
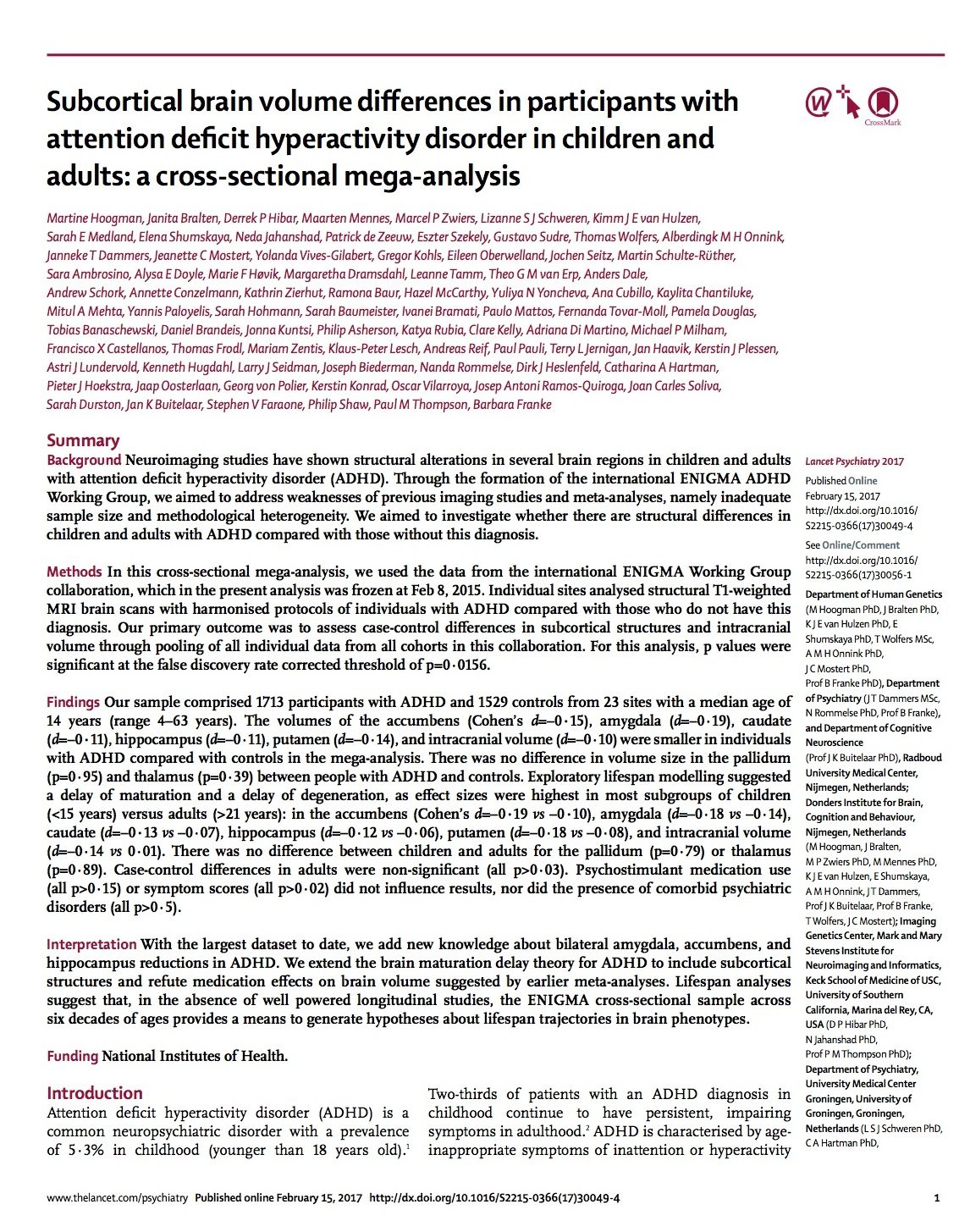
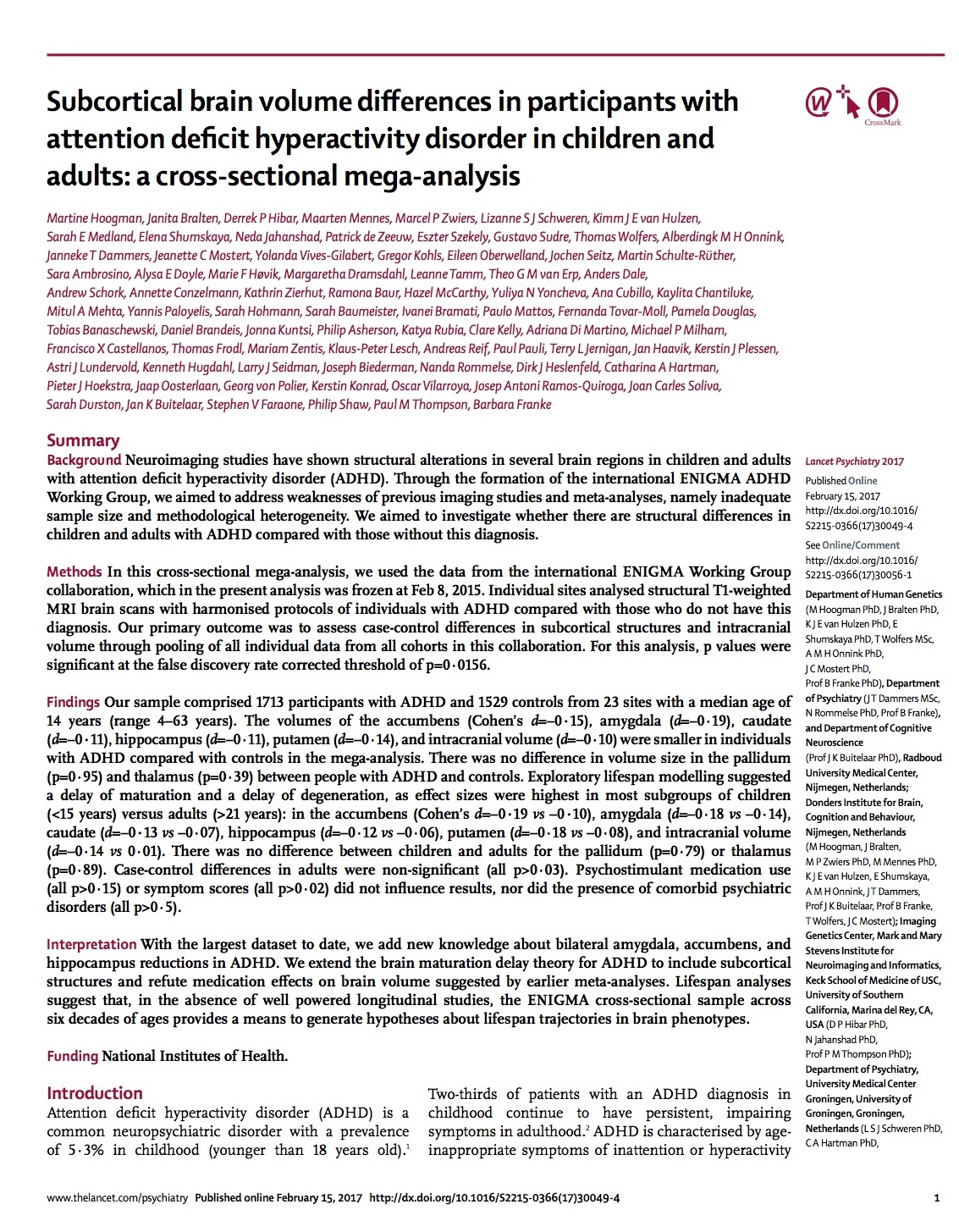
Lancet Psychiatry, a UK-based medical journal, recently published a study titled Subcortical brain volume differences in participants with attention deficit hyperactivity disorder in children and adults: A cross-sectional mega-analysis. According to the paper’s 82 authors, the study provides definitive evidence that individuals with ADHD have altered, smaller brains. But as the following detailed review reveals, the study does not come close to supporting such claims.
 The study is beset by serious methodological shortcomings, missing data issues, and statistical reporting errors and omissions. The conclusion that individuals with ADHD have smaller brains is contradicted by the “effect- size” calculations that show individual brain volumes in the ADHD and control cohorts largely overlapped. The authors also failed to discuss the fact that the ADHD cohort had higher IQ scores. (See editor’s update at end of article re IQ data.)
The study is beset by serious methodological shortcomings, missing data issues, and statistical reporting errors and omissions. The conclusion that individuals with ADHD have smaller brains is contradicted by the “effect- size” calculations that show individual brain volumes in the ADHD and control cohorts largely overlapped. The authors also failed to discuss the fact that the ADHD cohort had higher IQ scores. (See editor’s update at end of article re IQ data.)
{kind=link}
Despite such scientific missteps, the study made headlines in many countries around the world. Yahoo News suggested that the study was “proving the reality” of ADHD. Lancet Psychiatry should immediately retract the study and new media headlines must be aired to inform clinicians and parents of the true results from this study, including the IQ data.
The Study’s Claims and Headlines
In the study, Martine Hoogman and her 81 co-authors conducted a secondary data analysis of MRI scans used to measure brain volumes in 1713 patients diagnosed with ADHD and 1529 individuals who did not have this diagnosis. This data was gathered from 23 sites around the world. The authors wrote that their study, “using the largest dataset to date,” documented that “the volumes of the accumbens, amygdala, caudate, hippocampus, putamen, and intracranial volume were smaller in individuals with ADHD compared with controls” (p.1).
There are many similar statements in the paper suggesting that this study provides evidence that smaller brain volumes are specific to individuals with an ADHD diagnosis. In their analysis, the authors also stated that they had investigated the ADHD cohort’s exposure to stimulant medication and determined that the drugs played no role as a possible cause of the smaller volumes. “We . . . refute medication effects on brain volume suggested by earlier meta-analyses,” they wrote (p. 1).
This was a large international study, funded by the National Institutes of Health. Their results, the authors concluded, contained important messages for clinicians: “The data from our highly powered analysis confirm that patients with ADHD do have altered brains and therefore that ADHD is a disorder of the brain. This message is clear for clinicians to convey to parents and patients, which can help to reduce the stigma that ADHD is just a label for difficult children and caused by incompetent parenting. We hope this work will contribute to a better understanding of ADHD in the general public” (p. 7).
The press releases sent to the media reflected the conclusions in the paper, and the headlines reported by the media, in turn, accurately summed up the press releases. Here is a sampling of headlines: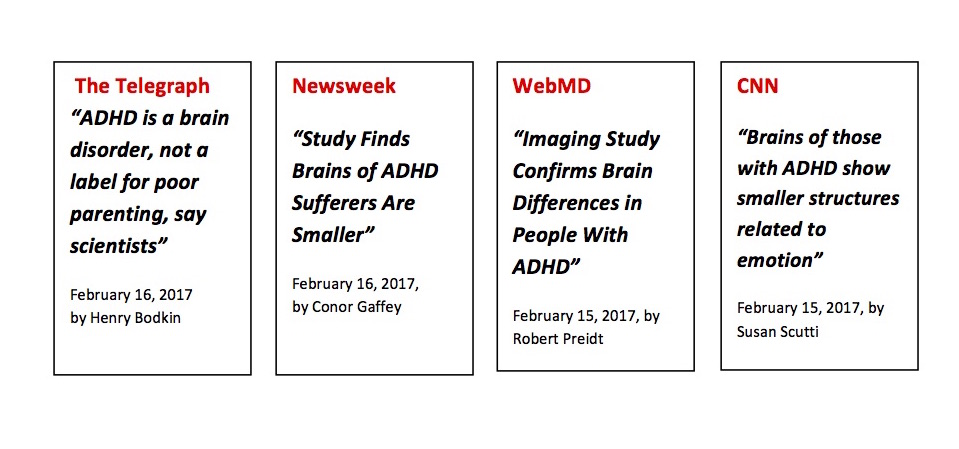
Together, the authors’ claims and media headlines make for a powerful public message. Parents of children so diagnosed will now perceive their children as having something wrong with their brains. The children themselves will understand that this is true, and this “knowledge” will further define their sense of self. While Hoogman and colleagues stated that this understanding will “reduce the stigma of ADHD,” the opposite is more likely true. It will increase the stigma, for it informs the public that the child diagnosed with ADHD is abnormal. The study implies that ADHD children suffer from an inferior “smaller brain,” and that this is true of every child so diagnosed.
Given the implications of this study’s claims, it deserves to be closely analyzed. Does the study support the conclusion that children and adults with ADHD have “altered brains,” as evidenced by smaller volumes in different regions of the brain? And did the authors present data that convincingly “refutes” earlier studies suggesting that medication exposure may be a cause of smaller brain volumes?
To begin this review, we’ll start with a surprising finding tucked away in an unusual place—the study’s appendix. We can then imagine what media headlines might have looked like if the authors had focused on this data.
Alternative Headline: Large Study Finds Children with ADHD Have Higher IQs!
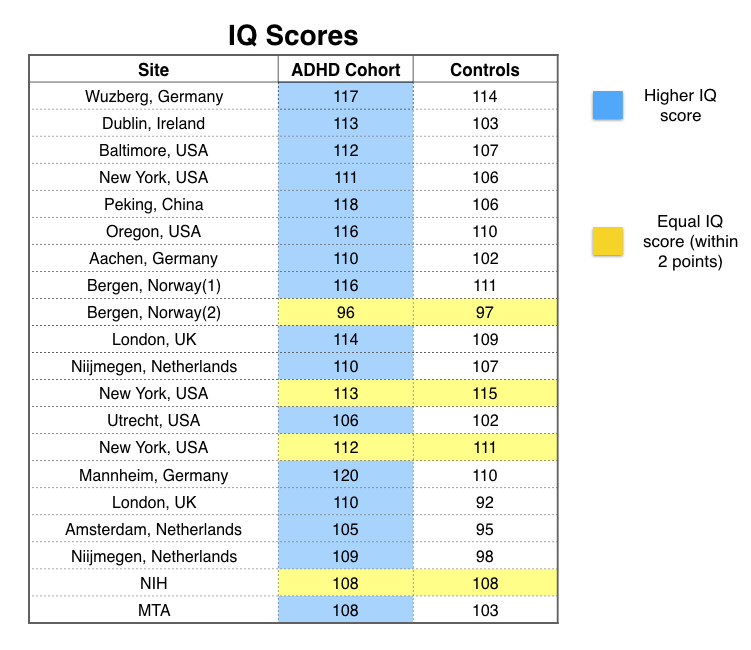
To discover this finding, you need to spend $31.50 to purchase the article, and then make a special request to Lancet Psychiatry to send you the appendix. Then you will discover, on pages 7 to 9 in the appendix, a “Table 2” that provides IQ scores for both the ADHD cohort and the controls.
Although there were 23 clinical sites in the study, only 20 reported comparative IQ data. In 16 of the 20, the ADHD cohort had higher IQs on average than the control group. In the other four clinics, the ADHD and control groups had the same average IQ (with the mean IQ scores for both groups within two points of each other.) Thus, at all 20 sites, the ADHD group had a mean IQ score that was equal to, or higher than, the mean IQ score for the control group.
 Now the usual assumption is that ADHD children, suffering from a “brain disorder,” are less able to concentrate and focus in school, and thus are cognitively impaired in some way. The authors of this study told of findings that show ADHD is a disorder of the brain. But if the mean IQ score of the ADHD cohort is higher than the mean score for the controls, doesn’t this basic assumption need to be reassessed? If the participants with ADHD have smaller brains that are riddled with “altered structures,” then how come they are just as smart as, or even smarter than, the participants in the control group?
Now the usual assumption is that ADHD children, suffering from a “brain disorder,” are less able to concentrate and focus in school, and thus are cognitively impaired in some way. The authors of this study told of findings that show ADHD is a disorder of the brain. But if the mean IQ score of the ADHD cohort is higher than the mean score for the controls, doesn’t this basic assumption need to be reassessed? If the participants with ADHD have smaller brains that are riddled with “altered structures,” then how come they are just as smart as, or even smarter than, the participants in the control group?
The authors, however, chose to bury the IQ data in an appendix, which isn’t easily obtained. Even after you purchase the paper, you have to make a special request to obtain the appendix. Why? And why didn’t the authors discuss the IQ data in their paper, or utilize it in their analyses? When a scientific investigation leads to a surprising result that basically contradicts the study’s main claim, authors are duty-bound—in terms of adhering to the ethical values supposed to govern science—to present those results. But the authors of this study didn’t do this, and this is a principal reason that the study needs to be retracted.
Indeed, if the IQ data had been promoted in the study’s abstract and to the media, the public would now be having a new discussion: Is it possible that children diagnosed with ADHD are more intelligent than average? Maybe we are drugging millions of bright children because they are more easily prone to boredom and schools aren’t providing them with stimulating learning environments.
