
After we published our report “Psychiatry, Fraud and the Case for a Class-Action Lawsuit” on August 13, psychiatrist Awais Aftab—who has staked out a public persona as a reformer and critic of his profession—weighed in with a review on Twitter. Here was his initial tweet:
I have to confess that I know very little of the Twitter world. I occasionally get notices in my email telling me of a tweet by critics of psychiatry, although I am not even sure how that notification came about. But I very much appreciated Aftab’s initial tweet—I mean, could anyone ask for a better review than “Holy shit”?
However, I figured that in his case, it wasn’t a prelude to a review that praised the article. And after his first “Holy shit” tweet, Aftab followed up with a longer thread of tweets, which told of his unhappiness with me and other “critics” of psychiatry, and that in turn triggered a number of tweets in response that Aftab didn’t appreciate, and he pulled the thread down.
As I am not a Twitter visitor, I didn’t follow the thread. I have long stopped worrying about such criticisms, and I imagined this was just more of the same. However, several people emailed screenshots of the thread, and once they did, I saw that Aftab had made a public accusation that couldn’t go unanswered. His was an accusation of journalistic malpractice, and it was designed, of course, to undermine the credibility of our report.
In his tweets, Aftab focused on a brief passage in our report that told of how the American Psychiatric Association (APA), in a page on its website still visible today, continues to mislead the public about the efficacy of antidepressants. He tweeted that I had “twisted the facts” about what was presented on the website, and that it was an example of how I “embellished” things, and how such “misrepresentation(s) add up.”
Now, it is easy to show that I did no such thing, and that the page misinforms the public about the effectiveness of antidepressants and, even more broadly, about the outcomes for patients that are treated for depression. Indeed, his accusation provides an opportunity to set forth in detail just how egregious the deception is, and in that manner add to the evidence of how the APA, as a guild, regularly misleads the public about the efficacy of its treatments.
His tweets are revealing in another way too. They tell of a powerful flareup of cognitive dissonance. While his tweets are his own, they are representative of responses by many psychiatrists to critics who have pointed out that psychiatry’s public pronouncements are, with some regularity, belied by its own research. The cognitive dissonance appears every time: the critics are dismissed as biased, or motivated by animosity toward the profession, and so on, and in this way the field avoids recognizing its own behavior as faulty and in need of reform.
This is why psychiatry cannot be expected to reform itself. The guild simply can’t bear to confront the reality of its own research. Perhaps public pressure could force such change, but medical professions in the U.S. are treated by the mainstream media as speaking with authority, and that limits the possibility of public pressure as a change agent. That leaves the law as the only possible lever for prompting such wholesale reform.
One way or another, our society needs psychiatry, as the medical specialty that oversees this domain of our lives, to provide us with honest information about the “biology” of psychiatry and the merits of its treatments.
Cognitive Dissonance as a Barrier to Reform
The premise of cognitive dissonance is that individuals experience psychological distress when their behavior is at odds with their ethical beliefs, or when they are trying to hold incompatible thoughts. Individuals experiencing cognitive dissonance have a desire to reduce their feelings of discomfort by attempting to reconcile their conflicting beliefs and behaviors, or their incompatible thoughts. Two social psychologists that have studied cognitive dissonance, Carol Tavris and Elliot Aronson, put it this way:
“Because most people have a reasonably positive self-concept, believing themselves to be competent, moral, smart and kind, their efforts at reducing dissonance will be designed to preserve their positive self-images—even when that perpetuates behavior that is incompetent, unethical, foolish or cruel.”
Dissonant states, they note, may be resolved in numerous ways. We are more likely to notice and remember information that confirms our beliefs, and ignore or discount information that threatens our beliefs. If we are forced to confront information that threatens our sense of self, we may simply reject the information (it’s just wrong), or metaphorically kill the messenger (he’s biased, or has evil motives), or find reasons to justify it.
Unfortunately, studies have found that we are unaware of our own cognitive dissonance. The unconscious mind seeks to resolve the psychological distress by constructing a narrative, on the fly, for the conscious mind that preserves one’s positive self-image.
“The nonconscious mechanism of self-justification is not the same thing as lying or making excuses to others to save face or save a job,” Tavris and Aronson write. “It is more powerful and more dangerous than the explicit lie, because it blinds us from even becoming aware that we are wrong about a belief or we did something foolish, unethical, or cruel. Dissonance theory therefore predicts that it’s not only bad people who do bad things. More often, the greater problem comes from good people who do bad things or smart people who cling to foolish beliefs, precisely to preserve their belief that they are good, smart people.”
Provoking Cognitive Dissonance
When Joanna Moncrieff, Mark Horowitz, and colleagues published their finding that there was no good evidence that low serotonin caused depression, it caused a great stir with the public, quickly garnering more than a million reads, and generating a measure of cognitive dissonance within the psychiatric profession.
A number of psychiatrists said this had long been known, dismissing it in importance, while others criticized the study, questioning the findings. Others sounded a “no harm, no foul” excuse: “Antidepressants work.” All of these responses had the effect of downplaying the significance of the paper and reassuring the public that antidepressants were a helpful treatment, and in that way soothed dissonant feelings that Moncrieff’s paper was an embarrassment for psychiatry.
Our MIA report published on August 13 was certain to provoke an even stronger dissonant response in psychiatrists who read it. The report documented how the APA continued to promote the chemical imbalance story to the public for years after its own textbook had declared it dead and buried.
That was a description of a guild’s unethical behavior. Patients were told they suffered from a chemical imbalance in the brain, the public understood that was true, and all the while academic psychiatrists—and APA leaders—knew that it wasn’t. This obviously presented psychiatrists with a “cognitive dissonance” moment: how could they reconcile those facts with their own self-image as medical doctors who treat their patients well, and in an ethical manner?
Many community psychiatrists, upon reading this, might have felt a dissonance of a different sort. Many undoubtedly had thought the chemical imbalance story was, in fact, true. So why would the guild deceive the public—and its own members—in this way?
In addition, our report investigated the “antidepressants work” response. That literature review told of how outcomes for “real-world” patients treated with antidepressants are poor, and that long-term studies provide reason to conclude that antidepressants increase the likelihood that a person will become chronically depressed and functionally impaired. This was sure to provoke the strongest dissonant feeling of all: psychiatrists had built their professional careers on the understanding that antidepressants and other psychiatric drugs “work.”
The research review, versus their understanding that “antidepressants work,” presented two “incompatible” thoughts. And so the obvious “cognitive dissonance” response: the report “twisted” the truth. The author “embellished” things. And now prescribers could relax: Antidepressants, after all, did “work.”
Aftab’s Tweets
Awais Aftab has staked out a presence on Twitter as a psychiatrist who readily engages with the public, and as a go-to person for the media when it is looking for someone to comment on critics of psychiatry, or on controversial papers that challenge conventional wisdom. He provided comments on Moncrieff’s paper, in ways that were not particularly flattering, and I wasn’t surprised to learn that he had quickly pushed the “send tweet” button on his phone after our MIA report was published.
There are several examples of cognitive dissonance in his tweets that can be easily identified. They don’t require much explication. However, his charge that I “twist” the facts requires an in-depth response, as it seeks to challenge the integrity of the report (and my reputation.)
- A Slip of the Tongue
In his initial “Holy shit” tweet, Aftab refers to Moncrieff’s paper as “infamous.” Now, the paper followed a clear scientific process, and from that perspective, there was nothing controversial about it, and yet here is the definition of infamous: “well known for some bad quality or deed; wicked; abominable.”
I imagine this was an unconscious choice of words. However, it revealed Aftab’s discomfort with a paper that put a spotlight on a falsehood that the public had come to believe.
- Introducing a Red Herring
In his opening tweet, Aftab asserts that I am calling for a class action lawsuit because Moncrieff’s paper “alleged” that the APA and other “entities engaged in medical fraud.” That is not the case at all.
Moncrieff’s paper didn’t allege that the APA or other entities engaged in medical fraud. I did. I wrote my paper in response to public comments by prominent psychiatrists that they had long known that the low serotonin theory of depression was false. These comments served as confessions, I wrote, of medical fraud. And then our report provided a detailed account of that fraud.
Aftab’s description of our report hides that theme of documented fraud. Instead, I am presented as relying on an “infamous” paper to attack psychiatry. And that is apparently so outrageous that it deserves a “Holy shit” exclamation—can readers believe what a monstrous thing this is to do?
- Kill the Messenger
This is a response that can be expected to surface whenever there is a presentation of information that threatens one’s beliefs or sense of self. The “messenger” is denounced as biased, or driven by animosity.
Here is a string of tweets that fit into the “kill the messenger” category:
Cheap vitriol, destructive impulses, disinformation, Brexit, Trumpism, QAnon, anti-vax movement, COVID-19 denialism, setting the system on fire, destruction of systems—that is an avalanche of disparaging adjectives, aimed apparently at me and others who go too far in their criticisms (beyond what Aftab can tolerate.) Meanwhile, he “struggles to counter disinformation while remaining receptive to critique.”
Hence the cognitive dissonant resolution: at least there is one person with an open mind to be found in this “debate.”
- Whitaker “Twists the Truth”
In terms of a cognitive dissonance response, this accusation is designed to be the one that puts the matter to rest. There is no reason to be disturbed by the report because it isn’t true.
However, given that this one disparages the integrity of the report (and my integrity as a journalist), this tweet needs to be responded to in detail.
Aftab’s Accusation
In response to Moncrieff’s paper, a number of psychiatrists voiced a “no harm, no foul” excuse. “Antidepressants work,” they said. In my MIA report, I examined that claim with this intent: Was this a statement that provided the public with “informed consent?” This was just one section in a long report, and so I quickly summarized three types of evidence relevant to the question:
- In industry-funded trials, antidepressants provide a greater reduction of symptoms than placebo by two points on the 52-point Hamilton Depression Rating Scale, a difference of questionable clinical significance.
- In studies of “real-world” patients, only a minority of patients respond to the drug, even for a short time, and stay-well rates at the end of one year are particularly poor.
- There is evidence that over the long-term antidepressants increase the risk that a person will become chronically depressed and functionally impaired.
At the conclusion of this section, I wrote:
This, of course, is information that would enable patients to make an informed choice about whether to take an antidepressant. Yet—and this is an example of how the APA continues to misinform the public—here is what the APA currently tells the public about the efficacy of antidepressants:
“Between 80% and 90% of people with depression eventually respond well to treatment. Almost all patients gain some relief from their symptoms.”
Those are the two paragraphs, in a report that was more than 8000 words long, that Aftab seized upon to accuse me of journalist malpractice.
And here’s the thread that followed:
Although I am not positive, I think Aftab is maintaining that the “80% to 90%” good outcomes figure is derived from research that shows that if a first modality doesn’t work (antidepressants), then a second modality can be tried (psychotherapy), and if that doesn’t work, then a third can be tried (ECT), and somehow at the end of this process, 80% to 90% of patients will have “responded well” to treatment, and nearly all will have gained some relief—e.g. nearly everyone is doing better than at baseline.
Thus, he is saying, the passage is not informing the public about the efficacy of antidepressants, but rather of the good outcomes that arise from psychiatry’s deployment of the three treatments mentioned on the web page: antidepressants, psychotherapy, and ECT.
The APA’s Web Page
Fortunately, there is a document that readers can review to assess the merits of his charge. Below is snapshot of the page that I had linked to (click on image to enlarge):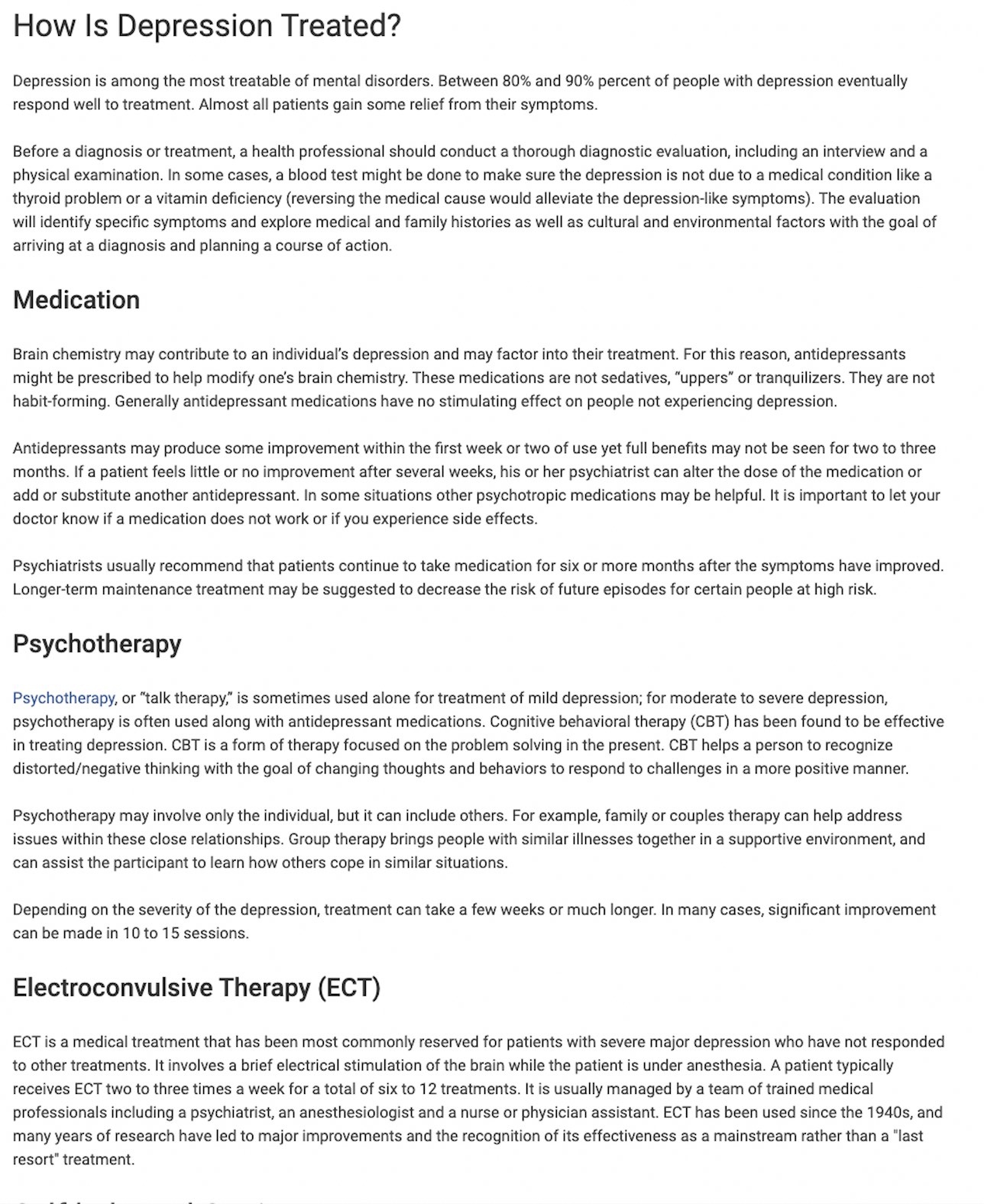
There is a subtle way that this text is informing patients of the “efficacy of antidepressants,” and it relies on a trick common to PR efforts.
