueY
Here’s his talk from 2015. “I’m not against the use of antipsychotics …”, bla bla … but reducing doses is only for first episode patients, the ones who take it for longer are basically f***d. Sorry, didn’t we warn you about that? (twitches his eye and grins sheepishly) No? But I can talk endlessly about our biological hypotheses … did I mention I know where the hypothalamus is … and better treatment is just around the corner … did I mention glutamate? It seems the brain needs it to keep it’s cells alive … could be a promising target treatment …
My advice, be patient, and take your time.
Report comment
He pronounces “antipsychotics” as “an die saikau diks”. Why can’t some people learn to pronounce words correctly in more than one language? A sheltered existence? Brain damage? Fear of other cultures? Lack of time?
Report comment
He’s a twitchy fellow. Must be the synapses.
A beer belly to boot.
Oops I judged his physique.
He literally talks about the brain as if he knows its process but the cake is, he calls the process a “disease”
The question remains. Does anyone have the right to treat the thing that he knows nothing about?
Does anyone have the right to name the thing he knows nothing about?
We are still studying monkeys, ourselves. Time to get over it. The novelty has worn rather thin and the boredom set in, hence the creation of the DSM.
Report comment
neo_liberalism_say_what, many thanks for your comments! I was very surprised by the author’s implication that the rate of recovery after the first episode of psychosis is very low even if people are not on antipsychotic maintenance treatment…
Report comment
And let me add…
We are just as confused—if even more—in this current ‘modern day’ as to what mental ‘illness,’ even mental ‘health,’ really is!!!
Report comment
cidrols,
The system never was good in any way, from it’s inception it has never been about help. It never was about “mental illness”.
Report comment
Finally…
What desperately needs to be considered is that MEDICATIONS ARE MORE LIKELY EXACERBATING THE PROBLEMS OF TODAY!
Report comment
cidrols,
You have it in one. “…that MEDICATIONS ARE MORE LIKELY EXACERBATING THE PROBLEMS OF TODAY!..”
Report comment
What this Valuable Research Article seems to support is that more people recovered from ‘Schizophrenia’ before ‘medication arrived’ than after.
Report comment
Thank You Dr Joanna, this article is very worthwhile.
Wunderink L, Nieboer RM, Wiersma D, Sytema S, & Nienhuis FJ (2013):-
In this Study I believe 40% of the dose reduction or discontinuation group made ‘Recovery’, and 17% of the Maintenance dose group made ‘Recovery’.
I made Recovery in 1984 as a result of carefully withdrawing from depot medication (with the help of practical psychology). Dr David Healy was there at the time.
(I was originally ‘diagnosed’ in 1980).
Report comment
.
Report comment
.
Report comment
According to Dr David Healys Historical Research 1896 to1996 at North Wales: A hundred plus, years before the ‘arrival of medication’ a ‘Schizophrenic person’ was NOT more likely than the average person, to take their own life. But that a ‘Present Day Schizophrenic Person’ ‘consuming medication’ is about 20 TIMES more likely than the average person, to take their own life.
Every hospitalization I experienced at Galway, Southern Ireland (bar the first) between 1980 and 1984 was a ‘suicidal event’ for me. But after (very carefully) coming off strong psychiatric drugs in 1984, I experienced no more hospitalizations; no more ‘Suicidal Events’; and no more Disability.
In my estimation Dr David Healys Historical ‘Morbidity and Mortality’ Research and Dr Joanna Moncrieffs Historical ‘Recovery’ Research combined, are Scientifically Groundbreaking.
The combined Historical Scientific Research clearly demonstrates that ‘Psychiatric Drugs’ administered in ‘UK Psychiatry Today’ are NOT helping ‘Patients’, but Disabling and (Mercy) Killing them.
Report comment
Gas ovens would be a cheaper and more humane way of killing us. But less profitable.
Report comment
Everyone seemed to be eager to bring the criminals to Nuremburg, only to continue the same shit under a new name.