The authors claim that their study should reduce the stigma of ADHD. If they were truly interested in reducing the stigma associated with ADHD, then reporting that the IQ scores of children so diagnosed were equal to, or higher than, the IQ scores for the controls at all 20 sites would have done just that.
They Did Not Find That Children Diagnosed with ADHD Have Smaller Brain Volumes
While the summary statement in the study and the associated press release tells of robust, definitive findings, leading to media headlines that “Study Finds Brains of ADHD Sufferers Are Smaller,” a review of the reported “effect sizes” reveals that they found no such thing.
When the public reads that a study proved that children diagnosed with ADHD have smaller brain volumes, most people will naturally assume this is a characteristic found in all children so diagnosed. The assumption is that the researchers must have established a “normal” volume (which would be the mean brain volume for a control group), and then determined that most, if not all, of those diagnosed with ADHD have smaller brain volumes than the norm.
But that was not the case here.
In this study, the authors pooled together MRI brain-scan data for the 3,242 participants in the study (which had been collected and archived at the 23 sites), and then calculated, for each cohort, mean intracranial volumes and mean volumes of specific brain regions. They reported the differences for each of these comparisons and the “effect size” of the differences. This is the critical aspect of the results to consider and understand: effect sizes reveal the true strength of the findings and how much overlap there is between the individual brain volumes in both groups, and thus establish the likelihood that an individual in the ADHD group has a smaller brain volume than an individual in the control group.
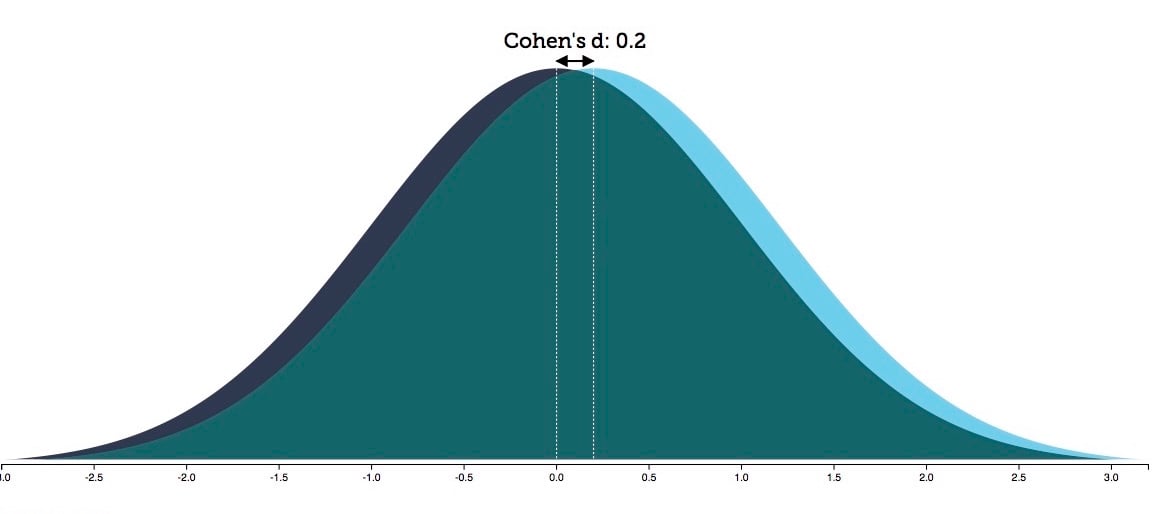
For instance, the authors reported a Cohen’s d effect size of .19 for differences in the mean volume of the accumbens in children under 15. According to the authors, “the accumbens, with its prominent role in reward processing, is central to motivational and emotional dysfunction in patients with ADHD” (p. 7). Cohen’s d effect sizes range from zero to three, and thus .19 is understood to reflect a small effect. Yet, in this study, for youth under 15, it was the largest effect size of all the brain volume comparisons that were made. (To learn more about what an effect size is, access this article by Robert Coe: It’s the effect size, stupid.) Specifically, as to what this effect size of .19 means:
- Approximately 58% of the ADHD youth in this convenience sample had an accumbens volume below the average in the control group, while 42% of the ADHD youth had an accumbens volume above the average in the control group.
- Also, if you knew the accumbens volume of a child picked at random, you would have a 54% chance that you could correctly guess which of the two cohorts—ADHD or healthy control—the child belonged to.
In short, if you just flipped a coin to guess which of the two cohorts the child belonged to, your odds of being right would be nearly the same. The diagnostic value of an MRI brain scan, based on the findings in this study, would be of little more predictive value than the toss of a coin.
There are ways to visualize the overlap of this data. If you plotted the individual accumbens measurements for all 1,637 children under age 15 in this study, and used a red dot to mark the ADHD participants and a black dot to mark the controls, you would see a mishmash of red and black dots. There would be a slightly higher percentage of red dots located in the lower half of the scale, and a slightly higher percentage of black dots in the upper half, but you could immediately see—from the mixed jumble of dots—that “small brain volume” was not a distinctive characteristic of individuals within the ADHD cohort. The individual brain volumes varied greatly, and that was true for both cohorts, and all the pooled data showed was that there was a slightly greater chance that any individual child diagnosed with ADHD, compared to a child in the control cohort, would have an accumbens measurement that plotted into the lower-volume half of the graph.
Indeed, if you drew a distribution curve plotting the individual accumbens scores for the two groups, the two curves would only be slightly offset. By rounding the .19 effect size up to .2 for illustration purposes, you can see there is a 92% overlap between the two curves.
The effect sizes for the other seven brain-volume comparisons made in children under age 15 ranged from .01 to .18. All of the effect sizes were quite small. And with this understanding of what effect sizes reveal, it is easy to see that the findings, as presented in the study and in the media, are completely misleading. The authors made it sound as though a child diagnosed with ADHD has a smaller brain volume as a matter of course, and that this is the defining characteristic of the disorder, when, in fact, the authors found that the individual brain volumes for the two groups largely overlapped.
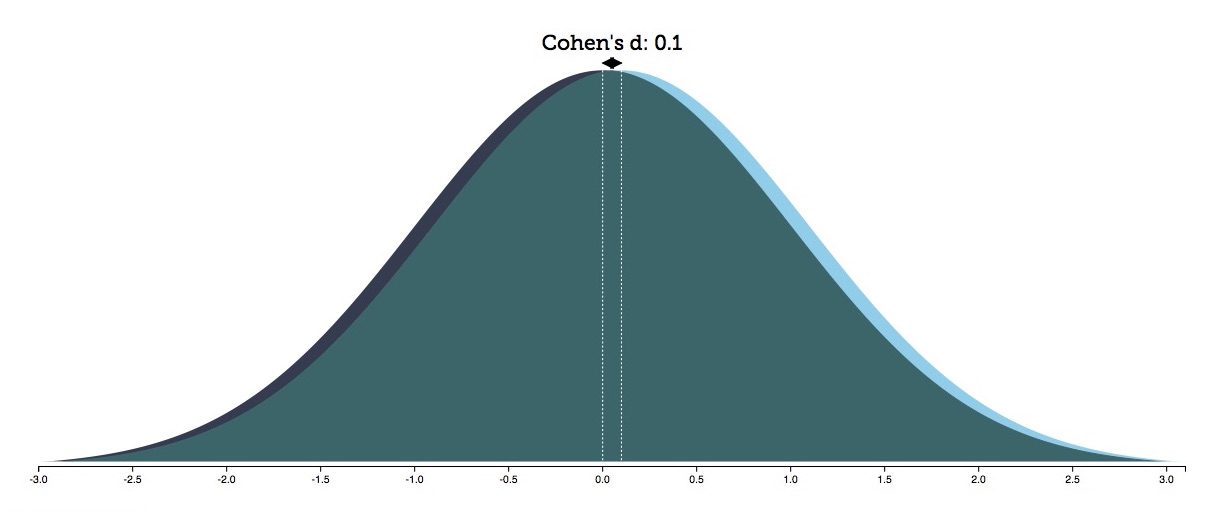
With a Cohen’s d effect size of .1, as was the case for the palladium brain-volume comparisons in children 15 and under, there would be a 96% overlap between the two groups.
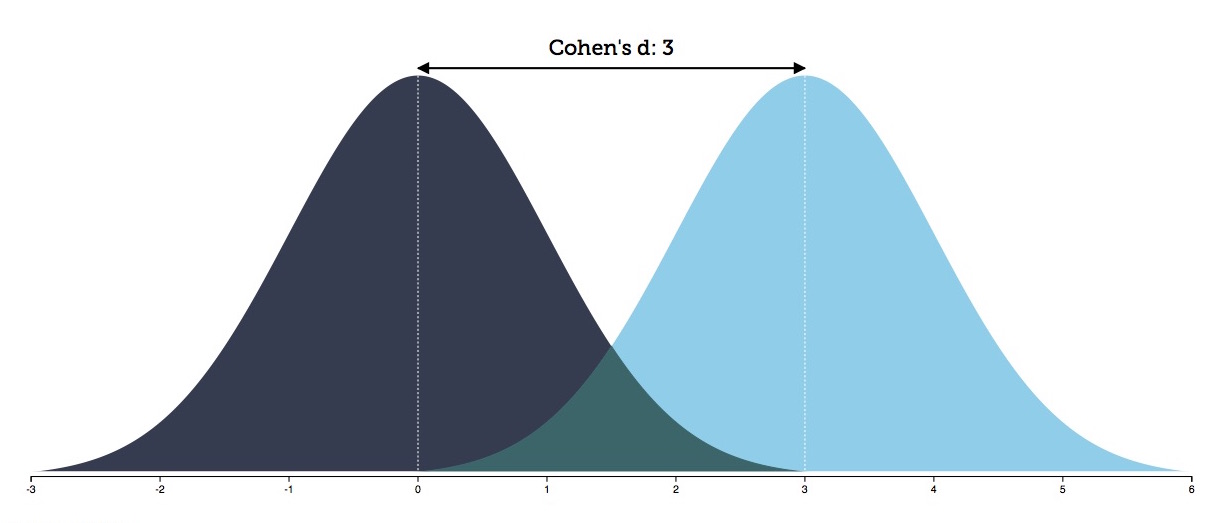
Now let’s return to the statement made by Hoogman and colleagues that their study showed that brain volumes are “smaller in individuals with ADHD compared with controls.” The Cohen’s d effect size of such a finding would be 3, because it is a statement implying that all those with ADHD have smaller volumes than the mean volume of the controls. In this case, there would only be a 13% overlap between the distribution curves of the two groups.
The scientific fallacy in the study is this: You can’t take data that tells of a mean difference in pooled brain volumes that is of a small effect size and generalize that difference to individuals in the ADHD cohort, and present it—as Hoogman and collaborators did—as a defining feature of ADHD.
The Medication Effect
As noted above, the authors’ findings show there were small differences in the mean brain volumes for children with ADHD and the control group. Previous studies had suggested that ADHD medications could reduce brain volumes, and thus Hoogman and collaborators assessed whether the small differences in mean brain volumes might be due to exposure to such psychostimulants.
To do so, they compared the mean brain volumes of two groups in the ADHD cohort: 82 who said they had never used stimulant medication (medication-naïve), and 637 who said they “had used stimulant medication somewhere in their lifetime for a period of more than four weeks” (medication-exposed). The authors reported that there were “no differences in any of the volumes” between the medication-naïve and medication-exposed groups, and thus concluded that their study “refuted” the earlier studies. (p. 5)
But there were notable shortcomings in their performing and reporting of this analysis. Specifically:
- They didn’t publish the mean volume data for the two groups. They simply declared that the volumes were the same.
- They didn’t report how many of the medication-naïve and medication-exposed patients were children and how many were adults. Given that it was mainly in children under age 15 that there were “statistically significant” differences in mean brain volumes between ADHD and controls, their effort to look at whether medication exposure was a factor in those differences should have isolated medication use in that age group.
- They didn’t provide any dosage-related information for the medication-exposed group, or information on how long they took the drugs. If a 30-year-old had taken a stimulant for four weeks as a child, could that really be expected to have a long-term effect on brain volume? And more to the point: were there volume differences between the “ADHD” children who had been on the drugs for several years and the children in the ADHD cohort who had never used them? That is the type of comparison that needed to be made.
- There is a missing group of patients in this comparison. At one point in their paper, the authors stated that they had information about medication use for 1254 of the 1713 participants in the ADHD group. Yet their comparison involved only 719 patients (82 plus 637). Why did they exclude 545 patients (1254 minus 719) from this comparison? [See footnote for a possible explanation for this.]
Without more comprehensive data presented and such questions related to missing data answered in the methods or results sections, there is no way to assess whether this study provides a “refutation” of concerns that ADHD medications may decrease brain volumes over time. We are just asked to take the authors’ word for it, and that is not an example of how you validate a scientific finding for a controversial issue.
Individual Site Data Also Belies the Stated Conclusion
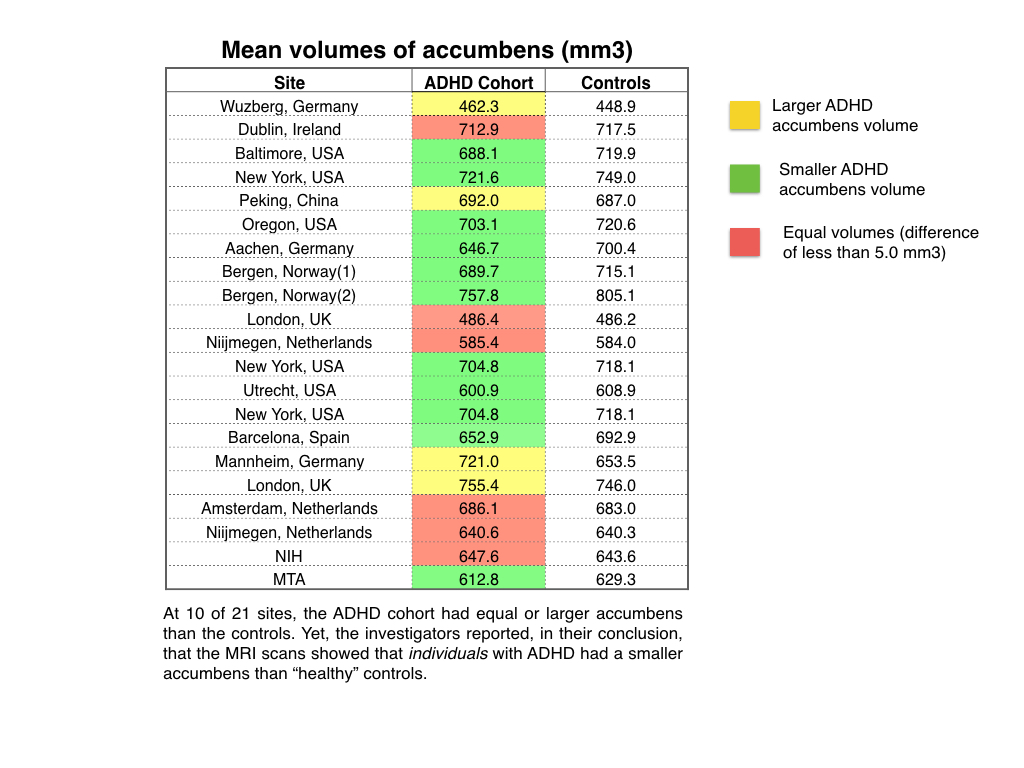
The authors reported that the “volumes of the accumbens, amygdala, caudate, hippocampus, putamen, and intracranial volume were smaller in individuals with ADHD compared with controls in the mega-analysis” (p. 1). If this is true, then smaller brain volumes should show up in the data from most, if not all, of the 21 sites that had a control group. But that was not the case.
Here are summaries of individual site results:
- Mean accumbens volumes: At 4 sites, the volume for the ADHD cohort was larger than for the control, and at another 6 sites, the mean volumes were basically of equal size.
- Mean amygdala volumes: At 5 sites, the mean volume for the ADHD cohort was larger than for the controls, and of equal size at 4 others.
- Mean caudate volumes: At 5 sites, the mean volume for the ADHD cohort was larger than for the controls, and of equal size at 2 others
- Mean hippocampus volumes: At 7 sites, the volume for the ADHD cohort was larger than for the controls, and of equal size at 4 others.
- Mean putamen volumes: At 5 sites, the volume for the ADHD cohort was larger than for the controls, and of equal size at 1 other.
- Mean intracranial volumes: At 5 sites, the volume for the ADHD cohort was larger than for the controls.
The problem here is obvious. If authors are claiming that smaller brain regions are a defining “abnormality” of ADHD, then such differences should be consistently found in mean volumes of ADHD cohorts at all sites. The fact that there was such variation in mean volume data is one more reason to see the authors’ conclusions—that smaller brain volumes are a defining characteristic of ADHD—as unsupported by the data.
