
Mad in America is about to turn eight years old, and as we are launching a fundraising effort to keep us going through 2020, I think it’s appropriate to ask the relevant question: Are we accomplishing what we set out to do?
Here is our existing mission statement:
Mad in America’s mission is to serve as a catalyst for rethinking psychiatric care in the United States (and abroad). We believe that the current drug-based paradigm of care has failed our society, and that scientific research, as well as the lived experience of those who have been diagnosed with a psychiatric disorder, calls for profound change.
I think it is time for us to slightly amend that statement.
Ever since the American Psychiatric Association published the third edition of its Diagnostic and Statistical Manual in 1980, our society has organized its care around what I call a “false narrative” of science. APA adopted a “disease model” in DSM III, and soon our society was being told that psychiatric disorders were caused by chemical imbalances, which could be put back into balance by a new generation of psychiatric drugs. That was a story that told of a great medical advance. Yet, science was actually revealing a very different truth: of diagnostic categories that were constructs, as opposed to validated disorders; of drugs that induced chemical imbalances in the brain, rather than fixed them; and of a rising burden of “mental illness” that resulted from this paradigm of care.
The resulting social injury is vast, and the most profound injury, I believe, is this: DSM III changed the way we viewed ourselves and viewed our children, and it gave us an utterly impoverished philosophy of being. Indeed, as you read DSM III, which sought to draw a line between the “normal” and the “mentally ill,” you are struck by how its authors appear to have never read Shakespeare, or any collection of novels, or even the Bible. All of that literature tells of how we humans are subject to raging states of mind, wildly imperfect behavior, and regular fluctuations in our emotions.
And somehow the Huck Finn we admired fifty years ago has been turned into the ADHD child of the modern era.
I am not trying to discount or minimize the struggles people may experience with their minds and emotions, or the difficulties that children may experience. My point is that the “false narrative” that was sold to us encouraged us to view those difficulties through a “disease model” lens, and that is what ultimately has led us astray.
As such, “rethinking psychiatry” is too limited of a goal. What our society needs to do is create a new narrative regarding this domain of our lives, one born—I believe—from a mix of science, philosophy, and mutual caring for each other.
Thus, I think our mission at MIA is two-fold. One is to help usher out the false narrative, and the second is to help usher in a new one.
Our Operations
The scope of our efforts has steadily grown over the past eight years. Here is a quick summary of what we do:
Research News
We publish reviews of scientific findings five days a week. Our science writers focus on presenting findings that the mainstream media rarely reports on, in part because such results contradict the prevailing narrative and thus are not promoted to the media by pharmaceutical companies and professional psychiatric organizations. You might say that MIA provides readers with the “rest of the story.”
Blogs/personal stories
Each week, we publish four to six new essays and personal stories, written by an international group of contributors. These posts explore both the failures of the disease model and the possibilities that arise from embracing new narratives. Our front page also provides calendar information, artwork, and a daily round-up of interesting news and articles published “around the web.”
MIA Journalism
We are now regularly producing our own journalistic articles, which are published as MIA Reports. These reports include:
- In-depth interviews with an international roster of researchers and activists (that also air as MIA podcasts).
- In-depth investigative reports.
- Political coverage of national legislation related to “mental health.”
- Features on innovative projects or initiatives.
- Critiques of the media’s coverage of this topic.
Since we ramped up this journalistic effort in March, we have published a total of 29 MIA Reports.
Informational Resources
This past year, we greatly expanded our reviews of the “evidence base” for psychiatric treatments. Specifically:
- We expanded our reviews of the “safety and efficacy” of psychiatric drugs (with a particular emphasis on their long-term effects).
- We published informational pages on non-drug therapies.
- We published reviews for both adults and children, as the risk-benefit equation is different for children than it is for adults.
- We enhanced our drug-withdrawal resources and created a running archive of science news about psychiatric drugs.
Special Sections: Parent Resources and Veterans
We have created two new sections for parents and veterans, who are regularly targeted by promoters of the disease-model narrative in their “educational” campaigns. The new sections provide a “landing spot” for those who are newly discovering the MIA critique of that model. We have also begun hosting online support groups for parents.
MIA Radio
We have aired 29 podcasts in 2019, which have featured interviews of researchers, activists, and leaders in the psychiatric survivor community. The podcasts have turned a spotlight on a wide variety of topics, ranging from psychiatric practices among the Maori in New Zealand to studies of zebra fish that tell of possible iatrogenic effects of antidepressants that are passed down through multiple generations.
MIA Continuing Education
In the continuing education world, many programs are directly or indirectly funded by pharmaceutical companies, and they typical promote conventional beliefs and “disease model” practices. We launched MIA Continuing Education to provide an alternative to that “schooling” of professionals. Our courses, which typically are composed of six to eight presentations, have focused on such topics as withdrawal from psychiatric drugs, informed consent, open dialogue practices, and promoting system change.
MIA Global
The impact of MIA can perhaps best be seen in our growing number of global affiliates, all of which are striving to “change the narrative.” We provide web hosting services for our affiliates and some technical support, while the editors of our affiliate sites provide the editorial content. We now have seven affiliates in Europe, South America, and Asia, and expect two more in Europe to launch soon.
Our Reach
As can be seen, all of our efforts are designed, in one manner or another, to help bury the old “disease model” narrative and usher in a new narrative of a radically different kind. And each year, our audience has grown. In 2019, we expect to have more than 3 million unique visitors and more than 300,000 downloads of our podcasts. Our MIA Continuing Education alumni now number more than 6,000.
Our Financial History and Values
From 2012 to 2014, we ran mostly as a volunteer organization, with our tiny budget used to pay for our IT needs and various web hosting and software expenses. Thanks to the generous support from our readers and several family foundations, we gradually transformed into a non-profit organization that could hire people as “staff” or as regular freelance contributors.
One quick note on our values: as we made this transformation, we wanted to make sure that all felt valued, and that there would be no disparity in pay between those with lived experience and those without such experience. Thus, we pay everyone the same hourly rate.
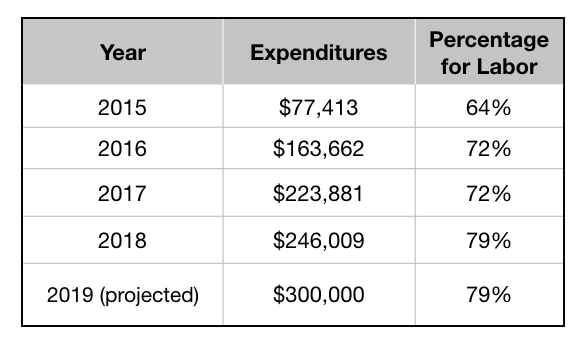
You can see in the following table that our expenses have steadily climbed over the past four years. Approximately 80% of our spending is for “labor” costs, and every person working for MIA, either as staff or as a regular contributor, is involved in developing editorial or educational content. The remaining 20% of our budget goes for web-related expenses, software, accounting fees, insurance, and a handful of other administrative expenses.