The first paragraph presents a statistic (80% to 90%) that tells of positive outcomes for patients who are treated for depression. The use of a statistic provides the passage with an aura of being scientific, and the lay reader is being prompted to think that this statistic comes from clinical research. However, there is no citation given for it, and equally important, there is no explanation for how it may apply to any one treatment. Nor is there any other “outcomes” statistic cited in this passage. It’s that vagueness that makes for effective PR: the statistic floats in the air, with the reader’s mind ready to apply to whatever he or she reads next.
That “next” moment tells of antidepressants, which of course is the treatment that is regularly prescribed for people with depression. The section begins by telling visitors a mild version of the chemical imbalance theory: “Brain chemistry may contribute to an individual’s depression and factor into their treatment. For this reason, antidepressants might be prescribed to modify one’s brain chemistry.” Then it informs readers of the efficacy of these drugs: “Antidepressants may produce some improvement within a week or two of use yet full benefits may not be seen for two to three months.”
The visitor to this APA page on depression will then learn that psychotherapy and ECT are effective too.
Now imagine that a visitor to this page shuts his or her computer after reading this text and a family member asks them what they learned about antidepressants. The visitor’s mind will recall the one outcomes statistic that was presented, that 80% to 90% respond well to treatment, and conclude that this is the outcome to be expected at the end of two to four months on an antidepressant when the “full benefits” arrive.
That is the power of that floating statistic. The reader will apply it to the antidepressant treatment—after all, “full benefits” will eventually arrive—and that becomes his or her understanding of the “efficacy” of this treatment. Indeed, as there is no claim in this passage that the 80% to 90% figure represents outcomes after all three treatments, visitors to this page might conclude that regardless of which of the three therapies they chose, they would have a 80% to 90% chance of “responding well.”
However, it is possible to see how Aftab’s mind exploited the vagueness of the APA’s claim in this web page. In order to capture that vagueness in my report, I should have written: Here is what the APA currently tells the public about the efficacy of antidepressants and its other treatments for depression. It was the absence of those last five words that enabled Aftab’s mind to think “gotcha,” and once he grabbed onto that idea he was all in. His mind needed to conjure up an explanation for the “80% to 90%” respond-well claim, and it quickly cobbled together the notion that it was cumulative outcomes the APA was talking about (even though there is no claim to that effect in the APA’s text), and once his mind had done that, voila—Whitaker “twists the truth!”
Only then a responder to his tweet, Pfluft, called him on his claim: he smelled “BS.” And so Aftab’s mind now had a new cognitive dissonance challenge, and it put together a quick addition to his defense of the APA’s “respond-well” claim: these were “eventual” outcomes, and it was over time that the respond-well outcome climbed to 70%, and no he didn’t have a source for that 70% figure, which admittedly was a bit short of the APA’s 80% to 90% figure, but that didn’t really matter, the important point was that Whitaker couldn’t be trusted. And it was then, I believe, that Aftab shut down the thread.
Such is cognitive dissonance at work. However, there is an important factual point to further review here. In the report, I cited the web page as evidence that the APA was continuing to deceive the public about the outcomes for patients treated with antidepressants. The real-world studies I cited in the report reveal just how egregious the APA’s ongoing deception is, and how far off Aftab was with his claim that eventually 70% of depressed patients respond well to treatment.
Outcomes for Real-World Patients Treated for Depression
As my review of the research regarding the risk/benefit profile of antidepressants was just one section in a long report, I did not describe the “real-world” studies in any detail. However, those studies belie Aftab’s claim that the outcomes for depressed patients in clinical settings “eventually” end up quite good. Together, these three studies did not just tell of poor outcomes with antidepressant treatment, but rather of poor outcomes for patients treated in clinical care settings. The patients were provided with various clinical supports, and in two of the three, many patients also received psychotherapy.
Study one: One-Year clinical outcomes of depressed public sector outpatients.
In a study of 118 real-world patients, the researchers explained that “treatment was delivered under conditions specifically designed to maximize clinical outcomes, which included the use of medication algorithms, additional trained clinical staff support, patient and family education, regular assessment of symptoms and side effects at all medication visits, the use of a clinical procedures manual, and expert consultation.”
Response and remission rates at the end of 12 months were 26% and 13%. These results “reveal remarkably low response and remission rates,” the researchers wrote. They further noted that these results were superior to a “treatment as usual group” that did not get the “enhanced treatment package,” and thus outcomes in ordinary clinical care were likely even worse than this.
When the NIMH launched its STAR*D study, it touted it as the “largest and longest study ever done to evaluate depression treatment.” This study in real-world patients, the NIMH investigators stated, would produce results that would guide clinical care in the United States. “Given the dearth of controlled data [in real-world patient groups], results should have substantial public health and scientific significance, since they are obtained in representative participant groups/settings, using clinical management tools that can easily be applied in daily practice.” The results, the NIMH promised, would be “rapidly disseminated.”
The study was designed to mimic real-world prescribing practices in outpatient settings. If the first antidepressant didn’t work, then a second one could be tried, and ultimately patients were given up to four tries to see if they could find one that would produce a remission of their symptoms (defined as seven or below on the Hamilton Depression Rating Scale). During this phase of active treatment, there was also the opportunity for patients to receive cognitive therapy alone or in combination with citalopram, a design that showed this would be a study, as the NIMH said, of “depression treatment” and not just of antidepressants. The patients treated with psychotherapy, the researchers concluded, had “similar response and remission rates to those assigned to medication therapies.”
The outcomes from this study were quite poor, so much so that the reporting of results by the NIMH-funded investigators is a story of a scandal. The investigators relied on various mathematical gyrations to tell the public that 67% remitted in the treatment phase, when in fact, as a re-analysis of the study data by outside investigators found, only 26% of the patients ever achieved this status.
The study also had a “maintenance” phase that sought to assess whether those who had remitted could stay well. During this year-long follow-up, “physicians were allowed to make any psychotherapy, medication and/or medication changes to maximize the likelihood of maintaining patients’ remission status.”
Once again, the NIMH investigators reported the results in such a confusing way that it was impossible to figure out the stay-well rate. It took several years of medical sleuthing for a group of outside investigators, led by Ed Pigott and Allan Leventhal, to identify the actual number. Pigott told Medscape of the bottom-line results:
“We found that out of the 4041 patients initially started on the SSRI [selective serotonin reuptake inhibitor] citalopram in the STAR*D study, and after 4 trials, only 108 patients had a remission and did not either have a relapse and/or dropped out by the end of 12 months of continuing care . . . In other words, if you’re trying to look at sustained benefit, you’re only looking at 2.7%, which is a pretty jaw-dropping number.”
Medscape then interviewed one of the principal investigators from the STAR*D trial, Maurizio Fava, and asked if Pigott’s conclusions could actually be true. The STAR*D investigators had published a graphic with that 108 number, although it had been nearly impossible to understand what it signified, and in the interview, Fava acknowledged that Pigott had it right. “I think their analysis is reasonable and not incompatible with what we had reported,” Fava said.
In a recent international study of 1,217 patients diagnosed with major depressive disorder, the investigators charted outcomes for those treated with an antidepressant alone and those treated with an antidepressant plus some form of psychotherapy. The results were virtually identical, and they were poor for both groups. Only 24% responded to treatment (e.g. experienced a 50% drop in symptoms); 34% were non-responders to treatment; and 41% developed treatment-resistant depression.
Here is a graphic that depicts the outcomes for the two groups:
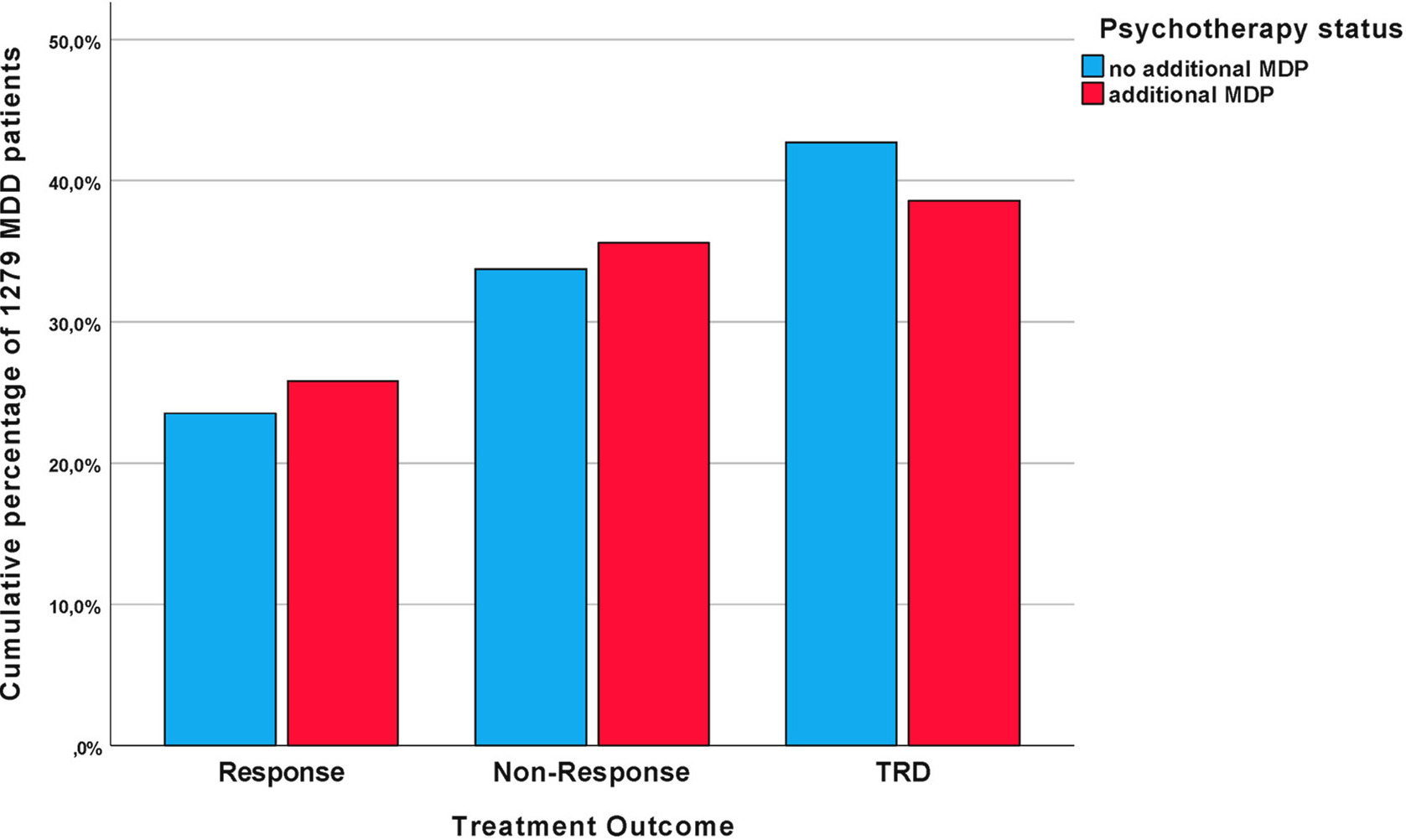
Thus, these three studies tell a similar story: the outcomes for “real-world” patients treated in clinical settings are quite poor. Only a minority of patients respond to treatment at some point, and only a small percentage get well and stay well.
Indeed, since the results from the STAR*D study were supposed to guide future clinical care and be “rapidly disseminated,” the APA, on its website today, could list the numbers from that study to inform the public of outcomes for patients treated for depression. Instead of the 80% to 90% “respond well” figure, it could tell of a remission rate of 26%, and a long-term stay-well rate of 2.7%. In that way, the public could be properly informed about what NIMH-funded research told about the efficacy of treatments for depression.
Where Did The 80% Figure Come From?
In his last tweet, Aftab acknowledged that he didn’t know the source for the “80% to 90% respond well” figure.
Fortunately, I do.
This is the very statistic that the APA has used to market antidepressants and its other depression treatments for at least 17 years. The APA’s 2005 brochure “Let’s Talk Facts About Depression,” which informed readers that “antidepressants may be prescribed to correct imbalances in the levels of chemicals in the brain,” said this about the efficacy of its treatments:
Depression is “among the most treatable of mental disorders: between 80% and 90% of people with depression eventually respond well to treatment, and almost all patients gain some relief from their symptoms.”
That’s the source that Aftab can’t remember. His mind stumbled on a “fact” that he heard in some place or another, which in his cognitive dissonant state he assumed was true, and all the while he was unaware that he was citing a statistic that could be found in a 17-year-old pamphlet that assured the public that antidepressants “correct imbalances in the levels of chemicals in the brain.”
The APA’s propaganda, unfortunately, seeps into the unconscious corners of the brain, particularly when it is repeated year after year.
The Path Forward
Two years ago, Mad in America interviewed Awais Aftab and had him as a guest on our podcast, and I exchanged emails with him a couple of times after that. I have appreciated his interviews of critical psychiatrists published on Psychiatric Times. Even so, I wasn’t surprised when I read his disparaging tweets. The language, the attribution of vitriol to me, and the claim that I twisted facts—it all spoke to an emotional cognitive-dissonance outburst, and that’s how I perceived it. As such, I didn’t really take it personally: To suffer from cognitive dissonance is to be human.
At the same time, his response leads to an obvious conclusion: Psychiatry cannot be expected to reform its ways. When push comes to shove, even those who would seek to reform the profession cannot confront the reality that exists in the research literature, which is so out of sync with the profession’s pronouncements to the public and with their own understanding of the merits of their therapies.
So what is our society going to do? Our society needs to organize its thinking and care around the “narrative of science” that exists in the research literature. It is a matter of great public health importance, and at this point, the only way that I can see this happening is through the lever of the law. The law requires a medical profession to provide patients and, by extension, the public, with “informed consent.” If that standard is applied, then the societal narrative will dramatically change.
Congratulations to the graphic artist. The image says more than where “the law” is now. Your article in the sentence, “And that leaves the law as the only possible lever for prompting such wholesale reform” indirectly is the key. For the idea in part would be realized a few years ago at the New York Academy of Science Meeting on Bipolar that featured Rif El Malik, from the University of Louisville and others. Seems the drug manufactures poured money into the session at the beginning of the Obama administration but were no where present.
So, in attending the event to learn, coming out of the elevator where one sees the bust of Darwin one can only hope for an evolutionary moment. From the presentations, one learned of simple tests performed on the lab rats, but when I self identified as a c/s/x, off the meds, the cognitive dissonance was experienced a bit in myself but more so, in the younger students making up the audience.