There were never any trials for the Bolsheviks. Pick and choose it seems, as to what is considered crime against humanity. Tsktsk at the UN to be persuaded to participate. Only act if in their eyes there is outrage by politicians. We need strong voices at the UN, unafraid to speak out against falsities.
We know from history that absolute power shifts. Perhaps it is a matter of time.
Even though I hate psychiatry for the deaths they caused to so many, it is inconceivable, the only punishment they should get is medication for the time they have left.
Report comment
Rachel777,
We know the score:- More people recovered before the arrival of medication than after the arrival of medication; and more people moved back to independence; and life expectancy was more or less the same as average.
Report comment
“While it may not live up to its own self-image as a modern and sophisticated technical enterprise, the system does, however, provide care for those who are unable to care for themselves, and containment for those whose behaviour is disturbing to others. Such people still include a mixture of those with organic disorders and psychological problems.”
Isn’t clear by now that psychiatry has nothing to do with “care,” and everything to do with destroying the lives of innocent people? Do you really want to continue to take part in that? Do you really want to continue to defend the pseudo-scientific system of slavery that masquerades as a medical profession?
Report comment
Hear hear.
How many are organically damaged and psychologically traumatized by shrinks? I’m struggling with TBI and ME inflicted on me by lying “mental health.” I am also grieving the life I will never have, isolation and poverty. I owe it all to the Mental Illness System.
I don’t want an institution. Those places scare me more than death itself.
A living Hell with doctors striving to abandon their humanity and take on the role of devils. May God have mercy on their own psyches.
Ariel Castro’s victims had a lot of problems. But no one suggested giving Castro permanent guardianship of them!
Why are articles at MIA arguing that our abusers have our best interests at heart and will take good care of us?
Report comment
They created the DSM instead of “asylums”. The labels are the admitting ticket.
What psychiatry is most busy with is constantly trying to adapt to present society.
So in that way, it names itself “medical”
Report comment
“…. I am also grieving the life I will never have, isolation and poverty…”
I hope not! I hope your life turns out very well.
Report comment
“What Can We Learn From the Asylum?”
We can learn that psychiatry is a pseudo-scientific system of slavery that masquerades as a medical profession. The sooner we learn that fact, the better.
Report comment
‘masquerades as a medical profession.”
They could never tell the truth. It had to change to medical, as human rights laws were being infringed.
“medical” is the use of labels and random chemicals.
The labels come first, after the “medical tests”
Report comment
Too true Sam
Not torture if the conduct is “inherent in or incidental to lawful sanction”. I think a study of the emergence of Mental Health Acts which are, after all, a means to exploit that statement in the Convention against the use of Torture (and enable human rights abuses) would be more valuable than the above. When did governments decide they needed to be able to torture their citizens and which ones went in boots and all. Certainly Australia’s willingness has been noted by the United Nations. But then again if one were to look at our relationship with our indigenous peoples it could hardly be called surprising.
I do hope that if Nations can be seen as being mentally ill that someone recognises a need for ‘intervention’ soon. I think perhaps an enema to remove the blockage in our political system might be a good start, and will not require the use of drugs lol.
Report comment
“Maybe the function of a mental health system is, after all, to provide care or “asylum,” while trying, at the same time, to foster people’s own abilities to recover.”
There are so many problems with this dangerous philosophy that I don’t even know where to start.
But let’s begin with the “mental health” system. There is no such thing as “mental health.” The only reason that people believe in “mental health” is because the psychiatric myth of “mental illness” is so pervasive. Psychiatry disseminates the myth of “mental illness” so effectively, that now nearly everyone has been deceived into thinking that there needs to be a “mental health” system to counteract “mental illness.” Balderdash.
The second lie is that this euphemistically termed “mental health” system fulfills the function of providing “care” or “asylum.” Nonsense. In practice, what does this really look like? It looks like the wholesale destruction of countless innocent lives, including the lives of children, the homeless, and helpless elderly people. It looks like the labeling, stigmatization, ostracism, drugging, and torture of the victims of psychiatry.
It is outright tyranny masquerading as medical care. It is, as the titles and content of Szasz’s book reveals, Coercion as Care, Liberation by Oppression, and the Medicalization of Everyday Life. It all begins with the pernicious myth of mental illness.
