
On August 26, VICE NEWS published a long article titled “The Movement Against Psychiatry.” The piece featured interviews with many people familiar to Mad in America readers, and Mad in America—this webzine—was also featured in the article, albeit at times in distinctly unflattering ways. The criticism of my book Anatomy of an Epidemic was something else altogether: it was an arrow aimed at the heart of all that we do.
Criticism is nothing new to Mad in America, and personally I have had my fair share of it. And while it is often best just to shrug it off—after all, if you challenge a conventional narrative in society that brings prestige to a medical guild and billions in profits to pharmaceutical companies, you can expect slings and arrows to come your way—in this instance deconstructing the article and responding to the criticisms provides an opportunity that shouldn’t be passed up.
Although Vice may not be “mainstream media,” it is a publishing venture that has gained a growing readership, particularly among younger adults, in the past few years. This article was also one of the first to report on the growing effort in American society to challenge the conventional narrative that psychiatry has told over the past 40 years. Thus, the article is of some importance in terms of societal understanding of this “movement against psychiatry.”
The article provides a three-fold opportunity. First, it provides us at Mad in America with a reason to set forth a clear explanation of our mission and why we do what we do. Readers of Mad in America may not have a good understanding of this, and without that understanding, it limits the impact we can have on this discussion regarding the merits of psychiatric care today.
Second, it provides us with an opportunity to publicly answer a criticism that defenders of the conventional narrative regularly make about me as the author of Anatomy of an Epidemic, and, to a lesser extent, a criticism of the Mad in America website. The criticism is that we distort the scientific record, and thus, our “critique” of the conventional narrative is an intellectually dishonest one. Vice aired this criticism the instant it introduced us into the article, and then sought to provide examples of this “distortion.”
Thus, by examining those “examples,” it becomes possible for readers, in their own minds, to assess the merits of this criticism. If the Vice article provides evidence of a distortion of science in Anatomy of an Epidemic, and evidence that Mad in America commits the same sin in its coverage of scientific findings, then I think it would be best if we shut down Mad in America tomorrow. We would be doing harm.
However, if a close reading of this article reveals the opposite, that in fact the criticisms are of a hollow kind, and that the examples cited in fact reveal an effort by defenders of the conventional narrative to explain away findings that belie their narrative, then the rebels—those said to be part of a “movement against psychiatry”—can take heart. They will know, more clearly than before, that science is on their side.
Third, it provides an opportunity to see how the media itself, in its reporting on psychiatry and its treatments, is resistant to challenging the conventional narrative.
The Vice article was presented as an exploration of the “movement against psychiatry,” and yet you can see, once it is deconstructed, how it told a story that surely pleased the promoters of the conventional narrative, and put the “critics” on the defensive at almost every turn.
Understanding Mad in America
As I have often written, I began this long journey of writing about psychiatry as a believer in the conventional narrative. The first time I wrote anything of note about psychiatry was in 1998, when I co-wrote a series for the Boston Globe on abuses of psychiatric patients in research settings.
One part of the series focused on studies that involved withdrawing schizophrenia patients from antipsychotics, which we said was “unethical.” My understanding at that time was that antipsychotics fixed a dopamine imbalance in the brain. They were—and this is what psychiatrists I interviewed for the series regularly said—“like insulin for diabetes.”
That was a metaphor that told of great medical progress. Researchers had come to understand the “pathology” of schizophrenia, with drugs now available that were an antidote to that pathology. However, while reporting that story I came upon two studies that belied that story of progress, and ultimately this is what motivated me to continue writing about psychiatry and its treatments.
One was a study by Harvard researchers that found that long-term outcomes for schizophrenia patients had declined in the past 20 years, and that recovery rates were now no better than they had been in the first third of the 20th century. The other was a finding by the World Health Organization that outcomes for schizophrenia patients were much better in three “developing countries” than in the U.S. and six other developed countries.
In addition, I had interviewed David Oaks from MindFreedom for that series, expecting to get a quote from him about how awful it was that researchers had conducted studies that involved withdrawing antipsychotics, and instead he told me how many people heartily disliked the drugs and found them extremely debilitating. Oaks challenged me: investigate what the drugs do to us, he said.
That was what led me to write Mad in America, which was published in 2002. And that was a book that broke with the conventional narrative that psychiatry told about its drug treatments.
In the conventional narrative, treatments before the arrival of antipsychotics in asylum medicine in 1955 are often depicted as unhelpful or even barbaric. But then, or so the narrative goes, chlorpromazine arrives and this drug kicks off a “psychopharmacological revolution,” a great advance in care. Chlorpromazine is deemed an “antipsychotic,” a name that tells of how it was a specific antidote to psychosis.
But while researching Mad in America, I found a much different story in the research literature. When chlorpromazine was introduced, it was described as a “neuroleptic,” meaning it “took hold of the nervous system,” and praised for causing a “chemical lobotomy,” a change in being similar to that caused by surgical lobotomy (which at that time was still seen as a positive comparison). Chlorpromazine and other first-generation drugs of this type powerfully blocked dopamine receptors in the brain and thus induced a deficit in the dopaminergic system similar to what is found in Parkinson’s disease. As for their long-term effect on psychotic symptoms, in the 1970s researchers worried that antipsychotics induced brain changes that made patients more biologically vulnerable to psychosis. Several studies found that many patients developed a severe, chronic psychosis after taking the drugs for a longer period of time. As for the World Health Organization studies that had first triggered my curiosity, the best outcomes were in developing countries where only a small percentage of patients—16%—were maintained long-term on antipsychotic drugs.
In this narrative, the conventional story of “medical progress” disappears. At the same time, Mad in America told of how the voices of those who were treated needed to be listened to. The “ex-patients” told of truths that were not found in the conventional narrative of progress.
In Anatomy of an Epidemic, I once again began with a question. After Prozac was introduced in 1987, our societal use of psychiatric drugs exploded. The newer psychiatric drugs were said to fix chemical imbalances in the brain, and if that were true, then one might expect that the “burden” of mental illness in our society would have gone down since then. Instead, all the public health data told of the opposite happening, and as a marker of that burden, I reported on the rise in the number of adults receiving disability payments due to mental illness. Thus I posed a question: how do psychiatric drugs affect outcomes in the long-term? What does the research literature show?
That is a question that arises from within a “medical model” conception of a “disease.” Is the treatment for that disease “effective” over the long term?
As I sought to answer that question, I first investigated the chemical imbalance story. This was a hypothesis that arose in the 1960s once researchers discovered how antipsychotics and antidepressants acted on the brain. Antipsychotics blocked dopamine receptors; perhaps psychosis was due to too much dopamine in the brain. Antidepressants increased serotonergic activity; perhaps depression was due to too little serotonin. However, years of research then failed to find that people diagnosed with schizophrenia or depression suffered from a chemical imbalance that was then fixed, in some fashion, by the drugs. You could find that admission in psychiatry’s own literature, with the American Psychiatric Association’s 1998 textbook telling of how the low-serotonin theory of depression had not panned out.
The question of the long-term effects of psychiatric drugs needs to be framed in this way: Does their long-term use produce superior outcomes to the “natural course” of the disorder? And when you dig deep into the scientific literature, you find a mix of various kinds of evidence, stretching across 50 years, that psychiatric drugs, on the whole, increase the likelihood that people will remain symptomatic over the long-term and become functionally impaired. This called for a rethinking of the use of these drugs.
That was the counter-narrative of science that was told in Anatomy of an Epidemic, and in the last part of that book I told of the financial and guild influences that had led psychiatry, as an institution, to tell its story of great medical progress, even while its own science was telling a very different story.
Madinamerica.com, our webzine, was born from that book. And the basic understanding was this: Our society had organized itself around a false narrative, and that doing so had led to great harm. This of course was true for many other societies as well. Our website has sought to be a forum for developing a new narrative to guide a society’s thinking and care.
From the beginning, we have tried to do so in three ways:
- Reporting on research findings. The pharmaceutical industry and psychiatry regularly promote research findings to the media that support the conventional narrative (and the results are often promoted in ways that exaggerate what was found). Research that belies that conventional narrative rarely makes it into the mainstream media. We have sought to fill in the gap, with daily reports of research findings that the public rarely hears about, yet tell a very different story about the merits of our current paradigm of care. It’s an effort designed to help our society create a new narrative that is informed by that full record of research, as opposed to the selective record of research that appears in the mainstream media and is tailored to serve guild and financial interests.
- Personal stories. Good medical practice relies on listening to patients. Those who are treated with a drug can tell of adverse effects they may be experiencing, whether the drug is working for them, and in a larger sense, whether they are finding a treatment helpful. Yet, psychiatry, as it has developed its “evidence base” for its treatments, has regularly dismissed feedback from its patients, and that is particularly true for those diagnosed with psychotic disorders. We publish personal stories so that the voices of those with lived experience can be heard, and be part of any societal “rethinking” of psychiatry.
- Blogs. While MIA’s mission is to serve as a forum for creating a new paradigm of care, we do not set forth our ideas of what we think that paradigm should be. We think that there needs to be a societal discussion of that topic, one informed by research and personal stories, and we publish blogs from a diverse group of international writers who, for the most part, share a belief that our current paradigm of care needs to be rethought.
I have detailed the roots of this webzine, and what we strive to do, in order to make clear that our critique of the conventional narrative does not derive from any “antipsychiatry” ideology, but rather from pro “good medicine” values. A society needs to organize its psychiatric care around an understanding of what science is revealing about the validity of psychiatric diagnoses and the merits of psychiatric treatments, and not around a story that, while it serves guild and financial interests, is out of sync with psychiatry’s own scientific findings.
The Vice Interview
Although readers of the Vice article may conclude that Vice interviewed me about MIA and its operations, that isn’t so. The reporter, Shayla Love, emailed me on August 18, a week before the piece was published, to tell me that she was finishing up a “feature article about antipsychiatry and critical psychiatry,” and she wanted to know, as soon as possible, if I cared to respond to three criticisms of MIA and me that she was planning to publish.
- That in Anatomy of an Epidemic, I “misinterpreted, misunderstood studies, and that for each of the studies included in the book, there are many others that come to the opposite conclusion, but are not included.”
- That “Mad in America doesn’t provide substantive policy recommendations for the improvement of psychiatric care.”
- That Mad in America highlights research that “negatively portrays diagnoses or treatments, but not dedicate space to research that finds the opposite.”
There was no questioning of what MIA does, or what our mission is. I responded in an email to Love that it would be nice if she would interview us about what we did, as otherwise it seemed like this piece was going to be a “bit of a hit job.” I then answered the criticisms in this way:
- I told her we weren’t an antipsychiatry website, but rather that we were better described as a “critical psychiatry” website.
- I said our coverage of research in Mad in America was designed, among other things, to tell of research findings that challenge or belie the conventional narrative, but “which are virtually never aired in the mainstream public.”
- I said that making policy recommendations is a function of policymakers, not journalists, but noted that on our website we have told “of innovative programs that are achieving good results and are exploring alternative paradigms of care. That is the journalistic function; not to recommend, but to highlight—and make known—these efforts.”
Finally, in response to the accusation that I misinterpreted studies in Anatomy of an Epidemic, and left out studies that came to an opposite conclusion, I said this: “There is a simple way to put this criticism to the test. If there are indeed studies that are misinterpreted, then this [critic of Anatomy] should say which studies she is talking about. Or if there are others that come to the opposite conclusion, this person can cite what those studies are . . . If this isn’t done, this is just idle criticism, which is really pretty slanderous.”
Love wrote back a few hours later. There were two studies that psychiatrist Joseph Pierre said I had misinterpreted. The first was a study of long-term outcomes of psychotic patients by Martin Harrow, and the second a study by Lex Wunderink on this same topic.
This perked up my interest. There is no study that belies the conventional narrative more than Harrow’s, with Wunderink’s a complement to his findings. If Love would actually investigate those results, this article could really stun readers.
In response, I told her she could easily determine whether the criticism of me had merit. She could read what I wrote about Harrow’s study in Anatomy of an Epidemic and Wunderink’s on Mad in America, and see if I had misreported those studies in any way. Better yet, I urged her to call Martin Harrow or his co-investigator Thomas Jobe to “see if they think I misinterpreted or misunderstood their study.”
That would be an easy way that she, as a journalist, could search for the truth. Yet, given that she hadn’t agreed to interview me, I feared the worst.
“If you air this criticism of Pierre’s without checking if it is accurate, I’ll be extremely unhappy,” I wrote.” I’ve seen this time and again, and it’s bad journalism. You need to see if his critique of me—which is saying I am a shitty journalist—has actual merit. Please call Jobe, and read what I actually wrote.”
Understanding Harrow (and Wunderink)
The criticism that Pierre had raised, with its focus on Harrow, is the same criticism that E. Fuller Torrey and others voiced when Anatomy of an Epidemic was published. And there is a reason that Torrey and others have done so.
Harrow’s study is, by far, the best and most rigorous assessment of the long-term outcomes of patients diagnosed with psychotic disorders since the arrival of chlorpromazine in asylum medicine, and his results—unless they can be explained away—tell of a paradigm of care that does harm. Criticizing me for misinterpreting the study is an effort to do just that, to explain away the results.
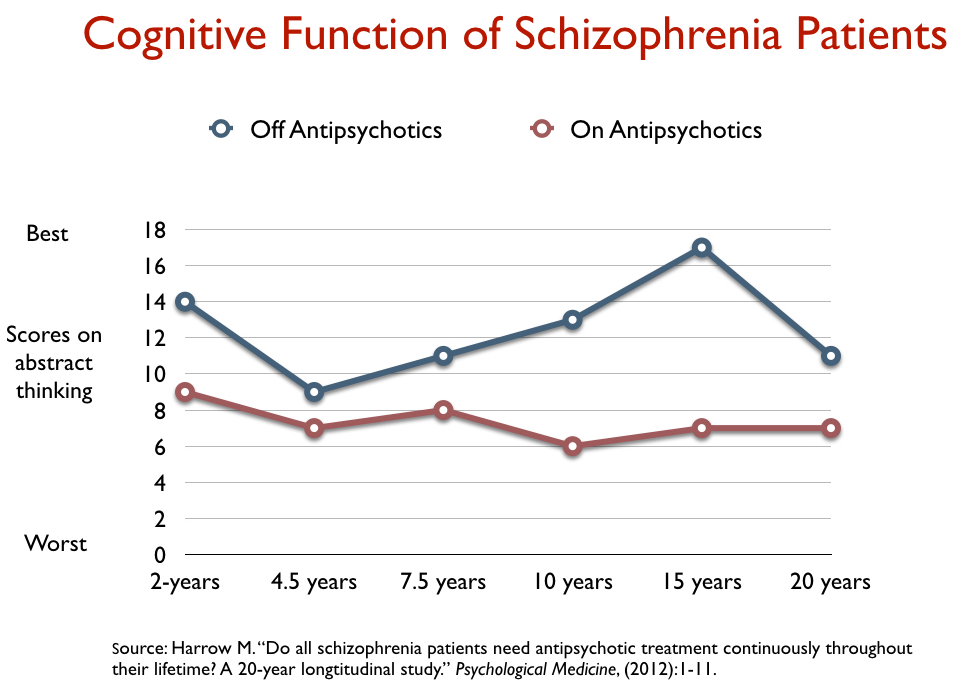
Beginning in the late 1970s, Harrow and Thomas Jobe recruited 200 psychotic patients into their studies, recruiting them from two Chicago area hospitals (one public and one private.) All were treated conventionally in the hospital with antipsychotics, and after they were discharged, Harrow and Jobe periodically assessed how they were faring (at 2 years, 4.5 years, 7.5 years, and so forth, with their follow-ups eventually spanning 20 years.) At each follow-up, they assessed the status of their psychotic symptoms, their social functioning, whether they were working, and their use of antipsychotic medication.
