

Twelve years ago, Ronald Kavanagh—who at that time was a reviewer of psychiatric drugs for the FDA—turned into a whistleblower, telling the Office of the Inspector General that his superiors at the FDA were turning a blind eye to the risks of a new atypical antipsychotic, asenapine, and doing so in collusion with Schering-Plough, the company that was seeking to market the drug. Asenapine, he argued, was ineffective as a treatment for schizophrenia and for bipolar I patients with mild to moderate symptoms, and yet approval would expose those two groups of patients to its hazards, which included a heightened risk of death.
Kavanagh was soon fired for his efforts, and asenapine was approved as a treatment for both schizophrenia and bipolar I. Schering-Plough’s CEO, Fred Hassan, used the impending approval of the drug to negotiate a merger with Merck, a deal that brought him and other Schering-Plough executives more than $100 million.
Kavanagh has never given up on that whistleblower complaint. He filed a qui tam lawsuit in 2012, and in the years that followed, wrote letters to President Obama, President Trump and Senator Charles Grassley, none of which provided him with any relief. In May of this year, he renewed his complaint once more, writing members of Congress and the Office of the Inspector General.
It might seem that there is little reason to revisit his complaint, given that it has never gained any traction in Congress, the OIG’s office, or the courts. It is unlikely that it will fare any better this time around. However, a review of documents in this case, including the FDA’s reviews of the New Drug Application (NDA) for asenapine, reveals much about the mindset of the FDA at the time and the standards it applied for approving a psychiatric drug. The documents support Kavanagh’s complaints, including evidence that the FDA downplayed—or even obscured—risks with the drug.
Kavanagh’s complaint also alleged that asenapine’s potentially lethal side effects were common to other atypical antipsychotics that, like asenapine, had proven to be ineffective for bipolar patients with mild to moderate symptoms. He warned that the use of atypicals would lead to 5,000 or more deaths each year in such patients, and there is evidence that this concern has proven true. He also warned that asenapine and other atypicals could cause deaths in newborns whose mothers were exposed to these drugs during pregnancy, and FDA Medwatch records reveal that there have been a number of infants under two years old who died due to exposure to an atypical antipsychotic.
Asenapine
Asenapine was synthesized by the pharmaceutical company Organon in the 1980s. After Organon conducted early-phase testing of the drug, in 2003 it entered into a co-marketing agreement with Pfizer, which then took the lead in conducting phase III trials of asenapine as a treatment for both schizophrenia and bipolar I disorder. Pfizer had paid Organon $100 million when it negotiated the agreement, but after analyzing the phase III results, which didn’t provide “conclusive” evidence of efficacy, it pulled out of the deal in November 2006.
However, Organon continued to develop the drug, and in the spring of 2007, Schering-Plough’s CEO, Fred Hassan, negotiated a deal to buy Organon from its parent company, AkzoNobel, for $14.4 billion. Organon had several compounds in late-stage development, and Hassan perceived asenapine as of particular value since Organon was preparing to file a New Drug Application for it. Organon filed its NDA on August 31, 2007, and in November, Schering-Plough completed the deal.
At that point, Hassan needed the FDA to approve asenapine, and even as he was closing the Organon purchase, he began poking the FDA to do just that, telling Fortune magazine that “when bureaucrats come under pressure, they tend to choose the path of asking for more data, as opposed to approving the drug.” His political message was clear: An FDA that didn’t quickly approve new drug applications was throwing impediments in the way of American business.
Hassan’s Record as a CEO
Prior to his acquisition of Organon, Fred Hassan had been feted for turning around the fortunes of two pharmaceutical companies he’d led: Pharmacia and Schering-Plough. In both instances, he and his companies did so by hiding adverse effects of their best-selling drugs, which subsequently led to a Congressional investigation, lawsuits, and multimillion-dollar settlements and fines.

Hassan was hired as CEO of Pharmacia and Upjohn in 1997. Two years later, he negotiated a merger with Monsanto, which had a hot new drug that had just come to market, Celebrex. This was the drug that could remake Pharmacia.
Monsanto had been co-marketing Celebrex with Pfizer, and now Pharmacia, together with Pfizer, told the public that this Cox-2 inhibitor, an NSAID for treating pain, didn’t cause an increased risk of cardiovascular events, including heart attacks and strokes. The two companies made this claim even though results from a clinical trial, which they had known about since 1999, had shown otherwise. The hiding of this potentially deadly risk proved profitable for both, with Celebrex sales totaling $10.2 billion from 1999-2003.
The two companies brought a second Cox-2 inhibitor (Bextra) to market in 2002, and once again they told the public of a drug that didn’t elevate the risk of cardiovascular events. Hassan successfully sold Pharmacia to Pfizer for $62 billion at the end of 2002.
A little more than a year later, it became known that the two companies had hidden the cardiovascular risks from the public. Bextra was pulled from the market, and the FDA, in 2005, put a black-box warning on Celebrex. Pfizer then spent years fighting lawsuits, eventually paying $894 million to patients harmed by the two drugs; another $486 million to investors who bought Pharmacia and Pfizer stock from 2000 to 2003; and a $2.3 billion fine to the federal government to settle criminal charges for its fraudulent marketing of Bextra and other drugs.
After negotiating the sale of Pharmacia, Hassan—hailed by Financial Times as CEO of the Year in 1999 for his success at that company—was hired by Schering-Plough in April of 2003 to be its CEO. This was seen as a difficult period for Schering-Plough, as the patent on its best-selling drug, Claritin, had run out in December of 2002. The company’s future was now seen as tied to Zetia (ezetimibe), a cholesterol-lowering drug that had been approved recently by the FDA. “Mr. Hassan’s success may depend on his ability to hawk Zetia,” the Wall Street Journal reported.
Statins like Lipitor and Crestor, which were billion-dollar drugs, inhibited the body’s production of LDL cholesterol, which in turn had been shown to slow atherosclerosis, the buildup of plaque on arterial walls that leads to heart attacks and strokes. Ezetime worked in a slightly different manner. It inhibited the absorption of intestinal cholesterol. While this lowered LDL cholesterol levels, it wasn’t as effective as statins in this regard, and it also hadn’t been demonstrated that this method of lowering LDL cholesterol slowed atherosclerosis.
Shortly before Hassan’s arrival, Schering-Plough had joined with Merck to launch a clinical trial called ENHANCE, which was designed to test whether a drug that combined Zetia with Merck’s Zocor (simvastin) would prove to be more effective than a statin alone in reducing the buildup of plaque. Simvastin was a statin that had gone off-patent, and their hope was that the trial would help make their combination drug, Vytorin, the No. 1 cholesterol-lowing medication. In 2004, before the ENHANCE trial had concluded, the companies obtained FDA approval to market Vytorin based on its cholesterol-lowering effects.
In late 2005, the two companies analyzed results from early enrollees in their trial, and found that there was no difference between the two arms of the study. The blind had not been lifted, but with this result it didn’t matter which arm was the combination drug and which was the statin alone—the fact that there was no difference between the two arms meant that the addition of ezetibime to simvastin had provided no benefit. The trial was completed in April of 2006, and not long after that, Schering-Plough and Merck definitively knew that Vytorin had failed the test.
ENHANCE was a high-profile study, and the cardiology community, as well as the investment community, expected that results would be announced at the fall 2006 meeting of the American Heart Association. That meeting passed without an announcement, and so too the association’s spring and fall meetings in 2007. During those 18 months, Hassan and Schering-Plough, along with Merck, busily promoted Vytorin’s effectiveness.
“The lower (cholesterol) is better story continues,” Hassan told investors in the fall of 2007. “Evolving medical science continues to find that reaching lower and lower goals for LDL is better for patients and Vytorin and Zetia provide very good options.”
The two companies filled the airways with ads in 2006 and 2007 that told of how Vytorin had been proven in clinical studies to lower cholesterol more than Pfizer’s Lipitor and AstraZeneca’s Crestor. The public pronouncements worked: Vytorin and Zetia generated $3.87 billion in global sales in 2006 and $5.2 billion in 2007, which produced nearly 70% of Schering-Plough’s profits that year.
Hassan was richly rewarded for this commercial success. In addition to his regular salary, his CEO contract provided for various cash and stock awards based on the company’s financial performance in 2007. Law firms that subsequently sued Schering-Plough and Merck for fraud calculated that Hassan received performance bonuses in 2007 worth $38.9 million. Other executives also received million-dollar bonuses, with one executive selling $28 million of Schering-Plough stock while its price was flying high.
However, Hassan and the other executives at Schering-Plough and Merck couldn’t keep this fraudulent story aloft forever. When the two companies didn’t announce results of the ENHANCE trial at the fall 2007 meeting of the American Heart Association, Congress initiated an investigation, asking for them to produce records by December. As a first response, the two companies—as the Wall Street Journal later reported—”created minutes of a crucial meeting about a major study on their cholesterol drug” to cover their tracks. Finally, on January 14, 2008, the company announced “preliminary results” from the ENHANCE trial, acknowledging that Vytorin had not shown any “statistically significant benefit” over placebo.
The attorneys general for New York and Connecticut announced they were launching an investigation, and then, on March 31, 2008, the two companies presented the results at a conference of the American College of Cardiology, with the New England Journal of Medicine publishing them the same day. Vytorin had produced “no result—zilch,” said principal investigator John Kastelein. “In no subgroup, in no segment, was there any added benefit.”
Five years later, Merck paid $688 million to settle lawsuits from investors who bought stock in one of the two companies while they hid the results from the ENHANCE study. But by that time, Hassan—with the many millions in his pocket from his performance awards—had moved on, his sights now set on getting asenapine approved. This drug, he told investors, was going to be a “blockbuster.”
Raising Red Flags at the FDA
Ron Kavanagh, who had come to work at the FDA in 1998, was an expert in clinical pharmacology, the study of how chemical agents are absorbed and metabolized, and their possible toxicities. He had earned his PharmD at the University of Texas and a PhD at the University of Washington, studying drug kinetics and pharmacodynamics. After finishing that training, he went to work for Merck in its division of internal regulatory affairs. “My job was to get drugs approved, and approved with regulatory agencies all over the world,” he said.

After he joined the FDA, he often gave talks and presentations to FDA reviewers and medical staff on how pharmaceutical companies developed drugs and the pharmacology tests a company needed to perform.
His first years at the FDA taught him to be wary of investigational new drugs. He started off in the agency’s endocrine division, where he worked with a colleague who had picked up on toxicities caused by a duo of obesity drugs, fenfluramine and dexfenfluramine, which led to their being banned in 1997.
Next he moved into the gastrointestinal division, where he reviewed Lotronex (alosetron hydrochloride), which was to be marketed for irritable bowel syndrome in females. Kavanagh thought there was evidence that the drug could cause ischemic colitis, a potentially fatal side effect. Although the drug was approved in 2000, it was recalled from the market a year later after its use led to five deaths.
The FDA’s recall of the drug, wrote Lancet editor Richard Horton, “reveals not only dangerous failings in a single drug’s approval and review process but also the extent to which the FDA—its Center for Drug Evaluation and Research in particular—has become a servant of the industry.”
Kavanagh then transferred into the division of neuro and psychiatric drugs, where he reviewed Eli Lilly’s NDA for Cymbalta (duloxetine). He warned of possible liver issues that could be expected with this drug, a concern that Eli Lilly “didn’t appreciate,” he said.
Next, he reviewed bifeprunox, an atypical antipsychotic that was similar to aripiprazole in its mechanism of action, as it had a mixed agonist/antagonist effect on both dopamine receptors and serotonergic receptors. However, bifeprunox caused a brain swelling and other toxicities that led to deaths in the clinical trials, and in 2007, thanks in part to Kavanagh’s review, the drug was not approved.
Even so, by that time, Kavanagh was becoming persona non grata at the FDA. Major companies had often complained about his critical review of their drugs, and he had also grown increasingly critical of the FDA. In 2005, he started taking his allegations to Congress, speaking to the Senate Finance Committee about “corruption in the psychiatry division and in the Office of Clinical Pharmacology and other FDA offices.” He also was upset with the off-label marketing of psychiatric drugs, particularly for their use in children, and in 2007, he was briefly suspended and told to stop his whistleblower efforts if he wanted to keep working there.
After Organon filed its NDA in August 2007 (Schering-Plough had not yet closed on its acquisition of the company), the FDA was required to assess whether the company had conducted the necessary pharmacological studies—a drug’s bioavailability, how it was metabolized, the possible toxicities of the metabolites and so forth—that would allow for a substantive review. In October, Kavanagh recommended that because of a “lack of validation of assays in pharmacokinetic studies,” the NDA was non-reviewable.
This turned out to be the first shot in what would become a war with his superiors at the FDA over asenapine. The director of the psychiatry division at the FDA’s Center for Drug Evaluation and Research, Thomas Laughren, overruled him, which meant that the review process—evaluating the efficacy and safety results from the trials—would now begin.
The Efficacy Data
Schizophrenia
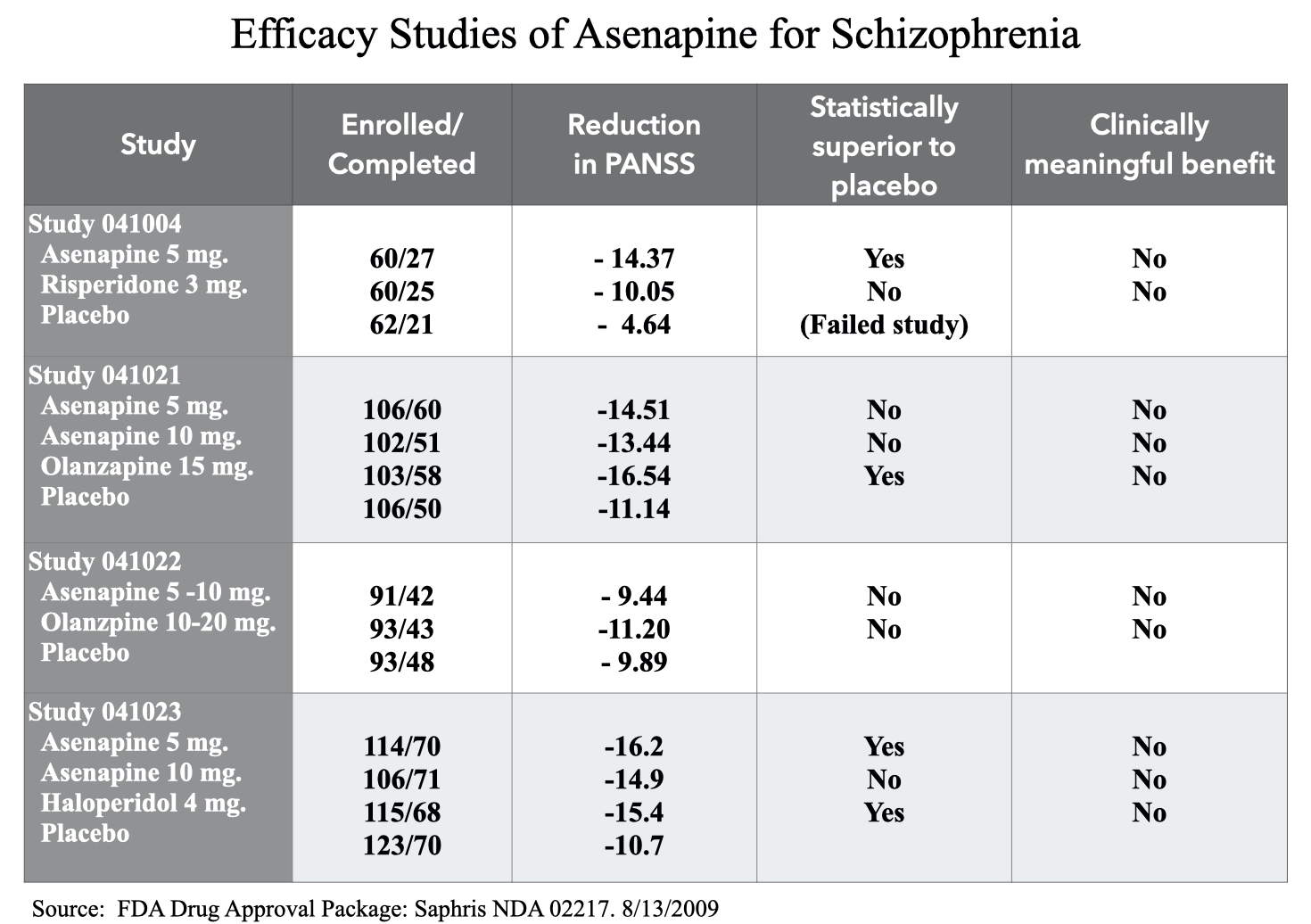
Organon conducted four six-week trials of asenapine as a treatment for schizophrenia. The patients recruited into the trials were withdrawn from whatever antipsychotics they had been taking and randomized either to asenapine, placebo, or a comparator drug. The primary endpoint was reduction in symptoms as measured by the Positive and Negative Syndrome Scale. PANSS assesses 30 symptoms on a scale of 1 to 7, which means that total scores can range from 30 to 210. The patients could also be given concomitant medications during the study: zolpidem, zalepam, chloral hydrate, a benzodiazepine, and anticholinergic medications to treat extrapyramidal side effects.
In the four trials, there were a total of six tests of asenapine versus placebo: three tests of a 5 mg dose (administered sublingually twice a day); two tests of a twice-daily 10 mg dose, and one test of a flexible dosing schedule (from 5 mg to 10 mg). In four of the six tests, asenapine failed to beat placebo. In the fifth, a 5 mg dose did provide “statistically significant” superiority over placebo, but the comparator drug—risperidone—did not, and when the comparator drug in a trial fails to best placebo, the study is deemed to have failed. As a 2008 paper published in the journal Psychiatry explained, “No conclusion can be drawn about the investigational drug in a failed study.”
Thus, there was only one instance—out of six tries—where there was a “meaningful” positive finding for asenapine. And in that instance, the decrease in PANSS was 16.2 points for the 5 mg dose, 14.9 for the 10 mg dose, 15.4 for haloperidol, and 10.7 for placebo. Although there was virtually no difference in symptom reduction between the 5 mg and 10 mg doses of asenapine (1.3 points on a 210-point scale), the 5 mg dose just made it over the line for “statistical significance” over placebo, whereas the 10 mg dose did not. A total of 70 patients in the group of 114 randomized to the 5 mg dose completed the six-week trial.
Such was the efficacy data. The fact that concomitant medications were allowed—three different sedatives, an antianxiety medication, and a treatment for Parkinsonian symptoms—also meant that there had been no testing of asenapine as a monotherapy for psychotic symptoms.
Finally, researchers have determined that there needs to be at least a 15-point difference on the PANSS scale between the drug and placebo at the end of the trial for a drug to provide a “clinically meaningful” benefit. Yet, in the four clinical trials, there was not a single instance where any dose of asenapine came close to this standard.
Bipolar I
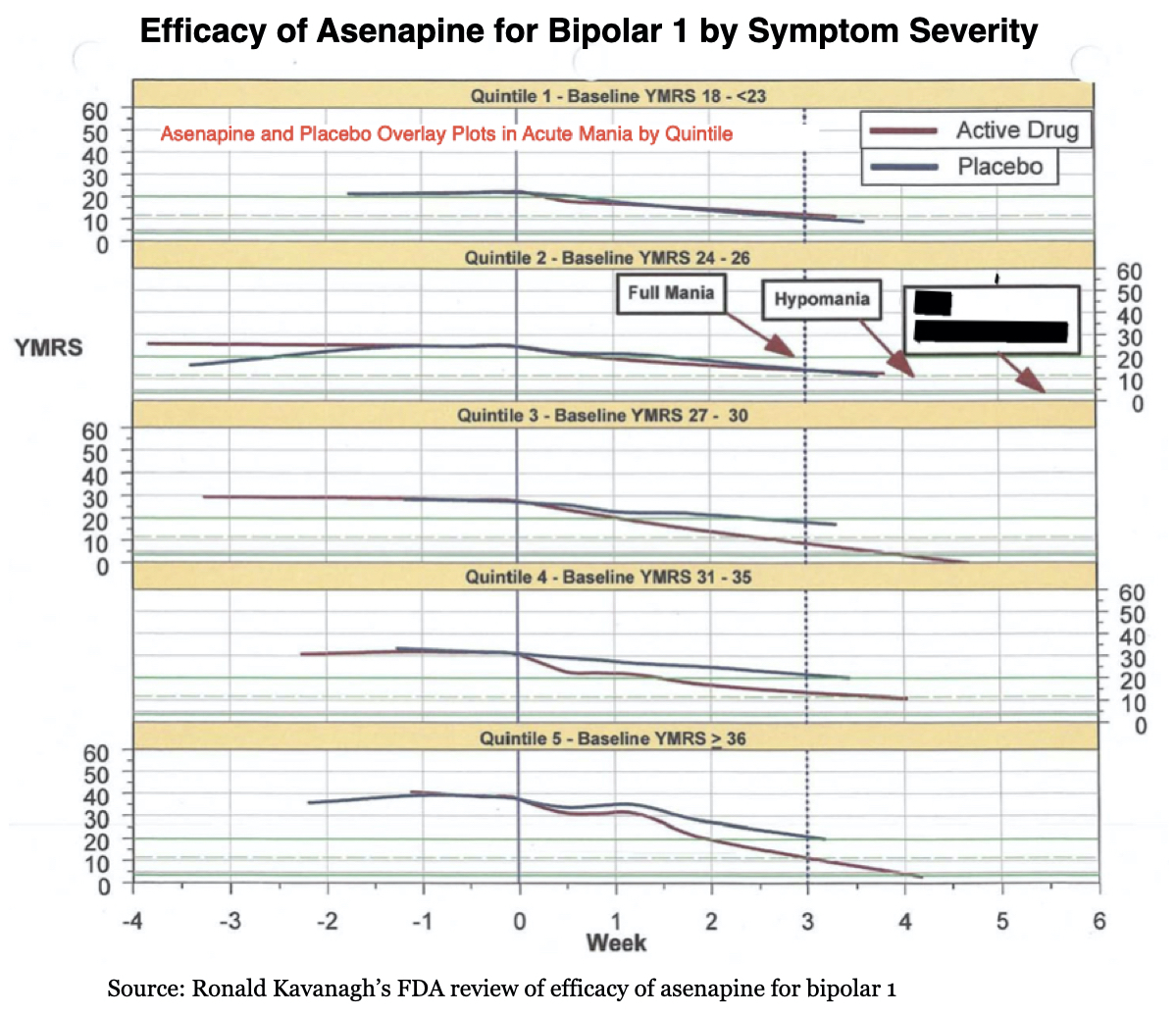
Organon conducted two three-week studies of asenapine, both at a flexible dose from 5 mg to 10 mg (twice daily), as a treatment for manic and mixed episodes in bipolar 1 patients. The primary endpoint was reduction in symptoms on the Young Mania Rating Scale (YMRS). This is a 60-point scale, and in this study, those enrolled had to have baseline scores of greater than or equal to 20.
In both studies, asenapine was seen as providing a statistically significant benefit over placebo. The difference between the two groups in one study was 3.7 points on the YMRS scale and, in the other, 5.3 points. However, in both studies, the comparator drug, olanzapine, provided a greater reduction of symptoms than asenapine.
As for the real-world benefit of this drug for bipolar, researchers have concluded that a 6.6-point difference on the YMRS scale is needed for a drug to provide a “clinically meaningful” benefit over placebo. Asenapine did not reach this standard in either trial.
Summary Safety Data
In the six placebo-controlled studies (four for schizophrenia and two for bipolar), there were 2,251 patients who had been exposed to asenapine. Eleven died, and 14% suffered a serious adverse event (life-threatening or requiring hospitalization). Seventy-eight percent experienced an adverse event of some type; the most common side effects were sedation, dizziness, weight gain, extrapyramidal symptoms, and oral numbness.
Organon had also conducted a number of non-controlled studies, and thus the complete safety database consisted of 3,457 patients exposed to asenapine. Twenty-two had died, including eight by suicide. There were eight who died from cardiac and respiratory events, and one neonatal death. The baby died hours after being born prematurely at 32 weeks to a woman in the trial who had been treated with asenapine.
Kavanagh’s Review
Although Kavanagh had earlier declared that Schering-Plough had not provided sufficient information to conduct an adequate pharmacology review, in the spring of 2008 he was assigned the responsibility for doing just that as part of the FDA’s overall assessment of asenapine’s efficacy and safety.
Early on, Kavanagh noted that the efficacy data for schizophrenia was unconvincing, particularly when the four studies—and six tests of asenapine—were viewed as a collective body of evidence.
At first glance, it did seem that the results from the bipolar studies were convincing, and easily passed the “two positive tests” standard for approval at the FDA. However, Kanavagh further analyzed the two bipolar studies, dividing the patients into “quintiles” based on the severity of their symptoms at baseline, and he found that in patients with mild to moderate bipolar symptoms (YMRS score less than 27), the drug had not provided any benefit. The rate of improvement in the placebo group and this subgroup of bipolar patients was virtually identical during the three weeks.
As such, the risk-benefit equation for schizophrenia patients and for around 50% of all bipolar I patients was evident. They would be exposed to the hazards of this drug without any benefit, and thus the treatment was certain to do more harm than good.