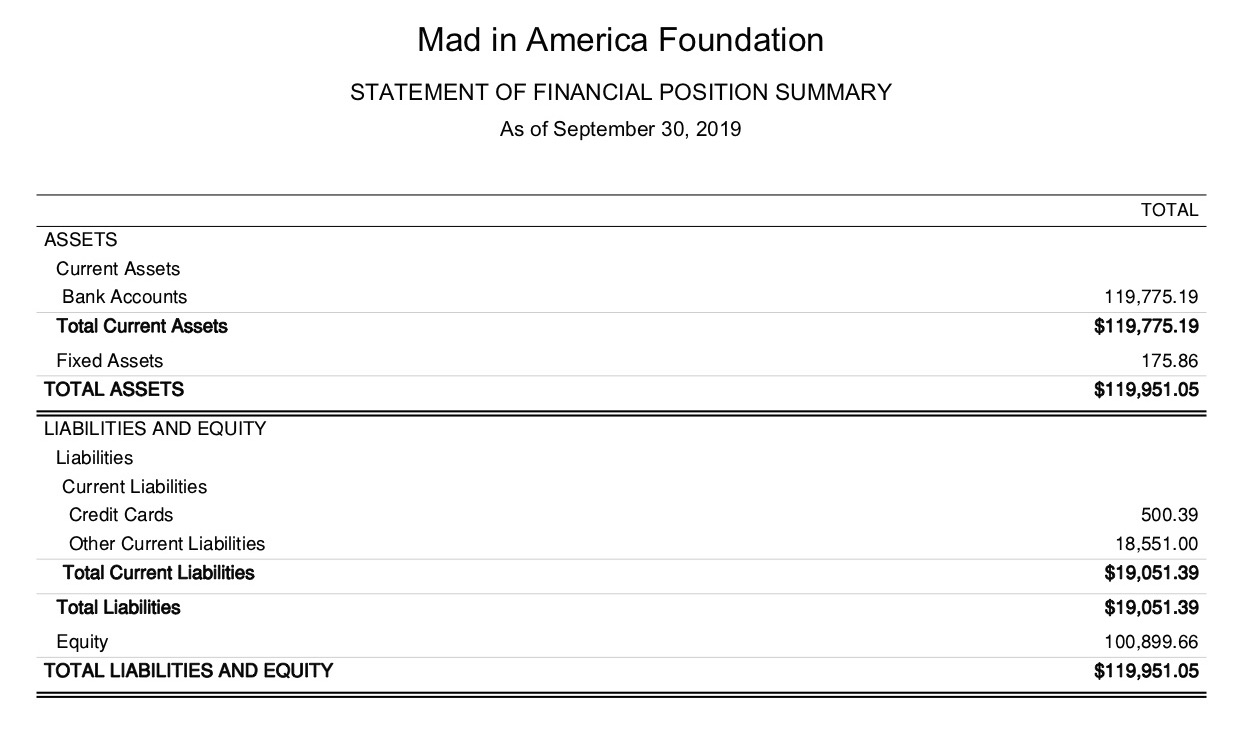
Here is our balance sheet as of September 30, 2019.
The Narrative is Changing
There are many organizations, groups, and individuals that are working to “change the narrative,” and I think it’s fair to say that MIA is the most prominent “broadcaster” of that collective effort. And this effort has morphed into a global movement, as is evident in the increasing number of MIA affiliates.
And I am certain that we are having an impact.
While it may seem that psychiatric practices in the United States and abroad remain hitched to the disease model, with the general public still believing in chemical imbalances and such, the narrative within psychiatry’s own journals and publication has notably changed in the past eight years. Even in those circles, there have been an increasing number of editorials and opinion pieces arguing for a rethinking of psychiatric practices.
The chemical imbalance theory has now been mostly relegated to the trash bin, and if you have any doubt about that, read this blog by Ronald Pies. There is a general admission in psychiatric research circles that outcomes with psychiatric drugs are poor. And with an increasing number of long-term studies finding that antidepressants and antipsychotics appear to worsen long-term outcomes, several researchers have written papers arguing that this may be because the drugs, in essence, induce chemical imbalances in the brain.
Here is how an editorial in the British Journal of Psychiatry described the “new” thinking about antipsychotics:
“It is time to reappraise the assumption that antipsychotics must always be the first line of treatment for people with psychosis. This is not a wild cry from the distant outback, but a considered opinion by influential researchers . . . [there is] an increasing body of evidence that the adverse effects of [antipsychotic] treatment are, to put it simply, not worth the candle.”
And so what are we seeing rising in place of the old narrative? The Norwegian government has ordered its hospitals to offer “medication free treatment.” Soteria homes are popping up in Israel. Open Dialogue efforts are underway in the United States and throughout Europe. And so on: the revolution is happening.
One of the leading voices for radical change is psychiatrist Dainius Pūras, the U.N. Special Rapporteur for the right to health. In a 2017 report on mental health, he argued that it was time to “abandon the predominant medical model that seeks to cure individuals by targeting disorders.” He wrote:
“The focus on treating individual conditions inevitably leads to policy arrangements, systems and services that create narrow, ineffective and potentially harmful outcomes . . . It paves the way for further medicalization of global mental health, distracting policymakers from addressing the main risk and protective factors affecting mental health for everyone.”
I know, for a fact, that Dainius Pūras and his staff are familiar with MIA, and, in particular, that they have been interested in our reporting on initiatives. You can read his report and see that we are indeed “having an impact.”
Our Fundraising Campaign
We greatly appreciate the generous support that we have received from so many this past year, and in the prior years as well. This generosity is what has enabled us to continually expand our operations.
Our goal with this end-of-year fundraising campaign is to raise $50,000. We have received a matching grant from one of our donors for this campaign, which means that every dollar donated will provide MIA with $2 of funding. Thus, if we can reach our $50,000 goal, the campaign will generate $100,000 in total funding for MIA in 2020.
And I hope that all who choose to contribute will take pride in knowing that they are helping to “change the narrative.”











{kind=link}
Hey Bob,
I’m glad to hear that MIA is growing and expanding and from your opinion, you seem to think the tide is turning: that’s very different from many other writers on this site who bemoan the lack of progress. I hope you are correct!
I’ve been frequenting this website for nearly 5 years. Philosophically, I thought I’d finally found a ‘home’ here, but then I learned I’m not really part of the in group because I’m not a survivor or a therapist and I didn’t stick my loved one in the system with horrible results. I’m just a husband who has spent the last 11 years, 24/7 doing everything and anything it takes to keep my wife’s story from being the same as most on this website. And for the most part we are thru it, together and better, both of us changed from the experience of walking it as a couple and family.
I’ve argued without effect that people in my role, the SO’s, family members and friends are the front lines in the battle. When people in mental distress begin to experience ‘extreme states’ as this site calls them, what’s a person going to do? Do they call the cops or experts? I haven’t seen anyone here teach others in my place how to deal with panic attacks, flashbacks, mini-seizures, going comatose, extreme anxiety, PTSD issues, dissociation, self-injury, hearing ‘voices’ and all the other things that typically drive them to call for help, for backup, even if it’s bad help and backup in the form of the mental health ‘experts.’ There’s not a single Open Dialogue practitioner here in Ohio: so who are people in my position going to turn to?
Maybe MIA has decided people in my position are not their core focus group, and that’s your right to do so. But I don’t see the tide truly turning until people learn how to deal with these issues on their own or have good help concretely available.
I do wish you and MIA the best,
Sam
Report comment
Dear Sam,
I think 11 years is a long time to be committed in love and in loyalty to your wife. For anyone. Congrats. There’s no competition from anyone. You don’t have to convince me that you’re the frontline, we all are the frontline. Even the teller is the frontline. And that’s part of the solution to erasing the stigma that’s been created (just to sell more solutions, billions). MIA is for everyone. Can I be forward? I’m impressed that you, as a SO, can enumerate the different symptoms of your SO’s distress, as occasional or as permanent as it may be. Just the fact you can name them tells me you know a little bit more than I do, for example. You could probably teach me – if you know what I mean. Why don’t you consider that. Maybe you know a little bit more than a few bozos (on benzos). A few years ago, when I was way young, I read a book called “Don’t Panic” by Reid Wilson and it changed my life. I don’t know what the person I have become would read today in the same book but when I was young – it changed my life. My point is: this site does mention a lot of alternatives to traditional North American care. Use teh “search” tool. It doesn’t even have to be open dialogue. I’m sorry I took so much of your time. I think I wanted to say “I applaud what you do”. Buy a surf board too because the wave is moving to a town near you Ohio. Take care. (Written with respect.)