At the start of the study, the average age of the patients was 22.9 years, with 46% experiencing a first hospitalization, and another 21% a second hospitalization. Thus, this study mostly followed a cohort that was newly diagnosed or from a time early in the course of their treatment. At the end of 15 years, Harrow and Jobe still had 145 patients in their study, 64 who were diagnosed with schizophrenia and 81 with milder psychotic disorders.
They found that the recovery rate, at the 15-year mark, for the schizophrenia patients off medication was eight times higher than for those who were medication compliant. This was the outcome that threatened to rock the grand narrative of progress:
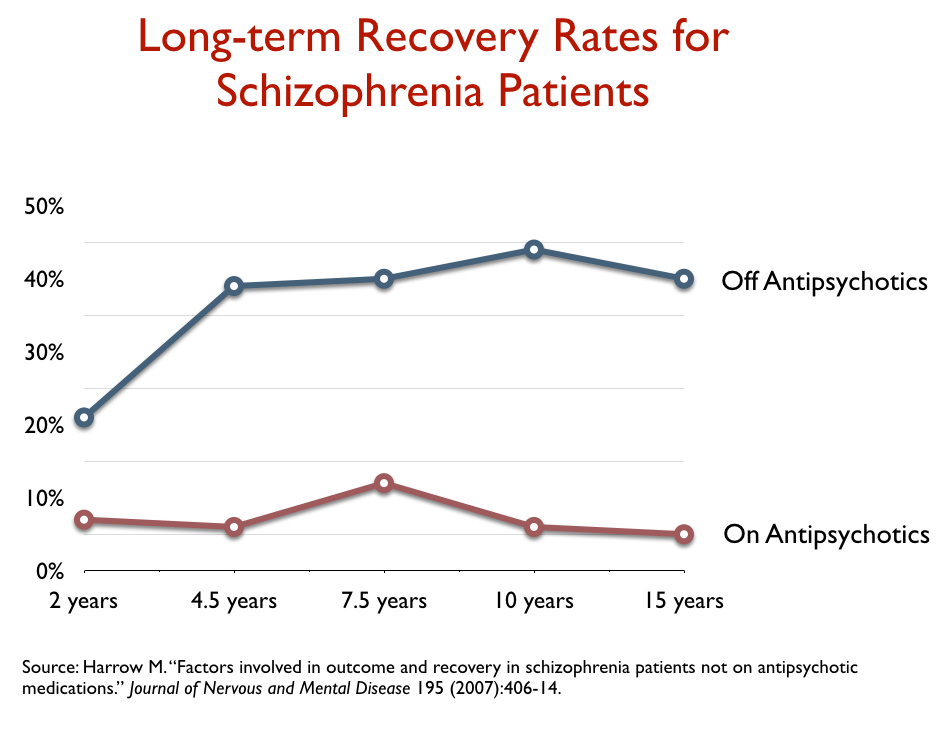
However, in their 2007 report on 15-year outcomes, Harrow and Jobe wrote that it wasn’t that the drugs had caused the bad outcomes, but rather that it was those with a good prognosis who were more likely to go off the drugs, and that could explain the difference in recovery rates. I reported on that explanation, which did spare the drugs of any blame, in Anatomy of an Epidemic (pages 116-118).
Yet, I saw in their reports findings that belied that explanation. They also reported outcomes for those with milder psychotic disorders, and if you created an outcomes chart for all of the patients in the study, it showed that those with milder psychotic disorders at baseline who stayed on antipsychotics had worse long-term outcomes than those with schizophrenia who got off the medications.
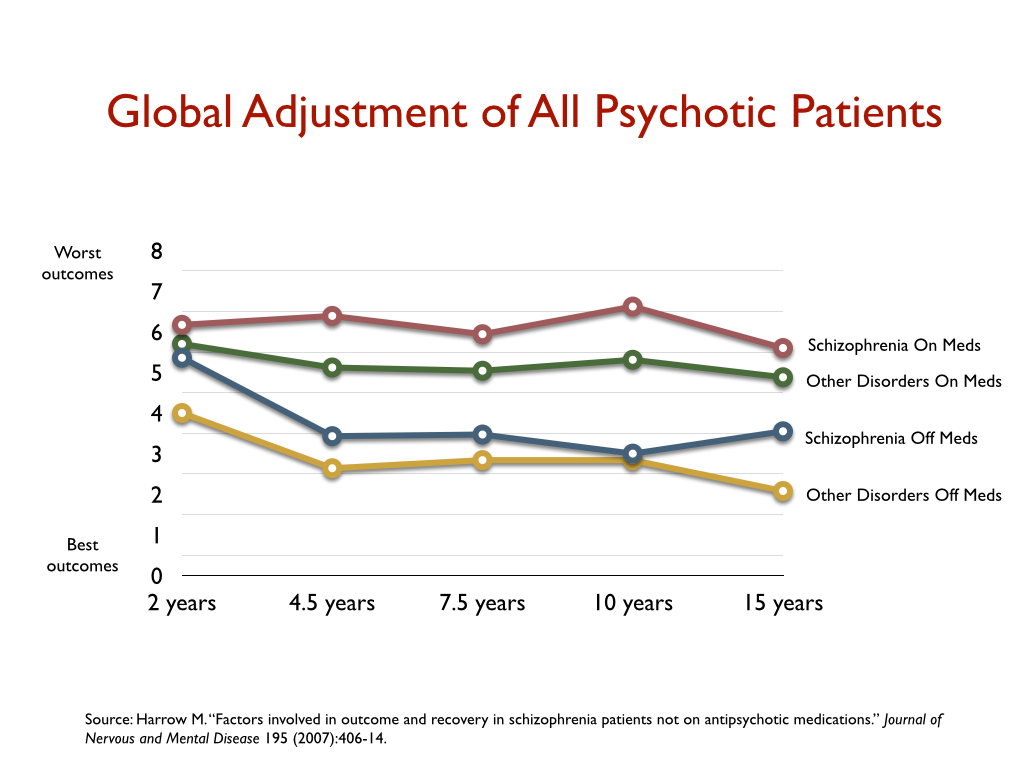
Now, in 2007, that was not a comparison that Harrow and Jobe made. It was in their data, but I was the one who compiled it into a graphic that illustrated this outcome and pointed it out. But as I explained in my email to Shayla Love, Harrow and Jobe subsequently continued to analyze their long-term data, and in one of their published papers, cited me as raising the issue of whether the drugs might worsen long-term outcomes (in the aggregate.) In these later papers, they published findings that told of drugs that increased the likelihood that patients would become chronically psychotic and functionally impaired.
Furthermore, Harrow and Jobe, in these subsequent papers, specifically stated that it was time for the field to address the question of whether antipsychotics might, in a causal sense, be worsening long-term outcomes. They wrote: “How unique among medical treatments is it that the apparent efficacy of antipsychotics could diminish over time or become ineffective or harmful? There are many examples for other medications of similar long-term effects, with this often occurring as the body readjusts, biologically, to the medication.”
Torrey, Pierre and others, in order to explain away Harrow’s study, argue that since it wasn’t randomized it was likely that it was the more severely ill who stayed on the drugs and that this could be the reason for the worse outcomes. But in making this argument, they are turning a blind eye to the evidence that belies that explanation. Those who were less severely ill at baseline who stayed on the drugs had worse outcomes than those who were more severely ill at baseline who got off the drugs.
As such, Pierre and others are the ones who could be said to be “misreporting” the outcomes in the Harrow study. But they need to do so in order to maintain a societal belief—and their own belief—in a narrative that tells of antipsychotics as a great advance in psychiatric care, with these drugs an essential long-term treatment for those diagnosed with psychotic disorders. If they were to incorporate the above graphics into their textbooks and the stories they told to the public, their narrative would collapse.
The Wunderink study can be seen as a follow-up of sorts to the Harrow study, and partially confirming its findings, because there was a randomization component. In this study of adults with a first episode of psychosis, all patients were stabilized on antipsychotics for six months (n=128), and then they were randomized either to a “drug discontinuation/drug reduction” arm (the DR group), or to standard drug maintenance (the MT group.) In other words, this was a randomized study designed to see which treatment protocol produced better outcomes: tapering first-episode patients from their antipsychotics (or down to a low dose), or standard drug maintenance, at usual doses.
At the end of seven years, those in the DR group had a much higher recovery rate (40.4% versus 17.6%). The difference in recovery rate was due to the fact that those in the DR group had much better functional outcomes.
Thus, this randomized study challenged conventional prescribing practices. It found that a dose-reduction protocol, which allows for the possibility that some patients could successfully go off their antipsychotic medications, produced superior overall results to the standard protocol of care, which emphasizes continual drug maintenance at higher dosages.
Together, Harrow and Wunderink together produced a one-two punch. There is reason to worry that antipsychotics worsen long-term outcomes, and there is evidence that a protocol that helps first-episode patients taper from the medications, or get down to a lower dose, will increase long-term recovery rates.
I handed all of this on a platter to Shayla Love. All she needed to do was read the studies, call Harrow or Jobe, and she could have had a blockbuster article, anchored by research that revealed there was a scientific rationale for a “movement against psychiatry.”
Deconstructing the Vice Article
I believe that Love, as she wrote this article, thought she was doing her best to be “fair” and to “tell both sides.” But when you deconstruct the article, and break it down into its various parts, you can see that it serves to defend the conventional narrative, and undercut the challenge to it.
Framing the Issue
When an article is titled “The Movement Against Psychiatry,” the first expectation of readers is that it will feature interviews that can explain the reasons for the movement. What is the nature of their critique of psychiatry? What evidence supports their critique? The article could be expected to present this case, and then, having done so, it could explore the merits of that critique and include responses from leaders in psychiatry.
That is not how this article is organized.
The article opens with two anecdotes of contrasting “patient” experiences. In one, a mother tells of how her grown daughter, after being diagnosed with bipolar in high school and treated for that diagnosis, refused to take the drugs after graduating and years later had landed in jail and was severely ill. It’s a story of a societal failure to force “helpful treatment” on an individual.
That failure is contrasted with a story told by Angela Peacock, a veteran of the Iraq War, who was diagnosed and treated with an array of psychiatric drugs, which led to her becoming debilitated. It’s a story—at least as presented in the Vice article—of “overmedication.”
The article then frames the “debate” in this way: “How could one woman be so overly medicated and diagnosed while another escaped any sort of proper care and ended up being abused in jail? Martha (the woman’s mother), influenced by her experience, has become an advocate for more medical mental health intervention, while Peacock says a medication-happy psychiatric system left her sicker than when she started. These contrasting positions are at the heart of anti-psychiatry and critical psychiatry.”
In journalism, this paragraph is known as the “nutgraph.” It sums up what the article is about. Yet, from these two anecdotes, readers are left to understand that the “movement against psychiatry” is, at its heart, related to both a failure to force treatment on certain people (e.g. undertreatment), and to overtreatment with psychiatric drugs. The pro-force people are, it seems, being included as part of a “critical psychiatry” movement.
Since this is an article about “The Movement Against Psychiatry,” Peacock’s anecdote would make for a good introduction. But lumping the two contrasting anecdotes together makes for a confusing start for an article so titled.
Whiffing on History
After that opening, the article jumps into an exploration of the “history of antipsychiatry,” jumping back to the ideas of Thomas Szasz, who wrote The Myth of Mental Illness nearly 60 years ago. This brief history then evolves into a suggestion that his arguments animate the “antipsychiatry” wing of the “movement against psychiatry” today, even though there is no-one quoted in the article who actually refers back to Szasz’s beliefs. And with that straw man set up, the article then quotes several psychiatrists who criticize Szaszian ideas as having come from a time when patients remained in hospitals for years and are now out of date. Thus a first message is delivered: This movement is led by people who are stuck in the past.
The article also describes a second arm of this supposed movement against psychiatry: Scientology and its discontents. This is actually a talking point regularly put forth by defenders of psychiatry, which they have employed to delegitimize challengers to their profession. The criticism is coming from a cult, who might as well be members of a flat-earth society.
This description of today’s “movement against psychiatry” completely misses the mark. The movement today is clearly driven by the activism of those with “lived experience” as patients in the system, including having been hospitalized. Its historical roots go back to the 1970s, when ex-patients published newsletters and organized protests that spoke of “freedom” from a system that forced treatment on them and locked them up, and of “liberation” from this oppressive arm of American society. This was, at its heart, a Civil Rights movement, and the book that served as their clarion call was not The Myth of Mental Illness, but Judi Chamberlin’s On Our Own. Ex-patients, who dubbed themselves “psychiatric survivors,” wanted the right to be the authors of their own lives.
That founding moment in the 1970s has surely metamorphosed into many forms over the last forty years, with a diverse range of opinions now present among activists with “lived experience.” But their collective voice, while amplified by professionals in the field who may speak critically of the current paradigm of care, remains at the moral and emotional center of any movement today against psychiatry.
This Vice article misses this fact, and by referring back to Szasz, with a nod to Scientology, it whiffs on presenting the nature of the “movement against psychiatry” today. Instead, those references serve to plant doubt in the readers’ minds about this “movement.”
Indeed, this article reveals that a public discussion about the merits of psychiatry would be greatly aided by a popular book that told of the rise of this movement, tracing its roots as a Civil Rights movement in the 1970s to the diverse voices and groups pushing it forward today.
Enter Mad in America
It is at this point that the article introduces Anatomy of an Epidemic, which then segues into a discussion of the merits of Madinamerica.com. Love begins with a note of flattery, describing Mad in America as the “most active and legitimate critical psychiatry platform that exists today.” Here are the ways that she then undercuts—and delegitimizes—the scientific critique that is at the heart of the book and our efforts at Mad in America.
1) Love describes Anatomy of an Epidemic as “a book that argues that an increase in mental health disability was caused by the long term overuse of psychiatric medication.” That puts the critique in Anatomy into the “overmedication” category, which would make it a critique of prescribing practices, rather than an investigation of the merits of the drugs. That fits with her opening anecdote about Angela Peacock: the problem is overmedication, and that is what people are rebelling against.
However, as I noted above, Anatomy tells of a failed paradigm of care, with an extensive presentation of scientific findings that, at the very least, provide reason to worry that psychiatric drugs worsen long-term outcomes. This mistaken characterization of the book keeps readers from understanding why the book is so threatening to psychiatry, and why it provides an “evidence-based” reason to fundamentally rethink psychiatry.