There were many evident worries in the safety database: cardiac risks, liver toxicity, kidney impairments, and so forth. And there was one other concern new to Kavanagh. He had been talking to a former FDA reviewer who had gone to work for industry and had experience with asenapine, and this “informant” had warned him that it was problematic because it acted as an “inverse agonist” of the 5HT2B receptor (a receptor for serotonin). Stimulation of this receptor by fen-phen had been identified as a possible cause of pulmonary arterial hypertension (PAH) and cardiac-valve stenosis. This led Kavanagh to worry that PAH could lead to miscarriages and an increase in neonatal deaths for babies that breast fed.
Kavanagh then focused his attention on the death records from the asenapine studies, reviewing the case report form for each one. These are the forms that the investigators at each site fill out for every patient, which are then summarized by the pharmaceutical company into a safety summary in its NDA. Kavanagh also revisited the animal studies and healthy volunteer studies that are expected to identify possible drug toxicities.
This investigation led him to identify a number of safety concerns. He also discovered specific instances where it appeared that Schering-Plough had obscured the possible risks with asenapine, or covered them up.
Neonatal Deaths
Although the case of neonatal death appeared in the safety summary, it hadn’t been flagged in the FDA’s preliminary medical reviews as a cause for real concern. The mother was said to have had previous miscarriages, and the thought was that this explained the infant’s death, even though the investigator who’d treated the woman had stated that the baby’s death was “possibly related” to asenapine.
The animal studies provided reason to think that might be the case. In both rats and rabbits, exposure to asenapine during pregnancy had led to an increase “in post-implantation loss at all doses,” meaning that there was an increase in deaths of the fetal pups prior to birth. In the rat studies, there was also a marked increase in “early pup deaths” through “day 21 postpartum.”
In addition, the animal studies warned of other congenital risks—abnormalities in bone formation and connective tissues, and—in one pup—a heart defect.
These findings had not been mentioned in the safety reviews Kavanagh had read up to that point. This was, Kavanagh thought, an instance where a possible toxic risk had been deliberately obscured when Schering-Plough filed its NDA.
Cardiac Deaths
There were eight patients exposed to asenapine who had died from cardiac and respiratory events. Although the FDA, in its preliminary reviews, didn’t identify these deaths as possibly related to asenapine, the drug had been found to cause QT prolongation in some patients, which meant that their hearts were taking longer than normal to recharge between beats. This was a warning signal of possible cardiac harm.
As Kavanagh dug through the healthy volunteer studies, he found that in one instance a 27-year-old man, described as fit and a non-smoker, went into cardiac arrest after being given asenapine. “There is no doubt that he became asystolic and as you pointed out you had to perform cardiac massage to sustain an output,” wrote the company’s cardiologist, Graham Jackson, in a December 1991 report. “This almost certainly has to be classified as a drug-induced effect with a serious adverse effect on the conducting system of the heart.”
Yet, Schering-Plough had described that incident differently in its summary of the healthy volunteer tests. The description there told of a 27-year-old man who had suffered an episode of “neurally mediated reflex bradycardia,” which, one FDA reviewer wrote, “is a benign, self-limiting event, and the most common cause of vasovagal syncope.”
These descriptions told of two very different events. Asystole is described in medical dictionaries as a “cardiac arrest rhythm with no discernible electrical activity on the EKG monitor. The heart is not functioning. It is a life-threatening condition that requires immediate action.” Vasovagal syncope is described in medical dictionaries as what “occurs when you faint because your body overreacts to certain triggers, such as the sight of blood or extreme emotional distress.”
To Kavanagh, this was a second instance of corruption: a cardiac arrest in a healthy volunteer had morphed into a fainting episode in the NDA.
Anaphylaxis
As Kavanagh went through the case report forms for the 22 deaths, he found one that told of a 57-year-old woman with schizophrenia who, after being treated with asenapine for 470 days, suffered a bout of “Quincke’s edema.” This is an allergic reaction that causes a swelling in the back of the throat or uvula which can close the upper airway, and the case report told of the woman having been on a ventilator for four days after she suffered this “respiratory failure.”
However, the safety summary for this woman didn’t tell of a possible allergic reaction. It simply stated that she developed “sudden respiratory failure . . . the cause of death was pulmonary embolism.”
Suicides
There were eight suicides in the 3,451 patients who were exposed to asenapine in the short-term and long-term studies of the drug (compared with no suicides in the 706 placebo patients in the short-term trials.) Five of the eight had occurred within 33 days of initial exposure to the drug: two by hanging, two jumped to their deaths, and the fifth by an unknown method.
This rash of suicides within a month of exposure to asenapine could be seen as a signal of suicide due to drug-induced akathisia. Akathisia is a known risk factor for suicide, and the safety summary in fact stated that 1 in 16 patients exposed to asenapine had experienced this adverse effect.
Moreover, Kavanagh reasoned, this drug acted on the serotonergic system, as did the SSRI antidepressants that had been found by the FDA to increase the risk of suicidal behavior in children and adolescents. This was another concern to be flagged and further investigated.
However, FDA reviewers, following the lead of Schering-Plough’s safety summary, were treating these suicides as a risk inherent with the “disease” (schizophrenia and bipolar). There had been four suicides in those treated with olanzapine, and once the suicide rate was calculated according to “patient-years” on each drug, it was the same for both: 1.3 suicides per 100 patient-years. Olanzapine had been on the market for more than a decade, and thus suicide didn’t appear to be a worry particular to this drug.
Is This a Class Effect?
After Kavanagh assessed the efficacy of asenapine for bipolar, finding that it provided no benefit for curbing mania in bipolar I patients with mild to moderate symptoms, he looked at the efficacy data for several other atypicals that had been tested for bipolar I: Zyprexa, Risperdal, Geodon, and Invega. He found that the pattern held true for those drugs as well: They were ineffective for those with mild to moderate symptoms.
As such, Kavanagh now saw a review process that had led to several atypicals being approved for a diagnosis even though 50% of bipolar I patients would receive no benefit and be exposed to the many hazards of these drugs. These drugs had a black-box warning that they increased the risk of dying in the elderly, and it was also well known that atypicals could induce metabolic dysfunction that increased the risk for early death. At the very least, Kavanagh reasoned, the FDA should put this information—that asenapine was ineffective for those with mild to moderate bipolar I symptoms—on the label, and add it to the labels for the other atypicals as well.
Kavanagh Blows the Whistle
Kavanagh’s clinical pharmacology review of asenapine was due on May 15, 2008, and at least a week before that he had sounded an alarm, stating in a large office meeting that he thought this drug was dangerous and largely ineffective, and that Schering-Plough had sought to hide the risks. While his 520-page report was filled with technical details regarding the drug’s bioavailability, how it was metabolized, and so forth, Kavanagh did have a personal history that was helping to fuel his opposition to this drug.
By his own admission, he suffered from “mental illness.” He had suffered more than a dozen episodes of depression, including one hospitalization, and he hadn’t found antidepressants to be particularly helpful. When he was about 40 years old, he told a psychiatrist of a time in his life when he had fallen in love, describing it as a period of great happiness. The psychiatrist viewed this as evidence of mania and newly diagnosed Kavanagh as bipolar. While Kavanagh didn’t agree with the diagnosis and didn’t take any bipolar medication, he spoke about this personal vulnerability when he raised his complaints about asenapine at the FDA.
As he later wrote: “I also said that the drug, as well as others, could be used not only for what it was currently under development for, but in the future could also be approved for illnesses that I or my child suffered from, or that I had been misdiagnosed with (which is common for people with psychiatric illnesses), or that it could be promoted for use or used off-label for our illnesses and so we were personally affected by this.”
On May 16, he wrote his superiors at the FDA that he was changing his recommendation to “non-approval.” He was worried about the deaths in the trials, and stated that he believed that this toxicity was “mediated by agonism of the 5HT2B receptor.” Moreover, he wrote, there was evidence that the “sponsor knew of this toxicity and specifically tried to prevent our detecting it.” And finally, there was the harm that would come from off-label uses of asenapine.
“I simply do not believe that there is anything that we can do that will adequately educate physicians and patients to the risks and that with off-label use we will be looking at an epidemic of potentially lethal cardiac and pulmonary toxicities in children several years from now,” he wrote.
A week later, with his emotions ramping up into higher gear, he emailed Janet Woodcock, the director of the Center for Drug Evaluation and Research, to inform her of an “imminent public health concern” related to asenapine and the prescribing of already approved atypicals to bipolar patients with milder symptoms.
He warned her that he was ready to go outside the agency with his complaints. “I have notified the clinical division of apparent criminal activity by the sponsor (i.e. not reporting Serious Adverse Events and deaths as required), and have requested a criminal investigation,” he told Woodcock. “Yet the clinical division has apparently tried to cover this up.”
That last sentence was sure to land him in hot water with his colleagues, and on May 30, Kavanagh wrote Woodcock that his superiors were “bullying him” and that he no longer trusted the agency’s internal “process” for responding to his complaints. From this point forward, he told her, “I prefer to deal with Congress.”
The agency, he told her, was failing to do its job.
“I don’t like what has happened over the past few years. Based on my experience I believe the review process has gone (at least at the reviewer level) from collegial, collaborative, efficient and trying to make to balanced decisions to being bogged down in bureaucracy, reviewers just cutting and pasting what the sponsors say without critical evaluation, being grossly inefficient, cutting corners just to make deadlines and to avoid being retaliated against, and everyone being defensive.”
Kavanagh contacted the Office of the Inspector General and Iowa Senator Charles Grassley. In June, he filed two amendments to his May 15 review, further detailing and documenting his concerns. His colleagues at the FDA, he wrote on June 30, were “complicit” with Schering-Plough in criminal activity.
By then, he knew that his future with the FDA was over. “When I began raising these safety issues in the beginning of May, I knew this was the end of my career,” he said.
Thomas Laughren’s FDA
By going to Congress to blow the whistle, Kavanagh was presenting the agency’s impending approval of asenapine as a deviation from the norm. Yet, there was a 20-year record of psychiatric drug approvals that showed that this was not the case. Under the leadership of Thomas Laughren, the FDA had a history of approving psychiatric drugs that were, at best, of marginal efficacy, and a history of doing so knowing that the sponsor company had sought to hide, or at least obscure, the drug’s side effects.
Given this history, which has been well documented, Kavanagh’s accusations in this case were really a charge against the FDA’s standard operating procedures, at least in the psychiatry division. And the asenapine NDA wasn’t a particularly egregious case.
Laughren had come to the FDA in 1985, first serving as a team leader in the Division of Neuropharmacological Drug Products. As Laughren later wrote, in this position he “directly supervised the medical officers involved in the review of all drug development activities conducted under INDs and the review of all NDAs and supplements for new psychiatric drug claims.” In 2005, he became the director of the Division of Psychiatry Products, where he continued to oversee the “review of all NDAs.”

The first NDA that Laughren would have reviewed in his team leader position would have been for Prozac (fluoxetine). While this drug was promoted to the public as a breakthrough medication for depression following its approval in late 1987, the clinical trials told a different story altogether.
Early during the clinical trials of fluoxetine, it was found that it could induce an intense agitation in some patients. In response, Eli Lilly amended the trial protocols so that patients could be given a benzodiazine as a concomitant medication. As Eli Lilly’s Dorothy Dobb later admitted in a legal case, this was “scientifically bad,” since it would “confound the results” and “interfere with the analysis of both safety and efficacy.”
Eli Lilly conducted five clinical studies of its drug, and when the results from all five studies were pooled, the improvement on HAM-D scores—the scale used to assess depressive symptoms—was only one point greater for the fluoxetine patients than for the placebo group, a difference that is meaningless. In addition, Eli Lilly had engaged in various coding shenanigans, directing its investigators to record drug-related adverse events as “symptoms of depression,” and changing reports of “suicidal ideation” on case report forms to “depression.”
The FDA’s medical reviewers spotted much of this deception. Eli Lilly, wrote FDA reviewer David Graham, had engaged in “large-scale underreporting” of the harm that fluoxetine could cause.
Even so, the FDA gave fluoxetine its approval, and the SSRI explosion was on. Other companies developed similar SSRI antidepressants, and the FDA kept to the standard it had set with fluoxetine. Pfizer conducted six clinical studies of sertraline (Zoloft), and in four of the six, it failed to beat placebo. There was a fifth study that was “questionable,” and a sixth that was positive for sertraline. As a Pfizer employee confessed in an April 11, 1991 memorandum, sertraline had “received an unfavorable review in a number of countries. The common key issue is that regulators are not convinced of sertraline’s efficacy versus placebo.”
But the FDA gave Pfizer the green light, and soon Zoloft was on its way to becoming a best-selling drug. The efficacy data for the SSRIs that followed were much the same.
Next up were atypical antipsychotics, with risperidone (Risperdal) and olanzapine (Zyprexa) leading the charge. Johnson & Johnson, in its risperidone trials, compared multiple doses of risperidone to a high dose of haloperidol (the comparator drug), a design that allowed Janssen to cherry-pick the best results from one of the three risperidone doses and compare it with a dose of haloperidol certain to cause many adverse events. This was a biased design that could be expected to make risperidone look good, and FDA reviewers weren’t fooled. As they noted, these studies were “incapable of providing any meaningful comparison of the two drugs.”
Similarly, FDA reviewers concluded that Eli Lilly’s trials of olanzapine were “biased by design” against haloperidol, and thus its large phase III trial, which wasn’t placebo controlled, provided “little useful efficacy data.” Twenty patients treated with olanzapine died in the trials, and the FDA’s Paul Leber warned that that “no one should be surprised if, upon marketing, events of all kinds and severity not previously identified [in the trials] are reported in association with olanzapine’s use.”
This was how testing of psychiatric drugs and their approval took shape during the first decade that Laughren served as a team leader in the FDA’s Division of Neuropharmacological Products. Drugs that showed little efficacy and were tested in biased trials were approved, even as risks were minimized or obscured, and then they were promoted as breakthrough medications, which rang up billions in sales.
Many of the pharmaceutical companies then aggressively marketed their drugs for off-label use in children and an ever-expanding percentage of adults. The FDA mostly stood by as this happened, and what can be understood today is that the selling of psychiatric drugs during this period evolved into a fraudulent enterprise. Eli Lilly, Johnson & Johnson, GlaxoSmithKline, Astra Zeneca, Abbot, Bristol Myers Squibb, Park Davis, Forest Laboratories, Novartis, Warner-Lambert, and Otsuka all eventually paid fines to the federal government for improper off-label marketing of their psychiatric drugs, with several pleading guilty to criminal charges.
Yet, even while he wore his FDA hat, Laughren helped promote psychiatric drugs and their off-label use. In a 2007 complaint to FDA Commissioner Andrew von Eschenbach, the Alliance for Human Research Protection (AHRP), a watchdog organization, prepared a detailed list of Laughren’s “collaborative ties with pharmaceutical industry officials and industry-financed psychiatrists in academia and professional associations.”
AHRP provided links to sourced documents in its complaint. Laughren’s activities included:
- Participating in an industry-sponsored consensus panel convened by the American Academy of Child and Adolescent Psychiatry that recommended off-label uses of psychiatric drug in children.
- Co-authoring more than a dozen articles with industry-funded “thought leaders,” who were being paid to act as consultants, advisors, and speakers. In one instance, he co-authored a book chapter with the chief medical officer of Eli Lilly, Leigh Thompson.
- Serving on a “development panel” for a “Mood Disorders” conference underwritten by major pharmaceutical companies. The 2002 report endorsed depression assessments for a broad range of patients with physical ailments—cardiovascular disease, cancer, Parkinson’s, AIDS, and others—that was sure to expand the market for psychiatric drugs.
Laughren also earned the ire of many parents when it became known that he had dismissed concerns about SSRIs stirring suicidal impulses in children. In 1996, AHRP’s complaint noted, a medical review officer at the FDA had reported a seven-fold greater incidence of suicidality in children prescribed sertraline. In response, Laughren wrote that “I don’t consider these data to represent a signal for suicidality in either adults or children.”
Then, in 2004, Laughren prevented an FDA reviewer, Andrew Mosholder, from speaking at a public hearing on whether antidepressants increased the risk of suicide in children and adolescents. Mosholder had concluded that trial data showed that to be so, but Laughren and other FDA officials, the Wall Street Journal reported, feared that he would “condemn the drugs too strongly before the advisory committee.” Laughren presented Moshholder’s analysis, but “stressed the unreliability of the data instead of the possible risk from the drugs.”
AHRP’s complaint detailed other instances where Laughren had worked to get a drug approved that other FDA reviewers had raised red flags about. In 2007, the FDA’s medical officers recommended that Eli Lilly’s application for pediatric use of Zyprexa should be rejected, both because of safety concerns and because nearly half of the data had come from Russia, which the FDA officers suspected might be fraudulent. Yet on April 29, 2007, Laughren overruled them and deemed Eli Lilly’s application for pediatric use “approvable.”
Such were the prevailing standards for approving NDAs of psychiatric drugs under Laughren’s leadership. There was a history of the agency bending over backward to find evidence of “efficacy,” tolerating trials that were “biased by design,” and letting sponsors get by with safety reports that, in one manner or another, sought to obscure the possible harms their drugs could cause.
Congress’s Mandate
While Laughren came in for a fair amount of public criticism, he was, in his efforts to get new drugs approved, following a congressional mandate that emerged in the 1990s. During the Reagan era, conservative groups regularly complained that the FDA, with its lengthy reviews of NDAs, was thwarting the commercial interests of pharmaceutical companies and by doing so—or so the argument went—compromising public health. Newt Gingrich, who rose to Speaker of the House in 1995, complained that the FDA was the “leading job killer in America.” The message was clear: The FDA needed to become an agency that helped bring new drugs to market.
The pharmaceutical companies also had newly gained financial influence over this review process. In 1992, Congress passed the Prescription Drug User Fee Act (PDUFA), which required pharmaceutical companies to fund the FDA’s reviews of its New Drug Applications. This provided the industry with financial leverage over the FDA—if the agency didn’t more readily approve drugs, the industry would lobby hard against this act when it came time, every five years, for Congress to renew it.
All of this served to corrupt the FDA. In a 2006 survey of FDA scientists, one-fifth responded that they had “been asked, for non-scientific reasons, to inappropriately exclude or alter technical information or their conclusions in an FDA scientific document.” Forty percent said they feared retaliation for voicing safety concerns in public.
Meanwhile, David Graham, who had warned about Eli Lilly’s underreporting of Prozac’s harms, told Congress in 2004 that he had been told “by his superiors to not warn the public about dangers of drugs like Vioxx,” which eventually was recalled. After he did warn the public, he testified that he was “marginalized by FDA management and not asked to participate in the evaluation of any drug safety issues. It’s a type of ostracism.”
The following year, Graham—who was then associate director of the FDA’s Office of Drug Safety—stated that the “FDA is inherently biased in favor of the pharmaceutical industry. It views industry as its client, whose interest it must represent and advance. It views its primary mission as approving as many drugs as it can, regardless of whether the drugs are safe or needed.”
Given this history and agency politics, Kavanagh’s protests, both within the agency and to Congress and the Office of the Inspector General, were almost certain to fall on deaf ears. There was nothing unusual with the agency’s impending approval of asenapine. And he could expect to be ostracized—and perhaps worse—for making a legal fuss about it.
This was just more of the same, and even as the FDA was going through the review process, Hassan publicly expressed dismay in a front-page Wall Street Journal article that asenapine had not yet been approved: “What will it take to get new drugs approved? The point is, we don’t know.”
The article, titled “Drug Makers Say FDA Safety Focus Is Slowing New-Medicine Pipeline,” was published on June 30, 2008. That was less than three months since the Zetia fraud had made headlines, and yet, in this article, Hassan was given a pulpit—and the high moral ground—to complain about the FDA being slow to approve asenapine.
Kavanagh’s Complaints Are Dismissed
Kavanagh’s whistleblower complaint was quickly dismissed. A couple of FBI agents interviewed him, but concluded this was a case of different opinions within the FDA about asenapine’s efficacy and safety. At the same time, both the FDA’s reviewer of safety data, Robert Levin, and Laughren wrote up summary reports that, within the agency, put the matter to rest.
In a June 26 review, Levin provided brief case histories of the 22 deaths of patients treated with asenapine. He dismissed all but two as “probably unrelated” to the drug, and even in the other two, he downplayed their possible significance.
There was a suicide by a 67-year-old man that an investigator, in the case report form, had concluded was “possibly” related to the drug, but, Levin said, the investigator had “provided no clear rationale for why that would be.” The neonatal death, while possibly related to the drug, could also be explained by the mother’s history “of 3 previous premature deliveries,” he wrote.
That was that: an approvable bill of health for the drug. There was no mention of a death due to an allergic reaction, either; as the company’s safety summary had said, the 57-year-old woman had died from a pulmonary embolism.
On August 1, Laughren determined that asenapine was approvable for both schizophrenia and bipolar I. He wrote a few lines about each of Kavanagh’s main complaints.
Re asenapine’s lack of efficacy for schizophrenia: “From what I have seen, he [Kavanagh] has not made any credible arguments to support these broad statements.”
Re asenapine’s lack of efficacy for bipolar I patients with mild to moderate symptoms: “I consider [his analysis] a flawed approach to looking at these data . . . . these severity scores have no diagnostic significance and it would not be appropriate to suggest that baseline severity could be used to select patients for treatment. In my view, the correct interpretation of these data is that asenapine has been shown to be effective in the acute treatment of mania and mixed episodes, and I think it should be left to clinicians to decide how to select patients for treatment.”
Re the company’s hiding of safety risks: There was no reason to think that the agonism of the 5HT2B receptor would be a particular risk; the pregnant woman whose newborn died had a history of troubled pregnancies; the healthy volunteer had suffered a fainting episode, not a stopped heart; there was no evidence that the 57-year-old woman had died from an allergic reaction; and suicide was a risk of the two diseases.
“I do not share [Kavanagh’s] view that the sponsor failed to report critical safety information that they possessed, or that they misrepresented what they did submit in an attempt to mislead, at least based on what I have reviewed,” Laughren wrote.
There was one aspect of Kavanagh’s Office of Clinical Pharmacology Report that Laughren found worthy, which was that the company needed to provide more information about the drug’s metabolites. “If OCP is correct in its assertions, however, we have little assurance that the animal carcinogenity data or reproductive toxicity data are relevant to humans, since we would know so little about what is circulating in humans. Until this issue is resolved, I am inclined to agree with OCP that this is a serious deficiency.”
Fifteen days after Laughren wrote his “approvable” report, Kavanagh was escorted from the FDA’s office. The termination letter he subsequently received stated that, in addition to behavior that could be linked to his whistleblower efforts, he was being fired for having been discourteous and aggressive in meetings with pharmaceutical companies.
The deficiency in Schering-Plough’s NDA regarding asenapine’s metabolites did slow the issuance of a formal approval letter, but that came in early 2009. An advisory committee meeting was held in July of that year, with the committee voting 10-2 to approve asenapine for schizophrenia and 12-0 to approve it for bipolar. Kavanagh was not allowed to speak at the meeting; his concerns were not aired. The drug, marketed as Saphris, was launched into the market that fall.
The Payoff for Hassan
When Hassan led Schering-Plough to acquire Organon, he knew that if asenapine were approved for both schizophrenia and bipolar, it would increase Schering-Plough’s value. In March 2009, shortly after the FDA notified Schering-Plough that asenapine was “approvable,” he negotiated the sale of his company, in the form of a merger, to Merck for $41.1 billion.
Published accounts of the merger stated that Hassan and nine other Schering-Plough executives would get $132 million in the deal. Hassan’s share of that was estimated to be $51 million in cash and pension benefits, although there were reports that put Hassan’s take much higher.
The merger with Merck closed that fall, and Hassan was once again hailed for his successful stewardship of a pharmaceutical company. In August of 2010, CBS News published an interview with Hassan titled: “How I beat the odds on a $14 billion drug deal.”
The key, Hassan told CBS News, was that the compounds that Schering-Plough acquired when it bought Organon, “proved valuable, specifically the schizophrenia drug asenapine, trade name Saphris.”
“Many people were generally not excited about Organon. There was a lot of skepticism about Saphris, which Pfizer had walked away from. The prevailing view was that Pfizer gave up on asenapine because they saw major problems with it either scientifically or commercially. Companies, Wall Street analysts, and even the press wondered aloud how we could succeed where Pfizer could not, and if eventually we would come to the same conclusion that Pfizer did. But Saphris did get approved by the FDA in August [2009] and subsequently launched . . . So this was something that we accomplished that was not previously clear to others. Very few deals turn out as well as this one.”
The merger, however, did not turn out particularly well for Merck. Saphris didn’t offer any advantage over the atypicals already on the market, and in 2013, with Saphris generating net sales of only $150 million that year, Merck sold its marketing rights for asenapine to Forest Laboratories for $240 million.
Laughren Psychopharm Consulting
In 2012, Laughren left the FDA to form Laughren Psychopharm Consulting with the goal of helping pharmaceutical companies bring their drugs to market. One of his first clients was AstraZeneca, a company he had helped out three years earlier when it was seeking to get Seroquel approved for a wider range of conditions, including for use in adolescents.
At the advisory panel meeting, Wayne Ray of Vanderbilt University told of his research that had linked sudden cardiac death to Seroquel when it was used with certain other medications. However, as Science magazine later reported, Laughren dismissed Ray’s research and told the panel that AstraZeneca’s own clinical findings, which had found no increased risk of death, should be considered the definitive research.