Report comment
Sam I think it is great what you are doing and have done for your wife but I don’t understand your negative comment here at all. That is precisely what Robert and MIA is all about, making an immense effort to call for changes that will actually support and help people to “help” those in distress, altered states etc as currently there is no other place than psychiatry to turn to in an emergency or try get what would be considered real “help”.
I wish people would be more appreciative of the immense work that Robert has been so dedicated to.
Report comment
Sam Ruck, this is typically how clients can feel actually going from shrink to shink–dismissed, not heard, on the outside, and that IS the front lines, right on the line of battle.
My question is always, why is this a battle? Should be a healing partnership. Although professional boundaries do not allow for the intimacy needed for this kind of healing. This is why that paradigm does not work, it’s always lopsided and is high risk for the client.
What you describe between you and your spouse is the same way my partner and I have a healing partnership. Over the many years of our evolution in life we’ve supported each other at different times, going through breakdowns and subsequent integration. We’ve both been through our shadow journeys, more than once, then back into clarity after doing the inner work. We’ve been back & forth with the roles of needing the support and being the supportive significant other, so I know of what you speak, and you are a wonderful example of what the world needs more–that is, you recognize your own healing as you support your wife, it is not one-sided healing.
Indeed, everyone grows in the process, or at least that is what should be happening. Otherwise the same old power struggles continue as well as the scapegoating, and that’s the problem at the core, from what I can gather, keeps all the divisiveness in place, status quo. Love motivates us to go the distance, to be creative, patient and innovative and stretch ourselves. That is the only way I know how healing and personal growth can occur!
I don’t see how this can truly come from professionals. This needs trickle into humanity at large, in our personal and community relationships. That is where we expect love and support, without a price tag. And it just doesn’t seem to be there enough, and neither is the trust. Society is healing from mass betrayal, it would seem.
You’ve shared valuable information regarding healing from your own lived experience and I believe it is highly respected and your work is admired. I’m no fan of the diagnoses, but I do believe that everyone’s experience counts. We’re all different and this is about the greater good, so everyone’s perspective needs to be taken into account equally for any movement against injsutice, oppression and marginalization of human beings to be authentic and powerful enough to create change away from these. Change begins with being an example of it. Thank you for the wisdom and experience you bring to the table.
Report comment
I fear our mental health concerns are much wider and broader than just focusing on “mental illness”. We are a society that is burning up, not only climate-wise, but psychologically. The “burnout” rates of all kinds of workers is rising, as well as parental burnout. The highest rates, perhaps because of systemic issues, is that of human and animal physicians. I suppose this is some sort of offshoot of not only the biological model, but how even that is blocked from whatever efficacy it can provide. Then there is the rising xenophobia and all the related discriminated against groups. We need a much broader mental health mission as far as I can tell.
Hey-Hey
Report comment
Thank you so very much for the article and the facts. I would love to see the day where the facts can be presented to the public in general, where we as a whole, the truths and philosophies of groups such as MIA have as much clout within the public sector to educate and make aware the myths that are paraded around as truths. It is the DSM that has to be seen as a mistake in history, a feeble attempt at explaining the unexplainable. If we make up theory it is no better and often worse than no theory at all. I have no interest in seeing a DSM rewrite. It is past cooperation with the psychiatric system and simply calls for a revolt and attempt to lessen their grip. I see no other way than to establish in the least another system besides psychiatry. If they will not admit, remove the bogus material that they use to indoctrinate, ruin people, then the choice is to become loud and present our own system. We will get there I believe. I have been lax about money, yet no system can operate without funds, so I will be sending my however small contribution. I always knew something was inherently sinister and dark within the psychiatric construct and I searched online where I found others of like mind. Psychiatry keeps repeating over and over the same mistakes, how anyone cannot see that psychiatry makes NO ONE better, rather makes people ill, on so many levels. Helpful systems have absolutely no interest in using descriptors that harm people on a psych-social level. As I said, I doubt we can change them, perhaps we can become stronger and tougher, exposing myths. Keep on doing what you do, and thanks.
Report comment
To RW and All the MIA Staff
There is much to celebrate in what MIA has accomplished over the past 8 years. MIA has become a powerful force on the internet and within our society exposing the overall oppressive Medical Model, and the particular role that psychiatry and Big Pharma play in promulgating that model. It also offers many empathetic alternatives for those needing emotional and psychological help.
I am heartened by RW’s and MIA’s willingness to continuously re-evaluate its mission and role in the struggle to end psychiatric oppression, and to establish a new narrative about the emotional and psychological difficulties of human existence.
And I do very much appreciate that RW, both solicits and responds to, the sometimes contentious and controversial views of the MIA readers and followers. In particular, the fact that the term “mental illness” was placed in quotes by RW represents part of this important evolution and growth of thinking that has taken place at MIA.
In conclusion, I want to say I support the changes and evolution in the MIA mission statement. I will add the following comments about the nature of our current society and the struggle to overturn the oppressive Medical Model:
While there has been progress in changing minds and gathering forces to oppose all forms of psychiatric oppression, we must be brutally realistic about what it will actually take to end the enormous harm done by the Medical Model.
Psychiatry, Big Pharma, and its related “genetic theories of original sin,” and its increasing role in society as a form of social control, has become TOO BIG AND IMPORTANT to the POWERS THAT BE, to be allowed to fail.
So what is likely to develop in the coming years is A VERY POLARIZED DIVIDE on the narrative questions that MIA has definitively staked out territory clearly on one pole. That is, a humanistic and empathetic understanding of human psychological distress as intimately connected to the daily stress related to social inequality, injustice, and trauma emerging out of a class based, profit driven economic and political system.
On the other side of this very polarized divide, stands deeply entrenched psychiatry, Big Pharma, the capitalist ruling class, and all those people in society who have consumed (often out of fear) the Medical Model narrative of chemical imbalances, genetic defects, and human psychological flaws as the explanation for why there is social inequality and enormous human angst in the world.
This type of divide I am describing is very similar (and in many ways connected) to the current divide in the U.S. over summing up the role of Donald Trump as a so called “fascist threat,” or as a “savior and protector of the glorious U.S. Empire.”
This system we live under, with its vast “market place of ideas,” can tolerate sharp political divides (like those over the Medical Model and Trump) for certain periods of time. But these types of political divides WILL NOT ultimately be resolved through a mere EVOLUTION, or just gathering more forces who accept the “new” narrative.
These sharp political divides I am describing must ultimately be resolved through major systemic change in society. Here I would argue that this will require replacing our current profit based/capitalist system with a new type of socialist model.
Whether or not people believe this is possible (or have other ideas for big solutions), please DO NOT be lulled into thinking that these major type changes related to the oppression of the Medical Model, will GRADUALLY CHANGE through slow evolutionary growth. This type of thinking is not only very unrealistic, but also extremely dangerous.
Any serious look at what is going on in the world tells us that “power concedes nothing without a struggle.” And psychiatry, Big Pharma, and other ruling class forces in society who DIRECTLY BENEFIT from what the Medical Model provides to HELP maintain the status quo, WILL NOT simply rollover and give up because we have the “facts” and significant forces gathered on our side.
We have a long and tortuous struggle ahead, and I am convinced that MIA can play a significant role in this struggle.
I salute MIA and its staff – keep up the great work. Dare to Struggle, Dare to Win! I already give a donation every year to MIA, but I will now add an additional one hundred dollars to the cause. Carry on!
Richard D. Lewis
Report comment
Richard I agree. great post.
Report comment
A decent analysis by Richard, particularly the second part which sums up the general state of affairs in the U.S. However the devil is in the details.
Report comment
“Psychiatry, Big Pharma, and its related “genetic theories of original sin,” and its increasing role in society as a form of social control, has become TOO BIG AND IMPORTANT to the POWERS THAT BE, to be allowed to fail.”