Indeed, imagine if each of the 21 sites (those with a control group) had published their data independently. The scientific literature would then be filled with a decidedly mixed bag of results. Some sites had found that the mean volumes for a particular brain region were larger in ADHD cohorts, others had found no differences, and still others had found the same regions were smaller in ADHD cohorts. Nobody would look at such confounding results and conclude that this literature confirmed that children diagnosed with ADHD had “altered brains” characterized by smaller volumes in various regions of the brain.
But once again, this reveals the flawed science—one might say absurd science—present in this “mega-analysis.” The authors used pooled data that ignored the conflicting findings at individual sites, and yet these pooled results are assumed to be representative of all the ADHD patients in the study. For example, the authors report that the accumbens region is smaller in ADHD patients, when at 10 of 21 sites, the mean volumes of the ADHD patients were the same as the controls or larger. The ADHD cohorts in those 10 sites don’t fit into the “pooled” finding at all, and yet the authors still write that “individuals with ADHD compared with controls” have smaller accumbens.
The Study is Riddled with Scientific Flaws
The diagnosis and assignment to cohort problem
For this study, it is explained and understood that there is one group that has ADHD, and a control group that does not. But given that there is no biological marker that can be used to make this diagnosis, how was this distinction made?
The methods section in the published paper does not provide any information about this critical question. Instead, the authors simply write that “diagnostic procedures for each site are listed in the appendix” (p. 3). So turn again to Table 2 in the appendix, and you find that there was no standardized diagnostic method applied at all sites. Instead, this critical distinction—ADHD versus no ADHD—was made in a haphazard manner.
First, two of the 23 sites didn’t even have a control group. So it’s hard to understand why the ADHD measurements from these two sites were included in the pooled data.
Second, it appears that none of the participants in the control groups at the remaining 21 sites were given a diagnostic assessment for ADHD. There is no report of any ADHD symptom scores for the controls. The participants labeled “healthy controls”—and thus seen as not having ADHD—were apparently never tested to see if they displayed the behaviors associated with this diagnosis.
Third, the authors didn’t test nearly a thousand of the participants in the control cohort to determine if they were “healthy.” They listed 867 in the control cohort as unknown related to comorbidity issues such as depression, anxiety, and substance abuse. Without such testing, it would not seem that this “not ADHD” group could be described as “healthy controls.”
There is, in fact, very limited information about the controls. Why would these individuals have agreed to participate in this study? Were they recruited via advertisements that promised them payment? Or were they patients at the clinics who were getting an MRI for other medical reasons? In the appendix, the authors did state that 30 controls were diagnosed with depression, 11 with anxiety and 39 with substance use disorders. But with so little comprehensive information provided, it’s impossible to know how representative of “healthy controls” this group is.
Fourth, at seven of the 23 sites, there aren’t any ADHD symptom scores listed for the ADHD cohort. One can only guess how the diagnosis at those sites was made. Did the authors have records from the participants’ doctors? Or did they rely on the participants’ own self-diagnosis or self-report that they had ADHD? There is no way to know.
Fifth, even when symptom severity scores were reported, there was no standardization of the “instrument” used to assess symptoms, or the classification system used to make the diagnosis (either DSM IV or ICD 10). In other words, the authors at a clinic in Brazil might have had one standard for diagnosing ADHD, and the authors in China a second standard, and the authors in the UK a third, and so forth.
Yet, despite this lack of diagnostic and methodological rigor, the authors still stated that “the brain differences we have reported are not caused by any comorbid disorders, medication effects or ADHD symptom severity, but are exclusively related to the ADHD diagnosis” (p. 7). This is a puzzling conclusion to make, given that a large percentage of the participants were not tested for comorbid disorders, or for severity of ADHD symptoms, or—in the case of the controls—even for ADHD.
The fact that symptom severity didn’t show any relationship to brain volume differences also presented the authors with an obvious conundrum. At 16 sites, they theoretically used symptom severity to assign participants into the ADHD cohort, and if the ADHD cohort had smaller brain volumes than the controls, then symptom severity should seemingly be linked to smaller brain volumes as well. But that was not the case. The authors’ explanation for this confounding result is quite revealing: “Not finding effects of symptoms scores might also be due to the heterogeneity of the [differing] instruments used for different cohorts in our study or difference in raters (i.e. clinicians, teachers, and parents)” (p. 8).
In other words, they explained away this confounding result by suggesting that the tests used for assessing ADHD symptoms at the various sites were too different to provide meaningful results. They also suggested that the diagnoses of ADHD were often made by unqualified adults, e.g. parents and teachers, who have no expertise in the use of the DSM or making an ADHD diagnosis (and also lack the legal authority to do so).
Yet, as statisticians well know, there is an easy way to standardize data when the tests or data measures are different (such as a lack of standardization in diagnosing ADHD, as was the case here). In regression analysis, this is called “centering” and easily accomplished by converting the different data into z-scores. But the authors of this study did not standardize the data, even though this lack of standardization may have thrown a wrench into their results.
The MRI reliability problem
There is a gee-whiz sense to MRI scans that leads one to think that brain volume measurements made with this technology must be very precise. The assumption is that this modern technology allows authors to see into the brain and distinguish with great clarity one brain region from another. But that was not the case in this study.
The first concern in a multi-site MRI study is that different MRI machines may be used, with different imaging powers, which most likely was true in this study. The second concern is that the threshold, color, contrast and ordinates a technician chooses to use for an MRI scan may vary greatly from site to site. The machines used to image the brain and measure brain volumes may not be standardized to measure the same thing consistently from place to place.
Typically, in order to account for such site-to-site variations in MRI measurements, the authors must make adjustments that “normalize” the results. In this study, the authors did report that “data for all sites were newly analyzed with harmonized methods.” However, their “harmonizing” of the data amounted to simply checking what version of software was being used by the machines, which does not account for differences in threshold, color, contrast and ordinate settings at each site.
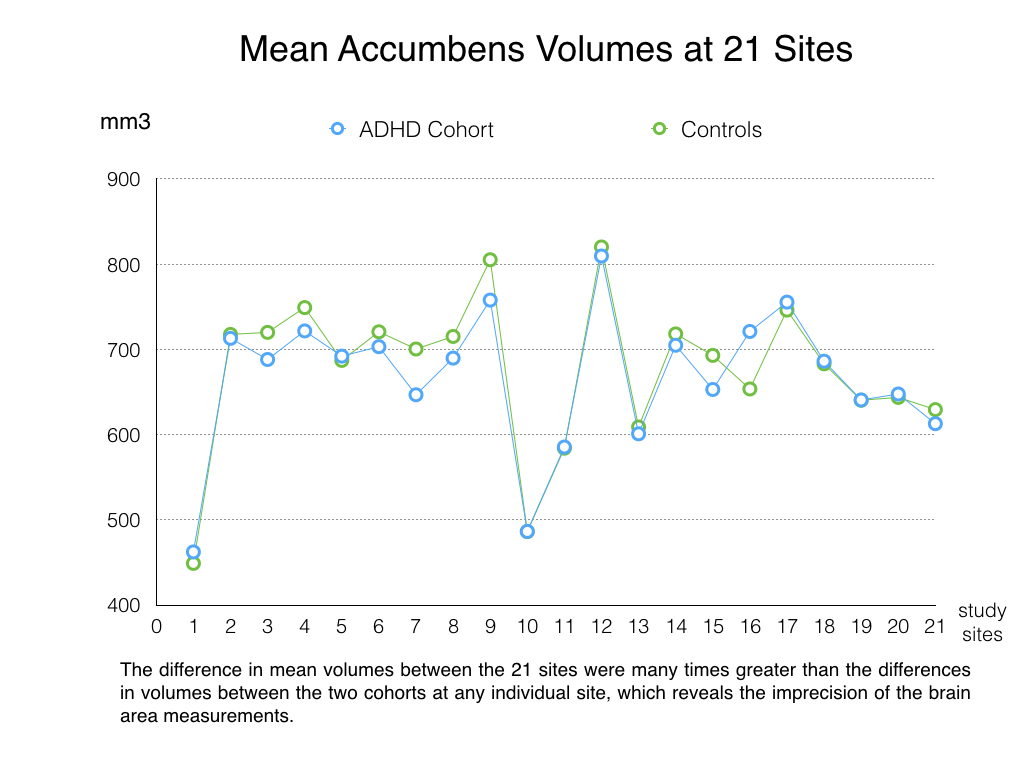
A quick comparison of volume findings at different sites reveals how imprecise the measuring methods were, even after this harmonizing effort. For instance, at the ADHD-WUE clinic in Wurzburg, Germany, the mean brain volume for the accumbens region, for the two cohorts together, was 455.6 mm3. Meanwhile, for the same region of the brain at the MGH-ADHD clinic in New York City, the mean was 814.8 mm3 for the two cohorts together. This was so even though the authors had adjusted these results for “age and sex.” We either have to assume that the accumbens region in children and adults in New York is 55% larger than the same region for children and adults in Germany, or conclude that the measurements of brain volumes in this study were remarkably imprecise.
 This was not a problem isolated to the accumbens measurements. Table 4 in the appendix provides a detailed account of the many large variances in brain volume measurements at the 23 sites. At an ADHD clinic in London, the mean brain volume for the amygdala was 1284.1 mm3. At a clinic in Dubai, it was 1824.1 mm3. The measurements appear to be very exact, with volumes reported to one-tenth of a mm3, and yet the gross difference between the mean volumes at the ADHD clinics in London and Dubai is a whopping 540 mm3.
This was not a problem isolated to the accumbens measurements. Table 4 in the appendix provides a detailed account of the many large variances in brain volume measurements at the 23 sites. At an ADHD clinic in London, the mean brain volume for the amygdala was 1284.1 mm3. At a clinic in Dubai, it was 1824.1 mm3. The measurements appear to be very exact, with volumes reported to one-tenth of a mm3, and yet the gross difference between the mean volumes at the ADHD clinics in London and Dubai is a whopping 540 mm3.
But if the MRI scans did not produce consistent measurements across the 23 sites, how can such measurements be deemed reliable and, most important, valid? And with such large differences in volume measurements between sites, how can the authors lay claim to having found meaningful differences in the averages of pooled volumes from the two cohorts, when those mean differences were so small?
Indeed, just as the authors acknowledged the lack of standardization in diagnosis, so too they acknowledged that “acquisition of imaging data . . . differed between sites, a limitation contributing to heterogeneity across samples” (p. 8). Again, these are methodological shortcomings that should lead researchers to refrain from making definitive claims of proof.
And there are still more problems
There are many more scientific problems with this study that could be identified. But in order to keep this critique of reasonable length, here are just a few more.
(1) Errors: In several instances, the statistics do not appear to have been reported correctly. For example, in Table 3, which details the small yet somehow “robust” Cohen’s d effect sizes for youth under 15 years of age, the difference in mean accumbens brain volumes for the ADHD cohort and controls is declared significant for diagnosis with p = .0001 and with a Cohen’s d effect size of -.19. Yet, the confidence interval (CI) for the effect size goes from -.29 to .10. If a finding is significant, its confidence interval usually doesn’t cross zero by going from a negative number to a positive number. This signals an uncertainty of whether the mean volume of the accumbens region is smaller (negative number for effect size), or larger in the ADHD cohort (positive number for effect size). In addition, there are numerous errors within the appendix. Were these errors due to typos, misunderstanding of the results, or, worse, inaccurate results being reported?
(2) Missing data: As we discussed above, there are many instances of missing data—missing ADHD symptom severity scores at some sites, no controls at two sites, no information about comorbidity information for nearly 1000 participants in the control cohort, and so forth. Textbooks regularly warn about how such missing data can lead to a misinterpretation of results and inaccurate findings. Yet it would appear their dataset was not cleaned appropriately for any of the analyses they performed.
(3) Omissions: The authors stated that they performed more than 10 analyses to come to the conclusions they did. But in the published study, they present limited results from less than one-third of the analyses. Without the results for each analysis, one cannot fully check their results for accuracy. Usually, in the peer-review process, such omissions would be identified, and the authors would be directed to provide the data that would enable readers to verify and better understand the stated findings. This did not happen in this study.
(4) Assumptions not met: There are multiple required assumptions that must be met for a researcher to perform specific inferential analyses, such as the regression analysis that the authors of this study claim to have performed. For a regression analysis, there needs to be random sampling procedures, normal distribution of the sample, and verification of the reliability and validity of the measurements in order to insure that the results are not being misinterpreted. It would appear that the authors did not meet any of the required assumptions needed to perform any of the 10-plus analyses. This is very critical point to consider.
For example, reliability represents a measure of how consistently an assessment measures the same thing over and over. Research documents that the less reliable your measurements are, the more likely your study’s statistical findings will be inflated. This can lead to what is called Type I error, when your findings appear to be significant but in reality they are not. Given the lack of reliability for assessing brain volume and ADHD in this study, the results were most likely inflated and reported inaccurately. And given that an assessment cannot be valid if it is not also reliable, then the authors cannot state with confidence that they indeed measured what they said they measured.
(5) Non-random convenience sample: As mentioned above, in an analysis that seeks to make generalizable claims of “fact” like this study does, the participants should come from “random sampling” of a larger population. For example, if you put the names of 250 patients with the same diagnosis into a hat, and drew 25 names for the study, then you could say you had a representative sample of the larger population being studied. This “sampling” allows researchers to feel more comfortable in generalizing their findings to the larger population.
But there was no random sampling in this study. Instead, the datasets that were pooled together could best be described as a collection of “convenience” samples. A convenience sample basically represents a group of people who were easy to find, as opposed to being representative of the larger group. This dataset consists of MRI scans of individuals who conveniently were clients that had signed off on allowing their assessments to be used in research, or who, for some unknown reason, agreed to participate in the study.
There are other statistical reporting errors and omissions that could be highlighted. But suffice it to say, the scientific shortcomings of this study are many: a hiding of the IQ data; small effect sizes that belie any finding that small brain volume is a defining characteristic of ADHD; a lack of data presented regarding the confound of medication exposure; no consistency of mean-volume findings across sites; no standard method for diagnostic assessment; unreliable measuring tools; no representative sampling of patients; and a remarkable lack of information about the cases and controls.
Lancet Psychiatry: Do the Right Thing
The media gave this study a great deal of attention. They presented this study—which was written by an authors’ group that included many who had close ties to pharmaceutical companies that sell ADHD medications—as proving that ADHD is a brain disorder, and that children so diagnosed have smaller brains. But this was not the media’s fault. Reporters were basically repeating what Lancet Psychiatry promoted to the media and what the authors wrote in the abstract and summary sections of their published paper. Their data, the authors wrote, confirmed that patients “with ADHD have altered brains; therefore ADHD is a disorder of the brain.”
But, as the effect size findings reveal, that is not true. The distribution curves of individual brain volumes in the two cohorts mostly overlapped (and that isn’t even taking into account the many scientific problems that provide reason to question the validity of even the small differences in mean volumes that were reported). As such, it is grossly misleading for the authors to present their results as definitive evidence that individual children with ADHD have smaller brains, or suffer from “altered brains.”
There is also this haunting question: Why did the authors hide the finding that the ADHD youth had higher IQ scores at 16 of the 20 sites? The hiding of this finding is, in its own way, as egregious as pretending that the pooled mean volume data, with its small effect sizes, showed that individuals diagnosed with ADHD have smaller brains.
The publication of this study, with its bottom-line message that ADHD children have smaller brains, does a great disservice to those children and to their parents, and ultimately to all of society. It essentially tells a lie, wrapped in the gauze of science, about those children. Lancet Psychiatry needs to retract this study, and inform the media that this has been done.
If you agree, please sign our petition at change.org.
*******
- One possible reason for the exclusion of the 545 patients, in the researchers’ inquiry into whether the small difference in mean brain volumes was due to the medication, is that the analysis software they used eliminated all data for the participants with missing data related to stimulant use. If so, the missing data here is a sign that the authors did not adequately clean their dataset to account for this problem in the first place. Failure to account for missing data greatly increases the chance of what is known as a Type II error in reporting results. In other words, due to missing data weakening the analysis, they might have assumed the stimulants showed no significant effect on brain volume size when in reality the drugs did.
*******
Update on 4/24/2017: Lead author Martine Hoogman said that IQ scores in published article were in error, with this error to be corrected in an Erratum published in May. The correction will state that the IQ scores for the ADHD and controls were mistakenly switched in the appendix, and that the controls in fact had the higher IQ scores.
Update on 4/29/2017: Lancet Psychiatry editor Niall Boyce told MIA that the journal will not retract this article.
Update on 5/8/2017: Lancet Psychiatry has published letters critiquing the paper, the authors’ response, and a correction.
Differences in brain volume may be attributed to factors such as trauma, abuse and neglect, so this “mega study” proves nothing
Report comment
Because those conditions also lead to the same indications, or signs and symptoms as they are referred as, that is “behaviors,” this is a serious confound to any attempt to make statistic inferences! While there is a recognition of the existence of a naturally adhd cohort, there is also recognition of a cohort who have developed so as to reflect diagnostic inclusive behavior. No study can get by if these groups are not treated as separate etiologies and if it does not reflect the difference between them. The first group, the naturally adhd, includes for the most those who go on to have anti-social behaviors, which is how under 18 years of age psychopaths are mentioned because admitting the serious stigma that goes with that diagnosis, they are shunted into the catchalls .