2) The Vice article then rightly ties the founding of the Madinamerica website to Anatomy. The book is described as “the bedrock of Mad in America,” and then in the very next breath, Love quotes Nev Jones, an assistant professor in the Department of Psychiatry at the University of South Florida, as stating that Anatomy “is just packed with misinterpreted, misunderstood studies that Whitaker uses to make claims that I think are demonstrably untrue.”
This is more than just a shot at me and Mad in America. The article is informing readers that the “most legitimate critical psychiatry platform that exists today” is built upon a foundation of “misrepresented” studies and “claims that are demonstrably untrue.” That signals to readers that the critical psychiatry effort movement—something much larger than MIA—is compromised by a misunderstanding of research and by falsehoods.
Having raised a charge like this, a journalist is duty bound to provide an example that could substantiate it. However, Love did not cite any example given by Jones to back up this charge (and it’s unclear whether she ever even asked Jones for an example).
3) What followed might be characterized as a bait and switch. With that “demonstrably untrue” charge hanging in the air, Love cites, as an example of Jones’ criticism, a critique raised by someone else, psychiatrist Joseph Pierre. His criticism, in fact, is of a much milder sort, which is that the studies by Harrow and Wunderink don’t prove, in a causal manner, that antipsychotics worsen long-term outcomes. It could be that those who stayed on the drugs were more severely ill and that’s why they had the worse outcomes.
Now, even on the face of it, this example doesn’t support Jones’ criticism. Pierre is speculating that this could explain Harrow’s results. Love also doesn’t present any evidence that I ever wrote that the results were “causal” proof that antipsychotics worsened long-term outcomes.
And indeed, Love then states that this example simply serves to show how a study can be interpreted in different ways!
It’s a rather confused few paragraphs, and Love does quote parts of my reply in my email to her about how I reported on the Harrow study. I imagine that, in her mind, this was an example of her being “fair.” But here is the journalistic failure: Love made no effort to see if Pierre’s mild criticism of me was true. She doesn’t present, with any detail, the findings in the Harrow study; she didn’t review what I had written about the studies; she didn’t see if Pierre’s speculation was supported by the evidence; and she didn’t interview Harrow or Jobe to find out what they thought.
And so, what will casual readers of the Vice article take from this section? They will surely remember the “demonstrably untrue” claim about Anatomy of an Epidemic, without recognizing that the author’s supposed example of that claim doesn’t address that charge at all.
As such, she did precisely what I had warned about in my email to her. She needed to contact Harrow or Jobe and see if Pierre’s critique of my reporting on their study was inaccurate. “If you don’t do this, and you just let Pierre get away with this criticism,” I wrote, “you are letting the ‘powerful’ trash those who would question their narrative.”
4) Love then extended this criticism to MIA’s coverage of research findings. While she included a note or two of flattery, that some of it is good, she summed up the collective effect of our coverage with a quote from psychiatrist Awais Aftab: “Readers who rely only on Mad in America will get a very distorted picture of what the state of research looks like . . . Sometimes their coverage of research is surprisingly insightful. But at other times I read the website and I just shake my head with disappointment.”
As an example of why our science coverage produces a “distorted picture,” Love cited snippets of writings from two blogs (neither of which was about research).
Blogs, of course, are not our articles. They are not reports on science from our science team. They are opinion pieces, and as I noted above, MIA serves as a forum for blogs written by a diverse group of people with lived experience, professionals, family members, lawyers, and so forth.
The day after the piece was published, Aftab wrote on his personal blog that Love had, in fact, taken his quote out of context. “Some felt that my comments were targeted specifically at MIA’s research news team, but that is not correct,” he explained. “When I said things like I ‘shake my head with disappointment,’ it is with regards to blogs and articles such as this one.”
That link went to a blog by dissident psychiatrist Peter Breggin.
5) In her concluding words about MIA, Love followed the same “flattery first, criticism second” routine. While some of the material on MIA is useful, she wrote, “the extreme anti-psychiatry articles threaten to obscure these [useful] voices with calls for the abolishment of psychiatry altogether, claiming that mental illness does not exist at all, or that all medication is toxic and causes all mental illness.”
Once again, a fact check would have been helpful here. There are no articles published by Mad in America staff writers, or freelancers that have written articles for us, that call for the abolishment of psychiatry, or claim that mental illness does not exist, or that all medication is toxic. Zero. And we have been at this for eight years now. There have been a handful of blogs that have advanced the first two sentiments; I am not sure there ever has been a blog on MIA that declared “all medication is toxic.”
Where these sentiments can be found frequently on our site is in the comments section. Those voices, of course, are not ours. That aspect of our site is designed to give voice to a community of readers, and given that many in this community had horrible experiences as psychiatric patients (or were forcibly treated in hospitals), you can find such sentiments there.
As a last thought in this section, having attributed the sentiments voiced by some of our readers to Mad in America, Love basically likens us in this regard to Scientology.
Media Watch
Mad in America publishes “Media Watch” reports because this can illuminate how the mainstream media covers psychiatry and its treatments, and how it reports on challenges to that conventional narrative. The Vice piece was a bit like a wolf in sheep’s clothing, often sympathetic in tone with some criticisms of psychiatry, yet bent on delegitimizing a critique grounded in a review of the scientific literature (which can be found in Anatomy and on MIA.)
There is, of course, nothing wrong about people criticizing MIA or me personally. The criticism can open the door to further discussions and debate, which you can hope will lead to a greater understanding of important issues.
With that in mind, I did want to speak to Nev Jones about her criticism of MIA, and to learn more about her interview with Vice. Jones is much admired for her research on peer initiatives, which we have covered on MIA. Shortly after the Vice article appeared, she presented a webinar for MIA Continuing Education on the history of peer support and its effectiveness, evidence of how she is admired within MIA. Nev, Sandy Steingard, and I had a three-way phone conversation, and they then engaged in a written dialogue related to this Vice article. Their piece can be found here.
In regard to her criticism that Anatomy of an Epidemic was packed with claims that are “demonstrably untrue,” Jones wrote the following:
“In the aftermath of the publication of the Vice article I’ve done a lot of reflecting on the state of public discourse about psychotropic medications, the tensions involved, and walk away with a renewed sense of the importance of dialogue and engagement between those with diverse (and sometimes conflicting) perspectives on this set of issues. In this context I regret the wording of the excerpts ultimately quoted and feel that it would have been much more effective to focus not on particular people, groups or texts but rather underlying beliefs. As I explain in my conversation with Sandy Steingard, that is, my concerns are most centrally not with Anatomy or Mad in America but rather with discourse that centers medications (in debates about mental health system reform) in ways that subtly (or not so subtly as the case may be) displace underlying structural determinants and the deeply complex entanglements of poverty, employment, race and disability. I also want to make it clear that none of my comments were meant to criticize the MIA Science Team, which includes a number of very talented graduate students, and has helped increase community access to dozens of important publications otherwise trapped behind pay walls.”
I also wrote an email to the Vice editor for this article, Timothy Marchman, asking if I could interview him for a Media Watch report on this article. I provided him with a copy of my email exchanges with Love, and listed a number of questions I wanted to ask:
- Given that MIA was going to be identified as central to this “movement against psychiatry,” why weren’t we interviewed for the article?
- Did he think it was fair to air a criticism that Anatomy was packed with misrepresented studies and claims that were demonstrably untrue, and yet not provide a single example to support that criticism?
- Why didn’t Shayla Love call Martin Harrow or Thomas Jobe to see whether they thought I had misinterpreted their study?
- Why did the article cite snippets from two blogs as supposed examples of MIA’s distorted coverage of science?
- Why did the article quote Aftab in a manner that implied he was talking about MIA’s science coverage, when in fact he was talking about opinions expressed in the blogs?
- Did he think this article was fair?
Here is how Marchman responded: “You were asked to respond to criticisms, did so—after asking for and receiving clarifications on several points—and now essentially object that the parts of the story dealing with your work weren’t written as you would have written them. What you describe is Shayla fairly and accurately laying out criticisms that have been made of your work, incorporating your responses in the story, and adding necessary context to, for example, show readers how, as she wrote, ‘the same study can be interpreted in different ways.’ All of this strikes me as a credit to her and her reporting.”
Marchman, of course, hadn’t answered any of the questions I had asked. There really was no way he could—the questions alone told of a journalistic piece that likely met the legal requirement for defamation. And there was nothing in his answer that told of a journalistic search for “truth.”
One Step Forward, One Step Back . . .
There is reason to celebrate the publication of this article. The fact that Vice decided to report this story is evidence that critiques of psychiatry are slowly making their way into general societal discussions about the merits of psychiatry and its treatments. This is a sign of progress.
As I said at the beginning of this article, the article also provided MIA an opportunity to explain, in some detail, our mission and why we do what we do.
Finally, I hope that deconstructing this article—and revealing the journalistic standards that are on display—helps reveal the depth of the challenge for those who would like to see “psychiatry reimagined.” Unfortunately, this struggle is regularly hindered by the fact that media are often poised to report in ways that protect the conventional narrative, and look askance at those who would challenge it. But as is the case in any struggle, it’s always good to know what you are up against.














It’s disappointing that the author of the Vice piece didn’t even do proper interviews or really delve into the particulars of the studies. It’s definitely a missed opportunity.
I just want to take a moment to thank you for this article and thank you for writing Mad In America. It was really quite life-changing when I found it in my university’s library. I had been launched into the world of psychology and psychiatry when I was six-years-old and until that point I had never thought to critique the system that I was submerged in.
And, to be frank, I was angry at first, dismissing the book as “anti-science” and that my medication was the only reason I was still alive and that I’d be so much worse without it.
But there was something that awoke in my mind.
And after I continued to get professional care, I was eventually led to a psychologist who was supposed to be the best professional in my area for the treatment of OCD. She did me a lot more harm than good when she forced me to fit into her CBT method even though my problems were manifestations of very complex and deep-rooted trauma.
And I just gave up, thinking that I’d never be “cured” and that my brain was broken and there was no way to fix it. I was just a broken person.
A few years later, I was still in treatment and doing worse than ever. Looking for SOMETHING to help, psychiatrists started turning to atypical anti-psychotics as a remedy for my OCD. I was prescribed Zyprexa and Risperdal, working up from a small dose to larger ones.
But there was just something in that side effect list that didn’t seem right to me. I mean, would a permanent movement disorder be a fair tradeoff for less anxiety? I’ve never been psychotic. The doctors were just turning to harsher drugs when SSRIs and benzos and tricyclics didn’t cure me.
Then I again bumped into Mad In America, in the form of this website. And I started reading about anti-psychotics and the often harsh and extreme side effects they have.
I never took a single pill of either of the drugs that I’d been prescribed after reading the information on this site. And I am thankful every day that I didn’t.
This website, a friend network, and Bessel van der Kolk’s “The Body Keeps the Score” changed my way of thinking about what I’ve been diagnosed with and I let go of the frantic search to to find some perfect syndrome or disorder to label myself with as if that label could erase my history.
And I’m still not well, but I have hope now.
Thank you.
Report comment
You once falsely believed the medication was the reason for everything you had. Now you recognize the truth, that you were stronger, more resilient, and more dedicated then you ever imagined. Strong enough to survive being put on however many horrible drugs for so long. I hope you can recognize the beauty, exceptionalism, and accomplishment of your survival like I now do.
Report comment
«Medicines» can be the cause of absolute, irreparable destruction. And the question is why to use such “medicines” to already suffering people?
Report comment
Because they’ve chosen to write off these suffering people as either beyond help or not worth helping. (By help I mean ordinary human help or TLC which you stop receiving once labeled SMI.)
The “medicines” often have the desired effect of turning intelligent but suffering people into docile, childish creatures. Incapable of independent living or any quality of life most adults prefer yet easy to “take care of” or control.
Like severing someone’s spinal cord so they’ll obey the caretaker ordering them to a lifetime of bedrest.
Or cutting off a songbird’s wings and severing the vocal cords so it won’t fly away or annoy its keepers by singing. The songbird is unhappy but what it wants doesn’t matter.
Report comment
“Because they’ve chosen to write off these suffering people as either beyond help or not worth helping. (By help I mean ordinary human help or TLC which you stop receiving once labeled SMI.)”
Yes, wishes of course inhuman. What would to rid of annoying, suffering people, to successfully control them (instead of helping them) – to turn them into living nothingness. About compassion and conscience are not to be mentioned here.
However, one noteworthy circumstance should be noted. –All the wishes of the “helping” “cure” activists come down to a simple, clear goal – these interfering sufferers must somehow be eliminated. Well, for such a task, a simple solution suggests itself. – These disturbing, inconvenient people can be put to death. Dead, they are definitely to anyone will not be anxiety. Why does such a decision not suit the merciless cynics? Why spend so much effort, time, resources to torture and destroy the victims with “treatment”? It would be much easier and much less cruel to simply kill these unnecessary people. However, for some reason this option does not suit assertive “healers”. As can see, they are driven by some other motives than just getting rid of objectionable people.
Report comment
I like Vice, but in fact, it is more of a tabloid than serious journalism. Shayla Love’s piece was a cut above its usual fare, but even “in depth”, very superficial in regards to the subject, and off-base when talking about the current state of “anti-psychiatry”, missing the substance of the protests of the injured patient movement entirely.
In this, one suspects her primary source was Joe Pierre, UCLA psychiatry professor and Acting Chief of Community Care Systems at the Veterans Administration West Los Angeles Healthcare Center, who is determined to ignore the potential of injury from psychiatric treatment. His position is rather fraught: Though he admits such injury might exist, he claims the way that people make noise about it on social media (primarily Twitter, because that’s where he hangs out) is inappropriate, thus justifying ignoring it.
There are some injured consumers on Twitter who have adopted the tactic of meanly trolling psychiatrists; from this, Dr. Pierre — a scientist of human emotion and behavior who fancies himself an expert on mass delusion — concludes there is a new “anti-psychiatry”, which he likens to anti-vaxxers.
Further, he (and 2 co-authors) claim consumers complaining of injury evidence a psychiatric disorder, an “attempt to find meaning in identity as an injured party”, described in a September 9, 2020 piece published on MedpageToday, “Op-Ed: Why Anti-Psychiatry Now Fails and Harms” (free registration), thus implying no such patient harm actually exists. (None of the 3 co-authors appear to have personally examined any of these consumers prior to coming to this diagnosis, instead referring to their experience of social media.)
Awais Aftab captured the consumer protest July 12, 2020 in an article on his own blog, “Primum non Nocere: A Psychiatrist’s Review of “Medicating Normal””.
Since new injured consumers are being generated by psychiatric treatment every day, we can be confident this consumer movement will not stop, and will continue to express itself on social media and elsewhere. Injured patients are injured patients, no amount of gaslighting from psychiatrists like Joe Pierre and Tyler Black will make them disappear.