Hence, how could cognitive dissonance not be occurring, in portions of the thought process. For law to confront the creation of law seemingly would be akin to Moses listening to Moses and then saying I got it! In breaking the tablets, the light was released but also entered through the cracks. To have the law be the lever, the assumption of the fulcrum being rooted to where the point operates might be ignoring the image of a fulcrum base planted on the ceiling, for then the overlap and intertwing of the Star would convey a different, more golden reality.
The stable of legal types are there, the invite and the coffers along with assemblage to move the material forward into legal form is only a matter of time. This is not a technical question, but rather how power is held and realized during periods of vulnerability. And in terms of medical malpractice, the role of the state and private hospital (as if there are private hospitals) in the corporate sense must figure out a way to realize accountability, of and by governance systems and then within the organization, the very people and research that realized funding and license to practice the deep mining of the brain, while never realizing the intersectionality.
The emergent words now, if not this effort to respond, may be in need of an edit effort. Perhaps the readers will also experience some joyful cognitive dissonance in realizing the gifts inherent to learning!
Where will the lawsuit be filed? Which state or court has the scales warming up? For the silence is killing us.
Report comment
Once again a brilliantly argued article by Bob. I look forward to reading how he imagines such lawsuits might be crafted. To think that such efforts might break through the din of misinformation, words carefully crafted by pharmaceutical and psychiatric wordsmiths – ahh….! I’ve been hoping for, working for, such change for almost twenty years.
Report comment
This is what happens when you threaten an industry and job and research program. With $50 billion + a year in the USA the racket will continue forever! Psychiatry is a LONG CON and when victims finally figure it out after the music stops it is too late.
They use words speak like “treatment response” which is vague and malleable. Psychiatry is actually quite successful in DESTABLIZING PATIENTS during the course of “treatment”. Outcomes don’t matter just that the patient be “under treatment” FOREVER until the rollercoaster ride abruptly ends leaving the patient hanging in the air.
Report comment
READ IT AND WEEP…oh you psychiatrists who think your way is correct.
READ IT AND WEEP…oh you critics of psychiatry who think your way is correct.
The TWO WEEPINGS need to come together in discussion. Accusation furthers no discussion. Why talk at all? If it be nothing but bickering acrimony?
Why not you psychiatrists contentedly believe what you believe? Why not you critics of psychiatry contentedly believe what you believe?
And leave each voice alone to be beautifully different?
The whole world is incinerating in acrimony. For the sake of justice…
Leave the world alone.
Report comment
good work!
Report comment
So many things I could comment on….but as a reader and someone who values supporting an argument with research, I’d say your writing and report win over anything the APA has to say. One thing that makes this debate about informed consent and revealing the absolute truth about the research on drug & ECT/TMS efficacy is that as a medical specialty, psychiatrists have more power than any other kind of doctor. They can forcibly have you committed to a facility, make you go to court to be released, and drug you and give you ECT without your consent. I find all of that power terrifying and believe we need to seriously hold psychiatrists and the APA to account for all the harm they have done.
Lastly, you are absolutely correct about your rhetorical analysis of the APA website and the use of the statistic in one PP followed by a paragraph on antidepressants. The word treatment in the 1st PP paired with the statistic is misleading and many people would believe the success rate is due to medication, without the APA directly saying it.
Keep up the great work!
Report comment
It’s experienced specialist attorneys who will be best able to gauge what sorts of lawsuits are most likely to succeed. And we have to try lawsuits and find the ones which will work. Always better if civilian atrocities can be resolved with the court house and the ballot box.
Without lawsuits, you maybe Anti-Psychiatry, but you are still sacrificing survivors to Psychotherapy and Recovery.
So yes, Good Work.
Joshua
Report comment
The Opiate disaster and con is similar to the anti-depressant and anti-psychotic promotion and misinformation campaign of the past few decades. It is all about the $$$ and in the US profiting from others misery is a business! The worse patients get the better it is for psychiatry because the more you need their “expertise” and interventions.
Right now it is silly psychedelics and now they are promoting medical devices and implants for the MI.
Report comment
“Presuppositions held uncritically can powerfully impede the growth of any branch of learning. Because of the tenacious and obstructive nature of unexamined assumptions, it has often been an intellectually, politically, and sometimes religiously difficult project to place the prevailing beliefs of the day in question before the dispassionate eye of reason. Intrepid souls who have insisted on doing this have often been harshly rewarded for their pains, for unexamined assumptions are often closely tied to vested disciplinary interests, while attempts to question those assumptions are apt to run aground on the shoals of what is perceived to be counterintuitive, in conflict with establishment belief, and therefore seen literally to be “para-doxical.” One of the central assumptions of both the practice and theory of traditional psychiatry and clinical psychology is almost never discussed in the literature, and even more seldom is it questioned” from Steven James Bartlett’s book: “Normality does not equal mental health: I need to look elsewhere for standards of good psychological health”
“Our society actually exists as a kind of negative afterimage. We all live in a crazy, backward world, often unaware of the lies and double messages we are given. If we could be free for a moment to catch a glimpse of our true situation, if we could view our society as a visitor from another planet, we would be stunned at the nightmare in which we live. The things we are expected to believe about ourselves and about society are frequently the very opposite of the way things really are. Unhappily, the individual and all the members of our society are often unconsciously working together to maintain a largely defensive and dishonest way of living”
From Robert Firestones book: “Psychological defenses in every day life”
Report comment
Dazzling.
Report comment
I respect Awais Aftab’s efforts. His recent tweets may mirror psychiatry’s cognitive dissonance as well as his own.
While in the past he has agreed publicly with all the points brought up in Moncrieff, et al., 2022, and may well agree in private with every point brought up by Bob Whitaker on MadinAmerica — he readily admits psychiatry needs to do serious soul-searching leading to change — he apparently fears that a disturbed hornet’s nest may make his work of persuading the hornets they need to become honeybees more difficult.
His outrage is that the kerfuffle ensuing from Moncrieff, et al., 2022 puts him, as a reformist centrist, in a difficult position. He wants to help, but as an astute politician, has to side with the dominant narrative to maintain his influence in the dominant culture.
Given the byzantine nature of medicine’s professional organizations, the copy on the APA’s “What is Depression?” page no doubt had to go through numerous approval levels. The page in question was no doubt deliberately constructed to imply that antidepressants lead in achieving a 80%-90% cure. Listing psychotherapy second must have occasioned a great deal of discussion. (Notably, the page does not mention how often untreated natural recovery occurs — a lot.)
I have no idea how the world might have been constructed differently to enable Dr. Aftab in his mission. Truth has a way of coming out, and even centrists have to deal with it. Psychiatry has been caught with its pants down, yet again, for something it should have corrected a couple of decades ago. There are plenty of other time bombs waiting to go off in psychiatry; the rotten places in the scientific literature indicate where. Its centrists may have to get used to the explosions.
Report comment
Short of “confrontation” by legal means – which is a difficult mess in many ways – the only practical way forward is for people like Aftab to bluntly embrace what he is so afraid of and hostile toward. People like Moncriefe or Whitaker will do what they do as best they can see to do it, but doing so alone pigeonholes them in a sense and puts them at odds with prominent voices doubling down on the status quo narrative and practice. When you have a reality that prompts scientists and reporters etc. to do their part and raise a dilemma, the next step is for more “authority” figures who have traditionally been seen as “not with ‘them'” to come out and just say to colleagues who may be lashing out, “no, stop, we have a serious and fundamental problem that we have been in denial over and it has to change and there has to be accountability for there to ever be hope of legitimacy for any of us”.
Unfortunately, despite a comment off-hand here or there about soul searching, it seems he has chosen to do the opposite. He might not be quite as bad as Ronald Pies, for example, but frankly, same difference. The details and content of these diatribes changes but what doesn’t change is a need to control and distort the discourse. He, like Pies, doesn’t focus on facts or harms or ethics or policy failures, but on how he is entitled to serve as the arbiter for what counts as valid “criticism” and what does not, and how in doing so he reasserts legitimacy by being open to review (his own) whole denying wrongdoing. It seems it really is hard for many people to get over themselves and do right when they are not forced to do so.
As Whitaker says, that’s where the lever of the law can step in to level the field. But it’s an extremely tall order. The legal system we have, perhaps moreso than psychiatry (well, that’s another topic) abhors the notion of systemic fault and correction and has adopted a loose scheme in this domain that defers to voices like Aftab’s by virtue of their position and defense of the status quo.
I was recently speaking to a psychiatrist about forcing a patient of his, who I was concerned about, into commitment and drugs despite a lack of illness and good understanding of the facts and an informed choice to not take drugs “just because”. It was a classic situation – the prospective recipient was mentally ill presently despite no evidence (and it has to be said, a clear and developed explanation for how everything had come about and then changed and what challenges remain and a commitment to flexible and responsible follow-up and self-management) of ongoing dysfunction and more than that, was “bad” and a host of other things for having the audacity to “question” him, the doctor, or not blindly validate what was asserted (it also has to be said – this person was unreasonably respectful, while the staff were… not reciprocal, yet still the projecting discomfort and consternation ontp the person being evaluated were evidence of that evaluee’s rudeness or still more vague problems) or for wanting to protect himself and his legal record and life. No, he was a subhuman thing, a sick, and a “bad” for not going along with it all and knowing his stuff and actually taking the situation seriously. Anyway, when it comes to the “need for treatment”, there is never-ending evasiveness. Somehow, they write their patient “will not consider treatment” (despite fighting them to even be allowed to be in therapy, on his own, which they seemed to view as undermining their process) because he won’t just “take his medicine”, which is prescribed for reasons that cannot be elucidated or justified beyond their inherent necessity following any history of a diagnosis. “Are you saying there is a chemical imbalance, or that there is some other reason his judgement should be discounted or different treatm–” interjecting with a scowl, “sir ‘these people’ need to take their medicine. You are not a psychiatrist and it is not your place to question me”. In his testimony to a court, he made vague statements or just blatantly lied (he also previously stated that he would “just say things”) – without question from the judge – in order to procure an order that the recipient comply with all treatments and orders from the facility. Despite what the law says on paper and what these talking heads claim, no vetting, no review, no evidence-based anything, no listening, no consideration of concerns or desires or even logical coherence for that matter. Nothing. Just “these people”, whatever that’s supposed to mean beyond the medico-legal circumstances that prompted the evaluation in the first place or a history, somehow somewhere, of a label, need to be processed, and that means having a DSM label – any label, really (he didn’t even know what the past diagnosis was or why) – and taking “their medicine” (and really any medicine in a category, and however more are tacked on) and validating what is done to them. Rubber stamp. Rinse, repeat. It’s a farce.
So these “arguments” in the media, journals, on Twitter, whatever… it’s not even discussing reality. That psychiatrist isn’t thinking about research he’s never read or legal rights or ethics quandaries he doesn’t care about. He waddled his way through the hoops and is a doctor now and his parents are very proud, and he was invited to a function last month, and he as a nice car (apparently), and thinking or caring or having integrity is not how he gets through his day. His job is rote bullshitting and paperwork at a facility that does things as it always has and expects compliance and validation. Everything else is fluff. He doesn’t care if there are or aren’t chemical imbalances or anything else and he doesn’t have “a more sophisticated understanding” of anything. He just wants to get on with his day without being “questioned” or thinking about it. That is psychiatry in practice. And I think focusing on whether or not “low serotonin” was pushed or some other thing is a trap for those who speak of soul searching or reform. If that were the problem – simple but legitimate misguided science capable of reflection and correction – we wouldn’t be here. If there is admission of misleading advertisements, nothing really changes. Some other nonsense that is a drop-in replacement will follow (or already has). The problem is that the whole thing is rotten on the ground.
Report comment
I think your last paragraph sums the attitude really. I have two psychiatrists in my family of origin who fit that description.
They both have the arrogance that comes with having almost absolute power. One told me once about giving forced treatment. He said he was doing it ‘for the patient’s good’. The patient was a 60 plus year old woman that was given ECT against her will. They both have relatively large incomes.
One of them was fulminating loudly when I met them a few years back at the actions of some members of the British Psychological Society that questioned the DSM Model – it was the anger that came from someone whose authority was being called into question. It’s sad because when they were young they themselves questioned authority but then just turned into standard bully to get status and power – one is a really horrible individual but then ruthlessness is normal in getting to consultancy level in most medical specialties anyway.
I think Robert Whitaker also gives a good description of how cognitive dissonance allows people to maintain a good self image as ‘kind’ people while doing things that are frankly monstrous.
Report comment
Upton Sinclair — ‘It is difficult to get a man to understand something, when his salary depends on his not understanding it.’
Report comment
It would be funny if it wasn’t so tragic that psychiatrists would try to shift attention to ECT in order to distract from the reality of SSRIs being exposed.
If I’m understanding it right, the message was that if SSRI antidepressants don’t work, there is still psychotherapy and ECT treatments, which if a patient engages in all three, they will have an 80% chance of remission/cure for depression (which is biologically based it goes without saying)? In my case, engaging in all three treatments (plus some extras like antipsychotics, and different labels) resulted in permanent disability.
Thanks again, Mr. Whitaker.
Report comment
The unasked question: what are the odds of “remission/cure” if they receive no “treatment” at all?
Report comment
“what are the odds of “remission/cure” if they receive no “treatment” at all?”
I think that question is answered partly by studies in places where they either can’t afford the drugs, or don’t want them because they are ‘intoxicants’ and therefore considered “prohibited”.
The two situations shouldn’t be confused, it isn’t necessarily the case that because people are not taking the drugs is because they can’t afford them. They simply don’t want them. But creating the illusion that if they had the money……..
Geez those ‘radical Islamists’ denying people access to drugs and treatments that work. (and interfering with expansion and profits from untapped markets). Wasting good money on unnecessary items such as food and clean water, when they could have these drugs.
Report comment
It’s worth noting many of these areas use traditional medicine focused on lifestyle and restoring the body to balance. If conditions like depression, psychosis, diabetes, cardiovascular disease, and Crohns are caused by the immune system being unbalanced then most medical professionals would agree lifestyle changes like should always be used instead of drugs.
Report comment
Careful, I asked that as a teenager on a SSRI in 1994 and they put me on Haldol.
Report comment
Exactly, Steve (but then, we always agree…) A quick look at Ch 8 of ‘Anatomy’ suggests that two thirds of cases of unmedicated ‘depression’ will remit after 6 months, and 85% after a year. So you must be doing something pretty spectacularly wrong to reduce long term recovery rates to 2.7%. The fact is, we are medicating a state of mind that doesn’t necessarily even need ‘treatment’ at all – either medical or psychological. And in doing so, we are creating a massive problem that is then cynically used to argue for more ‘treatment’, more psychiatrists, more research…. and on we go.