The panel voted overwhelmingly to approve quetiapine for new indications and it didn’t require any labeling about the risk of sudden cardiac death. Within two years, the FDA had received reports of 220 deaths due to cardiac events related to Seroquel use, and it then required AstraZeneca to warn of this risk on its label.
Science magazine’s article was titled: “FDA’s revolving door: Companies often hire agency staffers who managed their successful drug reviews.” Laughren, it seems, illustrated this career path best.
A Prophetic Warning
Kavanagh, for his part, has never put his “whistleblower” efforts to rest. Again and again, he has tried to bring public attention to the FDA’s approval of this drug and other atypicals for bipolar 1 and to the harms that have come from other FDA approvals. In addition, in his subsequent legal actions and letters to presidents Obama and Trump and to members of Congress, he has sought to make the argument that he was fired for his whistle-blowing efforts in 2008.
He has gathered some additional ammunition for his whistleblowing efforts along the way.
During the first 10 months that asenapine was on the market, the FDA received 52 reports of patients suffering a “serious allergic reaction” to the drug (type 1 reactions, which include anaphylaxis). Since it is estimated that only 1% to 10% of adverse reactions to a drug are reported to the FDA’s Medwatch program, this suggests that there were between 520 and 5,200 patients treated with asenapine during its first 10 months on the market who had a severe allergic response to the drug. On September 1, 2011, the FDA issued a warning related to this risk, requiring that it be added to the label.
A second worry of Kavanagh’s was that asenapine and other atypical drugs, when prescribed to pregnant women, would lead to neonatal deaths. In 2011, as Kavanagh was getting ready to file his qui tam lawsuit, he searched Medwatch reports for deaths due to atypical drugs, and found the following:
- The Seroquel file told of 1,844 deaths, with more than 5% of those deaths in infants less than two years old.
- From 1% to 3% of deaths from Risperdal, Geodon, Abilify, and Zyprexa were in this age group.

In his qui tam lawsuit, Kavanagh calculated that from 2000 to 2012, there had been about 3,500 infants under two years of age who had died due to exposure to atypicals, with this exposure—it would seem—coming during the pregnancy and through breastfeeding. Yet, even this number is undoubtedly an undercount: A 2015 review of neonatal outcomes with “exposure to antipsychotics” during pregnancy found that there was an increased risk for “major malformations, heart defects, preterm delivery, small-for-age gestational births and decreased birth weight.”
In his lawsuit, Kavanagh also sought to tally up the harm done to bipolar I patients with mild to moderate symptoms who are nevertheless prescribed an atypical antipsychotic. He estimated that 500,000 patients fall into this subgroup and, given a mortality rate of 1% to 1.2% for volunteers in antipsychotic drug trials, he calculated that this would lead to 5,000 or more deaths each year. “Not to mention,” he added, “the numerous other serious adverse effects that occur with antipsychotics including seizures, blood clots, heart attacks, diabetes, neurologic toxicities, etc.”
Since a qui tam lawsuit alleges that state and federal governments are being defrauded, in this case because Medicaid and Medicare were paying for drug treatments that Kavanagh alleged were ineffective and harmful, the possibility of success is usually dependent on whether the federal government “joins” the lawsuit. And while Kavanagh’s lawsuit alleged that the manufacturers of these drugs had sought to hide their harms, it also alleged that the FDA had been complicit in that fraud. The federal government would have had to throw its own agency under the bus to join the action and it chose not to do so, which led to the dismissal of his lawsuit in 2014.
After that, Kavanagh periodically renewed his petitions to elected officials and government agencies. He did so in 2016 and 2017, and this past May made one last push, sending letters and summaries of his complaints to President Trump, Congressman Jamie Raskin, Senator Charles Grassley, the House Committee on Oversight and Reform, and the Department of Justice’s Office of Inspector General, Investigative Division. This last effort of his is still pending.
Counting Up the Deaths
In his estimate of deaths, Kavanagh focused on bipolar I patients with mild to moderate symptoms. Yet, the FDA’s approval of atypicals for bipolar 1 disorder naturally led to these drugs being prescribed to bipolar II patients and those diagnosed with bipolar spectrum disorder, meaning they too are exposed to the hazards of the medications, even though there may be little evidence from randomized clinical trials that they provide a meaningful benefit for mania and mixed episodes.
Asenapine’s label told of a long list of health risks associated with its use, which were presented as typical of “atypical” antipsychotics. They include: akathisia, somnolence, neuroleptic malignant syndrome, extrapyramidal symptoms, dystonias, tardive dyskinesia, hyperglycemia, diabetes mellitus, weight gain, syncope, leukopenia, neutropenia, agranulocytosis, QT prolongation, hyperprolactinemia, seizures, potential for cognitive and motor impairment, body temperature dysregulation, and dysphagia.
Various studies have found that antipsychotics double the standard mortality rate (SMR) in non-psychiatric patient groups, and in general mental health care as well. Given this fact, it is not surprising that the “mortality gap” between bipolar patients and the general population has widened since the prescribing of atypical antipsychotics for bipolar disorders became commonplace.
In a large UK study, investigators found that the SMR for bipolar patients jumped from around 1.4 in 2006 to 2.5 in 2014. In Denmark, SMR rates for bipolar patients increased from around 2.4 in 1995 to 3.0 in 2014.
Translating that increase in mortality rates into a numbered death toll for bipolar patients is an uncertain task. Yet, even conservative calculations produce an estimated count of 15,000 additional deaths per year, or a total of 180,000 additional deaths since 2008, when Kavanagh first sought to warn of this risk.
The FDA Under Review
Revisiting Kavanagh’s whistleblower complaint provides a fresh way to see the FDA’s review process and “approvable” standards for psychiatric drugs in action. What can be seen is that the FDA will approve a drug that has shown marginal “statistical” efficacy in clinical trials, even though that “benefit” falls far short of being clinically meaningful and its use will expose patients to a long list of hazards. That is a drug-review standard that is certain to introduce drugs into the market that, in public-health terms, will do more harm than good.
****
MIA Reports are supported, in part, by a grant from the Open Society Foundations



Now that the FDA’s been exposed, I expect it to leap into action with attempts to take niacin and vitamin C off the market (“these deadly drugs have been ignored too long!”).
Report comment
How would this event at the New York Academy of Sciences fit into the time frame of your story? See: http://www.nyas.org/search-results/?searchedString=Bipolar Disorder an event that happened in Dec 15, 2009 I would attend because the local psychiatrist would be presenting and I am curious about science. To hear the three tests by which the meds were tested on animals was bizarre, to speak up and raise questions in an audience of up and coming physicians and researchers was even stranger. To have attended the meeting inside the first of the New World Trade Towers where the New York Academy of Sciences rents space weaves even a more twisted path into the stories shared on these pages. I think some cognitive dissonance would occur, some good trouble as some have been known to say, by my being in the room and asking some questions as one who once used the medications.
There seems to be some strange funding of this event, when inquiry into the source of the funders was made and people had realigned within the pharma industry.
But then when one considers the scale and size of this real estate and the families that own the real estate see: https://www.madinamerica.com/2020/05/jinxed-persecution-evan-durst-kreeger/ how could one not realize the threads by which our lives have been placed at risk or even shortened. Daniel Liebskind, an architect who was affiliated with the University of Kentucky, would guide the rebuilding of the Towers. One wonders about the wealth generated and lost, but more importantly, the stories of Prozac, Louisville and how the truth, the whole truths have been kept from surfacing.
This work is more than being a whistle! Thanks for the insights…. will have to study further….
Look at the location of where Shering-Plough was headquartered, the histories of the company and then try to understand the level of intelligence that was turning the merger mania…
Report comment
Bob, well done!
Thanks for this well researched and powerful exposure of the FDA and its incestuous connections to Big Pharma. All of which leads to an untold number of human casualties and an enormous amount of physical and psychological harm to millions of people.
It is difficult to decide which quote from this exposure to highlight, because it is packed with so many indictments of a thoroughly corrupt system at every level.
This is one quote that stands out:
“All of this served to corrupt the FDA. In a 2006 survey of FDA scientists, one-fifth responded that they had “been asked, for non-scientific reasons, to inappropriately exclude or alter technical information or their conclusions in an FDA scientific document.” Forty percent said they feared retaliation for voicing safety concerns in public.”
It is safe to assume (due to the issue of fear of retaliation) that the actual numbers are MUCH HIGHER when it come to direct efforts by Big Pharma to corrupt the research process into most drug approvals.
And when you look at the hundreds of billions of dollars that are at stake in all these transactions (with the multitudes of mergers and corporate buy outs, along with the swapping of jobs between pharma and the FDA), we must ask the question that is the one immense “elephant in the room” that simply cannot be ignored:
Given the pervasiveness of the capitalist profit incentive in almost every aspect and transaction affecting the scientific process of drug approvals, is it even conceivable that you could EVER have a fair AND safe approval process within a profit based capitalist system?
Obviously, ALL such drug research and approval needs to be completely INDEPENDENT from the marketplace. But is this type of reform really possible within a capitalist based system given the pervasiveness of the influence of the profit motive and its connection to the corruption process?
I say the answer is a resounding, NO! The System will tolerate these type of political exposures in the “market place of ideas” as long as it doesn’t FUNDAMENTALLY challenge the continuation of the status quo.
While these type of political exposure are incredibly valuable to educate people and rally forces to oppose this blatant type of death causing corruption, there is now a clear MORAL IMPERATIVE that we all have in the growing political crises facing humanity at this junction in human history.
That moral imperative REQUIRES US to always include some associative exposure of the capitalist profit motive and it pervasive NEGATIVE influence on every human transaction in all realms of society, especially as it affects both science and medicine.
To do anything less, is to fail our moral obligation to speak the truth, and face the actual systemic impediments to all human progress. “Dare to Struggle, Dare to Win!”
Carry on, Bob!
Report comment
Thanks for the essey. My profession is global agricultural policy in FDA and there are the same problems.
The co-operation with Monsanto (nowadays Bayer) and its corruptions has been known in food marketing. The EFSA trusts FDA and Bayer without scientific thinking. The food safety has taken down in the world because of GMO agriculture.
Monsanto (Bayer) has taken up suicides in Asian farms when it has said that GMO is the only possible agricultural form. “Buy the seeds of GMO or dye!”, says Monsanto (Bayer) in India since 2007.
Report comment
Yes, I have heard of these suicides among farmers in India. Tragic.
Report comment
There are some new educational policies in my country, subsumed under the rubric of “National Educational Policy 2020”. The wikipedia page states:
“More focus will be given to students’ health, particularly mental health, through the deployment of counsellors and social workers.”
Does this mean more psychiatry will enter into the lives of children at a very young age (especially in a country that is not yet as psychiatrised as North American and European nations)?
https://en.wikipedia.org/wiki/National_Education_Policy_2020
I know there are always children who endure some form of suffering (particularly teenagers). But I don’t know if they’d realise what they’re getting themselves into (especially at such a young age with very little power) and the future ramifications on their lives.
Report comment
From what I know, the situation is as you state.
Psychiatry is always in search of new populations that can be convinced to embrace their treatments.
Most of the “educated” world now laughs at the idea that psychiatry might NOT be have the highest level of expertise in the field of “mental health.” And so research and state policies continue to bend in their favor.
For me, it has come down to the need for an entire reorientation at a grassroots level. We can still fight against bad policy. But it seems the majority of policy makers have fallen for the psychiatric narrative. After all, the mind IS in the brain, is it not?
It isn’t. But who is willing to believe that? It starts with those who already realize something is wrong.
Report comment
Thank you Robert for the amazing amount of work you put into all you do.
Now we just have to figure out WHAT we can trust.
Educating the public is all that is left.
It’s not just “what” the pill pushing drug makers and the FDA hides that is scary, it’s what they don’t hide
and get away with.
And the continual push by psychiatry for more victims. Yes they do push for victims, by making people believe they are ill, via “mental health” propaganda.
Report comment
This is a very thorough piece of work, and I confess I could not make myself read the whole thing carefully.
But to me it tells a story of criminality that runs deep in this system. And it raises the question: Do we really need the incentive of high profits to create good medicines? Or is this incentive more likely to lead people to lie, cheat, and kill?
Though I turned away decades ago from the idea that some sort of anti-capitalist upheaval could result in a more ethical and less criminal society, the track record of the profit motive has included many dismal failures. My feeling is that any actual ethical “mental health” system would team up with a system of justice to identify the real criminals of society and restrain them from acting out their delusions on the population at large. If that could be accomplished, even if only partially, we would be on the right track, and ordinary people who the system currently labels “mentally ill” would be free to go about their lives with much less harassment from the truly sick.
Report comment
The collusion/codependance between psychiatry and the justice system is the worst of it all.
Psychiatrist can imprison, abuse and murder people basically at will, because judiciary is turning a blind eye in exchange for diagnosis of people they deem especially dangerous.
Report comment
They fail miserably at actually keeping society safe, since the prisons release dangerous offenders with warnings to the public that they are now at risk of these released people. Child rapists are released routinely…And for some reason, the actual dangerous offenders are not forced into psychiatry units lol. And yet someone that has never offended is court ordered. The ones psychiatry “treats” are the most vulnerable, starting with psychiatry being the perpetrators and next is no quality/honest medical care being awarded them, plus no honest legal representation.
And then of course we have the legal killings, where big pharma and the prescribers are responsible for many more. Licence to hurt or kill.
Report comment
Psychiatry already knows it can do nothing about the real criminals (chief among those, the ones known as having Anti-Social Personality Disorder). They admit to this in many popular articles. I wouldn’t be surprised if the whole concept of the “criminal mind” disappears from the DSM completely if and when it is revised again. And then they will be able to say, “we were wrong – there is no such thing.”
Report comment
Sam, that’s an interesting point about non-medicalized violent/extreme offenders vs court-ordered ‘non-offenders’. I’d like to see an article and data on that.
Report comment
Who publishes data? Most important, how is data gathered and on what precepts.
Even simple data that comes out of hospitals is rarely completely honest.
Now I can appreciate doctors messing with trying to keep people alive will be full of bumbling efforts because they are limited in what they are presented with. So I do not have issue with the limited abilities and knowledge, however, I have great issue with the dishonesty surrounding the treatments and following “data”. So the question is, can we ever fully trust any “data”.
Report comment
Sam thank you,
In any case, I thought your comment was relevant. Sorry for this long-winded response.
I understand your concerns, and no, we very often can’t trust data. I read a book in high school on the philosophy of statistics so I have been concerned with these ideas. I should have used the words ‘facts’ or better, ‘opinions’. Are you comfortable with those? Because even by saying that, I don’t pretend that facts or ‘truths’ are just boxes to be opened. I could have also said observations or interpretations. Do you have the same attitude toward this article and ‘inefficacy’ and danger of Saphris (asenapine)? I actually do, but I wouldn’t swipe left on the whole thing, which follows the trail and often takes for granted the ‘data’ of clinal trials, patient reporting and various data points, and the apparent accuracy of diagnostic scales, at least within their own definitions. There is obviously much to be desired throughout the whole thing, both the original sources and Whitaker’s and whistleblower’s whittling of the accrued ‘information’.
I’d be glad to hear a series of interviews/accounts with ex-violent-felons who completed their ‘penance’ as defined by law and their experience with or without psychiatry in and outside of prison. And I’d be glad to hear interviews/accounts with court-ordered, but not outright illegal or violent, people mandated to be in the psychiatric hospital or out-patient management. And I would consider some of this type of information ‘data’. Someone or a collaboration of people may choose to compare and contrast those interviews/accounts, trying to form insights and judgements.
Anyway, I get it. It’s all imperfect and nothing has the greatest history of valid or appropriate information for programs involving people. Still, I took statistics in college, and there is often — not always — a method to the madness of statistics; as well as explicit questions of assumptions and efforts to recognize misleading results. And I wouldn’t ever take that class again. When you put people into the picture as input, rather than classical physics or chemistry, it opens another can of worms.
Report comment
I_e_cox
You said: ” Do we really need the incentive of high profits to create good medicines?”
I believe there are tens of thousands of scientists (and young people who want to be scientists) who are purely motivated by the wonderment of science and discovery, AND definitely want their scientific creations to benefit humanity.
The profit motive actually distorts and corrupts science in ways that that seriously thwarts human efforts to advance our understanding of the world. Billions of dollars every year are spent researching and creating drugs that have no benefit for humanity, and are actually showing evidence of harmful effects.
Because Big Pharma CEO’s are purely motivated by the bottom line of profit (otherwise their job for the coming year is in jeopardy), they will do whatever it takes to continue promoting and producing certain drugs despite early knowledge that their initial investment was a complete failure.
Image how totally unleashed young scientists would be if this entire process was driven by a desire to make the world a safer and better place. Drug creations that did not work, or were unsafe, would be quickly abandoned, and all investment of time and money would be redirected in a different direction.
Richard
Report comment
I would argue rather that we need to remove the profit motive IN ODER TO make good medicines. Humanity needs antibiotics not antipsychotics. But, since those aren’t profitable…
Report comment
I think you might be right about this.
Report comment
The profit motive is bad for healthcare! This extraordinary report illustrates how. Healthcare provision freed of greed is available at much lower cost, more efficiently and effectively. For this reason most healthcare facilities until recently have operated on a professional non-profit basis.
It is possible and does happen that by and large trustworthy medical care is offered free at the point of care (paid for through taxes or other mechanisms). And it seems that still now most of the basic research and development of medicine (and technology generally) is conducted free of greed by reasonably honest scientists whose work is rigoursly examined and critiqued by colleagues. It’s only when something looks profitable that it’s hived off into the private for profit business sector. I was alerted to this fact by Noam Chomsky and confirmed it by research(sorry I’ve no links readily available). Pharma do have its own labs and research but their claim to need profits is pure poppycock, even in their own labs the scientist are not motivated by greed (who’d study science on the basis that it would make you rich) but nonetheless are under pressure to pander to the corporate bottom line. So they do do research and development but it’s hard to know how exactly how much as their ‘research’ budget includes do much of what is basically marketing! This doesn’t just apply to psychiatric drugs we’re it’s worst but to the other scandal of opiate dependence but to overprescription generally of anti biotic (fueling resistance) , statins, benzos, sleeping tablets, excessive unnecessary screening and testing.
Even in Europe our relatively effective health care systems (psychiatry not withstanding, although most people still believe mental distress arises from experience not biology this veiw hasn’t entirely infected the clinic for some strange reason although it has some effect) have not escaped the notice of business. A company previously best known for selling records and tourism has contracts worth billions to provide ‘mental health’ care and they havent being using it to enable people to dance around listening to their favourite or take us on holiday. Have you hoticed how you can walk into a therapists office with a love of music, hobbies and interests and walk out with ‘coping strategies’?
Report comment
I totally feel you on the “coping strategies.” There was a recent article on “ecotherapy” that made the same impression on me. Don’t take my hikes in the woods and turn them into some form of “therapy!” They are walks in the woods, and I love them, and that’s all that needs to be said! I don’t need “coping strategies”, I need meaningful and fun activities that make my life feel worthwhile. It’s not therapy, it’s called LIFE!
Report comment
Did just that Steve. A walk through the woods listening to the birds, the soft breeze rustling the leaves and along a river with its trickling sounds – beautiful, puts a smile on my face.
Report comment
@kindred:
I would not even mind drugs for severe depression and anxiety. But something without horrible side effects and which can be bought over-the-counter like aspirin or cough drops. At least the choice to take or not take them would be in your hands and you wouldn’t need the shrink system.
Report comment
Goes to show you the danger of the drugs. They need a script for the dangerous ones, 🙂 because Docs and drug companies cannot be sued. Not in any meaningful manner.
Report comment
Absolutely! Efforts are being made to repeal the “National Childhood Vaccine Injury Act” that Congress approved in 1986. No Vaccine manufacturer shall be liable in a civil action for damages arising from a vaccine-related injury or death associated with the administration of a vaccine.
Gates & Co want immunity from their coronavirus vaccine! This is insanity!
Report comment
The “efficacy” as treatment for people with “severe” symptoms of “schizophrenia” or “bipolar,” that any “anti-psychotic” supposedly is, pretty much isn’t true either. Suppressing symptoms, that aren’t objectively discernible amongst different “clinicians,” that are often politically based or biased, based on societal or cultural norms, don’t take into account that they might be expressing unexplored trauma or insights of any sort that’s not understood by the clinicians, or simply a need to break away beyond behavioral confines to allow for whatever else might be experienced there that could be critical to the development of the personality…
Even suppressing such symptoms, were it a sign of alleviating a disease, doesn’t pan out in the long run, where there’s more relapsing, more disability, loss of life, side effects, more paranoia against symptoms from society: might actually mean that symptoms can be best understood to be expressing something that can be understood in the long run, and not just “non-reality-based” neurology, a disruption, an annoyance, a danger.
Nor is the idea that a person is a danger to themselves and others panning out, because the treatment has proven to be more of a danger for the person receiving it and for society, given the epidemic, given the paranoia against what otherwise could be understood, and given the danger towards violence that psychiatric treatment can cause with it’s pharmacological agents: all clearly in correlation to the biological model for mental illness, a model that also clearly causes chemical imbalance, although it alleges it treats one.
Way back in 2003 the Hunger strikers https://mindfreedom.org/kb/2003/ very clearly pointed out how mental illness definitions are more based on societal constructs that define poverty, minority status, and war.
I hadn’t read the other articles yet, about the supposedly new drug, Lumateperone or Caplyta; How a drug 8 people or so have to be on for one of them to get improvement, and then the others most likely will get bad side effects, not to mention withdrawal symptoms would they want to get off of something that’s not “helping” them; when in reality that help (one in how many?) could be highly deceptive, highly fear based against symptoms that could otherwise be understood, given that in the long run what helps causes more relapsing, recycling, disability etc…..
And then in the article about Lumateperone: “As Lieberman and colleagues confessed in a 2017 paper, there has never been a “randomized, double-blind, placebo-controlled study” of an antipsychotic in medication-naïve patients. In other words, there is no good scientific record that these drugs are effective, even over the short term, in psychotic patients whose brains have not been changed by prior exposure to antipsychotics.”
I have read somewhere recently that whatever they identify as being the organic part of the disease turns up in people that haven’t been on medications yet, and those that are. That’s quite amazing. “WE HAVE FOUND A CAUSE WE CAN CALL BIOLOGICAL, but it turns up before and after medication.” They don’t mention that medication clearly caused swelling of the inner cortex, and shrinking of the frontal lobe, with anti-psychotics, but they said it was from the biological disease, before they were confronted with medications causing that problem; they also say schizophrenia comes from too much dopamine, but don’t share that anti-psychotics for “schizophrenia” in the end cause that as well, because the brain starts to produce more; same with anti-depressants causing serotonin depletion in the end.
People with a higher intelligence are more likely to have “psychotic episodes,” which means people who are going to be able to see past all of the corruption of “evidence”; people who are more creative are more like to have “psychotic episodes,” meaning people who can relate to an “invisible” world that expresses harmony, even thought it might seem “non reality based” because it’s invisible, people who are oppressed are more likely…
The dismissal of deaths, during the trials and afterwards, is like a war zone to take over a territory compromising the lives of who already live there, making those who live there scared of themselves, and if that doesn’t work make them out to be dangerous dissidents, and try to make everyone else believe it.
I’ve been “psychotic” and not only does society try to make you paranoid from understanding what the symptoms express, but it doesn’t even acknowledge that there was a reason for the anxiety or distress that lead to it, as if that never happened, no empathy for listening to a personal experience if it challenges their beliefs; as if it’s not expressing anything; beyond that when the subconscious starts creating perspective as “non reality based” as a dream that has meaning, but can’t be videotaped while it’s happening, that’s not acknowledged; and in such an environment where none of that very human experience is given leg room, is welcomed, is acknowledged, one starts becoming uncomfortable with the natural responses seeking expression, and pushes them away, resulting in a myriad of distractions to avoid such feelings, even what causes annoying “symptoms,” stuff that’s searching expression and won’t be pushed away; and then you might be told “don’t do that,” without again any acknowledgment of what cause and effect is – after years of this, and realizing every time I got “psychotic,” I started doing fill-in-the-blank again, at first fluctuating between the realization of it, and then acting it out again; until I finally realized I was pushing something away; but that also isn’t anything one can define in a “sane” way, it’s more OK, I don’t have to do anything, just feel this uncomfortable thing that isn’t going to hook up with society’s fear based demands that tell me survival isn’t being myself lest I find out who I am…….
And impossible things would always happen, they still do….
Report comment
Thank you, Robert, for helping to point out the FDA’s corruption, and why they’ve been approving neurotoxins for the psychiatric industry for decades.
“Asenapine’s label told of a long list of health risks associated with its use, which were presented as typical of ‘atypical’ antipsychotics. They include: akathisia, somnolence, neuroleptic malignant syndrome, extrapyramidal symptoms, dystonias, tardive dyskinesia, hyperglycemia, diabetes mellitus, weight gain, syncope, leukopenia, neutropenia, agranulocytosis, QT prolongation, hyperprolactinemia, seizures, potential for cognitive and motor impairment, body temperature dysregulation, and dysphagia.”
And this long list of horrendous side effects is okay to prescribe to anyone? Merely because it’s “typical of ‘atypical’ antipsychotics?” No, the antipsychotics are – and were – NEVER acceptable to approve, or prescribe, to anyone at all.