Recently, the UK’s Cumberlege review found systemic error in ignoring treatment harm, generalizable across healthcare. An article about it, “Cumberlege review exposes stubborn and dangerous flaws in healthcare” was published August 6, 2020 in the BMJ:
“Perhaps most striking was the testimony from hundreds of patients reporting lack of informed consent for their initial treatment, followed by years of dismissal by clinicians and regulators who did not want to associate life altering symptoms or injured children with their medical interventions. In a press release Cumberlege said that in years of reviews and inquiries she had never encountered anything like the intensity of suffering of these medically injured families. The review panel found that healthcare providers’ dismissive attitude toward patients was underpinned by a reluctance in all parts of the system to collect evidence on potential harms, by a lack of coordination that would allow clinicians and agencies to interpret and act on that information, and by a culture of denial that failed to acknowledge harm and error, impeding learning and safety.
….
These patterns are already familiar to all patients who have been harmed by medical care. What the Cumberlege team has flagged is the stubborn flaw that lies at the heart of the practice of medicine. It is often called “culture.” But this type of embedded attitude seems to go beyond culture, beyond fear of liability, and beyond the profit motive when that exists. It is a patronising and insufficiently curious way of doing business that is often at odds with the realities of helping patients heal and is increasingly out of place in a connected modern world. How to change it is still an unsolved problem. There have been inquiries, reports, and recommendations over the years, but the fundamental issues around power, justice, and compassion are still with us.””
Report comment
Yeah here – Cumberlege review: https://www.immdsreview.org.uk/downloads/IMMDSReview_Web.pdf
Report comment
“It is often called ‘culture'” wars. Yes, that’s what my systemic, child rape covering up, psychologist and psychiatrists’ worshipping, childhood religion calls it.
https://books.google.com/books?id=xI01AlxH1uAC&printsec=frontcover&source=gbs_ge_summary_r&cad=0#v=onepage&q&f=false
“But this type of embedded attitude seems to go beyond culture, beyond fear of liability, and beyond the profit motive when that exists.” I don’t know about that, it all seems to be about money worshipping to me.
However, I do agree, “It is a patronising and insufficiently curious way of doing business that is often at odds with the realities of helping patients heal and is increasingly out of place in a connected modern world.”
Report comment
“…Further, he (and 2 co-authors) claim consumers complaining of injury evidence a psychiatric disorder, an “attempt to find meaning in identity as an injured party”,
Well if that is what it takes to have “meaning”. It seems then that psychiatry creates meaning through injury, or at least the “attempt at”.
How wonderful they are capable of accomplishing so much with their “medicines” and mostly their broken record and repeat of their original precepts.
I wonder how many psychiatrist find “meaning” in their work. Is it meaningful to have a relationship with a subject, the subject that is the reason for your income or just meaningful to belong to a group of like minded colleagues.
Obviously our meaning has a lot to do with reward. People forget easily that the subject before them, not their colleagues before them is paying their wage. Never understood how it is allowed to be abusive to one’s employer.
Report comment
Are there any other businesses or medical professionals whose practice is to insult their consumers? Who claim their consumers need to keep taking the addicting drugs they sell because the consumers are too stupid to know they are really good? Who then turn around and say anyone who they have not insulted who says something negative about the drugs lacks insight to know how good they are?
Report comment
“Are there any other businesses or medical professionals whose practice is to insult their consumers?”
Comedians?
Report comment
In the VICE article Awais Aftab is quoted as follows: “These critics have no skin in the game because they are not the ones responsible for caring for these individuals; they are not the ones who have to witness the profound impairment of the psychotic individuals and the profound suffering of their families.”
I just wonder who he thinks cares for these individuals and their families and who has to witness their suffering once they have been profoundly impaired by psychiatric “medication”
Report comment
Especially since both the antidepressants and antipsychotics are medically known to create “psychosis,” via anticholinergic toxidrome. Which most of the so called “mental health” workers claim to be ignorant of this knowledge, since this toxidrome is not listed in their DSM “bible.”
Report comment
Such a good point.
Report comment
Thanks, Cole.
Report comment
I noticed that your crusaders didn’t go after the orthomolecular guys with the same vigor when they went after you. Of course, the orthomolecular types are more interested in real medicine than “psychiatric medicine” and use physical testing such as trace mineral analysis as diagnostic aids. Their patients frequently don’t have a psychiatric status, but will be diagnosed with physical ailments.
They’re some of the greater menaces to Big Time Psychiatry in recent decades and will become more so, as “psychiatric” diseases disappear to be replaced by garden variety physical ones.
Report comment
“One Step Forward, One Step Back . . .”
More like an attempt to nail one foot to the floor and watch as you walk in circles. I can’t find the quote form M Scott Peck but he says something like evil leaves waves of chaos in it’s wake, sorting out that chaos is much more difficult than making the waves. I don’t know how much of an analysis of the poo Love has thrown is of value, but you can be sure some of it will stick.
Find yourself explaining things you feel you have already made clear and that people should understand? I know I never thought I’d have to explain to the person who “protects consumers, carers and the community” and who “provides expert legal advice to the Minister” what a burden of proof in law is, and why his removal of “reasonable grounds” from the Mental Health Act provides carte blanche and opens up arbitrary detentions by mental health workers. Still, with slander and fraud as weapons, why would they need to respond to any valid questions? Simply make anyone who complains into a “patient” post hoc and begin ‘treatment’.
Surely claiming that making an allegation of torture by public officers is a mental illness is a direct violation of the Convention against the use of Torture, and constitutes “refoulment”? Particularly when the State has failed to retrieve the proof of those acts of torture?
Report comment
OMG where to start? Maybe here:
I told her we weren’t an antipsychiatry website, but rather that we were better described as a “critical psychiatry” website.
And herein lies the main problem as usual. MIA is not only NOT an anti-psychiatry site — very unfortunately — it has the effect of PROMOTING psychiatry when it uses psychiatric terms such as “schizophrenia” with a straight face and talks about “research.”
So many inaccuracies on both “sides” here, I’ll probably be adding comments all week. But we’ll start with this, which is the most basic.
Report comment
Oldhead, no one in general society would believe your “mental illness is a myth” pronouncement, because though we can understand what that means here, it doesn’t stop people from seeing everyday those who are depressed or anxious or suicidal or end up with strange beliefs. How would you approach this problem?
I don’t see the practical value in your standpoint given the ACTUAL state of things in the world and not merely intellectual idealism.
MIA doesn’t necessarily use those terms in order to promote psychiatry (even if that inadvertently ends up happening), but given how most people think and how psychiatry is organised, it becomes practically useful sometimes.
Report comment
We do not operate according to what people will accept, but according to what is true and false.
When one realizes that “mental illness” is literally impossible there remains no further reason to debate the legitimacy of psychiatry, only to strategize its demise. And this has nothing to do with MIA one way or another.
Once one realizes that the basic precepts of psychiatry are fraudulent it doesn’t matter how many people are “depressed or anxious or suicidal or end up with strange beliefs”; it is clear that psychiatry is not the answer.
MIA doesn’t necessarily use those terms in order to promote psychiatry (even if that inadvertently ends up happening)
🙂
Report comment
“MIA is not only NOT an anti-psychiatry site — very unfortunately — it has the effect of PROMOTING psychiatry when it uses psychiatric terms such as ‘schizophrenia’ with a straight face and talks about ‘research.’”
Especially given the fact that the so called “schizophrenia” treatments can create both the negative and positive symptoms of “schizophrenia,” via both neuroleptic induced deficit syndrome and anticholinergic toxidrome.
https://en.wikipedia.org/wiki/Neuroleptic-induced_deficit_syndrome
https://en.wikipedia.org/wiki/Toxidrome
Personally, I hope MiA is a website that understands the systemic crimes of the psychiatric industry, and their drugs, need to end. But I will say, it is still promoting the crimes of the DSM believing psychologists.
Both the psychiatric and psychological industries are scientifically “invalid,” DSM “bible” believing, systemic child abuse cover uppers for the mainstream religions.
So the religous child abuse covering up psychologists, who utilize the psychiatrists to make innocent people “psychotic,” via the psychiatric drugs, to cover up child abuse for their pastors, and are unrepentant child rape covering up criminals.
And such crimes are the number one societal function of both the psychiatric and psychological industries.
https://www.indybay.org/newsitems/2019/01/23/18820633.php?fbclid=IwAR2-cgZPcEvbz7yFqMuUwneIuaqGleGiOzackY4N2sPeVXolwmEga5iKxdo
https://www.madinamerica.com/2016/04/heal-for-life/
Which means MiA needs to speak out against both the psychiatrists, the psychologists, and all the systemic, child abuse covering up crimes of all the “mental health professionals” and mainstream religions.
Since the entire, scientific fraud based, “mental health” industry is a systemic child abuse covering industry, for the paternalistic mainstream religions, by DSM design.
https://www.psychologytoday.com/us/blog/your-child-does-not-have-bipolar-disorder/201402/dsm-5-and-child-neglect-and-abuse-1
Report comment
“Mental illness” is not a social construct so much as an etiological one.
A phrase which makes no sense when viewed too carefully.
How does “mental illness” differ from neurological or brain illness? is a question to ask. How William Glasser got me to reconsider the hopeless “disease” I’d been repeatedly told I had.
Report comment
Registered,
The lies were never that people suffer. The lie was pretending to understand it, then go on to define it. And worst and most draconian was to try and use knives to cut the thing out that was perceived to be the disordered parts. You obviously know that the drugs are the knives so it is now a thousand and some worse, since it is a “cocktail” and everyone loves a cocktail.
“how most people think” changes.
Report comment
Such a poorly written, shoddy piece of “journalism.”
Report comment
I was referring to the article RW critiques.
Report comment
Good point, Gerard. I also notice an implicit assumption in Aftab quote that “these critics” who “have no skin in the game” couldn’t possibly be ex-patients – who have all their skin in the game, not to mention their brains, livers, and every other organ; the assumption that a former patient… just as an example, I’ll use myself… couldn’t witness their own profound impairment and suffering that resulted from psych polypharmacy and for this reason became a vocal critic of the current paradigm of care. Aftab, for whatever reason, completely removed ex-patients from the pool of potential critics. The question is, why? Because I can say for certain that I am a critic and have way more skin in the game than I would ever wish for.
Report comment
“Aftab, for whatever reason, completely removed ex-patients from the pool of potential critics. The question is, why?”
Because as was stated in our Parliament here when a report detailing the levels of sexual assaults being experienced by female patients was tabled, our Minister for Mental Health responded with “You can’t listen to them, they’re patients”. It’s an attitude that comes with the turf i’m afraid. If they started listening, then they would hear things they don’t want to be true. Torture is NOT medicine because you call the person “patient”, but it sure is a great way to conceal your crimes. Especially when you can have police snatch anyone complaining from their beds and have them dribbling in a cell within the hour because “tomato” (remove the “reasonable grounds” protection from the law and what have you got? Arbitrary detentions and torture concealed as “inherent in or incidental to lawful sanction”)
Couldn’t help but laugh when I got to “not to mention their brains, livers ….. lol.
Report comment
“Mentally ill” people who are against the drugs lack insight and can be ignored and forced on the drugs.
People without those labels who are against the drugs can be ignored and slandered because they lack the insight from being “ill”
Psychiatry holds these two contradictory beliefs simultaneously. I’d say if anyone lacks insight it is the psychiatry people who can’t do basic logic.
Report comment
Just want to say, Thank you, Mr. Whitaker, for keeping up the good fight.
Report comment
I made a couple of comments on the original article, which initially got published. But I just checked and the comments section appears to have magically disappeared! I wonder why…
Report comment
“I made a couple of comments on the original article, which initially got published. But I just checked and the comments section appears to have magically disappeared! I wonder why…”
Post them here? Under this comment? Lets see if the Moderator is as tough as the guy around here lol
I must admit I did like her review of the medical movie Debbie Does Dialysis. And I agree with her that the use of the Police hit song Don’t stand so Colostomy was the best version they ever did.
Report comment
Well, there you go Steve, you did not agree. Why is an excellent question and is one they again have no logical
or intelligent answer that would make any sense.
Report comment
Um…
The article reads a bit like something from eonline or a gossip column. Albeit she has snippets of information from a whole array of areas, but she dots back and forth from this one to that one much like the reports of what so and so is wearing, who is together with another or not or was etc. There really isn’t much depth, as much as she’s trying to make out she has real concern. She’d have to go deeper into the issues than dotting back and forth.
It’s really depictive of people’s inability in general of maintaining attention, the ten second sound byte generation.
One of the things I find most distressing are the blips or blurbs of statements about or from Irene Hurford, whose article in the New York Times I also have read now, linked from the Vice article. Her article already is another catchy piece designed to pique people’s interest and doesn’t venture into the territory of people who don’t read such articles to entertain the knowledge of being up on things, people who are most likely to end up targeted by much of psychiatry’s diagnosis and lack of acknowledgment in their environment. And the strangest thing is that’s actually touched on in the article itself (buy Love rather than Hurford), like what I’ve seen from a church that comes to the local mission and hands out used clothes and ziplock bags full of peanut butter sandwiches, junk food, little bottles of shampoo and soap, other little tokens like a necklace with a crucifix on it; and then remains proud of doing their part when they do this twice a year or so and then lock their doors behind them. And the lack of real substance to me points out that she really doesn’t have the ability to relate to someone she deems as being “psychotic,” and instead uses her concern of something she’s incapable of relating to to mask her inability, making out she’s involved with critical decision making instead. And that’s the simple truth for me. There are people who don’t get alarmed about “psychosis,” have no need to analyze it, that leave it to work itself out, or are able to make a person feel supported enough, without that soft lurking quiescent buzz in the background of I-might-have-you-committed. She talks about someone who when his father came to visit him went off of his meds and started smoking dope a lot. There’s absolutely no discussion what so ever about why he was on meds to begin with, why there was no support enough that allowed him to relate to his feelings enough to see that smoking dope every day wasn’t helping him, which in this case wasn’t, all of the dynamics with his family that become apparent with anyone still cogent about cause and effect aren’t even referred to, and then he’s back in the school whose “medical” programs regarding what he’s been through mostly push that into the background to promote what he’s already been forced into. And dope and psychiatric drugs both mess around with brain chemistry, what’s going on with someone that they prefer disabling what their brain itself might be trying to express, something that one would think has become uncomfortable to them, which both sides of the supposed support system (Hurford or the family) seem to show why there’s such discomfort and the reflex towards disabling the mind to avoid thoughts and feelings that have become uncomfortable, whether it’s with psychiatric drugs or dope. Then she talks about someone who had Aids, came into the ER and said they were a profit: sorry I mistyped it’s spelled Prophet, that REALLY was a “Freudian,”. She had him medicated, and knows nothing about him from there on. Ending the piece with: “I never found out what happened to him. I think about him often; I question my decision each time I do.” Wow! That’s a sly way to point out you need help understanding what you’re doing, but not really going forth to find out because of reticence. Just that she wanted to help becomes enough. The badge the medical establishment gives her, and thus she has to do “something.”