Hey Richard, good to see your still pointing out such truths. I received a letter from our current Minister fo Health stating that he was saddened that I was still upset about my detention and referral after such a long time, and that I should seek professional help. I replied and told him that the greatest difficulty had been in having folk recognise that I had not been referred and detained, but tortured and kidnapped. Making me into a “patient” post hoc via fraudulent documents and threateneing witnesses doesn’t change the truth. But where would he be without the dog whistle slandering of folk who say things he doesn’t want to be true. Seek professional help, from who? The people who tortured and kidnapped me? Yeah right. Talk about false narratives? “Cover not the truth with falsehoods”
Problem for me has been all these folk who claim to want this to change are not prepared to take these matters on even when a win would be a forgone conclusion, precisely because of what you state. They run away from the fear of the ‘morality police’ who can snatch you from your bed and for no other reason than they want to leave you dribbling in a cell and call it medicine. Can’t say I blame them, history shows this as being how humans respond to such periods of National Socialism and Democracy (oh how I laugh after what I’ve seen the State do when I hear I live in one). The failure of folk to stand up when required is our greatest enemy I think. And enter MiA at that point.
As far as MiA goes, great work. Can’t say I agree with everything I’ve seen here but at least the area is open for discussion, which can not be said about most places where any deviation from the mantra will be dealt with more swiftly than a gay person in Raqqa. And let’s not forget some of the purposes psychiatry has been seen as ‘fit for’.
Report comment
I mean imagine, what sort of place would allow a private clinic psychologist to arrange the torture and kidnapping of an ex client (note not a “patient”) and allow the use of police resources to achieve this end and then when a complaint is made, access to legal representation is denied whilst they arrange to have the victim unintentionally negatively outcomed.
Seems that whilst our laws contain ‘protections’ they are easily overcome with negligence, fraud and slander. And then our Minister for Health tells us that whilst he ignores the protections in the Mental Health Act, he promises this won’t be the case with his Euthanasia Bill if they pass it for him.
Don’t believe me about the denialof legal representation? Think I haven’t tried over 8 years to have someone look at the proof? And all I have is a long list of the most incompetent claims i’ve ever seen. My doctor authorised the ‘spiking’ but when I ask what doctor I am not allowed to be told for reasons of National Security lol. And nothing more disgraceful than Police being so under resourced they don’t even have a copy of the Criminal Code.
A land of Sweeping Plains? I’d be real careful visiting this place if your of a mind that psychiatry shouldn’t have the powers it does, find yourself food poisoned and shipped of for ‘treatment’ before you get out of the airport. And there aint no lawyer going to help, they can threaten them to inaction with a telephone call.
A State that is acquiescing their duty to citizens (human and civil rights) and allowing the most vile conduct to be passed off as ‘medicine’.
Absolutely right they are not letting go of that without a fight Richard. Police have been given instructions to do what they are told by doctors and excercise their ‘discretionary’ regarding criminal conduct and well, I can’t see that ending well. But there is a War on against that sneaky mental illness which as was show in my case is there one minute and has disappeared when the drugs i’d been spiked with wore off. Luckily their attempts to have me injected with enough for an elephant failed, though I note in most cases they suceed in this endeavour. Ask the patients, oh wait, Minister says “you can’t listen to them, they’re mental patients”.
Report comment
hope you are right, and that we are going through peak psychiatry now, while we work with others to reframe the narrative so their defeatist and destructive views decrease rapidly all over the world
Report comment
Eileen, Psychiatry came about through a belief system regarding those people over there, the ones that act funny, or think funny. As in a schoolyard, they found others who delighted to talk about those ones over there. Eventually instead of whispering, they began to experiment on this behaviour, on this being, or they confined it for life. Back then families were afraid of psychiatry, after all they were doctors with scalpels and saws. They wore white coats and spoke with authority. People then started to go voluntarily because realistically the prospect of living in a chaotic world is difficult for some. By now a few had piped up about lifelong incarceration and lobotomies, so they created a pill and more pills that continued to hurt people. This was really not very long ago in the realm of things. Changes keep happening. It really is not so okay anymore to incarcerate or subject people to treatment. People are watching and talking. We have human rights, which are not working at their optimal and is another area that needs to be addressed. Change never happened quickly, but eventually it does. I am sincerely hoping that psychology could and would be brave enough to help it along, but it seems they like to cling to their own construct and keep their jobs.(PSST< ALL YOU PSYCHOLOGISTS) I really want that DSM gone, and the lies and theories about meds. It seems a no can do, but to adopt that thinking, then we are going by the fact that things don't seem to be changing today. WE, US, just like the psychiatrists have to stick to our belief systems and spread it around like butter on bread. Trust me, I know 3 women on meds, and we talk psychiatry. They hate it, yet buy it. But, I don't care, I plant a seed. I won't see a massive eureka moment in my lifetime, where the DSM is removed, Look at the changes and keep hope. Psychiatry is very aware they are hurting people and very aware that people are noticing. I spoke to a counselor who has a psychiatrist friend and the psychiatrist had told her that the practice is on it's way out. One thing that will never leave society is desire and need. There will always be those who seek to have control, but more and more we the sheep want some too. We are demanding autonomy. The numbers of people that are aware that to a degree we are by birth entitled to autonomy just like the next guy, is becoming pretty darn huge. Abuses will just not be okay anymore.
Report comment
Removed for moderation.
Report comment
I’ll contribute. Simply put, when I’m having a “bad day”, I come here and read a few articles and comments and usually, I feel better. Simple as that. No drugs, no dope, no booze, no soda, no cigarettes….just a little reading. It’s worth it. Thanks for your great sight.
Report comment
To Robert and all MIA staff,
As Richard Lewis noted, MIA is a powerful force and has many accomplishments to celebrate! Congratulations and thank you to all the staff at MIA for your dedication to this profoundly vital mission!
A huge thank-you and much gratitude to Robert Whitaker for starting and staying with this challenging humanitarian mission. This mission is extremely helpful and validating to those harmed by psychiatry and is helping to save children from falling prey to the same fate. It is also an acknowledgement of those who lost their lives tragically due to the harmful narratives and protocols of psychiatry. In my eyes Robert is truly the epitome of a hero and deserving of a humanitarian award!
I regularly read the Psychiatric Times and Lancet Psychiatry and am heartened to see the tone and narrative is changing there and in other venues as well. MIA played a huge role and surely is the most impactful and “prominent broadcaster” of that collective effort.
As Robert noted…“Thus, I think our mission at MIA is two-fold. One is to help usher out the false narrative, and the second is to help usher in a new one.”
Yes, I think it is great to now expand the MIA mission past “re-thinking” psychiatry. Until I tangled with a psychiatrist while in cancer treatment I was unaware of how utterly pathetic and damaging the narrative and protocols of psychiatry was. Psychiatry definitely needs to go. We need an entirely different concept to actually “help” instead of punish humans when they face crises or get overwhelmed by the many challenging stressors we all face at one time or another in life.
This huge MIA mission certainly needs funds to operate and I hope anyone who can make a donation of any amount will do so. I donate every second month and also plan to do as Richard noted by adding extra at year-end to help keep the MIA mission going. As well let’s all keep spreading the word and the link to the MIA website to keep growing this mission.
As a side note, I am on chapter nine of Anatomy of an Epidemic and it is mind-blowing information. This book should be required reading for every doctor and “mental health” professional!
Report comment
I recently sent a few links from here to former classmates who have been practicing psychotherapists for over 15 years now. They had witnessed my breakdown 20 years ago from years of being on psych drugs, and they also know how I was finally able to heal and transform my life after coming off the drugs, painful and rugged as that withdrawal was. They also know that I turned to other methods of healing outside of the mh industy. They had no idea there was controversy around any of this, much less a movement. At least they’re aware now, but they continue to snub me and this information.
This is exactly why I condemn this industry. Issues such as lack of communication, lack of trust, lack of staying informed, lack of acknowledging either scientific evidence or personal testimonial, anything against the programming is suspect, denied, and causes anger and ultimately, some kind of stigmatizing projection, can’t seem to get around it.