And, by the way, all doctors were taught in med school that both the antidepressants and antipsychotics can create psychosis, via anticholinergic toxidrome. And so called and unprovable “psychosis” is the number one reason people are prescribed these drug classes in the first place.
And the number one actual function of the psychological and psychiatric industries – those who “diagnose” people as “psychotic” – historically and today, is covering up child abuse.
https://www.indybay.org/newsitems/2019/01/23/18820633.php?fbclid=IwAR2-cgZPcEvbz7yFqMuUwneIuaqGleGiOzackY4N2sPeVXolwmEga5iKxdo
https://www.madinamerica.com/2016/04/heal-for-life/
Despite the fact that covering up child abuse is illegal. But the entire DSM “bible” believing “mental health” industry is a systemic child abuse covering up industry, by DSM design.
https://www.psychologytoday.com/us/blog/your-child-does-not-have-bipolar-disorder/201402/dsm-5-and-child-neglect-and-abuse-1
Report comment
Excellent report, Bob! The only problem I’m struggling with here is the timeline. I *know* for a fact that I was pushed to take Saphris in 2008 when I was erroneously placed on a drug unit at the local private mental hospital. IF this was indeed before Saphris was even FDA approved, I’m left to wonder if the attending psychiatrist was actually attempting to enroll me in a drug trial without my knowledge or consent. The timeline otherwise does not make sense to me. I was not at that campus again until 2014, at which point Saphris had been on the market for years. My refusal to try it was due to the lack of available information about it. What other explanation could there be? And is it legal to enroll inpatients into trials without their knowledge and consent?
I remember this time very clearly as both the physician and psychiatrist laughed and thought I was psychotic for claiming that the bites all over my body were from bed bugs. This, despite the fact that I had photographic proof of the infestation in my house, my boyfriend at the time was also bitten all over, I was participating in an online Flickr photo group sharing images of the bugs and their bites (with their unique ‘breakfast, lunch and dinner’ bite pattern, and had even taken a live bedbug in to show my outpatient psychiatrist. (And of course we all know now that bed bugs have made an explosive return thanks to the banning of DDT.) Yet I was told by the unit’s physician that bed bugs “didn’t exist” and had been eradicated 50 years ago. I was in fact, more educated on the subject than any of my treatment providers and yet treated like it was evidence of psychosis. It was a maddening experience. And I was pushed to try Saphris and told that my bites and itchiness were psychosomatic! It was absolutely summer of 2008. The only explanation I can think of is that they were attempting to wrangle me into a clinical trial.
I still have trouble wrapping my head around just how abusive psychiatry has been to me and how little credit I’ve been given in my ability to narrate my own story. Great article but it leaves me with more questions than answers.
Report comment
Kindred Spirit: If you were pushed to take Saphris in 2008, it would have been before it was approved for use. What happens is that after a company finishes its actual RCTs for NDA purposes, it then begins doing extension trials, which are unblinded and meant to show that the drug can be taken “safely” for longer periods of times. In this instance, there were so few people who were actually enrolled in placebo controlled trials that there was very little “safety data” with robust numbers of patients exposed to the drugs. So they ran these unblinded studies to get the exposure numbers up, which helps make it seem the drug has been throughly tested. And it meant a drug company payment to the psychiatrist who was trying to get you to take Saphris.
Report comment
Thank you for the clarification, Bob.
Report comment
That is appalling. I only wish it were surprising.
Report comment
The Power of the Pen.
Thank you Robert W. and Mr. Kavanagh.
” When he was about 40 years old, he told a psychiatrist of a time in his life when he had fallen in love, describing it as a period of great happiness. The psychiatrist viewed this as evidence of mania and newly diagnosed Kavanagh as bipolar.”
The twist, sadly.
Quick questions pertaining to Mr. Kavanagh’s most recent filing at the Federal level, with the current state of affairs, as they affect so many under “mental health providers care, custody and control”…
How many practicing actually administer and monitor these drugs in accordance to the recommended dosages? Is there ever a consideration for withdrawal timeframes of an individual by those practicing? Like an exit plan, is that mandated by States?
I have found in one instance, the loading dose and half life of the prescribed drug, (mentioned in the article) was found to be in the patient at 4X’s the recommended dose, yet never recognized. This situation meant an actual 5 month withdrawal.
As many remember as well, Jansen was the company during the timeframe of this investigative research- that was administering Invega to many nursing home elderly with deathly consequences until, a “civil” NOT criminal suit was brought.
In many instances it seems this may be the view of “cost of doing business”, at the inhumane expense of- life.
Mr. Kavanagh has shown to be fervent in his efforts to bring to light, the corruption within an unsustainable system. Thank you.
Report comment
Question. What do we DO about this? What are the conversations the politicians are having? Or are they having any?
Do they become curious about the “disabled” and dead numbers? The homeless? Do they become curious about the billions spent on harmful practices that are very visible to the naked eye? Has psychiatry helped the homeless beyond getting them a room in a rooming house with slum landlords? And IF that much.
So if psychiatry cannot prevent crime, and cannot produce happy productive people, then what service do they provide? Or does it matter? Is it the perfect economy where the poor and suffering ilk are the ones that actually keep everyone occupied in their paid by taxpayers jobs?
Then it would be reasonable to give that ilk more dollars, since they are employing many.
Report comment
Quite right, Sam. Government-paid employees are in charge of medicating “undesirables” in order to eliminate contact with the general population. Is this really a needed service, or is it a billing opportunity?
Who are these poor undesirables anyway? Are these products of society, the fruit of medicating circumstances and not a real and personal condition? Who would not feel depressed and desperate and suspicious in poverty and persecution? Medicating society: is it the old social engineering but with a more PC name?
Report comment
Perhaps we can “make friends” with some politicians and change their minds. This seems to be what psychiatry and Big Pharma has done.
The only other choice is to – very publicly – make the whole system appear as corrupt as it really is so that its base of popular support eventually erodes away completely. They will have only about 2% of the public left supporting them – the true criminals of this world.
Report comment
Politicians don’t think that way. They think “we need to keep a lid on mass shooters and show our constituents we care” and pass blank checks to fund the mh system. It doesn’t get much more nuanced.
Report comment
Politicians want first and foremost to keep their seats. For now they are ensuring as many people as possible are getting the ‘mental health care’ we so richly deserve. A British new Labour spin doctor frequently confesses to his battles with depression on public radio shows. For some reason he insists on calling it an ‘illness’ despite never being challenged on this point. As such despite being a man of considerable privelege and status he is simultaineously denied the insight he needs and acts in effect as an (unpaid) shill for psychiatry. He was in part the architect of the destruction of a party committed for all its faults to ‘the nationalisation of the commanding heights of the economy’ to one with unquestioned deference to neoliberalism and unqualified support for those ‘compassionate conservatives’ war. If this scandal is ever tackled properly it will maybe because of its impact on healthcare in the round and not bacause of its particular impact on psychiatry were people can be depended on not to care. I’m not holding my breathe but as the Poet Seamus Heany says –
History says, don’t hope on this side of the grave. But then once in a lifetime the longed for tidal wave of justice can rise up and hope and history ryhme.
Here’s hoping enough folk can struggle to escape the bludgeoning fog of capitalisms current blindness. We all depend on that, not just those of us afflicted by psychiatric adversity.
Report comment
Perhaps if survivors reacted in the way that black and white react to a death by cop, it would be helpful.
I have noticed that when a non black person gets shot, there is no “riot”.
The recent reaction again shows that a brother and sister have your back.
It might cause the politicians to at least notice. Talk and proof is not enough.
Report comment
Sam, it is not clear to me that riots occur when there are black people shooting other black people either.
Part of the ‘process’ is for every individual to make as much effective change within him or her self. ‘Be the change’ as it goes. Granted, easier said than done, to say the least.
Report comment
Nor riots from citizens killing police for that matter. But yeah.
Report comment
First – Know your enemy.
Report comment
Sam,
This organization is legitimate – with many action items: https://childrenshealthdefense.org/
Report comment
Thnx. I’ll say both positive shades & negative shades about this & asenapine. I’ve read Mad in America & The Zyprexa Papers, thoroughly appreciated them, & will add a couple comments about them at the end.
I wish the author would have elaborated more on the use of the PANSS scale. For example, obliteration of voices & visions (example of positive symptoms) as a test for efficacy is of course questionable, even if they are painful, interfere with work, etc. They are not illegal. In this sense, the fact that asenapine is not ‘effective’ for schiz might be a good thing. An example of what I mean is Dr. Carl Jung’s ‘psychotic break’ that amounted to authentic religious experiences and production of a book, The Red Book, that insures for $50 million dollars, bought & read by millions of people. Though somewhat unique, this shows how crippling & wiping away voices/visions & the mythopoetic imagination can be counterproductive. I’m fully aware of the complexities here, like homicidal command voices and running in the street naked, but I’ll set that aside for another time.
I’ve taken asenapine (as Saphris) for 5 years and was mostly unfamiliar with these details though not at all surprised. It’s the only ‘major tranquilizer‘ I’ve ever ‘liked’ or trusted, and moving to it from olanzapine (Zyprexa) was like a revelelation. One reason I am more friendly to it is I can take it once a night, instead of twice a day, which reduces ‘side effects’ like sedation during the day (after I can finally get up). Very unusual for this class of drug. Since starting (what I believe to be) an effective antidepressant, cheap generic ketamine, and along with nutrient supplements, I’ve been able to come down to 1.75mg-2.5mg from 20mg per day of asenapine since I was not brutally suicidal and ‘needed’ far less sedation. (I won’t highlight the psycho-social-environmental context right now). I cut the wafers to get these doses which is imperfect and tricky. I hope to get off completely, but right now, I can’t sleep without it. It’s hard to tease out these issues, as I’m basically addicted (habituated) to it. I’ve had various measures to get either free or lesser expensive supplies. Rarely my parents paid the $300 per month (at highest dose without coverage, it is $1500 per month). It is just now going generic, and they won’t be able to make as many billions of dollars off it. I’ve used their assistance program, Medicaid/Medicare coverage, and doctor’s request for free samples from their website. Of course, I would have preferred not taking it at all, but was long sucked into the rigmarole of conventional psychiatry.
Having said all that, I hope the authors of Mad in America (Whitaker) @ The Zyprexa Papers (Gottstein) take some time to analyze & highlight clinical nutrition & psychedelic therapy, though I’m very aware that we find many of the same issues as Big Pharma. Also to elaborate more on the notions of the personal & collective unconscious in ‘psychotic’ symptoms a la Carl Jung. I have found great benefit from these areas, and I believe can constitute ‘less-intrusive’ physical & psychological methods for mental health.
I’ve said a lot already, & I’ll leave it at that to very complicated topics. Thx again.
Report comment
Outstanding work, Bob. I am so grateful for you and all that you do.
What I find most troubling is this thought: what if the truth Kavanagh revealed about asenapine is broadly applicable to psychiatric drugs in general? I have no trouble believing the the poor efficacy and safety of asenapine – based on an honest and rigorous scientific assessment – applies to all or almost all drugs marketed as antidepressants, mood stabilisers, antipsychotics, etc. The implications of this possible or likely reality are staggering. It’s hard to disagree with Richard’s point that capitalism is ultimately responsible for this state of affairs.
Report comment
What Kavanagh and Whitaker reveal is applicable to every area of Big Pharma. The corruption goes way beyond capitalism. Pharma’s chemical warfare on humanity dwarfs the number of victims killed by all world wars and acts of terrorism combined. Here is a 6-part investigative journey, beginning with vaccine manufacturers. The same tragic b.s./corruption occurs with cardiac meds, pain meds, cancer meds, allergy meds, synthetic hormones/thyroid/insulin, ETC ETC ETC.
https://www.coreysdigs.com/vaccines-pharmaceuticals/measles-masterminds-millions/
And don’t forget medical devices: The Bleeding Edge: https://www.netflix.com/title/80170862
Parents are forced to administer chemo to children with cancer for 2-4 years AFTER they are in remission, (or risk children being taken away). Flipping The Script:
https://vimeo.com/ondemand/flippingthescriptparents
Report comment
“Parents are forced to administer chemo to children with cancer for 2-4 years AFTER they are in remission, (or risk children being taken away).”
There was a case like this here where the child was dying and his parents wished to take him home, but doctors wanted to try experiments on him. I can’t seem to find any of the information on the internet anymore. Winston Smith in the Ministry of Truth may be able to help lol
Point I wanted to make was that the parents get a choice, give the drugs or lose the child. Thus it is coercion, not force. Should they chose not to give the drugs, then force would be used but ……… most of them make the correct choice. I shuddeer when I think of how these people use the term ‘implied consent’. The odd fool like me needs to be ‘fuking destroyed’ publicly as a deterrent. Who said terrorism doesn’t work? Not Sun Tzu, see his demonstration about obtaining compliance for the Emperor of Wu.
And they are at War with the public. A quick look at what has become of our Police who are dressed ready for armed conflict and no longer police by consent but by force. Not wearing a bicycle helmet will get you pack raped in the cells lol. Let the punishment fit the crime eh?
Report comment
I’m reading KS and Robert, but I don’t want to overwork the reply button.
Rooting for you KS
Report comment
Why do I get an image of people sitting around discussing what type of wood is best for burning witches? The guy with the pine logs tampering with the data saying there was less screaming from the witches when they used his wood, and providing nice lunches for the Inquisitors.
“Hassan’s share of that was estimated to be $51 million in cash and pension benefits, although there were reports that put Hassan’s take much higher.”
Mr Hassan flips the bird from his yacht in the Bahamas and says “Wish you were here”, and the sad thing is, I do.
Report comment
I want to comment further as a supplement to what Bob has laid out here about Saphris and dysfunction (corruption) in the FDA drug approval process:
https://health.usnews.com/health-news/patient-advice/articles/2016-09-27/the-danger-in-taking-prescribed-medications
This very well sourced US News article reports that five times as many people die each year from taking prescription drugs as prescribed than die of either accidental drug overdoses or suicide, which would make this the fourth leading cause of death were it tracked. And these are not medical errors like dosage errors or misdiagnosis, but drugs prescribed appropriately for the patient’s condition. Johns Hopkins University tabulated separately that were it properly accounted for, medical error would become the 3rd leading cause of death. https://hub.jhu.edu/2016/05/03/medical-errors-third-leading-cause-of-death/
These articles are both from 2016, written in the lead up to the passage of the 21ST CENTURY CURES ACT, which we are all familiar with here at MIA, and which successfully eliminated many of the safeguards that were theoretically in place at FDA, but which Bob has shown were already inadequate to protect consumers from predatory pharmaceutical companies and their allies in the agency. https://www.theregreview.org/2019/05/07/kaplan-21st-century-cures-act/
A wider understanding of this corruption includes the influence of the prospect of future employment in the industry FDA regulators are tasked with policing. Bob detailed this with the case of Thomas Laughren, but it is best understood as a wide scale practice that puts ALL consumers at risk, not just psychiatric patients, as the revolving door between regulatory agencies and the industries they are tasked with overseeing has become the norm.
https://www.sciencemag.org/news/2018/07/fda-s-revolving-door-companies-often-hire-agency-staffers-who-managed-their-successful#
https://www.opensecrets.org/revolving/top.php?display=G
I understand the general public’s antipathy toward the psychiatrically labeled, but I don’t understand why the evidence of rampant financial corruption and hundreds of thousands of dead every year aren’t enough to generate widespread public outrage.
My father’s reaction to Lipitor led to his hospitalization where he contracted flu, which led to respiratory failure that ultimately killed him after 8 months on a vent in rehab. His death certificate simply claims “acute respiratory failure” with no mention of the initial prescription reaction or the hospital acquired infection. This system is broken. It’s broken across the board. And it’s been a bipartisan affair. Ronald Kavanagh sacrificed his career for the greater good, and we need to be clear about what we are really asking of those who stand up to the current power structure.
https://truthout.org/articles/former-fda-reviewer-speaks-out-about-intimidation-retaliation-and-marginalizing-of-safety/
https://www.govexec.com/management/2020/03/vas-whistleblower-protection-office-again-faces-allegations-retaliation-intimidation/163538/
https://www.brennancenter.org/our-work/analysis-opinion/whistleblower-explains-pitfalls-reporting-government-wrongdoing
https://www.govexec.com/oversight/2019/04/new-whistleblower-protection-office-under-investigation-retaliating-against-whistleblowers/156314/
Report comment
Great data! I will just take a moment to remind people that prescribing drugs within the standard of care is not a “medical error,” it is standard medical care. So the fourth leading cause of death in the USA is STANDARD MEDICAL CARE! There have been efforts to spin this as “medical errors,” so they can make it seem like these are mistakes made by “bad doctors.” But the truth is, this is not a result of “bad doctors,” the vast majority of these deaths, over 200,000 yearly, up to 400,000 in some estimates, result from standard medical care. This should be a terrifying statistic, yet somehow we are much more worried about the very rare possibility of a terrorist attack than we are about the carnage going on around us every day due to the awful outcomes of our own medical system.
Report comment
Between standard of care and legit errors, though, we’re talking numbers north of half a million deaths per year easily.
Report comment
Yeah, I think the 220k was just hospital deaths. I’m sure the larger number is correct. And very frightening!
Report comment
Yes indeed. The untruths is what is frightening. All those “respirators” waiting for covid are NOT a good thing.
Report comment
The numbers are certainly staggering, incredulous in fact. And very frightening indeed. Even reading Bob’s extraordinary report leaves me with a sense of disbelief and I almost want to insist it’s been fact checked(footnotes please), and I’ve been aware of these problems for decades. How can this scandal be happening?
I asked a professor of psychiatry for research evidence that the drugs ‘worked’ as she insisted over twenty years ago. She responded ‘Read a textbook’. To which I said I have. She couldn’t provide any proper rational for standard medical care. It’s over ten years since Irving Kirschs research showing that the tablets work no better than placebo more or less. I’m sorry but saying its ‘standard medical care’ doesn’t cut it. Professionals must be held to a higher standard than that, they are expected to have learnt something useful in order to qualify, to learn from an experience we can respect them for. I don’t know about you but were I come from we’re taught that ignorance is no excuse! If the evidence of the harms done by these do called ‘treatments’ is so readily ignored you have to wonder how this comes to be and why it’s not only allowed to continue but continues to get worse.
Report comment
Thanks Kindred Spirit
“Ronald Kavanagh sacrificed his career for the greater good, and we need to be clear about what we are really asking of those who stand up to the current power structure.”
I would like to ask him if he had his time over if he would do it again?
I know the interview I saw with Snowden he stated that the founding fathers were called traitors in their day. And yet now?
Report comment
Thank you Robert for MIA and another compelling report on rampant corruption in institutions the public are misled to believe are about patient safety. There has been harm from a variety of drugs that were pushed to the market but the harm and loss of life from psychiatric drugs is surely the most pervasive.
Silence is complicity. Thank God there are still some people left in this world who are willing to step up and speak out. Much respect and gratitude to Ronald Kavanagh for his integrity to fight against this corruption. I really hope his last effort has some success.
Report comment
“Silence is complicity.”
That’s my position Rosalee D. But what if I maybe just whisper rather than speak out? Will that get me off the hook when someone notices what has been done to so many people? A bit like those who expressed a hatred of the National Socialists once the war was over. There were that many? Gee , who’d have thought.
Report comment
Hey Boans, even voices that are not loud can get louder when they join the chorus. 🙂
Report comment
True Rosalee 🙂
Thanks for bringing tears of joy to a grumpy old mans face.
“I believe that one day this Nation will RISE UP………”
Report comment
There is another level to surface, if not already that shows the behavior of within organizations, governments, protected civil servants and “at will” or finance, how the “slavery” finds the numbers that lock up the silence within the administration of business (government, private and non-profit). This raises the questions that surround the nature of justice being blind? Or the challenge for this site and others to move the material forward for the scales to weigh in on the gravity of the situation. Many have been murdered, it seems indirectly or directly out of the arrogance of the medical practice or the We, the People as a silenced body rather than realizing the Art, as LIFE. –More later–
Report comment
Thank you, Bob, for another thorough and thoughtful essay. I have to say, reading all of this information about the corruption at the FDA as far as approving questionable and dangerous drugs, is it fair to assume that the same practices happen with other classes of drugs—-and vaccines? In relation to vaccines, most people I know are not eager to line up for the new Covid vaccine when it comes to market.
Report comment
“is it fair to assume that the same practices happen with other classes of drugs—-and vaccines?”
Yes indeed –
https://www.youtube.com/watch?v=vm4m28JvSUY
Covid vaccine – this is a Sars-Cov 2 virus. There has been no vaccine for Sars or Mers in 10 years.
Also see this Alina Chan paper:
https://www.biorxiv.org/content/10.1101/2020.05.01.073262v1.full.pdf
Report comment
Thank you! I will watch the video and read the Chan paper. I was really asking a rhetorical question—I actually don’t trust the FDA much if at all.
Report comment
The term ‘side effect’ is completely intentional; making a result such as death made to seem as innocuous as a spoonful of potato salad! ALL effects should simply, sadly, and accurately be called ‘effects’.
Report comment
Of course the word “anti-depressant” is in itself a misrepresentation. What causes “depression”? They don’t know and they don’t care.
Do the animals that these drugs are tried on have “depression”? How does the observer know? I mean the shrink establishes “depression” by an interview, yet he cannot interview an animal. And the cowering in the corner of a cage is fear, fear of another horrible test.
The observer also cannot ask an animal how it feels after an injection. Nor would he care if it could speak. There are no “chemical tests” no “scans” that can determine anything. The drug only ever makes it to market based on one thing, it did not kill the animal but it sure killed a bunch in horrific suffering before one was developed that did not kill within a few weeks.
The real trials happen on people. They are the ultimate guinea pigs. Also no real tests, just an interview and the only one that counts are the ones that lead to prescriptions.
The complaints are ignored just like the whimpering of an animal is ignored.
The only reason people ever tried these drugs is because of outright lies, misrepresentations, hope, trust, desperation.
Psychiatry decides you are sick before you show up for an appointment but they never told us it’s because no one in their right mind would see them.
Report comment
When they say that a cat food is “new and tastier” who tests it to make that claim?
Whats a euphemism for euphemism?
Unintended negative outcome or convenience killing that can not be proved because doctor keeps his mouth shut, and unlike the rest of the population can not be subjected to psychiatric torture (or can they?)
Report comment
Elan, it’s not just side effects, it’s withdrawal symptoms hiding addiction… both being used for further “diagnosis.” In fact that they even acknowledge such side effects and list various symptoms of what they also list as symptoms of a “disease,” considering that listed, it becomes pretty amazing that people don’t immediately start questioning what’s going on, but then again they feel safe being programmed to see pharmaceuticals as creating stability. Despite everything. And the withdrawal symptoms, if at all acknowledged also then are defined the same as symptoms of the disease….
And enough of the side effects are worse than the initial diagnosis needing “medications” also, as are the withdrawal symptoms.
It’s like thinking that having terrified a child to stop expressing their feelings, to stop having their own viewpoint, and thus to be open for indoctrination is how you raise children to be good productive beings. And then give them rewards. All to quake an alarm when they show that they don’t even know what they are thinking anymore (they’re “crazy” “psychotic”), and then suppress any method that might help them see it’s not a disease but an attempt to regain understanding of their own subconscious….
And the real break with reality is the people thinking they have to wield force to make people programmable, as well as disabling their minds with drugs to stop them from being able to question what’s going on.
As if truth is something you can only instill if you can coerce people into such beliefs by punishing them when they don’t believe it.
Report comment
Nijinsky, Thank you. I hear you. My heart goes out to the children, and my grandchildren. Public schools are criminally assaulting our children, especially those that comply with mandatory vaccination Children are forced to SIT indoors, 7-1/2 hours/day, with 27 minutes of outdoor recess. If the kids don’t comply with receiving a squirt of hand-sanitizer, (endocrine disrupting chemicals, EDCs), they are denied recess! The water at fountains is fluoridated. Lights are fluorescent. WiFi is showering 24/7 through all of them, from 4 years old and up. Junk in the cafeteria called food is endeathening! And then when they can’t perform to ‘the standard’, they are referred to school psychiatrist who of course, suggests ADD/ADHD drugs.
Lots of food for thought here. I appreciate the outlet. It’s rare to participate in such mature conversation. Thank you, to you and all contributors.
Report comment
Yeah, I use thieves oil diluted with olive oil, and I have a reverse osmosis water filter that takes out the fluoride. Fluoride it is said calcifies the pineal gland, and I noticed that would I sit down just to rest, especially when I was working on fiction, my mind would just go into hyper mode and spin images at me like at least two a second, as if it was trying to get me to dream but had to work against something, when I got a fluoride filter this stopped, and I didn’t dream for a month it seemed, there was so much more resonance in my sleep. But that would all be dismissed.
Which is another thing to bring up thieves oil, because that’s what was used with the big plague hundreds of years ago, and still works as good as any chemical agent, but then no one can have a copyright on it, and it’s biodegradable, and it doesn’t provoke the super germs like anti-biotics and the rest….