Hurford’s approach isn’t even all that mainstream, she will say that psychosis isn’t just non reality based garbage, but the question still remains WHY someone like her is given the power they have, when there are many people who don’t become alarmed, who don’t need to feel they are helping by taking on such a badge, but that have the ability to understand the symbolism, the need for reflexes, memories, beliefs to come out in the open through a means, in this case labeled psychosis, that might expose the reflexes, memories, beliefs whose interactions with the brain are labeled as symptoms of psychosis, and give them leg room to not remain hidden in the interplay or reactions to life, and then a person might move beyond their present limitations; but then we come across the very fabric of society, the people Hurford and Shayla Love know how to get to read their writings, dotted with acceptable blurbs for those who want to know “something,” where they can assimilate a host of things without going deeply enough into any of them to go beyond such hip hop repertoire. Safe stuff to go to any school, church, parks and recreation classes, neighborhood leagues, Girlscout or Boyscout get together, sports club, political party etc. and start sharing how up you are on stuff.
And Hurford talks about how “psychosis” is taking a person’s civil liberties away, which is a quite “amazing” concept. Decorated with their supposed inability to realize something is wrong, Thus she “medicates.” But speaking of what’s wrong, it’s not mentioned how psychiatric drugs have lead to more disability, relapsing, loss of life and paranoia about “psychosis” along with recycling of it with that paranoia strengthened and supported even when alternative approaches lead towards more recovery, whether the symptoms are gone because they were understood or simply not medicated; one wonders how one can respond at all to such an amazing convolution of what’s going on. “What we cause more of by taking away your civil liberties is taking away your civil liberties, so we continue to cause more of it to save your civil liberties, which we took away.” And WHAT is cause and effect!? That a psychotic person would have to deal with such indoctrination, such convoluted “logic,” and be a different effect from what those taking away their civil liberties are causing, and then have to figure out how to escape from such a situation!?
I also find this something akin to confusion technique, all of the hip hop blurbs, because there are too many references to too many people, without delving any deeper, and one becomes incapable of remembering anything beyond a blurb, with the amount of stuff popping up; and would you want to address any of it, you have to start looking deeper yourself, after having identified the stuff that needs looking into; and then further more knowing by then that you are going to encounter stuff that just doesn’t fit this hip hop blurb world. It’s not quick fix, fast food enough. Can’t get it at the drive through or order it online with a few clicks. Not hanging on the corporate media output tree where cherries are ready to be picked.
Shayla Love also mentions a clinician Nev Jones, who has concern about polarization, and mentions Robert Whitaker’s books as causing this: that parents refuse to allow their children to continue on medications (even when the medications were helping), or to start on them, this then is one anecdotal story from one clinician (one “cherry”); but has no reference to what extent the true evidence that’s not anecdotal is shared in Whitaker’s books, and yet implies that that shouldn’t be looked at or believed because of one anecdotal story. And the real polarization is apparent again. Don’t mention serious research that I can dot around and find one anecdotal story to contradict, when the serious research is already suppressed, and not in line with guilds, economic bubbles and corporate media.
So, if someone comes up to you and seems to be psychotic, and tells you they are a prophet, at least ask them how you spell that…
Report comment
And then Hurford talks about medications being like the “foundation” of a house. And without a foundation you can’t build the rest of the house.
WHAT!?
I have to laugh about something that totally isn’t funny…
Causing a chemical imbalance that’s been proven, in the guise of treating one that’s alleged, in the process causing a whole epidemic of the “diseases” said to be treated, and then saying one needs the leeway to be able to force treatment more or advocate for it, or advertise it, or more money for research because there’s “compelling” evidence you will find the chemical imbalance that’s alleged, although the evidence that the chemical imbalance you are causing by treating an alleged one isn’t just based on compelling evidence you will find it, being that the chemical imbalance you’re causing by treating the alleged one: it’s already there and been proven…..
And then it’s stated that the alleged chemical imbalance is taking away a person’s civil rights, which AGAIN is cause to take those away as well, along with causing a chemical imbalance that wasn’t there before while advertising you are treating one..
Give people a chemical imbalance they didn’t have before, by saying you’re treating one.
Take away civil rights because an alleged disease is doing that, which is quite amazing that “psychosis,” has THAT MUCH control over the whole judicial and medical system, which might actually mean that there is MORE psychiatric disease that’s not been diagnosed is it truly causing anyone to lose their civil rights, but then it’s those really taking away civil rights that need to be looked at.
I didn’t know Hurford had such insight, although her aim is a bit askew. It’s those people giving you the right to take away civil rights that are the psychosis, the alleged disease, investigate that a bit more and you might get somewhere….
HOW can one take this seriously!?
Oh I forgot. I’ts like diabetes. This alleged disease that’s said to be caused by a chemical imbalance so you treat it by causing a proven chemical imbalance that’s shown to cause an epidemic of the alleged disease (still not proven to be caused by a chemical imbalance unless it’s from treatment when one treats the alleged chemical imbalance by causing a proven chemical imbalance) and all of this is how you create the foundation, NOT mind you for an epidemic, but for how you treat this alleged disease…
And THEN you can start to build a house…
(!?!?)
Let’s see
the foundation is creating a proven chemical imbalance by saying you’re treating an alleged one
on top of that you can build a house
brick number one: “the relapsing and disability and loss of life, along with side effects, and the loss of civil rights and self determination, this is from a disease caused by an alleged chemical imbalance, not from the proven chemical imbalance that’s the treatment.”
brick number two: “If I or anyone with a diagnosis like mine doesn’t understand that, they have anogsognosia, which DOESN’T come from the medications causing the chemical imbalance, that’s treating an alleged one.”
brick number three: “That people in developing countries where there’s no money for such medications do better, doesn’t mean that rich countries might try that, it means that one should develop those countries to be more rich, although that depletes their resources sort of like the medications do to my body causing side effects, but that’s progress.”
brick number four: “It’s not that the arts, or philosophy, or great scientists in history that have created our culture had healthy minds, they’ve all been dubbed with psychiatric diseases as well, and it would be better if one could create a time machine to go fix them up, then society would be so much better, although there’s no proof for that either, as little as the chemical imbalance of the alleged disease has been found, but don’t suggest to create a time machine, that would be against the beliefs of statistical based norms and unhealthy emotionally, something the drugs can fix, again. And no, this isn’t because a time machine might disprove our theory.”
brick number five: “Go volunteer to be a peer support specialist, give up on the time machine.”
brick number six: “Don’t pay any attention to the foundation by now disintegrating, that’s because you need more medications.”
brick number seven: “put that on the new and improved foundation….”
brick number eight: “I know the foundation collapsed again, lets try shock therapy now.”
Report comment
But why keep reinventing the wheel (or in this case deconstructing psychiatry)? Time for the demolition crew. Wanna join?
Report comment
Interesting. A lot of the criticism of “antipsychiatry/critical psychiatry” actually comes from well-intentioned individuals who think that people of the antipsychiatry variety are against the notion that people suffer and that people who are suffering sometimes are utterly desperate for help. To some of them, this seems to stand for “people not getting the help they need”.
Also, I will say the article does have positive points as at least some consideration has been given to our voice rather than being a completely vicious attack dismissing, denying, labeling and gaslighting us. Some of the other pro-psychiatry sites are horrendous.
I will be the first person to say that suffering like depression, anxiety, panic and even stranger varieties of problems are real.
The article states: “But for Martha, that position is a painful one. What is the “meaning” behind why her daughter’s life has deteriorated the way it has? Martha is part of a Facebook support group for parents where she sees post after post of people desperate for help for their kids, for whom contextual support wasn’t enough. “I don’t know that anyone could say they’re happy or there’s meaning in the way my schizophrenic child is able to live their life,” Martha said”.
If what’s written is true I wish her child weren’t labeled a “schizophrenic” to begin with. That’s adding an additional layer of suffering to an already suffering individual. I wish them the best and also hope they have a permanent home that they own, and some cash in their pocket to keep afloat.
The article also states: “When Hurford wrote about her decision to treat a psychotic patient who believed he was a prophet, she got flak from both Mad in America supporters and more biological psychiatrists. “I engaged with both of them,” she said. “And I won neither battle.”
Again, I hope the man who thought he was a prophet is doing better now, but the dilemma expressed by Dr. Hurford exists on this side of the aisle as well.
The moment you’re on those drugs, it’s a trap. If it doesn’t work and does horrible things to you, you’re screwed. If it DOES work, you’re still screwed because when you accept the drugs you’re also forced to accept life-ruining behavioural labels, behavioural observations made by others on your character and conduct, electronically stored records, revolving door syndrome (partly because you’re forced back into that world for prescriptions) and you’re pretty much on a chemical leash tied to the psychiatric system which is held by mental health workers and family members (who, god forbid, have less than good intentions). This ends up getting tied to your ordinary medical problems too.
If you lose, you lose. But if you win, you still lose.
At the end of the day, problems when solved properly get people out of hospitals and don’t keep coming back over and over again to bite them in some form or the other. However, protracted and traumatic half-baked solutions do do that.
As an aside, there are lots of people for whom it’s all about the studies (partly influenced by science popularisers and the skeptics movement) and also fMRIs this and MRIs that (which is really more of a convincing tactic than anything that’s practically useful from the end user standpoint).
The sad part is, the actual experiences of the individuals (which can be brutal, traumatic and life-altering) are just dismissed as “anecdotes” by many. Hardly any of those dismissive individuals ever bother to find out the truth of those actual experiences of individuals till they or their loved ones experience it themselves in some form or the other.
There is no shortage of individuals (and I’m not talking just about mental health workers) in society who use behavioural labels to gaslight individuals. And it’s just as bad to see individuals who label themselves. Ask many of those who have experienced suffering, and they’ll say “I have OCD, ADHD, BPD etc. etc.” rather than speak about what’s ACTUALLY bothering them. Psychiatry just bolsters this type of thinking which is damaging.
The issues surrounding psychiatry exist beyond just medication damage.
I’ll say this. If people have found help in psychiatry and have had only positive experiences, good for them. They are entitled to their opinion. But don’t simply say that people are on the other camp are just rubbish to be dismissed away at your whims.
Report comment
While it’s good to have a platform for an anti-psychiatry discussion, I am far less concerned with the VICE article’s speciousness, or with arguing about fallacious “research” (and all research into “mental illness” and “medication” is fallacious by definition) than I am about some misrepresentations of the anti-psychiatry movement.
Its historical roots go back to the 1970s, when ex-patients published newsletters and organized protests that spoke of “freedom” from a system that forced treatment on them and locked them up, and of “liberation” from this oppressive arm of American society. This was, at its heart, a Civil Rights movement, and the book that served as their clarion call was not The Myth of Mental Illness, but Judi Chamberlin’s On Our Own. Ex-patients, who dubbed themselves “psychiatric survivors,” wanted the right to be the authors of their own lives.
Yes, the mental patients liberation/anti-psychiatry movement does go back to about 1970. But we need to stop speaking in past tense, because although the movement was defeated and forced underground for 30 years, we are finally reorganizing ourselves.
I don’t know why Robert puts “liberation” and “freedom” (from psychiatry) in quotes, as they are not figurative terms for us. Anyway, while some of us in the 70’s & 80’s saw ourselves as a “civil rights” movement, many also considered it a genuine liberation movement (and still do), fighting psychiatry as a form of domestic repression and cultural imperialism.
I was good friends with Judi Chamberlin throughout the time she was writing On Our Own and for years thereafter. (Coincidentally I was just filing away some of her old letters I found; people actually wrote letters then.) I can assure everyone that Judi was highly familiar with Thomas Szasz’s work and had great respect for him, and I’m certain they shared the same stage on occasion.
I have no idea why or on what basis RW would try to “distance” Judi from Szasz; by his own account psychiatry as an issue had never crossed his mind until 1998 — 15 years after the anti-psychiatry movement had been defeated and its most opportunistic “leaders” co-opted. There is no good reason to pit Judi’s book against Szasz’s work, or to say Judi’s book alone was the “clarion call” of the movement (which was well underway as she was writing it). Both On Our Own and The Myth of Mental Illness, and the writings of numerous others, had a seminal influence on the early movement (which was more than a few people gathered around Judi’s feet).
If RW is attempting to imply that the mental patients liberation movement was not anti-psychiatry — and I hope he isn’t — that assertion would be inaccurate. We were more militantly anti-psychiatry than anyone who wasn’t there could possibly imagine. While there were some reformist currents, as there tend to be in any movement, the thrust was not for “better mental health.” It was to end the concept of “mental health” — just as it is today.
All of this was articulated in formal anti-psychiatry principles and demands formulated at the International Conference on Human Rights and Psychiatric Oppression in 1976 and 1982 respectively, which described psychiatry as a “parallel police force” (among other things) which “cannot be reformed and must be abolished.”
Also, we did not call ourselves “survivors” in the 70’s — we referred to ourselves as “psychiatric inmates,” as the focus of psychiatric repression was on locked institutions, and most of the activists had been inmates. Today at least as many of us have been psychiatrized via the CMH system, which I guess is the reason that “survivor” has taken over from “inmate” as the preferred term. (I personally prefer the term “outmate” for those in the clutches of CMH.)
Also
That founding moment in the 1970s has surely metamorphosed into many forms over the last forty years, with a diverse range of opinions now present among activists with “lived experience
No no no. There is only ONE movement which represents the legacy of the Mental Patients Liberation (Anti-Psychiatry) Movement — that is the movement to abolish ALL psychiatry, still led by survivors of the psychiatric system.
The Mental Patients Liberation Movement for all practical purposes was decimated by the end of 1985, though David Oaks heroically tried to hold together the remnants for a number of years thereafter with the Survivors Coalition International, Dendron Magazine, and finally MFI. But gradually the anti-psychiatry focus got watered down.
In the current day, any purported “movement” which claims to be for “consumers,” or wants to “improve” psychiatry, is analogous to the Vichy government in occupied WWII France. Since 2017 there has been an active movement to resurrect what once was, but had been under occupation by psychiatry and its flunkies for so many years. A number of MIA survivors have worked with us in an “underground” capacity as we have sharpened our analyses and collectively articulated our demands and goals. We are almost ready to go public, and encourage any survivors who want to actively work to expose and defeat the psychiatric gulag to join us. If you want to get involved, or would like to see a copy of our basic principles, give us a shout at [email protected] .
Let’s show them what a “movement against psychiatry” REALLY looks like! 🙂
Report comment
PS Correction — David Oaks’ group that I referred to as “Survivors Coalition International” was actual named Support Coalition International.
Report comment
“I have no idea why or on what basis RW would try to ‘distance’ Judi from Szasz; by his own account psychiatry as an issue had never crossed his mind until 1998 — 15 years after the anti-psychiatry movement had been defeated and its most opportunistic ‘leaders’ co-opted.'”
The article pointed out why. Robert is married to the psychologist he wrote his book “Psychiatry Under the Influence” with, Lisa Cosgrove. And psychology and psychiatry both believe in the same “invalid” psychiatric DSM “bible.”