Report comment
We do seem too be on the same wavelenth! If you’re every in the West Coast USA, we should get lunch! I bet we’d have an AMAZING conversation!
Report comment
Upton Sinclair — ‘It is difficult to get a man to understand something, when his salary depends on his not understanding it.’
Report comment
I would say they are starting to ” Circle the Wagons” , or perhaps telling the surfs that they need to run inside the castle, the barbarians are coming…..Bob you don’t appear to be a barbarian….lol
Report comment
Good work, Bob! You’ll surely already know he didn’t waste any time banging out another retort. His impulsiveness may be his downfall. And his current one has a bit of an “I’m rubber, you’re glue” childlike quality to it. I’m quite enjoying the show.
Report comment
This is why I believe it is important to draw attention to parallels in other medical specialties and how they responded when their research was questioned. The American Psychological Association (the other APA) heard the whistle of cognitive dissonance and after reviewing their research blew an air horn on themselves in the form the the replication crisis. Recent developments in Alzheimers research are placing neurology and drug companies (again) where psychiatry was 15 years ago. Do they do what is right and correct the mistake or they do keep digging deeper and ignore the source of cognitive dissonance like psychiatry.
Report comment
Upton Sinclair — ‘It is difficult to get a man to understand something, when his salary depends on his not understanding it.’
This is a multi billion dollar industry and with research it could amount to $60 Billion dollars each year- a job program of sorts. Robert is challenging their golden egg.
Report comment
And you guys think you’ve got problems with ‘misrepresentations’? We have a Chief Psychiatrist who rewrites the law to remove the legal protections afforded the community. And when we speak about ‘killing the messenger’ …….. ‘no harm, no foul’? Only because they were rudely interrupted.
From the Mental Health Act
29 . Referring potential involuntary patients for psychiatric examination
(1) Subject to section 194, a medical practitioner or an authorised mental health practitioner who suspects on reasonable grounds that a person should be made an involuntary patient may refer the person for examination by a psychiatrist.
Who should be an “involuntary patient” is set out in s. 26 Persons who should be involuntary patients of the MHA 1996
The Chief Psychiatrist in his letter of response to the Law Centre writes;
“The referrer, in this case, a mental health clinician who has undergone training as an Authorised Mental Health Practitioner (AMHP), has only to ‘suspect’ on grounds they believe to be reasonable that the person requires an examination by a psychiatrist.”
Firstly, the “reasonable grounds ” standard has been removed, thus authorising arbitrary detentions based on nothing more than a suspicion.
Secondly, the criteria for detention has been removed by changing the belief that must be formed by the AMHP from “the person should be made into an involuntary patient” to “requires an examination by a psychiatrist”.
The MHA clearly sets out “who should be an involuntary patient” whereas, the Act has nothing to say about who should be referred for an examination by a psychiatrist. Possibly because it is quite easy to make a decision that someone ‘needs their head examined’.
The issue was that this was someone attempting to conceal KNOWN criminal offenses and human rights abuses, and the only way to achieve that was with such acts of gross negligence, and a belief that the Chief Psychiatrist has the right to change the law and remove the protections afforded the community by our lawmakers.
The Community Nurse had not met the burden placed on him by the Mental Health Act, so have the Chief Psychiatrist remove the burden with the above misrepresentation of the law and what was criminal, now becomes lawful. Having police retrieve the documents showing that the Chief Psychiatrist was fully aware of the offending before distributing the fraudulent and slanderous set of documents (the “edited” set) will be of benefit before sending out the letter of response.
Quite a three card monte, and such a shame that there were people harmed as a direct result of the deliberate delays and obstrutions and the overt threats and attempt to “fucking destroy” me by the State.
I find it fascinating that despite looking, that people simply can’t see what I’m saying. A large number of lawyers…. though do they obtain a benefit by NOT looking? Lawyers who deliberately don’t look at what they’re told to not look at by the State? I can see how that might make a mess of the justice system. But in this instance we are talking about people being deliberately brain damaged as a result of the ‘Fatwah’ that is issued against them by psychiatrists. Or the Community Nurse who makes you an “Outpatient” before calling for police assistance, and then has a knife planted on you for them to find. A risk being one of the criteria for referral.
Glad that at least someone is prepared to stand up and be counted on this issue of ‘anti depressants’. I wish the community where I lived felt as strongly about the person who is charged with protecting their human rights removing them from the law with his misrepresentation. The Minister telling me that the above is “not a misrepresentation”? What is it then? A delusional state brought about by no one telling the Emperor has no clothes, and that the public interest is to know that the Chief Psychiatrist is enabling arbitrary detentions and acts of torture by simply ignoring the law and changing it to suit the purposes of those who have a burden placed on them?
It IS an offense in my State to produce false documents as a means to procure a person not suffering from a mental illness. That offense is concealed by the misrepresentation of the law quoted above. The burden removed, and the ‘criteria’ setting out when a Authorised MH Professional can have police detain someone and have them transported for assessment changed. All the need do is call police and ask for ‘assistance’ with their “Outpatient” and forge the Forms for others to utter with
“assistance” from police where an “Outpatient” is concerned?
https://www.youtube.com/watch?v=oZ9UQKBUrsg&t=4s
Okay, you weren’t actually a ‘patient’ before being snatched form your bed, and the ‘diagnosis’ was done by a Community Nurse who hadn’t actually met you yet, and had done the ‘diagnosis’ on the basis of a telephone call but …….. Chief Psychiatrist is good with this. And they wonder why the statistics don’t match their beliefs that they’re doing a great job? A little more money would always help.
Good luck with your ‘law suit’ but given the power of psychiatrists to rewrite the law without the need for Parliament, I think you might be pushing crap uphill. What are y’all going to do when you find out you have no right to legal representation……. because your Bill of Rights has been “edited” by the APA?
And believe me, no one is prepared to confront the C.P. with his letter. Perhaps the cognitive dissonance it caused resulted in the lawyers and ‘advocates’ claim to have ‘unread’ the letter, rather than demand that ‘our’ rights be upheld, and the obstruction of justice cease?
Report comment
Brilliant! (Like all other Whitaker’s publications, of course)
Report comment
That was such a good response, good on you Robert- i bet hes got the magnifying glass out- cant wait for the response back…
Report comment
Thank you for the detailed essay, Robert.
What about neuroleptics?
How is the public marketing of neuroleptics at odds with the scientific evidence?
I have read Bruce Charlton’s “Why are doctors still prescribing neuroleptics?”
https://academic.oup.com/qjmed/article/99/6/417/2258701?login=false
Here is the introduction:
It is usually said, and I have said it myself, that the invention of neuroleptics was one of the major therapeutic breakthroughs of the twentieth century. But I now believe that this opinion is due for revision, indeed reversal. Neuroleptics have achieved their powerful therapeutic effects at too great a cost, and a cost which is intrinsic to their effect. The cost has been many millions of formerly-psychotic patients who are socially docile but emotionally blunted, demotivated, chronically neuroleptic-dependent, and suffering significantly increased mortality rates. Consequently, as a matter of some urgency, neuroleptic prescriptions should be curtailed to the point that they are used only as a last resort.
Report comment
I think antidepressant pills have been given not so much to treat low mood but to safeguard against skyrocketting stats on suicide. So often antidepressants have been asked for and given as a lucky talisman against death. This is how ordinary depression has become synonymous with death. There is much in life to cause despair enough to want to suicide. And suicide has become linked to rock star nihilism as if its a form of brave heroism to die young. But we have to factor in that iatrogenic effects while on pills long term may in some people make suicide all the more attractive. Hard to know what to do if one is a family doctor and a depressed person comes along with say trauma enough to want to end it that afternoon. Not easy to just say “no”. Which is why I have a huge compassion for doctors and psychiatrists caught in the tectonic expectations to provide an immediate miracle solution.
Report comment
So, does this mean I’m a point man for a host of the Khan’s barbarians when I say that depression isn’t a disease at all, but a syndrome arising from multiple conditions and that antidepressants alone don’t really treat any of them?
Report comment
Who you callin’ a barbarian, buddy? GET HIM!
Report comment
What is wrong about being motivated by animosity towards Psychiatry? How does that make you wrong by default? That animosity is a healthy and natural feeling to get motivated by.
It’s like saying you’re motivated by animosity to score the highest marks in class to shut the teacher who kept belittling you. As if that animosity somehow nullifies that achievement.
Report comment
I would love to experience a class action lawsuit against schizophrenia.com for enforcing and lecturing minors and young people that join that website about “the chemical imbalance theory” of schizophrenia. Not only do the moderators and others there lecture they Devoice, Edit, Delete Posts and Ban people that provide evidence to the contrary to their drug company propaganda, then their drug addict trolls stalk the “offenders” all over the “support” circuit of the Internet, libeling and attacking.
Report comment
mister-lister. Sounds like most of the hospital ‘programs’ designed to ‘help’ the ‘patients’ with their ‘social skills’. I was involved with a discussion with a group of patients one day at a coffee shop outing. We got around to the issue of drugs versus medicines, and one young lady said her doctor called them “products”. Long story short, I was told in no uncertain terms that such discussions was counter to the aims of the group, which was to ensure that these people followed the orders they had been given by their doctors.
Seriously? They are infantilised so much that they can’t even speak about their ‘treatments’ to others (their friends) for fear of……wanting to not take the drugs or products? And this ‘program’ was meant to help them?
I think such ‘closed shops’ as you describe are best left to their own devices. Not like they haven’t warned you that it is a delusional zone lol. They just want to drag people down to their level.
I once went to a premature ejaculators group for support, but found I was a day early.
Report comment
Kudos, and all power to the survivor and critics community in the US. We do need to fight for a legal response to the misstreatments and medical malpractice, it is outrageous how many lives are pushed to further suffering, years of life lost, people disabled and families, whole communities broken because of the hubris and prejudices, interests and all that is holding a status quo that benefits barely anyone.
Report comment
Robert, excellent description of the non-efficacy in the treatment of clinical depression with drugs, which is consistent with my review of the research literature on the subject. The only thing I would add is that the longer the depressed patient is on antidepressant drugs the worse the outcomes, which incidentally is also true with antipsychotic drugs in treating chronic schizophrenia. Psychiatrists retort to this published research by saying only the most serious cases do not respond but 80 to 90% get and stay better! To this I would add (1) both drug classes are addicting and (2) both drug classes impair the brain, which undermines the patient’s ability to learn and thereby solve distressing maladaptive life situations.
Report comment
Dr. Aftab is not only wrong about the facts, as Robert Whitaker demonstrates point by point, he is wrong about the facts and completely outclassed.
Report comment
Where does this scary term “treatment resistant depression” come from!? Can anyone even have the consideration to see how terrifying such a concept can be to someone, when the whole focus on what’s treatment, after a slew of confounding (corrupt) manipulations comes up with a total percentage of being “long term” effective for less than 3 percent of people!? 97.3 percent are “treatment resistant.” Yeah, and this is after one year. And I’m sorry but it’s not unreasonable (also given the results of such ideology when implemented that it’s a chemical imbalance) to consider that the whole premise is quite profoundly out of the ball park, so to speak. It’s like selling love spells or what the Catholic Church used to call indulgences and had to stop doing so directly, although its ideology still creates quite a call on people’s finances.
Not to be sarcastic, but what does this do to the environment, the emotional health of the society such people are in? In a “society” where after one year 97.3% looking for treatment for depression have a problem which according to mainstream, sometimes coerced, government and insurance funded “medical” treatment is then considered resistance to treatment, in other words there is no treatment for it!? SOMEHOW, I don’t think that makes the rest of the society happy. I don’t think it improves the society. EVEN THOUGH in typing this I have to laugh, because it more resembles something one would make up as a joke, as in when the crops fail slaughter another goat, your first born son, or a virgin. Oh that will help. FDA approved, folks. DO SOMETHING, DON’T JUST SIT THERE LOOKING BAFFLED OR UNCONVINCED, YOUR LIVES ARE IN DANGER! Were the true grounded statistics shared openly and honestly, no one would go for such “treatment” where after a year there’s 2.7 percent for that it “works” for. And the concept “treatment resistant,” wouldn’t be so scary as to make people think there’s something wrong with them were they 97.3% of anyone experiencing sadness believing there was “treatment” for such discomfort. And they wouldn’t have to deal with side effects, trying to get off of highly addictive medication, and thus withdrawal symptoms and iatrogenic disease they didn’t have before, the added frustration, sadness and defeat that they didn’t find what they were looking for.
And I’m just taking this lightly. How does this 2.7 percent balance off with all of the addiction, side effect, withdrawal symptoms, disability and confusion that go with the rest of the 97.3 percent. And beyond that “100%” how does this effect everyone that has to deal with the effect. All the mass shootings in association with black warning labels the drug companies tried to avoid, effects they lied about knowing before they were forced to. The added fear of normal responses to life that statistically didn’t to such a degree become disabling “diseases” before people were terrified into thinking there’s something wrong with them (supported by the fact that they can improve the lives of 2.7%, the rest being “treatment resistant”). People policing with good will an ideology that doesn’t really pan out, and all of the added frustration, and cognitive dissonance, and all of the investments in ideology, money and indoctrination that doesn’t add up.
The rest are “treatment resistant,” “non compliant,” or “misleading the public” !?
Report comment
“Treatment resistant” is a handy “explanation” for their chronic failures. There is no other industry where shortening your clients’ lifespan can be blamed on your clients!
Report comment
Sorry, I get “lost:” or rather over loaded: When I mentioned (in the prior post this is a response to): “after a slew of confounding (corrupt) manipulations comes up with a total percentage of being “long term” effective for less than 3 percent of people!? ” In supporting using the term corrupt I didn’t add the question regarding the even 2.7 percent of effectivity the drugs exhibit, how much does this come from the “2 week washout period” in the trials, where they actually took people out who already were in the trial and got better in the non control group, and thus weren’t counted. Which actually goes AGAINST the definition of washout period again, because that WAS supposed to happen BEFORE the trial, not DURING. So did they actually test people for two weeks to see if they were depressed, found they were, but if they got better AFTERWARDS without any treatment, they were “washed out” again when that goes against the very definition of wash out!? And all the rest of the games like giving people not just an anti-depressant but also a sedative because of akithesia (otherwise they weren’t getting the results they needed), of taking people already on psychiatric drugs into the trial, and not reporting how many people in the control group had to leave the trial because they had side effect that were THAT bad. Or not reporting it when there were suicides in the trial period, and then not acknowledging that effect still going on after FDA approval till they were forced to.
And HOW MANY trials did they have before they had trials they could report. If the majority of trials were so bad they didn’t report them, how could that be “science” to play all these games till you can through some deceptive device of convolution come up with WHAT!? after all of that is still quite bleak….. And then the 67% which was really 2.7 percent is the end result!?
Report comment
There is nothing scientific about it. It is all a very complex form of marketing.