I don’t know what the FDA would say about thieves oil, like what they made up about artemisia recently, not the FDA but some supposed scientific authority said that, although it’s been an effective cure for malaria for hundreds of years, and helps people that modern pharmaceuticals couldn’t, that using it could cause malaria to mutate, this when it’s been used for hundreds of years, still is fine, and there’s ample proof chemical agents provoke such problems and natural ones don’t. They’ve proven now that Artemesia extract helps with Covid, although the herb unextracted doesn’t seem to do that much, but no one hears about this.
https://www.dw.com/en/germany-scientists-test-artemisia-plant-against-coronavirus/a-53944514
In fact I think that helps with all viral infections….
Sugar, alcohol, medical treatments, heart disease from a bad diet, diabetes from a bad diet etc. all of that still kills more people than covid daily; so why isn’t that rationally dealt with if they care so much about our health, and would changing all of that (getting people off of sugar and bad processed foods, giving them good natural healing help rather than pharmaceuticals), how much would this help, or would it help more than what they are doing, because it would strengthen the immune system. And that doesn’t push one symptom away to create a whole array of new ones all targeted for new drugs that only get rid of one or a few symptom creating new ones (and addiction). And that’s not even mentioning slowing down the pace of life, getting rid of stress: “In addition, medical research estimates as much as 90 percent of illness and disease is stress-related” from https://nasdonline.org/1445/d001245/stress-management-for-the-health-of-it.html#:~:text=In addition, medical research estimates,been linked to stress factors.
or spiritual healing that always has been there and isn’t going away either, as little as our spirit or our soul is……
I didn’t even know that about hand sanitizer which is all over the place, I really just thought that it smelled offensive and made the hairs in my nostrils stand on end, like so many other harsh chemicals.
Report comment
.
Report comment
What causes “depression”? They don’t know and they don’t care.
Or maybe they DO know, generally speaking, but still don’t care, or at least their career interests are preeminent. “Depression” is often sadness on steroids, however the causes are systemic, not rooted in the individual..
Report comment
I appreciate the comments but have to ask readers, so what are you going to do about it.
The article in my view really doesn’t communicate the seriousness of this.
I suggest people read the actual whistleblowing disclosures that are linked to in the article. One at the front under “members of Congress” and one near the end under “Congressman Jamie Raskin”.
The disclosures noted that I reported this as murder to the FBI and elsewhere including in the latest disclosures. (Under Federal law murder is the unlawful killing of someone with malice aforethought and any murder by poisoning is murder in the first degree. Federal jury instructions include depraved indifference to the consequences as fulfilling the criteria for malice aforethought and as the most highly trained clinical pharmacologist at the FDA with the FDA having the largest concentration of clinical pharmacologists in the world it is my professional opinion that causing people to take a drug (where FDA officials admit it doesn’t work and where it’s also documented that they know it will kill people) is poisoning. In addition the FBI uniform crime reports includes poisoning by prescription medications as a method of murder that they track. Plus mass murder is defined as four or more murders as a result of a single act without a cooling off period which signing documents used for approval seems to me to be a single act.
I literally put my life on the line knowing full well what the likely outcomes might be in order to protect people who might take these drugs. Yet if people don’t do something to protect their own lives like start calling Raskin, Grassley, and their own representatives including President Trump and insist they do something. As well as call other news outlets such as the Washington Post, Foxnews etc. and ask why they aren’t reporting on it. Then this article is a failure and you shouldn’t expect anything different in the face of the pharmaceutical industry paying politicians $300 million per year since 1998. For that’s what your lives are worth, less than a dollar a piece. Not to mention all the advertising dollars, payments to physicians etc.
Report comment
P.S. By going public I have put myself and my family at risk.
Don’t show me that it was a foolish decision that will come to naught. Do something. For as Edmund Burke said:
“When bad men combine, the good must associate, else they will fall one by one, an unpitied sacrifice in a contemptible struggle.
Report comment
Thank you Ron from the bottom of my heart.
It was not a foolish decision. In the least the public gets that much needed education, through yours and Robert’s efforts. I pass on the articles to someone else, and I try to make sure they are the younger generation.
I believe there are many that would love to be truthful, but there are few brave enough to risk it.
There is and will be positive results that come from your risking everything.
I absolutely agree with that quote.
Report comment
Ron, I just read through much of the link for Congressman Jamie Raskin and to describe what you endured as ‘staggering’ would be an understatement. I live in Canada but did forward a link to this Mad in America report onto Donald Trump, Washington Post and Fox News via Twitter. I hope all US citizens who read this MIA report contact their government representatives and US news outlets and insist they report on this and do something about this corruption.
I am very sorry for what you and your family have endured in trying to protect others. God bless you.
Report comment
My personal observations of this type of corruption have resulted in the following.
Police don’t have a copy of the Criminal Code.
Police don’t take documented proof of the crimes, and then respond with a letter stating that there is “insufficient evidence”.
Police make threats to oneself and ones family, though these ‘coercive methods’ are simply called “a poor choice of words” should they be recorded making threats to have you pack raped in the police lock up. And it is a known fact that they are allowed to lie to people in order to get them to comply with their ‘instructions’ (shut up while were busy committing offences)
Lawyers and medical people can breach their codes of conduct and be actively used as ‘informants’ (see the case of Nicola Gobbo who was a lawyer, and a paid police informant. Conduct it is claimed could not happen again. Reason being the High Court made it lawful) Breaches of Privacy Act etc are never prosecuted on the grounds that the “extraordinary’ exclusions applied. For example, drop the target with a ‘spiking’ and they can no longer give consent to the release, and we can “imply” consent. Certainly one argument used in my instance to muddy the waters some more.
Ministerial authorisation means no accountability due to the Ombudsman not being allowed to investigate misconduct by a Member of Parliament. Kept that one quiet till the last minute.
A simple question of law is referred by our Attorney General to the Minister for Mental Health for “actioning”.
Complaining is proof that the target is suffering from a mental illness, and thus the questions of law remain unanswered.
Unlike yourself Mr Kavanagh I was simply too stupid to bow to the threats and intimidation and became an ‘accidental’ whistleblower. I posed a question to you above. Would you do it again if you had your time over? I now also ask. What can people outside the US do, as we are suffering the ‘flow on’ effects of this blatant corruption?
Report comment
An impassioned and inspiring speaker in Utah describes VERY WELL what is happening in America regarding Big Pharma. FDA corruption extends far beyond unethical vaccine approvals. Check it out at 2:30:00. https://www.youtube.com/watch?v=Wmpz8axYR4E
Report comment
Elan, that was Del Bigtree. He produced at least four documentaries in recent times about the attempted takeover of the US by Big Pharma. This a very real political fact. In some ways, it is only part of the story. But if people realized this, it would be a good start!
Report comment
Yes, I know Del Bigtree. He is a friend and a superb human being. There is so much more going on besides To Mask or Not to Mask, mandatory vaccines, and regulatory agencies that are asleep at the wheel — too busy counting their billions! At the top of the deep state pyramid is Big Pharma!
Report comment
I wouldn’t count on Big Pharma being at the top. Have you received data that made you think that’s where all this is coming from?
Report comment
Have I received data that made me think Big Pharma is at the top of the food chain? Surely you jest! Where have you been the past 6 months?
Report comment
I have been looking into a lot more than just Big Pharma! What makes you think they are on TOP? That is to say, what makes you think there is no person or group higher?
Report comment
l_e_cox says, “I have been looking into a lot more ways than just Big Pharma! What makes you think they are on TOP? That is to say, what makes you think there is no person or group higher?”
I recently heard on a news channel that the Big Banks are what’s behind Big Industry.
Report comment
If one has time to look into all this, a lot more information can be uncovered. I would not, however, rely on “news channels.” Read books or sites based on real research or experience.
Of course banking is essential to business life on Earth. So we can be assured that some bankers are involved in the effort to control our planet.
But I have also looked into spiritual control of the planet, and that takes us off world. There is a lot going on out there that we are not much aware of. It affects mental health and many other aspects of life. I use Courtney Brown as a researcher I trust, beyond the more basic research I have studied.
Report comment
Elan says:
“Yes, I know Del Bigtree. He is a friend and a superb human being.”
It is pertinent to this discussion for MIA readers to know if you work for Del Bigtree or any organization he is involved in? And are you in any way receiving compensation for promoting him and his ideas?
Richard
Report comment
Are you a spokesperson for all MIA readers? hm…
I’ve studied the history of the Rockefellers and ‘modern medicine’ for 10+ years, since my grand-daughter was born. You can’t get far along that journey without learning about Del and his work. I share what I’ve gathered along the way because it’s the humane thing to do. No compensation.
Conspiracy theories aren’t theories when they are true.
Report comment
Elan
Thanks for answering the question.
You said: “Conspiracy theories aren’t theories when they are true.”
Yes, you are correct that there are, indeed, some real conspiracies in the world, or at the very least, major forms of collusion between very dangerous institutions. This is certainly true when looking at psychiatry and Big Pharma, and also the FDA’s connection to the Medical Model.
BUT, Elan, you posted a link that promotes the theory that ONLY 6000 people have died from Covid 19 in the U.S.
Do you want to stand by that figure as representing true science?
Do you not see the potential harm in promoting that statistic if, indeed, it is wildly inaccurate from the actual number of 185,000 people, or more dying?
How can I take your other comments seriously at MIA, if you won’t retract your promotion of the link that grossly minimizes the medical dangers and harm done by the Covid 19 pandemic?
Richard
Report comment
To l_e_cox,
I agree that there’s a lot going on that we’re not very aware of. But I wish more people knew about or paid attention to psychiatry’s whistleblowers.
Report comment
Conspiracy Theory Alert!
I watched parts of the video posted by “Elan.” This is pure conspiracy theory nonsense that basically promotes the view that Covid 19 is a “hoax.” It is in its disgusting essence, just more pro Trump propaganda that supports an anti-science and politically fascist agenda. These are very dangerous theories that have very real world consequences.
Elan is posting many comments here at MIA that are glorifying the anti-vacine movement leader Del Bigtree. He is neither a doctor or a scientist, but rather a dangerous demagogue who is now making lots of money (on speaking tours) stoking the flames of every possible conspiracy theory related to the Covid 19 pandemic.
Part of Mad in America’s mission is to distinguish real science from pseudo-science, especially as it relates to today’s Medical Model for “mental health.” It requires a serious effort on our part to sort through all the vast amount of scientific questions in society and determine real truth from falsehood. Sometimes this is not an easy process . It is grossly irresponsible for people to advance conspiracy theories with NO substantial science to back up these wild claims.
Richard
Report comment
Could you please calm down about this? We are on an anti-psych website and you want to call someone out for forwarding a conspiracy theory? Let’s state our views without calling names.
Everyone has their own boundaries regarding “science.” Can I favor Intelligent Design and research into past lives, all done by very competent academics, or is that off limits, too? These subjects are highly relevant to questions of human psychology.
Report comment
Psychiatry has effectively divested itself of questions regarding human psychology. And its scientific boundaries are that of a psychological and spiritual prison. It’s made living life a medicalized gulag for too many people.
Report comment
And what we think of as medical care and services has become psychiatry. ALL of healthcare is infiltrated with psychiatry. The only way you will never see a mummifying stupefying drug is if you never yell out in pain or distress and live quietly until the end.
Report comment
Sam says, “ALL of healthcare is infiltrated with psychiatry.”
I agree, but I think it goes further than that. All of society has become infiltrated with psychiatry.
Report comment
I agree with Birdsong. The situation is extremely troubling.
Report comment
I should also note that the video elan linked to was a 3 hour coverage of a political rally about medical freedom versus medical tyranny. Not exactly the place anyone would look for carefully considered scientific research.
But in fact, the world of academia is doing an extremely poor, bordering on treasonous, job of digging up the facts of life so that we could understand it better. That pushes many of us to less reliable sources.
Yet, perhaps not that less reliable. I would not be too swift to judge a “conspiracy theory” just because it sounds outrageous. We still haven’t gotten the original event for which the term was invented right, and that’s been nearly 60 years ago.
Report comment
l_e_cox says, “Most of the ‘educated’ world now laughs at the idea that psychiatry might NOT have the highest level of expertise in the field of ‘mental health’. And so research and state policies continue to bend in their favor.”
I agree with l_e_cox.
l_e_cox further states, “For me, it has come down to the need for an entire reorientation at a grassroots level…It starts with those who already realize something is wrong.”
I couldn’t agree MORE –
Report comment
Removed for moderation.
Report comment
I watched a movie today about mental illness. Very interesting timing, indeed. The lens of my perception widened — to see with the eyes of the patient. Highly recommended! https://www.imdb.com/title/tt8045906/
Report comment
l e cox, Follow the money-trail. Who funds the W.H.O. and medical universities and regulatory agencies and governments? Vaccine manufacturers make $100 BILLION every year JUST ON VACCINES. The 1% that have the same amount of $ as the other 99% don’t even care about the money; it’s all about power. The cabal families that control medicine, are the same families that control water, food/Big Agra, energy/Big Oil, weather-technology/Big Tech. Corruption regarding approval of 1 or 2 anti-depressants sheds light on the current worldwide plandemic. What can we do? Share the truth! https://plandemicseries.com/
Report comment
Yes, so we see that some wealthy individuals and groups seem to control Big Pharma and are also involved in all the other multinational corporations who seem to be the “bad guys” in our current world. And that’s getting pretty high up on the pyramid of power. But I don’t know that it reaches the very top.
Their only real defense at this point is their secrecy. And my hope is that as we find more ways around (or through) that secrecy, they can be dislodged. But we should realize that if we take down the top of that pyramid, we will have to replace it with people who can deal with the same pressures that those people are dealing with in a way that is more honest and humane. Someone has to walk in those shoes.
Report comment
Someone has to replace sociopaths that commit massive crimes against humanity?
Report comment
Yeah, that’s a head-scratcher for me too — sounds suspiciously like saying you can’t oppose psychiatry w/o having something to replace it with. Por qua?
Report comment
I know there are some who see the whole “mental health” message and system as just a cynical or creative new way to oppress people, silence political dissent, etc.
Yet many are quite aware that “mental health” problems can be quite real. That is part of what keeps the current system alive. I have met people with real mental health problems. They don’t need drugs or to be locked up in a padded cell. But they do need skilled help, love and respect.
I think we should all be able to help each other in this way. I think we should be trained in how to do it starting at the age of maybe ten or twelve. But the current powers that be don’t want real help to occur and don’t have a clue what real help looks like. In this sense, the dream of “replacing” dishonest people with honest people might be just a dream. But I think it’s worth working on.
Report comment
Surprise, Surprise! CDC INFLATED COVID DEATH COUNT.
https://thetruthaboutcancer.com/cdc-inflates-coronavirus-deaths
Report comment
Once again, this is just more CONSPIRACY THEORY nonsense.
If you check out the website where this appears, and the authors promoting these Covid 19 “hoax” theories, you will find out that they also advocate for medical quackery for treating cancer.
Richard
Report comment
Here is a link that exposes the conspiracy theory being promoted in Elan’s above post:
https://www.msn.com/en-us/health/health-news/what-the-cdc-death-report-really-says-according-to-fauci/ar-BB18BCrl?li=BBnb7Kz
Richard
Report comment
Obviously you haven’t read the stats updates ‘buried on the CDC website.
Report comment
It is inappropriate to accuse anyone of forwarding “conspiracy theory nonsense.” This is a website about psychiatric abuse!
Report comment
You make a much needed point.
I would add this: The existence of bogus conspiracy theories does not prove that there are not conspiracies.
And this: Medical doctors’ beliefs may and may not represent validated science. A statement is not validated by the fact that an MD says it. A fact is not proven by a human; it is proven by valid scientific method. Opinion is not evidence.
Ad hominem or ad hoc? “You’re not a doctor” is IRRELEVANT. You can think. You can think while free of preconceived beliefs and training. That places you above MD “opinion leaders”.
Does prescribing-ability make psychiatry a branch of medicine?
Report comment
“The existence of bogus conspiracy theories does not prove that there are not conspiracies.”
Remove or “edit” the legal narrative, and a conspiracy to pervert the course of justice becomes a ‘paranoid delusion’ requiring a mental health referral by police for “hallucinating”.
You were drugged without your knowledge? That’s possibly the most common paranoid delusion known to mental health services.
You were drugged without your knowledge AND have the documentation proving it? Problem, I can’t take the documents because then I can’t refer you to mental health services for “hallucinating”, and might cause problems for the people who are conspiring to pervert the course of justice, and have put this note on the Police system to not take the documents from you and find “insufficient evidence” should you turn up here…….. ‘Their’ conspiring becomes my conspiracy theory…… though then they had to find out who else was aware that this was a criminal conspiracy, and not my ‘paranoid delusions’.
Problem, the Corruption Watchdog has been watching the whole time. They were the people who trained me in anti corruption techniques…….. see, not all anti’s are bad. Enjoy your “restructuring” Senior Constable.
Report comment
Beyond the preponderance of such name calling as Quacks and Conspiracy Theorists, which takes away from the ability to have a balanced discussion, I don’t agree that one can so quickly call something quackery, whether you agree with their overwhelming criticism of chemotherapy or not, they promote a lot of curing agents that are completely natural and non evasive, and wouldn’t compromise the immune system like chemotherapy does. And there are a number of people that were sent home by mainstream medicine to die because there was no cure – same as psychiatry and its story about chemical imbalances and their drugs being the only cure and what must be promoted, and when it doesn’t work there’s no cure – but there are people that changed their lifestyle and/or tried alternative methods, and recovered their health to become cancer free, despite being told there was no cure. That’s worth hearing about, but those stories and that evidence gets regularly shut down by the FDA, and its cronies. Same as one not hearing the stories of those that recovered from the psychiatric diseases demanding psychiatric drugs, when they did it because they got off of their drugs, or never were on them.
And a lot of what’s shared there that simply nurtures the natural immune system might be good for anyone, especially those who might be targeted, because of stress, for having a psychiatric illness.
Again, there are people that were told by the medical profession that there was no cure and that they would die, but were instead healed by alternative methods, quite the same as people told by psychiatry that if they didn’t take their meds they couldn’t function, there wouldn’t be any cure, and yet found alternative methods and recovered; that also should be freely shared, but isn’t.
And such terms as “nonsense” “conspiracy theories,” “hoax” and “quackery” all within the same two sentences, this does NOT point out to me that a person using such language is duly open to discussion about such points. The whole ARENA of stuff that’s called “conspiracy” theories every time it challenges mainstream academic, religious, political or medical doctrine…, if I would start going on about that I would have to fill books. If one disagrees, then you present a different viewpoint, or forward information, but all terms used above are just as easily used by people pumping up what this blog exposes as being misleading and should be exposed rather than labeled as “hoax,” “quackery,” “conspiracy theories,” or “nonsense.”
Neither do I think, same as with psychiatric treatments, you can simply dismiss that a lot of the “non quackery” cancer cures aren’t pumped up by money, and that more natural cures aren’t dismissed by the FDA, because of guild, wall street, corporate media, and corporate political pressures. Cancer is even bigger money than psychiatry.
Report comment
Thank you, sir.
Report comment
Nijinsky
If you read some of my past blogs and comments, you will know clearly that I am a committed anti-psychiatry and anti-capitalist activist.
I also believe that the FDA is a thoroughly corrupt institution, and the CDC is allowing its mission and science to be negatively influenced and swayed by the Trump political agenda.
I believe I have a very healthy skepticism and critical approach to all of western medicine,especially based on the fact that it takes place within a for profit capitalist system.
In my lifetime, I have had 3 different types of cancer, and during one of those cancers I had 2 rounds of chemo. And believe me, I read every science article and journal available before I decided on my course of treatment.
I, also, take supplements and believe there is a role for certain (well vetted) alternative forms of medicine and treatment.
I stand by my negative descriptors within the above comments. I could never EVER trust any alternative medical advocates like the Bollingers, who wrote the article that allegedly states that way under 10 thousand people died of Covid 19. Is this not another way of calling the Covid 19 pandemic a “hoax?”
And we do know what happened to Steve Jobs (the Apple creator) when he sought alternative medical treatment for (early stage) pancreatic cancer, and then seriously delayed surgery and possible chemo therapy to treat his cancer.
Given the oppressive system we live within at this time in history, we must carefully evaluate ALL the science being promoted in society. Some of the science (and the scientists who create the studies) is very legitimate and carried out with integrity and great purpose, AND it should be believed and followed in the real world.
Of course, other science and scientists cannot be trusted and should not be followed. But we ALL must VERY carefully siphon our way through this morass. And this requires much work and study on our part.
We should all hesitate to jump on any political bandwagon that appears to have, on its surface, an anti-system cover, but when looked at more closely is serving some type of reactionary political agenda.
The link referenced above by “Elan,” is not only pure nonsense when it comes to truth seeking, but highly dangerous in the middle of a serous pandemic. People will, and have died because they followed incorrect science related to the Covid 19 pandemic.
Respectfully, Richard
Report comment
Removed for moderation.
Report comment
I’d appreciate it if I didn’t have to deal with straw man responses, I am already busy enough. I never anywhere said you weren’t a committed proponent of anti-psychiatry or anti-capitalism at all, which you imply I was making out to be otherwise or unaware of; that also really isn’t pertinent to the discussion, nor does it indicate that psychiatry or capitalism don’t have elements that are helpful beyond such labels; what I posted was simple responses regarding how the cancer Industry could be controlled by guilds and pro-profit, and suppress alternative methods; I also never said that chemotherapy wasn’t an appropriate response that would help people who it would help; what I said is what I said, which I shouldn’t have to repeat, and that’s that the information for alternative methods also deserves representation so that people can make their own decisions. That people have gone for alternative treatment and it didn’t work for them I’m sure has happened enough as that people who went for chemotherapy also weren’t helped enough, nor did I say that those promoting alternative methods might dismiss chemotherapy when it could be helpful. THAT should be a person’s own decision which they can make when both sides are represented without discrimination.
Ameliorating what you invest in as being serious science that’s legitimate and then dismissing other information as pure nonsense and dangerous and that many people have died following such input doesn’t address anything deeper than more adjectives and what happens on both sides when people’ aren’t given enough information to make their own decisions, given instead “adjectives” and other means of persuasion no matter what side it comes from. I think a person, every person, would have the ability to follow their own instincts, their own intelligence, and their own insights and hopefully find what would work for them otherwise.
I’m quite capable myself of looking through material and deciding what of it I find helpful, and what I find true, I don’t need anyone patronizing me telling me that everything reported in said site is utter nonsense or any of the rest of your dissuasion to even consider there might be truth there that would be helpful, or even something to consider on my own, rather than having been told how to see it beforehand, even if it’s only part of what’s said on the site that I might find helpful, rather than the majority. Or the other way around that most of it is helpful and the truth to make it something to invest in.
And I really am starting to find it overloading to have to deal having to navigate through responding to insinuations that I’m not aware of what’s serious science, not aware of what kills many people, not aware of what can be trusted and what can’t; simply would I look into something someone else has clearly dismissed. Or that I’m not carefully siphoning through information would I not take part in such dismissal. Or that I’m jumping on a bandwagon that has a political cover, but is serving a reactionary political agenda.
NONE OF THAT deals at all with the material at hand, only ways to label it. I thought that goes on enough regarding how people are supposed to see things here in a blog that tries to give people an alternative viewpoint on “mental health” or how to see their own responses to life.
That you believe you have a healthy skepticism of Western medicine and take certain supplements, doesn’t validate your dismissive remarks regarding a site I’m not even supposed to entertain as having any truth to it at all. And I’m really tiring of even having to find words to respond to any of this.
I believe both sides of the argument are misleading when they start simply dismissing the other side in such a fashion. Same as any person or any situation you might come across that you are supposed to see as a source of evil or the like. It wouldn’t have come your way if there wasn’t something to see there, I think what you are meant to see will repeat itself then, without any loss of potential as if it will go away. That’s how truth works not having such limitations, and it’s wanting to see it that allows it to emerge, not making out that there’s something against it you have to dismiss.
Report comment
Sorry, in the above comment, where it reads “nor did I say that those promoting alternative methods might dismiss chemotherapy when it could be helpful” it should have read: “nor did I say that those promoting alternative methods don’t dismiss chemotherapy when it could be helpful,” It gets really to be something strident when both sides dismiss each other, leaving anyone trying to make a decision coerced into thinking there’s only one way, and the other wouldn’t work and should be prevented from being considered.
And Richard I’m glad you survived cancer however you managed it, that’s great, but I think you have to give people the freedom to follow their own instincts about what treatment to follow. Everybody is different, and everybody responds different to various types of healing.
Report comment
And sorry Richard, but the Bollingers could be “wrong” about how much the numbers are inflated. I looked myself and compared the numbers for my state with last years, and there are 4525 more deaths than last year, although the Covid deaths are listed as 5264; but there might be still a slight inflation because of the hype, although it doesn’t appear as if it’s to the extent the Bollingers claim. But sorry, the Bollingers I don’t see as not having logical reasons to be paranoid and mistrust the FDA or the CDC; given how alternative cures are suppressed, and what they have experienced as healing may not be given a voice, in comparison to what runs the economy. Someone who is “psychotic” may be paranoid that someone is after them, and be easily impressionable by anything (a chase scene in a movie, the news, church talk about demons etc.) but when you listen to them, and how they really feel, and what is going on with them, the feelings that never were given legroom, you understand why they fall back on that, and you learn that listening to them helps, as it would with anyone; and calling them psychotic, delusional, paranoid and all of the rest does as little as the adjectives you use of “hoax” “conspiracy theories,” “nonsense,” and fortunately I don’t remember the other one….