But thanks, old head, for helping to educate those of us new to the ‘movement,’ on the history of the ‘movement.’ And, just an FYI, that movement has to be against all the psychiatric, psychological, therapist, “mental health,” and social worker, psychiatric DSM believers at this point, not just the psychiatrists.
All psychiatric DSM “bible” believers and billers are now the problem.
Report comment
Thank you for the shout-out, Someone. So much is going on that I haven’t had a chance to check back here since I posted the above. And now I hear that complaints from a shrink have resulted in Phil Hickey’s response to all this being pulled from the site. Whoever is behind this it is frightening if not shocking to those of us for whom Phil is a beloved and trusted ally, and we are waiting with bated breath to see if another shoe is about to drop.
Report comment
that movement has to be against all the psychiatric, psychological, therapist, “mental health,” and social worker, psychiatric DSM believers at this point, not just the psychiatrists.
All these are branches. Psychiatry is the root.
Report comment
Bob
In this recent paper from prominent individuals..
https://www.researchgate.net/publication/343467517_Tapering_Antipsychotic_Treatment
…It is possible for people diagnosed with “Schizophrenia” to survive successfully without “medication” but it would be recommended they withdraw very carefully from neuroleptics, as these drugs can cause weaknesses in the brains systems.
As far as I know the authors don’t recommend any methods for dealing with the “Neuroleptic Exposure High Anxiety”
– this is what’s missing from the paper.
The solutions can be found in Straightforward Psychology.
Report comment
To Shayla Love: Abolish and outlaw psychiatry for major crimes against humanity – forced drugging causing akathisia/toxic psychosis inducing suicide, violence and homicide and a long list of other drop dead and slow burn horrors. Almost all psych drugs cause akathisia plus about 200 others. The one that doesn’t is lithium which also kills big time nuking kidney function at ‘theaputic’ dose. You think we’re wrong get yourself sectioned in a closed culture of abuse prision called a ‘hospital’ and forced drugged on neurleptics, sleeping tables, and benzos due to akathisia caused by doctors in the first place, then come back and talk to us – if you survive. btw where are the comments on the piece ? Why don’t you let us have our say and why not come on here – let’s get into it ?
Report comment
Yes it would be good for some “love” here. I doubt the true stories are sought after. Make believe sells. True stories might get an Awww.
Report comment
Mr. Whitaker,
Thank you. You have succeeded in providing an exceptional defense and critical analysis to the Vice article that is being countered and I sincerely applaud you for taking the high road and citing real references, making a clear argument against and in general demonstrating the poor journalism and incredibly weak material that the Vice’s author so feebly tries to present to her readers. And you did it in a respectful manner without taking personal shots at her character – that must have been difficult but I for one noticed and just want to tip my hat to you for that.
Coincidentally I did in fact read her article before yours and had spotted some of the same bias/baiting problems and unsubstantiated claims in it that you so eloquently laid out here – Her ‘piece’ disappointed me in so many different ways because it completely failed to capture what the true nature (speaking from personal experience) of what a conventional norm critic of psychiatry is really all about: the patient above all should have a voice and support to get them through what they are struggling with (just like any other patient who presents with something visible like a broken arm for example). One thing that I deplore is how much our (in the US) society stigmatizes those with mental illnesses, trauma, and disabilities – I cannot overstate how systemic and rooted it is yet how disastrous it is for the person and their caregivers to experience. Even if your condition is invisible (as is the case with most psychiatric disorders) it does not mean the impact to your life or your suffering is any less so.
In navigating each of our own individual struggles as they inevitably occur in each and every one of our lives – I always find it helpful to remember to think of at least one or two or more positive things about anything and everything in our lives that brings us into the present – and with that I would say (as yourself and others have also noted) that its not all bad though – as unpleasant (if I may) an experience this may have been – you have gained another follower and user on your platform, with personal exp and another perspective to share… and you can be sure that I will spread that spark to others as well to keep this movement alive and well.
I find comfort in knowing you and your team are part of a larger effort to redefine this part of our society – by all counts we will need more and more like yourselves going forwards. The things I have begun to read and encounter on your site almost immediately resonated with me – I can’t begin to describe my joy in finding this not just for myself and my family but for all others who need this community to listen and be heard as well. With content like this, you can be sure that I (and I hope others/we) will be behind you and with you backing you up, be that visibly or not. Thanks again – your dedication and generosity is very much appreciated.
Report comment
Well neuronymous,
“One thing that I deplore is how much our (in the US) society stigmatizes those with mental illnesses, trauma, and disabilities – I cannot overstate how systemic and rooted it is yet how disastrous it is for the person and their caregivers to experience. ”
Psychiatry was borne out of that stigma and bias. So if you hear psychiatry talk about “stigma”, remember it is a smokescreen to the easily impressed, when what they are really saying “look at all those bad people looking down on our poor “mentally ill”. (when most things people see are actually drug effects)
Who defines “mental illness”? Who labels it? Who drugs it into oblivion and kills? They simply created a job out of bias, prejudice.
And welcome. 🙂
Report comment
Multiple studies have indicated that the process of telling someone they have a “Brain disorder,” or telling someone else that “mental illness” results from brain malfunction, increases “stigma,” in contrast to telling people that it is the result of struggling with difficult life experiences. So a large percentage of the “stigma” is the result of the very psychiatric system that later decries it.
Report comment
The notion that I was hopelessly insane almost drove me to suicide.
Psychiatrists see only “bipolars” and “schizophrenics.” I see human beings.
Psychiatry exists to make a distinction between the “normals” with full rights as citizens and human beings and the “severely mentally ill” creatures who can be viewed as incompetent idiots (regardless of demonstrated cognitive abilities) or dangerous criminal masterminds (regardless of the content of our character.) Or both. Whichever psychiatrists–and any “normals” who know how to exploit us–find convenient.
Report comment
“Multiple studies have indicated that the process of telling someone they have a “Brain disorder,” or telling someone else that “mental illness” results from brain malfunction, increases “stigma,”
That may be so Steve, but in principle there is nothing wrong with having a “disorder” of any kind, period.
Report comment
It is true, we ought not to think less of people regardless of whatever struggles, physically or psychologically or whatever, they may experience.
My point is that how a problem is framed has a lot to do with what people believe can be done to resolve it. The placebo response is a perfect example – if people are given hope that they will improve, they can often rally their internal resources and they actually DO get better without intervention. This is particularly true of so-called “mental/emotional disorders.” Telling someone they’ve “had a rough childhood but that other people have experienced the same and have overcome it, let me connect you with some of them” will give the person both validation and hope. Telling someone their “brain is genetically defective and they’ll have to take drugs for the rest of their lives to deal with the symptoms, but there is no cure” removes agency and blunts hope. Since the latter has not been shown to be true in the overwhelming majority of cases, why would we not start with a framing that provides hope and agency, rather than one that promotes hopelessness and passivity?
There is a reason psychiatry frames things the way they do, and it has not much to do with helping people achieve better control of their lives.
Report comment
Hi Steve,
I cannot reply directly to your comment so I will just briefly reply here to my own but in principle I don’t think having a disability of any kind should promote these things. I think ableism and oppression does which can occur in movement spaces by well meaning people.
Pointing this out does isn’t an endorsement of psychiatry’s corruption. This is going to be my final comment. Thanks.
Report comment
I don’t think we really disagree with each other much here. I think we’re just emphasizing different aspects of the problem. Being biased against someone for differences is certainly not something invented by psychiatry. They just tend to make it a lot worse, and then blame others for their poor outcomes.
Report comment
Perhaps it is wrong to call something or someone “disordered”, unless of course it’s my neighbour, in which case I can tell him it’s okay, don’t be ashamed, it’s not wrong to have a “disorder”, even though the “disorder” was a made up disorder.
It is like a scientist curiously observing space and naming it chaos. There is definitely something “wrong” with making up names for people, especially if those names cause people to become that in all liberties extended to the “normal” population.
Report comment
I know I felt a hell of a lot worse when I believed I had multiple brain conditions that would never go away versus the notion that, at the end of the day, thoughts are just thoughts and that I didn’t need to give all this power over to my “bad” ones.
Like, multiple therapists and psychologists encouraged me to think of the “illness” as an invader in my mind, like a ghost that will permanently haunt me and who I had to grapple with for power over my own mind. That I had to be constantly vigilant and fighting it off or else I would “lose” and my “disorders” would become worse.
Report comment
Wow, anthropomorphizing your “disorders” as evil entities to be battled but never defeated! This takes disempowerment to a new level!
Report comment
Lightbulb, that is how they try and destroy. It is the weirdest obsession that psychiatry has, to knowingly hurt people. I’m so sorry they lied to you.
Report comment
I had a therapist who relied on the anthropomorphism for most of my treatment with her. To the point where it had a name (“It”) and characteristics (tall humanoid being composed of shadow, very much male in nature).
Most of my time was spent fighting “It” and losing. Because there was no way for me to really “beat” it once and for all.
Report comment
It is tough to fight a metaphor!
Report comment
I thought after the first post that it sounded like the plot from the Tarkovsky movie Solyaris. Now I’m pretty convinced it was a George Clooney fan after the remake was released lol.
$200 worth of quarters would go a long way to “beating” “It” in a pin ball parlor. And like a therapist you’ll be back next week to spend another $200.
Awwww now I got a Michael Jackson song stuck in my head.
“It is tough to fight a metaphor!”
Kick it in the analogies. Sink the slipper in it’s simile.
Report comment
“Multiple studies have indicated that the process of telling someone they have a “Brain disorder,” or telling someone else that “mental illness” results from brain malfunction, increases “stigma,” in contrast to telling people that it is the result of struggling with difficult life experiences. So a large percentage of the “stigma” is the result of the very psychiatric system that later decries it.”
The ‘crossroad’ lies in the attribution of cause.
Internal attribution (ie the brain disorder) results in the search for the right drug and then how to ‘tweak’ the cocktail for best effect.
External attribution (ie you were sexually assaulted for years by a priest at the institution you were raised in) results in the search for a way to cover up the abuse and ensure the perpetrator is not brought to justice.
Enter psychiatrist and Internal attribution, your brain is broken and here’s some drugs to shut you up. Oh, and here’s some stigma for you to try and overcome, and which will ensure that your right to access to legal system is guarded by the gatekeeper we have now assigned to you without your knowledge, your ‘carer’.
Martin Seligman whose work was used to induce helplessness at Guantanamo is a good start at understanding the damage that is being, in many cases, deliberately induced in “patients”.
Want to understand why there is what seems to be a significant correlation between teenage suicides and the amount of money provided for ‘care’? (What is the Pearsons r on this?) It’s basically got to do with the fact that the more money you provide, the more people are being made sick. Beat that donkey Balaam.
Report comment
Anyone who presumes to “define mental illness” is heading down the wrong path from the start.
Report comment
“That aspect of our site is designed to give voice to a community of readers, and given that many in this community had horrible experiences as psychiatric patients (or were forcibly treated in hospitals), you can find such sentiments there.”
At the heart of this is the delusion that proponents of psychiarty are rational and non emotional, while its critics are irrational and emotional.*
It is delusional for two reasons:
1. Psychiatrist are not unemotional. Critics of psychiatry being right would turn their life into a lie and make them criminals of the worst sort. Psychiatrists can not face this.
2. Critics of psychiatry are not irrational. It is the critics of psychiatry interpreting the data in a rational way. I.e. forced deprivation of liberty in case of suicide risk. Someone feeling better and becoming less suicidal by being locked up against their will is a very strong claim and counter to common human experience, therefore it would need strong evidence to support it. Alas there is none. Yet “experts” claim it’s the right thing to do.
*That’s tied into the sexism of man=rational=good and woman=emotional=bad. But that’s taking it too far here.
Report comment
“Critics of psychiatry being right would turn their life into a lie and make them criminals of the worst sort. Psychiatrists can not face this.”
Al Capone could, why not a psychiatrist? Kicking back on my yacht in the Bahamas, Cuban puffing smoke and a 600 year old snifter of Brandy, all paid for tax free by a drug company. And I’m going to worry about my life being a lie? It’s a pleasurable lie, and my conscience is clear.
The politicians that have been corrupted have created laws that allow my conscience to be clear. While one might look in an etic fashion and consider these ‘treatments’ to constitute torture and kidnapping, it is known from an emic perspective that the laws make that not so. It is “inherent in or incidental to lawful sanction” and as such is NOT torture or arbitrary detention. The National Socialists were quite good at this, in placing people by definition outside the scope of justice, thus allowing them to be of the opinion that they were ‘just doing their job’.
Oh, and should the State actually start torturing and kidnapping citizens, they could of course conceal those acts by making the citizen into a “patient” post hoc. Who would have thought that getting around the Convention against the use of Torture would be that easy? Think your protected? Ask your local politician where you make a complaint regarding the use of torture by Police or Mental Health Services. I think the non answer might surprise you. Complaining about torture is a mental illness you will receive ‘treatment’ for in the Emergency Dept. I do like the euphemism of ‘unintended negative outcome’, though the lack of a confession does not mean it was not intended. It simply means you will never reach the standard required for a prosecution (means, motive and opportunity, the motive being the card that disappears in the three card monte). Our Head of the AMA telling us that this requires a “sophisticated knowledge of the law”. Even Mr Capone could have told you to keep your mouth shut and there’s nothing they can do about it, though the ability to torture and conceal it as medicine does open up opportunities for law enforcement. If only they could find their copy of the Criminal Code.
Report comment
Thanks Robert, excellent article without having to defend yourself.
And that is the beauty of your intellectual honesty within your journalism.
It is ironic that a few or one person rather would use phrases such as “distort the scientific record”
“Finally, I hope that deconstructing this article—and revealing the journalistic standards that are on display—helps reveal the depth of the challenge for those who would like to see “psychiatry reimagined.” Unfortunately, this struggle is regularly hindered by the fact that media are often poised to report in ways that protect the conventional narrative, and look askance at those who would challenge it. But as is the case in any struggle, it’s always good to know what you are up against.”
I can assure you that you are most likely agreed and supported by far more in the biz than you know. But as you can see, once one stands up, everything will be done to try and discourage the public from thinking or rethinking. So it is not in the best interest for the “professionals” to come forward and show themselves. There is no truth in journalism if we do not ask the consumers, and you are the only journalist that was interested in digging deeper.
And this article prompted me to donate btw.
Report comment
There is, of course, nothing wrong about people criticizing MIA or me personally. The criticism can open the door to further discussions and debate, which you can hope will lead to a greater understanding of important issues.
Bob,
find a way to enlarge the circle of family members allowed to contribute at MiA. Thus far the only family I’ve seen allowed to contribute are those whose loved ones were caught up in the system. Why are their voices allowed, but those of us who have fought 24/7 for years to keep our loved ones OUT of the system are not allowed to share how we did so? Is the audience at this website, only and solely, composed of those caught in the system other than me? Is there really no interest in empowering families and SO’s to keep their loved ones totally out of the system?