Report comment
Time for an advertising break? Have you tried Brainwash? The new distillation of cognitive deviants, surely to break free any blockages, patterns of resistance in critical thinking? If so interested, pause and click .
Report comment
Fast food industry?
‘Diet resistant obesity’?
Report comment
I love it!
Report comment
There is another option to deal with “cognitive dissonance:” Accepting the fact that facts don’t fit with your conclusions to date, no matter how uncomfortable that process may be, and reconsidering those conclusions based on the new data. This is what we expect of actual SCIENTISTS, 100% of the time. Anyone who can’t deal with facts contrary to theory needs to stay far away from any scientific field!
Report comment
How does the journalist get to the “We”? When the struggle and challenge with the eye, the inner I and nature of bias can be creating waves the patterns? If the questions are not being framed to sift out a truth, then how can the understanding deepen to understand the simple as well as the complexities of dissonance in and through the cognition? Vast difference in the East to the West Coast conversation?
Report comment
If 97.3 percent seem to be treatment resistant to antidepressanting as part of treatment, is this a better result than the 99 percent being treatment resistant regarding the economy (in contrast to the 1%)? Psychiatrists only make it up to the the top 5%, though, regarding economic “health” stats. Are they doing better or worse?
Sorry, but this becomes rather difficult to take seriously. It’s like who makes it in Hollywood and who doesn’t. Who is better at hiding whatever isn’t turning up being blasted all over everywhere, with socially acceptable chase scenes involved, with holy regalia of what a hero or toy for the masses should invest in as salvation.
Report comment
“[Psychiatry] has fragile truths to defend & to provide care to those who depend on the services in an era of unprecedented need.”
When they start spouting platitudes like that, you know they are on the ropes. Let’s not let up now.
Psychiatry is not medicine. It is pseudo-medicine. They are applying the language of medicine, and the materials and methods of medicine, to problems which manifestly are not medical problems.
Do doctors who prescribe antibiotics for infections feel the need to engage in flatulent babbling about “fragile truths?”
Report comment
“flatulent babbling about “fragile truths?””
waaahahahaha
“[Psychiatry] has fragile truths to defend & to provide care to those who depend on the services in an era of unprecedented need.”
Psychiatry where I live allows the State to label anyone they wish as an “Outpatient” (sight unseen) and have police deliver them to a locked cage and do whatever they like to them and call it medicine.
Denying people access to the protection of the law in this manner can be extremely beneficial for the State. particularly when they can “edit” the documented legal narratives, to make whatever they have done to citizens into a ‘medical procedure’ conducted on a ‘patient’. And then deny them access to legal representation [or at best provide them with a shill from the Law Centre] And believe me, you really don’t want to try and make a complaint to Police…… once placed outside the protection of the law by a Community Nurse lying and calling you an “Outpatient” ….. the video of that man in Kansas (?) getting his ‘medicine’ administered? They run ‘patients’ over with vehicles here before stomping on their heads with boots. Video available on request.
Not a “fragile truth to defend” It’s a bare faced lie they cover up with fraud and slander. And the ‘care’ they are providing would be called torture if it weren’t for the “inherent in or incidental to lawful sanction” loophole in the Convention. Hence being able to make any citizen an “Outpatient” by telephone means all human and civil right s can be removed immediately, and the Chief Psychiatrist has rewritten the protections in the MHA to enable this. Not that anyone would dare look, let alone actually say something to him about his arbitrary detentions would they?
The “unprecedented need” has possibly been brought about by the paranoid delusions of the ‘elites’. The recent marriage of mental health services and police meaning that doctor can simply call the local station, and dispatch police to bring in anyone they might have an issue with. The “added protections” of the MHA ensuring that anyone who is a threat to their power (you know, anyone complaining about their misconduct, ……. ‘mental patients’) can be snatched from their beds and ‘treated’ for their “hallucinations” against their will and despite the damage to their brains.
“hallucinations”, according to police, is the belief that you have a right to the protection of the law. And I am not kidding about that. Of course as a result of the psychologist they tried to have ‘snow’ me, and the threats to his family as a result of him saying no, “it never happened”.
“flatulent babbling about “fragile truths?”” wahahahhaha Fart jokes always make me laugh.
Report comment
“As a result of human recalcitrance to acknowledge our own pathology, in the history of behavioral science, and in particular in the history of psychology and psychiatry, almost no effort has been made to gain an understanding of human pathology that has its roots in normal–as opposed to abnormal psychology. Primarily among psychiatrists there have been a few notable exceptions, including Menninger, Fromm, Peck, Milton Erickson, and others whose observations are discussed in Bartlett (2005), all of whom have had the courage to recognize the pathological constitution of the ordinary person who so often is a willing participant in inflicting suffering, death, and destruction. But despite the work of these few researchers, psychology and psychiatry have doggedly reserved the term `pathology’ exclusively for application to individuals and groups judged to be abnormal, that is, whose psychology deviates from the norm. This, as Bartlett (2005) attempts to show, is short-sightedness in the extreme”
From Steven James Bartlett’s book: “Normality Does Not Equal Mental Health: The Need to Look Elsewhere for Standards of Good Psychological Health”
I sent a hardback to Whitaker years ago hoping he or someone in MIA would do a generous review on Bartlett’s book. Heck, if I was a journalist, I’d ask Dr. Bartlett for a lengthy video interview because his cause is no different than MIA’s. To me, Dr. Bartlett is a scholar par excellence as his body of work reveals it.
Report comment
When they start babbling about Q-Anon, you know they’ve lost the argument. The only time I EVER hear anyone talking about Q-Anon — the ONLY time — is when people like Awais Aftab use Q-Anon as a straw man to support suppressing any opinion they don’t like.
Report comment
Using the law: This reminds me of the work of Robert Carter, PhD, who studies race-based trauma, especially how it shows up in the workplace and causes financial as well as mental and physical adverse effects on its victims.
When asked why he does not try to get this disorder into the DSM, he said (according to my recollection), the heck with that, that would change nothing and put more money in the pockets of the wrong people. It’s money that gets people’s attention and gets them to make changes, so he works on helping people sue and get monetary compensation for the damage done to them. One case, one corporation at a time. So maybe hit the wallet of one psychiatrist, one facility, one professional organization at a time…
Report comment
“When I was seeing patients, I never used the chemical imbalance theory, but instead that serotonin seemed to be increased in the brain with SSRIs.”
I’m very confused. Your comment is incredibly confusing grammatically, including that it seems to be omitting words. There should be a word or phrase after “instead” and before “that,” for that sentence to make sense. Examples might be:
Explained
Told patients
Assumed
Guessed
Conjectured
If you told patients, or if you just assumed, that serotonin seem to be increased with SSRIs, how did you *not* use the chemical imbalance theory? Did you say, I don’t believe serotonin has anything to do with mood however I’m going to prescribe something that seems to increase serotonin in your brain…. just because”?
Report comment
Let me put aside what some would think to be just the innocent mistakes that Mr. Whitaker made in his August 13th article about Psychiatric Times and the spelling of my name. Though perhaps irrelevant for his points, they point out carelessness with the truth.
I think what is important to discuss is the real life clinical work of many psychiatrists because even the best quality studies are not the same as everyday clinical work. When I was seeing patients, I never used the chemical imbalance theory, but instead that serotonin seemed to be increased in the brain with SSRIs. I was never all that enamored with the results overall, but many individual patients did well. Almost always, joint treatment with psychotherapy enhanced the results. The truth is: we don’t really know what is going on in the brain in the deepest and most important ways with depression, probably because the brain is so well protected, making usually research very difficult.
What we also keep forgetting are the for-profit systems that greatly influence treatment settings. These are the for-profit insurance companies, managed care companies, and Pharma. In many meetings, only 10-15 minutes are left to see each patient. That is absurd. (See my book The Ethical Way: Challenges & Solutions for Managed Behavioral Healthcare, 1997). They are our real mutual enemies. No wonder mental health workers from Kaiser Northern California are on strike.
I once write for this publication, but the animosity towards any psychiatrist that didn’t fall in line with the going criticisms of psychiatry made it worthless to continue. Not much is liable to improve unless we can work together more and improve the systems care care and future research.
Report comment
With all due respect, is it possible that the reason we “don’t know what’s going on in the brain in the deepest and most important ways with depression” is because we’re making an errant assumption that all depression is related to something “going on in the brain?” If that assumption is wrong, every attempt to discover “the answer” will fail to provide an answer, because we are barking up the wrong tree. That seems to be what the research is showing. Sixty years later, we still don’t know of a biological ’cause’ for depression, despite billions of dollars and millions of person-hours dedicated to the project. At what point do we admit that this is most likely because there IS no biological cause? What if “depression” is simply a description of a very complex state that organisms go into when exposed to a threat they can’t immediately manage? Would not then each case of “depression” result from potentially completely different “causes,” with the only thing shared in common being the depressive experience? Pain is a great analogy. What is the biological cause of pain? Is it certain neurons firing in a certain pattern? Or is it putting one’s hand on the stove or getting one’s foot run over by a car or being unable to digest X or Y or having a cancerous growth on an organ or experiencing extreme emotional distress that is expressed as physical pain or just not getting enough sleep for 5 nights in a row?
Why is the psychiatric profession so dedicated to proving a proposition that has yielded no deep understanding of the situation despite over 60 years of intensive research? When is it time to admit that the theory you’re investigating simply is incorrect, and start on a new hypothesis?
Report comment
All I meant by “going on in the brain” is what happens in the brain for any sort of mental disturbance, including “a very complex state” of trauma. That understanding may or may not help healing. There was no intent whatsoever to claim a biological cause, but rather a biological reflection of our inner and/or outer worlds.
Report comment
I’m glad we are on the same page. Then I challenge you in this way: are you suggesting that most of your colleagues are NOT using the idea that drugs are the solution because these issues are primarily biological in nature? Does the evidence not suggest that such colleagues (and reading the comments here should disabuse you of any notion that your views are in the majority) continue to spend most of their time and energy trying to promote or prove that biological solutions are the best solutions? What else does the average psychiatrist have to offer besides the drugs?
Whether or not it is stated overtly, in practice, the basic business of psychiatry appears to be to get people taking pills. And what about the hostility that Dr. Moncrieff has received for simply stating the scientific conclusion that 50-60 years of research has provided: that a serotonin imbalance is NOT associated with major depression. If the psychiatric profession is NOT invested in promoting primary biological explanations for “mental illness,” why is it so upsetting to have the actual science on that question reported?
Report comment
As I’ve tried to say, my fellow Steve, most psychiatrists try to do their best under pretty oppressive work situations over the last decade or two, resulting in an epidemic of our burning out. No, I’m not asking for any sympathy, just trying to point out again the system problems surrounding us all.
In view of these system problems, most clinical psychiatrists try to do what they can under very limited time, and that is medication. The serotonin issue is a red herring here. That same time pressure produces a need on both sides – us and patients – to try to make some sense, even the powerful placebo sense, of whatever practical steps are taken. I can assure you that most psychiatrists would like to have more time to do more psychotherapy. As to the uproar, most everyday psychiatrists couldn’t care less about this controversy; they just want to plug away and help wherever they can.
DSM 5 is a major problem and surely misleading. One growing alternative is a network perspective on psychological symptoms, pioneered by the Dutch psychometrician Denny Borsboom and colleagues. Depression in this viewpoint arises from a network of interactions among its constituent elements. Treatment then addresses those elements.
Report comment
Well, I am sure that most on the front lines psychiatrists do their best and probably believe sincerely they are being helpful. What I don’t understand is why the thought leaders are so committed to biological explanations. It can not be a result of not having enough time. People in high places continue to alter the known research in order to continue to justify biological treatments.
A very simple example: Stimulants are claimed to be effective in “reducing the core symptoms of ADHD.” However, decades of long-term research have shown little to no benefit in ANY long-term outcome. This was first observed in 1978 by none other than Russell Barkley. It has been the same result in 1993 (Swanson) and 2003 (OSU medication effectiveness study). Several long-term naturalistic studies (Quebec, Raine, MTA, Finnish/USA comparison) have supported these findings. It was demonstrated in the 1970s that open classrooms work very well for these kids, to the extent that professionals can’t even tell them apart from “normals” in this kind of setting. It has also repeatedly and undeniably been demonstrated that fully a third of “ADHD” cases go away if you simply wait a year before enrolling a child in kindergarten.
So why are we still insisting that ‘untreated ADHD’ leads to negative outcomes, when “treatment” does not improve them? Why is it insisted that ADHD is a biological problem that requires a biological solution, when it appears that a change of setting resolves most of the “symptoms”? Why is most of the research money still invested in “medication?” It’s not because clinicians don’t have enough time in the field. It is because the profession supports biological research even when the data does not support it.
This is most definitely not about “serotonin.” It is about psychiatry as a profession/industry needing to continue to support “medication” as a primary intervention, because that’s where they make their money. As an INDUSTRY, not as individuals. So sure, the system is designed so that doing therapy is not remunerative, that “med checks” make more money in less time, and so that people who question the biological paradigm (like Moncrieff) are attacked for doing so. It is easier to follow the path of least resistance. But what that means is providing “services” that are either ineffective or sometimes destructive over time, meanwhile making any other approach unable to be researched and so criticized as “not evidence based.” All the while spreading misinformation about the nature of these “disorders,” which are in actual point of fact simply descriptions of sets of “symptoms” that tend to occur together. Perhaps the most egregious damage is the prevention of research into ACTUAL causes of these “syndromes,” because we spend our money researching the DSM categories which embrace totally heterogeneous groups.
I’m not asking you to fix all of this, or even explain it. I’m asking you to acknowledge that psychiatry AS AN INSTITUTION is committed to following the biological track, regardless of whether it leads to results or not, and are frequently quite hostile to folks like Bob and Joanna who have the temerity to point out the facts that diverge from their desired narrative. Why else would Joanna be so roundly attacked for presenting information that supposedly “psychiatrists have known for years?” If psychiatry has known this for years, why else would official sites and training literature and even textbooks continue to portray this falsehood as truth? And why is the search for some “deeper biological reality” instead of being willing to question whether the quest for biological explanations is simply misguided and should be dropped for some more fruitful path? It is hard to deny that psychiatry is not on this path by accident, and that it is committed to biological explanations in a way that a scientific enterprise can not be allowed to be.
Report comment
I”m again rather astounded at the rather veiled attempt to hide what ends up being projections of what would CAUSE one to believe what works, what doesn’t, and a whole intimidation of what’s realistic and what isn’t.
“most psychiatrists try to do their best under pretty oppressive work situations over the last decade or two, resulting in an epidemic of our burning out”
“In view of these system problems, most clinical psychiatrists try to do what they can under very limited time, and that is medication.”