And simply beyond that, the deaths caused by such things as sugar, alcohol, processed foods, toxicity in the environment, toxicity in foods even when not processed foods, and the amount of stress people have to live in, and how fear is used as mind control; all of that kills more people, and has been killing more people every month than the Pandemic, and none of that is really dealt with in any way in comparison to the illnesses that are caused by what has been and still is killing people more than the pandemic. Stores are still full of food marketed to make people addicted, a sort of drug to avoid any feelings that are less stimulant oriented, stuff that pushes away more subtle arrays of thinking that simply need space as thought rather than stimulant or anything that physical, simple feelings, thought, space, nothing… and I wonder beyond anything Fauci is doing, would due attention really be paid to all of what I just brought up, how much that would help people simply because it strengthens the natural immune system; and even with social distancing and masks, would due attention be given to everything that has been killing people more and that compromises the immune system so that it can’t deal with illness, how much that would have saved more lives on top of the other measures still kept in place. Simply were it stressed rather than the other measures, WITH the other measures still kept in place. And yet the Bollingers do address those things.
And sorry, but I don’t look at stuff, to get fixated on one statement, and then give the whole site a label. I would be quite gullible and impressionable towards all sorts of stuff would I operate in such a fashion. Something it appears most ads advertising a commodity, whether it’s ideological or material, are designed to accomplish.
And what is highly inflated beyond conception, is how much measures taken against the covid pandemic are made out to lead to creating a healthy environment, when a whole host of other issues causing more disease, and having caused more disease the whole time, not only kill more people, but compromise the immune system enough that it also allows covid to cause more deaths. And those issues are not even brought out in a reasonable manner, when we are told the issue is preventing deaths.
Report comment
Nijinsky
My response to you was NOT any kind of criticism of your positions here at MIA. In fact, I took the time to respond to you because of my past respect for your contributions here at MIA going way back to when you were a major participant in a high level of discussion under a blog I authored on Cognitive Behavioral Therapy.
My response was focused on trying DEFEND my use of certain negative descriptors of what I view to be certain dangerous distortions of science and related political trends that seem to be spreading on the internet.
I only chose to state my overall positions on psychiatry and capitalism to provide more info and context (if you were somehow not previously aware of them) as to where I’m coming from, and the prism from which I view things in the world.
I agree that we can learn things from many alternative perspectives on health care, even those we may choose to ultimately reject for ourselves. And yes, I often learn the most when I read quite polarized perspectives on various topics. And yes, I may choose to retain a single nugget or two from a theoretical perspective that I overall strongly disagree with, and believe to be scientifically wrong.
However, there does come a time when actual scientific theories will be put to the test in the real world, and dire (life and death) circumstance, such as a dangerous pandemic, demands a specific course of action be taken to save lives.
It is during these times that we must do our best to make the most decisive decisions based on the best science available, and take actions that will benefit all of humanity on our entire planet.
In an attempt to go back to some of the key aspects for why I chose to use some strong negative descriptors for some of “Elan’s” comments and links that he promoted, I would like to focus on a few key questions. And Nijinsky, these questions are not directed only to you, but to all others in this discussion,
When is it appropriate (if ever) to draw a conclusion that a so-called scientific theory is “nonsense” and “dangerous” and/or a “conspiracy theory?”
Is it fair to be highly alarmed and use negative descriptors towards authors and theories that promote, as fact, that only 6000 people have died in the U.S. from Covid 19?
Is it fair to be highly alarmed and use negative type descriptors towards those who would make key (possibly life and death) political and medical decisions about mask wearing, social gatherings, and the means by which we achieve “herd immunity” in society, BASED on the theory that only 6000 people have died from Covid 19 , and that the dangerous prognostications related to Covid 19 might be,in fact, a “hoax?”
Richard
Report comment
Richard and Nijinsky,
I really see two very separate issues being argued here. One is that people can promote misleading information on the internet. It appears that both of you agree that is true and there is no real argument about it. The COVID discussion seemed more about what to DO if such information is put out by people who believe it is true. It seems the real point of disagreement is whether or not it is helpful to use pejorative language like “nonsense” and “dangerous” and “conspiracy theory.”
Clearly, people can disagree about the wisdom of using particular language. I guess the question I would ask is how it helps the discussion to use this kind of language? Does it discourage people from considering such information? Does it drive the proponents deeper into defending their positions? Does it create a meaningful discussion or does it undermine opportunities to truly examine the data that is presented?
I tend to agree with Nijinsky on this point. There really ARE conspiracies operating, and the term “conspiracy theory” has been used broadly to discredit any questioning of the status quo, no matter how rational or well supported. Antipsychiatry activists have been accused of being “conspiracy theorists” or “anti-science,” and it is a very effective way of silencing dissent. If we don’t want that kind of language used against us, I think we need to be more creative in our language rather than relying on general put-downs and characterizations that don’t involve any kind of analysis. I liked learning, for instance, the very low number of deaths claimed by the website in question. This was MUCH more influential in my assessment of this person’s claims than saying he is “promoting conspiracy theories” or “spouting nonsense.” To me, the more we stick to citing and responding to actual facts or claims, the more effective we can be in undermining inaccurate sources and theories. Calling names makes the name-caller less credible in my book, plus it legitimizes the kind of fact-free attacks that are often leveled at those who oppose psychiatry’s hegemony.
Report comment
How much is labeling things to discourage further delving into what’s stated any different from disabling the brain with chemical agents from being able to? All because one behavior or statement has been analyzed as dangerous, wrong, psychotic or delusional.
I lose track of how many times I’m reading through a blog or watching a video on youtube that has truly insightful information beyond the scope of what one is supposed to believe is credible, and then one hears something akin to the moon landing being staged, and a government hoax. And even if that IS conspiracy theory, that doesn’t make the rest of what’s shared the case.
It’s like people who have been diagnosed with a mental illness. Someone that’s called “schizophrenic,” is going to have gone through stuff that perhaps pushed them over the deep end, stuff they weren’t able to process, stuff they couldn’t get support just being listened to in regards, and stuff that’s beyond the perspective of what most people can even see going on; thus the person having gone through it is going to end up in the ghetto and beyond that the graveyard where such stuff is entertained, and having reached the incredible there is going to be stuff that’s concocted and not accurate, although perhaps symbolic. Stuff that gets in there just because it’s also beyond “sensible” boundaries where sensible boundaries have already been severely broken. But you don’t sort that stuff out dismissing anything that is seen as not sensible, when what the person already has experienced isn’t acknowledged and expression of that also is seen as not sensible.
Another such example is where there’s talk of close knit alliances that are secretive, and then you hear about a Hapsburg Dynasty cult where there’s cloning going on along with a whole array of leaders that can be entangled into that and other fantastic connections just because of their position. That doesn’t mean everything else that’s brought up regarding elitist alliances is false.
It’s quite common for a “schizophrenic” to think that there’s someone after them, or that there’s some sort of bugging, some sort of surveillance going on; that doesn’t mean that that’s all hoax, conspiracy theory or only psychotic paranoia. Someone having reached such a point as being called “schizophrenic” is already quite surveyed such that anything he does that’s not understood by those around him can be misunderstood, much like CIA surveillance in ways.
Using such catch phrases as “nonsense” “conspiracy theory” “hoax,” and the others such as “paranoid delusions,” etc. is very much akin to turning off the brain with neuroleptics disabling it from looking into the situation further. And when it has stopped doing that seeing it as a return of “sanity.” A psychotic delusion isn’t just paranoid nonsense, it could be expressing something that’s hidden; and when there’s one – even very loud outspoken – error of presumption or fabrication in what’s shared, that doesn’t make everything else fill-in-the-blank-with-label-and-dismiss. In fact, there’s quite a bit of information one might need to have that’s going to be included with other stuff that’s not quite processed yet or presumed, or fabricated; the same as what’s contained in “psychosis,” could be symbolizing something that needs to be understood, not dismissed.
Report comment
Nijinsky and Steve
You raise some interesting points here, and I am taking them into consideration as to how best to approach this controversial topic in the future.
To first clarify the use of certain terms: First as to the definition of “conspiracy theory.”
Wikipedia (which I believe has some merit here) states the following:
“A conspiracy theory is an explanation for an event or situation that invokes a conspiracy by sinister and powerful groups, often political in motivation,[2][3] when other explanations are more probable.[4] The term has a pejorative connotation, implying that the appeal to a conspiracy is based on prejudice or insufficient evidence.[5]
“Conspiracy theories resist falsification and are reinforced by circular reasoning: both evidence against the conspiracy and an absence of evidence for it are re-interpreted as evidence of its truth,[5][6] whereby the conspiracy becomes a matter of faith rather than something that can be proved or disproved.[7”
This definition makes me conclude that there are, indeed, real “conspiracies” in the world, BUT “conspiracy THEORIES” have taken on a whole different meaning in society. They are theories that are based mainly on *faith* and cannot be proved or disproved (for some people) because of a process of “circular reasoning” that many people employ for different reasons.
Many writers about “conspiracy theories” argue that the more they are “mocked” and “ridiculed” the more those people who are operating mainly on “faith” (not facts) will double down in their belief of these particular theories.
Now in general I do believe there is a place for sarcasm (at times) and ridicule for certain nonsensical and extremely harmful ideas in society. But I agree that there are better techniques to use in discussions and debates that are more effective. Many writers on this subject say the best technique to refute a “conspiracy theory,” is to show how it specifically (using facts and data) causes harm in the world.
So therefore, I will still correctly use the label “conspiracy theory,” at times, to describe certain “dangerous” theories circulating in society, BUT I will avoid using the term “nonsense” in my descriptors. AND I will attempt to show, in the real world (using science and facts), how these “conspiracy theories” are causing great harm to people.
As to the use of the term “hoax,” I have NOT used that term as critical descriptor. However, I have only pointed out that many conspiracy theorists (and people like Trump) have used that term to discredit the scientists and medical spokespeople who have declared the Covid 19 pandemic as a serious threat to humanity.
And yes, Nijinsky, we DO need to be careful when challenging the beliefs and thought processes of certain people, especially those people who are (or have in the past)) experienced extreme forms of psychological distress. And yes, there are very real (justifiable) reasons why some people may have certain thoughts that seem odd, or not based on consensus reality, and they must be explored with great respect.
So while I will definitely take your caution here into consideration in my future writing, I do want to make a distinction between people with very little power or voice in society, and those (like the Bollingers) who publicly form organizations and internet websites (often promoting “for profit” alternative medical treatments).
These are individuals who have the power and means to influence large numbers of people either for “good” OR very bad results, when it comes to medical treatment, or life and death type advice about the potential dangers of the Covid 19 virus.
Here, when it involves people like the Bollingers, Del Bigtree, Peter Breggin, Trump and all his medical spokes people etc. etc., we must hold them to a much higher standard. Their words AND theories can literally mean life and death for large numbers of people, and it is fair game (and a moral imperative on our part) to analyze and sharply criticize (and occasionally mock) them when the situation demands such action. And I believe this is one of those times.
The Covid 19 pandemic is exactly one of these historical moments where we must take dramatic steps to save lives. As much as I distrust ruling class representatives who are asking, and/or, mandating masks and social distancing, in this situation their sound advice cuts across class lines. This would be true (in a similar way) if the world needed to take action against an incoming asteroid that threatened the earth’s extinction.
Yes, we must make sure they (the ruling classes) don’t use these situations to further consolidate control and power over people, but there are serious existential threats that require universal cooperation on the planet, and I believe this is one of those situations.
Here again, we also must look at who are the most vulnerable victims of Covid 19 pandemic on the planet. It is people of color, and those who form the under classes in society. It is likely that Covid 19 will devastate countries in Africa and other poor Asian and Latin American countries.
And Nijinsky, I DO share your concerns about ALL the other problems facing humanity (diet, trauma and other health concerns etc) and how they intersect with the Covid 19 pandemic.
This is why I have often written here at MIA that the biggest impediment to human progress on the planet is the “for profit” capitalist system. I have even stated that I do not not believe we cannot truly end psychiatry, and all forms of psychiatric abuse, until we move on to a socialist type system in the world.
Steve and Nijinsky, I have learned from this discussion. The bottom line to my current thoughts are as follows:
1) The Covid 19 pandemic is real, and unprecedented efforts must be taken planet wide to save lives.
2) Efforts to combat the pandemic cuts across class lines. People should be wary of those in power in these times, but NOT hesitate to follow medical and political advice (even from people we would normally distrust) when it can truly be proven to save lives.
3) People in power, and organizations that declare the Covid 19 pandemic a “hoax,” or discourage safety measures that could save thousands (and perhaps millions) of lives should be sharply criticized and debunked, using science and facts to show how this will cause great harm and suffering to humanity.
4) While we must avoid turning every discussion here at MIA into a Covid 19 debate, we CANNOT wall off this pandemic threat to humanity from the vital issues we face when it comes to the oppressive Medical Model. These issues do insect on many levels, and we must find the right “balance” for how to appropriately draw the very real links between these issues.
5) i think we all agree that *real* science is under attack in society. MIA’s mission includes upholding and fighting for *real* SCIENCE and SOCIAL JUSTICE in the world. We cannot just fight vigorously over HERE against pseudo-science in the Medical Model, and, at the same time, let PSEUDO-SCIENCE and related conspiracy theories run rampant in other parts of society. If we build a wall separating these two different (but connected) arenas we will hopelessly FAIL at our mission to end all forms of psychiatric abuse.
Respectfully, Richard
Report comment
In case anyone wonders, by this time what the BLEEP this blog is about by now, down there somewhere I stated this:
“I think that the Bollingers would be quite able to see what this blog actually is about, and that’s about whistle blowers, and what happens to them. Natural cures have very much the same story, over and over again.”
Since this has gone way beyond the initial topic of the blog.
Richard, my point remains the same from the beginning, you are polarizing a discussion using the terminology you use. Pointing out what you think is flawed information from a blog which deserves caution in believing or not is something different than categorizing the whole blog, or the people. That also fails to point out what exactly is flawed information, but instead categorizes a whole site. There basically isn’t ANY source just about that doesn’t have errors in it, that’s just how the human mind works which is more in the world of mental constructs and working those out, so there’s going to be mistakes; which is part of human nature in trying out different beliefs.
Using such terminology also is nondescript, which you point out several times referring to “capitalism,” while defending mainstream cancer cures, and making it sound as if more natural cures here shared deserve the label of being seen as “capitalistic” and for profit oriented while natural cures don’t at all have the $$$$ to pay for the type of trials that the FDA demands (which the pharmaceuticals do have the $$$$$) although natural cures have been shown to work and there are other less expensive trials as accurate; beyond that the cures that aren’t pharmaceutical are often simply suppressed. And then you talk about who has a voice and who doesn’t, while natural cures DON’T have a voice in such a field and ARE suppressed. And what is the conspiracy theory then, a label or a belief that because they have such money and clout, that the drug companies and the big guys have the cures and the natural cures are “hoax” “nonsense” etc.?
And the info about the inflated death counts the Bollingers share seems to be quite incorrect (although I’m not going to say that one can simply believe, without question, what the CDC and/or Fauci doles out, but in this case that seems to be accurate from them) but disbelieving the CDC remains what people hold onto when they’ve encountered such suppression by the FDA, but that DOES NOT make them Trump supporters, as little as that Del Bigtree because he also disagrees with mainstream medical belief is in the same ballpark as Trump etc. And you don’t know that about them, and to put them in such a category, also bringing politics into the discussion as if that’s another way to brand them (either way, are they or aren’t they) is again labeling and polarizing and bringing the conversation away from being articulate. It also initiates the architecture of the two main parties needing such polarization as two parts of an arch leaning against each other for two way hegemony.
You’re creating factions and riffs and cleavages, and inciting divisions as if they are necessary; which is what leads to people getting lost thinking they need to chose sides, losing their voice, and without that they can’t find their way to know what their instincts tell them, which is the only way they can be themselves; and then they can’t find the treatment that would help them.
I think that the Bollingers would be quite able to see what this blog actually is about, and that’s about whistle blowers, and what happens to them. Natural cures have very much the same story, over and over again.
They (the Bollingers) state their beliefs very clearly in their “about” link on their site:
“And the truth is that we should all have the freedom to choose!
… freedom to choose the best cancer treatment protocol
… freedom to say “yes” or “no” to chemotherapy
… freedom to “try” a treatment that hasn’t been “approved” by the FDA
… freedom to vaccinate
… freedom NOT to vaccinate”
And I can NOT keep on responding to a debate that has gone way off topic and out of the ballpark, I don’t have a secretary to keep track of it, and I have other things to do with my time than spending trying to keep track of it which has already been overloading me. You’ve tried to equate a widely diverse group of people: ” the Bollingers, Del Bigtree, Peter Breggin, Trump” as under the same roof and to be treated the same way, when they aren’t at all. And except for a few points you use to group them together they are widely divergent, and I think everyone there but Trump would be quite in agreement with the stance here on psychiatric treatment, but I don’t know other than Breggin their beliefs regarding it.
And come to think of it in afterthought, you mention those most vulnerable to Covid, but fail to mention that they were already vulnerable to a host of issues such as inadequate, food, water, having to live in a toxic environment, high stress situations regarding economic standing; whether the Covid death rate is accurate again, HARPING on that, getting a whole planet obsessed with that, and overlooking more serious issues (that have been killing people more, and in all likelyhood looks like it will be allowed to continue) issues all of those people have had to deal with the whole time, again is using Covid media as a coverup to neglect more serious issues. Vaccinating everyone in Africa isn’t going to magically feed people or clean the environment there, nor stop wars for example, which is just ONE area.
Report comment
Nijinsky
You have stated that I am “polarizing a discussion” and “…creating factions and riffs and cleavages and inciting divisions….”
These are some pretty heavy accusations and negative descriptors that you have tagged me with. I have disagreed with some of your positions in this dialogue, but I have never resorted to this kind of language to describe you or your participation here.
Nijinsky, the reality is that there was already some serious “polarizing” conditions in this country and around the world focused on how to deal with the Covid 19 pandemic. The “riffs,”factions” and “cleavages” have existed for some time. I have created none of this.
I am NOT “inciting divisions,” because they already existed. I did not cause these divisions, I am merely CHOOSING SIDES on some very serious life and death decisions facing humanity in the coming months. And yes, choosing sides is sometimes very necessary at certain historical junctures in history. And we DO HAVE ENOUGH information at this point to make those decisions.
Because you have implied that the “jury is out” so to speak on people like Del Bigtree, the Bollingers, and Peter Breggin as it relates to their positions on Covid 19 and support for Trump and his related positions. I did some more research and reading on these people and their positions on key issues. and DEFINITE conclusions can and must be drawn because of the importance of these issues.
When it comes to Trump, Del Bigtree, the Bollingers, and Peter Breggin, they are CLEARLY Trump defenders AND enablers of the worst kind. Their websites and internet influence reach millions of people, and in today’s world their bad science could result in tens of thousands more deaths if people follow their advice. And this says nothing about their defense of a political leader who is promoting a fascist agenda, which is a far greater threat to humanity in the long run, than even their current positions on the pandemic.
Del Bigtree (in the video referenced above) called Trump a “hero.” And Breggin and the Bollinger’s position on Covid 19 (and with other code words they use) are lockstep in line with Trump on several medical and political positions.
The Bollingers who authored the book “The Truth About Cancer”, and who profit from speaking tours and promoting alternative supplements and fringe type treatments, are , indeed, dangerous charlatans. Nijinsky, read this review of their book on cancer which exposes their deceit and manipulation of fact and science. https://www.amazon.com/gp/customer-reviews/RZQWNYKKSLVDH/ref=cm_cr_arp_d_rvw_ttl?ie=UTF8&ASIN=1401952232
Nijinsky, you said:
“…whether the Covid death rate is accurate again, HARPING on that, getting a whole planet obsessed with that, and overlooking more serious issues …all of those people have had to deal with the whole time, again is using Covid media as a coverup to neglect more serious issues. Vaccinating everyone in Africa isn’t going to magically feed people or clean the environment there, nor stop wars for example, which is just ONE area.”
People WILL NOT be able to address, let alone solve, “more serious issues” in their lives, if they don’t FIRST SURVIVE the Covid 19 pandemic. Yes, i am “harping” on critical life and death questions facing humanity, and i make no apologies for that.
There is ENOUGH information and truth out there at this time to make critical decisions about a direction to take on Covid 19 AND Donald Trump. And those decisions will affect humanity for years to come.
These questions can no longer be treated as simply “academic.” There IS ALREADY a very real divide out there, and it IS time to decide. I’ve made my choice – what about you – WHICH SIDE ARE YOU ON?
Richard
Report comment
Hi, Richard,
I appreciate your inclusion of a lot more factual material in this comment. However, I do find using language like “Which side are you on?” does contribute to divisiveness. It reminds me of GW Bush’s “You’re with us or you’re against us” rhetoric back in the Iraq Ward run-up. I do agree that these issues are serious and we need to make our decisions based on facts rather than rhetoric, and that there are political agendas behind much of the supposed “facts” that we have been provided with. But not having reliable fact sources does put us all in the position of having to educate ourselves about how to evaluate what information is true. I’m hoping MIA will run an article or blog on this point, because I think people need help sorting out what is or isn’t true, and many don’t even know they need that help. I believe that acknowledging the point that it is difficult to know whom to believe is very important if we want to help more people make better evaluations of what “information” to believe.
Report comment
So now we ARE discussing COVID? If so I want to know, if we’re discussing “science,” what Ty Bollinger’s views on cancer or Breggin’s views on Donald Trump have to do with anything. There are thousands of natural healers out there, with different sorts of practices, who nonetheless share a basic understanding of holistic principles and the workings of the immune system, and who hold views on all this contrary to those of the corporate Pharma/medical establishment.
Report comment
I have become convinced that, though facts do help build certainties that people rely on, in this case things seem to be boiling down to a question of belief, or relative values. I value freedom over mere bodily life. Others seem to value mere bodily life over freedom. Although this involves a great and noble debate that has echoed down through the centuries, it is unlikely that “science” will ever resolve it. I am discouraged, though, by the way some of the key arguments that got this country (in its current form) off the ground, seem so weak and unpersuasive now.
Report comment
In response to Steve:
What is choosing sides?
Because that brings to mind when Mind Freedom had their freedom strike, a hunger strike and challenged the APA to prove mental illness was biological. Some platitude was delivered about how much disability there is and how much suffering that people can’t adapt to statistical based norms, without addressing at all the actual challenge (can you prove it’s a chemical imbalance), other than stating one should look in textbooks which actually state that there’s no proof, although they list medications as treatment…. that in colleges that since the early 80s have been fronts for investment institutions, although not exactly investment institutions in themselves, and so they’re going to go with the economics of what’s selling statistically and what isn’t.
But the term “statistical based norms,” that’s like you’re with us or on the other side, which characterizes exactly what kind of statistics are involved, because that isn’t the statistics showing what brings people together, when others are left out and are supposed to think there’s something wrong with them when they can’t adapt to such “statistics.”
And then there’s “consensual reality deportment,” along with “statistical based norms” used to perceive symptoms of a mental illness.
Both of us admire Richard’s ability to take care that people aren’t shod to go tramping around reporting false data,
But when one runs into people with a diagnosis, one runs into people that actually have reason to get disturbed from what they know (about politics and how it doesn’t work), and you learn everything that goes on in such a complex jumble of how not to do it, and it isn’t allowed to go anywhere, or being that that works it messes up our dreams of a better way which we mesmerize people with; so I can go on and on about it, now being assumed to want to take sides, but it’s disingenuous to dismiss the rest of what’s shared when someone doesn’t go along with the statistical based norms of what’s considered statistics regarding what’s coming from organizations that have been shown to put a spin on whatever is corporate enough to be part of mainstream economy, even when the site or group not part of mainstream hegemony is even further off. Simply because they share something that would otherwise be overlooked, and is needed for a complete picture.
Report comment
Steve
I am very surprised that you, also, would actually say my words (on choosing sides) are contributing to “divisiveness.”
Political activists for important social change have, at certain junctures in history, OFTEN used a version of the phrase “which side are you on.”
There is even a famous song for social change with that as its title.
And I am very offended that you would then somehow put me in the same category as George Bush when I used those words. I hope you walk back that comment. Any comparisons to George Bush are defaming and incendiary in this political context.
When I used the phrase “which side are you on” I was very specifically referring to behavior related to Covid 19 and the presidency of Donald Trump.
We DO have to CHOOSE in less than 60 days, whether or not we want Trump’s fascist agenda to continue in this country for another 4 years.
AND we DO have to CHOOSE NOW whether or not we believe that Covid 19 is a real threat to humanity AND whether to wear a mask, social distance, and at some point (when we deem it to be safe) take a Covid 19 vaccine.
I double down on my above statement; there is no longer room for agnosticism on these questions, especially from those who claim some level of political awareness.
It IS TIME to choose. There IS ENOUGH information and science out there to make such a choice.
WHICH SIDE ARE YOU ON?
Richard
Report comment
Well, if we’re talking about whom we support politically, there are sides. I took your comments to be referring to the larger questions of knowledge/facts regarding COVID and other issues that are in conflict. I was objecting to the idea that there are “sides” when it comes to exploring the truth of a particular assertion. I don’t consider science to have “sides,” except for seeking the truth and using “science” to avoid or distort it. But using “science” to distort truth is not science at all.