Enough is enough. The time has come to abolish psychiatry and to expose its pernicious myths for what they are. Psychiatry is the opposite of “care,” “asylum” or “fostering people’s own abilities to recover.”
“Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive. It would be better to live under robber barons than under omnipotent moral busybodies. The robber baron’s cruelty may sometimes sleep, his cupidity may at some point be satiated; but those who torment us for our own good will torment us without end for they do so with the approval of their own conscience. They may be more likely to go to Heaven yet at the same time likelier to make a Hell of earth. This very kindness stings with intolerable insult. To be “cured” against one’s will and cured of states which we may not regard as disease is to be put on a level of those who have not yet reached the age of reason or those who never will; to be classed with infants, imbeciles, and domestic animals.” – C.S. Lewis, God in the Dock
Report comment
Maybe the function of a doctor, after all, is to facilitate healing–instead of defaming, terrorizing, and neurologically mutilating the “patient.”
Report comment
Maybe I misread this, but is this piece actually trying to argue that there are actually benefits to the asylum? Anything being presented here is from all but the patient’s (hear prisoner’s) point of view. I’m sure those in the sex trafficking business say good things about their drugged up, imprisoned victims too, after some time in the “system”, ie. less combative and agreeable. And they give them food too.
This piece was very uncomfortable to read and had me asking myself “why?” throughout.
Report comment
To be accurate history, we need much more than a record kept by staff.
Personal accounts are not relevant since “mental illness” makes for
unreliable testimony? Is that the reason?
We have to remember that doctors consider themselves as “objective”.
In that analogy, I also am objective about psychiatry.
Why philosophy does not rip psychiatry to shreds I don’t know.
https://tomstockmann.wordpress.com/2014/12/07/opendialogue-part-2/
Report comment
“The asylum programme predates the formation of the psychiatric profession and the triumph of the medical approach to madness, so they were not intended for medical purposes, at least not as we would understand these today. What function did these places fulfil, therefore?”
But they were intended for “medical purposes”. People have called themselves “doctors” for eons. “objective observers”, “experts”….
And how do we “understand medical purposes” today?
I realize that you seem to be saying we have not made advances, and I believe you are not daftly suggesting asylums since we do indeed have them, sounds as if you come to that conclusion also.
It is good to see articles that point out the never ending failures of psychiatry and their ability to see that they are indeed NOT a “medical specialty”. I realize they CALL themselves “doctors”, and they refer to people as “patients”…
They went wrong with that all along. Big mistake, which has them now desperately trying to ‘prove’ themselves, yet dig themselves deeper.
It is the most difficult thing to come to terms with how it all went south. Unsatisfying job to keep promoting something they lost faith in.
What is worse is to keep accepting new “students”, and preaching the same droll crap over and over.
Psychiatry really should just become a philosophical field, although I doubt most would qualify.
Report comment
We already have psychology.
Report comment
Thank you for all the comments. I have read all of them but will just pick up on a couple of things. Yes, the study was a one sided view via the medical records, written by the asylum doctors. And yes, like today, their views of what counts as normal behaviour and what counts as mad are shaped by ideas that were current at the time. From the records of the national inspectorate, there were cases where people appealed their admission. I don’t know how many won and if there are any records of that- I didn’t come across any. There are some accounts by patients/inmates of life in other asylums at other periods, and some report shocking cruelty. Frank mentioned how there was an increase in the apparent frequency of madness when the asylums were built. I would agree, and the asylum population continued to climb throughout the 19th and early 20th centuries. The records I looked at reported several building programmes initiated to accommodate rising numbers of patients. Historians favoured explanation for this is that families, under pressure of the capitalist, industrial economy, could no longer care for their dependent or disturbed members at home, as they had done in previous eras (sometimes with the support of the local parish). Explanations in the 20th century may be different.
I was not making a plea for the return of the asylums, but I agree with Rachel that what we have now, for many people is ‘an asylum without walls’. That sort of system of control is more difficult to challenge and scrutinise, and that worries me.