Report comment
The whole difference, should there actually be one, may easily be explained by the increased ADHD diagnosis of children who are the youngest (and smallest) in their class. Unless this is extremely accurately controlled for by using months of age for all participants, the data is totally invalid.
Report comment
…and why is the blatant deception inherent in this study so unsurprising?
The truth is that psychiatry and pharmaceutical companies will do ANYTHING possible to ensure the continuing flow of human fodder to ensure their money-making machines continue to grow. It doesn’t matter to them that it’s CHILDREN who are being irreparably damaged and hooked into the system for life – they see it as a major achievement.
And what’s more, it’s children of higher than average intelligence whose parents are being sold the lie that their children are quite fundamentally defective.Tragic.
Can psychiatry become any more morally and ethically bankrupt?
Report comment
“Can psychiatry become any more morally and ethically bankrupt?”
They’re working on it, Mik. With Murphy the Merciless at the helm I’m sure they’ll find new levels of depravity and turpitude to sink to.
Report comment
its a money making industry that the drug companies and psychiatry are peddling these days so its not surprising that children are now a target the way the age keeps decreasing all the time with those diagnosed maybe soon we see babies being diagnosed as i mentioned before did anyone say its medication madness ??? Spot on Doctor!
Report comment
One group was even trying to convince people that babies in the womb were already Bi-Polar! So, let’s start drugging people before they are even born into the world!!! One wonders how much more disgusting all of this can become but psychiatry and the drug companies never cease to amaze. This is all morally, ethically, and professionally wrong.
Report comment
Thanks for identifying the Psychopaths!
Madness involves concocting theories that a reasonable person would rubbish, and this is exactly what ADHD is.
Report comment
I do not see where Mad coppped to doing this. I posted in a reply about ADHD being used along with anti-social disorder etc to weasel out of an early but “stigmatic” diagnosis of psychopathy for those under 18. psycopathy Dx requires 3 years of the symptoms, they must start before 15… in other words, like some statute laws that control minors, so diagnosis is controlled by issues of social sentiments and prevailing interests of ll sorts, all on a base of don’t speak poorly of the children, which is normally o.k. except when the child is trying to commit murder by age 10!
Report comment
All mental illnesses are controlled by social sentiments and prevailing interests of all sorts of (wealthy, powerful) groups. Psychiatrists have the power to vote various “illnesses” in and out of existence. Doctors can’t do that with cancer.
There are no biomarkers used to diagnose mental illness. While the brains of “bipolar” patients shrink, it seems to correspond to the length of time spent in “treatment” rather than how long the person has experienced mood swings. Furthermore, they have no control group. Conveniently they claim it’s unethical to examine the brains of the “treatment naive.”
I wouldn’t be surprised if there were something similar going on with these claims that “ADHD” kids have unusually small brains.
Report comment
some, not all, ar so controled. But then so is diabetes/pre-diabetes. so is “morbidly overweight. So does tht mean these dont exist? there are “bio-markers here. How are they interpreted, that is the valid issue.
give me a citation for the time/dose dependence of shr inkage is due to psy drugs assertion tou make. you are aware of some, citations, i assume. Are you refuting the neroprotective qualities of a variety of drugs from pot and morphene to several of the psy drugs as well?
i hope.
Report comment
I thought I’d add a comment about my own autodidactic studies. Perpetual emotional trauma can indeed alter the brain’s structure and chemistry.
When you consider the emotional trauma that occurs with mental illness labeling and various “treatments” even if the victim is willing, the effect of treatment-induced trauma needs to be considered in examining the brains of the “mentally ill.” This would be a factor too, even though not directly linked to the drugs.
Report comment
They have been labelling people with “bipolar disorder” due to SSRI/Ritalin induced mania for quite sometime now, even though such episodes would never likely have occurred without the drugs in the first place.
The comparisons to diabetes miss out key points.. You cannot be harassed or abused into getting diabetes. However, I could lock you up in a room and torture you to the point that you exhibit all the features of a “paranoid schizophrenic”.
Also, labelling a person as a diabetic will not influence the diabetes itself. Labelling a person with a DSM label will influence the person’s mental state in various ways, in terms of self-image and how people treat them as well, thereby becoming a causal factor in the behaviours that compile the very label itself (which becomes a self-fulfilling prophecy)
Behavioural labels, in theory, are far more susceptible to creation than non-psychiatric labels, because there is a massive set of behaviours someone may want to pathologise.
At the level of family, it may be a spouse accusing their significant other of being insane, and at the global level, it may be coming up with treatments for “Internet Gaming Disorder”, all of which will have neural correlates because there is no mind without a brain.
Report comment
Thank you so much for doing this work. It is so important to expose these types of science-frauds. I am just in shock about what is going on. Money and power and status corrupt; there is nothing new about that. But they are going after our children now……
Report comment
There are other very basic problems too.
1. The classical “correlation is not causation” applies perfectly to this study. If there were a difference, it could be that a highly active body leads to smaller brain structures, or hundreds of other factors that would be very different between very active children and the more conventional.
2. Size of brain structures is not necessarily an indication of lower function. Women have smaller brains than men, with a much larger difference than what is found in this study. Height is very strongly correlated with brain size, 3 grams pr cm of body length. Should we therefore conclude that small women are disordered and tall men are the most intelligent? The brain actually goes through a pruning process in childhood, to get rid of brain cells that are not needed. Maybe the slight difference ,( if we should accept the results) is a result of children having streamlined their brain in this way?
3. In MRI studies, there are so many structures that are studies. If the researchers pick out regions that are smaller from 100, then even if there is no difference, 5 of the regions will be smaller at a statistically significant level. Seems to fit with number of regions in this study.
4. There is no reason to think bigger is better. Bigger structures would necessarily have slower processing. That is why pruning takes place to get more efficient structures.
Report comment
Kjetil, this is a great comment and I’m surprised no one except markps2 has yet commented similarly about how brain size does not necessarily reflect level of functioning. As you wrote, other researchers have found that the brain goes through a neural pruning process as it matures and I know that some studies have shown that people with higher grey matter in one part of the brain actually tend to have poorer cognition on some measures. Larger does not necessarily mean better. But psychiatry researchers often jump to conclusions.
Report comment
a larger startle response system should be related to a smaller executive function. Is this controversial at all? There is no sense, just nonsense, in talking in such general terms if you want to move the discussion forward. Scientist do jump to conclusions. Scientists have a way of calling them for it. It is the scientiifooc method. It iis fine to hold you and others trying to improve the wrld by using science in different settings to use some of the method as well. the article, though I see some errors in it just like the reserach they criticize, is at least a start. However I feel Mad often foes past the start gate with its own conter-“mainstream” agenda, often a decade behind trends there.
Report comment
bigger does not imply slower. Active should make more processing mass, not lead to higher pruning. On these two points you are missing the basics of morphology and development.
otherwise:
Size DOES relate to body size. Some adjust for this. We have no indication even from the mad review if this was done or not, so I can not condemn the report. want to take a look or ask a mad person who investigated?
Report comment
Did anyone notice that the same Martine Hoogman who conducted the study also writes in her conclusion that ADHD must be understood as a brain disorder “just like major depression, schizophrenia and bipolar disorder”? Wow, that woman really is a genius! Like the female Einstein. I must have missed something then. When did science prove that those three can also be seen in the brain? Or did she make that up too?
Report comment
Well informed scientist that Hoogman is I assume she made that up.
Report comment
give it up, the research here is overwhelming. The real problem is not the scientific evidence. The real problem is the continuing sloppy diagnostics of the industry. There i completely agree with Mad in America. It is too bad they don’t do more beyond a simple condemnation and then moving on to the anti-lab science beat down. By shorting the strong argument and fighting the lost argument they do not move the issue forward significantly.
Report comment
As an individual who has taken B3 for over 40 years, I’ve seen my share of this sort of thing in periodic sensational attempts to “refute” its use for treating psychiatric syndromes, generally featuring some kind of “double blind” study that never uses hidden controls like niacinamide or inositol hexanicotinate, which would make such studies truly double blind- niacin, itself, can’t be double blinded because it causes flushing when one starts taking it.
Report comment
Fish oil, zinc and other b complex. Yet when i try to find any mention on NIMH pages? nothing comes uo! not a good indication that this is an open debate. sad is it not!
http://impactadhd.com/organize-your-life-and-family/treating-top-vitamin-mineral-deficiencies-adhd/
Report comment
Why should NIMH, an arm of psychiatry, criticize the psychiatric industry? Why should it say anything positive about alternatives to psychiatric drugs?
Report comment
thats a rhetorical question as you pose it. Following on your first words, i dont see much room for open debate near you either. I point to a sad state and you jump in with the cut and paste arguments. come on, you can perform at a higher level than that! you act as if a large bureaucratic army doing many things somehow magically speaks in unison here. why, read all the contradictions allowed between papers they produce. who do you think decides where difference is allowed, where no? who do you suppose has no better way to spend time?
Report comment
Sorry. Your sentences are too convoluted for me to make sense of them either here or in your previous post.
Report comment
Try some kippers!
Report comment
Mr. Corrigan,
Excellent analysis of the study you’ve done, and a great model for someone like me learning how to critique psychiatric studies of other things such as “schizophrenia.”
My thought from the beginning of reading your article was that, in a sense, almost everything you discussed was more than was necessary, because the diagnosis of ADHD is made based on subjective judgment, without biomarkers, and thus lacks validity. The sequence is that these researchers label people with ADHD based on vague criteria – and THEN seek to look for differences between these kids and others arbitrarily labeled “normal” – rather than FIRST identifying a clearly observable disease process and going from there. It is the same thing as usual in psychiatry – circular logic and assuming one’s conclusions.
You did eventually get to that point:
“For this study, it is explained and understood that there is one group that has ADHD, and a control group that does not. But given that there is no biological marker that can be used to make this diagnosis, how was this distinction made?”
But in my opinion one could have begun the analysis by undermining their whole study on this basis alone. Still, the other critiques are useful, so thanks.
Report comment
a great model for someone like me learning how to critique psychiatric studies of other things such as “schizophrenia.”
Just chiming in with my standard point, i.e. “schizophrenia” is NOT a “thing.”
Report comment
lol, oldhead.
Report comment
I was just thinking – that I might like to critique a few published papers!
There’s a lot of b*llsh*t out there..
Report comment
I agree, “it” isn’t a thing. I will make this point in future writing.
Report comment
Schiz is a spectrum of distinct clusters of predisposing factors and of separate often but not always overlapping “behaviors” as well as the lack of some behaviors. of course it is not a thing. So what? When is the last time you looked into the current lab research? I find M in Am. to be guilty of ignoring too much of it because they are not willing or able to reconsider the arguments that have “succeeded” so far to maintaining a place in the conversation. If they dont stay current they will pass into history. While I have big issues with the group, I recognize them as an important voice and would not like to see them disappear.
While there is always subjectivity in such, so also in medical conditions such “subjectivity” plays a part.
The issue with diagnostic evidence as with infections is a trope that should be abandoned. the issue should be the lack of using the diagnostic evidence (as one factor, not as conclusion- this is how it really works, not just opinion of one doc one short moment. (this should be recognized as a real problem and severely criticized when discovered!) Mad should learn to pick its battles better is all I wanted to say.
Report comment
Ever try Mary Boyle’s Schizophrenia: A scientific delusion? The last word on an intellectually dishonest concept.
Report comment
If they ever find real proof it doesnt matter. Saying that people with ADHD traits have something wrong with their brains kind of like saying white people have something wrong with their skin. Maybe all white folks should take tanning pills that contain canthaxanthin, a naturally occurring chemical found in several plants and animals. Because canthaxanthin dissolves in lipids, which make up the tissue directly below the epidermis, the color attaches the cells under your skin, and gives it a darker tint.
Neurodiversity is the fact that neurological differences like so called ADHD are the result of normal, natural variation in the human genome, we don’t need to drug one in six boys, that is as insane as the tanning pills for white people.
Right now, the most typical person in the world is a 28 yo male, right handed person of Chinese descent. That will change in a few years, as the Indian population is poised to pass China, though. There are nine million people who match that description, more than any other on the planet.
Report comment
Correction: I said one in six boys the NYT says one in five. This is absurd the idea one in five boys has a broken brain.
“Nearly one in five high school age boys in the United States and 11 percent of school-age children over all have received a medical diagnosis of attention deficit hyperactivity disorder, according to new data from the federal Centers for Disease Control and Prevention” http://www.nytimes.com/2013/04/01/health/more-diagnoses-of-hyperactivity-causing-concern.html
Report comment
This is the result of a completely broken government school system that thinks it can produce cookie cutter citizens. I’ve always thought the ‘Little Boxes’ intro song from the television show Weeds described it perfectly. We are all nothing but commodities to consume and be consumed.
Report comment
Believe me I know. They refuse to modify the schools to fit the children and instead try and use drugs to modify the children to fit the schools but its deeper then that.
Common Core’s real goal? ‘Dumbing down people’
“That is primarily because the phony remedies, which will extort taxpayers for more billions, only purport to treat the symptoms rather than the root cause – the fact that the system was literally designed to dumb down American children as a crucial element of replacing liberty and self-government with collectivism and tyranny.”
In “Crimes of the Educators” Newman and coauthor Samuel Blumenfeld expose many of the false solutions to America’s education woes. They write about the increased use of psychotropic drugs to try and treat ADD and ADHD in children. http://www.wnd.com/2015/04/common-cores-real-goal-dumbing-down-people/
Report comment
Oh, it’s not broken. It works quite well at creating docile, unquestioning, anxious sheep. We only believe it’s broken because we have the mistaken impression that schools exist to create truly educated citizens. In truth, that’s the last thing our corporate owners want.
Report comment
I find your animus to the school system quite fine. I disagree about what it produces. More than seeing than docile sheep I see the school to detention to prison pipeline as the major “accomplishment” Some corporate owners realize there is little place in the future for more docile competitors for jobs that are disappearing to automation. Without big deadly wars to control population (as were the crusades of earlier ages of too many youths) the prison owners are poised to out do the old industries seeking that docile product.
Report comment
first they dropped the vocational schools, then they dropped music then recess and time to use all the normal childhood energy. Then the unions decided to champion all the lousy teachers who were there for the retirement package and were not willing to be creative ( creativity is harder when the school is shorted cash to supply materials like art supplies and musical instruments and…)
Report comment
20% of all boys drugged up mean lots of $$$$. That’s all the Mental Illness Makers care about. Plus they can curry favor with all the castrating misandrists and thought police. It’s tough to be male nowadays. (I’m a woman.)
Report comment
Wa-wow! How about doing a study to determine whether ivy leaguers have bigger brains than other college educated people, or if professionals have larger brains than industrial workers, and then whether the same is true of college trained professionals and workers, and their untrained colleagues, or not? You can also do the same regarding information on skilled laborers, and unskilled laborers. I imagine conventional wisdom would say yellow brains have to be bigger than white brains, and white brains have to be bigger than black brains, but we’d still need to sift through the data to arrive at a conclusion. Anyway, they’re just out to pick on poor students, aren’t they?
One thing I am certain of is that this insistence that the drugs don’t have any effect must be bogus. Fry a person’s brains with amphetamines (standard treatment for ADHD), and, you know, if they were all there before, they aren’t going to be all there afterwards. Of course, these guys are so far in with the drug companies that they aren’t going there under any circumstances.
I think one must remember that before you had ADHD, you had ADD, and before you had ADD, you had something called minimal brain dysfunction (MBD). Apparently these 80 something psychiatrists have determined to their satisfaction that you still have minimal brains dysfunctioning. Such a determination, of course, supports the profession of psychiatry, and keeps a growing river of customers for the treatments, primarily drugs, that they are selling. If the treatment leads to no cure, or no recovery, all the better, there’s job security in that, and this at a time when the claim is being made that we need more, many more, psychiatrists in order to service the many customers we are creating. Excuse me, of course I meant to administer to all the as of yet untreated “sick” people we are finding inhabit the world today.
Report comment
By these standards of judgement shouldn’t whales and elephants be the smartest mammals? (Actually whales may be but that’s a different issue…I think).
Report comment
Aren’t the smartest mammals those who don’t go to war with each other, don’t destroy their environment, don’t promote overconsumption and the inherent inequality that goes along?
I think ‘human intelligence’ is a bit of an oxymoron.
Report comment
Lol, kindredspirit. It does seem we have the dumbest or most insane people in control right now … never ending wars against “terrorism,” a concept??? It’s absurd.