What also lacks in this industry is common sense, that’s been overtaken by these false beliefs about people. Disagreements becomes personal and can get rather nasty as all neutrality is lost, and supporters of this industry can become downright mean in the process, casting shame where there is dissent, creating scapegoats. It’s cultish, very scary.
This is why sitting in a chair opposite a clinician in their office can be so dangerous. Our voices do matter and truth is ultimately more powerful than illusions, but it is indeed a never-ending struggle to get the truth heard in this industry. It functions in denial and resorts to cheap shot projections to keep the light off so that people will stay in the dark. Undue suffering is the result of this.
Keep going, this industry needs a good hardy awakening which it has been resisting vehemently at all cost. I would love to see that ridiculously low glass ceiling shattered to bits. It is absolutely toxic.
Report comment
Alex, they snub because they do not want to see. They most likely feel ashamed of living the lies, and we do everything we can to protect the industry. The churches, ruled forever, however the majority now chooses to believe what they consider their truth.
Report comment
Yes, I agree, and while that might be understandably human on one level, it is also a huge red flag, when you consider why most people go into therapy in the first place. How much of the client and their personal truth will the clinician “not want to see?” Insert projection, judgment, stigma, counter-transference, whatever you want to call it. This is where great harm is done, and it goes unnoticed, which is why I am highlighting it here. This is where the shame gets projected, rather than owned, and it is passed back & forth like a hot potato. I think that’s where things can get stuck.
Everyone makes mistakes and has had regrets, that’s just part of the human experience, how we learn and accept ourselves on a deeper level. Plus we all come from programming, and healing is about facing our shadows with courage, humility, and self-compassion. That, alone, moves us along in a big way, toward clarity and wholeness. As humans, we ALL have the capacity to forgive ourselves for past mistakes and make amends by waking up and getting our heads out of the sand, to start with. It’s never too late to take that first step, and then we’re on a healing path, things will change and we will grow.
I am enjoying your truth, sam plover, wonderfully insightful posts!
Report comment
Alex, It is amazing how we inadvertently walk through those doors. It helps to have a healthy dose of ‘oppositional’ ‘defiance’ and ‘avoidant’ disorders. And thanks
Report comment
I not only asked to be diagnosed and drugged (I was extremely programmed and believed at the time this was the responsible thing to do, the only option of which I knew at the time, so that I could stabilized my anxiety and go back to work) but I also eventually went into the field. I was REALLY asleep to the truth, believed in all kinds of insitutions from how I was raised.
It was through a series of encounters in grad school with professors and other students, and in my training with supervisors, and the negative effect I could feel these were having on me, that I learned about “energy suckers” and, eventually, “toxic psychiatry” because by this point, I could tell the drugs were destroying me from the inside. That was my “aha!” and it led to awakening, coming off the drugs and ditching any diagnosis because I could see easily by this point that these are made up and meaningless and it had nothing to do with me or who I was in any way, shape or form, and I went in an entirely different direction in perspective, beliefs, and new practices. Major life transformation happened as a result of this change in perspective.
I had felt stupid and duped for a long time for believing in all of this and falling prey to it, and wondered if my life had been ruined forever, really angry at these maliciously arrogant and rather mean-spirited quacks (which I discovered when I questioned their perspective about me), as I went on to heal the multiple injuries from this experience, now that I knew what had caused them. I found a good healing path for myself, thankfully.
Plus this experience did wake me up to what caused my extreme anxiety in the first place, what led me to seek help. The socially divisive and marginalizing mindset reminded me of my family. Yet another, “aha!” Painful awakening, but truth nonetheless. I had to deal with it and grow from this by individuating from toxic communities and seeing myself apart from these, not participating on that level and not allowing myself to be a victim any longer, while owning that I had put myself there in the first place. It was my journey to take.
Now I am awake and my life is different than I would have imagined. It is not a product of programmed beliefs but instead, it is a reflection of who I am, that’s the idea, and I own it and am now in full control of it once again, as my whole self. No regrets, it is life education. Advanced course!
Report comment
At Tim McCarver once said, “They should call it ‘uncommon sense,’ because if it were so common, more people would have it!”
Report comment
Ha! And while I see the logic in this, I’m referring to the fact that these taught ways to view humans and the human experience–the programs which lead to all kinds of “models of being, behavior, thinking,” etc. which are applied in the mh industry and field of pscychology–are simply false and irrational, pure ivory tower. They are illusions which are divisive and which create a false hierarchy of power, while defying logic and disregarding and dismissing all kinds of evidence–and people!–which is why the industry is an unequivocal mess and making more of it in society. This perspective, including the subsets of the overall psychological perspective of being human, should not be the standard. It obviously does not work to bring truth, clarity, healing, or balance to the world! On the contrary, it brings chaos, conflict, chronic issues, and marginalization.
So, using this phrase in a sentence now as I intend, I would believe that common sense says go by the evidence–I can’t imagine anyone saying it should be otherwise–and yet hard evidence and personal truth are blatantly ignored and vehemently denied, causing stigmatizing labeling to occur instead, that’s the m.o., which is the essence of dehumanizing.
Common sense also would tell me that this is the trouble here and a huge roadblock to progress, and yet it is perpuated time and time again. Therefore, what I see from this is lack of common sense. But you’re right, and sadly, it’s not so common here. The programming is thick and dense, makes things very challenging. It’s quite a process to go from programmed to truth–the healing journey, in fact, to wake up.
Report comment
The idea of common sense suggests that a person with little to no education should be able to see the truth in it intuitively. I truly believe this is the case when it comes to understanding human beings and what we need from each other. Too much training, as you say, creates more and more confusion, because they’re making things more complicated than they really are. And then we get weird studies showing that “racism and oppression increase mental illness symptoms.” Gosh, who knew? It really isn’t that complicated, though it requires courage and willingness to experience intense feelings to fully understand, and that’s where a lot of “professionals” fail.
Report comment
Yup, well said, Steve. The more we live, reflect, and share with and listen to others, the more wisdom comes to light and unfolds naturally. Life educates, trains, and brings opportunities to apply it all, see how we’re doing. And on and on, learning as we go.
You’re right, it’s not that complicated, and I agree also that the wisdom is found in the feeling of the experience, that’s the gold. Sometimes. however, life just thrusts us into it and we find ourselves feeling the challenges, can no longer avoid it. It’s very often not a conscious choice, life just happens. That’s when the journey of healing and awakening really begins.
Report comment
See the “naive psychology” of Fritz Heider. And this would leave a psychiatrist/psychologist attributing behaviours to ????? Uncommon sense?
Report comment
I agree, Alex, Sam, and Steve. “Issues such as lack of communication, lack of trust, lack of staying informed, lack of acknowledging either scientific evidence or personal testimonial, anything against the programming is suspect, denied, and causes anger and ultimately, some kind of stigmatizing projection, can’t seem to get around it.”
I have the medical evidence there’s lots of projection of doctors’ “dangerous paranoia” onto an innocent patient, to proactively prevent a non-existent malpractice suit, and cover up a “bad fix” on a broken bone, by the PCP wife of the “attending physician” at the “bad fix.” Not to mention proof of gas lighting by a psychologist who wanted to profiteer off of covering up the abuse of my child, for her pastor, according to her medical records, and my child’s medical records.
I totally agree, “What also lacks in this industry is common sense, that’s been overtaken by these false beliefs about people,” and their “invalid,” BS DSM stigmatizations. Our psychiatrists incorrectly believe common sense is “millions of voices,” rather than a rational internal voice of common sense or reason.
I agree, all our “mental health” workers should “feel ashamed of living the lies, and [they] do everything [they] can to protect the industry. The churches, ruled forever,” and the churches are in bed with the DSM “bible” believing “mental health,” primarily child abuse covering up, profiteers, unfortunately. They’re even teaching the DSM “bible” theology in the seminary schools today.