I do know the song you refer to. But as I recall, it was in reference to being on the side of those who are exercising power for their own benefits, vs. on the side of those who are attempting to come together to resist them. This seems pretty different from questions regarding what the actual threat from COVID is and how best to deal with it. As I have already stated clearly, politicians from both sides have tried to engage in “information management” or “messaging” to take advantage of this world-shaking issue and benefit themselves. I’m definitely NOT on their side. But I can’t embrace the idea that there is a “side of truth” and a “side of dishonesty” in this particular case. (Well, OK, there MAY be a side of dishonesty!) The sides I see are the side of using a disaster to manipulate people to support or oppose a political agenda, and those who are trying to figure out the best thing to do to ensure the safety of our population while remembering the limitations of our knowledge, and maximizing our ability to remain engaged and productive in our lives. That’s the only side I support fully.
What I don’t support is the idea that there are those who believe and agree with everything you said above and those who don’t think COVID is real and don’t give a crap about anyone else but themselves (or those who are too foolish to avoid the deception of the Forces of Evil). I’ll provide a simple example: should one wear a mask while hiking in the woods, or at least when passing someone else on a hike? If I told you that the science suggests that outdoor mask-wearing outside of a close gathering of people is pretty much pointless, would you consider me part of the “other side?” Well, a recent tracking study in China tracked 7000 cases as to origin. Exactly ONE case out of 7000 was caught outdoors, and that one case involved a person talking to an infected person at close range for more than 15-20 minutes. So I don’t wear a mask outdoors, unless I am in a crowd. This is in violation of the CDC guidelines, which from a scientific point of view appear to be wrong. Does that make me one of those deceived by the forces of evil? Do I have to wear a mask while hiking to be considered on the “right side?”
To reiterate: Politics has sides. Science does not have sides. Things are proven true, proven false, or are uncertain. Very, very few things fit into the first category. Generally, things are scientifically false or are uncertain. Uncertain situations require judgement, and judgement is based on data, not political agendas. Mixing science with politics creates bad science.
I hope that clarifies my point. As to the Bush comment, it was just what came to mind when you said what you said. I’d certainly never compare you to Bush II, with whom I’d guess you have almost nothing in common. But I’m also not going to apologize for what thought came to mind when you said it, nor for sharing it. I hope it gives you pause to consider that you may be creating an impression that you don’t want to create.
Report comment
In reply to Steve, adding on to his comments.
Since this blog is about whistle blowers being suppressed, an attempt to get it back on topic.
I think it’s divisiveness that divides the two political parties that together with their arch of two polarized poles pressing against each other create basically the business party, one big party. Divide and conquer. Both parties that it’s made up of exploited to be causing the divide demanding that people chose between the two. And it’s exactly that which has kept the hegemony and the economy of the psychiatric treatment that this blog and Robert Whitaker’s amazingly articulate exposé tries to point out treats whistle blowers the way it does.
I also find it divisive to lineup everything that appears to be on someone’s political platform, that regarding politics where it could change at any moment, certainly after elections; and then to tag anyone that at any point is in accord with anything in that line regarding certain issues as being a supporter of that side, next comes the label of what’s wrong with the whole “other” side. That’s like saying if you buy ANY groceries at the wrong store, you’re ruining the economy. One place might have better vegetables, and another better of something else, and the third that one thing you need although everything else you don’t find up to par.
If Del Bigtree supported one stance of Trump regarding one particular political issue calling him a hero, doesn’t mean he voted for Trump. He actually works much more with Robert Kennedy Junior, who certainly isn’t in Trump’s party. Are we then to be on Trump’s side because of Del Bigtree working with Kennedy? Are all Democrats supposed to not be in agreement with the Republicans, or Trump or be on the wrong side; or are the Republicans not supposed to agree with the Democrats and not with Trump, or are the Democrats supposed to be in agreement with Trump but not the Republicans; or should they all disagree with themselves and each other to make sure no one is supporting the wrong side; everyone making sure they don’t work with or agree with anyone at all regarding anything on any political platform that could end up supporting the wrong side!? Same with the Bollingers to bring religion into it as well. You’d have to ask them who they actually voted for or support in the next election not just look at one stance they have with one or two issues. And whether they voted for Trump or still support him, which I wouldn’t know but to me looks like they don’t, that has nothing to do with whether their book has helped people, a book that has 88% five star ratings. And they have many success stories helping people with cures. Am I on the wrong side would I want to read the book even if they are Trump supporters when I don’t know if they are and don’t necessarily believe someone else labeling them as such, or am I supposed to e-mail them and anyone else to ask first would I be interested in them or overlook their statement about covid death statistics, although I don’t believe that particular statement but am interested in the extensive research they’ve done on alternative cancer cures?
And yes I’m being floridly sarcastic spinning something into the absurd to make a point. One should simply be able to have interest in good things one sees in another faction regardless of other points of disagreement.
This also was about people promoting holistic health and alternative methods. That remains something radically different than what Trump has been touting, save a few points.To round up in such a manner making a conglomeration of so and so’s political platform stating one is on said side given their stance on those issues I think that’s polarizing and exactly how Trump got the support he did; grouping resentments together inside of what’s for who knows what reason called populism, as if it’s popular to just be reactive. In fact I remember that all of the other candidates on their own did better against the other side than Trump did (as Sanders also was polled to do better than Clinton); but Trump went along with polarity and its numbers.
When you compare a person’s actions to Bush with “you’re for us or against us,” I see that as a clear analogy with content rather than just labels. I find that a clear example of what happens when you dismiss anyone who has political points the same as another seen as the wrong side, and refuse to look at a whole array of other issues; the same anyone not for Bush’s war was seen as against him, regardless of any other issues or any other way. That example has nothing to do with Bush either, it’s an example of behavior not of a person, to dismiss that as incendiary and defaming because Bush is involved, is yet another cleavage. And that’s an example of such behavior rather than excusing it if you are on the “right” side, in this case dismissing those in accord with one specific issue one is against, rather than a military war, thankfully. Beyond that there might also actually be Bush supporters that could use examples of his behavior that were commendable, and that might actually also be so in regards other issues, even ones not involving politics at all.
Naomi Klein coined the phrase disaster politics, exploiting the fact that a disaster destabilizing a region makes vulnerable people more prone to suggestion; the basic method such psychiatrists as Cameron took part in with MK-Ultra, and what Naomi delineates turned into what she calls the Shock Doctrine in taking over whole economies. And how is this paralleled when someone (mentioned above as a whistle blower) tries to point out that said commodity people desperately might think they or others need isn’t really doing what it’s touted to, and might make things worse?
Sadly people are dying of covid, but how much is that used as disaster politics because people are desperate for an answer, and in the process of looking for one are assaulted with various factions touting one method and discarding others rather than anyone being allowed or encouraged to take what’s good from all of them. And people that promote holistic health or natural cures really aren’t the ones with all of the money that have been playing disaster politics the whole time.
Report comment
Steve and Nijinsky
Steve, you have created a “straw man” argument for the view that you are criticizing here. NOWHERE have I EVER indicated that science has “sides.
Science is NOT partial to a any “state” or “class” or any other social category in human society. It is an objective experimental process (free from all bias or partiality) to determine the structure and behavior of of various phenomena in the natural world.
Steve, in your criticism of me somehow being “divisive” by asking people to “choose sides” on certain key issues, you are so far failing to identify a dangerous trend of “agnosticism” running rampant through some of the comments in this blog and other places on MIA and the internet.
I now “triple down” on my above comment:
“We DO have to CHOOSE in less than 60 days, whether or not we want Trump’s fascist agenda to continue in this country for another 4 years.”
“AND we DO have to CHOOSE NOW whether or not we believe that Covid 19 is a real threat to humanity AND whether to wear a mask, social distance, and at some point (when we deem it to be safe) take a Covid 19 vaccine.”
In this above statement (or anywhere else) where have I said science has “sides,” and how is urging people to take a stand on life and death questions in the world, somehow being “divisive.?”
Of course we don’t yet know everything (or every nuance) about the nature of the Covid 19 virus or how best to protect humanity from it. BUT WE NOW KNOW ENOUGH LEGITIMATE SCIENCE TO MAKE SOME KEY DECISIONS ABOUT OUR BEHAVIOR.
Agnosticism (or outright denial) on the questions of whether or not the virus is both REAL and DANGEROUS to humanity, and that MASKS and SOCIAL DISTANCING are necessary as a needed deterrent, can no longer be debated in such a way that it leads to INACTION or DISREGARD on these key questions. Do You agree, Steve?
As to a vaccine, notice I said in my above quote that we need to act on taking a vaccine when “we deem it to be safe.” At some point in the near future we will have enough LEGITIMATE science to determine, when and if, it is safe to take a vaccine for Covid 19. BUT the question of whether or not most past vaccines (polio, small pox etc.), or the value of vaccines in general, SHOULD NOT and CANNOT be disputed using the scientific method.
If a safe and effective vaccine is developed soon, and the organized anti-vaxx forces undermine society’s desire and choice to take it, this will cause more deaths and more human suffering. And their efforts to suppress a vaccine’s use MUST BE VIGOROUSLY OPPOSED!
There is clearly a huge divide (that cuts across class lines) in society based on both ignorance and the related influence of nefarious political agendas on the question of Covid 19 AND the most essential behaviors to effectively combat it.
For anyone here at MIA who claims some level of scientific and political awareness , THERE IS, INDEED, A “SIDE” TO CHOOSE. Tens of thousands (and perhaps even millions) of human lives may depend on our CHOICE on these questions.
And remember, there is another powerful and well financed SIDE out there that is working to undermine all our efforts to effectively combat Covid 19. At this point in this battle over the truth on these critical questions, there is a moral imperative to CHOOSE SIDES. Agnosticism and/or “fence sitting” at this scientific and political juncture in history, will only lead to more human deaths and suffering.
As to the second CHOICE referred to in my above comment: that is, can humanity afford to have four more years of Donald Trump? There is MORE THAN ENOUGH information and knowledge out there as to make a choice on that question.
If we are unable to drive Trump out of office BEFORE the election, then there is a moral imperative to vote him out of office. The threat of outright fascism cannot be understated here. This is unlike any presidential election in my lifetime in terms of what is at stake here.
As an anti-capitalist and pro-socialist activist since my early 20’s, I will be voting in my very first presidential election (that is a long discussion). I condemn both the Republican and Democratic parties as being oppressive representatives of the ruling class. But I WILL vote for Biden as VOTE AGAINST TRUMP in this election.
We can no longer be agnostic or treat our current CHOICES here on Covid 19 or Trump as simply another exercise in “academics.” It is certainly now MORALLY APPROPRIATE to ask people “where do you stand on these two choices?” OR again use the title from the famous union and civil rights song, “WHICH SIDE ARE YOU ON!”
Richard
Report comment
Richard, it is too difficult and time consuming for me to address the various assumptions and implications in your responses. You’ve made your point, people can read it, and I’ve made my point, people can read it. It is time to end this conversation, as it is not only going in circles, but going on extreme tangents at this point. We agree that COVID is real and that it needs to be taken seriously and that there are people with hidden agendas opposing taking it seriously or taking advantage of it for political gains, and that those forces need to be opposed. Let’s focus on what we agree upon and move on.
Report comment
It’s quite disconcerting to see Richard, who claims to be a communist, taking a side in bourgeois “Democrat/Republican” politics, and to be so apparently invested in stoking COVID hysteria.
On the ground it appears that COVID continues to subside in most of the US, and that any “2nd wave” will be comparatively mild. The US experience pretty much correlates with the European experience in terms of “cases” and deaths, despite constant implications that there is some great disparity.
And there continues to be almost zero interest in tracking down and prosecuting those who design these viruses; if we don’t there will be plenty more.
Report comment
Removed for moderation.
Report comment
Oldhead labels my writings as “stoking Covid 19 hysteria,” for urging people to take the pandemic seriously, wear masks, and social distance.
Since when is someone ‘”stoking hysteria” to acknowledge the danger of a disease that has killed over a 190 thousand people since last February, AND for the past month, 1000 people have died EVERY DAY.
This is the equivalent of 3 jumbo jets crashing everyday. “Hysteria, you say???”
Oldhead says:
“it appears that COVID continues to subside in most of the US, and that any “2nd wave” will be comparatively mild. The US experience pretty much correlates with the European experience in terms of “cases” and deaths, despite constant implications that there is some great disparity.”
Gee, this forecast sounds eerily similar to someone who said “it will simply disappear, just like a miracle,” and continues to minimize a disease that he actually knew was far more dangerous than the worst kinds of flu.
I am completely dumbfounded and almost speechless at some of the comments I’ve recently been reading from certain people regarding Covid 19.
I am afraid that some people have been drinking Peter Breggin’s Kool Aid. Is it time to consider that a former asset to the struggle against psychiatric abuse has now become a major liability?
I am saddened by these transformations, but shocked into greater motivation to pick up the pace in future battles.
Richard
Report comment
Posting as moderator:
OK, that’s it! Everybody out of the pool! This thread has deteriorated and has become nothing but a back and forth between people completely fixed in their positions. It is time to end it. Again, I am not “banning posts on COVID” or “censoring,” I am stopping this deteriorating thread of subtle insults, straw-man arguments, defensiveness and disrespectful analogies. EVERYONE has had their say. I will not post any more comments on this theme on this thread.
We can do a lot better than this, folks!
Steve
Report comment
P.S. I do not exempt myself from the criticism contained in the above moderating post.
Report comment
“Everybody out of the pool!”
https://www.youtube.com/watch?v=TPxiXGr9nFM
Report comment
Good points stated well, Nijinsky. I intend this cumulatively, for all your posts in this thread. And while it’s hard to separate COVID from the rest, as they both involve the same advanced corruption, I’ll try very hard.
There are other ways of seeing the chronically sad state of U.S. health and medicine from an anti-capitalist perspective than simply blaming “capitalism” for the spread of a virus, or cancer, or any other physiological condition per se. These are symptoms of varied systemic issues within the bodies of individuals.
We live in a toxic stew created by capitalist industry, even though we are often complicit. Once we’re sufficiently toxified we exhibit “symptoms,” qualify for “Capitalism 201: The Cure” and are subjected to medical poisoning, mutilation and other abuses in pursuit of “treatment” (i.e. “symptom” suppression), designed so that the afflicted might return to the assembly line as soon as possible, literally or figuratively.
All this is capitalism.
Rather than trying to put the genie back in the bottle “anti-capitalists” should be focusing on and decrying how industry and corporate medicine has created a population of unhealthy immune-compromised people highly susceptible to relatively minor viral mutations. And, rather than calling for billions to be continually tossed to willing corporate medical receipients, maybe screaming for further viral manipulation to be discontinued completely.
The general approach of all AMA/allopathic medicine is to suppress or eliminate “symptoms,” which are often part of the body’s innate healing process. And much if not all medical “treatment” adjusts one problem by creating another, and so on. Coincidentally the most organic cures tend to be the cheapest by far, so…Cha-Chng.
Anyway it’s hard to draw the line in an article which is after all devoted to medicine and Pharma. But I’ll stop here. I’m tired anyway.
Report comment
On the topic of Capitalism: I know we have some anti-Capitalists here. But I urge you to inspect how connecting an economic practice with what is essentially the political practice of psychiatry could muddy the waters of any argument against the latter.
Practices like psychiatry have thrived under Monarchy, under Oligarchy, under Fascism, under Communism, under Socialism, and, yes, under Capitalism. And so has crime. Crime plays no political or economic favorites! It exists to steal and destroy, not to create a healthy economy and society.
Decry crime in the “free” nations of Earth. Decry crime in the offices of corporate power, or political power. And you will have my full agreement.
Decry an economic idea that has served us well, if not perfectly, for many centuries, and I become confused by your arguments. This is no longer something that is obvious to me. I wonder why it seems so obvious to you.
Report comment
Psychiatry and capitalism have a symbiotic relationship. This doesn’t mean that psychiatry and other (theoretical) systems of rule couldn’t also have mutual back-scratching arrangements.
Report comment
I like to consider what occurs when the values of a psychiatrist come into direct conflict with the values of the State.
Given a first strike policy who wins if a gay psychiatrist tries to have one of the morality police detained in Iran? Does it depend on where the exchange takes place? A Mexican standoff in an Emergency Dept in a hospital in Tehran lol. Whose ‘lack of insight’ takes precedence?
The needle or the rope?
He does have a point Oldhead. We see the same behavious from Islamic State who make the claim that anyone who doesn’t agree with their interpretation of ‘reality’ lacks insight and requires ‘treatment’ to correct their straying from the path. This lack of insight, called jahiliyyah, is what has allowed Muslims to kill other Muslims despite their being a strict prohibition on such action. They don’t even recognise that they are no longer Muslim and therefore can be killed. (they don’t even recognise they are ill and require treatment against their will argument used way before Jaffe came along. See the work of Sayeed Qutb)
Report comment
You guys, I’m having to laugh at even trying to make sense out of words like capitalism or then socialism, which so often is made out to be the bad guy then..
What goes on here with whistleblowers being persecuted, because they’d interfere with $$$$$$$$ actually points to a system that is basically what capitalist fundamentalists would say is what’s wrong with socialism, that an elite few can control others, and suppress dissenting information, so…..
Quite rampant in corporate politics, such “socialism.”
Or religions that say that the devil is out to torture you and your enemy, but then use him as their “disciplinarian” or “deterrent” would anyone not conform to their ideology and end up in a Hell that would have no function and might dissipate all together did they not need such a “deterrent” for mind control.
Report comment
Nijinsky you are essentially correct — there is no common definition of capitalism OR socialism here so all discussions of such are inherently flawed to at least some degree; I support not using them without defining them.
P.S. Check the new sub-thread I started at the bottom and addressed to you.
Report comment
The two political parties (in the USA) that have created the deadlock (one has maybe 10 percent more change than the other, and we need at least 60 percent) are both actually, as Chomsky states, together the business party, and it’s such behavior that causes the suppression of people like Kavanagh, which this blog is about, because of business interests. Both parties facilitating suppressing whistle blowers regarding the FDA.
I also think that the war between the two parties is pushing more sensitive issues to the side (including what this blog is about), issues that will continue to kill more people, if not addressed, than covid is going to. And I’ve stated those issues clearly, neither does that mean I’m not concerned about covid or negating those deaths, or overlooking data regarding it, or overlooking how to deal with covid, or agreeing with false statements regarding covid. I don’t think one can discard major issues regarding health and what supports the immune system regardless that other issues are handled badly such as whether one wears masks, whether there’s social distancing and the death count. I think people should wear masks, I go along with social distancing and I don’t think the death count is exaggerated to the extent that’s reported, but I also believe that would people take care of themselves, would they have adequate water, would their environment not be as toxic, would they have any kind of decent working conditions and further more would they be able to take care of themselves that then along with the other measures that that might save more lives than just the measures that are stressed. And I am saying that that goes along with the other measures, not instead of it. But that might save in addition more lives, and also would continue to keep saving lives that were lost before covid ever turned up. To go back on topic, such a lack of being able to take care of oneself given economic standing and environment is used as a means to diagnose people with a mental illness, because of the symptoms that emerge from such lack, such disregard, rather than their living conditions are acknowledged.
Richard, I’m not on either side, and I’m not going to contribute to the architecture that’s caused the deadlock. As I mentioned regarding polarization, both political parties in the US lean on each other creating an arch with two beams, both beams pressing against each other creating an arch supporting each other blocking any other party or more alternative views; and although you criticize me for stating you are polarizing, say that’s a heavy accusation and negative descriptors, you then do exactly that asking me what side I’m on, as if do I see any good in the other I’m on the wrong one, or that I have to chose sides. That’s polarizing, plain and simple. I’m not going to add to the pressure on either side holding the whole blockage in place.
Also trying to intimidate that people have to take sides, in whatever conflict, as if that’s the only way or they are required to, also creates the kind of stress that not only causes inability to relate to what’s human on the other side, but causes the immune system to break down with the fight or flight response, which in this case is the fight response.
My responding to your posts is also over now, your last post was radically off topic and I feel I’m being exploited playing catch for or thrown into someone else’s issues that already are highly off topic and distracting.
Report comment
Removed for moderation.
Report comment
Richard, Mr McCrea requested no more COVID posts. Buh-bye!
Report comment
POSTING AS MODERATOR:
I have allowed a lot of off-topic remarks regarding COVID on threads that have nothing to do with COVID. I think it is time to stop this. We are not a site about COVID, and it is a very controversial subject that goes very far afield from rethinking or ending the practice of psychiatry. I am not going to allow any more COVID posts that are not directly relevant to the article at hand. There are plenty of other forums where such discussions are more appropriate to conduct.
Report comment
This decision is causing me COVID anxiety lol.
Report comment
That will probably appear in the next DSM – “COVID anxiety disorder” or “pandemic anxiety disorder.”
Report comment
Is that a dead give away? Pandemic Anxiety Disorder or PAD, where we were all locked down into (our pad).
I mean when they were going to label the invasion of Iraq: “Operation Iraqi Liberation, and then found what the acronym of that spelled out to be a bit of a give away, and they changed it to whatever it was, which I can’t remember….
That’s quite an acronym though: PAD
Report comment
“PAD” – I love it!
Report comment
Like the meeting to create the Fast Action Response Team. Glad they decided against the use of sniffer dogs.
Actually they do have a PAD here. Psychiatric Assistance Dogs. The website has these pictures of cute puppies (a little dachshund with the cutest eyes) but the dogs they are using in the regional areas of the State are Rhodesian Ridgebacks more at home in the hands of Belgian Police in the Congo. I don’t know why but I got that image from Abu Ghraib in my head where they ‘exploit the phobias’ of inmates.
Psychiatric Attack Dogs maybe? Because there is a significant fear of dogs among our indigenous population. All part of the Coercive Assistance Techniques or CATs lol
Report comment
l_e_cox is right. Mental health problems are very real and some people may need skilled help. But those skills should not include psychiatric diagnosing, or forced drugging, or holding people against their will. And working towards ending these injustices in whatever way possible is more than a dream. It’s a moral imperative.
Report comment
There are people with problems. The body is not split at the neck, we are a whole being. Our environments can make us miserable, Perhaps all our lives. This does NOT mean illness. States of feeling and experiences are so complex, that we could not call a mind healthy or unhealthy as in some physical sense. And that is why there are no experts on someone’s mind. That is why they make random drugs that do absolutely nothing except try to disrupt whatever is happening. Disruption is not “making well”.
They will warn about harms of prednisone because as all drugs do, it affects ALL of the body. But psychiatry or the general population actually pretends that psych drugs affect only the brain, AND in some “good way”.
It’s so incredibly stupid of what people have been led to believe and as time goes by, I find I am more and more shocked. So I’m hoping I get to a point of not being shocked.
In general, we are getting more stupid.
Report comment
“But psychiatrists or the general population actually pretend that psych drugs affect only the brain, AND in some “good way.”
Thank you for mentioning this important distinction regarding biological psychiatry. I don’t find this kind of flawed thinking anywhere near as often with other kinds of doctors and the medications they prescribe.
I think psychiatry’s having to rely on a book of “diagnoses” based on committee-voted checklists is the reason most psychiatrists unreasonably defend the substances they prescribe, and doing so makes them insecure.
Report comment
I took Asenapine (Saphris) for a couple of years 2012-2014. It was initiated against my wishes under the psychiatrist’s orders. I had been taking it for several months when I developed severe symptoms of autonomic neuropathy. An attempt to suggest a connection between the two was laughed off as ‘paranoia’.
Several years on, I am now severely disabled due to progression of autonomic instability and neuropathy. It affects my cardiovascular system, my digestive system, and my urinary system.
I am told, by the psychiatrists, that there is no evidence that Asenapine could do this harm and that it’s just ‘bad luck’. I actually have no real idea whether Asenapine is truly to blame. The timing may, I guess, have been coincidental. But this attitude from the psychiatrists that the drugs simply can’t be bad because they are FDA approved is extremely dangerous. It also leaves survivors, like me, feeling discouraged that we were ‘unlucky’ to develop a mental illness and then ‘unlucky’ to develop a serious physical one during ‘treatment’. I should clearly never play the lottery!
As an aside, I also managed to be forced onto Seroxat as a teenager and became one of those who developed serious suicidal ideation as a result. But, again, it was insisted that there couldn’t possibly be a connection.
Report comment
Malaika, they are lying and dead wrong to boot. Even their lies are full of holes.
It is simply their word against yours. It has NOTHING to do with “medicine” and everything to do
with power. They are vile creeps and they OWE you a life.
They have no clue what it’s like to be hurt by power. Their hurt was burried under hatred, it is my only explanation of why they do what they do.
Report comment
“I should clearly never play the lottery!”
I once said to my wife “What would you do if I won Lotto?” to which she replied “I’d take half and leave you for a younger man”. I said to her ” I won 5th division, here’s $15. I’ll be seeing you”, and i’ve been living the Lotto life since lol.
Seriously though Malaika, what kind of dose of Asenapine were you on?
Report comment
Thanks for making me laugh boans. I needed that.
During that time I was given 20mg Asenapine a day, along with 5mg haloperidol, some promethazine, lorazepam, and procyclidine. Possibly sodium valproate, too, although I can’t be certain that that was concomitant.
I’ve been given so many drugs over the years and, in total, spent over 7 years of my life in hospital involuntarily before the age of 28 including time on an ‘experimental unit’ that was later closed down and the ‘doctor’ in charge struck off. I have no doubt whatsoever that psychiatrists destroyed the life I could have had (not just physically, mentally too). But proving any of it seems impossible when faced with an institution that believes they can do no wrong.