Report comment
I was being facetious. Consider, for instance, if I had made male sexual endowment contingent upon brain smallness. The scale doesn’t change, does it? There is a great deal of more difference between any two species than there is within any one species, despite those differences that do exist.
I wouldn’t consider ‘human intelligence’ an oxymoron, but I would certainly differentiate between mere intelligence and the wisdom that might, or might not, come of such intelligence. We can teach people to be smart, no problem. Can we teach them to be wise? I’d say that is a much more nebulous subject, and, unfortunately, there might be a fork in the road whereby the road to success branches off from the road to wisdom.
Report comment
You state my sentiment more eloquently than I do. Your last sentence sums it up perfectly.
Report comment
Is ‘ human wisdom’ an oxymoron or just more than thejobs worth for these people.
Report comment
Cats have brains no bigger than unshelled peanuts. They seem pretty smart to me, though.
Report comment
Wayne Dyer had his butterfly story where he spoke of brains the size of pinpricks guiding beings basically made of tissue paper through transcontinental flights and back to the same places from which they started.
Report comment
Which came first the label or the brain scan? Isn’t ADD A Daddy’s Drama? :p
Report comment
After reading this excellent article I googled the Lancet Psychiatry study. Maybe I didn’t look hard enough, but there was universal acceptance of the study’s conclusion that individuals with ADHD have a brain disorder. This was the case on sites that are written for the general public as well as on sites written for health care professionals. Unfortunately, I’ve found that the problem of fake science is not limited to psychiatry. It is rampant.
Report comment
“Unfortunately, I’ve found that the problem of fake science is not limited to psychiatry. It is rampant.”
‘Science’ is the religion of the 21st century and ‘science’ worshippers are rampant. I’m always reminded of the quote “information is not knowledge” when I hear of the latest scientific discovery being hailed as ultimate truth.
Report comment
Science is one thing, scientism another.
Report comment
Scientism is essentially what we’re left with at the end of the day though. I found interesting:
https://www.expat-journal.com/is-science-overrated/
Report comment
Indeed, a mathematician asked if ADHD was a valid construct might look at the data and go reductio ad absurdum!
Report comment
Fake history, too. Psychiatry has managed to develop it’s own fake history for the fake disease of ADHD. When history involves imposing the present on the past, too, straightening the matter out can appear more than a wee bit intimidating.
Report comment
and it is NOT limited to the mainstream side. There is plenty of absurd new age idiocy as well, there have always been snake-oil vendors. patent medicines and “cures” that gain credibility by screaming how they are repressed.
Report comment
That certainly is true. But they don’t have the legal authority to lock you up and force these ineffective and/or harmful “cures” on you.
Report comment
I am used to skewed studies, but this one seems like a record-setter! I am stunned that The Lancet or any other journal would accept such a questionable study, especially the unwarranted conclusions. It is disturbing that such crap is passing for “science” these days. I wonder who got paid off?
Report comment
I just listen to a talk on bilingualism today, by a pedagogue and researcher who is actually rather good at what he does. He also told us this anecdotal story of how English speaking Americans were feeling offended (in modern talk) by all the bilingual schools all over the country, that they paid some folk off to prove once and for all that bilingualism, particularly when introduced at a young age, is damaging to a child’s development. This happened around 150 years ago, and might actually still hold a place above the one presented here on that record list. That guy did a whole lot of digging, and really did find the original documents to prove this is the real reason why most countries in the Western world is still so ridiculously, even unnaturally, monolingual.
Report comment
positive results always are move likely to be published. So there are research leaches who capitalize and hack their own science to get published, and they even send out pre-publication promotional literature. You must have laughed at how many clickbait websites look like blatant cut and paste from them?
secondly thee overpriced journals get content and thanks to the publicity and citation stats for the articles, they get impact scores that bestow prestige. meantime the research community is in open revolt. interesting times, are they not?
Report comment
17 years ago my colleagues and I showed that the IQs of children with ADHD were normally distributed [1]. Interestingly, the reason we even investigated the question is because at that time there were many claims that children with ADHD were unusually intelligent. Seems sort of funny now.
Thanks for writing this analysis.
[1] Kaplan BJ, Crawford SG, Dewey D, Fisher GC (2000). The IQs of children with ADHD are normally distributed, J Learn Disabil, 33: 425-432.
Report comment
Hi Bonny,
We all have this imaginery illness – do you not have it yourself?
Report comment
Bonny, not trying to say you didnt see what you saw in that study. I wonder though with such constructs as ADHD and yes, even the schizophrenias, that treating these constructs as a single “entity we re not setting up to find no differences. I have little to no trust of the statistic methods applied even now in most instances. They belong to ca.1980 and before!
Having said this, I admit I find such results as a strong finding in the lancet article to be “extraordingary” enough to require some “extraordingary” evidence. The confounds of meta studies are well and fairly laid open in this critique.
Could you share some of your distribution data? I wonder how perfectly the line was. regression math is always an assumptive process. It hides our presumptions behind cold math. I hear some go to third derivative analysis to find whatever they want to find from these “distributions.”
Report comment
Great criticism of an obviously flawed study, thank you gentlemen.
You stated that, “This was a large international study, funded by the National Institutes of Health.” So I take it this is proof that the NIMH’s Thomas Insel’s promise to defund research into the scientifically invalid DSM disorders has been rescinded?
As to, “Is it possible that children diagnosed with ADHD are more intelligent than average? Maybe we are drugging millions of bright children because they are more easily prone to boredom and schools aren’t providing them with stimulating learning environments.” I do think this is a conversation that would be infinitely more productive and beneficial to society, especially more so than just continuing to force medicate millions of children with amphetamines, which is insane and morally reprehensible. I will add that the only time I ever got a call from the school social worker was when my son surprised the school by getting 100% on his state standardized tests, and the call was not to congratulate me oddly. My point being the school social workers do have some sort of odd desire to get their grubby little hands on the highly intelligent children.
You also mentioned, “there was no standardized diagnostic method applied at all sites. Instead, this critical distinction—ADHD versus no ADHD—was made in a haphazard manner.” Isn’t it always? Well, except that it’s overwhelming given to the youngest children in a classroom, if I’m not incorrect.
“They also suggested that the diagnoses of ADHD were often made by unqualified adults, e.g. parents and teachers, who have no expertise in the use of the DSM or making an ADHD diagnosis (and also lack the legal authority to do so).” This happens all the time, I’ve been at cocktail parties listening to “unqualified” adults diagnosing children for sport. Personally, I think the adults should take the logs out of their own eyes, prior to trying to take the splinters out of the children’s eyes.
Report comment
Big brain vs small brain as an illness is stupid, because the description of big or small does not specify which brain works better.
How tiny is a fruit fly’s brain and look at what it can do. http://www.futurity.org/fruit-flys-tiny-brain-finds-food-well/
In the case of a heart, an enlarged heart is a bad thing. Where metaphorically to have a big heart is a good thing.
http://www.dictionary.com/browse/big-hearted
VS
https://en.wikipedia.org/wiki/Cardiomegaly
No behavior or misbehavior is a disease. http://biologicaldentalhealth.com/video-no-behavior-or-misbehavior-is-a-disease-or-can-be-a-disease/
Report comment
They call this a highly powered mega study. The reasonfor including so many in the study is that then you can find a difference between two groups even if it is so small that it has absolutely no significant or noticable effect.
It is interesting that they compare ADHD to depression in terms of how clear it is that it is a brain disorder:
“We hope this work will contribute
to a better understanding of ADHD in the general public,
and that it becomes as apparent as major depressive
disorder, for example, that we label ADHD as a brain
disorder”
Google on how to download research paper for free, and you may be able to download the whole paper.
Report comment
Excellent work on revealing what is shockingly sloppy work, all the more egregious given the number of researchers and person-hours that went into this thing. It’s not even like this investigation took sophisticated statistical analyses to detect subtle infractions–just patience, persistence, and logic.
That being said, I will stick my neck out, and add some comments that most readers might find unpalatable.
First, while this study does nothing to support the “ADHD is a brain disease” theory, neither does it confirm that ADHD is NOT a neuropsychological disorder.
Second, while the buried IQ data represents a shame of scientific miscommunication, it also says nothing about the nature of ADHD as a disorder.
Third, I find it unfortunate that arguments against ADHD as a diagnosis often resort to school misbehavior being misperceived. That is, kids who have ADHD are really just unable to manage an unreasonably restrictive school system, so of course they are going to climb the walls. What is unfortunate is that this is only trying to account for one domain of functioning. Say what you will about the inadequacy of the DSM diagnosis, but one of its foundational criteria is the behavior must occur in at least two separate contexts.
Fourth, methylphenidate (Ritalin) does not “fry your brain.” The differential effect that stimulants have on ADHD vs. non-ADHD kids should be a sign that areas of their brain are functioning differently (notice I said nothing about size, which I agree is a ridiculous variable to target in developing brains). I am NOT advocating for prescribing stimulants for diagnostic purposes, heavens no. I also don’t think they should be prescribed for more than 2-3 years tops (check the MTA study for why).
Fifth, whatever you choose to call the pattern of behaviors and difficulties faced by these kids, there is no denying its existence–at least not by those who have experience in working with them. That is, there is a percentage of the population, maybe 3-5%, who have ADHD. YES, kids as a whole are overdiagnosed and inappropriately diagnosed kids are wrongly medicated. But this is a baby-bathwater situation. Clearly, if someone is behaving in a markedly different manner than the people around them, then, guess what, their brain is doing it. Now, what one chooses to do with that information is a separate consideration.
I hope that those of you who have chosen to read this far can do so with a balanced mindset.
Cheers
Report comment
Maybe we should inject children who can’t sit still for prolonged periods of time with toxins to paralyze their leg muscles. Because if a child keeps getting up and walking around their legs must be responsible.
Report comment
Good one! It is just as absurd a premise as paralyzing their brains, though cultural mythology allows the latter premise to sound viable.
Report comment
When I used to teach, if the kids got restless and fidgety, I would have them get up and run in place or do jumping jacks. It always worked too.
Report comment
For active children, medication would be no different from paralyzing their brains. I’m in the lucky situation that i know quite a lot about as many as 230 children between 6 – 16 years of age. I also know that as many as 2-3 of those children have gotten ADHD medication that helped them concentrate rather than paralyze their brains. Which means I’m certain of two, but the last one is a half guess.
One of those sadly got on medication way too late, and spent years unable to concentrate on anything. That one wasn’t more active than others, there were boys in their class who had much more problematic behavior, but this individual really only had problems with acquiring knowledge from either reading or listening. But after they finally got medication, they were suddenly reading books and enjoying it.
But that’s the tiny percentage which may not even be as much as 2%. Unless medication helps a child concentrate and learn, it should be discontinued since the effects of the medicines haven’t been studied enough or in the right way yet, and thus really only should be used if they enhance the user’s quality of life significantly.
Report comment
sounds like you dont want to listen to a reasoned but out of step with the sheeple feeding Mad Party Line. This is why the movement to reform practice does not listen to your side either. Thats a sad corner to paint yourselves into.
Report comment
As far as my experience go, MIA has helped me escape a tiny prison cell called Mental “Health” after 25 years. It seems odd you talk about “painting ourselves into a corner.” What compromise do you propose? For the Psychiatric Establishment the only compromise offered is the Tyrant’s Compromise. You can be free by accepting your slave status. You can be at liberty as long as you stay in prison. You can move about as you wish–so long as you wear a ball and chain.
Report comment
With several scientists from the Netherlands I have written a response to The Lancet Psychiatry, due for publishing June, 2017. Our criticism is mostly centred around the overlap between the research groups, mentioned here as well. The authors of this petition add some great points to this. However, I do concur with Kjetil Mellingen who comments on some important missing things, like the correlation-causation error, and the fact that brain size differences do not necessarily implicate dysfunction. Additionally, the fact that brain size catches up later in life –and growth is another bell-curved variable in which people vary- is an extra argument that emphasizes that brain size does not equal illness or disorder. In my view these points could have replaced some of the weaker arguments of the petition.
Personally, I think a little too much has been made of the apparent error in the paper with regard to the confidence interval of the Accumbens. As figure 1 of the paper shows, this is a typo (the figure indicates that the authors have meant -0.10). Additionally, I do not think the fact that several sites that provided data for the study show different, sometimes even bigger, brain parts should be an argument for retraction necessarily. Increasing power by adding sometimes conflicting findings seems one of the points for doing a meta-analysis. Also, the fact that not all controls were healthy does not seem like a strong argument. Arguably, the common use of well-controls is more problematic as they are not representative of ‘normal’ people and thus impede generalizability.
However, the far-fetched conclusion of the research article not justified by the data is sufficient reason for retraction and the editors of the Lancet Psychiatry should have prevented such clear logical and scientific fallacies from being published. The unreliability of the results and the resulting validity problems the authors of the petition expose in addition to this are additional strong arguments why these far-fetched conclusions should not have been published.
Report comment
Wonderful work! As a speech pathologist still working now and then in the schools, I’ve long seen schools serve as factory farms for Big Pharma, and have refused to participate. I will never forget one little boy from an El Salvadorean immigrant family who was put on ADHD meds due to being “all boy”. Prior to the drugs, he was a sparkly little thing. After being drugged, the light just went out of his eyes.
Report comment
I appreciate all of this feedback, and that people are signing the petition. In response to sanneman, I am glad to hear that you and several scientists have written a letter to Lancet Psychiatry. As for the fact that “smaller” doesn’t necessarily implicate dysfunction, I of course agree. But I have to confess that of the two of us (Michael Corrigan and me), I was the one who argued against including that point, for I thought it would somehow be seen as a concession that this study showed that “smaller” brain size and altered structures were indeed common to those diagnosed with ADHD. It raised this response to the study: Even if the ADHD cohort had slight smaller brains, so what? What does that mean? A valid point, but I thought we should stay focused on the fact that the data didn’t show that smaller brain size is a distinguishing feature of ADHD (and thus didn’t raise the question of what might be the implications of having a “smaller brain.”) We also thought that the IQ data argued persuasively against any finding that the brain scans showed some sort of dysfunction. But others who have signed the petition have also made note of the “smaller doesn’t equal dysfunction” point and so this is a mea culpa on my part, for leaving that out. As for the confounding results from individual sites, we thought this was evidence that once again argued against their claim that individuals with ADHD have smaller brains, and thus provided yet another reason to see that their bottom line claims didn’t hold up.
Again, I am very glad to hear that you have written a letter to Lancet Psychiatry that will be published.
Report comment
Thanks for clarifying!
Report comment
Dear Robert,
With regard to your stance on the ‘smaller-is-not-a-dysfunction point’: that is an interesting angle. My perspective was that not mentioning this would leave the option open that those diagnosed that do have smaller brains indeed have a verified brain disorder. With regard to the IQ argument: I think this is also a very interesting point. Seems very plausible that some in the heterogeneous group diagnosed with ADHD indeed are simply bored and unruly because of this, although I would not expect all that much from this -the IQ scores are merely averages as well-. Many diagnosed will probably have IQs as the rest the of us mortals – they’re almost normal humans :-). However, I personally do not feel that leaving the IQ scores out attests to a lack of ethics as it wasn’t the research question of the authors. Although we were not aware of this -we didn’t see the appendix- it would not have been our central argument I think. It is great that you retrieved this additional info though as it is indeed an interesting finding in itself. Thank you for this thoughtful petition, I hope my thoughts help to sharpen your thoughts even further.
Report comment
I think what it reflects is the bias of the investigators, who claim that “ADHD” diagnosed kids have smaller brains (however unsupportable that claim) and yet intentionally buries the data that these supposedly “smaller-brained” individuals appeared to have higher IQs. The higher IQ point is less important than the fact they chose not to comment on it when it didn’t support their thesis.
Report comment
Dear Sanneman, Indeed your thoughts have helped sharpen my thoughts, and I think this is really what needs to happen, that there should a public response, composed of many voices, related to this study. The discussion helps point out for all the many flaws of this study, and how it misleads the public (and many within the psychiatric community, who would see it as validating their belief that ADHD is a biological brain disorder.) Thank you for contributing to that discussion here.
Report comment
“Phrenology (from Greek: phren, “mind”; and logos, “knowledge”) is a defunct field of study, once considered a science, in which the personality traits of a person were determined by “reading” bumps and fissures in the skull. […] However, it has no predictive power and is therefore dismissed as quackery by modern scientific discourse.” (From: https://med.stanford.edu/medwebtraining/shc-class/student5/treatments/phrenology-lab.html)
The modern day version of this quackery has moved from measuring the skull to measuring/scanning the brain and making vast and sweeping conclusions stated as true science. And what a catastrophe! So many people and now our children put on chemicals leading to iatrogenic brain damage on a scale never seen before.
Naturally I have signed but observing how psychiatry works, this appalling piece of research signed by 82(!!) authors will, from now on, be pulled out of the proverbial hat when some poor unknowing parent comes because their child’s teacher thinks little Johnny shows signs of ADHD.