Sam
Report comment
Posting as moderator:
Anyone who wants to post here is allowed to post, as long as they follow the Posting Guidelines. We have never moderated family members who chose to participate based on their being family members or on their not having a family member embroiled in the system. It is true that some of our community distrust family members’ intentions, based on their own experiences. But family member voices have always been welcome at MIA. I’m not sure where you are getting the idea that family members are “not allowed to post” if their loved ones are not caught up in the system. What would stop such a person from posting?
Report comment
Steve,
I’m not talking about the comments section, and I don’t want to say more because I only kind of get things 2nd hand, and I don’t really understand the objections as I’ve seen other family members have blogs published, so maybe it’s just me, specifically…
Sam
Report comment
Thanks for the clarification.
Report comment
Sam, I have been allowed. I am in a church, but a different one from yours. We fight to keep people, especially kids, out of the system. (I myself only drifted near the system for a short time.) But, alas, my church is looked down on these days. Many traditional churches are also under pressure. And so our larger “family” is being encouraged to splinter and fight among ourselves. Too bad. Shouldn’t we all be working together on issues like this?
Report comment
Great rebuttal of what was really a dreadful hit piece from Vice. Disappointing that the author didn’t interview Dr. Whitaker while developing her article, and only sought a response late in the writing process to Whitaker’s critics whom she had granted interviews — this does not comport with the process I was taught in journalism school (in the halcyon days of…2008). Besides that, the author seems to have limited subject matter knowledge, and was probably the wrong choice to assign the piece in the first place. It appears Vice hasn’t changed much in the past decade even as they’ve expanded their breadth and scope of reporting and embraced the aesthetics (only just) of social justice; work like the article in question evinces poor editorial oversight and questionable staffing practices, problems which have always plagued the rag and clearly do still. Oh well!
I’d like to add my voice to the chorus thanking Whitaker and MIA for providing this platform. As I no longer have institutional access to academic journals, I come here primarily for research news, but the blogs (and comments!) are a breath of fresh air even if I don’t always agree with everything in them.
Also, this is a bit of a long shot, but Google has been no help in this: does anyone know of a site like MIA, but focusing rather on critical perspectives on drug policy and addiction treatment?
Report comment
Thank you Robert Whitaker for continuing to fight to show the evidence of the effectiveness of the psychiatric drugs over time.
Yes the psychiatric medications used to be called neuroleptics, and they should be continued to called neuroleptics because if you personally have not been forced to, coerced to, or willingly have taken the drugs, you do not know the effects. The term “Anti-psychotic” medicine makes the “chemical lobotomy” palatable to the person who has not taken the drug.
Advice to the recovering schizophrenic in regards to the chart “Psychotic symptoms in schizophrenia” 23% VS 79%. What is psychotic? It means different things to different people. Today we have digital cameras. Get one and photograph your psychotic symptoms.
It is not surprising to me that being tied up for 15 years makes it unlikely to recover. A person needs a fully operating brain for a mind to work.
And they want the frog to work after they cut off its legs? https://lowres.cartooncollections.com/animals-amphibians-frogs-frog_s_legs-restaurants-animals-NL700109_low.jpg
Report comment
Once I discovered the hoax about the “chemical imbalance” I look back on what I’ve been through with anger.
The drugs which were supposed to prevent cognitive deterioration (according to my doctor) did the opposite.
I frequently beat up on myself for my inability to find gainful employment, have decent human relationships or keep my house clean. Now I can do all the three.
They were forcing us to hobble around with our feet in fetters and ridiculing us for not running laps like they could. (Clubhouse/Day Treatment/NAMI) Disabling us while pretending to help us.
NAMI
National
Advocates for
Munchausens-by-proxy
Iatrogenics
Report comment
I too can ” look back on what I’ve been through with anger.”
and this anger at the injustice can be named “psychosis” by those who claim to be helping with “medicine”.
So I must forgive , but not forget, and be grateful for what I still have.
Report comment
Yes. I mustn’t live in the past or might-have-been but what is.
Report comment
I was going through some second hands books at a store today Rachel and came across one called Mrs Frisby and the Rats of NIHM. And then I came across a t shirt that says
Tyler Durden for President.
It’s only after you’ve lost everything, that your free to do anything.
So I picked a fight with the shop keeper and got them both for $5 lol
Report comment
I remember the rats of NIMH — never read it though.
Report comment
NAMI
National
Advocates for
Munchausens-by-proxy
Iatrogenics
lol
Report comment
LOL!
Report comment
In the scale they use for studies for neuroleptic drugs, psychotic symptoms include: suspicion, grandiose thoughts (so disagreeing with the psychiatrist), excitement, and hostility. Don’t even need hallucinations, delusions or disorganized thinking to score as psychotic. Though since it is all subjective disagreeing with psychiatry can be a delusion.
In SSRI and drug studies used for depression/anxiety the person going from saying they are not ill to saying they are ill produces a larger “benefit” than the total short term drug benefit. No need to even address that these studies are cherry picked withdrawal studies because when you know what they define as “better than placebo” you realize the drug is worse than worthless.
Report comment
So Willowweed,
It seems then that the psych industry is psychotic?
And I had always known that really we were dealing with projections and bias. Founded on the crazy that represents humanity. It was actually psychiatry that gave me a more realistic view of just how crazy one can be and try to be immune to being seen as part of that fabric. Just how delusional people can get in their beliefs.
Report comment
“psychotic symptoms include: suspicion, grandiose thoughts (so disagreeing with the psychiatrist), excitement, and hostility. Don’t even need hallucinations, delusions or disorganized thinking to score as psychotic.”
I hope someone noticed that our Premier is acting a little strange lately. he claimed that he was “ambushed” by our Prime Minister recently without any evidence. And of course without any proof, all he has is a paranoid delusion.
He has also decided to sue a wealthy businessman for comparing him to Adolf Hitler (hostility), and has already spent the money he is claiming (mania?). Which is a real concern because the best defense from being sued for libel/slander is that what you said was the truth. Surely Mr wealthy businessman would only need to present evidence to the court to support his claim such as the Euthanasia Act they have passed? I mean this would be considered plagiarism translating something from German to English and then claiming it as your own work.
How embarrassing when the court decides it was a fair comparison to make. And this got me thinking, who did people compare Hitler to in his time? Did they say things like, “He’s as bad as Vlad the Impaler”? “Is he related to Cesare Borgia?” I get it that he turned out to be in a league of his own but ……. surely people made comparisons?
I did like the comment from one opposition member who commented about the frivolous/vexatious litigation being brought by the Premier when he said “I didn’t realise we had elected a Princess for a Premier” waaahahahahahah. ‘we’ll be seeing you in Court for that’. I mean, who could be offended by being called “princess”?
Perhaps his paranoia is justified. Maybe they really are all out to get him.
Report comment
From the Vice article, a statement by Nev Jones:
“Yet Jones said that in the time she’s been involved in pushing for better mental health treatment, she has seen increasing polarization, and much of that she contributes to Whitaker and his work. She gets contacted by parents semi-regularly who have read Whitaker’s books and then refuse to let their children start or remain on anti-psychotics—even in cases where medications were working well and the young person wanted to continue with the medication. “This is not at all getting away from coercive relationships,” Jones said.”
And then from the blog on this site, a conversation between her and Sandra Steingard:
“And overall, there’s so much we don’t know, so much we don’t understand. So, acknowledging heterogeneity, acknowledging a very high degree of uncertainty about just about everything, including ways of addressing long-term disability—I personally see this as the necessary starting point of any discussion. Instead, at least at the time, I think it was common to see Open Dialogue deployed as a quasi-magical bullet and means of (for some people literally) eliminating psychosis. And likewise, I felt that many people took up Anatomy as ostensible proof that antipsychotics were the primary cause of sustained or chronic psychosis (through supersensitization) and also that the case was more or less settled with respect to long-term iatrogenic harms.”
I find this particularly misleading to bring up heterogeneity, and then try to discredit so much that truly brings in information and methods that otherwise would be dismissed and/or overlooked. That way anything that might dissuade a person from mainstream convenience or practice supposedly gets in the way of heterogeneity, despite the whole play on words, and the catch phrase “acknowledging heterogeneity.”
Open Dialogue and Healing Homes of Finland have been shown to work; and they should be tried, should be allowed to be tried out in the USA without prior discriminatory fabrications. The reason they haven’t been tried is because they would go against the mainstream biological model of mental illness, its ideology the unproven chemical imbalance; anything contrary to that is, as we hear again, called a fantasy, is made out to be unrealistic. Methods that work should be tried before anyone decides whether it’s a “fantasy” that they would work.
And those methods really aren’t anything like:
“Well, we have these “medications,” that don’t really work in the majority of cases, but we promote that to be the case when they work for an interim, although afterwards there’s more disability, more relapsing, loss of life, side effects, withdrawal symptoms and fear of symptoms that might otherwise have been experienced and understood so that they quiet down or dissolve altogether. There’s also a spike in the diseases these medications are said to heal, along with the added disability, more relapsing and the other things I already mentioned. And we say it’s treating a chemical imbalance, but really causes one by disabling the mind, which we also see as healing, although we’re basically lying to you, but that’s to get you to take your drugs. Now beheading someone also alleviates psychiatric symptoms, but we find the side effect of death a bit too severe, although the medications, for say psychosis, do in general take 20 years off of your life expectancy disabling your mind, it’s not the sudden death as in beheading, and so we can disable that little noggin up there and keep you alive for awhile, although there’s loss there. OK!?”
I also find it distressing that a clinician would go against parents that were responsible enough to read non mainstream material, gain information that’s more accurate than they were told, information that was suppressed: in fact information that would their child end up in the mental health system and put on such medications, would the child themselves express the scientific truths of how the medications aren’t really treating a chemical imbalance and how the medications are causing iotragenic harm, the child could be seen as non compliant and forced on the medications. To read that Nev said she’s disturbed by parents taking their children off of medications, she says were working, although statistically those medications if they are helpful are only helpful for an interim, and people do better to get off of them eventually, Nev also mentioning that people then also don’t want to try medications that can be extremely difficult to get off of, and cause further problems, as if there’s something wrong there: that further makes me question what’s going on. It also sounds to me that Nev has convinced some of her clients that the drugs work, saying that children don’t want to get off of the medications, and then goes against the parents, even when they don’t want the children to start on the medications. THAT, in fact has caused children to be taken away from their parents. Parents who are dilgent enough to do research beyond the boundaries of standard treatment propping up Wallstreet games, corporate media control, and it’s “economy.” Mindfreedom has two such stories of children that their parents took to the ER, the children were understandable distressed about a physical condition, then advised to try an anti-depressant, and the parents simply stated the scientific truth about such medications, which then was seen as a danger to the children (to know the truth, what’s shared in for example Robert Whitaker’s books); two different mother’s lost their daughters to being institutionalized for simply expressing the scientific truth about anti-depressants. And it also was the daughter’s own choice to not go on such drugs. And with the amount of med students on anti-depressants https://www.idealmedicalcare.org/75-med-students-antidepressants-stimulants/ and the propaganda that’s indoctrinated, it’s not unreasonable to wonder how many nurses and doctors there are that think that such dangerously addictive substances should be administered when there’s normal distress that would go away with proper medical help for a truly physical conditions, which is why someone would go see a nurse or a doctor. In fact that’s happened with someone I knew. A lady came to the US from an East Block country, had been promised work, that and some paper work that should have been cleared weren’t for some bureaucratic reason, and she was left without work, and the distress about that. THEN she had to deal with some nurses who promoted anti-depressants, but the lady had a mother that was a nurse back in her homeland, and the mother had diligently studied the truth about anti-depressants and was wary about that, so the lady said she didn’t think that was a good idea, and probably shared some information that then caused the nurses to start becoming vigilant against her, and her children were taken away from her, basically because her house wasn’t as neat as they felt it should be. The lady was quite responsible and clear in her head, she just had a lot going on and her house was a bit messy, which it often is with children, and she went against being advised to to on anti-depressants.
Since I’m going on about such stuff, involving paranoia and the mental health system. I also ran into a woman out of nowhere at a bus stop about a decade or so ago, started talking to her, and found out she had been hauled across state lines and put in jail, in my city again, because social workers had talked to her mother, and the mother had accused her of stealing her money. The truth actually being that the mother at one point could have ended up in jail but the daughter decided she should be looked at by the psychiatric division to avoid being put in jail; the mother apparently was treated and then went back to live in her house but took an alcoholic in with her there, she could have lost the house, the daughter put her whole 401K into the house with a reverse term mortgage, but the mother managed to mess that up as well; ended up somewhere in a foster care or so, and then accused the daughter of something she hadn’t done at all, and the nurses believed that. The nurses or social workers believed that the daughter had stolen her mother’s money, when in reality she had lost her 401k trying to help the mother, that managed to still lose the house the 410k of the daughter had prevented from being repossessed at first. The poor daughter wasn’t allowed even a credit card when the police picked her up with several SUVs, was hauled across state lines, held in jail overnight, then had to talk to a judge on video camera who said: “you’re fine, you just have to do some paperwork, you can go home,” where upon the daughter asked how she was supposed to do that, she had no credit card or ID? The judge said that was her problem, and then I happened to run into her after she went to see if friends of hers were around, using her last change for a bus ride; but her friends were on vacation or so. I actually gave her money for a bus ticket, which she returned to me as soon as she got home, by sending me a money order; I helped her find a center for women where she could spend the night before taking the bus, and prevented her from losing her job because she couldn’t get home in time. All of that impossible situation because the nurses again think something is going on, and wouldn’t care to find out beyond that.
And who is prone to believe in fantasies!?
Report comment
Ouch! I am sorry Robert Whitaker for the disappointment I share with you about the state of journalism; the corruption of a journalistic ethic that you describe is staggering.
Although I agree with much of Oldhead’s criticism, it seems like a heavily edited version of this blog should be widely published as a query about the state of journalism elsewhere.
Report comment
Yes, I agree Steve S. It’s disturbing the state of journalism standards and ethics have gotten so low that Shayla Love and VICE publish what is in my opinion irresponsible, unvetted and biased propaganda.
My deepest appreciation and respect goes to Robert Whitaker for his high standards, integrity and community service. Thank you Robert for your perseverance in forging ahead to uncover and speak the truth to try prevent harm and save lives. Please carry on, your exemplary work and journalism is greatly needed.
“In a time of deceit, telling the truth is a revolutionary act.” — George Orwell
Report comment
“In a time of receipts, telling the [redacted] is a remunerative act”
I still shake my head at the standard of journalism where I live when I think about the article that assisted in getting the changes required to open up ECTs for use on children here.
Speaking of shaking my head, ummmmm what happened to Doc Hickeys article, or are we ignoring that for now?
“To learn who rules over you, simply find out who you are not allowed to criticize” Voltaire.
Report comment
I still think the article has given some credence to our thoughts. This is vastly different from what I’ve seen on other sites. I understand the anger and revulsion completely. But I also understand the author’s point of view.
Report comment
“That puts the critique in Anatomy into the ‘overmedication’ category, which would make it a critique of prescribing practices, rather than an investigation of the merits of the drugs.”