Report comment
Thank you Dr. Moncrieff.
I really enjoyed your book The Bitterest Pills.
I felt vindicated–though privately– on learning that I wasn’t lying or delusional when I kept telling my psychiatrist that the Haldol made my psychotic symptoms worse. In addition to the seizures. He maintained that neuroleptics “never did that” and insinuated to my poor parents–also traumatized–that I was faking the “spells” I experienced at least once a day on that horrible stuff.
🙁
Report comment
Thank you so much for your follow up. When I read this, I know I had an emotional response due to my life experiences.
Report comment
Joanna, do you defend psychiatry?
Do you really believe, even after all of your research and writing, that the “mental health” system or psychiatry provides asylum or healing to people?
I’m genuinely curious.
Report comment
Your article reminds me of the Bob Dylan classic:
How many roads must a man walk down
Before you call him a man?
How many seas must a white dove sail
Before she sleeps in the sand?
How many times must the cannon balls fly
Before they’re forever banned?
The answer, my friend, is blowin’ in the wind
The answer is blowin’ in the wind
How many years can a mountain exist
Before it’s washed to the sea?
How many years must some people exist
Before they’re allowed to be free?
And how many times can a man turn his head
And pretend that he just doesn’t see – the answer
The answer, my friend, is blowin’ in the wind
The answer is blowin’ in the wind
How many times can a man look up
Before he sees the sky?
How many ears must one person have
Before he can hear people cry?
And how many deaths will it take ’till he knows
That too many people have died?
The answer, my friends, is blowin’ in the wind
The answer is blowin’ in the wind
Oh, the answer, my friends, is blowin’ in the wind
The answer is blowin’ in the wind
Report comment
WOW so perfect Redcat.
Love this.
Report comment
What we can learn from asylums is that torture centers tended to have nice architecture.
Report comment
THAT made me laugh!
Report comment
Me too. Outloud.
Report comment
“What we can learn from asylums is that torture centers tended to have nice architecture.”
A “Gruen Transfer”
In shopping mall design, the Gruen transfer (also known as the Gruen effect) is the moment when consumers enter a shopping mall or store and, surrounded by an intentionally confusing layout, lose track of their original intentions, making consumers more susceptible to make impulse buys. It is named for Austrian architect Victor Gruen, who disavowed such manipulative techniques. (from wiki)
Imagine being able to force drug people to disorient them even more, and make impulse ‘purchases’. “Would you like to add a personality disorder to your Schizophrenia today madam?”
Report comment
LOL Boans.
Label shopping. Designer labels at that.
Too bad, no designer drugs, just a bunch of random chemicals for those er um, synapses, neurotransmitters, dopamine, serotonin.
Ever see a shrink point to areas of his head when he seriously describes the different areas of the brain?
It is the oddest thing ever. How stupid do they think people are.
Report comment
Boans, I’m sure you love a good buy one get one sale like most everyone else does, I mean, Biederman knows my doc loves gift shopping at a good BOGO too… but didn’t anyone ever tell you to stay out of the Comorbidity Department? That limited time offer BOGO “sale” they have going on, well that’s just a ruse…It runs every day of the year…
And anyway, there’s a sale going on elsewhere right now…You can get a pretty good deal on a nice off-season Seasonal Affective Disorder…I checked it out and they threw in a free ankle bracelet no charge…
Report comment
Is the ankle bracelet made with little pills?
We could call it “strung out”
Reminds me of those candy necklaces. I hope I didn’t give pharm an idea.
They might just make them for kids
Report comment
Strung out…nice one! “Try our new ankle bracelets..now in neurotoxic flavor!”
Report comment
We’ve been having some trouble with shoplifters here, a few too many unintentional negative outcomes disappearing from the shelves with no effective accounting system to show where and when they’re flying out the door. Though the wrappers are being found in the morgue.
I guess its just one of the costs of doing business and surely covered by insurance. Fortunately with legislation the way it is supply is plentiful, send out the Community Nurse to snatch a few from their homes.
Report comment
Yeah we have a problem with porch pirates getting into people’s homes where I am too…
Report comment