If any of the 82 authors read this very valid critic of their joint article, please support retracting the article from the Lancet and know that you are making a difference for our children… and yours.
Report comment
Thanks Olga.
A “paper” allegedly “authored” by 82 contributors has undermined any status as a scientific endeavour and takes on the perceived purpose as a conspiracy to deceive, and to disseminate the propaganda upon which the grotesque deception of drug-dependent psychiatry is maintained.
A scientist is someone willing and able to change their mind on the basis of accurate observation, analysis and presentation of study data.
By definition, these 82 “experts” cannot therefore be regarded as scientists.
In genuine scientific endeavour, it is the unexpected observation, that which contradicts the underlying hypothesis, which is truly fascinating and which drives forward knowledge and understanding.
By kicking the IQ data into an appendix, this inconvenient yet compelling observation is sidelined allowing focus to remain on the undiluted propaganda.
Who were the referees supporting this publication for Lancet Psychiatry?
They appear to have failed in their duty don’t they?
TRM 123. Retired Physician.
Report comment
I do not have time to carefully examine the details of this study, but I think it is worth considering the fact that the structure of the brain changes with one’s experiences (a phenomenon known as ‘brain plasticity’). Several studies including animal studies (where for example restrained animals have been tested) indicate that the structure of the brain changes as a result of psychological stresses. Now, when one is given a DSM label using a check-list (for ADHD or any other “disorder”), then thereafter, the person is considered to be a “person with that disorder” – this label itself can cause a great deal of stress to the person who has been assigned the label (i.e., the person can get depressed and stressed thinking that one is somehow different from others). As a result of the label, others may treat this person differently as well (e.g. not including the person in their social circles because he/she has that “disorder”). All this psychological stress would then result in changes in the brain and this difference could be what the scientists have observed. As I said, I do not have the time to carefully go through the study details, but if a few years have passed between people being assigned a ADHD label and the testing of brain differences, then we would expect to find structural differences. But as I explained, these differences are a direct result of the psychological stresses caused by a diagnostic label itself – not a result of having some kind of “disorder.”
Report comment
This is unnecessary and turns the argument into a weak — if not fallacious — emotional one:
“Together, the authors’ claims and media headlines make for a powerful public message. Parents of children so diagnosed will now perceive their children as having something wrong with their brains.”
Well, there is something wrong with my brain. Dopamine dysregulation is what’s wrong. It’s “wrong” in the sense that it inhibits optimal functioning. In a different environment it could be what’s right with my brain, but nonetheless, I live in a society where that’s not the case.
“It will increase the stigma, for it informs the public that the child diagnosed with ADHD is abnormal.”
I am abnormal.
The article is largely good, but these quoted parts are ridiculous.
Report comment
“The article is largely good, but these quoted parts are ridiculous.”
Speak for yourself. I, for one, don’t like being referred to as abnormal. Human variation falls on a bell curve. There is no standard definition for what is normal when referring to dopamine, serotonin, or any of the other neurotransmitters. Without there being a standard, how is anyone to be considered abnormal?
It is not weak and fallacious to protect children from being told they are fundamentally broken. The stigma against so-called “mental illness” is very much real. It is damaging. I just fired one of my medical care providers on Monday after overhearing her talking to another about “all the crazy people shooting up the world”. What gets reported to the media has very real implications for those targeted as being the “crazies”. Then those sensational stories get spread on social media. Talk about fake news!
Report comment
we are supposed to qualify all the diagnostic indications with ” to a degree that interferes with …[leading an independent life, having participation in community school job etc..]”or in other words having a life. Since it is obvious many do have these issues, we are merely debating the line of how good is good enough. We set a line of 85 I.Q. for the ability to compete in the open market of this modern world. In 1200 it would be absurd to do so. Times change, should we not attend to how that affects the people living in changed times?
Standards? we have ranges for heart rate, for blood pressure and for other diagnostically usefull quantifables. The lines are always hedged bets. There is nothing profoundly perverse or wrong with this fluid state. Being rigid is the issue, still: 5 ft 5 and 450 pounds? A resting heart rate of 115? By your logic, with not “standard” these are just fine.
Report comment
Genetic variation is the key to species survival. It is only our weird society that requires certain variations to be eliminated for the benefit of those in control.
Besides which, there is no evidence to support a general conclusion of a “dopamine dysregulation” in all or most “ADHD”-diagnosed children. I’m open to hearing something to the contrary, but I’m very familiar with the literature on the subject and know of nothing supporting that other than a few odd studies which have never been duplicated.
And why would we expect to see that all or even most kids that act a certain way have something “wrong” with them, or the same thing “wrong” with them? It is not a logical conclusion that you can diagnose a physiological problem from behavior. Kids act hyper for tons of documented reasons – chaotic families, trauma histories, boredom,lack of sleep, malnutrition, iron deficiency, sleep apnea, certain drug reactions, the list goes on and on… It is ludicrous that you can tell that someone’s brain is malfunctioning based solely on a somewhat arbitrary collection of behavioral indicators, all of which can be summed up as behavior that makes it inconvenient to have this kid in a classroom or to parent them.
I say this as the parent of two “ADHD” type kids who turned out to be very productive adult citizens without a milligram of stimulant drugs. If you feel these things help you out, by all means, use them, but don’t make out that all kids who don’t like to pay attention to boring lectures or follow adult directions are in some way diseased or disordered. There is simply insufficient evidence to even vaguely support such a notion.
— Steve
Report comment
Steve,
Please read the following Study:
Our unclear understanding of ADHD — Neuroscientifically…
http://www.neuroscientificallychallenged.com/blog/unclear-understan...
Nov 10, 2014 … By 2011, about 1 in every 10 children ages 4 to 17 in the United … dopamine dysregulation may not be the primary cause of ADHD. … If a dopamine deficiency isn’t the underlying cause of ADHD, then what is? … del Campo, N., Fryer, T., Hong, Y., Smith, R., Brichard, L., Acosta-Cabronero, J., Chamberlain, …
I believe they are asking the wrong questions Steve. The question should be, What is the cause of ‘dopamine dysregulation’. The answer to that question would be the primary cause of ADHD.
As you know, I believe Kids diagnosed with ADHD are perfectly NORMAL both mentally and physically. In fact, they must have a very good sense of ‘right and wrong’ for ADHD behavior to work for them.
Dr. George Still ruled out ‘Idiot and Imbecile’ behavior 115 years ago, because ‘they’ have no sense of right or wrong.
Report comment
Or an even more basic question: Is “ADHD” actually an entity that can validly be studied at all? That’s my point re: genetic variation. We can pick any spectrum and choose to cut of the end of it we don’t like, and call it a “disorder.” Why would we assume that just because some kids don’t like sitting still, there is something wrong with them? I know, I’m preaching to the choir here, but I think studying “ADHD” is idiotic. If there really were a small percentage who DID have something wrong with their brains, we’d never find it by studying a group of kids who happen to have a hard time tolerating the generally very oppressive atmosphere in the average elementary school classroom.
Report comment
whereas I see this as the perfect reason to study the diagnostic label and what lies under the hood(s) of those given the D.X. we both are pointing to a variety of malfunctions, from bio to situational and more. Anyone truly scientific would want to see whats what, not blatently say these people go here and these don’t , on some acceptance of the infallability of the “bible” the SDM.
I am not of the choir, but I do appreciate and have a lot of points where we agree. Thats a good thing, yes?
Report comment
We don’t really disagree, except on the point that calling this an entity “ADHD” to me really just confuses things. Why not say “Hyperactive behavior” or “inability to pay attention” and study the underlying various reasons for it. Since the people grouped together as having “ADHD” may have nothing in common as to the cause, calling it a disorder is nothing but misleading. Of course, the REAL reason that ADHD was constructed was not to figure out the cause but to sell the “cure,” and many other “disorders” were constructed for the same purpose. Rational people like you and me without conflicting interests could certainly study “ADHD” as to underlying cause with little confusion, but sadly, there is a huge financial and social incentive to call these things “disorders” so that drugs and patented therapeutic interventions can be sold for a profit.
Report comment
“There is no blood or other biological test to ascertain the presence or absence of a mental illness, as there is for most bodily diseases. If such a test were developed…then the condition would cease to be a mental illness and would be classified, instead, as a symptom of a bodily disease.” —Dr. Thomas Szasz, Professor Emeritus of Psychiatry, New York University Medical School, Syracuse
If such a test were developed…then the condition would cease to be a mental illness and would be classified, instead, as a symptom of a bodily disease !
Report comment
Mental Illness is a figure of speech – but some medical professionals promote “mental illness” as real, and this is frightening.
Report comment
As a rule we don’t even have an adequate definition of “mind”!
Then there is the confusion as to whether mind and consciousness are simply emergent properties of matter, or whether they have a reality at another level.
I prefer the Buddhist definition of “coarse mind” ( the consciousness that is wedded to this body) Subtle mind (the consciousness that passes from birth to birth) and very subtle mind- or pure awareness.
Now plenty of people won’t subscribe to the idea of reincarnation, but I like the idea of consciousness being entangled with the body. In that sense the entire distinction between mental illness and bodily illness becomes much more subtle. In fact it is subtle- as can be seen by the number of phrases for mental illnesses and emotional states that reference the body- ie a jaundiced view, bitter and twisted, the straight man.
However these problems would still exist even if we used some other label for them. There are good descriptions of the ADHD phenotype in the 18th Century by Alexander Crighton (a Scottish physician) and Melchior Adam Weikerd (a German physician), and a probable example from Hippocrates too. We do not gain much by simply relabelling them.
Report comment
@The_cat, Fiachra: I do not understand why some people on this website quote the same old crap that the opposition will expect and easily counter?
I mean if you want to quote Szasz, there is much better stuff to quote instead of that line which people will not understand in the context that it is implied in. Most people who quote Szasz haven’t even read him, it seems. For example:
“We can influence others in two radically different ways-with the sword or the pen, the stick or the carrot. Coercion is the threat or use of force to compel the other’s submission. If it is legally authorized, we call it “law enforcement”; if it is not, we call it “crime.” Shunning coercion,we can employ verbal, sexual, financial, and other enticements to secure the other’s cooperation. We call these modes of influence by a variety of names, such as advertising, persuasion, psychotherapy, treatment, brainwashing, seduction, payment for services, and so forth.
We assume that people influence others to improve their own lives.The self-interest of the person who coerces is manifest: He compels the other to do his bidding. The self-interest of the person who eschews coercion is more subtle: Albeit the merchant’s business is to satisfy his customers’ needs, his basic motivation, as Adam Smith acknowledged, is still self-interest.
Nevertheless, people often claim that they are coercing the other to satisfy his needs. Parents, priests, politicians, and psychiatrists typically assume this paternalistic posture vis-a-vis their beneficiaries. As the term implies, the prototype of avowedly altruistic domination-coercion is the relationship between parent and young child. Acknowledging that parents must sometimes use force to control and protect their children, and that the use of such force is therefore morally justified, does not compel us to believe that parents act this way solely in the best interest of their children. In the first place, they might be satisfying their own needs (as well). Or the interests of parent and child may be so intertwined that the distinction is irrelevant. Indeed, ideally the child’s dependence on his parents, and the parents’ attachment to him, mesh so well that their interests largely coincide. If the child suffers, the parents suffer by proxy. However, if the child misbehaves, he may enjoy his rebellion, whereas the parents are likely to be angered and embarrassed by it. Thus, what appears to be the parents’ altruistic behavior must, in part, be based on self-interest.”
“Oh, there is no test or scan” blah blah. Yes, that makes a difference. But not in the way people here write.
If you have a fever, there is no “test” except the fact that you put a thermometer in your mouth and measure your temperature, and then take Tylenol if you are too hot. You will not wait till you find out which infection is causing the fever in every case.
Similarly, if a man is psychotic or delusional and believes that aliens are communicating with him through radio waves, that behaviour itself (analogous to your body being too hot itself) will make most people want him to take drugs.
If you want to argue, at least do it more sensibly, because all it does is give this site a shitty rep and make it totally vulnerable with same old “no test” crap.
“Mental illness” is a truth-obfuscating term. There are plainer and truer words to describe people’s behaviour.
Report comment
“While I maintain that mental illnesses do not exist, I obviously do not imply or mean that the social and psychological occurrences to which this label is attached do not exist.
Like the personal and social troubles that people had in the Middle Ages, contemporary human problems are real enough. It is the labels we give them that concern me, and, having labelled them, what we do about them.
The demonological concept of problems in living gave rise to therapy along theological lines. Today,
a belief in mental illness implies – nay, requires – therapy along medical or psychotherapeutic lines.” -Szasz
Report comment
The brain shrinks over the course of the day, ending up smaller in the evening – before returning to its full size the next morning. That’s according to a neat new study based on an analysis of almost 10,000 MRI scans. It’s published today in Neuroimage.
Kunio Nakamura and colleagues of the Montreal Neurological Institute 06/08/2015
Surely these researchers corrected for this inconvenient Fact.
The Cat….You are correct. No empirical evidence has ever been found, that would allow ADHD to be classified as a Disease or Disorder. Those of us who have worked with ADHD kids know that it is a Behavior Problem…We humans do and say things (behavior) because we receive some benefit from those behaviors, either consciously or unconsciously.
So, what benefit does a ADHD kid get out of “Bad Behavior”? There are two imperatives ingrained in all human minds. 1. To stay alive. 2. to multiply. ADHD has its basis in #1, ‘The fight or flight response’.
Anyone interested in the entire hypothesis, contact the editor. I’d be happy to have it critiqued here on MIA.
Report comment
Here is the catch ceebee, the behaviours that are a problem in ADHD are not voluntary. They do not occur because they are being rewarded. They usually are not even driven by threat in the environment- (though that can worsen them). The behaviours represent escape of behaviours, and that escape will happen pretty much as soon as our back is turned and our awareness focusses on another subject.
We do actually know better, we don’t like them, but it is very hard to suppress them.
Yes- things like hostility in the classroom or home will effect us, as will inadequate physical exercise and too long at the computer– they will affect anyone- but we tend to be the first affected. All this creates considerable stress and worsens the problem, but correcting those will not fix the problem.
We are told to just pay attention and be disciplined- but paying conscious attention is effortful and there are a limited number of things anyone can attend to at one time. What is really going on, as best as I can understand that the routinising of subbehaviours (components of larger behavioural repertoires) has not worked well.
You can take the simple example of clumsiness as a good analogy (and also appropriate given the prevalence of clumsiness in ADHD). If you are clumsy, and trip on things all the time, you have to pay more attention to walking and that limits what other things you can do when walking. The same with typing or handwriting- more effort has to go into the basic act of getting the thought on paper- and that leaves much more chance of losing track of your train of thought.
Report comment
Barliman June 23, 2017 at 2:06 am
Here is the catch ceebee, the behaviours that are a problem in ADHD are not voluntary.(True, they are coming from your subconscious mind). They do not occur because they are being rewarded. (Wrong, you just got an increase in your dopamine level). They usually are not even driven by threat in the environment- (though that can worsen them). ( They are driven by your need to avoid a threat in your environment { the fight or flight response}). The behaviours represent escape of behaviours, and that escape will happen pretty much as soon as our back is turned and our awareness focusses on another subject. (Exactly, your behavior got you what you needed and you are on to other things).
We do actually know better, we don’t like them, but it is very hard to suppress them. ( Of course you know better; ADHD behavior would not work for you unless you had a good sense of ‘right and wrong’).
Please see my comment on the Blog “Researchers Question the Utility of an ADHD Diagnosis”. Cheer-Up! Your Normal.
Chet Bush
Report comment
Thanks for pointing out these discrepancies, some so amusing I laughed out loud, especially the little convenient part about hiding the stuff that didn’t fit. This is my Very Scientific Observation. We have skulls. This is part of the exoskeleton. They grow until we are a certain age. Then, they’re solid. Our brains, which are a bunch of mush, keep growing. It is not possible, not physically possible to have a brain that is so large that it outgrows one’s skull. This means if you have a small-sized skull, as I do, you are doomed to have a small-sized brain. I was assured as a child that even though I was doomed by heredity to be mini, this had no bearing on intelligence nor had any bearing on anything else to do with what I thought about nor my brain’s capacity to do what it had to do. It seems that now, nearly six decades later, my mini-sized brain is functioning just fine. Actually no shrink ever pinpointed a specific “abnormality” in my brain. Perhaps its very existence was offensive to them!
I have also concluded that these MRI-based arguments that we used to hear, as the authors here have pointed out, do not have much validity. The psych establishment only uses them to make intelligent-sounding arguments when they can’t think of anything else to say. The MRI has limited usefulness, except a neurologist might use it to pick up a massive blood clot if it’s obvious enough. It might show torn cartilage in a joint when an xray does not, but I am sure it tells us nothing about the way humans think. In fact, I got a good idea if anyone’s wondering. How about asking the person? Isn’t it cheaper?