“They should call it ‘uncommon sense,’ because if it were so common, more people would have it!” I hope most people have it, but I do agree, the “mental health” workers do not have common sense.
Thanks to MIA for what you do, it’s very important. Thank you for letting us work together for a much needed paradigm shift. I’ll try to get a donation in during the donation matching period.
Report comment
I believe the paradigm shift is that we are working together, inherently, that is nature. We’re all connected, one person’s energy affects others, and so on, rippling into the collective. Clients and therapists, for example, are mirrors of each other and are easily interchangeable, as far as “playing the role” goes. Each can influence and affect the other in a variety of ways, positive and negative. The titles, degrees, and suits are merely illusions of separation, with a false premise of what is, in reality, true personal power vs. control & manipulation of others. How we present in the world and who we really are can often be a great divide. Being authentic is what I consider to be courageous.
Report comment
Removed for moderation.
Report comment
SomeoneElse…..you are so right that the DSM is being adopted by sects. some years ago when I again felt I needed ‘professional help’ (looking for insight) I looked online in my city and did my research to try and find someone far removed from psychiatry. I looked at literally hundreds and I don’t know how often I saw they got their degree from religious institutions. Wow so many out there, willing to help for $150 per hour, so willing to listen authentically.
Report comment
Yes, Sam, the mainstream religions were co-opted by the “mental health” workers long ago. They’re actually teaching the DSM “bible” in the seminary schools today. It was actually confessed to me by an ethical pastor that this systemic, for profit, “conspiracy” against abuse survivors, by the religions and “mental health” workers, is known as “the dirty little secret of the two original educated professions.”
Report comment
Thank you Robert Whitaker and everyone else at MIA.
Without the support I found here (and also SA which I heard about through this site) I could not have come off my drugs due to the debilitating withdrawals after 25 years of being the “perfect consumer.”
The scariest decision I ever made. But worth it.
Report comment
At this time of reflection, I salute the community service of this website and its evolving mission statement!
Report comment
The Envoy of Mr. Cogito
BY ZBIGNIEW HERBERT
TRANSLATED BY BOGDANA CARPENTER
Go where those others went to the dark boundary
for the golden fleece of nothingness your last prize
go upright among those who are on their knees
among those with their backs turned and those toppled in the dust
you were saved not in order to live
you have little time you must give testimony
be courageous when the mind deceives you be courageous
in the final account only this is important
and let your helpless Anger be like the sea
whenever you hear the voice of the insulted and beaten
let your sister Scorn not leave you
for the informers executioners cowards—they will win
they will go to your funeral and with relief will throw a lump of earth
the woodborer will write your smoothed-over biography
and do not forgive truly it is not in your power
to forgive in the name of those betrayed at dawn
beware however of unnecessary pride
keep looking at your clown’s face in the mirror
repeat: I was called—weren’t there better ones than I
beware of dryness of heart love the morning spring
the bird with an unknown name the winter oak
light on a wall the splendour of the sky
they don’t need your warm breath
they are there to say: no one will console you
be vigilant—when the light on the mountains gives the sign—arise and go
as long as blood turns in the breast your dark star
repeat old incantations of humanity fables and legends
because this is how you will attain the good you will not attain
repeat great words repeat them stubbornly
like those crossing the desert who perished in the sand
and they will reward you with what they have at hand
with the whip of laughter with murder on a garbage heap
go because only in this way will you be admitted to the company of cold skulls
to the company of your ancestors: Gilgamesh Hector Roland
the defenders of the kingdom without limit and the city of ashes
Be faithful Go
——————————————————
—————————————————-
https://www.youtube.com/watch?v=XQEGoO67PUM
https://www.youtube.com/watch?v=HY-vp_YcnjY
James Hillman – “Re -visioning psychology”.
This is an answer, it is not mine, it is from the victims of the psychiatry.
Report comment
MAD and it’s website have come a long way since I discovered it back in 2014 while researching the Internet for information about my vast array of physical and mental problems that were added to my life, problems VA psychiatrists, psychologists, nurses, therapists and M.D.’s were failing to address and accept as resultant of prescribed medications.
This year, I will give a donation in appreciation for everything Mad in America and Robert Whitaker have contributed to my greater understanding, and to others, of human behaviors and conflicts that produce mental and emotional dis-ease with themselves and towards others.
Thank you all, for everything you’ve done to inform the public about the myths that were held too long in psychiatry, and for introducing new treatment approaches and humanistic paradigms. Kudos to the writers for their well-written articles which Mad in America has published over the years.
Jane Reoch
Report comment
I earn 250$ a month but l will continue to give to MIA in the new year as it is very important work that you do.
Thank you for your efforts and your truth telling.
Report comment
Robert, what you have involved yourself with is a testament to your integrity. You have personally changed people’s lives for the better. I am very honored to know you and the many who make this site possible, the commenters included. Your words, your knowledge, facts and understanding are extremely important and valuable on a global scale. I realize I made a comment already, but I watched several of your videos and had to return. And with that, I am very aware that education needs funding. Your education is fundamental for parents, would be parents, teachers, and the children. I really would like to see children educated in that their feelings and/or behaviours are not brain disorders or disease. In the least to present both options. For psychiatry to be allowed to present ONE model and with unfounded material should be illegal. People often do not have the ability to think through what is presented to them, and if told that these meds here work, it’s not as if they think “hmm well, if it’s serotonin, how do they know I’m lacking it, and what test is there to see if my numbers of serotonin are now perfect?”, or “hmmm, if this pill seemingly settles a person down, is it really settling or making them unable to react… what else is it doing in an area that science knows zero about?” People seem to think that because science creates a drug, it is some magic pill that targets one minute particle. They have no clue that the brain is who you are, that indeed that pill is circulating throughout every cell. And that the brain is vaster than space itself and psychiatry depends on people not being curious, and if you are, then you are paranoid. Psychiatry is just too ridiculous to be believable, it is purely a matter of more education to expose their pretenses, lies.
Report comment
“HUGS, NOT DRUGS” Trouble with the Mental Health Professionals I met is that they would interpret this in their unique way and think that it could be perverted into strangling someone in a cell and calling it a HUG. In fact, let me dig out that report into the people who had their necks snapped during restraints, the one about the unintended negative outcomes. Oh I see, Humane Undersupply of Gas for Service-users – HUGS lol.
One of the biggest problems I see, and i’m unsure if this is the same in America, but that the Minister is immune from prosecution. Thus if they give the green light to something, for example the use of torture, then basically that immunity runs all the way down to the cleaner beating the “patient” with a broom in the seclusion area. Not a damn thing you can do about it because the immunity is seen as being part of the ‘clinical team’. Mind you the use of torture does have the clause which says there is “no superiour authority” but ineffective investigation and cover ups are just so cheap and easy to do with hot shots in EDs
Report comment
Hugs=straight jackets.
Get Big Pharma to mass produce those. And get the marketing/propaganda agents to work.
Publish a bunch of articles on various sites and magazines. “Science Has Shown Therapeutic Value in Straight Jackets!” “Straight Jackets Now Proven Highly Effective for Depression and Anxiety!” “Straight Jackets Valid Modality of Treatment for ADHD!”
Real SCIENCE folks. 😀
Report comment
(The sound of sirens) P.C Police
They’re called hetrosexual jackets these days Rachel777
🙂
Report comment
HAHAHA
Report comment
Over 70% of the US population is overweight, so all is fine as long as they aren’t narrow jackets. 😀
Report comment
Regarding “rethinking psychiatry”, I do not believe it necessary to create a completely new narrative, as it already exist another narrative. However, this narrative is not well established in the Anglo-American world. It is the narrative of education and educational science. In the Anglo-American world, education is conceived in relation to schools and teaching and educational research is seen as the study of this conception by other disciplines; including psychiatry if necessary, wherease education in the continental world is an independent scientific discipline with different branches and a much broader field of view than schooling and teaching. As such, it serves as an alternative narrative to the discipline of psychiatry, seeing the same audience and problems from educational perspectives with educational solutions – including educational perspectives that is built upon an ethics of mutual caring for each other. So in “rethinking psychiatry” and broadening the goal, considering the continental discipline of educational science in its totality as an alternative narrative, in addition to others, may be profitable.