Robert, since you are largely the speaker for all those of us whose concerns are unworthy of hearing, according to psychiatry. Please feel free to utilize my medical research finding, that all doctors are taught in med school, that both the antidepressants and antipsychotics/neuroleptics (both anticholinergic drugs) can create “psychosis,” via anticholinergic toxidrome, aka anticholinergic intoxication syndrome.
https://en.wikipedia.org/wiki/Toxidrome
https://www.drugs.com/interactions-check.php?drug_list=1744-1113,2330-1540&types%5B%5D=major&types%5B%5D=minor&types%5B%5D=moderate&types%5B%5D=food&types%5B%5D=therapeutic_duplication&professional=1
I will say that the head of family medicine at the Cleveland Clinic was so impressed with my medical research, and he agreed with it, that he called me a “one in a million” medical researcher. And he had me teach one of his students that now that we all live in the information age, “sometimes the patients will know more than the doctors.”
Those of us who are critical of psychiatry are NOT merely discussing misdiagnosis and “overmedication,” which does happen frequently. But we’ve also found the medical proof that the psychiatric drugs create “psychosis,” via anticholinergic toxidrome, which is not even listed in the psychiatric / “mental health” workers’ DSM “bible.”
So the majority of the “mental health” workers are ignorant of the fact that the psychiatric drugs do create “psychosis.”
Report comment
So let’s summarize what just happened here.
Members of this community talked to this journalist (who is by no one’s assertion anything close to a content expert in this area) for god know’s what purpose? Promoting some neoliberal non-profit garbage, perhaps.
And now, Whitaker has spent god knows how much time and effort to show the journalist he knows more than she does about the topic. Because the article made this blog look stupid.
In the meantime, has anyone noticed it is 1938 Germany-ing outside? Who were the first ones to get the gas? Oh yeah. You all need to buy a clue.
Report comment
“In the meantime, has anyone noticed it is 1938 Germany-ing outside? Who were the first ones to get the gas? Oh yeah. You all need to buy a clue.”
https://www.youtube.com/watch?v=Feg6rS70o1Q&t=191s
We did try to pass a clause in our new Mental Health Act to allow the forced sterilisation of children without parental consent, but it was removed after ‘outside influences’ started making noise. There is little doubt in my mind who this clause was to be used against, and it really was based on racial grounds (see Foetal Alcohol Spectrum Disorder [FASD] and the statistics of who is most affected by this). This failure, and the success of the passing of a Euthanaisa Act (what was termed in the German sense as being a ‘wild’ or decentralised Euthanaisa) a concern for the community.
No discussion of this law being introduced before the election, and a simple claim that more than 90% of the population wants it (no data produced as proof), and it was done. They do seem to want to follow up and ensure that any comparison to the laws passed in Germany would be a criminal offence, and in fact our Premier is now suing a wealthy businessman for making such a claim. After they have passed laws providing them (politicians) with immunity from prosecution for ANY criminal acts.
Yup, I noticed. And might I say calling Noah mad, did not stop the rain. Did they seek a second opinion? lol
Report comment
Members of this community talked to this journalist (who is by no one’s assertion anything close to a content expert in this area) for god knows what purpose?
Hear hear! These are more the sort of questions that need to be asked.
MIA is not part of the “movement against psychiatry” in the first place, by its own admission; it is a site dedicated to “critical” psychiatry. Though its opponents in the psych industry portray it as “anti-psychiatry” this has never been the case. Questions about the actual movement against psychiatry should be addressed to those who are part of it.
Report comment
Getting back to the quote above — everyone here needs to understand the institutional role of the media better, as well as the priorities of reporters. There is this recurring illusion that some reporter somewhere is going to see the light and “break the story” about psychiatric fraud. Why do you think that hasn’t happened yet?
So yes we need to exercise responsibility before giving interviews to opportunistic “media” just because they’re there (or because we want to see our names in print, which is a dangerous ego fixation).
Report comment
It hasn’t escaped my notice, and I would guess others are also aware of the current situation. How would you suggest we focus our efforts since what we are doing now demonstrates cluelessness?
Report comment
Well, really, anything, or even nothing, would be preferable to the current state of “activism” in this community. In fact, nothing (literally) might be preferable because it would stop all the “peer” co-optation, the “critical clinician” nonsense, and especially the “dissident practitioner” garbage. It is my understanding there are different flavors of anti psychiatry now, similar to anarchy and coffee I suppose? A proactive suggestion would be to bun the system to the ground, I suppose. This community has been hell bent on its own destruction for years, but god, it is worse than it has ever been. YAWN
Report comment
Yep – very good first and second comments !
“In the meantime, has anyone noticed it is 1938 Germany-ing outside? Who were the first ones to get the gas? Oh yeah. You all need to buy a clue.”
Been making the link for sometime here and have noticed Healy blog has started to as well. Was going to kick off again on a Phil Hickey post on all this but Robert seems to have pulled Phils post…. why ?
Can’t see wood for trees comes to mind….
Report comment
“Can’t see wood for trees comes to mind…”
Voltaire once wrote: “To find out who rules over you, simply find out who you are not allowed to criticize.”
Report comment
Anti-war activists work to end war. Anti-racist activists work to end racism. And anti-psychiatry activists work to end psychiatry!
There is only ONE primary flavor of anti-psychiatry — the one that actually wants to rid the world of psychiatry for good. Those interested — anti-psychiatry survivors in particular — should give us a shout while you still can: [email protected]
All else being equal however I’ll take chocolate pecan.
Report comment
I haven’t read far into the article yet but I figured I needed to comment already. Jeez, just when I felt the tide had turned and the revolt was underway and would be as fast as the civil war at hand, sigh… I’ll read the article.
Also to people who know me, I was in a car crash, triple ankle break, broken back, ribs… and in the war on opioids. Yay.
EDIT: both these articles are long and I’m in too much pain to focus. I should be taking 4mg dilauded ooral or 1-2mg iv every 3-4 hours with 20mg of norco every 4-6 hours (I have a history with surgeries and drugs pre and post war on opioids), instead I have 5mg of norco every 6 hours and for only 3 days and aspirin and tylenol.
Anyway, if I survive this, and I’m not holding out hope, then I will comment in the coming weeks. Try to do something with my story if I never return, blahblah.
Report comment
Okay after reading this; MIA is a non-profit. I think MIA should sue for slander and whatever else it can. I think MIA should start becoming aggressive one way or another, or in every way actually.
Also, I am very happy to hear that Whitaker is married to Lisa Cosgrove, as I imagine this is something positive that has occurred in his life during this “intellectual journey”, but what business does vice have of even mentioning it?
But back on the topic of aggression; why doesn’t MIA join MSM in some regards and go on attacks? Why isn’t MIA investigating the personal lives of Jeffrey Leiberman? Did Joseph Biederman sexually rape any of the children whose lives he destroyed with forced drugging induced brain damage? Has anybody bothered to find and interview these now-adults about how they were treated at “bader-5” and in his studies? I could go on and on…
Report comment
Robert, your analysis of the Harrow study provided inspiration for one of my early cartoons:
“Recovery begins with non-compliance!” http://www.auntiepsychiatry.com/Auntie%20Psychiatry.html#Rebel
This is not my slogan, I borrowed it from the early anti-psychiatry freedom fighters, but it rings truer today than ever.
David Healy explains why in his latest blog…
“An old phrase comes to mind – first, they came for a bunch of us with nothing wrong with us and hypnotized us into taking chemicals for risk factors, then they came for our teenagers turning those who don’t kill themselves into eunuchs, male and female, and now – well if you’re sleeping soundly good on you.”
Non-compliance is a healthy act of human resistance, a forceful way to kick back against the corrupt powers-that-be. Right now, our leaders are pleading with us to comply with their dehumanising and degrading demands to muzzle ourselves in public and deny our innate need for human contact. If, like me, your instincts are telling you this is deeply abusive and inhuman, then refusing to comply is a powerful way to re-assert your autonomy.
Recovery begins with non-compliance!
Report comment
Brilliant.
Psychiatry is a crime scene, MiA is now looking like a smoke screen.
Report comment
They would argue (I am assuming) that non compliance would be “kicking against the pricks”, they being the embodiment of Jesus and the ‘pricks’ (ox goad) being psychiatry.
The argument has some merit.
Though I think that what the work of people like Mr Whittaker shows is that they are not only goading the ox, but poisoning it, hamstringing it, and engaging in all sorts of conduct not conducive to productive work, but in the soul interest of hearing it cry out in agony. I think at that point it becomes apparent that the person in control of the prick has lost their moral compass, and is more deserving of the goading than the ox (a lesson Balaam was fortunate enough to learn. Some not so fortunate, and it only shows in their eyes when it’s much too late).
But it is so nice becoming drunk with power, that is until they see the writing on the wall. mene, mene, tekel, parsin
https://www.youtube.com/watch?v=OnhBp16nBs8
Here, take these before we run away
The keys to the Gulag.
Report comment
They aren’t Jesus. But they love to play God and take on the role of Messiah.
Only instead of offering themselves up to be crucified, they expect us to allow ourselves to be. Voluntary would be nice–but not essential. Actually that makes us martyrs…or is that unwitting test subjects?
“You need to suck it up. We all have to make sacrifices,” says the doctor making a 7 digit income off those like you, driving his luxury car off to one of his million dollar mansions. After successfully destroying your livelihood, adult independence, ability to feel happy, and all your ability to have ordinary human relationships. Ain’t doctors swell?
Report comment
And consider, these are people who hate your Nation so much they have found ways of perverting your Constitution, and are being allowed to do so by others ensuring that the Rule of Law is not applied to these people. (think about questions of law being referred from an Attorney General to a Minister for Health. They can not possibly allow these questions to be subjected to logic and reasoning, in as much as the National Socialists couldn’t. The flawed logic would not allow a “just doing my job” attitude)
Police can’t lock you up or charge you for refusing to answer a question, your Miranda warning and 5th Amendment rights see to that. Not so with psychiatry, your refusal to answer a question is seen as justification for locking you up and force drugging you with chemicals with little or no medicinal benefit until you DO answer the question.
Consider, in my State they now have a means to have you forced into a confession (psychiatric interrogations with police present) which can then be used to remove all of your property. Not that it is being used on wealthy individuals who can afford to access legal services when subjected to vexatious and frivolous litigation…… for now. They started small in other places too, but the big bucks have got to be like blood in the water to a shark.
And I thought Americans would have been upset about that great document being thrown into the trash, No flag burning but …… tear the Constitution up and you can be
“the doctor making a 7 digit income off those like you, driving his luxury car off to one of his million dollar mansions. After successfully destroying your livelihood, adult independence, ability to feel happy, and all your ability to have ordinary human relationships.”
and all done in direct opposition to the values of the Nation. By ensuring that the courts and legal system can not be accessed, lawyers are complicit in these crimes against humanity. Though I do think there is some merit in the way it is being run like a mafia (outlaws) to at least ensure some controls over the rampant abuses.
God bless America.
Report comment
We miss you Auntie, more than you could possibly know.
No matter what you do, please don’t ever take down that site — it is your legacy!
Report comment
Hugs Aunty!
From across the Pond.
Report comment
We should not forget, gentlemen, that many patients are subjected to “treatment” forcibly. Their протест is not taken into account at all.
Report comment
Great Rebuttable! I note that Ms. Love interviewed “Joseph Pierre, a clinical professor at the David Geffen School of Medicine at UCLA,” but not his colleague Dr. David Cohen!! Hence, not an investigative report, but rather cherry picked trash.
Report comment
As a psychologist in clinical practice and a trainer in alternative treatments to emotional and behavioral health that employ neither empirically validated therapies nor psychiatric medication, Mad in America and Anatomy of an Epidemic are essential reference tools. Thank you, Bob Whitaker for your unwavering efforts.
Report comment
Robert, you really shouldn’t have called my church a “cult.” That was very bad manners. You could have just said that our objections were faith-based and therefore not really about the science of the situation.
But, what IS the science of the situation? As you have ably explained, that’s not really the purpose of this forum. However, it is my purpose to point to one or more places within the realm of academia where the nature of the psyche and alternative explanations for mental distress have been explored. I usually mention Ian Stevenson (a psychiatrist!). No one yet has taken me up on my invitation to discuss the work of Stevenson’s group. Perhaps no one ever will. But it is the key work within the realm of Science that would inform this problem.
We are, it seems, hindered by certain aversions to certain data, aversions that we all seem to share. If more of us are unwilling to decide to look in those “taboo” places, I believe we face a future in which our freedoms will continue to be eroded by fearmongering, intimidation, and ridicule. You might well be accused of being a member of a “cult.” I have been. Yet, I wish to support your work. May I?
Report comment
We had a Prime Minister who called Islam a “Death Cult” l_e_cox. Funny but I like the guy, at least he has the courage of his convictions, and is not going about backbiting people while smiling to their faces and kissing their babies.
I will repeat what I said in another post regarding your church, and in line with someone of my faith (Muhammad Ali). No Scientologist ever called me psycho, nut job or window licker.
Report comment
No, you may not. I am an Asatruar of sorts (I was lead there on my own personal journey, realizing when I was 17, no indoctrination, etc), and may share a spiritual link to Wodan/Odin, therefore I can not support MIA or Robert Whitaker’s works, yet I do it anyway.
Or to put it another way; leave religion at the door.
https://ibb.co/3T1QWjS
Report comment
Jeffery C, I would guess we do not understand each other’s religions very well. Mine teaches that “mental health” should not be divorced from spiritual concerns. You see things differently?
Report comment
I was being sarcastic. Sorry.
What I mean is that, I don’t think religion should matter when it comes to issues that affect everyone, people need to come together and put aside whatever religious conflicts they may have for the greater good. I’m in a lot of pain from a car crash and it’s making me kind of wacko, so I apologize for that flamboyant comment.
Report comment
Hey, it’s OK. But this is what my religion teaches (we are non-denominational) so I’d like to see everyone join the discussion, too. That’s why I try to stress the spiritual side of the problem without naming the teaching I use. That’s one reason I mention Ian Stevenson so often. His work serves to bridge that gap.
Sorry to hear about the car crash. I’ve had those in my family. It’s good you survived.
Report comment
I love Ian Stevenson.
Report comment
What do you like most about him?
Report comment
Psychiatric drugs are nothing more than chemical straightjackets. They’re not designed to cure anyone. They’re designed to merely ATTEMPT to suppress symptoms and turn each and every psychiatric patient into a customer – for life. That’s what brings in the most profits. When my son was psychotic, and all the psychiatrists said he was “incurably” mentally ill with “bipolar with psychosis,” I finally began treating him with orthomolecular treatment. (It’s BIOchemical rebalancing – not “chemical” rebalancing – because we are BIOchemical beings.) Within 7 months, my son was 100% free of his three daily anti-psychotic Rx drugs. He found a job and began living on his own. American-style psychiatry is nothing but a racket – and there is NO law against it. The American Psychiatric Association could treat patients with voodoo, if they so chose, and that wouldn’t even be breaking the law – because there is no law to break. –Linda from Facebook, “A Dose of Sanity,” and Youtube “Linda Van Zandt’s Mental Health Recovery Channel”
Report comment