Where is the epidemic, and which system is oppressive to whom, and what can be done? Adding to an epidemic (on either side) is hardly doing what one can under limited time, when one’s job is to tend to it. FURTHER MORE, Saying the psychiatrist and the patient have to work together, while EXCUSING with watered down propaganda or slight of hand remarks (using the term medication erroneously) so that the Psychiatrist is not only allowed but expected to lie to the patient. The patient being someone already under EXTREME distress looking for an answer or answers, or having been put in a situation by othesr that they don’t understand and find oppressive: waving the flag of “we-did-something-we-medicated,” once again returns to something akin to the “stress reduction” of sacrificing a goat, a virgin or your first born son. You DIDN’T medicate, neither does the placebo effect turn it into that.
STOP misusing the English language.
And poor Steve has to try to respond to this, which I can imagine becomes being at such a loss for words that the phrase “path of least resistance” comes up. Least resistance to what? Yeah seems easier doesn’t it? Might that have to do with the epidemic (the burn out of the psychiatrists as well as the increase in the problem they are said to be tending to). Getting lost in a maze that’s highly deceptive isn’t even really a path, that’s how you get lost. The path of least resistance to not being a path…..
And the rest is excuses.
I completely don’t see how advertising “I never went for the chemical imbalance theory” spiced up with “I stated that SSRI’s seem to increase serotonin,” how this is not avoiding articulately caring about a patient. The difference might be dismiss-able between treating chemical imbalance[S] and saying that increasing said substance helps depression, but dissolves when one points out your (and you are) [you’re] as “spelling” mistakes go) ADVERTISING messing around with brain chemistry and denying chemical imbalance (that would be what the anti-depressants cause, which isn’t theory it’s proven science); added to this anti-depressants don’t “seem” to increase serotonin, they block the re-uptake which increases the amount left over because the brain has been GIVEN a chemical imbalance by the “medication”, then the brain stops making as much [serotonin], and you have less. That’s no explanation, it’s avoiding an explanation, it’s not informed consent, it’s not true, and sorry but this becomes a problem when one gets a degree in medicine to habituate such statements, to have others believe it is authoritative. It’s actually AGAINST true medical science.
Consistently making watered down highly triggering statements to already overloaded confused people, who if they don’t have the matrix, the syntax, to look past the deception are going to feel it, this is highly insensitive. People already feeling overloaded consequently getting more stressed out; and then when someone DOES have the syntax to see how they are being deceived, won’t excuse the cloaking rhetoric, to then call them agitated (delusional, whatever it takes to fit them into the “medication” matrix), and say that is: “animosity towards any psychiatrist that didn’t fall in line with the going criticisms of psychiatry.”
No, it’s not OK to spin out a second untruth, acting like you’re helping those who could see past the first one.
And it’s not going to work, and it’s redundant….
Also, I think that it’s “systemic problems” not system problems. System isn’t an adjective, you can’t use it color whatever as if it being a “system” it’s one of those constructions that works, or you have, or it’s a good idea to stay with it to be part of things. It’s problems of that system, not “system problems,” I think. Which in other cases is problems of “the system.”
Report comment
So what do we do with the ‘problems’ if their is no hope of a cure?
Not again.
Report comment
Imagine a bath half full of water. Then take a marker pen and scibble around the sides of it names like heart and spleen and gametes and liver and bowel and bladder and womb and even consciousness if you wish. And lastly scribble at the top the word “brain”. The water or fluid that affects the heart and spleen and liver and so on and so forth is the same fluid that one way or another affects the brain. It is not as if the brain is in a separate partitioned off splendid isolation position within the body of water within the bath tub. The fluid of LIFE goes EVERYWHERE and affects all organs and systems. So I believe that when a person feels “heartbroken” it will increase their chance of a heart attack and it will also affect the brain that is in the same fluid one way or another.
I think the prevailing view here that says nothing can go wrong with the brain is naive.
I think the alarm over the idea that things can go wobbly within our entire bodies and bodily systems is because these bodily areas have been treated so atrociously by psychiatry.
But I shall not let past history taint the way the brain belongs to the whole body and the whole body belongs to the brain.
Many a young woman madly in love knows that having her “heart” so radient on this fluid of love causes her brain to become befevered with rapture such that she can barely utter a word of sense.
People should not be for the decoupling of the brain from the beautiful body. THAT is what psychiatry of old kept doing and THAT is why there is a knee jerk animosity to mere mention of the brain, as if saying…
“Hands off our brains”. As if the brain has gone into hiding and its whereabouts cannot even be spoken of in a comment lest it become the property of bad medicine again.
I think it is a shame to let the way the brain has been mistreated stop it from sharing the company of the rest of the body, where it belongs. Sharing company of the rest of the body, holistically, for the orphaned brain, is a homecoming basic human right.
I say all of this because at times it seems like people want to partition off the top section of the bath and declare that the water that envelopes the human brain is utterly divorced from the systems that reside in the rest of the whole body. Excitingly, for new paradigms of care, a more holistic vision is being born, but to leave out the brain for fear that mentioning it might generate lucrative bad treatment of it, leaves it aside like an amonite fossil. It is similar to the way pregnant mothers get jittery at anyone even mentioning foetuses. The delicate promise of life must be veiled in secrecy lest it be dragged out into the harsh light of a soulless laboritory and chipped away at like a hard fossil.
These are the nuances I hear in all the arguments. But I must cease my nuance super sleuthing as it gets me no respect.
Report comment
I object to the statement that the “prevailing view” is that nothing can be wrong with a brain. I haven’t heard anyone say that at all. Just for the record.
But I do get what you are saying, and it ought to be carefully considered, whatever “treatment” is being administered. The mind affects the whole body (including the brain), and the body affects the mind. The idea that some little spot in a brain can be “treated” and have no effect on the rest of the body is a very dangerous idea. But it’s also true that imagining the body can be ignored when working on the mind can lead to a lot of errors and potential damage. Psychotherapy for Lyme Disease is not going to help any more than giving antidepressants to a mother in a domestic abuse situation. Everyone is different and deserves an individualized approach not based on dogmatic insistence of the “helper” that their approach is the RIGHT way regardless of how the poor client feels or reacts!
Report comment
We don’t yet understand how the chemistry of the paint makes people appreciate the aesthetic beauty of French impressionistic paintings. We only know that it plays a critical role in some way.
Report comment
Excellent example! But since not ALL people appreciate French impressionists, there must be SOMETHING wrong in the brains of those who fail to recognize their beauty!
Report comment
LSD can help with that. And it would then be correcting the chemical imbalance causing the disorder. Which would please my local drug dealer no end, because his function in society would take a step in the right direction. Having police deliver his ‘clients’ to him handcuffed and being able to force them to take their ‘medicine’…. for a fee.
Report comment
Well, at least the “involuntary clients” aka prisoners would have some lovely artwork to look at!
Report comment
Via the process of backward reasoning, the authors of the 1980 French-based DSM alternative concluded that people who failed to appreciate French impressionist paintings presumably suffered from a chemical imbalance, most likely a deficiency of lead. Subsequent theorists posited the issue could be explained by broader dysregulation in the brain’s lead system. Currently, more sophisticated theorists have speculated about the complex interplay between relative surpluses or deficiencies, or various unknown complex interactions thereof, related to lead, cobalt, manganese, cadmium and chromium. Despite these intriguing hypotheses, the emergence of brain imaging and genetic testing technologies, and the increasingly molecular nature of our understanding of paint and paint-related chemicals in the brain and body, these theories remain speculative yet intriguing. That is why the painting industry has pledged $2 billion in research support through 2030, making the 2020s the French “decade of paint.” Unfortunately, to date, neuroscientists (who receive 92% of taxpayer-supported research grants into French impressionist paintings), have yet to confirm these intriguing hypotheses or determine in which parts of the brain and body they might manifest. The French NIMH director counterpart, Jacques Gordone, theorizes there may be a complex, heretofore unknown to anatomists, bodily circuit related to paint-related chemicals determining French impressionist painting assessment and ability, which can best be studied at the molecular or possibly even sub-atomic level. Such research, so his director’s blogs say, may hold the key to revitalizing and revolutionizing the French impressionist painting industry, thereby catapulting French society into a new golden age.
(Steve: mic drop – your turn!)
Report comment
I can say no more to expound upon this enlightening theory! Thanks for the laughs!
Report comment
I was so astounded by this immense wisdom from Brent Deacon PhD, and the unceasing alacrity behind it, that it has taken me this long (THREE WEEKS!) to remember I also have encountered the same truths elsewhere: was it in thought or did an angel tell me?
This regards American corn.
You may think this is just something thrown out of society and forced to do its business in the fields, but no! It has a long history, and immense indigenous help and respect, something akin to the holy land. Very much the same as Israel needs nuclear defense, corn needs fertilizer and pesticides. Yes, the same as that French impressionist paintings couldn’t exist without the lead in them, something called poison by the unenlightened. NAY I say to it being poison, and YAY I say to the fact that it must have universal properties, the magic of alchemy and it is our duty to see that in reality it is GOLD! Putting as much money as Brent Deacon has pointed out is necessary is just a beginning, a beginning in finding the nature of our origins. How could money be put into the new James Web space telescope, and not into finding the alchemy of lead (which is an ingredient in the most beautiful paintings ever to emerge out of human consciousness)!?
But now corn, and fertilizer and insecticide. And genetics too, forsook I almost forgot that this was mentioned to me. It being of such immense substance and distinction that I fail to recall if it just floated into my mind, or did a friend from Heaven speak to me. Of course there’s something genetic going on with anyone that has problems with what has turned corn into an international source of experiencing the American Spirit, something heralding nature and indigenous spirit as well: insecticide and fertilizer have done this. In turn, we must find genetic flaws with anyone not supporting these spiritual buttresses! Our origins as sentient life and the Universe depend on it! The same, when you see someone walking around naked, in OUR society, don’t you immediately respond with alarm!? Can you imagine people seeing this and not being alarmed? Isn’t that ALSO a sign of chemical imbalance on THEIR part as well as genetic abnormalities that MUST be investigated? This is WHY the legal system can force a person in to treatment! To save their soul!
Just as we must investigate how lead must be what leads to Gold, what Brent Deacon has pointed out is in the process thanks to much good will, we MUST find the gold in corn as well, and look into how what has made it bless the rest of this little wonder of a planet, that being insecticide and fertilizer, how those two MUST be inherent in natural processes such as thought! If insecticide and fertilizer can help a plant blossom out of the soil, so MUST IT be fundamental in how thought blossoms out of the brain! There HAS TO be a chemical link there!
Report comment
Holy Shit! again.
To begin with, regards for the truth is in the content, not in spelling someone’s name. Further more (AGAIN) SSRIs do not increase serotonin, they for a few weeks might do that, but then the brain compensates, and there’s less serotonin. That’s also the truth (not what “seems” to be going on), regardless of how I spell serotonin. To then talk about the “deepest” and “most important ways” not being known, after making erroneous statements about what is known regarding SSRIs using generic statements from an industry that numerous times has tried to make out that the clear scientific evidence pointing out how their treatments damage the brain is the result of what they call “diseases:” this further isn’t going to herald the truth, no matter how much you put together such propaganda with correct spelling. Neither is calling such industries our “mutual” enemy, while perpetuating their fraudulent statements.
Bizarre nebulous statement such as: “I was never all that enamored with the results overall, but many individual patients did well. Almost always, joint treatment with psychotherapy enhanced the results.” Also do nothing but promote complacency regarding something that is already said to not really work that well (if at all), as if implying that when one isn’t enamored one is critical enough, and then bring in anecdotal evidence. How those people are doing does not depend on what you believe is going on, nor what you report here as “many individual patients did well” nor whether or not desperate people come to you for help (as little as that people regularly going to Mac Donald’s for food are indulging in healthy nutrition when they keep going there), or whether you make enough money to try to humiliate people that are interested in the truth, and have the leisure to be fussing about spelling mistakes rather than content. We would have to talk to those patients themselves, and also the ones that tried to get help but left.
Someone that truly is interested in helping others with challenges involving cognition I think would have deeper understanding of life that trying to promote that correct spelling determines whether someone is interested in the truth. Further more caring to use correct spelling to disassociate from the truth, and pepper this with such deceptive logic when the truth is indeed challenging, to say that that is how one deals with depression, is more using sadness as an excuse to AVOID the truth and disable the mind from having the courage to face it. And THERE you have your “disease.”
Fussing about spelling, reiterating false statements, using anecdotal stories, the rest of it and who knows what else this is about avoiding the truth, THAT is not something Robert Whitaker indulges in.
It becomes abusive when someone made out to be professional repeatedly hauls out such games, it takes a populous of people having been through such lies to have to straighten them out, and then once again hear such a “professional” say it’s worthless to continue respecting those who simply try to express how their lives were ruined, because of the lies, and the indifference.
Report comment
I didn’t even catch this at first, but is this REALLY an attempt to display the ability to diagnose? Spelling mistakes are a symptom of disregard for the truth because of carelessness?
How many people believe this?
Might it be the other way around. I think spelling is something one is taught by rote, it’s not inherent in the truth, given history it certainly isn’t permanent. And this regarding the English language where there are so many variables regarding spelling that it can be quite irrelevant of pronunciation.
And to start such a whole fallacy with the idea that there aren’t just “innocent” mistakes going on and “some people” might think there are….
Is THIS an innocent mistake!? Here:
“I think what is important to discuss is the real life clinical work of many psychiatrists because even the best quality studies are not the same as everyday clinical work. When I was seeing patients, I never used the chemical imbalance theory, but instead that serotonin seemed to be increased in the brain with SSRIs.”
Overlooking clear evidence in studies by promoting anecdotal evidence and supporting a marketing ploy about antidepressants which doesn’t pan out but is the opposite (in the long run antidepressants cause less serotonin)….
One wonders what other kind of excursions into “magical” statements one is to encounter would one continue, this regarding someone trying to point out mistakes that aren’t “innocent.”
There’s a difference between lack of innocence, and lack of indoctrination, or lack of brainwashing…..
Report comment
“It is said that one should not hesitate to correct himself when he has made a mistake. If he corrects himself without the least bit of delay, his mistakes will quickly disappear. But when he tries to cover up a mistake, it will become all the more unbecoming and painful. When words that one should not use slip out, if one will speak his mind quickly and clearly, those words will have no effect and he will not be obstructed to worry. If there is, however, someone who blames a person for such a thing, one should be prepared to say something like, “I have explained the reason for my careless speech. There is nothing else to be done if you will not listen to reason. Since I said it unwittingly, it should be the same as if you didn’t hear it. No one can evade blame.”
Hagakure, Yamamoto (did I spell that right?)
Speaking of cover up of mistakes, and the consequences……. how unbecoming and painful must it be to continue flogging the dead horse while people watch?
Why does Balaams Donkey come to mind?
Cast
Balaam played by ‘the psychiatrist’
Donkey played by ‘the patients’
Balak played by ‘the drug companies’
Are you sure we can’t pay to to forgo “First do no harm” and tell a “noble lie”? A little bit of snake oil never hurt nobody right?