Report comment
HI Bob, Congratulations on all of the fine work that MIA is doing, and I have no doubt that you are having an impact for the better. This site publishes so many thoughtful and well-researched articles, and there seems to be no end of the variety of topics that are covered. And while some people are convinced to make a change once they learn facts, others need a combination of facts and personal stories, which you provide as well.
I’m happy to read that the major medical journals are publishing pieces that challenge the old narrative, but in my dealings with friends, I find that kind of information hasn’t filtered down to the average person yet, nor do I see much of the new narrative in mainstream media.
While the chemical imbalance narrative may have the sound of being scientific, its utter failure to deliver should render it powerless. I take comfort from the work of Masuro Emoto who wrote Messages in the Water. He talks about the idea of morphic resonance and how if something is happening in one part of the world, that energy makes it possible for the phenomenon to happen somewhere else. For example, if “medication-free” treatment is possible in Norway, it’s possible here as well. MIA is helping to build the critical mass that is moving us inexorably to a tipping point where great change can happen. I’m happy to contribute to the fine work everyone at MIA is doing. As I’ve told you before, your book saved my life, and I’m sure countless others as well.
Report comment
Ann Bracken, lovely comment. Indeed just as psychiatry spread and is trying to infect globally, so can anti-psychiatry spread.
Report comment
Removed for moderation.
Report comment
Thank you all for your comments, your encouragement, and for your support of MIA. At a community level, this is a David and Goliath struggle, but David, so to speak, is making progress.
Report comment
Apparently my intended statement of support, which contained a critical analysis of the “anti-biological psychiatry” approach, has been deemed unsupportive. I guess this is a conversation for another day. However lest my absence from this thread be misinterpreted I will repeat my closing statement:
The level of consciousness about psychiatric oppression evidenced by those who write and post at MIA is unparalleled when compared to society at large. MIA helps people make valuable personal and theoretical connections, and deserves support on that basis alone from those who are able to offer it.
Report comment
A quick note of thanks: I am so appreciative that MIA exists, takes psychiatric survivor issues seriously, represents a number of viewpoints, seeks to operate with integrity, and effectively reaches the public. In the earlier days of the internet, I remember Furious Seasons and The Icarus Project as the only refuges I could find for thinking critically about mental health and society. MIA has stepped into a huge need, bringing critical analysis to issues that otherwise cruise by. Y’all are doing important, incredible work, and I look forward to what you continue to grow into.
Report comment
Bob, it was your Mad In America book that gave me the knowledge I needed to muster the determination to get off the drugs. This month marked three years pharmaceutical free for me. December will be 6 years since my last (overnight) hospital stay at JHU Mood Disorders Unit, where they removed my bipolar diagnosis and replaced it with MDD. It’s been 9 years since my last actual hospitalization for more than one night. My diagnosis was further downgraded last year to PTSD and Mood Disorder Due To a General Medical Condition, reflecting my ongoing struggle with Lyme Disease and coinfections. I embrace these only as they help me get my basic needs met – specifically my service dog. I don’t know where I’d be right now if it were not for the information and support I’ve found through MIA.
Although I am regularly critical of articles posted here, please count me among your biggest fans. I do think that your book and this site are very slowly changing the narrative in the public discourse. When I read mainstream news stories praising psychiatric advancement and its newest “treatments”, it is very heartening to read the massive pushback in the various comments sections. Whether using real names or pseudonyms, it takes bravery to put oneself out there at all to stand up against the prevailing narrative. But people DO seem to be seeing through the lies and it is truly unique to have this site in particular where former patients have been given space to tell their stories of harm. I have particularly appreciated the recent articles written by those who are currently under ACT orders – a particularly marginalized group. Please keep up this focus on those who are most directly impacted by mental health treatment and policy – current and former patients.
In short, thank you.
Report comment
“ACT” or “Assisted Community Treatment” is a euphemism for Pharmacological Torture.
The definition of Pharmacological Torture is the use of drugs–including psychotropic–to punish a person. The aim is to force compliance by causing distress. This can be in the form of pain, anxiety, psychological disturbance (ironic huh?), immobilization, and/or disorientation.
Only with Psychiatry it doesn’t matter how “good” you are in some cases. They’re Hell bent on tormenting people till they die.
Report comment
Preach it, sister Rachel! And let the choir sing.
Report comment
Holy, holy, holy…
Report comment
“Only with Psychiatry it doesn’t matter how ‘good’ you are in some cases.” I’d say in pretty much all cases, since a school social worker wanted my child drugged, because he’d healed from preschool child abuse, and went from remedial reading, after the abuse, to getting 100% on his state standardized tests by eighth grade. And a psychologist I recently spoke to about this confessed that murdering the best and brightest Americans was the actual goal of the “mental health” workers. Since their mission is actually about proactively destroying all potential competition for the self proclaimed, globalist “elite.”
The psychiatrists are “Hell bent on tormenting people till they die.” I do agree with that, though. And the proof is they fraudulently claim all their non-diseases are “lifelong, incurable, genetic” diseases.
Report comment
Means, motive and opportunity.
Means to torture are available. We know which drugs and what amounts cause psychological and physical pain. Any doubts let me get my prescription pad. Take lithium until signs of tardive dyskinesia appear then drop it back a ‘notch’. Maximum damage with minimum signs.
Opportunity to torture comes when a distressed person enters into a doctor patient relationship. Dinner with a rapist I call it. If he is paying for dinner, your putting out. You just consented by agreeing to dinner right? And you anasognosia is getting in the way of you having a good time. Not even necessary in my State, drug em with benzos without their knowledge, and then have police jump them and provide a referral. They are consenting before you know it. Simply call them “patient” and police will do the work for you.
Motive to torture. This is where it all gets difficult if doctor decides to keep their mouth shut about their motive to torture. You can’t prove it and minus a confession well, sorry police are going to turn you away. So doctor can sit back smug in their position and bait you while they know nothing can be done about their conduct. And the angrier you get, the more money is made by the doctor and the pharma companies :).
It’s a win/win situation. As long as “patient” is excluded from the equation.
Report comment
Don’t forget that:
1. The “mentally ill” are monsters
2. The “mentally ill” mean yes when they say no
3. Most of the “mentally ill” eventually relax and enjoy their “meds”
4. Normal people don’t get labeled and locked up
5. Psychiatrists are only guilty of minor wrong doing when they lie to and about their ‘consumers”
Psychiatry is bolstered by the cultural view that all psychiatrists are irreproachable gods and all they treat are dangerous AND irrational.
Report comment
And the belief that people are always talking about someone else when 1 in 5 are being actively psychiatrized.
Report comment
Oh no, Rachel777, we are not monsters, we are mentally ill. A good line in psychiatry “you’re not crazy, who said you are crazy? Do you think you’re crazy?”
Oh and be very careful to mention certain words, well those words could be anything really, but if you sit there and say nothing, that will also mean something, and if you make idle chat, that also means something. I wish they had a little booklet of words or sentences one can say.
Why would they be so predictable? It really is a joke, I wish they did not take themselves so seriously. If not for that, shrinks could learn to have fun with people other than shrinks. My GP says it is easy to spot a shrink in med school. Must be why they spot so many MI’s.
Report comment
You’re not crazy. Who said you were crazy?
Yes, you’re completely irrational. Nothing you say should be taken seriously. You are definitely a danger if left untreated. Your complaints are all proofs of your psychotic lack of insight.
Innately defective yes. Lacking empathy. Potential serial killer without my help. Flawed at your core due to being born a genetic throwback.
All your thoughts and emotions are merely symptoms. Meaningless projections of your broken brain.