Report comment
Hey Julie, my 4″9′ sister would agree with you here 100%!
Report comment
I mentioned elsewhere that this isn’t the first time The Lancet has published erroneous information and refused to retract it. I had a chance to do a quick search and found the issue is actually much larger than I realized. I only mentioned the issue I was personally aware of since it affects me, the publishing of a falsified study which proclaims that Graded Exercise Therapy (GET) and Cognitive Behavioral Therapy (CBT) were proven to be effective treatments for Myalgic Encephalopathy (ME/CFS). In fact, the research which was part of what is referred to as the PACE trails did NOT show ANY patients improving and contrarily most worsened with GET. The findings of the PACE trial were published in The Lancet and have been the basis of the ONLY recommended and approved treatment for patients with ME/CFS worldwide.
Researching the illness on government websites, Wiki, in medical textbooks, an in general turns up this misinformation which is severely detrimental to patients. This has prevented any research dollars being allocated towards the illness which is actually terminal in some patients, let alone any research for hundreds of millions of patients who have been desperate for help and a cure for decades. There are so few specialists and most physicians are so grossly misinformed that they treat the condition as though it is a mental condition. I don’t think I have to explain to most of you how poorly people are treated who are thought to have any sort of mental condition, especially when physicians are convinced that the patient is causing the debilitating symptoms themselves.
I did a quick search this morning on Google as I was sure there must be other controversies associated with The Lancet if the two of these existed. Sure enough, there are a whole string of them which have been going on for decades. Furthermore, it seems that they have previously stated they would publish a retraction but failed to do so. I will continue to hope for your sake as well as the sake of everyone who could be affected by their cavalier attitude and inability to see people as human beings that they do indeed at least print the one tiny little retraction. However, I’m not holding my breath.
Report comment
Excellent analysis thank you, both scientifically detailed and clearly written. So many researchers involved in the article yet such basic errors already acknowledged, and I will be interested to see what conclusions their promised critiques amount to – and whether The Lancet will stand by its supposed reputation and actually publish something to all the media outlets who inadvertently misled so many over this.
Report comment
Garbage like this filters down into families. Abusive members of families will perpetrate further abuses and gaslighting towards their victims, especially if those victims are psychiatrically labelled, using these media reports etc. as food.
Report comment
My mother always had trouble understanding me. But her emotional and verbal abuse didn’t start until after my “severe mental illness” label at age 20. Part of it stemmed from shame that she had brought forth a defective child. Also “scientific experts” told her that my brain was broken, I was hopelessly out of touch with reality, and despite all the “safe and effective treatments” they could offer I would only get worse over time as my “disease” progressed. Somehow this led Mom to believe my thoughts and feelings were unimportant so it didn’t matter how I was treated as long as I got my “meds.” Dad believed brute force was necessary now in his dealings with me. So he took to slapping or cuffing me after my diagnosis.
Thanks a lot Psychiatry! 😛
Report comment
@Feelin:
Not an uncommon story. I too have endured massive harassment and gaslighting from an abusive father (a surgeon) because of being psychiatrically labelled.
He harasses me to the point that it disturbs my mental equilibrium and then uses my agitation as proof of “mental illness”.
The funny thing is, the man himself is a total psychopath, criminally and morally insane, and someone who should be locked up, but he gets away with it because he is a surgeon. You could make out his aberrant behaviours and his psychopathic (and slightly psychotic) nature if you heard some of the recordings I have (which are in a language which you will not understand).
I have spent the last 10 years running around from place to place to escape him, and am also seeking some legal counsel. I cannot even adequately represent myself in a court of law because of this “psychiatric history”, a lot of which was created by abuse.
I was also labelled bipolar because SSRIs prescribed for depression and anxiety caused mania (something which would never have happened without the drugs). The label is also something the man conveniently uses against me.
I have recordings, photographs, so much evidence against him, and it is STILL difficult to get justice. I am hoping something good will come my way soon. Laypeople and even most lawyers cannot understand the depths of psychiatry very well, and such cases require specialised lawyers.
The person who should have been on the end of “treatment” never received it, but I sure did. And this is happening over and over again, the world over.
Report comment
Did your dad ever join NAMI? I’m sure Pete Earley and the NAMI mommies would recognize him as one of them and welcome him with open arms.
The sad thing is, neither of my parents is truly evil. They never would have abused me if Psychiatry hadn’t encouraged this behavior.
Report comment
Leon Eisenberg, Father of (the creation of) ADHD, admitted that he made up the ‘disease’, that it was a real money maker, so, in other words, ADHD is not real and is just another idea based on nothing but a love for money and coming from a bunch of our fellow citizens trained and given appropriate, Government-permitted names such as Psychiatrists, Psychologists, other -ists, to con us all into forgetting about feelings of pain, grief, anger, overly excited, happy, joy/joyful, disgusted, etc., things that every thinking, breathing, feeling creature, whether human or animal, has so that we will be believing in things that are not true and thus, the Thought Docs and their Thought Police will have succeeded in turning us all on each other and ourselves with false ideas which means that they are enjoying knowing that we are all becoming totally deluded/delusional. Oh, how the current-day stealth Nazi Reich has people wrapped around it’s little finger. The Drug Trade, namely Opium and the U.S. Government’s want for people to still use it in whatever form they are serving it up to them and their ability to indoctrinate them all into believing that there is something wrong with their thoughts is astounding.
Report comment
UH OH,
Just a slight problem….Eisenberg is not the ‘Father of ADHD’. Most ADHD ? Scholars ? would give that honor to Dr. George F. Still, who described the condition ‘we now call’ ADHD, 20 years before Eisenberg was born. Please see: adhd-npf.com/history-of-adhd-1902-sir-george/
ADHD is real. ADHD is not a disease or disorder. ADHD has only a ‘pathway’ connection to genetics. ADHD presents differently in Boys than in Girls, for a very good reason. Kid presenting typical ADHD behavior are perfectly normal kids, both mentally and physically. As someone pointed out earlier on this thread, “WE CANNOT SOLVE OUR PROBLEMS WITH THE SAME THINKING WE USED WHEN WE CREATED THEM “.
Albert Einstein
I believe Eisenberg was suffering from Notoriety Disorder, while on his death bed.
Report comment
In the “old days” ADHD was not a problem. Kids only spent 5-6 hours sitting in school. They did physical chores and helped with spring plantings. Originally Summer Vacation was not a vacation–they helped their parents run the farm. Even their play was usually active. And no TV, so no vegging out for 10 hours a day!
Of course Lancet Psychiatry doesn’t recommend healthful stuff like more physical activity, little or no refined sugar, and restricting screen time to 1 hour a day. More $$$$ in drugs!
Report comment
very nice piece, fellows Keep up the good work
Report comment
As with all research we see the biases of the author coming out in statements like “Their data, the authors wrote, confirmed that patients “with ADHD have altered brains; therefore ADHD is a disorder of the brain.””.
In fact ADHD, like all other DSM categories (I believe the term diagnoses is semantically incorrect) consists of a population defined by their common behaviours.
We have plenty of evidence of neuroplastic brain changes, so inevitably a set of commonly repeated behaviours will result in predictable changes in the brain. In making the comment above I believe the authors simply unconsciously expressed the biases inherent in their professional orientation.
There is a great deal of confusion about ADHD, but as I say it is defined as an inherent part of the DSM, and no amount of tinkering with the definitions will make it go away unless we jettison the whole DSM and all the diagnoses. That’s not practical, as all these definitions have clinical utility. My ADHD was finally picked up 9 years ago- at age 45. It would have been helpful to know about it earlier. Though it has not prevented me from working as a doctor, it has caused an awful lot of misunderstanding in interpersonal situations and made work much harder. In adults most of the impulsivity and hyperactivity diminish greatly, but the inattention remains, and causes a great deal of difficulty with mislaying necessary items and being disorganised. These inevitably create the impression that one is an uncaring partner.
The neuropsychologist Leonard Koziol has written extensively on the role of subcortical structures and cognition, including a book called “ADHD as a Model of Brain -Behaviour Relationships” his comments about the diagnosis ADHD are interesting:
First, ADHD is a behaviorally defined diagnosis as it is charac- terized in the DSM system. And in this regard, we com- pletely agree with Carmichael and colleagues’ (this issue) bold statement that from a neuropsychological perspec- tive, ADHD does not exist. There are absolutely no broad-based neuropsychological test batteries that can ever lead to that diagnosis nor is there any ‘‘litmus test’’ for the disorder called ADHD (Koziol, Budding, & Chi- dekel, 2013; Koziol & Stevens, 2012). However, the fact of the matter is that from the behaviorally defined DSM system, ADHD does exist.
and….clinical neuropsycholo- gists are compelled to agree with the proposal that history, observation, and behavioral rating scale data are the primary methods for diagnosing ADHD (Barkley, 2006). In fact, we go a step beyond that viewpoint in stating that these simple behavioral meth- odologies are the only justifiable means for making that diagnosis. This conclusion is based on one simple fact: If a clinician is bound by the DSM system
( “Attention and other constructs:Evolution or Revolution” Koziol et al APPLIED NEUROPSYCHOLOGY: CHILD, 0: 1–9, 2015)
Now while the category ADHD, which is behaviourally defined, is a useful construct as far as it goes, it is also misleading as it focusses attention only on behaviour. It is now becoming accepted that cognition essentially involves the internalisation of movement and developing the skill to execute ever more complex movements- so why is this area not investigated?
It is already well known that there is a significant overlap between dyspraxia, dyslexia and ADHD, but these disorders are separately classified. They should not be because all three disorders share a common neurological basis with problems in the planning and perfection of routine movements (cerebellar), and the routine switching between tasks at will (basal ganglia).
Furthermore, when you look around you will find that therapists dealing with ocular convergence and coordination issues in children use screening questionnaires that actually borrow many of the same questions that would be used to diagnose ADHD. A classic feature of cerebellar issues is difficulty adjusting movement to the requirements of the moment- with a tendency to overshoot or undershoot the target- and that issue is most marked
Additionally the German Orthopedic surgeon Heiner Biedermann (book- Manual Therapy In Children) headed a multidisciplinary team looking at the consequences of birth injuries to the upper cervical spine, (which is common, and becoming commoner as babies get bigger). He found that the injuries tended to persist due to ongoing instability in the upper cervical spine, and the children would develop dyspraxia and dysgnosia (a broader term than dyslexia) as well as common postural issues. He found that these children were effectively behaviourally indistinguishable from other ADHD children, but that early manual therapy was effective in greatly reducing the ADHD symptoms, and usually in ceasing medication.
The association of the upper cervical region is interesting because most of the proprioceptive (body position) information comes from the muscles at the top of the neck, and there is ample evidence that abnormal tension in these muscles can impact on eye coordination and dynamic visual acuity. Biedermann’s book also covers other types of incoordination.
Since my diagnosis I have seen several hundred ADHD adults, and have had the chance to physically assess them. Issues with balance and coordination are virtually universal, and of varying severity. Many ADHD adults have developed mastery in one sport or another, but have frequent injuries, and also have a history of frequently tripping on minor floor irregularities or bumping in to furniture- usually in their home or workplace (where they are less vigilant). A thorough physical examination will almost always reveal mild cerebellar signs, and problems with eye movements. However the signs are more mild than we as doctors are used to looking for in more severe cerebellar disorders.
So the point is that while the label ADHD is useful it is limited by the fact that psychiatrists mostly think about thoughts and cognitive processes. The way this plays out at the moment is that it obscures the real physical issues that are driving the problem.
Stimulants are often helpful, especially when the situation is spiralling out of control, but their effect is not long lasting, and tolerance will inevitably develop.
Addressing the underlying problems is going to be a more permanent solution – good manual therapy to correct underlying postural issues, rehabilitation of the coordination problems ( and I would include specific play therapy like one to one work to improve ball handling skills- which will allow ADHD kids to enjoy sports, as the clumsy ones usually get excluded) and a substantial reduction in the amount of seated time in class, and in front of screens will all help.
Report comment
Barliman,
This is a seemingly neatly and rationally written comment.
But let us cut out the mental masturbation for a moment.
You have written “My ADHD was diagnosed 9 years ago”
How does one get an ADHD label? Let us see some criteria from the Vanderbilt’s scale:
a.)Has difficulty keeping attention on what needs to be done
b.)Does not listen when spoken to directly
c.)Has difficulty organising tasks and activities
d.)Is forgetful in daily activities
And so on, the list goes on.
Practically by “my ADHD was found x years ago”, you mean you had difficulty doing some of these tasks and taking drugs called stimulants helps you.
“I have X behaviours which I find distressing and taking Y drugs helps me” is all it ultimately boils down to in practicality (it is your choice to use drugs in a responsible manner which benefits you and no one should stop you from doing so). There is no need for the “sub-cortical this and that” and yada yada.
Fine, that’s great. Take what you want to and move on with life. No one here has a problem with it.
Telling people that they have broken brains and labelling them for a set of behaviours (which will cause other problems further on), and then telling them that they need to be on drugs for the rest of their life for a set of behaviours in that specific individual is massively dangerous. Not to mention, if those drugs cause side effects (for example mania caused by stimulants) they will be re-labelled with another label like “bipolar disorder” (if the drug indeed does cause mania) and the person will then be someone who has “comorbid ADHD and bipolar disorder”. What then? Next will be imaging for co-morbid “conditions”?
There is too much of “brain brain brain” crap everywhere in psychiatry, which in practice does nothing except imbibe a scientistic view of thinking of everything through the prism of “malfunctioning brain” in people who are so labelled (and also taking away power from their hands with regards to their own lives). And the broken brain messages being pumped into the media make things worse.
In practice, psychiatry is never going to check anyone’s brain for anything.It is nothing more than truth-obfuscation at its finest of what practical psychiatry is like.
The end all and be all is finally “I feel like X1 which is hampering my performance and I want to feel like X2. Taking drug Y may help me go from X1 to X2”.
Report comment
You seem to have missed the whole point of my comment.
I am saying that the ADHD label is a real label describing a discrete problem, that does have distinct features that can be linked to particular areas of the brain.
I do not agree that stimulants are the best solution in most cases. In fact I support the treatment recommended by Biedermann- manual therapy where there is an identifiable suboccipital problem, but I would add physical rehabilitation to address the physical issues like coordination and ocular congergence issues.
Stimulants can help, but not all people benefit from them. The real issue is that psychiatry has got dumbed down to medication only treatments or preoccupied with complex and often unhelpful talk therapy ( I hate to think how much I personally wasted going down that path).
I had intended to follow my previous post up with a comment that the issue with ADHD being a psychiatrist’s diagnosis is that they have a VERY limited repertoire of treatments and they tend to overuse their tiny arsenal of medications when usually non medication approaches are better.
The problems caused by unreliable attention have actually been the subject of discussion for some millenia, and if you look carefully you will see that what the Buddha said boils down to “suffering occurs because of inadequate attention (to the nature of reality).
I have highlighted the common issues with coordination and also the fact that these link well to predictable brain areas. If you cannot understand the subcortical (and therefore utterly unconscious) nature of ADHD symptoms it is difficult to offer any useful advice to us which does not sound like more of the same abusive nonsense tht we have been subjected to since we entered school.
However having an understanding of the nature of the problem in brain terms actually points to better solutions:
We have clear evidence of the value of meditation in reducing anxiety and stress, and good evidence of brain changes that correlate to that activity. If we broaden our view a little, some other meditative practices like Tai Chi (which involves slow and precise movements repeated until they are perfect and the underlying posture is also perfect) are working on the areas of the brain which are not working so well.
This sort of knowledge is empowering- not disempowering.
The latest material linking brain areas with particular problems is extremely useful, but it is not the last word. My own position is far from the “Scientism” point of view (which I am utterly at odds with) that the brain is the seat of consciousness. We have more than enough material from near death experience studies to support the continuation of consciousness after the cessation of neural activity.
However ADHD is a behavioural disorder, and all behaviour is expressed through the nervous system, so the nervous system is of interest to those keen to deal with the problem, rather than just take positions.
Report comment
Of course, the ADHD label is real and the behaviours that it encompasses like not being attentive etc. are real.
“I am saying that the ADHD label is a real label describing a discrete problem, that does have distinct features that can be linked to particular areas of the brain.”
Then why can a psychiatrist not do a brain scan in a specific individual (not statistical studies) in clinical practice to prove this so-called “discrete” problem. After all, if it is so discrete (like a hematoma in the brain), one does not need checklists. Do a scan, end of story.
There are long timers in psychiatry who end up with 10 labels. For example, one individual will have the labels of “schizophrenia, borderline personality, OCD, bipolar disorder, schizoaffective disorder, panic disorder, ADHD” etc.
These individuals have all these “discrete problems” in one brain?
Since there is no mind without a brain, even “Internet Gaming Disorder” (which is also a real label describing a real problem) will have neural correlates. So what?