Report comment
https://www.fiercepharma.com/pharma/fda-approval-axsome-touts-auvelity-potential-game-changer-treatment-depression
Meanwhile, a new antidepressant is headed to the market, notwithstanding the fact that we don’t understand anything about the brain.
Report comment
How long until they figure out Zyprexa blocks the effects?
Report comment
https://www.nytimes.com/2022/08/27/health/teens-psychiatric-drugs.html
…was surprised to see this article on the front page of the NY Times. It profiles a teenager who was poly-drugged.
Report comment
Don’t get your hopes up, the NYT published the ‘Zyprexa Papers’ and now it’s in a new form and back under patent.
It’s like the doctors are passing around a rubics cube in a circle with each doctor using a different strategy and not being able to figure out why their strategy doesn’t work.
Report comment
Yep, it’s obvious from the comments section of that article that the “professionals” just want to dig in their heels and blame everything under the sun except for their own “treatment practices”. Some of the psychiatrists commenting are accusing the NY Times of having an “anti-psychiatry bias”, which couldn’t be farther from the truth. The fact that they put this article on their front page just shows how big the problem is (and that even privileged, college bound teens with “good” parents aren’t safe from being poly drugged.)
Report comment
As someone who had great insurance as a teenager in 90’s I can can tell you it is not much better. Inpatient stays were based on how many days your insurance covered instead of any medical need. I think they overtreated the kids with good insurance to offset the insurance with lower payouts.
Report comment
Let me be the first to agree, Steve!
I would put it like this. If we stop asking ‘What causes depression?’ – as if ‘depression’ is a ‘thing’ and indeed a unitary ‘thing’ – and instead, ask ‘What causes people to feel desperate, hopeless, anguished, miserable and suicidal?’ – then the only possible answer is ‘Lots of things.’ And if you explore what those ‘lots of things’ might be in any particular case – which will vary, although there will be common themes – then you may be able to suggest a way forward. And it will be pretty obvious that the answer will not be found in a pill.
Report comment
Very well said. It appears we agree once again wholeheartedly!
In my time as a therapist, I always assumed I knew NOTHING about a person I met, regardless of what I might have read in the file. I always knew that if anyone had the answer, it was the person in front of me, and it was my job to help them tell me about it, verbally or nonverbally. And every single situation had different contexts and reasons and possible solutions. Sometimes I had to be very quick on my feet and try something totally off the wall! And the most off the wall strategies almost always worked!
The fact that the person was “depressed” told me exactly NOTHING about what I had to do. I considered “diagnoses” mostly a waste of time, if not a detriment to progress. Every single case is different!
Report comment
Agree!
Report comment
I’m sorry but having so recently been in suicidal cliff dropping desperation I know for me that had I not imbibed something I would have been a goner. There is a valid argument about what ought not to be imbibed but often at such a doomy crossroads time is of the essence and so convenient “fixes” are the miracle choice people do seem eager to opt for. Suicidal states are not just a low mood, they can have multiple unfixable reasons behind them, such as a cancer diagnosis. My late husband killed himself after that diagnosis. People who are suicidal do not get better all of a sudden with a popsicle and a cheek pinch. They crave a profound release from suffering RIGHT NOW.
I only say this, and it is not to disagree with other things you say, but just to highlight that one can see HOW doctors and family got to the exhausted point of agreeing to the suicidal person’s high hope in the flimsy dream of curative potions. Take the potions away, such as they are, but they could have bought placebo “time”, which is not to be smirked at, when not even love will make a dying person revive.
Time flies when you are dragged underneath time and you cannot even slow time enough to escape it.
Report comment
Not sure how accurate the attached is, but maybe the “right to vote” is contingent… “Laws in 39 states and Washington, D.C., allow judges to strip voting rights from people with mental disorders ranging from schizophrenia to Down syndrome who are deemed “incapacitated” or “incompetent.” Some of those states use archaic language like “idiots” or “insane persons” in their statutes.” https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2018/03/21/thousands-lose-right-to-vote-under-incompetence-laws
Report comment
Some of those states use archaic language like “idiots” or “insane persons” in their statutes.
And that’s ‘archaic’ language? These would be considered respectful terms by any ‘patient’ who had the misfortune to have been dealt with by OUR police. Some of the terms they use not really technically included in the DSM, but we know what they mean by the terms “window lickers”, “nut jobs” and “psychos”. The nuances and subtleties of the language can be sorted out by the wordsmiths doing the ‘verballing’ at the ‘hospital’.
Report comment
What can possibly go wrong eh? A backlash may be coming. It may be against what it perceives as “whining demanding entitled people” who use their “mental illness” as “excuses” to drop out of social responsibility by pressuring people to regard themselves as long suffering victims. It will be an attempt to erase the term mental illness. But along with it will be an attempt to dismiss the extent and phenomena of “trauma”, as if “mental illness” and “trauma” and “victim mentality” are all part of the same thing, as though that cluster denotes self indulgent, self pitying attitudes worn like medals of weakness. After that no one may be “allowed” to say they feel particularly upset about anything, not even child abuse. Alternatively a different backlash may be about saying that people who say they are traumatized are liars who need sent to metaphorical or actual hospital to get their diagnosis of mental illness writ large. So a return of merciless authoritarianism. Neither of these respect the basic human right of the individual to freely choose to hold differences of opinion.
So one backlash says “mental illness” and “trauma” and “victim declaring” are all abdecations of social responsibilty and resilience and are avoidance of putting others first. And the other backlash is the clamping down of “the social contageon” of “trauma” by calling outbreaks of that “social contageon” so bad for society that it is like a mental illness left untreated.
I am “for” each dear individual having their OWN CHOICE.
It is just that my own choice for “me” alone is not especially popular. But neither was Christianity at certain times in history.
Report comment
What we are all learning of is the vital connection between personal free choice and wellbeing. We are learing this by every individual on the planet who bind to any “side” getting their own personal choice villified unendingly by opposition who want to impose control over free choice and lecture those choices to be different…and lecture menacingly. This menacing of each other turns each person into a mini nuke. On a planet bristling with springloaded nukes. So the other learning, aside from how precious each individual’s own free choice to see life the way they uniquely see it is, is the learning of how few choices are worth Armagedon for.
That tension requires a keen understanding of the importance of flexible, yin yang, give and take, easy natured BALANCE. Yes, your wellbeing matters hugely. Yes, your choice to have strawberry ice cream is essential to who you feel you are. No choice like strawberry ice cream is worth incinerating the globe over.
Humans are having to get to grips with how to have their hearts desires and choices fullfilled but “constructively” not “destructively”.
Humans must cooperate with nature “constructively” not “destructively”.
Report comment
That is so beautifully written Diaphanous Weeping…. I love reading your writing, the way it flows. The deep resonant colors….
No choices are worth Armagedon…
Report comment
Aw Thank you Njinsky. I feel honoured to read your reply. Your comments have been insightful and truth talking to me.
Report comment
Just to let you know Daiphanous Weeping, I got off of sugar a year or two ago, and I wouldn’t want strawberry ice cream for the life of me. A healer name Charlie Goldsmith stresses how we are brainwashed with advertising to go for certain foods, and they have addicting stuff in them (MSG, sugar, salt, who knows what else) and everything tastes so much better without sugar, actually. Simple meals are like from Heaven, instead. Fried eggs with rice, some beans 9kidney, garbanzo, etc.), maybe some vegetables and curry powder, that’s like from Heaven, so are many other things. So, no worry regarding me needing that fix of strawberry ice cream and investing in nukes to defend it. Goes pretty much for everything, or anything else needing such backing, I’d think.
Report comment
https://images.app.goo.gl/ttUgXBsNJ35vbbY67
When ticklish feet form a nuclear silo shape in order to share the choice of strawberries.
Report comment
Bob, Thank you for again distilling and presenting the abysmal findings of antidepressant research! You continue to give me courage to not follow the pack in my field. Your writing and work give me much needed encouragement and backing and to treat depressed patients without using pharmaceuticals. Until we can make real systemic change, I will keep sharing the message and keep finding other ways to help people- one suffering person at a time. Best regards! Tricia
Report comment
Holy Moses, psychiatry’s relationship with Police on display.
Not sure if police are using mental health services to extract information from ‘citizens’ (who are easily made “Outpatients” for the purpose of ‘coercing’ and well….. torturing if you consider the unlawful detention a means to exploits the loophole of the Convention. Not applicable in the US hence possibly a lack of understanding of how to do this).
As you can imagine, the ability to use doctors such as Selwyn Leeks for the ‘treatment’ of ‘patients’, and of course providing the doctor with a list of questions you would like answered is of great benefit to the State. In fact, so much that they are enabling the “editing” of legal narratives and the concealment of crimes committed by public officers to get people the ‘treatment’ they need ……….to have them ‘confess’ or provide the information required by police.
I sort of accidentally came across this when the Police thought they had retrieved documents showing them doing arbitrary detentions for mental health, who in turn torture and then conceal that torture with “editing” of legal narrative. “inherent in or incidental to lawful sanction” makes it NOT torture, hence the “edited” narrative changes the act post hoc.
Denial of access to legal representation, and the most bizarre letter of response from the Chief Psychiatrist (yeah, we know …… it’s sometimes necessary to torture, and we will look the other way while you enable it) doing a cover up.
Problem being that I still had the documents showing the crimes….. so police concealing the ‘little arrangement’ they have with mental health services to exploit the unique position they find themselves in (in return for some assistance with arbitrary detentions) being exposed? So then they had to steal my laptop, and threaten the psychologist I had been speaking to and have him find out “Who else has got the documents?”
I mean, don’t get me wrong, I’ve got no real problem with police torturing people, and in fact no real problem with the ….ehem…… ‘unintended negative outcomes’ being done by the State to ensure their reputation isn’t tarnished. I mean people are not going to willingly attend these services if they are aware of their real function (thinking of the shower trick here, always leave them with that faint glimmer of hope that “They wouldn’t do that”).
But I do have a problem with a Private Clinic psychologist with a Masters degree selling information to the public as to how they can use the little ‘coercion program’ being run by police and mental health to have someone kidnapped and subjected to torture. The State then responsible for mopping up the mess with their “editing”.
And then there is the problems caused by what to do with the ‘complainant’, given that police are now looking the other way while ‘doctor’ extracts the information with the chemical kosh or electricity. Thankfully someone interrupted that little accident that was arranged but …….. then they had to cover up because the State can’t have these people being held to account…… they’re enabling them in their human rights abusing (and setting up plausible deniability as a means of defending their positions) In the case of the Chief Psychiatrist actually removing the protections afforded the community by the law (care to see the letter anyone?)
If police are arbitrarily detaining and using mental health to torture, and mental health are then “editing” the documents and police refuse to take evidence of that “editing” and identify the offences?
Yeah I get it why y’all are not looking at the documents.
Wander in the desert for 40 years with your ‘chemical imbalance’ myth. Worshiping the golden calf?
They’ve been covering up police using mental health for purposes other than designed. That really is disgraceful when you think about it, and no wonder they simply ignore the facts ….. because the truth would expose their cognitive dissonance regarding their outward claim of honor, and their inward belief that sometimes a little torture can be for good right?
$200, and a little bit of preparation for access to the State sanctioned kidnapping and torture program? Bargain if you ask me, because they took everything, and I mean everything. And now, despite being fully aware of the level of offending, they simply ignore the truth.
Still imagine if police didn’t have access to a means of torturing citizens using mental health services as ‘informants’ and some of the more zealous ‘practitioners’ who will actively harm to obtain information?
The police sure will miss Selwyn Leeks. The use of an ECT machine on the testicles of a 12 year old boy?
https://www.youtube.com/watch?v=2LE0KpcP05I
Report comment
Once again, Robert, you’ve hit several nails squarely on the head in this rebuttal to Dr. Aftabs criticism of your “Psychiatry, Fraud and the Case for a Class-Action Lawsuit”. One of those nails:
“This is why psychiatry cannot be expected to reform itself. The guild simply can’t bear to confront the reality of its own research. Perhaps public pressure could force such change, but medical professions in the U.S. are treated by the mainstream media as speaking with authority, and that limits the possibility of public pressure as a change agent. That leaves the law as the only possible lever for prompting such wholesale reform.”
Yes, indeed…and I learned, very sadly, that the legal profession holds doctors in similar unassailable high esteem. My wife and I were in the process of renewing guardianship of our daughter, for the express purpose of protecting her from the potential ravages of psychiatric coercion. The attorney working with us cautioned us not to criticize psychiatrists in the process, because “judges regard doctors with near reverence.” We were relieved that our guardianship was renewed but, sadly, it turned out to be useless in stopping the hospital psychiatrists from forcibly brain-shocking her and then forcing her onto a medication that was contraindicated by genetic testing and that induced terrible side effects and started a cascade of additional psych meds. As you know, her story (published here on the first anniversary of her death, July 29) had a very tragic ending.
I agree that lawsuits may be the only way to effect change, but when you understand just how stacked the deck is it is not at all encouraging. It is virtually impossible to find an attorney or law firm that will take on any case against psychiatry, at least when it comes to medical malpractice. But your suggested class action suit would not involve medical malpractice, per se, so maybe there’s a better chance.
I’m not dismissing the legal avenue, but I’ve come to believe that the “court of public opinion” may be the best avenue to advance reform. If we continue to find ways to “get the word out” to the public, such as through this website and others, and build a grassroots of activism to expose the fallacies and very harmful practices within conventional psychiatry, I believe it could build a groundswell of calls for reform. At least that’s what I’m hoping for.
Report comment
I know that I weep when I see parents whose children have died, attempting to get some redress via the court system.
I fear that they are simply not aware of what the State means by “edited” documentation.
So for example, as a means of meeting the Articles of the Convention against the use of torture, the Chief Psychiatrist has opened a path for legal representatives, on provision of a confidentiality agreement, to have access to unredacted documents (no hiding acts of torture that way). Problem being that the hospitals are then in a position where they don’t really want to hand over the documents showing acts of torture and arbitrary detentions, or any other criminality that their colleagues may have been involved in.
They are then in a position where they would need to request the lawyers to engage in a criminal conspiracy to pervert the course of justice (which they obviously wouldn’t want to do in writing, bad enough they are doing it on the telephone)
So, knowing that the parents or guardians wouldn’t know what the lawyers had been provided with, they “edit” the legal narrative.