But you’re definitely not crazy!
Report comment
“…we are not monsters, we are mentally ill…”
Don’t you think psychiatrized is a lot like demonized? The shrink establishment and the cop establishment are totally in cahoots when it comes to slandering people with the “monster” and the “sick” labels. Especially when merged.
Crazy is not as bad a term as “mentally ill”. Crazy we all are to one degree or another. Silly, anyway. People, on the other hand, are very “serious” about “mental illness”. “Mentally ill” is an expression demanding converts.
“We believe in your bipolarity.” Etc.
Nobody is frivolously “mentally ill” except for people who are not “truly” “mentally ill” which says a lot for frivolity.
Report comment
Well put, Frank. Especially the difference between crazy and “mentally ill”.
I’ll add that this is why I don’t identify as “mad”. Anyone can become mad under the right circumstances and it isn’t a solid state one becomes but rather one that is passed through. It isn’t something binary that some people are and others aren’t.
Report comment
“I wish they had a little booklet of words or sentences one can say.”
This went quite well and may work 🙂
https://m.youtube.com/watch?v=poMWgGC82bw
Report comment
MIA is the voice of reason in mental health. The mission is not entirely fulfilled, but its getting there, and perhaps faster than one might think. I find the research news to be particularly useful, as it points me towards important scientific articles that I would not otherwise find. The recent articles on SSRI withdrawal have been directly helpful to my practice as I can put some statistics on my opinion, such as those in the Fava articles. Patients show up at the office educated and empowered by what they read on MIA. Not just survivors, but people who are considering getting psychiatric care and have not started on any drugs. It is hard to know how may people may have avoided going down the rabbit hole of psychiatry after reading MIA. Thanks Bob. Your hard work is appreciated.
Report comment
Thanks so much for these thoughts and questions. I think MIA is doing amazing work to usher out the old, and bring in the new. The Narrative is changing, and MIA is a big part of that! I’m so grateful for all MIA does, and I’m curious what they will do next! Thanks again for your amazing work!
Report comment
Where I was earlier this year, the psychology ‘therapy’ personal would – each week – coerce a group of patients to say positive things that had happened on the ‘ward’ that week. They knew the whole situation was abuse and were using the patients to cover-up. There was one chap who’s eyes were enlarged… one eye didn’t fit his socket.. he was in constant pain and required a specific non-psych drug. He was denied this drug and put on psych drugs.. he quickly saw through this use of ‘psychotherapy’ that and his pain meant he absolutely blew-up. Ofcourse this led to police incarceration. The last I saw of him.. he was in the middle of two policemen being marched out. I’m sorry to say that, in my view, non of what happens here has any affect in places like that, and many other such psychiartry controlled places, else where in the world.
Report comment
Streetphotobeing.
Why not write a personal experience on MIA regarding your experience and the man who was denied the medication prescribed to him by the medical system itself? Or try a local newspaper? Any vehicle to expose malpractice. Medicine as a whole needs to be exposed. Physicians should take up patient’s complaints that they were not given their pain meds in psychiatric units.
I myself know someone that has severe (suicide) pain, which is ongoing because of a botched treatment, and another botched treatment that tried to correct the first botched treatment. She is/was a nurse, yet it was getting harder and harder for her to get drugs for her pain. She rationally opted for leaving earth, however she was discovered and rushed to ICU, then transferred to a psych ward, where no pain meds were given. She was absolutely abused, by withholding due care.
We can say that the medical system as a whole is responsible for not ensuring that people in Psych do not get their meds.
Slavery took 200 years to abolish, and that with protests, deaths, abuse, escape.
Honor killings still exist in some areas and our system would abhor honor killings, yet honor killings are nothing more than a killing through not agreeing with the victim’s behaviour. Witches are no longer burned at the stake, and homosexuals lived in fear and isolation, or prisons for eons.
There was a beginning to these abuses and a slow eradication. Education is paramount in the exposure of abuse. It is when people give up, that change does not happen. Sooner or later people of influence within this nutty system might be embarrassed enough not to become vocal or act.
We need to address the medical schools, government, and put forth the malpractice being TAUGHT and practiced. It should be taught and a requirement for a psychiatrist, that he cannot withhold prescribed meds, nor allow a patient to suffer through withdrawal from street meds and that correct medical withdrawal protocol be followed when a patient suffers from addiction. Neither should anyone be subjected to enforced medication and if a patient is a danger to others, real proof should be given such as footage. Shouting and distress is not proof of being a danger to others.
The system that exists now is riddled with human rights violations. That violation begins with seeing behaviour as something to be controlled or abused. Human rights organizations, lawyers, the UN are busy being fearful, and psychiatrists that agree with us are keeping mum.
For any changes to happen, it always begins with the public. I have done a tiny bit by talking to anyone around me. The apathy from my own spouse is astounding, however my kids are not that way, and neither will their kids be.
I do know for a fact that education is not for nothing. Psychiatry spread their religion, and with a lot of lies. Our job is to spread the truth about psychiatry and the medical system in general.
As it is right now, doctors are complaining and grumpy that they no longer are respected as they were years ago. Translated it means we are no longer fearful of them and no, we do not respect authoritarian behaviour within a system that is supposed to help people, especially if it is laced with lies, innuendos, coercion and force or threats. They exposed themselves and is WHY it is becoming more public. It is not JUST the ‘MI’ that see what is happening.
Report comment
I’ve been through all the organisations that are suppose to oversee doctors and their institutions in the UK: GMC, CQC, PHSO and numerous others… you get fobbed off. So I’ve sent a link to my writing on here to the UN Special Rapporteur on Torture and other Cruel Inhuman or Degrading Treatment or Punishment Nils Melzer. If they contact me, will more fully inform them of what I was subject to and witnessed, also the factual evidence of a consultant lying about the polypharmacy I was subject to over a number of years, what Akathisia/Toxoic Psychosis is and what it does to people. What we need is a pharmacogenetics Cytochrome P450 gene test and for serotonergic metabolism to be offerd to the public independent of ‘doctors’ and this should now be a human right. I’ve asked labs who offer this test but am ignored. These tests will pretty much prove the actions or future actions of doctors caused/will cause or likely to cause drug toxicity, inducing illness right up to suicide ideation acutual suicide, violence, homicide ideation and actual homicide. I can only hope Nils Melzer can take note and grasp the scale of all this. The causation is known… it is iatrogenic not absent causation. Also The wider public need to grasp the importance of this and the enormous scale of it.
https://www.ohchr.org/EN/Issues/Torture/SRTorture/Pages/Call.aspx
Report comment
Could you explain more precisely what this test would be used for and what it would demonstrate?
Also wondering if in light of your most recent experience you’ve modified any of your conclusions about the existence of “mental illness”? (Not talking about psychiatry-induced illness.)
Glad to see you back here raging against the machine.
Report comment
The test is used to identify an individual’s specific phenotype (slow, intermediate, normal, rapid, extra rapid) of specific drug metabolising enzymes. Important ones being 2D6, 2C9, 2C19, 1A2, 3A4 and serotonergic pathways – 5-HTTLPR (Serotonin Transporter Polymorphic Region) (gene)and 5-HTR2A genotype, ‘So standard is to have two long alleles. If you have one short + one long you get problems and with two short alleles there are greater problems.’ The really important ones with regard psych drugs are: CYP2D6 and CYP3A4.
An individuals metabolism enzymes can activate and inactivate drugs, if you can not inactivate drugs you become toxic. The more drugs you have the more likely your enzymes are to being overwhelmed. Akathisia/Toxic Psychosis is an outward expression of this. It’s like a silent bomb going off in the head, you move to try and escape/find some relief. But unless you come off the drugs, there is no escape. This is what causes suicide ideation, actual suicide and other violence. My bouts of anxiety are real and have happened independent of any drugs. They do not cause suicide ideation/suicide or any other violence, but it is pretty awful.
Report comment