Report comment
Yes. I was “schizoaffective” till a doctor changed me to “bipolar 2.” At the time I didn’t realize how weird this was. How can a doctor–however smart and educated with X years of experience–transform one disease to another at the stroke of a pen?
“Dr. Smith diagnosed you with walking pneumonia, but I think I’ll change it to—oh, the mumps instead.”
“An illness like any other” my foot!
Judging from the behavior of Creepy Pete and the NAMI mommies, even they don’t buy into the bovine excrement they foist upon the gullible public.
Report comment
Yes. The more number of psychiatrists you come in contact with, the more labels you get, which is something people do not realise or know until it is too late.
Report comment
You can’t do a scan in an individual to come up with a specific label because the labels are based on clusters of behaviours.
So a syndrome like ADHD is always going to be heterogenous and there will be great variations between individuals.
However, as I said, finding neural correlates is important and helpful as it allows us to tailor interventions down to specific rehab exercises, and that decreases the need for medications.
Plenty of kids with ADHD grow out of it for many years, but the underlying problems do tend to crop up again in middle age, as we age, and as we are forced to work in sedentary positions Not only that but they also show up in other ways- like a chronically overactivated stress syndrome, and as chronic pain as the body takes more and more wear and tear from one’s clumsiness.
I can only agree that the use of labels in psychiatry is often clumsy and over -rapid, but that does not mean the labels are useless.
Report comment
You say it is a heterogeneous problem, but at the same time you also say it is discrete and specific. Which is it?
You’re right, the labels aren’t useless. They have great use in truth obfuscation and making already vulnerable people doubly endangered (which is not, in some eyes, their intended use, but those intentions don’t matter at all).
Doesn’t matter if the labelling is rapid or done over 20 years. Once done, and once a person has 10 labels, he is left with little standing as a person.
If only we could put psychiatrists on the other end of
the same practices.
“You can’t do a scan in an individual to come up with a specific label because the labels are based on clusters of behaviours. So a syndrome like ADHD is always going to be heterogenous and there will be great variations between individuals.”
Which is also my point. It is a rewording of behaviour.
“finding neural correlates is important and helpful as it allows us to tailor interventions down to specific rehab exercises”
Interesting. Tell me a few rehab exercises which have been based on scans in clinical practice.
Report comment
I think the problem is that while the behaviors so labeled do exist, there is no reason at all to believe that all people so labeled have anything wrong with them at all, or have the same problem if they do have something wrong. The DSM itself admits this in its introduction, saying that, it is not assumed “that all people having the same diagnosis are alike in all important ways.” So what’s the point of labeling something based solely on external observations when the group so labeled is completely heterogeneous? It’s like saying that everyone with a skin rash has the same problem. Some of them have poison ivy, some have prickly heat, some have the measles, some have syphilis. Might be a good idea to figure out which one the person has before you start treatment, eh?
Not to mention, a lot of kids labeled “ADHD” have nothing wrong with them at all. A number of studies have replicated the finding that admitting a child to school one year later reduces the “ADHD” diagnosis rate by 30% or more! So while there may be a small number of “ADHD”-diagnosed kids and adults who actually have something biologically wrong with them, there is no way to distinguish these from those kids who are simply bored or who have a naturally active personality and don’t like to sit still or who don’t get enough sleep at night or who have low iron or whose parents are violent or whose parents are neglectful or lack parenting skills. Calling all such cases “ADHD” simply creates confusion and prevents us looking into what might really be causing these subjective “symptoms.”
— Steve
Report comment
Steve, how many times have the studies regarding age at diagnosis been replicated?
I do agree that there is a real issue with kids going to school too early and spending too much time seated doing work that they could compete in 1/4 of the time if they did it a year later.
Equally, the structure of DSM is not powered to identify causes. I’m sure that a significant group of the kids who experienced many adverse childhood events would be classifiable as having ADHD if they were fully assessed.
I remember a paediatrician commenting that an ADHD diagnosis should be the start of investigation- not the end.
Report comment
I’m sure that a significant group of the kids who experienced many adverse childhood events would be classifiable as having ADHD if they were fully assessed.
And what will then happen? The people who caused those adverse events will use the label to claim that the “adverse events” and the kid’s agitation are due to a brain disorder in the kid. It happens all the time. This site is replete with those cases. And neither psychiatry/psychiatrists, nor the law will be able to truly help those kids from being re-abused (but will, in fact, unintentionally retraumatise the individual).
“Having” “ADHD”, “having” “bipolar disorder” is just a quasi-medical rewording of things like not being able to focus, being depressed etc.
It is simpler and more importantly, truer, to avoid truth-obfuscating labels and call things what they are.
“I remember a paediatrician commenting that an ADHD diagnosis should be the start of investigation- not the end.”
And how will that help, when the label screws over the kid and makes him susceptible to even more labelling?
As I have already said (your notions on rehab and little use of medication are another thing), everyday, many of those kids are being prescribed stimulants (which if the kid benefits from, is fine), which in a subset of kids will cause mania, which will be used as “proof” of a “latent bipolar disorder”. The “start” of the investigation will be ADHD, and the end will be “co-morbid ADHD and bipolar disorder”.
Report comment
I know of at least three different studies from different locations – one in Kentucky, one in Canada, and I can’t recall the third. All found the same result. I think there were even a couple more that someone else talked about, but I didn’t read them. They looked at kids just before the age cutoff for admission and those who were just after the age cutoff, and so started almost a year later. All three reported something around 30-33% reductions in diagnosis rate.
Some related links from a one-time google:
http://www.inquisitr.com/2512234/delayed-kindergarten-enrollment-reduces-adhd-in-children/
http://www.medicalnewstoday.com/articles/307678.php
Looks like Australia is the third:
http://www.metronews.ca/life/health/2017/01/23/youngest-kids-more-likely-to-be-medicated-for-adhd-study.html
Report comment
And the DSM admits it’s not powered up to designate causes, but it’s used as if it is. Most of the folks I know who went to psychiatrists (and I worked 20 years with foster kids, so I have known A LOT!) say that the psychiatrist told them they have an imbalance of brain chemicals that causes their difficulties. It is not the beginning of an investigation – it is THE END.
Again, there is no point to “diagnosing” someone with something where those with multiple causes are lumped together based on external observation alone. It only adds confusion. Syphilis is a diagnosis. A rash is a sign. If ADHD is the start of investigation, it’s a sign, not a diagnosis, just like a rash.
—- Steve
Report comment
According to Barliman the DSM is not used for finding causes. Good point! All it’s “diagnoses” are lists of symptoms grouped into clusters which are voted on by elite psychiatric professionals. Since they deal with various behaviors as symptoms, they really aren’t diseases at all but bad habits or even quirks some find annoying or odd but are harmless.
My bad thyroid causes me to experience long term sadness (depression.) Since the thyroid is at the root of the problem the diagnosis that will help is one of hypothyroidism not clinical depression or bipolar 2.
If ADHD is a bunch of symptoms with many causes, then ADHD really is not a diagnosis at all and has no business in any medical manual. You don’t find Itching in any diagnostic manual. Or Chronic Sniffles. If you have those problems seeing a doctor is a good idea, but a diagnosis should be based on the pathology responsible for the problem and not just a reiteration of the symptoms already described by the patient.
Report comment
Steve,
thanks for the links- I was only aware of the Australian one- and there are questions about the independence of one of the people involved in it. I will look into them.
It disturbs me that so few practitioners are aware of the nature of DSM. All you have to do is read the introduction– but it seems that that is rarely done.
The “chemical imbalance’ model is just nuts ( unless you are talking about depression due to hypothyroidism or some such problem). The proponents of that model can never account for the fact that these neurotransmitters subserve multiple functions in many parts of the brain, and that in most cases chemical therapies are “shotgun treatment”. In that regard I suspect that the stimulants are the most pathway specific medications, as the dopaminergic pathways are quite limited in the brain.
I do think that there is value in making the syndromal diagnosis- simply because it predicts a lot of the sort of problems that the individual will experience. In particular people with ADHD are being told they are being wilfully lazy, and to just try harder. That sort of help usually makes the problem worse and it betrays a fundamental misunderstanding of the nature of the problem.
Report comment
The studies you mentioned lead to an interesting conclusion:
If the rate of ADHD diagnosis is related to age of entry to school, and ADHD is being conceived as a neurodevelopmental problem, then this logically suggests that school is not a good environment for the development of young children. That seems like a logical conclusion to me.
Report comment
Hi all, my immediate impression having looked at the methodology, subject selection and stats is a very unprofessional ‘usual Lancet rubbish’. I must disclose that I have fallen out with both editors of the Lancet and BMJ about overdramatising findings to gain readership and maintain their high impact factors, as exemplified by the MMR (Lancet) and Statin (BMJ) stories. I did suggest to the 2 that next time I would complain to the Press Complaints Commission. They also got upset with me as I suggested that critical analysis of their papers was better in the Daily Mail (whose health editor is very good). I would stick to the Nature journals, and NEJM.
On the study specifics, this was a brave attempt to get big numbers, but with all the attendant problems of an international multicentre study, which have been described in before (I was involved in the Intercept study on the suicide protection potential of Clozapine in psychosis). A snapshot process of subjects of a large variety of ages, will come up with overlap between subject / control findings, all very predictable. I think they were hoping to get separation in basal ganglia areas but couldn’t, so focussed on the hippocampal / amygdala changes instead. They forgot to mention that the Hippocampus and Amygdala are the most plastic of brain organs, readily reducing in volume in response to persistent high stress and Hypercortisolaemia (caused by all kinds of conditions, both physical and mental adversity, including mixed abuse by elders).
The IQ difference between subjects and controls is interesting, I am sure the authors are regretting not controlling for this in their initial subject selection, as it totally moves the focus to this statistically more robust finding. I was pleased to find that ADHD drugs did not seem to make a blind bit of difference, and is used simply for sedation and school room control, and might explain hippocampal / amygdala loss due to these children struggling to use their preferred way of learning, and getting stigmatised by teachers and peers. School would be a horrible experience for them (need a good naturalistic study on this I think).
Finally the authors provide their own criticism; the need to concentrate on longitudinal structural imaging to look at brain maturation in these different conditions. This is best done at a single centre, and needs much smaller, but carefully selected group of subjects and controls. However, there are ethical issues involved in annual MRI screening, including confounding study results. This is being done by NIH in early onset psychosis.
Ethically, my fear is how politicians and the general public would interpret the finding of ‘smaller brains in ADHD’ This has the (sickly) smell of Eugenics and Social Darwinism, with the potential to reduce reasonable adjustments to help these children learn in their preferred way. Also, when selecting for apprentice schemes and jobs, could a diagnosis of ADHD based on MRI scans limit success in employment, limit driving licences being given? What happened in Germany in the late 1920’s (A life not worth of life) is not that long ago.
Shola
Report comment
Also, the more basic question (forwarded by eugenicists and social Darwinists); can you assume that smaller brains or part of brains imply less competent social, occupational and spiritual competency?
Current neuroscience understanding is that the more important bit is interneuron connectivity, especially between distant regions of the brain, both frontal to more posterior (sp. occipital, cerebellar) and inter hemispheric. This is not directly connected with volume, and is more associated with white matter integrity (which is why serious imaging researchers are concentrating on DTI imaging in psychiatric conditions).
I think comparing brain volume is a bit like what we (as naughty boys in the wee room) did in nursery and primary school. At least when we moved to year 2, compared how far the wee went, a much better measure of function, but equally questionable without looking at long term outcome in terms of prostatic enlargement in late life. Sorry to bring the tone of this discussion down to my usual (Geordie) standards, but it is so very silly.
Shola
Report comment
Better now than never.
What’s up with confusion about IQ scores? Were really mistakenly switched? If so, that control group has really higher IQ, why they didn’t expose this fact? In this view ADHD means not only smaller brain but also lower IQ? Did I miss something?
Report comment
In the end these brain volume issues really apply only to small and quite specific areas. They really are visible evidence of different ways of processing information (which may be maladaptive).
The real trouble is that because ADHD is defined by psychiatrists they take arather limited view of it- neglecting the physical signs which should by all irghts be identifiable in a neurological condition. Things are less backward in Europe though:
A Swedish study:
http://onlinelibrary.wiley.com/doi/10.1111/j.1469-8749.2009.03407.x/full
“Reliability and validity of the assessment of neurological soft-signs in children with and without attention-deficit–hyperactivity disorder”
Additionally we are getting stronger and stronger evidence of problems like oculomotor problems – which are stimulant responsive:
https://www.ncbi.nlm.nih.gov/m/pubmed/12672781/?i=4&from=/24691355/related
Altered control of visual fixation and saccadic eye movements in attention-deficit hyperactivity disorder.
Oculomotor Abnormalities in Children with Attention-Deficit/Hyperactivity Disorder Are Improved by Methylphenidate.
Bucci MP, et al. J Child Adolesc Psychopharmacol. 2017.
https://www.ncbi.nlm.nih.gov/m/pubmed/28452866/?i=1&from=dopamine%2C+fatigue%2C+oculomotor%2C+exercise
Which is:
Effects of Dopamine and Norepinephrine on Exercise-induced Oculomotor Fatigue.
So lets think about this- attending with the eyes (reading) is a major part of the disability in ADHD,
it is correlated with ocuomotor deficiencies that are improved with stimulants
The same set of problems can be demonstrated in athletes who are exercised past their fatiguing point.
So we have a plausible mechanism for oculomotor symptoms as a cause of ADHD symptoms, we know that they are ameliorated by stimulants. We also know that at least in the earl stages of treatment they substantially improve attention and learning (until you learn too much, read too much and exacerbate the problem.
If we take this a little further we see that behavioural optometrists use a questionnaire that asks many questions that overlap with ADHD questions.
Now these oculomotor problems are treatable by behavioural optometrists and by people who specialise in neurological rehabilitation/ functional neurology, most of whom are highly trained chiropractors.
I have discussed the issue with one of them (when I was seeing him for treatment for my ADHD/Oculomotor issues [now almost full settled]) and he agreed with my reasoning that given the serious oculomotor fatigue and problems with training in bad habits during neuro-rehabilitation, the use ofsimulants then may be indicated.
That’s pleasing really- hitting relevant mechanisms, and aiming to minimise duration of treatment.
however, I do not think there is any sense in denying the problem exists, and zi think there is no sense at all in labelling a condition as a neurobehavioural condition without doing a proper physical examination. This approach is rare in psychiatry though.
Report comment
“Among patients with ADHD, rates of criminality were lower during periods when they were receiving ADHD medication.”1(p2006) Among 25,656 patients with ADHD, pharmacotherapy for the disorder reduced criminality by 32% for men and by 41% for women.”
There was no place to respond to the contention that ADHD meds do no good over the long run.
Report comment
https://news.fiu.edu/2022/adhd-medication-alone-doesnt-improve-classroom-learning-for-children-newresearch
From James Swanson, et al, who is a proponent of the use of stimulants for “ADHD.” This is a review of ALL reviews to date (in 1993) and so is a compilation of ALL research to that date, not just one study:
What Should Not Be Expected
1. Paradoxical Response
a. Responses of normal children are in same directions
b. Responses of normal adults are in same directions
c. Responses of affected adults and children are similar
2. Prediction of Response
a. Not by neurological signs
b. Not by physiological measures
c. Not by biochemical markers
3. Absence of Side Effects
a. Infrequent appearance or increase in tics
b. Frequent problems with eating and sleeping
c. Possible psychological effects on cognition and attribution
4. Large Effects on Skills or Higher Order Processes
a. No significant improvement of reading skills
b. No significant improvement of athletic or game skills
c. No significant improvement of positive social skills
d. Improvement on learning/achievement less than improvement in behavior/attention
5. Improvement in Long-Term Adjustment
a. No improvement in academic achievement
b. No reduction in antisocial behavior or arrest rate
https://escholarship.org/content/qt4jr2777t/qt4jr2777t.pdf
“In the short term, stimulant medication is effective in reducing the symptoms of ADHD and appears well tolerated with relatively minor side effects. In the long term, much of the benefit of stimulant medication disappears after medication is ceased. Studies have demonstrated only marginal improvements in adult outcomes following a period of treatment in childhood.”
https://pubmed.ncbi.nlm.nih.gov/16623654/
There are also the RAINE study in Australia, the Quebec ADHD study, the long-term data from the MTA study in the US, and a comparison study between Finnish and US “ADHD”-diagnosed children showing that there were little to no differences between groups, despite the Finnish group using far less stimulant treatment. And the OSU medication effectiveness study, though somehow the original reports on long-term outcomes don’t seem to be available any longer.
I’m afraid the jury is in on this point – there is no general long-term benefit to stimulant treatment of any significance. One can certainly find individual studies that claim these effects, but large reviews of huge amounts of data show no real benefit of mass treatment of “ADHD” with stimulants. This of course doesn’t mean that some individuals are not positively affected, perhaps in very significant ways, but as a group, stimulants have not proven to improve long-term outcomes for “ADHD.”
Report comment