Currently my brain hurts trying to figure out how long I took the Asenapine for. My memory has been largely destroyed – it’s full of huge black holes. I did pull my medical records, which I received on two USB sticks, but they’re incomplete, mainly indecipherable and are presented (I believe deliberately) as though someone threw all the notes in the air and stapled them together in whatever order they landed. I remember where and when I was started on it but can’t figure out the end date. I know it had been stopped within four years as I recall 20mg haloperidol at that point with no Asenapine.
Report comment
Ouch Malaika.
I did try a small dose of this drug after I returned to the hospital that tortured and kidnapped me. No way they were going to allow me to stay on the ward without some form of drug taking. It was when the psychiatrist went on leave and another guy who literally didn’t know what day of the week it was (insisting in front of a half dozen staff it was Wednesday on Tuesday, and no one other than me prepared to challenge his ‘error’. I called him “The Proverbial” from that point on) tried to get me to take it at levels that would have taken my legs out from under me that I needed to leave. I had what I needed by that time anyway.
“I did pull my medical records, which I received on two USB sticks, but they’re incomplete, mainly indecipherable and are presented (I believe deliberately) as though someone threw all the notes in the air and stapled them together in whatever order they landed.”
I wrote and thanked the FOI office for the jigsaw puzzle they sent me, which consisted on the redacted sections and left me to figure out where those sections were cut out from the redacted documents they had already sent me. I thought it important to make a note that these people were engaged in an attempt to conceal something (that something being a criminal offence, and that offence carries a mandatory prison sentence). They really upped the stakes at that point and were assuming the ‘lotto’ was fixed in their favor.
Bit of a worry for the FOI officer that she had me with a knowledge of the FOI process banging at the door, and the lawyers at the Mental Health Law Centre making application for documents that would expose serious criminal offences including acts of torture, and she had been conspiring with my wife to pervert the course of justice on the matters. Pure coincidence that I documented the date on which they finally informed me about the spiking in a letter to the FOI office. Otherwise they could have claimed there was no record of it and ….. not another mistake that assists in concealing their criminal conduct? The luck of some people lol.
I have taken this matter of fraudulent documents up with our Minister. mainly because it seems to me that if hospitals are allowed to distribute fraudulent documents to citizens legal representatives, then how can the public be assured that we are protected given our new Euthanasia Act? I understand the need for the redaction of certain information to protect people, but there is an Operational Directive in place which allows legal representatives, upon provision of a confidentiality agreement, to be provided with unredacted documents with the confidential information marked and an explanation of why that information is not to be shared with their client. Imagine, in my instance they would have been marking criminal offences an saying don’t inform your client because we don’t want to go to prison, aka asking lawyers to conspire to pervert the curse of justice IN WRITING. That wasn’t going to work for them so they found a way around it, committing further more serious offences, and thinking they would just have me killed in the E.D. (and of course tamper with the paperwork and trick the Coroner. They are allowed to do that from what I have seen given the now ex Minister for Mental Health says they can “edit” legal narratives to manufacture truths).
End of the day I hope that time heals you enough to allow you to sort out some of their poisonous conduct. These vicious psychological assaults and misconduct being enabled by these people we vote for one of the reasons I see our communities being destroyed. They are being allowed to leave a trail of destruction behind them, and not a lot prepared to hunt them down and deal with them. Shame really coz it can be fun when you see someone who didn’t believe in a God running screaming to that same God they didn’t believe in just a short time before when they think their time is up. One minute he is bearing false witness on statutory declarations before a God he doesn’t believe exists, the next he is running and hiding asking that same God to help him when I ask him about why he concealed the ‘spiking’ from me and allowed police to torture me. Comedy Gold lol. I’m sure they have drugs for his paranoid anxiety.
He made me into a monster in his mind in order to justify his detention of me, ‘verballed’ the forms and took the victim of domestic violence and made me into a psychotic, knife weilding, drug abusing, wife beating paranoid delusional. Then of course when I approach him to try and resolve why he did this, he runs from me terrified of the monster he created lmao. Surely it makes more sense to drug him, rather than have him drug the whole world? Because as far as he is concerned we’re all sick and in need of his ‘treatment’, and he has found that by defrauding the system he can achieve that end with anyone he wishes..
Report comment
Mr McCrea, where does the corruption begin and end exactly??? Completely relevant, IMO. We are ALL being suppressed under medical tyrrants! But I get it. It’s your blog. Nice dicsussion — while it lasted.
Report comment
There are no clear lines – it extends into every aspect of life in our “marketing culture.”
Report comment
I can tell when the shrinks are reading. 🙂
Report comment
The lies psychiatrists are used to in are sort of individual phenomenon. Is not a proper conspiracy (collaboration between wrongdoers), but more like sort of inertia of the system, born out from independent contributions of individuals. These lies survived because nobody exposed them, nor are talking the psychiatrists to each other about them.
This is why such articles affect them: they expose them not only to the public, but to each other.
Report comment
This is a common perception about many professions, that the resistance they see to more truthful narratives is simply a matter of individual personal conflicts or ignorance. But this is not the lesson of history. And beyond that, all the professions have professional organizations, and there are other organizations that connect those organizations. We know that. They don’t even try to hide it any more. You may think if you wish that no cabal exists concerning this or other subjects of great concern in society today. But there can be no doubt that the potential for cabal exists.
To the extent that a potential for collusion exists, and that some investigators have found it when they looked, an offhand brushoff from peers or our “betters” seems not much more than gaslighting. In the case of psychiatry, historical cabal has been proven. This could be seen as reassuring. Perhaps if the grip of corrupt leaders could be loosened or broken, then fewer would be tempted into corruption.
That is, after all, what this article is all about.
Report comment
Every claim in this article is backed by objective reference and the conclusions are as unbiased as they can be.
I have no words to describe my admiration for Mr. Whitaker’s activity and results and for the activity of the other people at MIA.
I would just want to point out that this information and understanding is made accessible only to people at scientist level and for that reason, the process of changing the minds is slow.
Finding a way to address the masses an adapted version of same things may help a lot, demolishing their blind trust in ‘specialists’ that so often are as dishonest as unprofessional they are.
Report comment
Ways have been found. They are underutilized, but more widely used than you might suppose. There is a lot of mass opposition to psychiatry. But at the level of policy making, there is almost blind support for “mental health.” I think the problem lies at this level and above.
Report comment
Hey Boans!
About emotional stuff and emotional service dogs: At a Red Cross disaster shelter I met a nurse who had named her service dog, Faux Pas.
Okay, its not much of a laugh, but right now we need something to ease the tension.
Bananas
Report comment
lol Bananas.
Bit like me, when I said to the hospital “Hey I think you guys might have tortured and kidnapped a citizen and i’d like to make a complaint”, what I really meant was “Thank you for your concern about my welfare and I look forward to being helped by you in the future”.
Terrible faux pas on my part it seems lol
I had a guy try and sell me a talking dog last week. When I said “get out of here, a talking dog” the dog spoke up and said “No. It’s true, I can speak. In fact I’m actually quite a good singer and nearly won an episode of Australian Idol. And next month I will be taking a team of huskies to the South Pole and back in record time, and will be entered into the Guinness Book of Records”.
I looked at the guy and said “Well I never. A talking dog. Why on earth would you want to sell it?” to which he replied “I’m sick of the lies”
A bit like many of us with psychiatry huh? Or is it that i’m sick of the criminals pretending to be medical people to avoid being held to account?
Report comment
Yep! The only thing that psychiatry has in common with medicine is the ability to prescribe drugs. Years ago, at a site for some human problem, a psychiatrist said that his job was to find the right combination of drugs that would give him the result that he wanted. The result that he wanted? Creepy Creepier still is the fact that he was able to imprison and force these drugs.
Report comment
“… give him the result that HE wanted.” There, indeed, is the rub. The psychiatrist wasn’t concerned with the result the client wanted, only the result the psychiatrist wanted. Paternalism/authoritarianism in a nutshell. He knows better than the person he was purporting to help. If they disagree with him, they’re a “resistant client!”
Report comment
Regarding that one is supposed to show the change the psychiatrist, or the result, that he wants, but is the psychiatrist even dealing with the person he’s trying to change at all. And what if the person actually believes this?
I’ve actually walked around for many years (about 25), a fraction of the time (maybe 10 to 15 percent ) being in a state psychiatry could call psychotic, although…
What am I supposed to say about that,
It really ended up being as simple as not realizing that I was reflexively pushing thoughts to the side or feelings I had encountered in my youth that then had already received such a critical response that the feelings themselves coming up made me uncomfortable, restless with the unconscious memory of the response to them, and I’d start doing something like drinking too much coffee, sometimes way too much. An attempt to disassociate. Well, then those feelings end up expressing themselves in a sort of dream state, with symbolism, that’s not just psychosis and non-reality based thoughts. And coffee (cigarettes too) act like psychiatric drugs, or are in ways, as is sugar. How they effect dopamine and with coffee at least also serotonin. And any restless anxious behavior trying to get away from an unconscious memory one isn’t able to comprehend can effect the brain, from the simple anxiety. Although ADHD drugs and antidepressants aren’t necessarily an attempt to disassociate from feelings and thoughts, that could be the case, or it could be that a person is forced to see their response as having something wrong with it, a symptom of a disease rather than their own nature an attempt at unconscious dissent or a response to their environment, that’s then called symptoms if it has anything to do with it, but ADHD medications and antidepressants also mess around with brain chemistry enough that one in 20 or so on those drugs end up with a bipolar diagnosis, right next to schizophrenic or schizo-effective. More drugs.
I knew this the whole time about psychiatric drugs, and how they cause chemical imbalance when they disable one from expressing symptoms, and don’t treat a chemical imbalance but cause one which we are supposed to believe, so I wasn’t going for that; but the amount of ridiculous social behavior from people thinking they “know” you have a disease, and with all of the media hype regarding dangers of unmedicated people, when mostly the danger comes FROM how the medications disable the mind, you get so incredibly targeted by brainwashed people I’m still quite shocked how much that goes on, the same one is shocked at any number of false things people believe, or historically have. And they start talking about you en mass as if you’re some object completely disconnected from your own experience, and when you don’t believe them and/or aren’t following set method anything you do can be misinterpreted, when it’s at all unusual. Anything. Nor are people adverse to lying about you. It’s like I’m supposed to be someone else I never could be, and have tendencies I never could have and convince people that that’s not going to happen, which never could to begin with, in order for them to consider how I actually experience all of this, when I’m experiencing this, not them, although they think they know what’s going on. And that’s not just from psychiatrists who I actually didn’t have to deal with since the psychiatrist I saw gave me the leeway to not take medications and seek alternative routs. And the social behavior I just mentioned is just the instances when they have decided you have a disease, that’s not the hatred the bullying and the mobbing, which anyone being at all different can encounter, whether they have a diagnosis or not.
I imagine this psychiatrist was talking about the result he wanted, much like someone promotes exerting their ego and redecorating their house, which makes me laugh already: How would the psychiatrist respond would you try to point out that he seems to be quite phobic about listening to what his clients really want? and I wonder how one could conflate that with him thinking his house might talk back to him.
“Sir, you seem to be so scared of me having my own ideas it makes me wonder whether you have heard you house express dissent from how you redecorated it, and thus can’t deal with anything your brain might entertain that you think is psychotic.”
One guy that used to live in an apartment underneath me, had been force treated, and had to see a “therapist” but didn’t want to. He told me it ruined his whole day, and he just hadn’t gone to see her, then she called him up and asked him if he needed a ride, where upon he either said no or hung up the phone. The next day the police showed up to escort him to the asylum because the “therapy” he said ruined his whole day was not something he wanted to go to, and in the asylum the psychiatrist asked him whether he thought anyone was after him….
I was visiting someone at an asylum, she basically had needed someone to talk to as a child, had gotten for some reason hyperactive, and her parents had been told to put her on a drug that caused her to gain weight to such an extent that her father chased her around with a belt chastising her for that, she also couldn’t stay awake to pay attention because of the drugs, where she was further disciplined at school, and her parents told to take part in that. And as it seems endless to go on about such stuff I’ll try to continue, but there’s so many off shoots I don’ t know where it will end up. She had a relationship with a guy, and they were talking about getting married, which the father heard about from the guy but wasn’t supposed to, who you can pretty much guess wasn’t capable of much discussion with such matters, and the girl freaked out and put herself in the asylum and was voluntarily getting shock therapy. I understand that after that she was in a state asylum for a year, but a few (maybe 5 or 6) years ago I ran into her, and I asked her if she had someone to talk to, and she mentioned she lived with her mother and she could talk to her. Seems like a rather bumpy road just to find that (someone to talk to). Anyhow, back in the asylum I went to visit her in, there was a guy standing there that I had seen around, and he was standing at the central desk behind which the attendants and a secretary or so dwelt (computers and other recording devices such as pens at hand, and a phone probably also at their disposal); he looked so much like someone had propped him up there, with his jaw sagging as if he had just watched the most inexplicable thing happen, and so I asked him: “what are you doing here?” and he replied: “I don’t know.” So I simply stated: “Just follow the rules and do what you’re told, and you’ll get out.” When I got to the visiting area, the girl I was visiting and another patient started bounding back and forth like a tennis match with information as to why the guy was there. He had gone to the local “Catholic” hospital in the middle of the city, and had announced that he was pregnant. Now, I have to add that years before this, on a whim to do something crazy, I had called that same hospital and ask a joke inquired whether they had pregnancy tests for males. The lady that answered in a quite mundane voice stated that they didn’t have such tests. In fact she responded so blandly that I later for years wondered if it would have made any difference had responded by asking her to not put her makeup on while I’m asking her a serious question, and repeat the inquiry. I don’t know whether she actually was putting makeup on, it just gave that impression. But of course when this guy walked in there, not only did they not tell him that they didn’t have the ability to determine if he was pregnant, or what that might mean to him, they escorted him to the asylum, where he had been for maybe a month, and was so drugged up he looked like a zombie. The girl I was visiting and the other patients mentioned that the psychiatrists couldn’t figure out whether he thought he was pregnant, or whether he thought he was female. Serious diagnosis! Etc.. And why I’m going on about this is that the other patient had also mentioned how a psychiatrist had asked him whether he had homicidal thoughts: “Would you be here if I had homicidal thoughts,” he said he had responded. And then had of course been asked whether he had suicidal thoughts, and responded in the same vein with: “Would I be here if I had suicidal thoughts,” which he said seemed to make the psychiatrist mad enough that he was happy about that.
Do you have homicidal thoughts?
Do you have suicidal thoughts?
Do you think anyone is after you?
“No sir, when you force me on treatment, ruin my day by forcing me to talk to someone I can’t stand, I know that’s for my own good…”
The guy that had some sort of pregnancy did get out, and when I ran into him in the park I later found myself feeding a whole group of sea gulls. Throwing pieces of bread up in the air which they caught.
I for awhile did this more regularly, fed seagulls. In fact, I had found a whole loaf of discarded bread, which seemed to be in the works for the seagulls. It was just lying there askance half on the sidewalk half on the grass along the path I was riding on my bike after visiting my parents. I could have just left it there, but remembered the seagulls. I had taken it home squeezed and twiddled the soft bread into little balls, where it ended up in the freezer for awhile, till I put it in my back pack and took it with me having it long enough that the balls had melted. I ended up at a store with a big parking lot where the bus stops, and there always are a score of seagulls around there. I started throwing the bread up for them to catch, and I’ve never seen anything like it. The whole colony of seagulls was in the air, together, in complete harmony, and one by one, they took turns catching a piece of bread I threw up, never fighting about it, and letting the next one take his turn. It was the most amazing magnificent thing, and also as mundane to me as being able to breath air whose molecules have the same harmony. I think that the state I was in then could have easily been called psychotic by many people, in fact had I been “sane” I might have tried to make too much out of it, and it wouldn’t have happened.
That’s called murmurating perhaps, if you’ve seen a whole flock of birds moving through the sky as one, https://theconversation.com/starling-murmurations-the-science-behind-one-of-natures-greatest-displays-110951 An incredible phenomenon of nature. Not something you can accomplish when the goal is the “result” you want, I think you have to be more in tune with harmony than that.
Report comment
Uh, there is one more little thing folks — studies of psychiatric labels such as “schizophrenia” are all tainted and bogus from the start, since they falsely assume that there is a disease of “schizophrenia” which has “symptoms” that respond to “medications.”
If people truly understood this basic misconception Bob W and lots of other people could save a lot of time reinventing the wheel when it comes to discrediting the psychiatric drug industry.
Report comment
NIJINSKI if you’re still around — damn, you have history! I’m starting a new sub-thread or whatever since the last one is unwieldy and the subject matter deemed inappropriate.
I was no longer active during that hunger strike era, but would have opposed it as a tactic if I had been, as it was based on a convoluted gandhi-esque approach rooted in the idea that we need to suffer to achieve our goals. But fuck that, we suffer enough — let THEM suffer if anything! — in the form of lost profits, lost status and in some cases prosecution. I still believe that for survivors hunger strikes are masochistic and disempowering, and romanticize self-destructive behavior as they risk physical harm. And to what end — getting shrinks to unequivocally admit they’re full of shit? First it ain’t gonna happen and two why do we care? What’s important is taking their power away.
Report comment
Going back to the essence of the article, I have to admit to feeling pretty useless.
Here is someone who has risked everything to speak out in solidarity with those who have suffered as a result of drug approvals that should never have happened. He has sacrificed so much to stand up for people like me and yet I feel I can do very little in return. I can (and will) write a couple of letters, but it feels insignificant.
The drug companies, the FDA, the attitudes of so many mental health workers…these are just overwhelmingly huge. Change is desperately needed but where does an individual even begin? I’m in awe of Kavanagh’s courage and determination and I really wish I could also stand up to be counted in some way. Yet I fear I fall too easily into the box marked ‘victim’ and, with that, any power I may have simply vanishes.
I feel increasingly inadequate when faced by the enormity of the battle. Surely I’m not the only one?
Report comment
Oh, believe me, you’re not the only one! I’m still waiting for that moment of crystallization when suddenly it becomes clear to enough people that something shady is going on. In the meanwhile, I keep trying to educate and support, educate and support. But it doesn’t feel very hopeful.
Still, I never thought the Berlin Wall would come down, and it did. So the world can surprise us sometimes. I’m hoping it will be sooner rather than later! What will it take for the masses to rise up and say “NO!”
Report comment
First they need to figure out what they are saying “no” to.
Report comment
It’s getting worse
On a quick look through the public documents from a MH health Trust in the UK
“two patients have absconded over the fence and subsequently died on the M5 motorway”
“Violence and aggression remain the highest reported category”
“The Committee received a report on the Do Not Attempt Resuscitation (DNAR) procedure for people receiving Learning Disability services”
“Serious Incidents (SI)
Unexpected deaths continue to account for the majority of SIs reported across the organisation.”
Report comment
Kate Shemirani Natural Nurse in a Toxic World links up WWII eugenics psychiatry with what is going on now – Do Not Attempt Resuscitation (DNAR) :
https://www.youtube.com/watch?v=3bvwTNoUnwc
Report comment
Malaika,
You are far from being the only one. Yes the ones that expose them, end up
in the “bad camp”, but something does shift. Education provides people a basis
to become more conscious.
And I think the best thing we can do is to educate that parent or that teenager, to keep
them out of harms way.
I’m sure there are a few shrinks that actually like people and want to keep unsuspecting kids and adults
away from their colleagues. Psychiatry is now stuck in a field where they know what they are and have been
doing is stupid, and very wrong on many levels, and not knowing what else to do.
Like one of their co-opted words, “stigma”, which they themselves create, was nothing more than a smokescreen. And we know that they are stigmatizing and shunning people like Kavanagh.
Report comment
I feel bad if Mr K was hoping to see some immediate change resulting from the article. The FDA is not on our side and neither is industry.
Report comment
Mikaika,
Things can always seem dark. We have to have hope and persevere. Even if there are changes that come about because of this eventually they will be forgotten and chipped away at. We can see that with so many other things.
Just because you haven’t seen results yet does not mean we should give up. In fact I was just contacted by Congress they didn’t tell me anything but normally I never hear anything and so I have believe that the people who have written Congress are making a difference. What we are need are more people to say things and to petition their representatives and to tell others and to not let this die on the vine.
For as John Philpot Curran said “The condition upon which God hath given liberty to man is eternal vigilance.”
When I decided to whistleblow I thought of the admonition by Hillel:
“If I’m not for myself, then who will be for me.
If I am only for myself, what I am I.
If not now, when?”
These issues and the larger issues with the corruption in the FDA endangered my own life and my child’s and so I needed to protect us. I could have just avoided certain drugs but there were so many that I hadn’t worked on and so knew I had no clue as to what had been covered up. Plus what about everyone else. I couldn’t protect ourselves and not others. There are so many acts of corruption that occur in the FDA but people will often just not listen and so often times it’s the better part of valor to try to do what you can internally to fight knowing that you will fail and be overridden. So most of the time I felt it wasn’t worth falling on my sword over things. However in the face of I what I saw as mass murder I felt that if I wasn’t willing to stand up and risk everything then when would I ever stand up.
Similarly with all the corruption that I saw in the FDA in the 2000’s and especially with psychiatry (both inside and outside the FDA) it made me think of the famous saying by Martin Niemöller regarding the Holocaust where there are various versions but where I was especially aware of the one where he said:
“First they came for the socialists, and I did not speak out—because I was not a socialist.
Then they came for the incurables (i.e. mentally ill), and I did not speak out— because I was not an incurable.
Then they came for the Jews, and I did not speak out—because I was not a Jew.
Then they came for me—and there was no one left to speak for me.”
Consequently I believed that what I was seeing was just the canary in the coal mine and that government attacks on citizens could grow worse.
So please everyone, please continue to write and don’t let up. Write Congress. Write newspapers with op-ed pieces. Don’t let up. It’s draining and I know it appears hopeless at times and it’s going to be a never ending battle to have integrity in the system but we can’t give up.
Report comment
Evanhaar, If I create a concept and gather data, is that reliable data?
I create ADHD, then create criteria, then gather data on how many have ADHD,
is that then factual data?
All it shows me is that some kids don’t like sitting in a classroom. It
does not show me that they are or have a disorder.
So the data is false since it presented itself as being a disorder, and
did not present itself as a “disordered” classroom. And it led
to further “data” within the drug industry. So the “data” serves
to uphold a concept of normalcy that someone designed for that child.
The normalcy does not even reside in it’s residency or it’s classroom, he
is simply a victim in the concept and precepts, being the unlucky
kid who becomes data.
Report comment
I would like to point out that there are some statements in this article that are either attributed to me that I did not say or that might erroneously be assumed that I that said but did not.
1. I did not say that I didn’t find antidepressants particularly helpful. What I said is I can’t tell if they worked for me or not as each time I started antidepressants I also pulled back from overwork in high stress environments. Where the change in my work conditions might well have allowed me to improve. In fact I think this is likely as I often saw major improvement in my symptoms within 2-3 days. This doesn’t mean that the antidepressants weren’t helpful over a longer time. You simply can’t tell in any individual patient in the vast majority of cases (including yourself), and because of the high percentage of people who improve without drug which means that most people on antidepressants would have improved anyway.
2. Regarding akathesia and suicide. Although people claim this and it’s possible that it may be true. The signals I saw of suicide and suicidality with antipsychotics did not include any evidence of akathesia and it’s entirely conceivable that akathesia and suicide may be completely unrelated. In other words I simply don’t know and I’m not claiming that they are related or not.
There may be other things in the article I disagree with but I’m not going to go through everything now.
Report comment
I appreciate your scientific mindset in not ruling things out when you really don’t have data to draw a conclusion. I wish more folks had that attitude.
I will add here that it is in my experience very difficult, in fact often next to impossible, to detect “signs of akathesia” beyond a person telling you what is going on. There are sometimes external signs, like being unable to stay in one place for long, or restless legs and that sort of thing, but it is described as an INTERNAL sense of restlessness and agitation. It may or may not be accompanied by obvious externals symptoms, and a meaningful discussion with the subject would be necessary to make a definitive diagnosis. It is also easily overlooked or seen as symptoms of “the disorder” rather than recognized for what it is.
Report comment
Aren’t the “signs of akathesia” the means to ensure that the maximum amount of damage to the brain is being done, whilst remaining undetected? For example, one doctor I am aware of takes his ‘patients’ to the point of shaking uncontrollably with lithium, and then backs it off a notch. A bit like a welder who blows holes in the metal and then turns the amps down by 5. Nothing magical about that.
The real magic lies in the motive for wanting to blow holes in the metal, and the inability to prove the intent. (you have no idea the problems that were caused when doctor here went into a police station and provided them with the murder weapon, the place the body had been disposed of, and a full and unconditional confession [means, motive and opportunity. Motive not usually present when doctor doesn’t ‘confess’]. The Police had to dig up the wrong body to be able to find “insufficient evidence” lol. The major problem of a joint enterprise (given the decision by the UN that the State IS responsible for the crimes of it’s officers) resolved now with our Euthanasia Laws (and the ability of the State to “edit” legal narrative and deny access to effective legal representation)
I note Himmler resolved the ‘issue’ he was faced with in Dachau after the report of Hartinger in the same manner. (Führerprinzip)
Report comment