In my instance that “editing” changed the facts that I had been ‘spiked’ with date rape drugs to them being my “Regular Medications” (fraudulent prescription), AND that I had been an “Outpatient” of the hospital concerned for more than ten years, rather than someone who was NOT a ‘patient’ of anyone (remove the documents showing no valid referral source for someone Police were told was an “Outpatient” with a knife, collapsed in his bed after being ‘spiked’ with date rape drugs, and insert other misleading documents creating the appearance of an “Outpatient”)
Any further complaining about the matter and the people complaining are now poisoning their character with the fraud prepared for precisely that purpose, to slander them, and have them do it t themselves. Those who know what the ‘coding’ of the documents means will no doubt assist in that slandering. In my instance complaining about being ‘spiked’ was my paranoid delusions and not a fact because they had retrieved the evidence……. well, so they thought. Did I mention he carries a knife? Or so police told me, …… well, they didn’t actually find it but it was planted for them to find…… as good as finding it right? So I am now ‘flagged’ with police as a mental patient who carries a weapon, not bad for someone starting with nothing but a phone call.
This sort of “editing” compounds the offending, and when you add to this the forging of a letter of response from the Chief Psychiatrists by the Law Centre to complete the cover up of such human rights abuses…… there could not possibly be a ‘fair’ outcome for anyone other than ‘mental health services’ who are quite adamant that they will “fucking destroy” you and your family should you decide to proceed where they know they have a need to conceal their abuses. And they have quite the support network in place to ensure their success, with police able to retrieve any offending evidence/proof of their misconduct, and threaten and intimidate anyone who was a witness to the violations.
So the laws appear to provide protections from such human rights abuses, but it is a literal death sentence to try and access those protections should there be a need to conceal their offending by compounding the offences.
Not a lot of options other than obstructing justice once there are a whole bunch of ‘eyes’ on the matter, and Police are wondering “who else has got the documents”. Okay, caught but there is nowhere for you to go with a complaint because the State doesn’t torture, they merely “edit” documents post hoc to forge the narrative they want to be true.
I’m sure there are many here who have personally witnessed, and in fact even participated in such “editing”. And ‘we’ understand your silence. Plenty of room at the Hotel California.
So I weep along with the doctors who have no choice in remaining silent over the death of a 7 year old girl, knowing that the legal narrative being presented to the Coroner is likely to have been “edited”.
Orwell wrote in 1984 that “If the Party could thrust its hand into the past and say of this or that event, it never happened—that, surely, was more terrifying than mere torture and death.”. And from personal experience, I know he was right.
I read an old comment I had made in 2018 this morning, someone wondering what I had done to deserve what had been done to me. Beyond the victim blaming, it’s an interesting question. My first mistake calling the use of electricity a “barbaric practice” to the wife of a shock Doc working in a private clinic as a psychologist, and who had knowledge of how to do ‘remotes’ and access the State sanctioned kidnapping and torture program. Though I’m sure that being an anti psychiatrist was NOT why they justified my ‘treatment’ (no political ‘outcomings’ and all that rubbish), and the fabricated lie about my wife saying I was an abuser? Interesting the uses that ‘mental health services’ can be put to in that regard. Though I think that the drugging of such abusers may actually increase the likelihood of intimate partner violence and homicide. See the guy who was also possibly ‘spiked’ and who then set his own children on fire …. legal narrative changed to “Regular Medications”?
A song for all those who are aware of what it is the State is doing to conceal their human rights abuses disguised as ‘medicine’.
https://www.youtube.com/watch?v=TqhOVY58zIo
Report comment
“If the Party could thrust its hand into the past and say of this or that event, it never happened—that, surely, was more terrifying than mere torture and death.”
I spoke to a psychologist (one with a PhD) for more than a year about what I had been through. he helped me a lot……. at first.
I managed to get back on my feet and went and spoke to a number of people regarding the “editing” of documents (one being a Member of Parliament who examined the two sets of documents in detail). But when I went to the Police and tried to make a complaint, they then rang mental health servies and asked that they come and pick me up because I was “hallucinating”.
(I have since come to realise that this is how police deal with unwanted complaints, arbitrarily detain and refer to mental health for a chemical kosh, rather than take a complaint. called ‘stitching’ where I live.)
So after police realised that the psychologist had seen the documents they thought had been retrieved to conceal the human rights abuses, they then had to take a different tack with me. Trying to arrest me for having my medical records (which I explained I had obtained via FOI). Sot hey had to get me out of the Police Station without taking the documented proof of the offenses…… so they pretended to copy them and sent me on my way with an Incident Report Number (came back “insufficient evidence” mainly due to their willful negligence).
So I go back to the psychologist and we have a laugh about the police calling him and trying to have me referred for “hallucinating”. The Social Worker who was with me at the Police Station confirmed in an email to us that I gave no such appearance.
As you would expect, they must have wondered about the ‘flag’ placed on me to not take the documents, and reported back to the source of that ‘flag’………..
So then I go back to the psychologist and as a result of my laptop being stolen and other ‘strange’ occurrences……and I make mention of the Police trying to refer me to him (I had also told him about the meeting with the Member of Parliament).
Without being able to look me in the eye, the psychologist tells me “it never happened” (reread that Orwell quote again). Something we both knew had happened, he was now denying to my face. This and his questioning of me with regards “who else has the documents?”
I explained that I had provided them to a large number of people, Members of Parliament, MH Commissioner, Corruption watchdog, …. a homeless guy at the traffic lights with a sign (“edited”) saying “need food for family”. At that point he sort of panicked, and said he was afraid for his family (and given what I had told him about what they had done to mine, I don’t really blame him)
But I had no idea Police were using psychologists at mental health as a means to access information they would otherwise not get access to. That is, who else had the documents showing their use of torture and kidnaping of me for a Community Nurse…. which was then “edited” for my legal representatives. That and the theft of my laptop because well….. I was chatting with you guys here and …….had spoken to some people who might have recognised a ‘pattern’. The bucket was leaking really badly, and police weren’t sure who knew, and who they could trust with their covering up. Honest, it was all Adolf’s idea.
Not that any help has been forthcoming, double down again and cover up the bad cover up of the cover up. I did try my Consulate but it seems that they too find looking the other way the best policy when it comes to these sorts of matters…. human rights abuses that is. they too have families.
I guess what I’m saying is that a lot of people talk tough. The ‘i’d have stood up for the Jews had I been there in Germany’. the fact is they will willingly throw you under the bus at the first sign of trouble. They are hypocrites, and will do exactly nothing to help anyone but themselves. I’m assuming that most of the survivors of the camps are fully aware of this, and it’s a horrible reality to find out that this is the government you offered your life to protect…… only to be knifed in the back with a fountain pen.
But I assume things are different in America, and that when people say “they wouldn’t do that” it is because there are people who will actually do something about such corruption and human rights abuses. See for example “Betraying the Badge” where Federal Officers ensure the integrity of the Police rather than actively corrupt it for gain.
So good luck with the lawsuit. But just keep in mind that there are people who will use their positions to “fucking destroy” you and your families, and they have the full support of the State in that regard. See, they have one advantage over you, you didn’t even know your an “Outpatient”…. but you will be with a little bit of “editing” post forced drugging and electricity for your ‘hallucinating’
Report comment
Russell, I agree with you! The legal system is part of the larger mainstream neoliberal system! The only way as I see it is to continue to grow Mad In America and other alternative communities.
Report comment
Psychiatry has more to do with the legal system than actual medicine. If a cancer patient suddenly decides that he or she does not want any more chemo and stops treatment that is allowable, but not so with patients labeled with MI. The “health expert” has a legal requirement and obligation to drag a MI person to a psychiatric ward and force treatment on the person if they are deemed a danger to themselves or unable to make decisions for themselves.
Report comment
I agree. It is all up to them according to their whim, according to their self-interest. I was abused as a child. My two older brothers both had psychotic breaks before they turned 20. They got hospitalized. My parents actually spent a fortune, but of course it did no good because they were just labeled and drugged. By the time I reach my teens, I was a suicidal mess, but my parents decided that it would be too risky for them to have another mentally ill child, as the doctors had already questioned whether there was abuse happening in the home. So they denied it. They just said I was a spoiled brat looking for attention, that I was inherently bad. The high school guidance counselor saw there was something wrong with me and made several calls to my parents over a period of months telling them that I needed treatment. They ignored the phone calls. I dropped out of high school in junior year. At that point, the board of Ed started paying for me to see a psychiatrist once a week. She immediately put me on Elavil. I saw her for a year, once a week, took the Elavil as prescribed, graduated on time and then immediately found out that she was ending treatment since the money train was stopping. The board of Ed stopped paying and she knew that my parents wouldn’t, so she just dropped me, goodbye good luck, no word on what to do if I needed help even though I was still living in an abusive environment, no word as to what to do about the elavil. That fall I called her from my dorm room at college and told her I was suicidal. It was the first time I’d spoken to her since she dumped me. Next thing I knew there were cops at my door and they took me away to a locked psych ward and Providence Rhode island. I was kept there overnight, didn’t see a doctor, and out on the street the next day. I finished out the terrible year at school and then spent the summer in hell in my parents home. I can’t remember what went on that summer but knowing my mother she was probably telling me to kill myself like all the time. She’s evil. That August I took the entire bottle of Elavil that had been lying around for a year and a half. My parents couldn’t call an ambulance because there had already been too many ambulances in police at our house because of situations with my brothers. So they carried me into my father’s car and drove me to this s*** hospital that didn’t have records on our family already. My mother insisted to the ER doctors that I was not depressed and there were no problems in the family. They pumped my stomach, put charcoal down my throat, I had tubes in my nose, I couldn’t speak and there was my mother telling the doctors what a complete spoiled brat I was. Well apparently the doctor believed her because he didn’t even question why I had a prescription for Elavil. He had a demonic look on his face as he ripped the tubes out of my nose.
They force help on people when they don’t need it, they deny people help who are begging for it. They are the most selfish self-interested evil and titled money grubbing horrible people I’ve ever met in my life. The only reason I hope that there is any kind of an afterlife is the glimmer of hope I feel about them being punished for how they treated me. They sentenced me to a lifetime of hell.
Report comment
“If a cancer patient suddenly decides that he or she does not want any more chemo and stops treatment that is allowable, but not so with patients labeled with MI. The “health expert” has a legal requirement and obligation to drag a MI person to a psychiatric ward and force treatment on the person if they are deemed a danger to themselves or unable to make decisions for themselves.”
In fact Gilbert, certainly in my State, it is as simple as a Nurse making the ‘cancer patient’, or anyone for that matter, into an “Outpatient” and police can be dispatched to go pick them up.
https://www.youtube.com/watch?v=oZ9UQKBUrsg
The Chief Psychiatrist writing that should any citizen have a ‘reaction’ to this type of treatment, then the “observable behaviours” are what matters and NOT the cause. He is also in support of the “editing” of documents to remove such “concerning aspects” from the legal narrative, and running with the fraud in the legal system.
So the idea that ‘cancer patients’ or anyone else has some sort of ‘protections’ that those labelled Mentally Ill is simply wrong. You can pay $200 to a psychologist (with a Masters degree) to have them provide access to the ‘system’ and arrange to have anyone you like “fucking destroyed”. Simply have a Community Nurse tell Police that the person is an “Outpatient” and the wheels start a rollin…..,
And the ‘authorities’ will ensure that absolutely nothing is done about the breaches of the law and human rights because they find it quite easy to “edit” documents post hoc, threaten families and witnesses, and arrange a little ‘accident’ for the person who had the audacity to complain.
They have tried other ‘methods’ but it’s just so much cheaper for the State to dispose of them in this manner. Human life of little value once you become desensitized to the processing of ‘units’ in such ‘facilities’.
And the community would only be concerned if it were they who were being subjected to such ‘treatments’, totally unaware that their human and civil rights have been removed without their knowledge. The Chief Psychiatrist and lawyers simply ignoring the facts or truth in favor of a fantasy fabricated by those “editors” of documents at the ‘hospitals’ concerned.
I went from being a citizen who had been ‘spiked’ with date rape drugs, and then snatched by Police who thought I was an “Outpatient” with a knife (planted when I collapsed) to an10 year “outpatient” of the hospital. I was a violent psychotic drug abusing wife beater (instead of the victim of some serious criminal conduct by the Community Nurse) with the “editing” of the documents for my legal representatives.
I believe that they had a need to “fuking destroy” my family because if we ever got together and spoke about these matters it would become obvious that not only was I defrauded, but they too had words put into their mouths for the concealment of the offending. y wife telling me she had said no such thing regarding me beating her (consistent with the truth, though I was certainly shocked to see they had quoted her on that ‘fact’ in a statutory declaration. Putting words into her mouth as well as mine to forge the risk required by the Act)
I note the way the ‘honoring’ (by politicians) of our soldiers who died for these protections from oppression, is these days used to do ‘deals’ over weapons of mass destruction, for the benefit of large weapons manufacturers. Turn in their graves? They’re being bulldozed out of them, at the very monuments dedicated to their bravery. It seems these soldiers died for the right of our politicians, to remove ‘our’ rights, no questions asked (by a lame propaganda machine called ‘the press’).
The Dogs of War. (Dealing in death is the nature of the Beast)
Imagine what can be achieved with Euthanasia Laws and the ability to “edit” legal narrative in secret before anyone has the right to examine documents related to the ‘treatment’? It was what the public wanted our politicians who didn’t even raise the issue before the election tell us. Or perhaps it was more a case of it was what THEY wanted?
Report comment
Sorry to hear about your daughter, Russell. While lawsuits and pubic awareness are understandable ways to fight back against psychiatry and if we had a movement to help bring it down, what do we have to replace it that will not have the same fate as psychiatry? I looks like psychiatrists who refuse to question their own profession could use some therapy themselves. Apparently, they see this as an existential threat.
This reminds me of Daniel Dennett’s The Clergy Project, https://clergyproject.org/stories/ a “nonprofit organization that provides peer support to current and former religious leaders who no longer have faith. The group’s focus is to provide private online forums for its participants and assistance through career transition grants, and subsidized psychotherapy sessions”(Wikipedia)
So it’s not just psychiatry that is failing us, it’s religion too. It seems we are in the midst of a crisis even though we don’t feel it as such. While calling out these archaic institutions is quite in order, replacing them will be a huge challenge. MIA is excellent in diagnosing the fallacies within psychiatry but where are the proven transformative psychotherapies/treatments that can finally send mainstream psychiatry to the dustbin of history? If this became a reality, we would have no need for lawsuits.
Report comment
May this be the tipping point!
love it or hate the social media but one area that I think it will show its most impact is how do we move forward of psychiatry and its secrecy. Next, people need to record doctors talking and publish!
Report comment
I think the pandemic itself will be a tipping point for mental health. All the people who sought mental health treatment for the first time have now been on the meds long enough realize they don’t work and possibly make things worse. We can see this in the way the general public reacted when given access the facts on the drugs. The mRNA vaccines are setting a new standard for what the public expects in openness in research. Now they want that openness on psych drugs and they are realizing the benefits are not enough to justify the potential harm.
Report comment
Putting the cart before the horse is standard practice for Psychiatry (and Psychology). This is an industry of 60 billion dollars are at stake in the USAW why is anyone surprised by the reaction?
Psychiatry (and to a lesser extent it enablers like psychologists and social workers) are con artists running a LONG CON.
Report comment